daniel jaimes albornoz mir aaborto, pérdida fetal recurrente, óbito fetal: extensos y...
TRANSCRIPT

Daniel Jaimes AlbornozMIR 4 Hematología y HemoterapiaHospital Universitario A Coruña

↑ Fibrinógeno↑ II, VII, VIII, X, FvW↑ Marcadores de trombina
↑ Resistencia Proteína C↓ Proteína S↓ Actividad fibrinolítica de
TAFI, PAI 1 PAI 2
ESTROGENOS/PROGESTAGENOS
Arterias espirales / circulación placentaria
ESTADO HIPERCOAGULABILIDAD
CAMBIOS FISIOLOGICOS EN LA GESTACION

VASCULOPATIA PLACENTARIA
INFARTOSVELLOSOS
Unicos o múltiples
INFARTOSVELLOSOS
Unicos o múltiples
NECROSIS FIBRINOIDEVASOS DECIDUALESNECROSIS FIBRINOIDEVASOS DECIDUALES
HIPOPLASIAPLACENTARIAHIPOPLASIAPLACENTARIA
TROMBOSIS DE ARTERIAS ESPIRALESTROMBOSIS DE
ARTERIAS ESPIRALES
RCF, EHE, DPP, PERDIDA FETAL, PARTO PRETERMINO

Bourjeily G, Paidas M,Khalil H, Rosene‐Montella K, Rodger M. Pulmonary embolism in pregnancy. Lancet. 2010;375:500–512
Cambio en componentessanguineos
Cambio en flujo
Cambio en paredde vasos
Rudolph Virchow 1858
Egeberg O. Inherited antithrombin deficiency causing thrombophilia. Thrombosis et Diathesis Haemorrhagica 1965; 13: 516‐30.
Mannucci PM, Vigano S. Deficiencies of protein C, an inhibitor of blood coagulation. Lancet 1982; 2(8296): 463‐7.
Schwarz HP, Fischer M, Hopmeier P, Batard MA, Griffin JH. Plasma protein S deficiency in familial thrombotic disease. Blood 1984; 64(6): 1297‐300.

TROMBOFILIA
HEREDITARIA
ADQUIRIDA SAF
FVLPT G20210ADEFICIT DE ATDEFICIT DE PCDEFICIT DE PS
COMPLICACIONESTROMBOTICAS
ETV TVP EPTrombosisarterial
COMPLICACIONESVASCULARESOBSTETRICAS
ABORTOSEHEDPPRCF
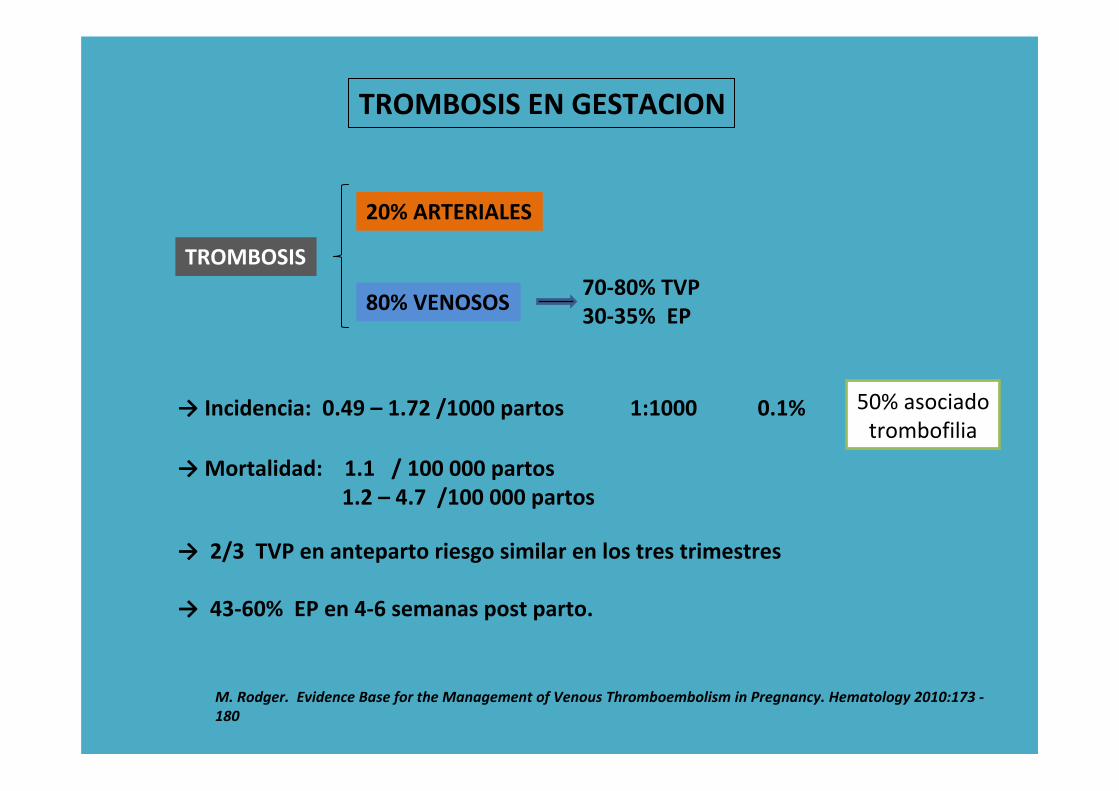
TROMBOSIS EN GESTACION
TROMBOSIS
20% ARTERIALES
80% VENOSOS70‐80% TVP30‐35% EP
→ Incidencia: 0.49 – 1.72 /1000 partos 1:1000 0.1% 50% asociadotrombofilia
→Mortalidad: 1.1 / 100 000 partos1.2 – 4.7 /100 000 partos
M. Rodger. Evidence Base for the Management of Venous Thromboembolism in Pregnancy. Hematology 2010:173 ‐180
→ 2/3 TVP en anteparto riesgo similar en los tres trimestres
→ 43‐60% EP en 4‐6 semanas post parto.

1T 2T 3T P 1s 3s 6s
4‐ 5 veces7‐10 veces
100 veces
15‐35 veces
No gestante
gestante
1ss >>>>>> 6ss >>>> P >>> 3T >> 2T > 1T
Riesgo de ETV
Gestación

RIESGO DE TROMBOSIS EN GESTACION
Factores de riesgo de ETVmas relevantes
Factores de riesgo de ETVmas relevantes
Previo ETV 15‐ 25 % son recurrentesPrevio ETV 15‐ 25 % son recurrentes
Antecedente trombofilia 20‐50 % de trombosisestán asociados a trombofilia
Antecedente trombofilia 20‐50 % de trombosisestán asociados a trombofilia
ETV gestacional: Proximal, masivo, EEII izq, influencia estrogénica.Trombosis venas pelvicas 10‐12%, 2% EESS en relación areproducción asistida
ETV no gestacional: Distal, EEII der o izq. T. venas pelvicas < 1%.
A James. Pregnancy‐associated thrombosis Hematology 2009: 277‐285

A James. Pregnancy‐associated thrombosis Hematology 2009: 277‐285

Reducing the risk of thrombosis and embolism during pregnancy and the puerperium. RoyalCollege of Obstetricians and Gynaecologists. Green‐top guideline Nº 37a. Nov 2009.

Wu O, Robertson L, Twaddle S, Lowe GD, Clark P, Greaves M, Walker ID, Langhorne P, Brenkel I, Regan L, et al. Screening for thrombophilia in high‐risk situations: systematic review and cost‐effectiveness analysis. The Thrombosis: Risk and Economic Assessment of Thrombophilia Screening (TREATS) study.Health Technol Assess. 2006 Apr; 10(11):1‐110.

A James. Pregnancy‐associated thrombosis Hematology 2009: 277‐285
James AH, Jamison MG, Brancazio LR, et al. Venous thromboembolism during pregnancy and the postpartum period: incidence, risk factors, and mortality. Am J Obstet Gynecol. 2006;194:1311‐1315.
Robertson L, Wu O, Langhorne P, et al.Thrombophilia in pregnancy: a systematic review. Br JHaematol. 2006;132:171‐196.

ACOG Practice Bulletin #113. Inherited thrombophilias in pregnancy. Obstet Gynecol 2010; 116:212.

RIESGO DE TROMBOSIS EN TROMBOFILIA HEREDITARIA
RIESGO ALTO RIESGO MEDIO RIESGO BAJO
DEFICIT DE ANTITROMBINA
DOBLE HETEROCIGOTO PARAFVL Y PT G20210A
FV LEIDEN HOMOCIGOTO
PT G20210A HOMOCIGOTO
DEFICIT DE PROTEINA C
DEFICIT DE PROTEINA S
FVL HETEROCIGOTO
PT G20210A HETEROCIGOTO

TROMBOFILIA
HEREDITARIA
ADQUIRIDA SAF
FVLPT G20210ADEFICIT DE ATDEFICIT DE PCDEFICIT DE PS
COMPLICACIONESTROMBOTICAS
ETV TVP EPTrombosisarterial
COMPLICACIONESVASCULARESOBSTETRICAS
ABORTOSEHEDPPRCF

La trombofilia se asocia a complicaciones trombóticas en gestantesy no gestantes pero…
se asocia realmente a complicaciones obstétricas?????
Aborto Preeclampsia
Abruptio
Restricción delcrecimiento fetal

Aborto, pérdida fetal recurrente, óbito fetal:
► Extensos y contradictorios datos existen en la literatura asociando trombofilia hereditariay aborto.
► Los estudios tienen definiciones diferentes de aborto, limitaciones metodológicas y son en su mayoria de tipo casos control , asi como estudios de cohorte de pequeño tamaño.
► Estos estudios no son suficientes para extraer datos concluyentes.
► No todas las trombofilias hereditarias se asocian a perdida fetal: déficit de antitrombinano parece asociarse. El resto puede tener alguna asociación.
► No existe consenso acerca de la relación entre trombofilia hereditaria y perdida fetal.
Preston FE, Rosendaal FR, Walker ID, et al. Increased fetal loss in women with heritable thrombophilia. Lancet 1996; 348:913.
Sottilotta G, Oriana V, Latella C, et al. Genetic prothrombotic risk factors in women with unexplained pregnancy loss. Thromb Res 2006; 117:681.
Roqué H, Paidas MJ, Funai EF, et al. Maternal thrombophilias are not associated with early pregnancy loss. Thromb Haemost 2004; 91:290.
Rodger MA, Betancourt MT, Clark P, et al. The association of factor V leiden and prothrombin gene mutation and placenta-mediated pregnancy complications: a systematic review and meta-analysis of prospective cohort studies. PLoS Med 2010; 7:e1000292.
Rodesch F, Simon P, Donner C, Jauniaux E. Oxygen measurements in endometrial and trophoblastic tissues during early pregnancy. Obstet Gynecol 1992; 80:283.
Clark P, Walker ID, Govan L, et al. The GOAL study: a prospective examination of the impact of factor V Leiden and ABO(H) blood groupson haemorrhagic and thrombotic pregnancy outcomes. Br J Haematol 2008; 140:236.

Restricción del crecimiento fetal
► No parece existir una relación consistente entre trombofilia y RCF.
► Un solo metaanálisis sugiere una relación entre déficit de proteína S pero no de proteínaC con RCF, sin embargo el número de pacientes es muy pequeño
Alfirevic Z, Roberts D, Martlew V. How strong is the association between maternal thrombophilia and adverse pregnancy outcome? A systematic review. Eur J Obstet Gynecol Reprod Biol 2002; 101:6.
Dudding TE, Attia J. The association between adverse pregnancy outcomes and maternal factor V Leiden genotype: a meta-analysis. Thromb Haemost 2004; 91:700.
Von Kries R, Junker R, Oberle D, et al. Foetal growth restriction in children with prothrombotic risk factors. Thromb Haemost 2001; 86:1012.
Preeclampsia
► La evidencia actual sugiere que la trombofilia hereditaria no esta asociado con un incremento de riesgo de preeclampsia
Dizon-Townson D, Miller C, Sibai B, et al. The relationship of the factor V Leiden mutation and pregnancy outcomes for mother and fetus. Obstet Gynecol 2005; 106:517.
Lin J, August P. Genetic thrombophilias and preeclampsia: a meta-analysis. Obstet Gynecol 2005; 105:182.
Morrison ER, Miedzybrodzka ZH, Campbell DM, et al. Prothrombotic genotypes are not associated with pre-eclampsia and gestational hypertension: results from a large population-based study and systematic review. Thromb Haemost 2002; 87:779.
Kahn SR, Platt R, McNamara H, et al. Inherited thrombophilia and preeclampsia within a multicenter cohort: the Montreal Preeclampsia Study. Am J Obstet Gynecol 2009; 200:151.e1.

Desprendimiento de placenta
► Una consistente asociación entre abruptio y trombofilia hereditaria no ha sido demostrado
Dizon‐Townson DS, Meline L, Nelson LM, et al. Fetal carriers of the factor V Leiden mutation are prone to miscarriage and placental infarction. Am J Obstet Gynecol 1997; 177:402.
Rodger MA, Betancourt MT, Clark P, et al. The association of factor V leiden and prothrombin gene mutation and placenta‐mediated pregnancy complications: a systematic review and meta‐analysis of prospective cohort studies. PLoS Med 2010; 7:e1000292.
Kjellberg U, van Rooijen M, Bremme K, Hellgren M. Factor V Leiden mutation and pregnancy‐related complications. Am J Obstet Gynecol 2010; 203:469.e1.
Robertson L, Wu O, Langhorne P, et al. Thrombophilia in pregnancy: a systematic review. Br J Haematol 2006; 132:171.
Screening de trombofilia hereditaria de mujeres con antecedente de pérdida fetal temprana recurrente o no, RCF, Abruptio o Preeclampsia
no esta recomendado debido a la falta de evidencia entre su asociación causal y la falta de evidencia que la
administración de anticoagulantes puedan mejorar o prevenir un resultado gestacional adverso.

RIESGO DE TROMBOSIS EN TROMBOFILIA HEREDITARIA
RIESGO ALTO RIESGO MEDIO RIESGO BAJO
DEFICIT DE ANTITROMBINADOBLE HETEROCIGOTO PARA
FVL Y PT G20210AFV LEIDEN HOMOCIGOTOPT G20210A HOMOCIGOTO
DEFICIT DE PROTEINA CDEFICIT DE PROTEINA S
FVL HETEROCIGOTOPT G20210A HETEROCIGOTO
Cuando anticoagulamos y por cuanto tiempo???Con que fármacos anticoagulamos???Monitorizamos la anticoagulación???

Numerosos estudios han valorado la relación entre trombofilia hereditaria en lagestación y ETV. Diferencias en los diseños de estudio entre otras limitaciones metodológicas
no permiten la comparación de resultados.
Todas las trombofilias hereditarias han mostrado alguna relación estadísticamente significativa en incremento de riesgo de ETV
Recomendaciones de varios grupos ( ACCP, ACOG, RCOG, SETH, SEC etc) se basanmayoritariamente en estudios casos y controles, pequeños estudios de cohorte
y generalizaciones por extrapolación de estudios en mujeres no gestantes

HNF
HBPMHBPM
AVKAAS
Que fármacos usaremos????

AVK
►Warfarina. No estudios con otros AVK
► Categoria D FDA.
► Puede usarse en la lactancia
► Efectos adversos
▪ Aborto 15‐56%▪ Teratogenicidad, 4‐8/ 6‐9/ 6‐12 ss dosis dependiente. Margen < 5mg
Osteocartilaginosos: Condromalacia, hipoplasia nasalSNC: atrofia cerebral, microcefalia, espasticidad, hipotonia, RM
▪ Hemorragia fetal durante parto parto (3ºTrimestre) Suspender 34‐36 ss
Chong MK, Harvey D, de Swiet M. Follow‐up study of children whose mothers were treated with warfarin during pregnancy. Br J Obstet Gynaecol 1984; 91:1070.
Pauli RM, Lian JB, Mosher DF, Suttie JW. Association of congenital deficiency of multiple vitamin K‐dependent coagulation factors and the phenotype of the warfarin embryopathy: clues to the mechanism of teratogenicity of coumarin derivatives.
Am J Hum Genet 1987; 41:566.
Wesseling J, Van Driel D, Heymans HS, et al. Coumarins during pregnancy: long‐term effects on growth and development of school‐age children. Thromb Haemost 2001; 85:609.
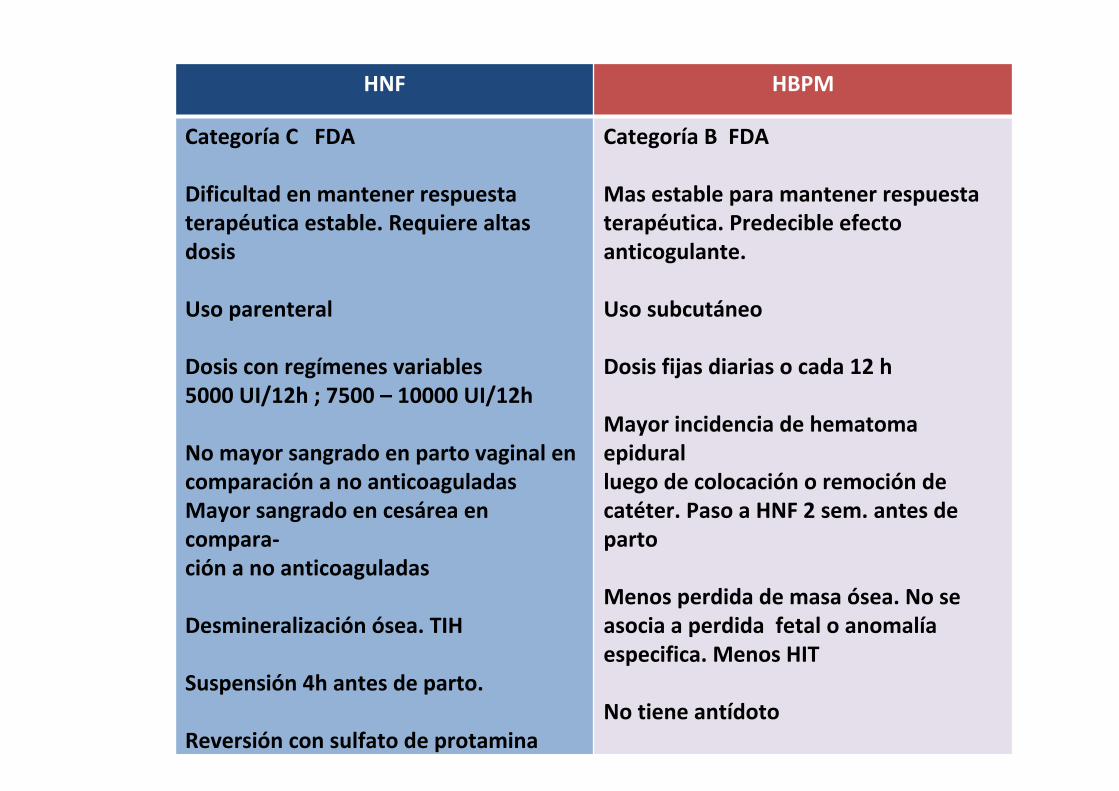
HNF HBPM
Categoría C FDA
Dificultad en mantener respuesta terapéutica estable. Requiere altas dosis
Uso parenteral
Dosis con regímenes variables5000 UI/12h ; 7500 – 10000 UI/12h
No mayor sangrado en parto vaginal encomparación a no anticoaguladasMayor sangrado en cesárea en compara‐ción a no anticoaguladas
Desmineralización ósea. TIH
Suspensión 4h antes de parto.
Reversión con sulfato de protamina
Categoría B FDA
Mas estable para mantener respuestaterapéutica. Predecible efecto anticogulante.
Uso subcutáneo
Dosis fijas diarias o cada 12 h
Mayor incidencia de hematoma epiduralluego de colocación o remoción de catéter. Paso a HNF 2 sem. antes de parto
Menos perdida de masa ósea. No se asocia a perdida fetal o anomalía especifica. Menos HIT
No tiene antídoto

ACOG Practice Bulletin #113. Inherited thrombophilias in pregnancy. Obstet Gynecol 2010; 116:212

A James. Pregnancy‐associated thrombosis Hematology 2009: 277‐285
James A, et Al Thrombosis, thrombophilia, and thromboprophylaxis in pregnancy. Clin Adv Hematol Oncol. 2005;3:187‐197.

‐ Dosis profilácticas: Enoxaparina 40 mg/24hDalteparina 5000 U/24hTinzaparina 4500 U/24h
‐ Dosis Intermedias: Enoxaparina 40 mg/12hDalteparina 5000 U /12h
‐ Dosis Terapeuticas: Enoxaparina 1 mg/kg/12h o 1,5 mg/kg/24ho “ajustadas” Dalteparina 100 U/kg/12h o 200 U/kg/24h
Tinzaparina 175 U/kg/24h
‐ Dosis profilácticas: 5000 – 10000 U/12h o 5000 – 7500 U/12 h en 1ºT7500 – 10000 U/12h en 2ºT 10000 U/12h en 3ºT
‐ Dosis Intermedias: HNF /12h anti‐Xa 0.1‐0.3U/ml 6h post inyección
‐ Dosis Terapéuticas: >10000/12h TTPa 1.5 – 2.5 6h post inyeccióno “ajustadas”
HBPM
HNF
Anticoagulación postparto: Dosis profilácticas HBPM o HNF por 4 – 6 semanaso AVK por 4 ‐ 6 semanas con INR 2‐3 con heparinacomo terapia puente

RECOMENDACIONES ACCP
● En gestantes con trombofilia sin previo ETV recomendamos que no se use de forma rutinaria la profilaxis anteparto en cambio se realice valoración individual del riesgotrombótico (Grado 1C)
● En gestantes sin antecedente previo de ETV pero con déficit de antitrombinarecomendamos profilaxis anteparto y post parto. (Grado 2C)
● Para todas las otras gestantes con trombofilia sin previo ETV recomendamos en elanteparto vigilancia clínica o profilaxis con HBPM o HNF seguido de anticoagulación posparto (Grado 2 C)
Bates S, Greer I, Pabinger I, Sofaer S. Venous thromboembolism, thrombofilia, antithrombotic therapy and pregnancy: American College of Chest Physicians Evidence‐ Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133:844S–886S.
Prevención de ETV en gestantes con trombofilia sin antecedente de ETV

RECOMENDACIONES ACCP
● En gestantes con trombofilia que han tenido único y previo episodio de sinanticoagulación a largo plazo recomendamos: Profilaxis o dosis intermedias de HBPM o HNF en el anteparto o vigilancia durante todo el embarazo, seguido de anticoagulación en el postparto mas que los cuidados rutinarios o la anticoagulación con dosis ajustadas (Grado 1C)
● En gestantes con alto riesgo trombótico (deficit de AT, doble heterozigoto de FVL yPT G20210 u homozigotos de los mismos) que han tenido previo episodio de ETV y sinanticoagulación a largo plazo recomendamos profilaxis o dosis intermedias de HBPMo HNF en el anteparto seguido de profilaxis en el postparto mas que la vigilancia clínica(Grado 2C)
Bates S, Greer I, Pabinger I, Sofaer S. Venous thromboembolism, thrombofilia, antithrombotic therapy and pregnancy: American College of Chest Physicians Evidence‐ Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133:844S–886S.
Prevención de recurrencia de ETV en gestantes con trombofilia

ACOG Practice Bulletin #113. Inherited thrombophilias in pregnancy. Obstet Gynecol 2010; 116:212

TROMBOFILIA
RIESGO ALTORIESGO ALTO RIESGO BAJO
SI ETV NO ETV SI ETV NO ETV
TerapéuticaIntermediaprofiláctica
‐Anticoagulación6 sem‐Intermedia‐Terapéuticas
‐Anticoagulación4‐6 sem
‐ Anticoagulación4‐6 sem‐ Intermedia
‐Vigilancia‐Anticoagulación4‐6 sem simás factores
Profiláctica IntermediaProfilácticaVigilancia
VigilanciaProfiláctica
ANTEPARTO
POSPARTO
Adaptado de ACOG Practice Bulletin #113. Inherited thrombophilias in pregnancy. Obstet Gynecol 2010; 116:212

NO TROMBOFILIASI ETV
IDIOPATICO GESTACIONACO
GESTACIONACO
OTROSFACTORE
S
‐ Profiláctica‐ Intermedia‐ Vigilancia
‐Anticoagulación4‐6sem‐Intermedia
‐Anticoagulación‐4‐6 sem‐ Intermedia
Anticoagulación4‐6 sem
Vigilancia‐ Vigilancia‐ Profiláctica‐ Intermedia
ANTEPARTO
POSPARTO
Adaptado de ACOG Practice Bulletin #113. Inherited thrombophilias in pregnancy. Obstet Gynecol 2010; 116:212

TROMBOFILIA O NO>2 ETV
Anticoagulaciónprevia
Sin anticoagulaciónprevia
Terapéutica
Reiniciar anticoagulación
‐ Profiláctica‐ Intermedia‐ Terapéutica
‐Anticoagulación‐4‐6 sem‐Intermedia‐ Terapeutica 6 sem
ANTEPARTO
POSPARTO
Adaptado de ACOG Practice Bulletin #113. Inherited thrombophilias in pregnancy. Obstet Gynecol 2010; 116:212

Reducing the risk of thrombosis and embolism during pregnancy and the puerperium Royal College of Obstetricians and Gynaecologists. Green‐top guideline Nº 37a. Nov 2009.

Reducing the risk of thrombosis and embolism during pregnancy and the puerperium Royal College of Obstetricians and Gynaecologists. Green‐top guideline Nº 37a. Nov 2009.

MUY ALTO RIESGO
ANT. ETV CON O SIN TROMBOFILIA
+ AVK
ANTENATAL TERAPEUTICA
POSPARTO AVK
ALTO RIESGO ETV SIN AVK‐ETV+TROMBOFILIA‐ETV IDIOPATICA‐ETV GESTACION‐ETV HISTORIA FAMILIAR
TROMBOFILIA ASINTOMATICA DE AR O COMBINADO
ANTENATAL PROFILÁCTICO
POSTPARTO HBPM 6 SEM
RIESGO MODERADO
ETV CON FACTORES DE RIESGO TRANSITORIOSSIN TROMBOFILIA NI HISTORIA FAMILIAR
TROMBOFILIA DE BAJO RIESGO SIN HISTORIA
VIGILANCIA ANTENATAL
POSTPARTO HBPM 6 SEM
La trombosis en el embarazo y parto. SETH SEC 2008

Se debe monitorizar el tratamiento anticoagulante??
● No esta claro que deba monitorizarse anticoagulación con HNF o HBPM en dosis profilácticas, intermedias o ajustadas/terapéuticas.
● No existen protocolos “formales” para distintas dosis de HNF o HBPM incluso en otras poblaciones de pacientes: obesos, nefrópatas.
● No existen ECA que ofrezcan evidencia importante en este aspecto.Recomendaciones actuales se basan en opiniones de expertos.
RECOMENDACIONES ACCP
HNF dosis terapéuticasMantener TTPa 1.5‐2 veces control o anti‐Factor Xa 0.35‐0.70 UI/ml. Control semanalPlaquetas c/2‐3 días en primeras 2 ss.(Prevención HIT)
HBPM dosis ajustadasMantener niveles anti‐FactorXa 0.6 – 1.0 UI/mlControl cada 1‐ 3 meses. Medir 4‐6 h después de administración de HBPMNo esta indicado control plaquetario de forma rutinaria
Bates S, Greer I, Pabinger I, Sofaer S. Venous thromboembolism, thrombofilia, antithrombotic therapy and pregnancy: American College of Chest Physicians Evidence‐ Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133:844S–886S.

TROMBOFILIA
HEREDITARIA
ADQUIRIDA SAF
FVLPT G20210ADEFICIT DE ATDEFICIT DE PCDEFICIT DE PS
COMPLICACIONESTROMBOTICAS
ETV TVP EPTrombosisarterial
COMPLICACIONESVASCULARESOBSTETRICAS
ABORTOSEHEDPPRCF

International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS) Journal of Thrombosis and Haemostasis, 4: 295–306

Sindrome antifosfolipido● Los anticuerpos s (APLAs) han mostrado actividad inhibitoria contra la invasión y proliferación del trofoblasto asi como en la adecuada implantación del embriónpromoviendo la apoptosis trofoblástica.
● El riesgo de abortos recurrentes en gestantes con APLAs pero sin enfermedad autoinmune esta asociado a la presencia o persistencia de estos anticuerpos.
● No hay una asociación clara entre APLAs y otras complicaciones obstétricas: RCFpreeclampsia, abruptio.
Shannon M. Bates Consultative Hematology: The Pregnant Patient Pregnancy Loss. Hematology 2010: 166‐172

Es efectivo el tratamiento anticoagulante o antitrombótico ????
● La combinación de HNF y AAS ha mostrado ser eficaz en la reducción de perdidas recurrentes en gestantes con APLAs. HBPM y AAS no es superior a AAS no utilidad de esteroides.
● Revisión sistemática de 13ECA y 849 gestantes. Esta conclusión se basa en 2 estudios de 148 pacientes
Empson M, Lassere M, Craig J, Scott JR. Prevention of recurrent miscarriage for women with antiphospholipid antibody or lupus anticoagulant. Cochrane Database Syst.
Rev 2005;(2):CD00285.pub2.
● Asociación de AAS y HNF o HBPM podría mejorar resultados gestacionales
Mak A, Cheung MW‐L, Cheak AA, Ho RC. Combination of heparin and aspirin is superior to aspirin alone in enhancing live births in patients with recurrent pregnancy loss and positive anti‐phospholipid antibodies: a meta‐analysis of randomized controlled trials and
metaregression. Rheumatology. 2010;49: 281–288.
● Aunque no hay estudios que comparen HNF y HBPM, podrían ser equivalentes tanto HNF+AAS como HBPM+ AAS.
●Muchos centros utilizan HBPM con AAS debido a la seguridad, comodidad de uso y menos efectos adversos.
Shannon M. Bates Consultative Hematology: The Pregnant Patient Pregnancy Loss. Hematology 2010: 166‐172

Bates, SM, Greer, IA, Pabinger, I, et al. Venous thromboembolism, thrombophilia, antithrombotic therapy, and pregnancy: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133:844S.
*perdida tardía o múltiples perdidas tempranas: P I HNF o P HBPM + AAS (50‐100)Preeclampsia 50 ‐100. no HNF ni HBPM

Anticoagulación en situaciones concretas
ETV
Primeras 24 horas: HNF o HBPM dosis terapéuticas +/‐ Disp. compresión graduadosMonitorizar anti‐FactorXa 0.5 ‐1.1 U/ml (3‐6h post inyección)
Si inestabilidad: Trombolisis TPAr
Subagudo (1d‐1m): HBPM dosis terapéuticasMonitorizar anti‐Factor Xa semanal.
Periodo Medio(>1m): Reducir dosis a ¾ dosis terapéutica. No monitorización.
Periparto: Si Dx a término: FVC, revertir antes de labor. Nunca revertir sin FVC <2 semSi Dx 2‐4 sem antes de parto: Pasar de HBPM a HNF antes de parto
Si Dx 1‐3 m antes de parto: Ultima dosis de ¾ un día antes de labor divididoc/12h. Reiniciar dosis ¾ 6h post parto
Si Dx >3m antes de parto: Ultima dosis de ¾ un día antes de labor divididoc/12h. Reiniciar dosis ¾ 12‐24 h post parto
Post Parto: Continuar HBPM hasta 6 semanas post partoM. Rodger. Evidence Base for the Management of Venous Thromboembolism in Pregnancy. Hematology 2010:173 ‐180

Cesárea
● Un factor de riesgo adicional: Profilaxis con HNF o HBPM o tromboprofilaxis mecánica
●Múltiples factores de riesgo: HBPM dosis profilácticas + tromboprofilaxis mecánica
● Alto riesgo trombótico: Profilaxis 4‐6 sem post parto
Bates S, Greer I, Pabinger I, Sofaer S. Venous thromboembolism, thrombofilia, antithrombotic therapy and pregnancy: American College of Chest Physicians Evidence‐ Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133:844S–886S.
Anestesia neuroaxial
Antes colocación catéter después retirar catéterHNF profiláctico 4 – 6 h 1hHNF terapéutico 4 – 6 h (8 – 12 sc) 1h HBPM profiláctico 12 h 4hHBPM terapéutico 24 h 4h
AVK INR <1.4 inmediatamente
Regional anaesthesia and antithrombotic agents: recommendations of the European Society of Anaesthesiology Eur J Anaesthesiol 2010;27:999–1015

Anticoagulación en portadoras de válvulas cardíacas mecánicas
1. HBPM dosis terapéuticas (c/12h) para alcanzar anti‐FactorXa 4h post inyección(Grado2C) durante todo el embarazo (Grado 1C)
2. HNF a dosis terapéuticas (c/12h) para alcanzar TTPa 2 veces el control o anti‐FactorXa enrango 0.35‐0.70 (Grado 1C)
3. HNF o HBPM hasta la semana 13 y luego cambiar por AVK (warfarina) hasta finales del 3ºtrimestre. Luego pasar a HNF o HBPM hasta el parto (Grado 1C)
4. Muy alto riesgo recomendamos AVK durante todo el embarazo hasta finales del tercertrimestre donde se pasa a HNF o HBPM hasta el parto. Complicaciones maternas son equivalentes a daño fetal. (Grado 2C)
5. Muy alto riesgo puede asociarse dosis bajas de AAS (75 – 100 mg/24h) (Grado 2C)
Bates S, Greer I, Pabinger I, Sofaer S. Venous thromboembolism, thrombofilia, antithrombotic therapy and pregnancy:American College of Chest Physicians Evidence‐ Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133:844S–886S.