avaliaÇÃo tomogrÁfica da morfologia e de …
TRANSCRIPT

PONTIFÍCIA UNIVERSIDADE CATÓLICA DE MINAS GERAIS
Programa de Pós-graduação em Odontologia
Tania Mara de Souza Ianni
AVALIAÇÃO TOMOGRÁFICA DA MORFOLOGIA E DE POSICIONAMENTO DO
PROCESSO CONDILAR EM PACIENTES COM MÁ-OCLUSÃO
Belo Horizonte
2020
Tania Mara de Souza Ianni
AVALIAÇÃO TOMOGRÁFICA DA MORFOLOGIA E DE POSICIONAMENTO DO
PROCESSO CONDILAR EM PACIENTES COM MÁ-OCLUSÃO
Dissertação apresentada ao Programa de Pós-
graduação em Odontologia da Pontifícia
Universidade Católica de Minas Gerais, como
requisito parcial para obtenção do título de
Mestre em Odontologia, Área de Concentração:
Clínicas Odontológicas, Área Temática:
Radiologia Odontológica e Imaginologia.
Linha de pesquisa: Métodos de diagnóstico por
imagem, radiobiologia e radioproteção.
Orientador: Prof. Dr. Amaro Ilídio Vespasiano
Silva
Belo Horizonte
2020

FICHA CATALOGRÁFICA
Elaborada pela Biblioteca da Pontifícia Universidade Católica de Minas Gerais
Ianni, Tania Mara de Souza
I11a Avaliação tomográfica da morfologia e de posicionamento do processo
condilar em pacientes com má-oclusão / Tania Mara de Souza Ianni. Belo
Horizonte, 2020.
63 f. : il.
Orientador: Amaro Ilídio Vespasiano Silva
Dissertação (Mestrado) - Pontifícia Universidade Católica de Minas Gerais.
Programa de Pós-Graduação em Odontologia
1. Articulação temporomandibular - Tomografia. 2. Maloclusão -
Tratamento. 3. Tomografia computadorizada de feixe cônico. 4. Côndilo
mandibular. 5. Diagnóstico por imagem. 6. Mandíbula. I. Silva, Amaro Ilídio
Vespasiano. II. Pontifícia Universidade Católica de Minas Gerais. Programa de
Pós-Graduação em Odontologia. III. Título.
CDU: 616.314-073
Ficha catalográfica elaborada por Fernanda Paim Brito - CRB 6/2999

Tania Mara de Souza Ianni
AVALIAÇÃO TOMOGRÁFICA DA MORFOLOGIA E DE POSICIONAMENTO DO
PROCESSO CONDILAR EM PACIENTES COM MÁ-OCLUSÃO
Dissertação apresentada ao Programa de Pós-
graduação em Odontologia da Pontifícia
Universidade Católica de Minas Gerais, como
requisito parcial para obtenção do título de
Mestre em Odontologia. Área de Concentração:
Clínicas Odontológicas – Área Temática:
Radiologia Odontológica e Imaginologia.
COMPOSIÇÃO DA BANCA EXAMINADORA:
1- Profa. Dra. Cláudia Assunção e Alves Cardoso – Faculdade Promove BH 2- Prof. Dr. Flávio Ricardo Manzi – PUC Minas 3- Prof. Dr. Amaro Ilídio Vespasiano Silva – PUC Minas
DATA DA APRESENTAÇÃO E DEFESA: 21 de fevereiro de 2020
A dissertação, nesta identificada, foi aprovada pela Banca Examinadora
Prof. Dr. Amaro Ilídio Vespasiano Silva Prof. Dr. Rodrigo Villamarim Soares Orientador Coordenador do Programa de Pós-graduação
em Odontologia

AGRADECIMENTOS
À minha querida mãe por ser meu amparo e proteção, meu porto seguro
sempre.
À Beatriz, antes de filha, amiga e confidente.
À Helena, por preencher tudo com sua alegria.
À Márcia, Andrea, Carlinha e Claudinho, obrigada por todo esse amor e
amizade. A confiança de vocês me faz acreditar sempre.
Ao professor, orientador, mas antes de tudo amigo, Amaro Vespasiano.
Obrigada pela paciência nesta jornada e principalmente pela generosidade em
compartilhar seus conhecimentos. Seu apoio tornou tudo mais simples. Sua
simplicidade tornou tudo possível.
Ao professor e amigo Flávio Ricardo Manzi pela confiança e por ser sempre
uma inspiração como profissional e como pessoa.
Aos colegas do mestrado pela amizade, companheirismo.
Aos funcionários da PUC pela ajuda, em especial Silvania e Angélica.
Agradeço de maneira muito especial à Deus por tudo que tem me ajudado e
por todos que coloca em meu caminho.

RESUMO
O objetivo no presente estudo foi analisar a articulação temporomandibular (ATM),
utilizando tomografias computadorizadas de feixe cônico (TCFC), verificando se
alterações de posição e morfologia, estão relacionadas com os tipos de má-oclusão
de classe I, II e III. Os métodos consistem na análise de 329 imagens de TCFC de
pacientes provenientes do banco de imagens da Clínica de Radiologia do
Departamento de Odontologia da Pontifícia Universidade Católica de Minas Gerais.
Esses pacientes foram classificados em más-oclusões classe I, II e III pela
metodologia proposta na análise de Steiner. A posição condilar foi aferida por meio
da medição dos espaços articulares (anterior, superior e posterior), da profundidade
da fossa mandibular, da inclinação dos processos condilares nos planos sagital,
coronal e axial e ainda pelo alinhamento dos processos condilares. A classificação
da morfologia foi realizada no plano coronal, definindo as formas condilares como
arredondadas, planas ou anguladas. Os dados obtidos foram submetidos à análise
estatística pelo teste de ANOVA com um critério com nível de significância de 5%,
além de correlacionados entre si, a fim de se verificar possíveis correlações entre as
variáveis e as más-oclusões de classe I, II e III. Foram obtidos resultados
estatisticamente significantes na inclinação sagital entre os grupos classe I e II, e
classe II e III. Na inclinação coronal entre os grupos classe II e III. No grupo de
classe II o espaço articular posterior mostrou-se significativamente maior, quando
comparados com os espaços anterior e superior. Comparando-se o espaço superior
entre os três grupos vemos uma diferença estatisticamente significante entre os
grupos de classe I e III. O teste estatístico utilizado para análise morfológica foi o
Teste de Kruskall Wallis (p 0,05) e mostrou uma predominância do formato redondo
nos três grupos. Após analisar todas as medições, podemos concluir que há uma
menor inclinação sagital e maior inclinação coronal no grupo de classe II. Este grupo
apresenta ainda a cabeça da mandíbula anteriorizada enquanto nos grupos de
classe I e III o processo condilar apresenta-se centralizado. O espaço articular
superior apresenta-se significativamente maior no grupo de classe III. Houve uma
predominância do formato condilar arredondado em todos os grupos estudados.
Palavras-chave: Má-oclusão. Tomografia computadorizada de feixe cônico. Côndilo
mandibular. Diagnóstico por imagem. Mandíbula.

ABSTRACT
The objective of the present study was to analyze the temporomandibular joint (TMJ),
using cone beam computed tomography (CBCT), verifying changes in position and
morphology, related to the types of class I, II and III malocclusions. The methods
consist of the analysis of 329 images of the TCFC of patients using the image bank
of the Radiology Clinic of the Dentistry Department of the Pontifical Catholic
University of Minas Gerais. These patients were classified into class I, II and III
malocclusions by the methodology proposed in Steiner's analysis. A conditional
position was assessed by using the articular spaces (anterior, superior and
posterior), the depth of the mandibular fossa, the inclination of the conditional
processes in the sagittal, coronal and axial planes and also by the alignment of the
conditional processes. The classification of the morphology was performed in the
coronal plane, defining conditional shapes as rounded, flat or angled. The analyzed
data were analyzed with ANOVA test analysis with a significance level of 5%, in
addition to being correlated with each other, in order to verify possible correlations
between variables and class I, II and III malocclusions. Statistically significant results
were selected in sagittal inclination between the class I and II, class II and III groups.
In coronal inclination between class II and III groups. No class II group or posterior
joint space showed a greater increase, when compared to the anterior and upper
spaces. Comparing the upper space between the three groups, we see a statistically
significant difference between the class I and III groups. The statistical test used for
morphological analysis was the Kruskall Wallis test (page 0.05) and showed a
predominance of the round shape in three groups. After analyzing all the
measurements, we can conclude that there is less sagittal tilt and greater coronal tilt
in the class II group. This group also presents the head of the anterior mandible,
while in the groups of class I and III or conditional process it is centralized. The upper
articular space is larger in the class III group. There was a predominance of the
rounded shape in all groups studied.
Keywords: Malocclusion. Cone-beam computed tomography. Mandibular condyle.
Diagnosis by image. Jaw.
LISTA DE ABREVIATURAS E SIGLAS
ANB Ângulo formado pela diferença entre SNA e SNB
ATM Articulação Temporomandibular
CBCT Cone-beam computed tomography (Tomografia computadorizada de
feixe cônico)
FOV Field of View (campo de visão)
PUC Minas Pontifícia Universidade Católica de Minas Gerais
SNA Ângulo formado entre o plano Sela-Násio e ponto A
SNB Ângulo formado entre o plano Sela-Násio e ponto B
SN-MP Ângulo formado entre plano Sela-Násio e Plano Mandibular
TCFC Tomografia Computadorizada de Feixe Cônico

LISTA DE FIGURAS
Figura 1: Classificação da amostra .......................................................................... 21
Figura 2: Classificação baseada na Análise de Steiner ............................................ 22
Figura 3: Profundidade da fossa mandibular ............................................................ 23
Figura 4: Inclinação do processo condilar/plano sagital ........................................... 24
Figura 5: Inclinação do processo condilar/plano coronal .......................................... 24
Figura 6: Inclinação do processo condilar/plano axial .............................................. 25
Figura 7: Espaços articulares: anterior (A), superior (B) e posterior (C) ................... 26
Figura 8: Alinhamento dos processos condilares ..................................................... 26
Figura 9: Classificação da morfologia do processo condilar ..................................... 27

SUMÁRIO
1 INTRODUÇÃO ...................................................................................................... 17
2 OBJETIVOS ......................................................................................................... 19
2.1 Objetivo geral ................................................................................................... 19
2.2 Objetivos específicos ...................................................................................... 19
3 MATERIAL E MÉTODOS ..................................................................................... 21
3.1 Seleção da amostra ......................................................................................... 21
3.2 Obtenção das imagens .................................................................................... 23
3.3 Análise da posição do processo condilar ...................................................... 23
3.4 Análise da morfologia condilar ....................................................................... 26
3.5 Análise estatística ............................................................................................ 27
4 ARTIGO CIENTÍFICO ........................................................................................... 29
5 CONSIDERAÇÕES FINAIS .................................................................................. 55
REFERÊNCIAS ....................................................................................................... 57
ANEXO A - Parecer Consubstanciado do CEP PUC Minas ................................. 59

17
1 INTRODUÇÃO
A articulação temporomandibular (ATM) é uma articulação bastante
especializada que possui uma série de características próprias e pode apresentar
considerável variação de forma. Articula os arcos dentais: superior e inferior, onde
os dentes exercem uma grande influência nas posições da mandíbula e nos seus
movimentos (TEIXEIRA, REHER, 2012).
O processo condilar, bem como as outras estruturas da ATM, é importante
para sustentar uma boa oclusão e um sistema estomatognático balanceado. Existem
vários fatores que podem afetar a morfologia e a posição desta articulação, como
idade, sexo, padrão de crescimento facial, alterações patológicas e/ou funcionais,
atividade muscular diminuída ou aumentada, força oclusal e alterações da oclusão
dentária (ARIETA-MIRANDA et al., 2013).
Com a introdução da tomografia computadorizada de feixe cônico (TCFC) na
odontologia, exames tomográficos são cada vez mais utilizados, pois oferecem
benefícios para o diagnóstico das estruturas ósseas craniofaciais, especialmente a
posição e a morfologia da ATM (ROQUE-TORRES et al., 2018).
Parece haver uma mudança posicional condilar apenas em pacientes com
tendência de crescimento vertical mostrando que o padrão de crescimento tem
influência na posição condilar (GANUGAPANTA et al., 2017). A morfologia condilar
varia de acordo com morfologia facial vertical e esta variação deve ser considerada
para predição e estabelecimento de plano de tratamento adequado para desordens
temporomandibulares durante tratamento ortodôntico (PARK; KIM; PARK, 2015).
Em pacientes que apresentam desvios de linha média dentária ou esquelética
ou que apresentem ainda má oclusão de classe II subdivisão, ocorre uma assimetria
de posicionamento dos processos condilares (MATTOS et al., 2017; ROQUE-
TORRES et al., 2018).
Deslocamento anterior dos processos condilares independente do tipo de má
oclusão e prevalência de morfologia convexa em grupos de má oclusão de classe I e
II foram achados em pesquisas que buscam avaliar a concentricidade e posição
condilar (MERIGUE et al., 2016).
Articulações com desordens temporomandibulares apresentaram o ângulo
médio do côndilo axial menor, significando que os côndilos das articulações afetadas
podem girar para dentro (AL-RAWI; UTHMAN; SODEIFY, 2017).

18
Algumas medidas lineares, angulares e volumétricas dos processos
condilares diferem significantemente entre os três padrões esqueléticos (I, II, III) e a
posição vertical dos côndilos e altura do ramo mandibular podem contribuir
significativamente para o deslocamento do queixo (ZHANG et al., 2013).
Esforços para relacionar os processos condilares com as más oclusões
mostraram um posicionamento anteriorizado em pacientes com padrão esquelético
classe II (PAKNAHAD; SHAHIDI, 2017).
Podemos observar que a pesquisa da morfologia e do posicionamento
condilar, não obstante a ajuda de uma ferramenta de imagem de grande acurácia,
como a TCFC, ainda não é unânime em sua relação com as más oclusões
ortodônticas.
Correlacionar o formato do processo condilar e sua posição dentro da fossa
mandibular com as más oclusões ortodônticas podem oferecer subsídios para um
plano de tratamento ortodôntico e das disfunções temporomandibulares mais
adequado e abrangente.
19
2 OBJETIVOS
2.1 Objetivo geral
O objetivo neste estudo foi verificar a relação entre posição e morfologia do
processo condilar da mandíbula com as más-oclusões de classe I, classe II e classe
III, por meio de TCFC.
2.2 Objetivos específicos
a) mensurar os espaços intra-articulares superior, anterior e posterior
relacionando com o tipo de má-oclusão;
b) classificar o formato do processo condilar e relacionar com o tipo de má-
oclusão;
c) avaliar e comparar a posição do processo condilar nos planos sagital,
coronal e axial.

21
3 MATERIAL E MÉTODOS
Este trabalho foi aprovado pelo Comitê de Ética em Pesquisa da Pontifícia
Universidade Católica de Minas Gerais, CAEE: 97241718.5.0000.5137 (ANEXO A).
3.1 Seleção da amostra
Figura 1: Classificação da amostra
Fonte: Elaborado pela autora
Este estudo é uma pesquisa do tipo corte transversal retrospectivo onde
foram utilizados 329 exames de TCFC, previamente obtidas de um banco de
imagens, por meio de uma amostra de conveniência, derivada da população de
pacientes que procuraram o Departamento de Odontologia da PUC Minas, Clínica
de Radiologia, para diagnóstico inicial de tratamento ortodôntico.
As imagens selecionadas para este trabalho foram obtidas de pacientes sem
perdas de dentes permanentes (exceto terceiros molares), abrangendo toda a
329 indivíduos
176 mulheres/153 homens
189 classe I
60 classe II
80 classe III

22
estrutura crânio-maxilofacial, sem apresentar grandes assimetrias nas estruturas
faciais, com idade entre 18 e 60 anos (idade média de 39 anos).
Foram usados como critérios de exclusão os pacientes com história de
cirurgia ou trauma na região crânio facial, presença de doenças sistêmicas que
afetem a morfologia articular como doenças inflamatórias ou degenerativas das
articulações. Pacientes com história de desordens temporomandibulares como: dor,
desconforto articular, presença de ruído, crepitação e limitação de abertura também
foram excluídos.
Todas as 329 imagens tomográficas dos pacientes foram classificadas como
má oclusão classe I, II e III baseado na metodologia da análise de Steiner (Fig. 2).
Nesta análise o ângulo ANB é dado pela diferença dos ângulos SNA (formado
pelos pontos Sela, Násio e ponto A) e SNB (formado pelos pontos Sela, Násio e
ponto B). Pacientes com ângulo ANB entre 0 e 4,5 foram classificados como má
oclusão de classe I, maior que 4,5 como má oclusão de classe II e menor que 0,
como má oclusão de classe III (OLIVEIRA JÚNIOR et al., 2007).
Figura 2: Classificação baseada na Análise de Steiner
Fonte: Elaborado pela autora

23
3.2 Obtenção das imagens
As imagens de TCFC foram adquiridas utilizando o tomógrafo i-CAT® (Imaging
Sciences, Hatfield, PA, EUA), com os parâmetros de exposição de 120kV e 7 mA,
tempo de aquisição de 40s e de reconstrução de 62s, com voxel de 0,3 mm e FOV
(Field of View) de 23 x 17 cm. Todas as imagens utilizadas nesse estudo foram
obtidas com os pacientes posicionados sentados, com a posição da cabeça
estabilizada pelos próprios dispositivos do aparelho, de modo que o plano sagital
mediano ficasse perpendicular ao plano horizontal e o Plano de Frankfurt paralelo ao
plano horizontal.
Todas as imagens utilizadas no presente estudo apresentavam-se adequadas
nos aspectos de densidade, contraste e nitidez para avaliação das estruturas
pesquisadas, além de se enquadrarem nos critérios de inclusão da pesquisa.
3.3 Análise da posição do processo condilar
Os dados tomográficos para posição foram reconstruídos pelo software Kodak
Dental Imaging Software® versão 6.11.7.0-B, (Carestream Health, Rochester, Nova
York, EUA).
A profundidade da fossa mandibular (Fig. 3) será a medida de uma reta
perpendicular que passe pelo ponto mais superior da fossa mandibular (C) em
direção ao plano formado pelo ponto mais inferior do tubérculo articular (A) e o ponto
mais inferior do canal auditivo (B) (ROQUE-TORRES et al., 2018).
Figura 3: Profundidade da fossa mandibular
Fonte: Elaborado pela autora
A
C
B

24
A inclinação do processo condilar no plano sagital corresponde ao ângulo
formado entre o longo eixo do processo condilar e o plano oclusal em uma
reconstrução sagital (Fig. 4) (ROQUE-TORRES et al., 2018).
Figura 4: Inclinação do processo condilar/plano sagital
Fonte: Elaborado pela autora
A inclinação do processo condilar no plano coronal corresponde ao ângulo
formado entre o longo eixo do processo condilar e o plano oclusal em uma
reconstrução coronal (Fig. 5) (ROQUE TORRES et al., 2018).
Figura 5: Inclinação do processo condilar/plano coronal
Fonte: Elaborado pela autora
A inclinação do processo condilar no plano axial (Fig. 6) corresponde ao
ângulo formado entre uma linha que passe pelo centro geométrico do processo
condilar da mandíbula até o plano sagital mediano (plano que une a espinha nasal
anterior e espinha nasal posterior), em uma reconstrução axial (ROQUE TORRES et
al., 2018).

25
Figura 6: Inclinação do processo condilar/plano axial
Fonte: Elaborado pela autora
O espaço articular anterior (A) corresponde a distância linear da superfície do
processo condilar e a parede anterior da fossa mandibular sobre a bissetriz anterior
formada entre os planos vertical e horizontal que se tangenciam no centro
geométrico do processo condilar. O espaço articular superior (B) corresponde à
distância linear entre a superfície do processo condilar e a cortical do ponto mais
superior da fossa mandibular seguindo o plano vertical que tangencia o centro do
processo condilar. O espaço articular posterior (C) corresponde à distância linear
entre a superfície do processo condilar e a cortical da parede posterior da fossa
mandibular sobre a bissetriz posterior formada entre os planos vertical e horizontal
que se tangenciam no centro geométrico do processo condilar (Fig. 7) (ROQUE-
TORRES et al. 2018).

26
Figura 7: Espaços articulares: anterior (A), superior (B) e posterior (C)
Fonte: Elaborado pela autora
Para o alinhamento dos processos condilares foi realizado a medida da
distância entre os pontos dos centros geométricos dos processos condilares direito e
esquerdo projetados perpendicularmente sobre plano sagital mediano (ROQUE
TORRES et al., 2018).
O ponto que representa o centro geométrico do processo condilar direito
projetado no plano sagital mediano é considerado o ponto 0 (zero). Os valores
localizados acima do ponto zero serão considerados positivos, e abaixo, negativos
(Fig. 8).
Figura 8: Alinhamento dos processos condilares
Fonte: Elaborado pela autora
3.4 Análise da morfologia condilar
A classificação da morfologia do processo condilar foi realizada em um plano
coronal, baseado no proposto por Kinzinger, Kober e Diedrich (2007) que define as
formas condilares como arredondadas (a), planas (b) e anguladas (c) (Fig. 9).
Ponto zero
Acima valores positivos
Abaixo valores negativos

27
Figura 9: Classificação da morfologia do processo condilar
Fonte: Elaborado pela autora
3.5 Análise estatística
Para avaliação das mensurações da profundidade da fossa mandibular, dos
espaços articulares (anterior, superior e posterior), da inclinação dos processos
condilares nos cortes sagital, coronal e axial e posição geométrica no plano axial, o
teste estatístico executado foi ANOVA um critério e no caso de significância
estatística executou-se o pós-hoc de Tukey. Para avaliação da morfologia dos
processos condilares foi utilizado Teste de Kruskall Wallis (p 0,05). Toda a análise
estatística foi realizada considerando nível de significância de 5% (α =0.05).

29
4 ARTIGO CIENTÍFICO
Tomographic evaluation of the morphology and positioning of the
condillary process in patients with malocclusion
Artigo apresentado de acordo com as normas do periódico
Dentomaxillofacial Radiology (Qualis A2).
Normas para submissão de artigos podem ser encontradas no endereço
eletrônico: http://www.birpublications.org/page/manuscripts/dmfr.

30
Tomographic evaluation of the morphology and positioning of the condillary process in
patients with malocclusion
T M S Ianni¹, P P S Carlos2, M N Azevedo¹, F R Manzi
3, A I V Silva
3
1 Master, Department of Dentistry, Pontifical Catholic University of Minas Gerais, Belo
Horizonte, Brazil.
2Graduation Student, Department of Dentistry, Pontifical Catholic University of Minas
Gerais, Belo Horizonte, Brazil.
3PhD, Department of Dentistry, Pontifical Catholic University of Minas Gerais, Belo
Horizonte, Brazil.
Correspondence to: Amaro Ilídio Vespasiano Silva, Pontifical Catholic University of Minas
Gerais (PUC Minas), Department of Dentistry – Radiology, Av. Dom José Gaspar, 500,
Prédio 46 - Coração Eucarístico, ZIP 30535-901, Belo Horizonte, MG, Brazil, Phone.: +55 31
3319-4414, Fax: +55 31 3319-4410, E-mail: [email protected].
31
Author Contribution Statement
DMFR requires that for all submitted papers:
all the authors have made substantive contributions to the article and assume full
responsibility for its content; and
all those who have made substantive contributions to the article have been named as
authors.
The International Committee of Medical Journal Editors recommends the following definition
for an author of a work, which we ask our authors to adhere to:
Authorship be based on the following 4 criteria [1]:
Substantial contributions to the conception or design of the work; or the acquisition,
analysis, or interpretation of data for the work; AND
Drafting the work or revising it critically for important intellectual content; AND
Final approval of the version to be published; AND
Agreement to be accountable for all aspects of the work in ensuring that questions
related to the accuracy or integrity of any part of the work are appropriately
investigated and resolved.

32
Please list below all authors of this work and a brief description of how they each contributed
towards your submission:
Author name Contribution
Tania Mara de Souza Ianni Acquisition, analysis and interpretation of research data;
Writing the content of the work
Paula Perdigão Starling Carlos Data acquisition for Research
Mariana Neves Azevedo Critical content review
Flávio Ricardo Manzi Interpretation of research data
Amaro Ilídio Vespasiano Silva Conception and design of the research; final approval of the work
Please continue on further pages if needed.
1 The International Committee of Medical Journal Editors, Roles and Responsibilities of
Authors, Contributors, Reviewers, Editors, Publishers, and Owners: Defining the Role of
Authors and Contributors, http://www.icmje.org/roles_a.html

33
Morphological and positioning evaluation of the condylar process in patients with
malocclusion, in CFFC
Morphology / position evaluation of the condylar process in patients with malocclusion
Type of manuscript: Research article
Tania, MS Ianni - MSc - Department of Dentistry-Radiology-Pontifical Catholic University of
Minas Gerais
Paula, PS Carlos - Graduation Student - Department of Dentistry-Radiology-Pontifical
Catholic University of Minas Gerais
Mariana, N Azevedo – MSc - Department of Dentistry Pontifical Radiology Catholic
University of Minas Gerais
Flávio, R Manzi - PhD - Department of Dentistry-Radiology-Pontifical Catholic University of
Minas Gerais
Amaro, IV Silva - PhD - Department of Dentistry-Radiology-Pontifical Catholic University of
Minas Gerais
The present study had no external sources of funding and the authors state that there is no
conflict of interest in this research.
34
Abstract
Objectives: The objective of the present study was to analyze the temporomandibular joint
(TMJ), using cone beam computed tomography (CBCT), checking whether changes in
position and morphology are related to the types of class I, II and III malocclusions.
Methods: The methods consist of analyzing 329 CBCT images of patients from the image
bank of the Radiology Clinic of the Dentistry Department of the Pontifical Catholic
University of Minas Gerais. These patients were classified into class I, II and III
malocclusions based on the methodology of Steiner's analysis. The condylar position was
measured by measuring the joint spaces (anterior, superior and posterior), the depth of the
mandibular fossa, by measuring the inclination of the condylar processes in the sagittal,
coronal and axial planes and also by aligning the condylar processes. The classification of the
morphology was performed in the coronal plane, defining the condylar shapes as rounded, flat
or angled. The data obtained were subjected to statistical analysis by the ANOVA test with
one criterion, significance level of 5%, in addition to correlating each other, in order to verify
possible correlations between the variables and class I, II and malocclusions III.
Results: Significant results were obtained in the sagittal inclination between the class I and II,
and class II and III groups, as well as in the coronal inclination between the class II and III
groups. In the class II group, the posterior articular space was significantly larger when
compared with the anterior and superior spaces. Comparing the upper space between the three
groups, we see a statistically significant difference between the upper spaces between the
class I and III groups. The statistical test used for morphological analysis was the Kruskall
Conclusions: We can conclude that there is less sagittal inclination and greater coronal
inclination in the class II group. This group also presents the anterior mandible head while in
the class I and III groups the condylar process is centralized. The upper articular space is
significantly larger in the class III group. There was a predominance of the rounded condylar
shape in all groups studied.
Key Words: Malocclusion. Cone beam computed tomography. Mandibular condyle.
Diagnosis by image. Jaw.

35
Introduction
The TMJ is a very specialized joint that has a number of its own characteristics and
can vary considerably in shape. It articulates the upper and lower dental arches, where the
teeth exert a great influence on the positions of the jaw and its movements.1
The condylar processes, as well as the other structures of the TMJ, are important to
support a good occlusion and a balanced stomatognathic system. Several factors can affect the
morphology and position of this joint, such as age, sex, facial growth pattern, pathological
and/or functional changes, decreased or increased muscle activity, occlusal strength, and
changes in dental occlusion.2
Cone beam computed tomography (CBCT) in dentistry was an extraordinary advance
in the quality of diagnostic tests, and its superiority in evaluating the morphology and position
of condylar processes is clear among researchers.3-5
Although there has been research relating the characteristics of the TMJ with facial or
dental asymmetries2,6-9
, presenting samples with symptoms or asymptomatic10,11
, or with
normal occlusion12
, the findings are controversial.
For some time, interesting studies have been carried out on this joint using CT scans,
looking for evidence to show the relationship between the type of malocclusion and the shape
or position of the condylar process.2,13-20
Assessing the concentricity of the condylar processes, a prevalence of a more anterior
positioning of them, regardless of the type of malocclusion, was observed.13
Class II growth
pattern patients presented with the condylar processes previously positioned in comparison
with the class I and III groups.15
Al-Rawi NH et al.10
, comparing the condylar position in normal joints and with
temporomandibular disorders, observed that the affected condylar processes may be turned
inward.

36
Park et al.20
found that the morphology of the condylar process varies according to the
vertical facial pattern, and this variation must be considered for the prediction and
establishment of an adequate treatment plan for temporomandibular disorders during
orthodontic treatment.
As we can see, the results of the most current studies have brought important
information about the relationship between condylar position/morphology and growth
patterns or malocclusions. As occlusion is a factor that influences the temporomandibular
joints, the evaluation of the position and morphology of the condylar processes may help in
orthodontic planning. Despite the quality of the CBCT exams and the efforts of researchers,
there are still gaps in the knowledge of this relationship that can be useful in clinical practice
in the diagnosis and prognosis of orthodontic treatments and temporomandibular disorders.
Material and Methods
This work was approved by the Research Ethics Committee of the Pontifical Catholic
University of Minas Gerais, CAEE: 97241718.5.0000.5137.
In a retrospective cross-sectional study CT scans, previously obtained from an image
bank. The sample comprised 329 patients, 176 men and 153 women, and was a convenience
sample derived from the population of patients who sought the PUC Minas Dentistry
Department/Radiology Clinic for initial diagnosis of orthodontic treatment.
The images selected for this study were obtained from patients with no permanent
teeth loss (except third molars), covering the entire craniomaxillofacial structure, without
showing major asymmetries in the facial structures, aged between 18 and 60 years (mean age
39 years).
Exclusion criteria were patients with a history of surgery or trauma in the craniofacial
region, the presence of systemic diseases that affect joint morphology such as inflammatory

37
or degenerative diseases of the joints. Patients with a history of temporomandibular disorders
such as pain, joint discomfort, presence of noise, crackling, and limited opening were also
excluded.
All 329 tomographic images of the patients were classified as class I, II, and III
malocclusions according to the methodology of Steiner's analysis (189 class I patients, 60
class II patients, and 80 class III patients) (Figure 1). In this analysis, the ANB angle is given
by the difference between the angles SNA (formed by points Sela, Násio, and point A) and
SNB (formed by points Sela, Násio, and point B). Patients with an ANB angle between 0 and
4.5 were classified as class I malocclusion, greater than 4.5 as class II malocclusion, and
less than 0 as class III malocclusion.21
TCFC images were acquired using the i-CAT® Tomograph (Imaging Sciences,
Hatfield, PA, USA), with exposure parameters of 120 kV and 7 mA, 40s acquisition time, and
62s reconstruction time, with 0,3 mm, and FOV (Field of View) of 23 x 17 cm. All images
used in this study were obtained with the patients positioned seated, with the head position
stabilized by the device's own devices, so that the median sagittal plane was perpendicular to
the horizontal plane and the Frankfurt plane parallel to the horizontal plane.
All images used in the present study were adequate in terms of density, contrast, and
sharpness for the evaluation of the researched structures, in addition to meeting the inclusion
criteria of the research.
Tomographic data for position were reconstructed using Kodak Dental Imaging
Software® version 6.11.7.0-B (Carestream Health, Rochester, New York, USA).
Depth of the mandibular fossa
The depth of the mandibular fossa (Figure 2) will be the measurement of a
perpendicular straight line that passes through the uppermost point of the mandibular fossa
38
(C) towards the plane formed by the lowest point of the articular tubercle (A) and the lowest
point of the canal auditory (B).3
Inclination of the condylar process in the sagittal plane
The inclination of the condylar process in the sagittal plane corresponds to the angle
formed between the long axis of the condylar process and the occlusal plane in a sagittal
reconstruction (Figure 3).3
Inclination of the condylar process in the coronal plane
The condylar process inclination in the coronal plane corresponds to the angle formed
between the long axis of the condylar process and the occlusal plane in a coronal
reconstruction (Figure 4).3
Inclination of the condylar process in the axial plane
The inclination of the condylar process in the axial plane (Figure 5) corresponds to the
angle formed between a line that passes through the geometric center of the condylar process
of the mandible to the median sagittal plane (plane that joins the anterior nasal spine and
posterior nasal spine), in an axial reconstruction.3
Joint spaces: Anterior (A), Upper (B) and Posterior (C)
The anterior articular space (A) corresponds to the linear distance from the surface of
the condylar process and the anterior wall of the mandibular fossa on the anterior bisector
formed between the vertical and horizontal planes that are tangent in the geometric center of
the condylar process. The upper articular space (B) corresponds to the linear distance between
the surface of the condylar process and the cortical of the most superior point of the

39
mandibular fossa following the vertical plane that touches the center of the condylar process.
The posterior articular space (C) corresponds to the linear distance between the surface of the
condylar process and the cortical of the posterior wall of the mandibular fossa on the posterior
bisector formed between the vertical and horizontal planes that tangent in the geometric center
of the condylar process (Figure 6).3
Alignment of condylar processes
For the alignment of the condylar processes, the distance between the points of the
geometric centers of the right and left condylar processes was projected perpendicularly over
the median sagittal plane.3
The point that represents the geometric center of the right condylar process projected
on the median sagittal plane is considered the point 0 (zero). Values located above the zero
point will be considered positive, and below, negative (Figure 7).
The classification of the condylar process morphology was performed in a coronal
plane, based on the one proposed by Kinzinger et al.22
, which defines condylar shapes as
rounded (a), flat (b) and angled (c) (Figure 8).
To evaluate the measurements of the depth of the mandibular fossa, of the articular
spaces (anterior, superior and posterior), of the inclination of the condylar processes in the
sagittal, coronal, and axial sections, and geometric position in the axial plane, the statistical
test performed was ANOVA a criterion, and in the in case of statistical significance, Tukey's
post-hoc test was performed. To evaluate the morphology of the condylar processes, the
Kruskal-Wallis test was used (p0.05). All statistical analysis was performed considering a
significance level of 5% (α = 0.05).

40
Results
At the end of the analysis of the depth of the mandibular fossa, it was found that there
are no statistically significant differences between the groups of patients with class I, II, and
III malocclusions. However, analyzing the data, a slightly greater depth of the mandibular
fossa is noted in patients with class I malocclusion, although without statistically significant
differences (Table 1).
The analysis of the sagittal inclination of the condylar process showed statistical
significance in the comparison between the class I and II groups, where the class I
malocclusion group shows a greater sagittal inclination in relation to the class II malocclusion
group. There was also statistical significance in the comparison between the class II and class
III malocclusion groups, showing a greater sagittal inclination in the class III malocclusion
group. When comparing groups, I and III, there were no statistically significant differences.
When evaluating the three groups, the highest sagittal inclination of all groups is noted in the
class I group (Table 1).
After analyzing the inclination of the condylar process in the coronal plane, it was
found that there was a statistically significant difference between the groups of patients with
class II and III malocclusion, with patients with class II malocclusion having a greater coronal
inclination when compared to the coronal tilt of class III patients. There was no statistically
significant difference in the class II group when compared with the class I group and when we
also compared the class III group with the class I group (Table 1).
We can also see that the inclination of the condylar processes in the axial plane did not
present statistically significant differences between the groups of patients with class I, II, and
III malocclusions, and the axial inclinations of the three groups had approximate measures
(Table 1).
41
In the evaluation of joint spaces, the results showed statistically significant differences
only when we analyzed the upper joint space. This difference could be observed between
patients with class I and III malocclusion, where we found larger upper joint spaces in
patients with class III malocclusion (3.1 ± 1.3 mm). There were no significant differences in
the upper joint spaces when comparing the patients in the class I and II and class II and III
malocclusion groups, as shown in Table 2.
The tests did not show statistically significant differences for the anterior spaces.
However, in the data analysis, larger anterior articular spaces are observed in the class III
malocclusion group (3.1 ± 1.5), evidencing a more posterior positioning of the condylar
process in class III patients and joint spaces of very close sizes in class I patients, thus
demonstrating a trend towards centralized positioning of the condylar process in class I
patients.
When analyzing the posterior joint spaces, we found no statistically significant
differences between the three groups, but we can see the smallest sizes (2.8 ± 0.8) in the class
I malocclusion group.
The analysis of the alignment of the condylar processes in the axial plane did not show
statistically significant differences between the patients with class I, II, and III malocclusion,
although it can be observed in the patients of the three groups that the geometric centers of the
condylar processes are below the point considered zero point (projection of the geometric
point on the right side perpendicular to the median sagittal plane), as shown in Table 1, where
we only observed negative values.
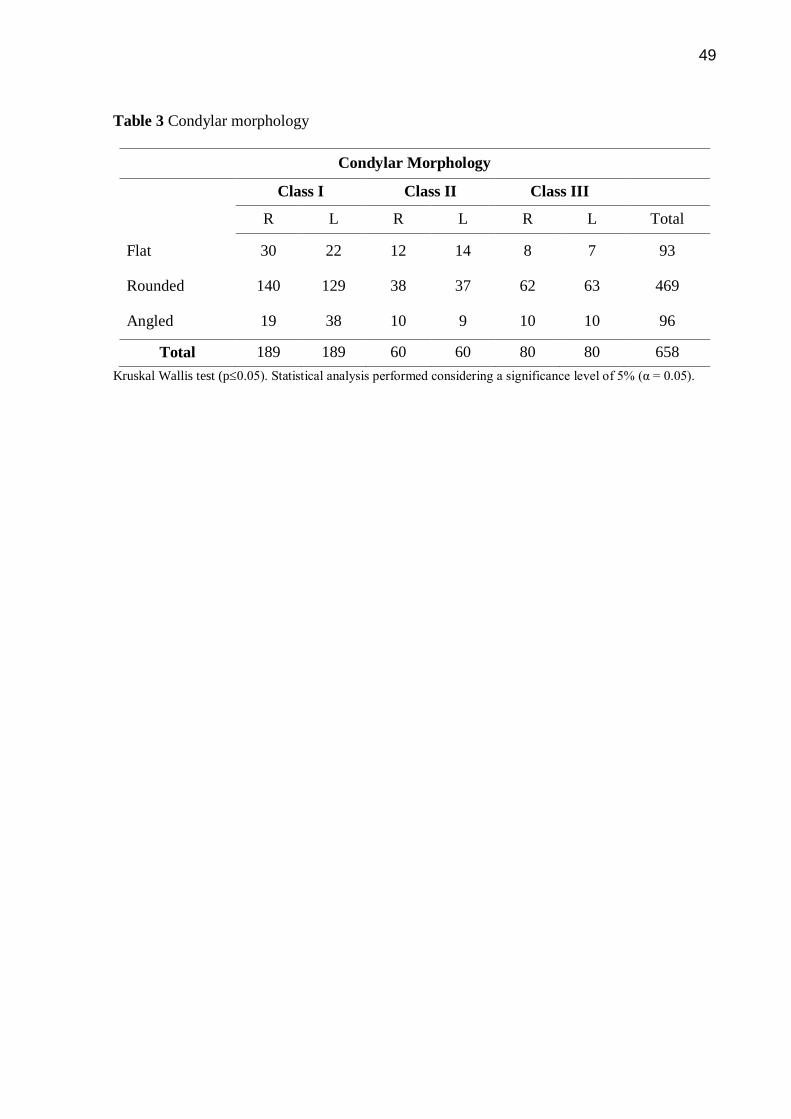
The statistical tests for the morphological analysis showed that there is a
predominance of the rounded shape in the three groups studied, on both sides, left and right,
as shown in Table 3.
42
Discussion
In this research, the tomographic exams of the evaluated patients were previously
divided into class I, II, and III patients using the methodology proposed by Steiner's analysis,
which is based on the size of the ANB angle. Other studies were based on vertical
classifications2,15,18,20
on overbite and growth pattern14
, or even in normal occlusions.12
Different classifications of sample malocclusions can make it difficult to compare the
findings. For future research, standardized classifications of the types of malocclusions can be
useful in comparing the concentricity and morphology of the condylar processes.
Some studies sought to verify whether mandibular asymmetries observed on the face6
or asymmetric malocclusions such as subdivision class II malocclusion8,9
were also found in
condylar positioning. In the study by De Mattos et al.8, patients with class II subdivision
malocclusion presented right and left glenoid fossa asymmetrically, with class II side distally
and laterally, despite the condyles being positioned symmetrically within the glenoid fossa.
This shows that despite the asymmetry of the glenoid fossa, there was concentricity within the
joint. In our study, which did not aim to relate concentricity to midline deviations, a
concentricity of condylar processes was also found in the class I and III malocclusion groups.
Comparing the two studies, we can say that regardless of the type of malocclusion, the
condylar processes tend to be positioned concentrically within the glenoid fossa.
In their 2017 work, Huang et al.9 observed dental characteristics of the class II
subdivision malocclusion: the asymmetry and sagittal position of the upper and lower first
molars between the two sides and significant lingual inclination of the lower first molar on the
class II side. Condylar morphology and asymmetries in the position of the glenoid fossa were
the major components of skeletal asymmetry and were well correlated with the three-
dimensional position of the first molar. The findings of these authors show that the
asymmetries seen in the dental and facial midlines or the mandibular asymmetries are also

43
revealed in asymmetries in the position of the condylar processes. In the present study, the
correlation between midline deviations and malocclusions was not evaluated, but it is
worthwhile to highlight the influence of these asymmetries on condylar positioning.
In the work by Park et al.20
, among the several variables studied, a significant
difference was found in the upper condylar space in the hypodivergent and hyperdivergent
groups. In our study, we can also see that the class III malocclusion group presented the
largest upper joint space in a statistically significant way when we compared the three groups
of malocclusions. Although the samples are numerically different, and the classification of
malocclusions is not the same, there was agreement in the findings.
In their comparative study, Ganugapanta et al.14
evaluated individuals with normal
occlusion and malocclusion and found a significant change in the position of the condylar
process in patients with a vertical growth pattern compared to the average of patients with a
horizontal growth pattern. The left condylar process was more anteriorly located than the right
one in all groups they studied. In our research, we found statistically significant measures for
sagittal inclination in the group with class II malocclusion, showing the smallest measures for
this inclination, revealing the condylar process also more anterior. In Ganugapanta et al.14
paper, no significant change was found in the vertical depth of the mandibular fossa in all
three groups studied, another finding that also coincides with the findings for assessing the
mandibular depth of our research that found no significant differences for the depth of the
mandibular fossa for the three groups of malocclusions studied.
Our results are not in accordance with the study by Arieta-Miranda et al.2 in relation to
joint spaces. Arieta-Miranda et al.2 found a significant difference in the anterior joint space
when comparing class I with class II and class III groups; the superior articular space was
smaller in class II and class III when compared with the class I group and, finally, there was
no statistically significant difference in the posterior condylar space between the groups. Our

44
research found condylar processes with approximate values suggesting concentricity in the
class I and III groups, a statistically significant greater posterior joint space in the class II
group, suggesting an anteriorization of the condylar processes in this group, and even higher
upper joint spaces that are statistically significant in the class III group. Despite the disparity
in results, the two studies used the same methodology for classifying malocclusions, although
there is a considerable difference in the sample size.
In our study, the condylar morphology found, evaluated in a coronal section, was
predominantly rounded for the three groups of malocclusions studied. Merigue et al.13
most
often found convex condyles in their sample, which also used coronal slices in the
assessment. Park et al.20
found that condylar morphology varies according to facial
morphology. In fact, the findings of these authors do not coincide with our study, which
suggests that the sample size may have had an influence on the results, since these studies
have samples of 49 and 60 patients, respectively.
Conclusion
In all evaluations and tests in this sample of 329 patients, we can observe a lower
sagittal inclination and a greater coronal inclination in the class II group, as well as a tendency
towards centralized positioning of the condylar process for patients in the class I and III
groups, and positioning for patients in the class II group, in this population studied. We also
observed a predominance of the rounded shape in the morphology of all studied groups.
45
References
1. Teixeira LMS, Reher P. Anatomia aplicada à odontologia. 2. ed. Rio de Janeiro.
Guanabara Koogan; 2012.
2. Arieta-Miranda JM, Silva-Valencia M, Flores-Mir C, Paredes-Sampen NA, Arriola-
Guillen LE. Spatial analysis of condyle position according to sagittal skeletal
relationship, assessed by cone beam computed tomography. Prog Orthod. 2013; 14:36.
3. Roque-Torres GD, Peyneau PD, Costa ED, Bóscolo FN, Almeida SM, Ribeiro LW.
Correlation between midline deviation and condylar position in patients with Class II
malocclusion: A cone-beam computed tomography evaluation. Am J Orthod Dentofacial
Orthop. 2018; 154:99-107.
4. Ma RG, Yin S, Li G. The detection accuracy of cone beam CT for osseous defects of the
temporomandibular joint: a systematic review and meta-analysis. Sci Rep. 2016;
6:34714.
5. Ladeira DB, Cruz AD, Almeida SM. Digital panoramic radiography for diagnosis of the
temporomandibular joint: CBCT as the gold standard. Braz Oral Res. 2015; 29:1-7.
6. Endo M, Terajima M, Goto TK, Tokumori K, Takahashi I. Three-dimensional analysis of
the temporomandibular joint and fossa-condyle relationship. Orthodontics (Chic.). 2011;
12:210-221.
7. Zhang Y, Che B, Ni Y, Zhang H, Pan Y, Wang L, et al. Three-dimensional condylar
positions and forms associated with different anteroposterior skeletal patterns and facial
asymmetry in Chinese adolescents. Acta Odontol Scand. 2013: 71:1174-80.
8. De Mattos JM, Palomo JM, Ruellas AC, Cheib PL, Eliliwi M, Souki BQ. Three-
dimensional positional assessment of glenoid fossae and mandibular condyles in patients
with Class II subdivision malocclusion. Angle Orthodontist. 2017; 87:847-854.

46
9. Huang M, Hu Y, Yu J, Sun J, Ming Y, Zheng L. Cone-beam computed tomographic
evaluation of the temporomandibular joint and dental characteristics of patients with
Class II subdivision malocclusion and asymmetry. Korean J Orthod. 2017; 47:277-288.
10. Al-Rawi NH, Uthman AT, Sodeify SM. Spatial analysis of mandibular condyles in
patients with temporomandibular disorders and normal controls using cone beam
computed tomography. Eur J Dent. 2017; 11:99-105.
11. Dalili Z, Khaki N, Kia SJ, Salamat F. Assessing joint space and condylar position in the
people with normal function of temporomandibular joint with cone-beam computed
tomography. Dental Res J. 2012; 5:607-612.
12. Vitral RW, da Silva Campos MJ, Rodrigues AF, Fraga MR. Temporomandibular joint
and normal occlusion: Is there anything singular about it? A computed tomographic
evaluation. Am J Orthod Dentofacial Orthop. 2011; 140:18-24.
13. Merigue LF, Conti AC, Oltramari-Navarro PV, Navarro RL, Almeida MR. Tomographic
evaluation of the temporomandibular joint in malocclusion subjects: condylar
morphology and position. Braz Oral Res. 2016; 30:1-7.
14. Ganugapanta VR, Ponnada SR, Gadam KP, Perumalla K, Khan I, Mohammed NA.
Computed tomographic evaluation of condylar symmetry and condyle-fossa relationship
of the temporomandibular joint in subjects with normal occlusion and malocclusion: a
comparative study. J Clin Diagn Res. 2017; 11:29-33.
15. Paknahad M, Shahidi S. Association between condylar position and vertical skeletal
craniofacial morphology: A cone beam computed tomography study. Int Orthod. 2017;
15:740-751.
16. Lingchem D, Qiang Z, Meiy T, Chao H, Xuetao C, Qing L. Comparative study of the
condylar positions in different sagittal skeletal facial types with cone-beam computed
tomography. West China J Stomatol. 2014; 32:383-386.

47
17. Fraga MR, Rodrigues AF, Ribeiro LC, Campos MJ, Vitral RW. Anteroposterior condylar
position: A comparative study between subjects with normal occlusion and patients with
Class I, Class II Division 1, and Class III malocclusions. Med Sci Monit. 2013; 19:903-
907.
18. Paknahad M, Shahidi S, Abbaszde H. Correlation between condylar position and
different sagittal skeletal facial types. J Orofac Orthop. 2016; 77:350-356.
19. Kaur A, Natt AS, Mehra SH, Maheshwari K, Sing G, Kaur A. Improved visualization and
assessment of condylar position in the glenoid fossa for different occlusions: A CBCT
Study. J Contemp Dent Pract. 2016; 17:679-686.
20. Park IY, Kim JH, Park YH. Three-dimensional cone-beam computed tomography-based
comparison of condylar position and morphology according to the vertical skeletal
pattern. Korean J Orthod. 2015; 45:66-73.
21. Oliveira WM Jr, Vigorito JW, Tuma CESN, Cabral LS, Maia AS, Maia DSP.
Determinação dos valores cefalométricos de wits em jovens amazonenses, com oclusão
normal. Rev Dent Press Ortodon Ortop Facial. 2007; 12:118-124.
22. Kinzinger G, Kober C, Diedrich P. Topography and morphology of the mandibular
condyle during fixed functional orthopedic treatment - a magnetic resonance imaging
study. J Orofac Orthop. 2007; 68:124-47.

48
Tables
Table 1 Condylar positioning
Class I Class II Class III
Depth of the mandibular fossa (mm) 8,4 ± 1,3 A 8,2 ± 1,2 A 8,2 ± 0,9 A
Inclination of the condylar process in
the sagittal plane (°) 123,3 ± 8,5 A 111,8 ± 13,5 B 121,4 ± 7,9 A
Inclination of the condylar process in
the coronal plane (°) 98,1 ± 6,4 AB 99,9 ± 7,2 A 97,3 ± 6,8 B
Inclination of the condylar process in
the axial plane (°) 70,3 ± 7,6 A 69,7 ± 9,5 A 71,5 ± 7,5 A
Alignment of condylar processes (mm) -0,4 ± 1,9 A -0,5 ± 0,9 A -0,3 ± 1,6 A
Means and standard deviation followed by distinct letters, uppercase vertically and lowercase letters horizontally
differ statistically from each other, by the ANOVA test with a criterion
Table 2 Condylar positioning/articular spaces
Articular spaces
Class I Class II Class III
Anterior 2,6 ± 0,7 Aa 2,6 ± 0,9 Ba 3,1 ± 1,5Aa
Upper 2,8 ± 0,7 Ab 2,8 ± 1,6 Bab 3,1 ± 1,3 Aa
Posterior 2,8 ± 0,8 Aa 3,8 ± 1,9 Aa 3,0 ± 0,9 Aa
Means and standard deviation followed by distinct letters, uppercase vertically and lowercase letters horizontally
differ statistically from each other, by the ANOVA test with a criterion
49
Table 3 Condylar morphology
Condylar Morphology
Class I Class II Class III
R L R L R L Total
Flat 30 22 12 14 8 7 93
Rounded 140 129 38 37 62 63 469
Angled 19 38 10 9 10 10 96
Total 189 189 60 60 80 80 658
Kruskal Wallis test (p0.05). Statistical analysis performed considering a significance level of 5% (α = 0.05).

50
Figure Legends
Figure 1 Classification based on Steiner's Analysis
Figure 2 Depth of the mandibular fossa
Figure 3 Inclination of the condylar process / sagittal plane
Figure 4 Inclination of the condylar process/coronal plane
Figure 5 Inclination of the Condylar process/ axial plane
Figure 6 Articular spaces: anterior (A), upper (B) and posterior (C)
Figure 7 Alignment of condylar processes
Figure 8 Classification of the condylar process morphology

51
Figure 1
Figure 2
Figure 3
A
C
B

52
Figure 4
Figure 5
Figure 6

53
Figure 7
Figure 8
Ponto zero
Acima valores positivos
Abaixo valores negativos

55
5 CONSIDERAÇÕES FINAIS
Nesta população estudada não ocorreu a associação de um posicionamento
do processo condilar à uma má oclusão, embora o exame de tomografia
computadorizada de feixe cônico ofereça uma imagem precisa. Mas podemos
observar uma clara predominância do formato arredondado nos processos
condilares avaliados.

57
REFERÊNCIAS
ARIETA-MIRANDA, J.M. et al. Spatial analysis of condyle position according to sagittal skeletal relationship, assessed by cone beam computed tomography. Progress in Orthodontics, v.14, p. 1-9, Oct. 2013. AL-RAWI, N.H.; UTHMAN, A.T.; SODEIFY, S.M. Spatial analysis of mandibular condyles in patients with temporomandibular disorders and normal controls using cone beam computed tomography. European Journal of Dentistry, v.11, n.1, p. 99-105, Jan./Mar. 2017. GANUGAPANTA, V.R. et al. Computed tomographic evaluation of condylar symmetry and condyle-fossa relationship of the temporomandibular joint in subjects with normal occlusion and malocclusion: a comparative study. Journal of Clinical & Diagnostic Research, v.11, n.2, p. ZC29-ZC33, Feb. 2017. KINZINGER, G.; KOBER, C.; DIEDRICH, P. Topography and morphology of the mandibular condyle during fixed functional orthopedic treatment - a magnetic resonance imaging study. Journal of Orofacial Orthopedics, v.68, n.2, p. 124-147, Mar. 2007. MATTOS, J.M. et al. Three-dimensional positional assessment of glenoid fossae and mandibular condyles in patients with Class II subdivision malocclusion. The Angle Orthodontist, v.87, n.6, p. 847-854, Nov. 2017. MERIGUE, L.F. et al. Tomographic evaluation of the temporomandibular joint in malocclusion subjects: condylar morphology and position. Brazilian Oral Research, v.30, n.1, p. 1-7, 2016.
OLIVEIRA JÚNIOR, W.M. et al. Determinação dos valores cefalométricos de Wits em jovens amazonenses, com oclusão normal. Revista Dental Press de Ortodontia e Ortopedia Facial, v.12, n.1, p. 118-124, jan./fev. 2007.
PAKNAHAD, M.; SHAHIDI, S. Association between condylar position and vertical skeletal craniofacial morphology: a cone beam computed tomography study. International Orthodontics, v.15, n.4, p. 740-751, Dec. 2017
PARK, I.Y.; KIM, J.H.; PARK, Y.H. Three-dimensional cone-beam computed tomography-based comparison of condylar position and morphology according to the vertical skeletal pattern. The Korean Journal of Orthodontics, v.45, n.2, p. 66-73, Mar. 2015. ROQUE-TORRES, G.D. et al. Correlation between midline deviation and condylar position in patients with Class II malocclusion: A cone-beam computed tomography evaluation. American Journal of Orthodontic and Dentofacial Orthopedics, v.154, n.1, p. 99-107, July 2018.
TEIXEIRA, L.M.S.; REHER, P. Anatomia aplicada à odontologia. 2. ed. Rio de Janeiro. Guanabara Koogan, 2012.

58
ZHANG, Y. et al. Three-dimensional condylar positions and forms associated with different anteroposterior skeletal patterns and facial asymmetry in Chinese adolescents. Acta Odontologica Scandinavica, v.71, n.5, p. 1174-1180, Sept. 2013.

59
ANEXO A - Parecer Consubstanciado do CEP PUC Minas

60

61

62

63