2009-ar-76 artigo de revisÃo miocardiopatia não...
TRANSCRIPT

Recebido para publicação: Julho de 2009 • Aceite para publicação: Setembro de 2010Received for publication: July 2009 • Accepted for publication: September 2010
1847
ARTIGO DE REVISÃO
Miocardiopatia não compactada - revisão a propósito de oito casos [133]
ALEXANDRA TOSTE, LUÍSA MOURA BRANCO, ANA GALRINHO, ANA LOUSINHA, ANTÓNIO FIARRESGA, MÁRIO M. OLIVEIRA, JOÃO
ABREU, JOÃO JOÃO MENDES, LURDES FERREIRA, ANA LEAL, RUI CRUZ FERREIRA
Serviço de Cardiologia, Hospital de Santa Marta, Lisboa, Portugal
Rev Port Cardiol 2010; 29 (11): 1847-1864
RESUMO
A miocardiopatia não compactada isolada éuma doença geneticamente determinada
cuja patogénese parece envolver umaparagem no desenvolvimento do
endomiocárdio. Morfologicamentecaracteriza-se pela presença de
trabeculações proeminentes separadas porprofundos recessos preenchidos por fluxo e
como tal por Doppler a cor no estudoecocardiográfico. No sentido de melhor
caracterizar esta entidade recentementedescrita, de prognóstico pouco esclarecido,
fazemos uma revisão dos casosdiagnosticados no nosso hospital,
descrevendo as características clínicas,electrocardiográficas e ecocardiográficas,
bem como a terapêutica instituída eseguimento clínico. A propósito da revisão
dos casos, é feita uma exposição e discussãoda literatura mais relevante relativamente a
etiopatogenia, clínica, critérios dediagnóstico, terapêutica e prognóstico.
Palavras chave: Miocardiopatia não compactada isolada;
Cardiomiopatia; Ecocardiografia Doppler;Insuficiência cardíaca; Diagnóstico;
Terapêutica; Prognóstico
Noncompaction cardiomyopathy– A review of eight cases
ABSTRACT
Left ventricular noncompaction is a geneticdisorder that is thought to be related to anarrest in endomyocardial development. It ischaracterized by the presence of a promi-nent trabecular meshwork and deep recess-es. In order to better characterize thisrecently described disorder, whose progno-sis remains unclear, we review eight casesdiagnosed at our hospital, describing theirclinical, electrocardiographic and echocar-diographic features as well as therapy andfollow-up. We also discuss the most relevantdata from the literature concerning patho-genesis, clinical presentation, diagnosticcriteria, therapy and prognosis.
Key wordsLeft ventricular noncompaction; Cardiomyopathy;Doppler echocardiography; Heart failure; Diagnosis;Therapy; Prognosis.
2009-AR-76 Dezembro

INTRODUÇÃO
Amiocardiopatia não compactada isolada(MNC) é uma miocardiopatia primária de
origem genética(1), em que a morfogénese doendomiocárdio é comprometida, pensa-se quepela interrupção do desenvolvimento normaldo ventrículo esquerdo (VE) entre as cinco e asoito semanas de gestação(2). Caracteriza-se poruma trabeculação excessiva das paredes doVE associada a recessos profundos que comu-nicam com a cavidade ventricular, mas nãocom a circulação coronária(3). Era consideradauma doença rara, com mau prognóstico, asso-ciando-se frequentemente a insuficiênciacardíaca crónica, eventos tromboembólicos,disritmias ventriculares graves e morte súbitacardíaca(4). No entanto, o recurso generalizadoà ecocardiografia e a realização cada vez maisfrequente de ressonância magnética nuclearcardíaca (RMN), bem como a evolução destastécnicas imagiológicas, levaram à identifi-cação de um número cada vez maior de indiví-duos que preenchem os critérios diagnósticosde MNC, muitos dos quais assintomáticos ecom um prognóstico pouco claro. Esta pato-logia parece abranger um largo espectro clíni-co e a sua história natural pode ser bem melhorque aquela assumida inicialmente.
Neste trabalho pretendemos apresentar ascaracterísticas clínicas, electrocardiográficas,ecocardiográficas e a evolução de casos de mio-cardiopatia não compactada seguidos no nossoserviço.
MÉTODOS
Estudámos retrospectivamente os doentesque realizaram ecocardiograma transtorácicono laboratório de ecocardiografia do Hospitalde Santa Marta (ecocardiógrafos Vivid 7, Vi-vid 3 e System 5 da General Electric) e quepreenchiam os seguintes critérios ecocardio-gráficos de MNC:
- presença de múltiplas trabeculaçõesproeminentes;
- presença de recessos intertrabecularespreenchidos com sangue a partir da cavidadeventricular demonstrados por Doppler a cor;
INTRODUCTION
Isolated left ventricular noncompaction(LVNC) is a primary cardiomyopathy of
genetic origin (1) in which there is incompletemorphogenesis of the endomyocardium,thought to be due to an arrest in the normaldevelopment of the left ventricle (LV) betweenthe fifth and eighth week of gestation(2). It ischaracterized by excessive trabeculation ofthe LV walls with deep recesses that commu-nicate with the ventricular cavity but not withthe coronary circulation(3). It was formerly con-sidered a rare disease with poor prognosis,frequently associated with chronic heart fail-ure, thromboembolic events, severe ventricu-lar arrhythmias and sudden cardiac death(4).However, widespread use of echocardiographyand increasingly frequent use of cardiac mag-netic resonance imaging (MRI), together withtechnical advances in these imaging methods,mean that an increasing number of individualsare identified as meeting the diagnostic crite-ria for LVNC, many of whom are asympto-matic, and prognosis is far from clear. Thepathology appears to cover a broad clinicalspectrum, and its natural history may be con-siderably less bleak than initially thought.
This study aims to present the clinical,electrocardiographic (ECG) and echocardio-graphic features and clinical course of casesof left ventricular noncompaction followed inour department.
METHODS
We retrospectively studied patients whounderwent transthoracic echocardiography inthe echocardiographic laboratory of Hospitalde Santa Marta (using General Electric Vivid7, Vivid 3 and System 5 scanners) and whomet the following echocardiographic criteriafor isolated LVNC:
- multiple prominent trabeculations;- intertrabecular recesses filled with blood
from the ventricular cavity, documented bycolor Doppler;
- ratio of >2 between thicknesses of non-1848
Rev Port Cardiol Vol. 29 Dezembro 10 / December 10
2009-AR-76 Dezembro
- relação entre a espessura da camada nãocompactada e a espessura da camada com-pactada do miocárdio > 2 (telessístole);
- ausência de anomalias cardíacas signi-ficativas coexistentes.
Foram confirmados por RMN os casos emque subsistiam dúvidas após estudo ecocar-diográfico, quer por uma inadequada visua-lização do ápex ventricular esquerdo, quer poruma relação entre as duas camadas (compac-tada e não compactada) limítrofe. Os critériosde diagnóstico de Petersen e colaboradores(5) –relação entre espessura da camada não com-pactada e espessura da camada compactada >2,3 em telediástole - foram empregues nosdoentes submetidos a RMN. O equipamentode RMN utilizado foi General Electric Signa eas medições foram obtidas na sequênciadinâmica b-Steady State Free Precession (b-SSFP) - FIESTA Gated, 1,5 Tesla. A monito-rização com electrocardiografia-Holter de 24horas foi realizada em todos os doentesexcepto num, que faleceu antes do exame.
RESULTADOS
Analisámos oito doentes com uma médiade idades de 56,6 + 17,3 anos (28 - 80 anos),dos quais quatro eram do sexo masculino. Ascaracterísticas clínicas estão resumidas noQuadro I.
À data do diagnóstico apenas dois doentesestavam completamente assintomáticos; doisdoentes encontravam-se em classe II da NewYork Heart Association (NYHA); três doentesestavam em classe III e outro em classe IV daNYHA (Tabela 1). Em nenhum dos casos se do-cumentaram patologias coexistentes nomeada-mente dismorfias faciais ou doenças neuro-musculares.
Alterações electrocardiográficas no ECGbasal estavam presentes em 88% dos doentes.Episódios de taquicardia ventricular não man-tida (TVNM) foram documentados em electro-cardiografia-Holter em 50% dos casos (Qua-dro I).
As características ecocardiográficas estãoresumidas no Quadro II.
compacted and compacted layers of myocardi-um in end-systole;
- no other significant cardiac abnormalities.MRI was performed to confirm cases in
which doubts remained after echocardio-graphic study, either because of inadequatevisualization of the LV apex or because theratio between the two layers was borderline.The diagnostic criterion of Petersen et al(5).(ratio between noncompacted and compactedlayers of >2.3 in end-diastole) was used inthese exams. The MRI scanner used was aGeneral Electric Signa and measurementswere made using balanced steady-state freeprecession (b-SSFP) (gated FIESTA) at 1.5Tesla. Holter 24-hour ECG monitoring wascarried out in all patients except one, whodied before the exam.
RESULTS
Eight patients, mean age 56.6±17.3 years(28-80), four male, were studied. Their clini-cal characteristics are summarized in Table I.
At the time of diagnosis only two patientswere completely asymptomatic; two were inNew York Heart Association (NYHA) class II,three in class III and one in class IV (Table I).No other pathologies were recorded in anypatient, including facial dysmorphisms orneuromuscular disease.
Alterations on baseline ECG were presentin 88% of the sample. Episodes of nonsus-tained ventricular tachycardia (NSVT) wererecorded on Holter monitoring in 50% ofcases (Table I).
The patients’ echocardiographic character-istics are summarized in Table II.
On echocardiography, four patients hadbaseline LV wall thickness at the upper nor-mal limit, and LV dilatation was found in 75%of cases. Mean ejection fraction at diagnosiswas 29.9±17.8% (12%-64%). Care was takento exclude trabeculations when determiningventricular volumes. Although ejection frac-tion was generally low (normal in only onepatient), only four patients were in NYHAclass ≥III (Tables I and II). 1849
Alexandra Toste, et al.Rev Port Cardiol 2010; 29: 1847-1864
2009-AR-76 Dezembro

A ecocardiografia revelou paredes do VEde espessura no limite superior da normalida-de a nível basal em quatro doentes e dilataçãoventricular esquerda em 75% dos casos. Afracção de ejecção média à data do dia-gnóstico foi de 29,9 + 17,8% (12%-64%). Nadeterminação dos volumes ventriculares foramexcluídas sistematicamente as trabeculações.De salientar que, apesar de terem fracções deejecção baixas (apenas um doente tinhafracção de ejecção normal), só quatro doentesse encontravam em classe NYHA ≥III (Qua-dros I e II).
Apenas um doente apresentava alteraçõessegmentares, tendo-se neste caso excluído apresença de doença coronária através da rea-lização de angiografia coronária. Todos os ou-tros doentes com compromisso da função sis-tólica apresentavam hipocinésia global, ou se-ja, mesmo os segmentos que se apresentavammorfologicamente normalmente compactadosestavam hipocinéticos.
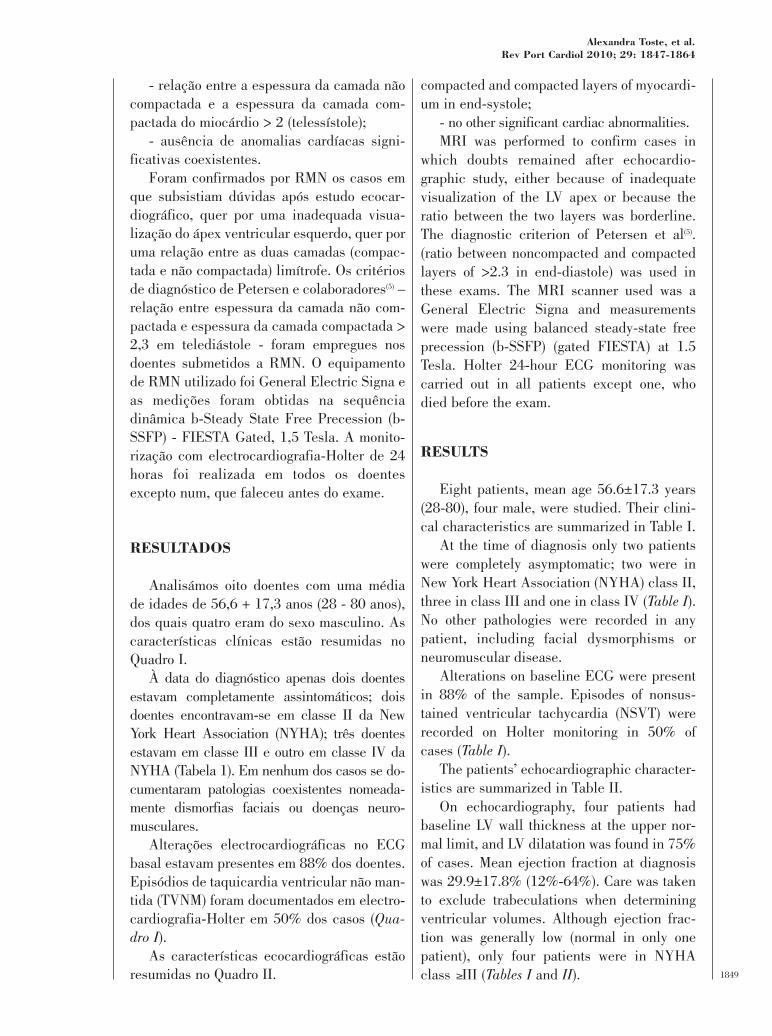
O Quadro II revela-nos quais os segmentosque cumpriam critérios de não compactação.A zona de não compactação mais frequente foia parede lateral, seguida da parede posterior,com um predomínio de atingimento mediano e
Wall motion abnormalities were seen inonly one patient, in whom coronary artery dis-ease was excluded by coronary angiography.All individuals with impaired systolic func-tion presented global hypokinesia, meaningthat even morphologically normal segmentswere hypokinetic.
Table II shows the segments that met crite-ria for noncompaction. The most frequentlocation was the lateral wall, followed by theposterior wall, mainly the mid and apical seg-ments (Figure 1). In the case with the mostsevere initial clinical presentation (NYHAclass IV), the noncompaction also involvedthe right ventricle (Figure 2A and Table II).
Mural thrombi were documented in twopatients (Figure 2), one of whom suffered anembolic stroke, although without sequelae.
Five patients were prescribed singleantiplatelet therapy, and one (with a mechani-cal mitral valve prosthesis) was prescribedanticoagulant therapy. The two patients withmural thrombi were prescribed anticoagulantand antiplatelet agents. All patients receivedstate-of-the-art treatment for heart failure. Acombined cardiac resynchronization therapydefibrillator was implanted in one patient with1850
Rev Port Cardiol Vol. 29 Dezembro 10 / December 10
2009-AR-76 Dezembro
D Idade Sexo NYHA TE ECG Holter1 72 F II - FA TVNM2 61 M II - FA EV frequentes3 69 M III - RS; BCRE TVNM4 28 F IV Trombo IV RS; HVE, HEA TVNM5 44 F I - RS Sem alterações6 80 F III - Pacemaker Não disponível7 55 M I - RS; BCRE Sem alterações8 44 M III Trombo IV SR; LVH NSVT
stroke
Quadro I. Características clínicas dos doentes com MNC
Patient Age Gender NYHA TE ECG Holter1 72 F II - AF NSVT2 61 M II - AF Frequent VES3 69 M III - SR; LBBB NSVT4 28 F IV IV thrombus SR; LVH, LAH NSVT5 44 F I - SR No alterations6 80 F III - Pacemaker ND7 55 M I - SR; LBBB No alterations8 44 M III IV thrombus SR; LVH NSVT
Stroke
Table I. Clinical characteristics of patients with LVNC
FA: fibrilhação auricular; TVNM: taquicardia ventricular não mantida; RS: ritmo sinusal; BCRE: bloqueio completo de ramo esquerdo; HVE: hipertrofiaventricular esquerda; HEA: hemibloqueio esquerdo anterior; EV: extrassistolia ventricular; IV: intraventricular; AVC: acidente vascular cerebral.NYHA: New york Heart Association; TE - eventos trombo embólicos
AF: atrial fibrillation; IV: intraventricular; LAH: left anterior hemiblock; LBBB: left bundle branch block; LVH: left ventricular hyper-trophy; ND: no data; NSVT: nonsustained ventricular tachycardia; NYHA: New York Heart Association functional class; SR: sinusrhythm; TE: thromboembolism; VES: ventricular extrasystoles

apical (Figura 1). No caso com a apresentaçãoclínica inicial mais grave (classe IV NYHA),a área de não compactação abrangia também oventrículo direito (Figura 2-A, Quadro II).
O desenvolvimento de trombos murais foidocumentado em dois doentes (Figura 2), umdos quais com acidente vascular cerebral em-bólico do qual não resultaram quaisquer se-quelas.
Cinco dos doentes foram submetidos a an-tiagregação simples e um doente a anticoagu-lação (por apresentar concomitantemente umaprótese mecânica mitral). Os dois doentes queapresentavam trombos murais foram subme-tidos a terapêutica com anticoagulação e an-tiagregação plaquetária. Todos os doentes fo-ram submetidos a terapêutica para insufi-ciência cardíaca de acordo com o estado daarte. Num dos doentes, com bloqueio com-pleto de ramo esquerdo (BCRE) e dessincro-mia mecânica detectada através de estudo eco-cardiográfico, foi colocado um ressincroniza-dor / desfibrilhador implantável.
Até à data, nesta pequena série com umseguimento mediano de 14 meses (1 - 53
complete left bundle branch block andmechanical dyssynchrony detected onechocardiography.
In this small series with a median follow-up of 14 months (1-53 months) there havebeen two deaths. One was the patient with theimplantable cardiac resynchronization defib-rillator, who after eight months of slight clini-cal and echocardiographic improvement, wasadmitted several times for respiratory andheart failure and died of pneumonia in a set-ting of decompensated heart failure. The otherdeath was an 80-year-old woman who initiallypresented in NYHA class III and died of stroketwo months after echocardiographic diagnosisof LVNC.
DISCUSSION AND THEORETICALREVIEW
Left ventricular noncompaction was onlyrecognized relatively recently as a distinctcardiomyopathy with a specific cause andprognosis (1, 4, 6). It is being reported with 1851
Alexandra Toste, et al.Rev Port Cardiol 2010; 29: 1847-1864
2009-AR-76 Dezembro
Figura 1. Distribuição das áreas de não compactação do VE.
Figure 1. Distribution of areas of LV noncompaction.
Septo anterior basalBasal anteroseptal
Septo inferior basalBasal inferoseptal
Inferior basalBasal inferior
Posterior basalBasal posterior
Lateral basalLateral basal
Anterior basalBasal anterior
Septo anterior medianoMid anteroseptal
Septo inferior medianoMid inferoseptalInferior mediano
Mid inferiorPosterior mediano
Mid posteriorLateral mediano
Mid lateralAnterior mediano
Mid anteriorApical anterior
Apical lateralApical inferiorApical septal
Distribuição das áreas de não compatação do VEDistribuition of areas of LV noncompaction
0 2 4 6 8Nº de doentesNo. of patients

1852
Rev Port Cardiol Vol. 29 Dezembro 10 / December 10
2009-AR-76 Dezembro
Figure 2. Apical 4 câmaras (A e B), Apical e longitudinal paraesternol longo eixo (C) de um doente com MNC revelando envolvimento do VD e trombo no VE
Figure 2. Apical (A and B) and parasternal short-axis (C) views of a patient with LVNC, with right ventricular involvement and LV thrombus
Figura 2-A
Figura 2-B
Figura 2-C
meses) verificaram-se dois óbitos. Um delescorresponde ao doente que colocou o ressincro-nizador; após oito meses de melhoria clínica eecocardiográfica ligeiras, seguiu-se um perío-do de vários internamentos por insuficiênciascardíaca e respiratória, tendo acabado porfalecer no contexto de intercorrência infec-ciosa – pneumonia - com descompensação da
increasing frequency, due to improvements inimaging techniques and to heightened aware-ness on the part of cardiologists. Its preva-lence in the literature ranges from 0.014% to0.3% in adults (3, 4, 7) and is 0.14% in children(8).However, its real prevalence is believed to beconsiderably higher, since most series onlyinclude index cases and not relatives with a 1853
Alexandra Toste, et al.Rev Port Cardiol 2010; 29: 1847-1864
2009-AR-76 Dezembro
D SC VE td VE td VE ts SIV PPVE Fr.ej. Alterações Área de Outra(m2) (mm) (mm/m2) (mm) (mm) (mm) (%) segmentares trabeculação
1 1,7 60 35 45 12 13 25 Hipocinésia global Mediano e apical
2 1,8 60 33 52 12 6 20 Hipocinésia global Parede lateral Prótese mecânicae posterior mitral
3 1,5 77 51 73 12 10 12 Acinésia da Parede inferiorparede inferior e septal posteriore septal anterior
4 1,7 74 43 64 11 10 14 Hipocinésia Parede lateralglobal e posterior
5 1,6 50 31 30 9 11 64 - Parede antero-lateral e ápex
6 1,7 70 41 42 13 15 40 Hipocinésia Todas as paredes Pacemakerglobal
7 1,8 59 33 48 10 10 43 - Segemento aplicaldas paredes laterale anterior
8 1,8 55 31 52 9 10 22 Hipocinésia Segemento medianoglobal e aplical das paredes
e anterior
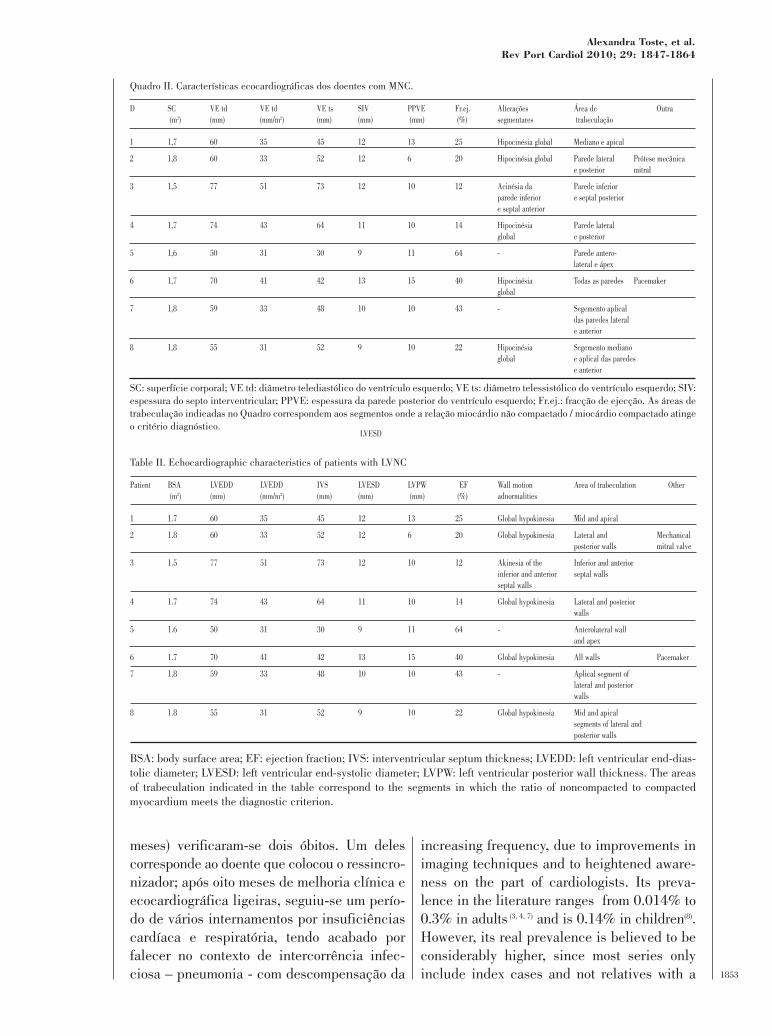
Quadro II. Características ecocardiográficas dos doentes com MNC.
Patient BSA LVEDD LVEDD IVS LVESD LVPW EF Wall motion Area of trabeculation Other(m2) (mm) (mm/m2) (mm) (mm) (mm) (%) adnormalities
1 1.7 60 35 45 12 13 25 Global hypokinesia Mid and apical
2 1.8 60 33 52 12 6 20 Global hypokinesia Lateral and Mechanicalposterior walls mitral valve
3 1.5 77 51 73 12 10 12 Akinesia of the Inferior and anteriorinferior and anterior septal wallsseptal walls
4 1.7 74 43 64 11 10 14 Global hypokinesia Lateral and posteriorwalls
5 1.6 50 31 30 9 11 64 - Anterolateral wall and apex
6 1.7 70 41 42 13 15 40 Global hypokinesia All walls Pacemaker
7 1,8 59 33 48 10 10 43 - Aplical segment oflateral and posteriorwalls
8 1.8 55 31 52 9 10 22 Global hypokinesia Mid and apicalsegments of lateral andposterior walls
Table II. Echocardiographic characteristics of patients with LVNC
SC: superfície corporal; VE td: diâmetro telediastólico do ventrículo esquerdo; VE ts: diâmetro telessistólico do ventrículo esquerdo; SIV:espessura do septo interventricular; PPVE: espessura da parede posterior do ventrículo esquerdo; Fr.ej.: fracção de ejecção. As áreas detrabeculação indicadas no Quadro correspondem aos segmentos onde a relação miocárdio não compactado / miocárdio compactado atingeo critério diagnóstico.
BSA: body surface area; EF: ejection fraction; IVS: interventricular septum thickness; LVEDD: left ventricular end-dias-tolic diameter; LVESD: left ventricular end-systolic diameter; LVPW: left ventricular posterior wall thickness. The areasof trabeculation indicated in the table correspond to the segments in which the ratio of noncompacted to compactedmyocardium meets the diagnostic criterion.
LVESD

insuficiência cardíaca. O outro caso de óbitoverificou-se na doente de 80 anos, comapresentação inicial em classe III da NYHA,que faleceu no contexto de acidente vascularcerebral dois meses após estabelecimento dodiagnóstico ecocardiográfico de MNC.
DISCUSSÃO / REVISÃO TEÓRICA:
A MNC foi reconhecida como uma miocar-diopatia distinta, com causa e prognóstico es-pecíficos há relativamente pouco tempo(1,4,6).Tem sido descrita com uma frequência cres-cente, devido não só à evolução das técnicasimagiológicas como também ao maior estadode alerta por parte da comunidade cardioló-gica. A prevalência reportada nas publicaçõesvaria dos 0,014% aos 0,3%(3, 4, 7) na populaçãoadulta e é de 0,14% na população pediátri-ca(8). No entanto, pensa-se que a verdadeiraprevalência desta patologia seja bem superior,uma vez que grande parte destas sériesincluem apenas os casos índex e não os fami-liares com uma forma mais benigna, até mes-mo assintomática de MNC(9). Em Portugal oprimeiro caso foi descrito por Coelho L. ecolaboradores(10) em 2000. Desde então foramdescritos mais sete casos(11-16). Recentemente,Sá M.I. et al(17) estudaram o envolvimento car-díaco num grupo de doentes com Distrofia mio-tónica tipo I, tendo detectado a presença decritérios de não compactação do VE em 8 dos46 doentes estudados.
Apesar do número de doentes não ser ele-vado, decidimos publicar este artigo por setratar da primeira série portuguesa publicadade doentes com o diagnóstico de miocardio-patia não compactada. Esta série de oito doen-tes teve início em 2005; desde então, o nossolaboratório de ecocardiografia realizou umtotal de 25 082 ecocardiogramas transto-rácicos, 17 dos quais correspondem a estesoito doentes.
Esta patologia afecta predominantemente osexo masculino numa percentagem que rondaos 70%. Na nossa série verificou-se uma dis-tribuição equitativa entre os dois sexos, o quenão pode ser sujeito a extrapolações face ao
more benign, even asymptomatic, form ofLVNC(9). The first case in Portugal was des-cribed by Coelho et al. (10) in 2000, and sincethen seven more have been reported (11-16). Sá etal.(17) studied cardiac involvement in a group ofpatients with type 1 myotonic dystrophy anddetected criteria of LV noncompaction in eightof the 46 patients studied.
Although the number of patients is small(eight), we decided to publish this article onthe grounds that it is the first Portugueseseries of patients with a diagnosis of noncom-paction cardiomyopathy. Since the seriesbegan in 2005, our echocardiographic labora-tory has performed 25,082 transthoracicechocardiograms, of which 17 were in theseeight patients.
LVNC mainly affects males (around 70%);in our series there was an equal distributionbetween the sexes, but this cannot be extrap-olated to other populations given the smallsample size. According to some authors, thelocation and extent of noncompaction differsby gender: in a recently published series,Stöllberger et al. reported that the anterior,lateral and posterior walls were more ofteninvolved in women, while in men noncom-paction mainly affected the apex, and that thearea of noncompaction was larger in women,although with no repercussions on symptomsor mortality(18). There are various possibleexplanations for the difference in prevalencebetween the sexes. Some forms of LVNC areX-linked, which increases the prevalence inmales, while women may be affected by moresevere forms, leading to higher early mortali-ty, which is supported by some pediatric seriesin which females predominate.
Another possibility is that the diagnosticcriteria are inadequate and need to be adjust-ed for gender. Most criteria are based on theratio between the thicknesses of the noncom-pacted and compacted layers. The greater theabsolute value for each layer, the more appar-ent the trabeculation and the more likely thediagnosis; there is known to be a direct rela-tionship between body surface area and wallthickness, which is usually greater in men(23).
Current diagnostic criteria are based main-1854
Rev Port Cardiol Vol. 29 Dezembro 10 / December 10
2009-AR-76 Dezembro

1855
Alexandra Toste, et al.Rev Port Cardiol 2010; 29: 1847-1864
2009-AR-76 Dezembro
Figura 3. Apical; 4 câmaras (A e B e parestendal curto eixo (c) de um doente com MNC, relevando trabeculação proeminente do VE
Figure 3. Apical 4-chamber (A and B) and parasternal short-axis (C) views of a patient with LVNC, shoung prominent LV trabeculation.
Figura 3-A
Figura 3-B
Figura 3-C

ly on echocardiography, although MRI isincreasingly used in this context. However,there are as yet no universally accepted crite-ria. Jenni et al.(24) proposed the following: 1)the existence of two layers, one thin and com-pact (C) and the other noncompacted (NC),and a ratio of NC/C >2 when measured in end-systole in short parasternal axis view; 2)absence of other structural cardiac anomalies;3) numerous, excessively prominent trabecu-lations and deep intertrabecular recesses; 4)intertrabecular spaces perfused by blood flowdemonstrated by color Doppler.
The need to exclude other heart defects isrelated to the pathogenesis of LVNC. In nor-mal development the myocardium condensesand the intertrabecular recesses are reducedto capillaries, but if there is an arrest in thecompaction process, deep intertrabecularrecesses covered with endocardium mayevolve that communicate with the ventricularcavity. A similar morphology may be seen inother congenital cardiac anomalies includingleft or right ventricular outflow tract obstruc-tion, bicuspid aortic valve and other forms ofsemilunar valve obstruction, all of whichexpose the ventricle to excessively high pres-sures during intrauterine development, lead-ing to the formation of persisting sinusoidscomparable with hemangiomas in communi-cation with the coronary arteries. By contrast,in isolated LVNC there appears to be a genet-ically determined arrest in the normal com-paction of the endomyocardium and theresulting intertrabecular recesses do not com-municate with the coronaries but with the ven-tricular cavity (24). This explains the need toexclude pathologies that could mimic LVNC.
It is worth noting that one of the patients inour series had concomitant heart disease, hav-ing had a mechanical mitral valve implantedfor rheumatic valve disease characterized byregurgitation. This patient was includedbecause he presented two clearly distinguish-able myocardial layers, one noncompactedand the other compacted, with a mean ratio of2.5, which would not normally be expected ina case of simple mitral regurgitation, as point-ed out by Jenni et al. (24). The fact that the seg-1856
Rev Port Cardiol Vol. 29 Dezembro 10 / December 10
2009-AR-76 Dezembro
pequeno número de doentes incluídos. A pró-pria localização e extensão da não compac-tação difere consoante o sexo segundo algunsautores(18). Numa série recentemente publica-da, Stöllberger et al descrevem que as mu-lheres apresentavam mais frequentemente asparedes anterior, lateral e postero inferior atin-gidas, ao passo que nos homens a zona de nãocompactação predominante era o ápex. Por ou-tro lado, as mulheres apresentavam uma áreade não compactação mais extensa, sem que issose repercutisse sobre a sintomatologia ou sobrea mortalidade(18). Existem várias hipóteses parajustificar esta diferença de prevalência entre osdois sexos; por um lado, existem formas comhereditariedade ligada ao cromossoma X, o queaumenta a prevalência da doença nos homens;por outro, é possível que as mulheres sejamafectadas por formas mais graves, pelo que amortalidade precoce seria mais elevada, hi-pótese que é apoiada por algumas séries pediá-tricas, em que o sexo feminino predomina.
Uma outra hipótese a considerar é a uti-lização de critérios diagnóstico inadequados,surgindo portanto a necessidade de es-tabelecer critérios de diagnóstico ajustadospara o sexo. A maior parte dos critérios de dia-gnóstico baseiam-se na relação entre a espes-sura da camada não compactada e a da cama-da compactada. Ora, quanto maior for o valorabsoluto de cada uma das camadas, mais apa-rente é a hipertrabeculação e como tal o dia-gnóstico, e é sabido que existe uma relação di-recta entre a superfície corporal e a espessurada parede do VE, que geralmente é superiornos homens(23).
Os critérios de diagnóstico actuais ba-seiam-se sobretudo na ecocardiografia, aindaque a RMN esteja a ganhar cada vez maisespaço neste contexto. No entanto, ainda nãoexistem critérios de diagnóstico universal-mente aceites. Jenni et al(24) propôs como cri-térios: 1) existência de duas camadas, uma dasquais fina e compacta (C) e a outra não com-pactada (NC), que, quando medidas em teles-sístole no paraesternal curto eixo, apresentamuma razão NC/C > 2; 2) ausência de anomaliasestruturais cardíacas coexistentes; 3) nume-rosas trabeculações excessivamente proemi-

nentes e recessos intertrabeculares profundos;4) recessos perfundidos por sangue, com fluxodemonstrável no Doppler cor. A necessidadede exclusão de outra cardiopatia relaciona-secom a própria patogénese da MNC. No desen-volvimento embrionário normal, o miocárdiocondensa-se e os recessos intertrabecularessão reduzidos a capilares. No entanto, se hou-ver uma paragem nesse processo de compac-tação, desenvolvem-se recessos profundosdelimitados por endocárdio, que se encontramem comunicação com a cavidade ventricular.Uma morfologia semelhante pode acompanharoutros defeitos cardíacos congénitos, taiscomo obstrução à câmara de saída do ven-trículo direito ou do ventrículo esquerdo,bicuspidia da válvula aórtica e outras formasde obstrução das válvulas semilunares,condições estas que expõem os ventrículos apressões excessivamente elevadas durante odesenvolvimento intrauterino, levando à for-mação de sinusóides persistentes comparáveisa hemangiomas, em comunicação com ascoronárias. Pelo contrário, na MNC isoladaparece existir uma interrupção, geneticamentedeterminada, da compactação normal doendomiocárdio; os recessos intertrabecularesdaí resultantes não comunicam com as co-ronárias, mas sim com a cavidade ventricu-lar(24). Daí a necessidade de excluir patologiascuja patogénese possa levar a uma morfologiaque mimetiza a MNC. De notar que um dosdoentes incluídos no nosso estudo apresen-tava patologia cardíaca concomitante: tinha jásido submetido a implantação de prótese me-cânica mitral por valvulopatia reumática compredomínio de regurgitação. A inclusão destedoente deve-se ao facto de o doente apresentarclaramente duas camadas, uma NC e a outraC, cuja razão era em média 2,5, o que não é detodo espectável numa regurgitação mitralpura, como sugerido por Jenni e colabora-dores(24). A presença de segmentos afectadosapenas nas paredes lateral e posterior é igual-mente sugestiva de se tratar de MNC, quegeralmente poupa a parede septal (sobretudoos segmentos basais), ao passo que oremodelling ventricular induzido por valvulo-patias se caracteriza pela dilatação ventricular
ments affected were in the lateral and posteri-or walls only is also suggestive of LVNC,which usually spares the septal wall, particu-larly the basal segments, while ventricularremodeling induced by valve disease is char-acterized by LV dilatation and wall involve-ment that does not spare the septum.
Chin et al. (25) suggest as a diagnostic crite-rion an X-to-Y ratio ≤0.5, where X is the dis-tance between the epicardial surface andtrough of a trabecular recess and Y is the dis-tance from the epicardial surface to the peakof the trabeculation, as measured in images ofthe LV apex and free wall in end-diastole.
Stöllberger et al. (26) propose as criteria theexistence of more than three trabeculationsprotruding from the LV wall, apical to the pap-illary muscles, visible in a single image plane,and intertrabecular spaces perfused from theventricular cavity, visualized by color Doppler.
Kohli et al.(3) report that of 199 patientswith LV systolic dysfunction, 23.6% met atleast one of three echocardiographic defini-tions of LVNC, and suggest that the currentcriteria are insufficiently specific. At the sametime, only 29.8% of patients with a an estab-lished diagnosis of LVNC conformed to allthree definitions.
Echocardiography has well-known limita-tions in assessing the LV apex, which is thearea most often affected by noncompaction.Hence the advantages of MRI, with its excel-lent spatial resolution and good visualization ofthe LV apex. Petersen et al.(5) suggest as a crite-rion an NC/C ratio of >2.3 in diastole, since thiscutoff is highly accurate in distinguishingLVNC from the hypertrabeculation observed inhealthy, dilated or hypertrophied hearts.
In our small series, the diagnosis wasestablished in most cases by echocardiogra-phy using Jenni’s criteria. MRI was used dueto uncertainty in echocardiographic diagnosisin only four patients, the diagnosis of LVNCbeing confirmed in all cases (Figure 4).
Despite the objectivity of the proposed cri-teria, diagnosis of this entity is not alwayseasy. Degrees of hypertrabeculation consid-ered pathological in white patients are rela-tively common in blacks (3), while marked 1857
Alexandra Toste, et al.Rev Port Cardiol 2010; 29: 1847-1864
2009-AR-76 Dezembro

esquerda e envolvimento da parede que nãopoupa o septo.
Chin et al(25) sugerem como critérios dia-gnósticos a presença de uma razão X/Y ≤0,5,onde X representa a distância desde a su-perfície epicárdica até ao fundo de um recessoe Y é a distância desde a superfície epicárdicaaté ao pico de uma trabeculação. Estasmedidas baseiam-se nas imagens do ápex e daparede livre do VE em telediástole.
Já Stollberger et al(26) propõem como cri-térios a existência de mais de três trabecu-lações com origem na parede do VE, mais api-cais em relação aos músculos papilares, visí-veis num único plano de imagem, e espaçosintertrabeculares perfundidos a partir da ca-vidade ventricular, visualizados no Doppler cor.
Kohli e colaboradores(4) descrevem que em199 doentes com disfunção sistólica do VE,23,6% preenchiam pelo menos uma das defi-nições ecocardiográficas de MNC, sugerindoque os critérios actuais seriam pouco especí-ficos. Por outro lado, apenas 29,8% dos doen-tes com diagnóstico estabelecido de MNCobedeciam às três definições de MNC.
Como é sabido, a ecocardiografia apresentalimitações importantes na avaliação do ápexdo VE, reconhecido como a área mais fre-quente de não compactação. Neste contexto,surge a RMN, com uma excelente resoluçãoespacial e com uma boa avaliação do ápex doVE. Petersen et al(5) sugerem como critério apresença de uma razão NC/C >2,3 em diás-tole, uma vez que este valor separa com umaelevada acuidade diagnóstica a MNC da hi-pertrabeculação observada em corações sau-dáveis, dilatados ou hipertrofiados.
Na nossa pequena série, o diagnóstico foiestabelecido na maior parte dos casos por eco-cardiografia recorrendo aos critérios de Jenni.Apenas quatro doentes realizaram RMN por in-certeza no diagnóstico ecocardiográfico, e emtodos os casos o diagnóstico de MNC foi con-firmado (Figura 4).
Apesar da objectividade dos critérios pro-postos, o diagnóstico desta entidade nem sem-pre é fácil. Na verdade, a hipertrabeculação émais frequente nos indivíduos de raça negra eníveis de hipertrabeculação considerados pa-
hypertrabeculation has been observed in eliteathletes (23). In other cases, hypertrabeculationis associated with LV hypertrophy whether ornot valve disease or hypertension are present,meeting criteria for hypertrophic cardiomy-opathy, particularly apical (27-29). Differentialdiagnosis is also with endomyocardial fibrosis,which frequently involves the LV apex. Theimportance of rigorous application of the diag-nostic criteria adopted, in order to avoid over-diagnosis, cannot be overstated.
A genetic criterion would considerablyincrease diagnostic accuracy in this patholo-gy. A familial origin is identified in over 50%of cases, and most authors accordingly recom-mend echocardiographic screening of rela-tives. However, as in other primary cardiomy-opathies, it is genetically heterogeneous, withmultiple mutations and forms of transmissionhaving been described, which partiallyexplains its phenotypic variability. The mostcommon form of inheritance is autosomaldominant, but cases of X-linked recessive andmitochondrial inheritance have also beenreported. Various mutations in different geneshave been identified, including those for G4.5,α-dystrobrevin, dystrophin, LIM domain pro-tein 3, lamin A/C (30) and β-myosin heavy chain(31). Mutations in the G4.5 gene on the X chro-mosome are responsible for a form of isolateddilated cardiomyopathy (DCM), but also causeBarth syndrome, characterized by heart dis-ease in the form of DCM or LVNC, recurringneutropenia and growth retardation. Mutationsin the dystrophin gene cause predominantlyneurological conditions such as Duchenne orBecker muscular dystrophy, with varyingdegrees of cardiac involvement, or primarilycardiac pathologies (DCM or LVNC) with sub-clinical myopathy. Mutations in the lamin A/Cgene (autosomal dominant inheritance) areassociated with familial DCM or LVNC, con-duction disturbances and myopathies. Thefrequent association between LVNC and neu-romuscular disease is the reason thatStöllberger et al. recommend routine neuro-logical assessment in patients with LVNC (26).Mutations in the β-myosin heavy chain gene,which are known to be linked to hypertrophic,1858
Rev Port Cardiol Vol. 29 Dezembro 10 / December 10
2009-AR-76 Dezembro

tológicos na raça caucasiana são relativa-mente frequentes na raça negra(3). Por outrolado, têm surgido casos de hipertrabeculaçãomarcada em desportistas de alta compe-tição(23). Noutros casos, a hipertrabeculaçãoassocia-se a hipertrofia ventricular esquerda,quer na presença de patologia valvular ou hi-pertensiva(24), quer na sua ausência, preen-chendo critérios para miocardiopatia hiper-trófica nomeadamente apical(27-29). O diagnós-tico diferencial deve ser feito também com afibrose endomiocárdica, que frequentementeenvolve o ápex ventricular esquerdo. Efectiva-mente, nunca é demais enfatizar a necessi-dade de uma aplicação rigorosa dos critériosde diagnóstico adoptados de modo a evitar aomáximo o sobrediagnóstico desta entidade.
Na verdade, um critério genético aumenta-ria em muito a acuidade diagnóstica nesta pa-tologia. Em mais de 50% dos casos é possíveldetectar uma origem familiar, razão pela quala maioria dos autores preconiza um rastreioecocardiográfico dos familiares. No entanto, eà semelhança de outras miocardiopatias pri-márias, é uma entidade geneticamente hete-rogénea; estão descritas múltiplas mutações eformas de transmissão, o que explica em partea variabilidade fenotípica. A hereditariedademais frequente é autossómica dominante(AD), sendo que também foram descritoscasos de hereditariedade recessiva ligada ao
restrictive and dilated cardiomyopathy, havealso been reported in families with LVNC (31).The range of mutations linked to LVNC goessome way towards explaining the variations inthe disease’s phenotype and the existence offamilies with morphologically different car-diomyopathies. The frequency of each of thesemutations is low and the genetic basis of thedisease is unclear in a large proportion ofpatients with LVNC, which means that inclu-sion of a genetic component in the diagnosticcriteria will require considerable furtherresearch. Genetic study of our small series ofpatients is in progress.
The most common clinical manifestations,as also seen in our series, are heart failurewith systolic and diastolic dysfunction, throm-boembolic phenomena, ventricular arrhyth-mias and sudden cardiac death. However, thepathophysiological mechanisms are poorlyunderstood. There appears to be microvascu-lar dysfunction causing a chronic subendocar-dial and transmural perfusion deficit anddiminished coronary reserve (32), which in turncontributes to systolic and diastolic dysfunc-tion and arrhythmogenesis. Precordial pain isin fact observed in 26% of patients (4) despiteabsence of angiographically significant coro-nary lesions, as in one case in our series.
Half of our patients were in NYHA class Ior II, which is in agreement with published 1859
Alexandra Toste, et al.Rev Port Cardiol 2010; 29: 1847-1864
2009-AR-76 Dezembro
Figura 4. RMN cardíaca de um dos doentes com miocardiopatia não compactada. Eixo curto, sequência dinâmica b-SSFP (FIESTA Gated).
Figure 4. Cardiac MRI of a patient with LVNC. Short axis view, dynamic b-SSFP sequence (gated FIESTA).

cromossoma X e hereditariedade mitocon-drial. Foram identificadas múltiplas mutaçõesem vários genes envolvidos, nomeadamente o(4.5,) a a distrobrevina, a distrofina, a proteínade ligação ao domínio LIM 3, laminina A/C30e o gene da cadeia pesada ß miosina(31).Mutações no gene G4.5, localizado no cromos-soma X, são responsáveis por uma forma demiocardiopatia dilatada isolada, mas tambémoriginam o Síndrome de Barth, caracterizadopela presença de cardiopatia (sob a forma demiocardiopatia dilatada ou de MNC), neutro-pénia recorrente e atraso no crescimento. Mu-tações na distrofina podem originar quadrospredominantemente neurológicos como a dis-trofia muscular de Duchenne ou de Beckercom atingimento cardíaco mais ou menos pro-nunciado, ou quadros predominantemente car-diológicos (miocardiopatia dilatada ou MNC)com atingimento miopático subclínico. Muta-ções da laminina A/C, de transmissão AD, as-sociam-se a miocardiopatia dilatada familiarou a MNC, perturbações da condução e mio-patias. De facto, a associação frequente deMNC a doenças neuromusculares está na baseda recomendação, por Stollberger et al, daavaliação neurológica por rotina dos doentescom MNC(26). Mutações no gene da cadeiapesada ß miosina, que se sabe estarem asso-ciadas a miocardiopatia hipertrófica, mio-cardiopatia restritiva e miocardiopatia dila-tada, foram também descritas em famílias comMNC(31). É portanto compreensível a variedadefenotípica daqui resultante, bem como o apa-recimento de famílias com miocardiopatiasmorfologicamente diferentes. A incidência decada uma destas mutações é baixa e a basegenética da doença está por esclarecer numagrande proporção de doentes com MNC, peloque a inclusão de um critério de diagnósticogenético requer ainda um longo trabalho deinvestigação. O estudo genético da nossa pe-quena série de doentes encontra-se em curso.
As manifestações clínicas mais frequentes,também documentadas na nossa série, sãoinsuficiência cardíaca com disfunção sistólicae diastólica, fenómenos tromboembólicos,arritmias ventriculares e morte súbita cardía-ca. No entanto, os mecanismos patofisiológi-
series (4, 7, 33, 34). Mean ejection fraction was29.9±17.8 % (12%-64%), and was dimin-ished in 88% of cases, which is also in agree-ment with the literature (7).
In our series, the area of noncompactionwas mainly in the apical and mid segments ofthe lateral and posterior walls. The process ofcompaction of the embryonic myocardiumprogresses from epicardium to endocardium,from the septum towards the lateral wall, andfrom the basal segments to the apex, whichmay explain the fact that it is the apical andlateral wall segments that are predominantlyaffected, as seen in our series as well as inother studies (18, 24). The interventricular septumis usually spared, at least its basal and midsegments.
The fact that in the patients studied thehypokinesia was not limited to the regions ofnoncompaction suggests that LVNC is a gen-eralized rather than focal cardiomyopathy andthat global myocardial function is affected.The hypokinesia would thus be due to gener-alized dysfunction (probably linked to theabove-mentioned microvascular dysfunction)rather than to the morphology of noncom-paction. On the other hand, global hypokine-sia could simply be the result of advanced car-diomyopathy in the dilated phase, in whichinitially unaffected segments eventually suc-cumb to chronic overload.
The high prevalence of LV dilatation in thestudy population is worth noting, as it promptsthe question as to whether this is the conse-quence of noncompaction or in fact the causeof acquired hypertrabeculation throughmyocardial remodeling. Differential diagnosisbetween LVNC and DCM is not straightfor-ward. Studies by Frischknecht et al. (35) suggestthat a significant percentage of patients withDCM may present intertrabecular recessesfilled with blood on color Doppler (48%) anda two-layer, noncompacted and compacted,myocardial structure (26%); however, end-systolic wall thickness of affected segments isconsiderably greater in LVNC (mean of 23 mmin noncompacted and 11 mm in compactedsegments, as opposed to 15 mm and 9 mm,respectively, in DCM). The increase in wall1860
Rev Port Cardiol Vol. 29 Dezembro 10 / December 10
2009-AR-76 Dezembro

cos estão pouco esclarecidos. Parece existiruma disfunção microvascular responsável porum deficit crónico de perfusão subendocár-dica e transmural e por uma reserva coronáriadiminuída(32), que por sua vez podem contri-buir para a disfunção sistólica, diastólica epara a arritmogénese. De facto, em cerca de26% dos doentes está descrita precordialgia(4)
apesar das coronárias não apresentarem le-sões significativas na angiografia, como era ocaso de um dos doentes da nossa série.
Metade dos doentes da nossa série encon-travam-se em classe I ou II da NYHA, o que estáde acordo com as séries publicadas na literatura(4,
7, 33, 34). A fracção de ejecção média aqui obtida foide 29,9 ± 17,8 % (12% - 64%), encontrando-sedeprimida em 88% dos casos, o que está tambémde acordo com as séries publicadas(7).
Na nossa pequena série, a área de não com-pactação atingiu sobretudo os segmentos apicaise medianos das paredes lateral e posterior. Defacto, o processo de compactação do miocárdioembrionário inicia-se a partir do epicárdio emdirecção ao endocárdio, do septo em direcção àparede lateral, e dos segmentos basais em direc-ção ao ápex, o que poderá explicar o predomíniode atingimento dos segmentos apicais e da pare-de lateral, documentado nesta série mas tambémdescrito noutros trabalhos(18, 24). De uma forma ge-ral, a não compactação poupa o septo interven-tricular, pelo menos nos seus segmentos basal emediano.
O facto de as zonas de hipocinésia não selimitarem, nos doentes estudados, às zonas denão compactação, sugere que a MNC é umamiocardiopatia generalizada e não focal, comatingimento funcional de todo o miocárdio. Ahipocinésia dever-se-ia portanto a uma dis-função generalizada (provavelmente secundáriaà disfunção microcirculatória descrita) e não àmorfologia de não-compactação. Por outro lado,a hipocinésia global pode ser simplesmente oresultado de uma miocardiopatia avançada, jáem fase dilatada, em que os segmentos queinicialmente não estariam atingidos acabariampor sofrer os danos de uma sobrecarga crónica.
De notar uma elevada prevalência de di-latação ventricular esquerda na população es-tudada. Poder-se-ia, neste contexto, questio-
thickness should be considered an importantcriterion for distinguishing LVNC from otherpathologies, particularly DCM. Furthermore,the presence of hypertrabeculation and a tra-becular meshwork was highly specific toLVNC in our population, of whom only threepresented severe LV dilatation and hence thepossibility of DCM, and in these the presenceof a pronounced trabecular meshwork made adiagnosis of LVNC more likely.
Only two of our patients developed thrombi.In early series of LVNC, a high percentage ofthromboembolic events was reported (21-38%)(4, 26, 36), but more recent reports suggest a lowerfrequency (4-5%) (33, 34). The development ofthrombi may be related to the highly trabeculat-ed LV which is prone to thrombus formation inthe intertrabecular recesses, to impaired globalsystolic function resulting in ventricular stasis,or to coexisting atrial fibrillation.
The percentage of patients in our serieswith intraventricular conduction block waslower than that reported elsewhere (44%) (4).Nonsustained ventricular tachycardia wasdetected in 50% of our patients on Holtermonitoring, which is in agreement with the lit-erature (sustained or nonsustained VT in 20-47% of patients (4, 7, 33), with the exception of aseries by Lofiego et al. (34) which showed aprevalence of 6%). In a study of 30 patientswith LVNC and mean follow-up of two and ahalf years, Stanton et al. (37) reported mortalitysimilar to that for non-ischemic DCM, sug-gesting that LV dysfunction rather than non-compacted myocardium is the main cause ofdeath, arrhythmic or otherwise, which sup-ports the standard practice of treating LVNCin accordance with heart failure guidelines.
There is, in fact, as yet no specific treat-ment for LVNC. Patients receive state-of-the-art treatment for heart failure when this ispresent. Similarly, prevention of malignantarrhythmias can consist of pharmacologicaltherapy or implantation of an ICD when indi-cated. There is disagreement concerning theuse of anticoagulation therapy due to the con-siderable variation in frequency of throm-boembolic events in different series. Mostauthors recommend antiplatelet therapy for all 1861
Alexandra Toste, et al.Rev Port Cardiol 2010; 29: 1847-1864
2009-AR-76 Dezembro

nar a etiologia da dilatação ventricular es-querda: seria a consequência da não com-pactação ou, pelo contrário, seria ela própria acausa de uma hipertrabeculação adquiridamediada por um processo de remodellingmiocárdico? De facto, o diagnóstico diferen-cial entre MNC e miocardiopatia dilatada nãoé linear. Estudos realizados por Frischknechte colaboradores(35) sugerem que uma percen-tagem considerável de doentes com miocar-diopatia dilatada pode apresentar recessosintertrabeculares preenchidos Doppler a cor(48%) e o padrão de miocárdio com dupla ca-mada, NC e C (26%); no entanto, a espessuraparietal telessistólica dos segmentos envol-vidos é significativamente superior na MNC(em média 23 mm nos segmentos NC e 11 nossegmentos C da MNC versus 15 mm nossegmentos “NC” e 9 mm nos segmentos “C” damiocardiopatia dilatada). O aumento daespessura da parede envolvida deve serconsiderado um importante critério na distin-ção de MNC de outras patologias, nomea-damente miocardiopatia dilatada. Por outrolado, a presença de hipertrabeculação e derede trabecular revelou-se, nesse trabalho, al-tamente específico de MNC. Em relação aonosso grupo de doentes, em apenas três dosnossos doentes a dilatação ventricular esquer-da é grave, e portanto à partida apenas nessescasos poder-se-ia colocar esta questão; e nes-tes, a presença de uma rede trabecular exube-rante pareceu-nos mais sugestiva do diagnós-tico de MNC que de miocardiopatia dilatada.
Apenas dois doentes da nossa série desen-volveram eventos trombóticos. Nas primeiras sé-ries, os eventos tromboembólicos estavam docu-mentados numa elevada percentagem, entre os21 e os 38%(4, 26, 36). No entanto, séries mais recen-tes sugerem uma frequência inferior, entre os 4 eos 5%(33, 34). O desenvolvimento de trombos podeestar relacionado com a presença de um VE ex-tensamente trabeculado e como tal propício àformação de trombos no espaço intertrabecular,com a diminuição da função sistólica global econsequente estase intraventricular – à seme-lhança do que acontece noutros tipos de miocar-diopatia dilatada – ou ainda com a coexistênciade fibrilhação auricular.
patients, combined with anticoagulation onlyin high-risk situations, such as a history ofsystemic embolism, the presence of intraven-tricular thrombi, severe LV dysfunction (ejec-tion fraction <25%) or atrial fibrillation (7, 34).Murphy et al. (33) suggest that the presence ofdense and extensive trabeculation is itself isan indication for oral anticoagulation, irre-spective of ejection fraction, while Oechslin etal. (4) propose routine oral anticoagulant thera-py for all patients.
According to Aras et al. (7), mortality can bepredicted from initial ejection fraction andlast functional capacity assessment. The firststudies reported rates of death or heart trans-plantation of around 47% at 44 months (4),while later series show much lower rates (3%at 46 months) (22). There were two deaths in ourseries of eight patients with a median follow-upof 14 months: one patient died of stroke andthe other had the worst functional class andejection fraction at diagnosis. Of the six sur-vivors, four are currently in NYHA class IIand the other two are in class I.
CONCLUSION
Isolated left ventricular noncompaction isa primary cardiomyopathy with a familial ori-gin in over 50% of cases, and most authorsaccordingly recommend echocardiographicscreening of relatives. It has a broad clinicalspectrum, from absence of symptoms to severeheart failure, as demonstrated in this series, inmost of whom LV ejection fraction was seri-ously impaired. The most frequent location ofnoncompaction was the lateral and posteriorwalls, particularly the apical segments, whichis in agreement with the literature.
There is as yet no specific treatment forLVNC; patients essentially receive treatmentfor heart failure and prevention of malignantarrhythmias. All should take antiplateletagents and most authors recommend anticoag-ulation only in high-risk cases. We recordedtwo deaths in a 14-month follow-up.
1862
Rev Port Cardiol Vol. 29 Dezembro 10 / December 10
2009-AR-76 Dezembro

A percentagem de doentes com bloqueio dacondução intraventricular foi, na nossa série,inferior ao que está descrito - 44% dos doentes(4).Em 50% dos nossos doentes documentaram-seTVNM no registo de Holter, o que está de acordocom a literatura (TVNM ou mantida em 20-47%dos doentes(4, 7, 33) com a excepção de uma sériepublicada por Lofiego et al(34) que documentauma prevalência de 6%). Stanton e colaborado-res(37), num estudo com 30 doentes com MNC ecom um seguimento médio de dois anos e meio,reporta uma taxa de mortalidade semelhante àverificada em doentes com miocardiopatia di-latada não isquémica, sugerindo que a disfunçãoVE, e não o miocárdio não compactado, é a fonteprimária de mortalidade, de causa arritmogénicaou outra, o que apoia a prática clínica correntede tratamento desta entidade de acordo com asrecomendações clínicas para a insuficiênciacardíaca.
De facto, até à data não existe terapêuticaespecífica para a MNC. Estes doentes têm sidotratados de acordo com o estado da arte para ainsuficiência cardíaca, sempre que esta se en-contra presente. Da mesma forma, a prevençãode arritmias malignas pode passar pela tera-pêutica farmacológica, bem como pela implan-tação de CDI quando estabelecida essa indi-cação. A decisão de anticoagular estes doentesnão é consensual, o que advém da grandediscrepância entre as frequências de eventostromboembólicos entre as várias séries. A maiorparte dos autores preconiza a antiagregaçãopara todos os doentes, à qual se deveria associaranticoagulação apenas perante coexistência desituações de alto risco, nomeadamente histó-ria de embolismo sistémico, presença de trom-bos intraventriculares, disfunção ventricularesquerda grave (fracção de ejecção <25%) oufibrilhação auricular(7, 34). Murphy e colabora-dores(33) sugerem que a presença de trabecula-ção densa e extensa por si só pode constituir in-dicação para anticoagulação oral, independen-temente da fracção de ejecção. Por outro lado,Oechslin e colaboradores(4) propõem anticoa-gulação oral para todos os doentes por rotina.
A mortalidade depende, segundo Aras et al,da fracção de ejecção aquando da apresentaçãoinicial e da capacidade funcional na última
observação. Os estudos iniciais reportavam umataxa de morte ou transplante cardíaco na ordemdos 47% aos 44 meses se bem que estudos maisrecentes documentam uma taxa de transplan-te ou morte bem mais inferior (3% aos 46 me-ses)(22). Na nossa série de oito doentes, com se-guimento mediano de 14 meses, reportamosuma mortalidade de dois doentes, um dos quaispor AVC. O outro caso tratava-se precisamentedo doente que tinha, aquando do diagnóstico,pior classe funcional e fracção de ejecção maisbaixa. Dos seis doentes sobreviventes, quatroencontram-se actualmente em classe II e osrestantes em classe I da NYHA.
CONCLUSÃO
A MNC é uma miocardiopatia primáriacom origem familiar em mais de 50% doscasos, motivo pelo qual a maior parte dosautores recomenda o rastreio ecocardiográficodos familiares. Apresenta um espectro clínicomuito abrangente, que varia desde a ausênciade sintomas até à insuficiência cardíaca gravecomo demonstrado nesta série. A fracção deejecção do VE revelou-se geralmente muitocomprometida neste grupo de doentes. A zonade não compactação foi mais frequente a níveldas paredes lateral e posterior, sobretudo nosseus segmentos apicais, o que está de acordocom a literatura.
Actualmente não existe terapêutica espe-cífica para a MNC, sendo que esta passa so-bretudo pelo tratamento da insuficiênciacardíaca e prevenção de arritmias malignas.Todos os doentes devem estar antiagregados ea maioria dos autores preconiza anticoa-gulação apenas em doentes de alto risco. Du-rante o seguimento mediano de 14 mesesreportamos a mortalidade de dois doentes.
Pedido de separatas para:Address for Reprints: Alexandra TosteMorada: Rua de Santa Marta, nº 50 1169-024 LisboaTelefone: 213 594 000e-mail: [email protected] 1863
Alexandra Toste, et al.Rev Port Cardiol 2010; 29: 1847-1864
2009-AR-76 Dezembro

1864
Rev Port Cardiol Vol. 29 Dezembro 10 / December 10
2009-AR-76 Dezembro
Recebido para publicação: ????????????? • Aceite para publicação: ?????????Received for publication: ????????????? • Accepted for publication: ?????????
1. Maron B.J. Towbin J.A. Thiene G. et al. Contemporary definitions andclassification of the cardiomyopathies: an American Heart AssociationScientific Statement from the Council on Clinical Cardiology. Heart Failureand Transplantation Committee; Quality of Care and Outcomes Researchand Functional Genomics and Translational Biology InterdisciplinaryWorking Groups; and Council on Epidemiology and Prevention. Circulation2006;113:1807-16.
2. Elshershari H. Okutan V. Celiker A. Isolated noncompaction of the ven-tricular myocardium. Cardiol Young. 2001;11:472-475.
3. Kohli S.K. Pantazis A.A. Shah J.S. et al. Diagnosis of left-ventricular non-compaction in patients with left-ventricular systolic dysfunction: time for areappraisal of diagnostic criteria? Eur Heart J (2008) 29. 89-95.
4. Oechslin E.N. Attenhofer Jost C.H. Rojas J.R. Kaufmann PA. Jenni R.Long-term follow-up of 34 adults with isolated left ventricular noncom-paction: a distinct cardiomyopathy with poor prognosis. J Am Coll Cardiol2000;36:493-500.
5. Petersen S.E. Selvanayagam J.B, Wiesmann F. et al. Left Ventricular Non-Compaction: Insights from Cardiovascular Magnetic Resonance Imaging. JAm Coll Cardiol. 2005 Jul 5;46(1):101-5.
6. Richardson P, McKenna W, Bristow M. et al. Report of the 1995 WorldHealth Organization/International Society and Federation of Cardiology TaskForce on the definition and classification of cardiomyopathies. Circulation1996; 93:841-2.
7. Aras D, Tufekcioglu O, Ergun K. et al. Clinical Features of IsolatedVentricular Noncompaction in Adults Long-Term Clinical Course,Echocardiographic Properties, and Predictors of Left Ventricular Failure. JCard Fail. 2006 Dec;12(9):726-33.
8. Pignatelli R.H, McMahon C.J, Dreyer W.J, et al. Clinical characterizationof left ventricular noncompaction in children: a relatively common form ofcardiomyopathy. Circulation 2003;108:2672-8.
9. Belanger A.L, Miller M.A, Donthireddi U.R, Najovits A.J, Goldman M.E.New classification scheme of left ventricular noncompaction and correlationwith ventricular performance. Am J Cardiol. 2008 Jul 1;102(1):92-6.
10. Coelho L, da Silva A.M, Martins R, Sá e Melo A, Providência L.A.Isolated non-compaction of left ventricular myocardium. Rev Port Cardiol.2000 Jun;19(6):727-31.
11. Pereira A, Thomas B, Tavares N.J. Magnetic resonance imaging findings innon-compaction of the left ventricle. Rev Port Cardiol. 2007 Mar;26(3):303-4.
12 Galrinho A, Rosário L, Loureiro C, Mourão L. A case of heart failure withan uncommon etiology. Rev Port Cardiol 2001 Jun;20(6):681-4.
13. Magno P, Freitas A, Gil V.M. Não compactação do ventrículo esquerdo:revisão da literatura a propósito de um caso clínico. Rev Port Cardiol 2007;26 (12): 1381-1391.
14. Botelho A, Providência R, Cavaco D. et al. Uma etiologia rara deextrassistolia ventricular: ventrículo esquerdo não compactado. Rev PortCardiol 2008; 27 (2):231-240.
15. Sá M.I, Reis H, Cabral S, et al. Não compactação do miocárdio ventricular.Rev Port Cardiol. 2006 Sep;25(9):835-44.
16. Cortez-Dias N, Varela M.G, Sargento L, et al. Não-compactação doventrículo esquerdo: uma nova mutação associada a capacidade de contra-remodelação ventricular? Rev Port Cardiol. 2009 Feb;28(2):185-94.
17. Sá M.I, Cabral S, Costa P.D. et al. Envolvimento cardíaco na DistrofiaMiotónica tipo 1. Rev Port Cardiol. 2007 Sep;26(9):829-40.
18. Stöllberger C, Blazek G, Winkler-Dworak M, Finsterer J. Diferencias desexo en la ausencia de compactación ventricular izquierda con y sin trastor-nos neuromusculares. Rev Esp Cardiol. 2008;61(2):130-6
BIBLIOGRAFIA / REFERENCES
19. Stöllberger C, Keller H, Finsterer J. Disappearance of left-ventricularhypertrabeculation / noncompaction after biventricular pacing. J CardiacFail. 2007;13:211-4.
20. Hofer M, Stöllberger C, Finsterer J. Acquired noncompaction associat-ed with myopathy. Int J Cardiol. 2006;121:296-7.
21. Finsterer J, Stöllberger C, Schubert B. Acquired left ventricular non-compaction as a cardiac manifestation of neuromuscular disorders. ScandCardiovasc J. 2008 Feb;42(1):25-30.
22. Bowles N.E, Towbin J.A. The failing heart. Nature. 2002;415:227-233.
23. Monserrat Iglesias L. Left Ventricular Noncompaction: A Disease inSearch of a Definition. Rev Esp Cardiol. 2008;61(2):112-5.
24. Jenni R, Oechslin E, Schneider J, Attenhofer J, Kaufmann PA.Echocardiographic and pathoanatomical characteristics of isolated left ven-tricular non-compaction: a step towards classification as a distinct car-diomyopathy. Heart 2001;86:666-671.
25. Chin T.K, Perloff J.K, Williams R.G, Jue K, Mohrmann R. Isolated non-compaction of left ventricular myocardium. A study of eight cases.Circulation 1990;82:507-513.
26. Stollberger C, Finsterer J, Blazek G. Left ventricular hypertrabeculation,noncompaction and association with additional cardiac abnormalities andneuromuscular disorders. Am J Cardiol 2002; 90:899-902.
27. Monserrat L, Hermida-Prieto M, Fernandez X. et al. Mutation in the alpha-cardiac actin gene associated with apical hypertrophic cardiomyopathy, left ven-tricular noncompaction, and septal defects. Eur Heart J. 2007; 28:1953-61.
28. Pantazis A.A, Kohli S.K, Elliott P.M. Images in cardiology: Hypertrophiccardiomyopathy and left ventricular hypertrabeculation: evidence for anoverlapping phenotype. Heart. 2006;92:349.
29. Biagini E, Ragni L, Ferlito M. et al. Different types of cardiomyopathyassociated with isolated ventricular noncompaction. Am J Cardiol.2006;98:821-4.
30. Xia S, Wang H, Zhang X, Zhu J, Tang X. Clinical Presentation andGenetic Analysis of a Five Generation Chinese Family with Isolated LeftVentricular Noncompaction. Intern Med. 2008;47(7):577-83.
31. Hoedemaekers Y.M, Caliskan K, Majoor-Krakauer D. et al. Cardiacbeta-myosin heavy chain defects in two families with non-compaction car-diomyopathy: linking non-compaction to hypertrophic, restrictive, and dilat-ed cardiomyopathies. Eur Heart J. 2007;28:2732-7.
32. Jenni R, Wyss C.A, Oechslin E.N, Kaufmann PA. Isolated VentricularNoncompaction Is Associated With Coronary Microcirculatory Dysfunction.JACC Vol. 39, No. 3, 2002 February 6, 2002:450-4.
33. Murphy R.T, Thaman R, Blanes J.G. et al. Natural history and familialcharacteristics of isolated left ventricular non-compaction. Eur Heart J2005;26:187-92.
34. Lofiego C, Biagini E, Pasquale F. et al. Wide spectrum of presentationand variable outcomes of isolated left ventricular noncompaction. Heart.2007 Jan;93(1):65-71.
35. Frischknecht B.S, Attenhofer Jost C.H, Oechslin E.N. et al. Validation ofnoncompaction criteria in dilated cardiomyopathy, and valvular and hyperten-sive heart disease. J Am Soc Echocardiogr. 2005 Aug;18(8):865-72.
36. Ritter M, Oechslin E, Sütsch G, Attenhofer C, Schneider J, Jenni R.Isolated noncompaction of the myocardium in adults. Mayo Clin Proc1997;72:26-31.
37. Stanton C, Bruce C, Connolly H. et al. Isolated left ventricular noncom-paction syndrome. Am J Cardiol. 2009 Oct 15; 104(8):1135-8. Epub 2009Aug 28.