imunoterapia: manejo de efeitos colaterais agudos e tardios · slide cedido dr carlos dos anjos....
TRANSCRIPT
Fernando Costa SantiniMédico Titular do Centro de Oncologia do Hospital Sirio Libanes
Médico Assistente do Instituto do Cancer do Estado de Sao Paulo
Especializado em Oncologia Torácica pelo Memorial Sloan Kettering Cancer Center
Oncologia Clínica pelo Hospital Sirio Libanes
Hematologia pela Universidade de São Paulo
Imunoterapia: Manejo de efeitos colaterais
agudos e tardios
• Pesquisa Clínica – Como investigador: Roche, BMS
• Apresentações científicas – Como palestrante convidado: MSD, Novartis, BMS e AstraZeneca
• Advisory Board – AstraZeneca, BMS
Conflitos de interesse
Mudança de Paradigma
Slide cedido Dr Carlos dos Anjos
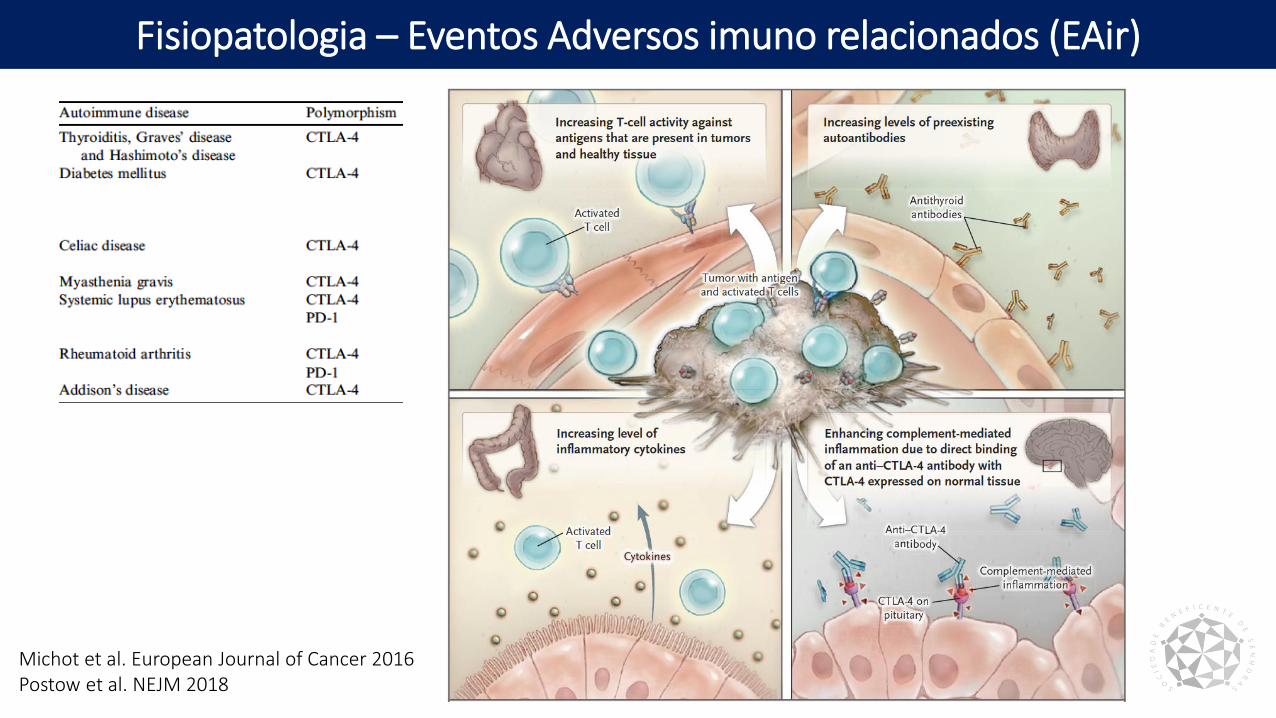
Fisiopatologia – Eventos Adversos imuno relacionados (EAir)
Michot et al. European Journal of Cancer 2016Postow et al. NEJM 2018
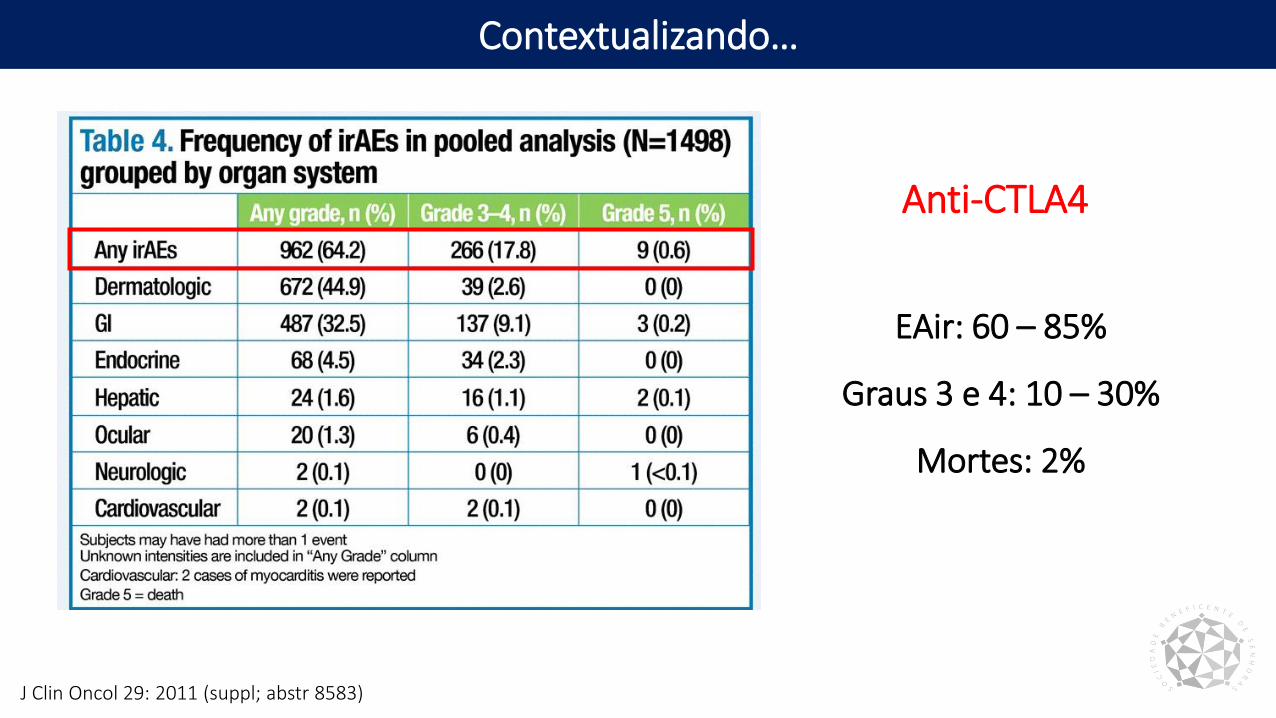
Contextualizando…
J Clin Oncol 29: 2011 (suppl; abstr 8583)
EAir: 60 – 85%
Graus 3 e 4: 10 – 30%
Mortes: 2%
Anti-CTLA4
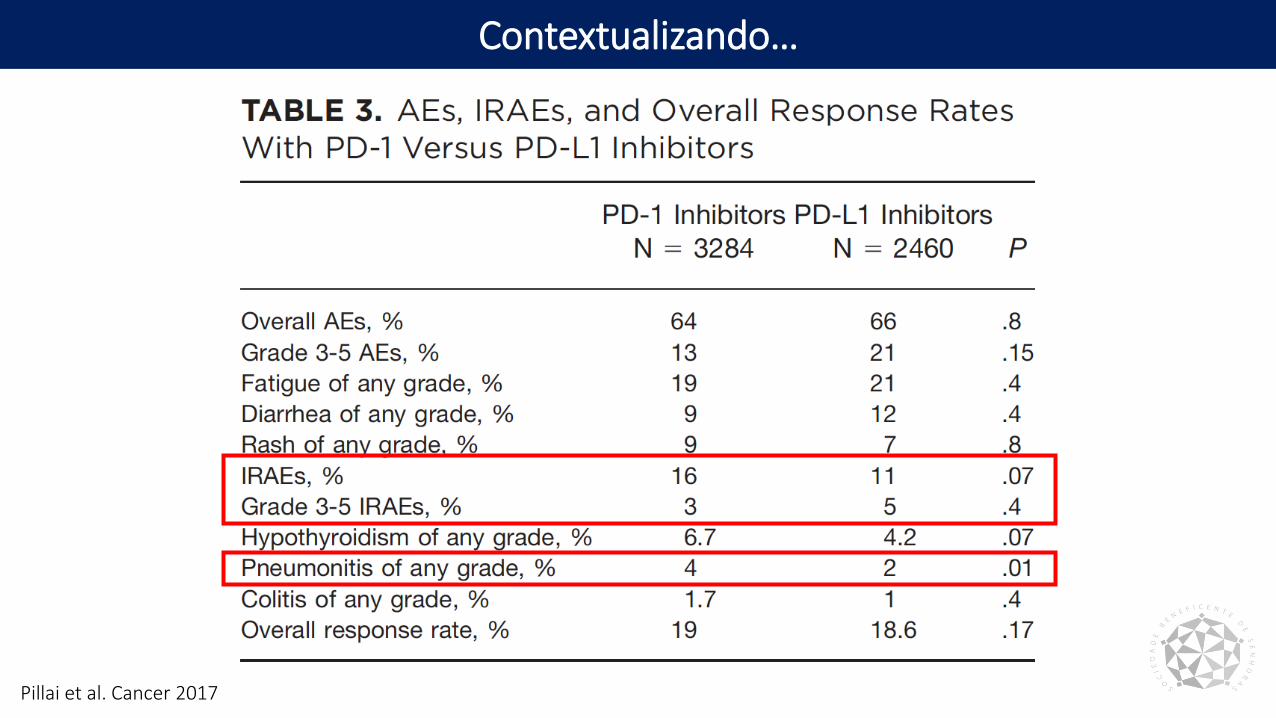
Contextualizando…
Pillai et al. Cancer 2017
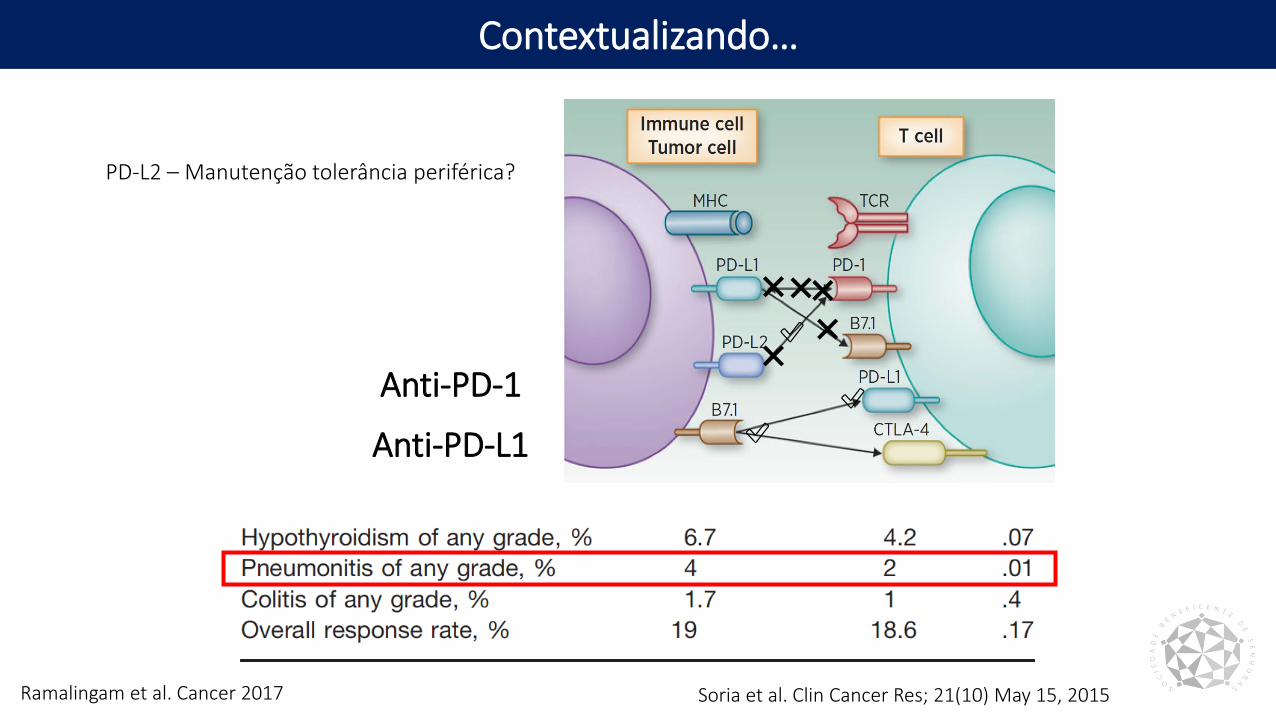
Contextualizando…
Ramalingam et al. Cancer 2017 Soria et al. Clin Cancer Res; 21(10) May 15, 2015
❌❌
❌
❌
✅
✅Anti-PD-1
Anti-PD-L1
❌✅
PD-L2 – Manutenção tolerância periférica?
Nivo 3 Q2W+ Ipi 1 Q12W
(n = 38)
Nivo 3 Q2W+ Ipi 1 Q6W
(n = 39)Nivo 3 Q2W
(n = 52)
Any grade
Grade 3–4
Any grade
Grade 3–4
Any grade
Grade 3–4
Treatment-related AEs, % 82 37 72 33 71 19
Treatment-related AEs leading to discontinuation, %
11 5 13 8 10 10
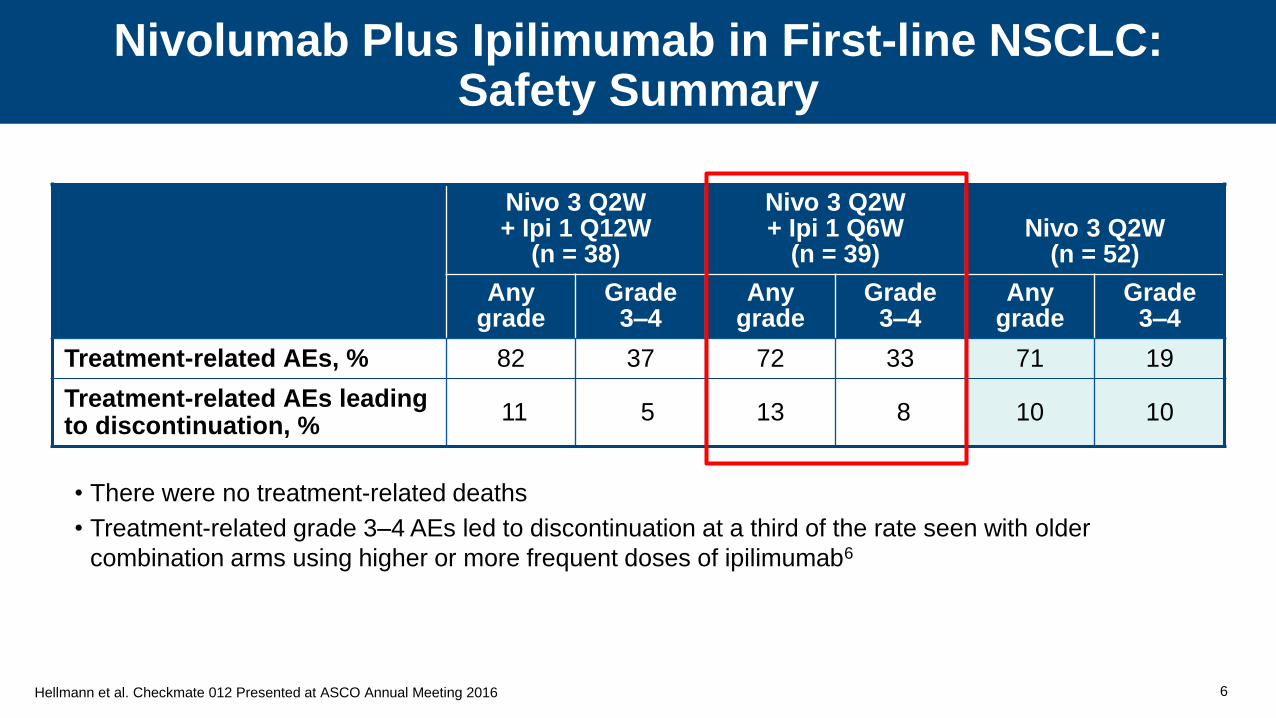
Nivolumab Plus Ipilimumab in First-line NSCLC:Safety Summary
6
• There were no treatment-related deaths
• Treatment-related grade 3–4 AEs led to discontinuation at a third of the rate seen with older
combination arms using higher or more frequent doses of ipilimumab6
Hellmann et al. Checkmate 012 Presented at ASCO Annual Meeting 2016
Contextualizando…
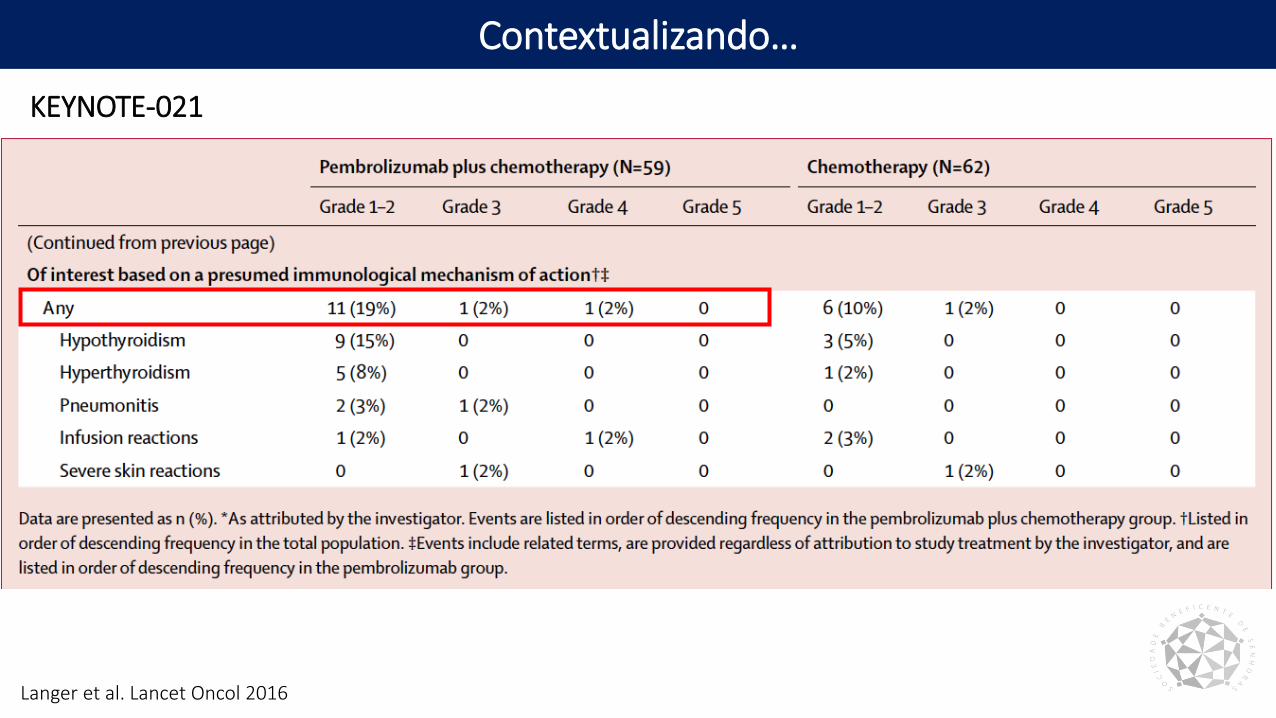
Langer et al. Lancet Oncol 2016
KEYNOTE-021
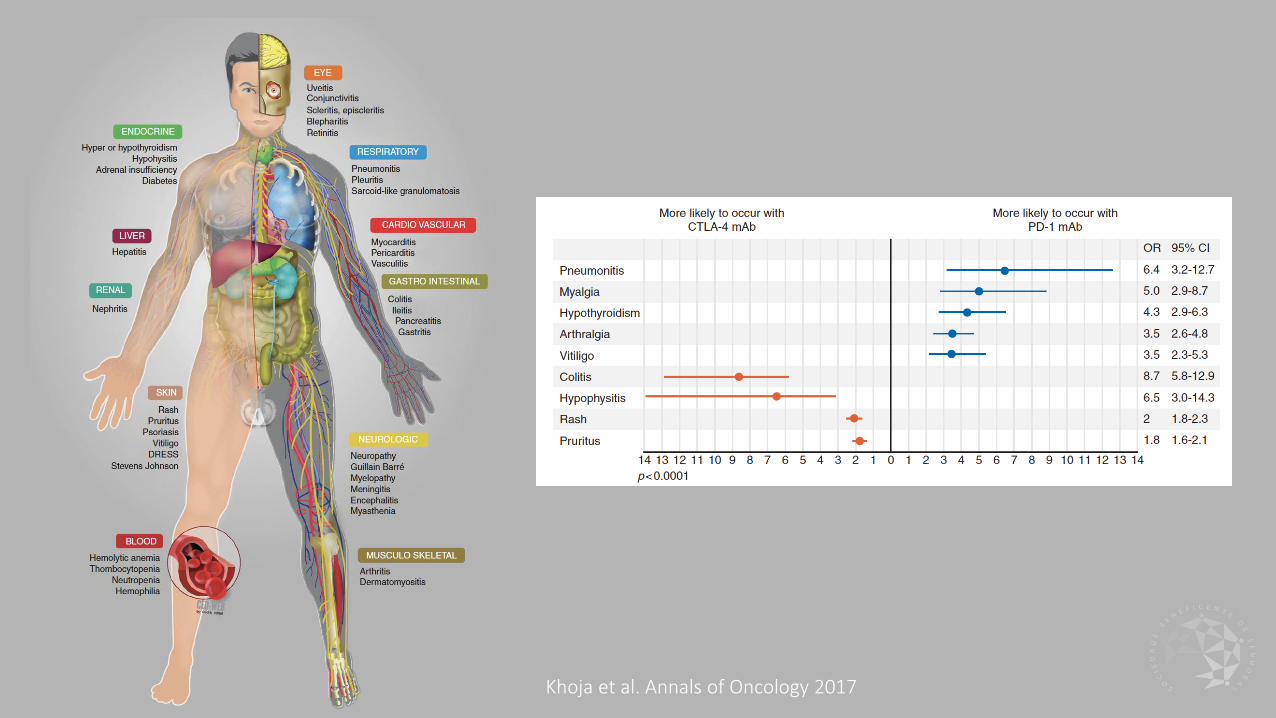
Khoja et al. Annals of Oncology 2017
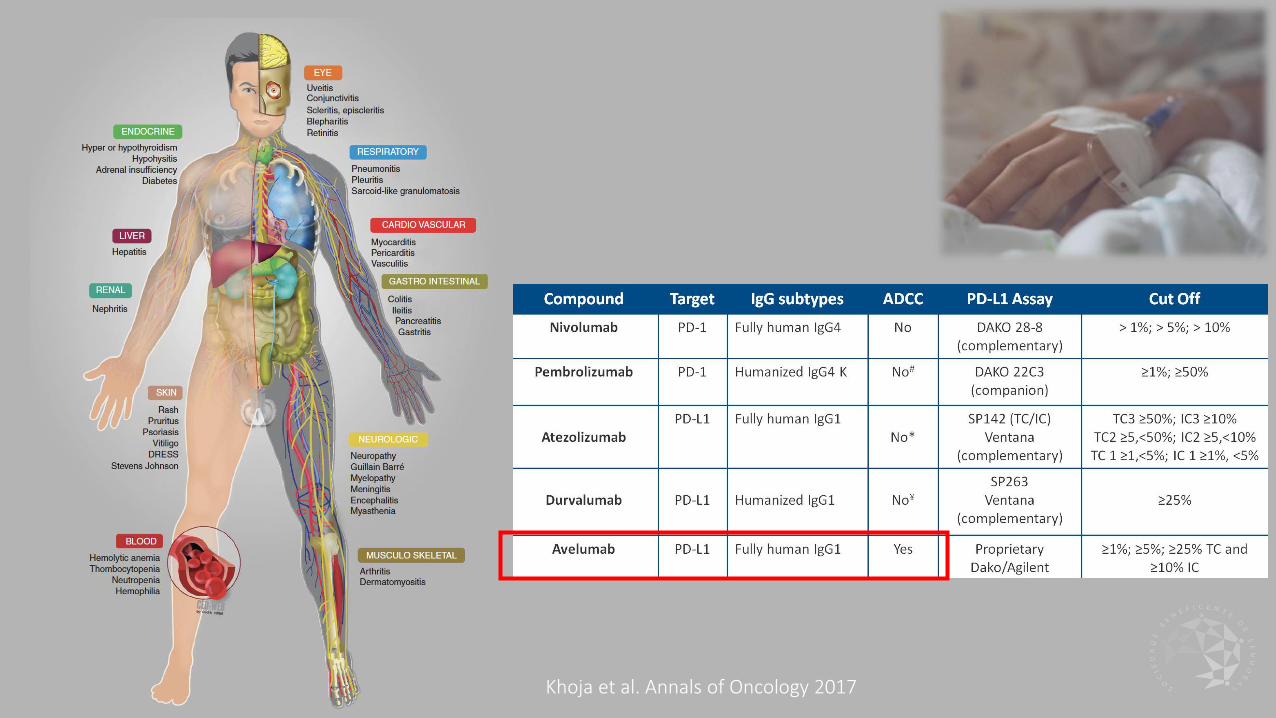
Khoja et al. Annals of Oncology 2017
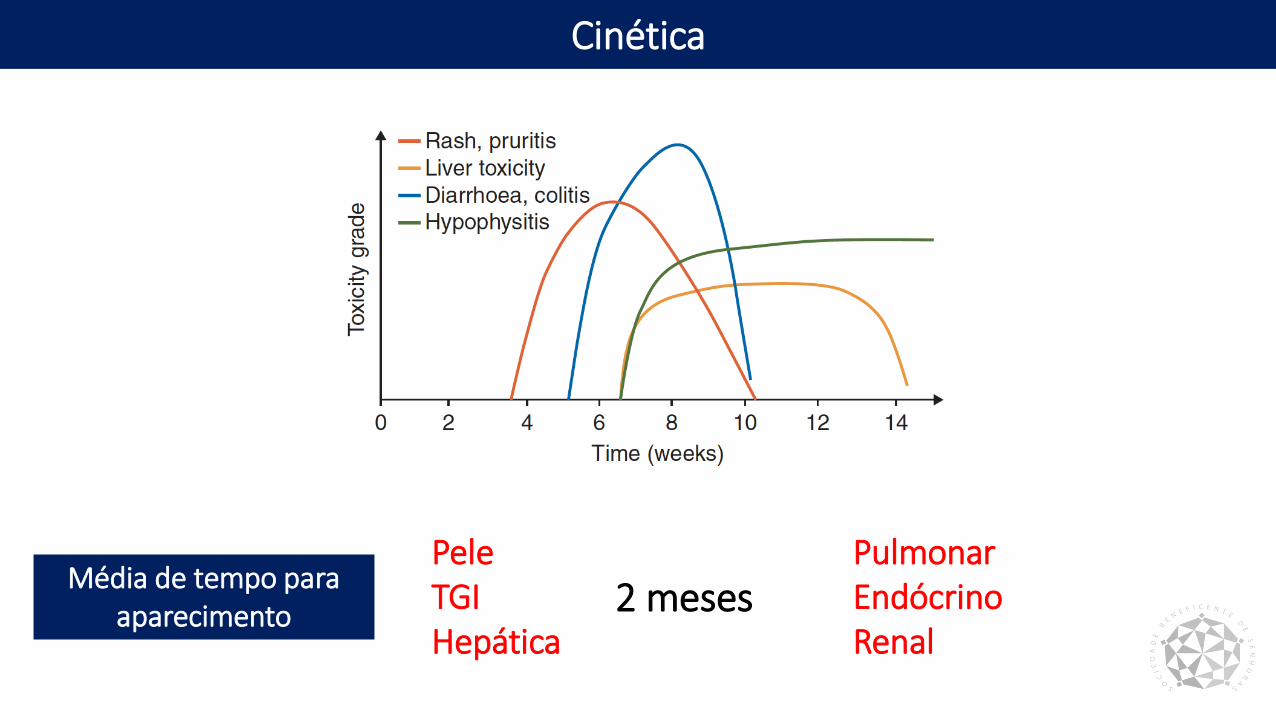
Cinética
Média de tempo para aparecimento
PeleTGIHepática
2 mesesPulmonar EndócrinoRenal
Manejo Adequado
Champiat et al. Annals of Oncology 2016
• Conhecer os EAir• Fatores de risco• Patógenos oportunistas• Medicação• Condições especiais
• Diagnósticos diferenciais• Progressão
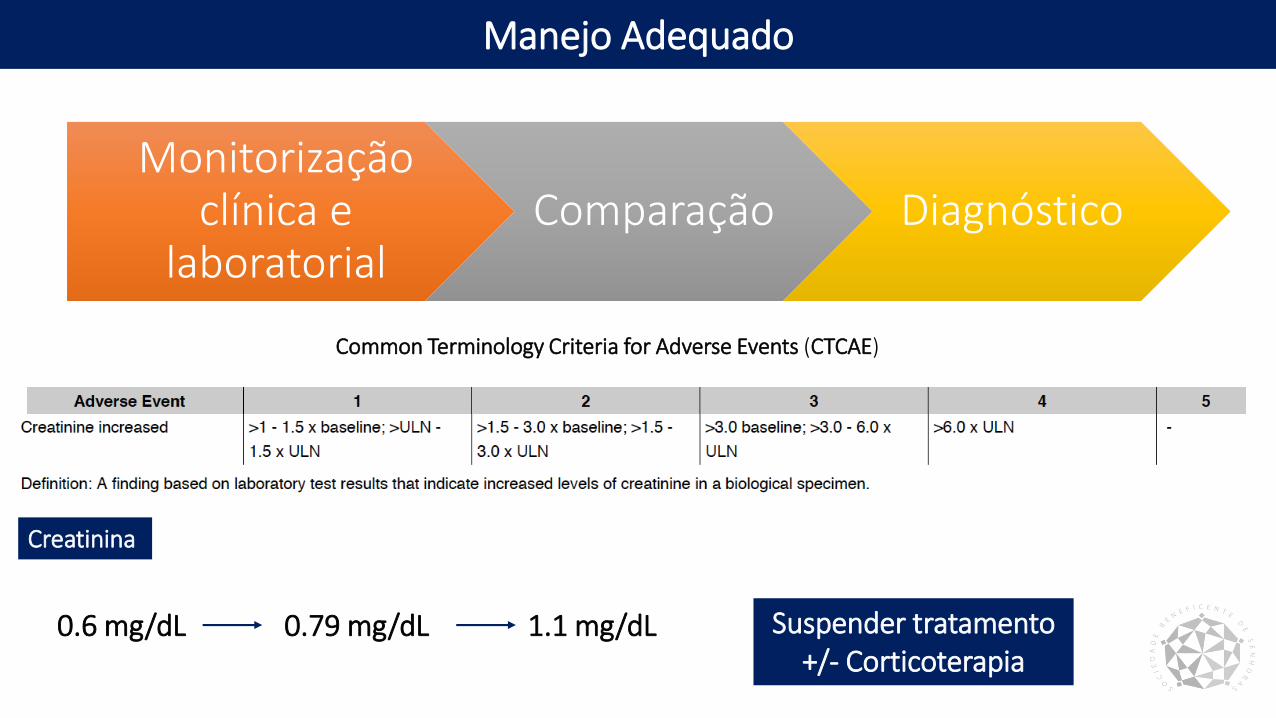
Manejo Adequado
Monitorização clínica e
laboratorialComparação Diagnóstico
Creatinina
0.6 mg/dL 0.79 mg/dL 1.1 mg/dL Suspender tratamento+/- Corticoterapia
Common Terminology Criteria for Adverse Events (CTCAE)
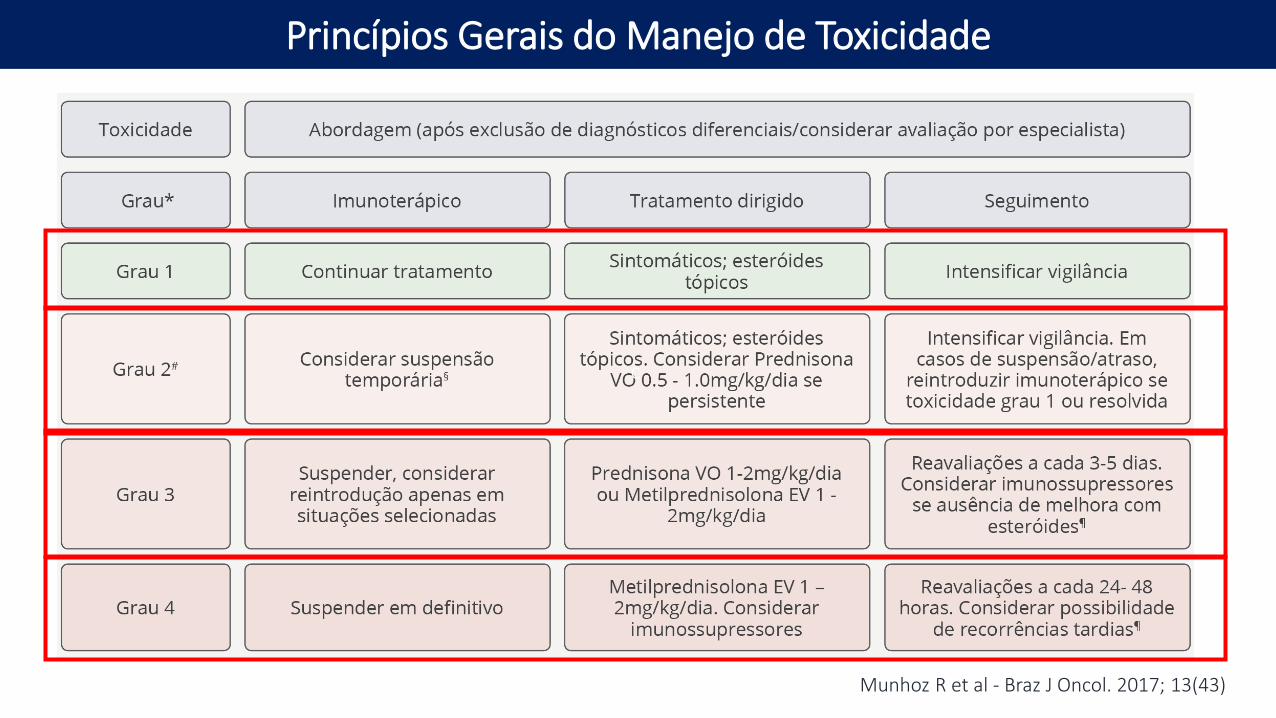
Princípios Gerais do Manejo de Toxicidade
Munhoz R et al - Braz J Oncol. 2017; 13(43)
c
Fadiga
Pele
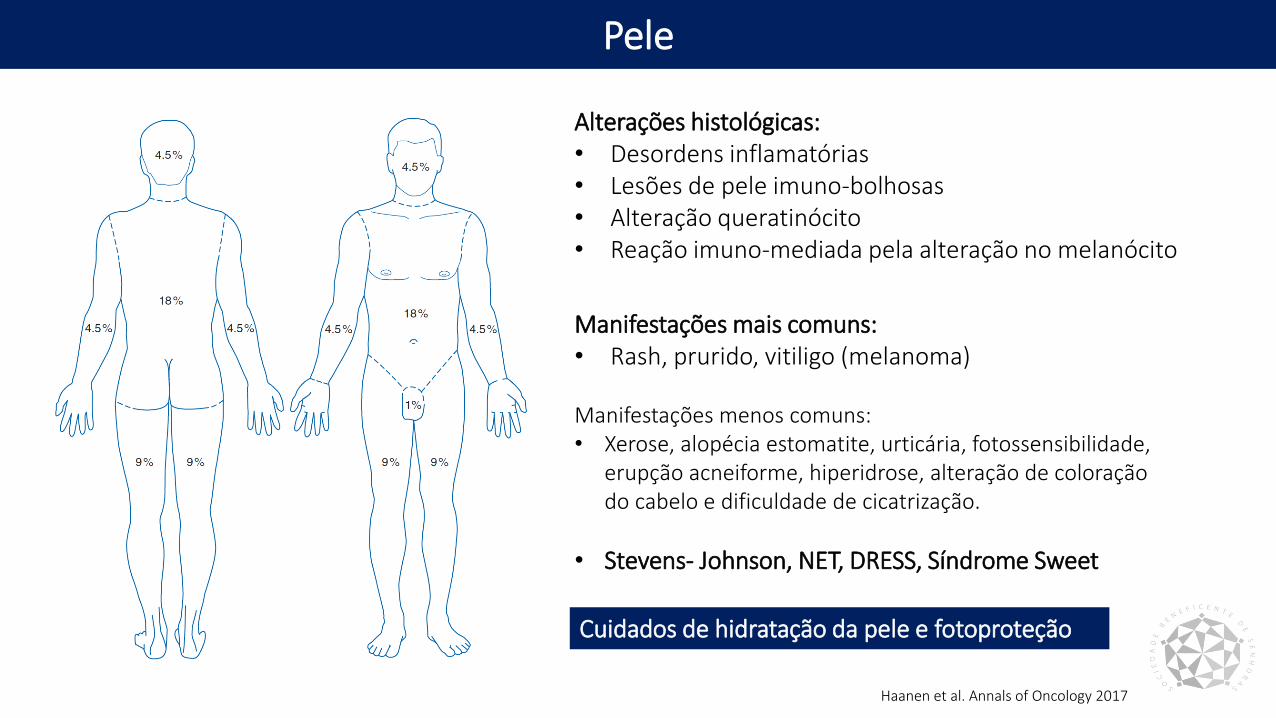
Alterações histológicas:• Desordens inflamatórias• Lesões de pele imuno-bolhosas• Alteração queratinócito• Reação imuno-mediada pela alteração no melanócito
Manifestações mais comuns:• Rash, prurido, vitiligo (melanoma)
Manifestações menos comuns:• Xerose, alopécia estomatite, urticária, fotossensibilidade,
erupção acneiforme, hiperidrose, alteração de coloração do cabelo e dificuldade de cicatrização.
• Stevens- Johnson, NET, DRESS, Síndrome Sweet
Cuidados de hidratação da pele e fotoproteção
Haanen et al. Annals of Oncology 2017
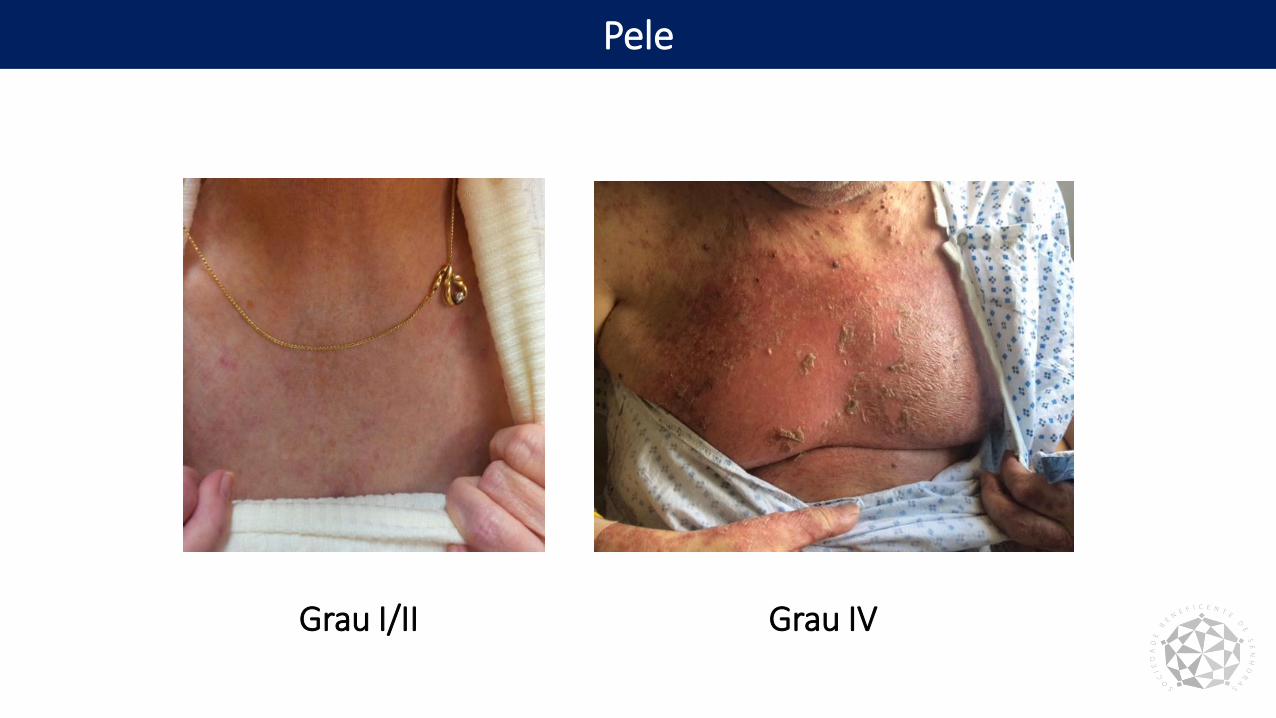
Pele
Grau I/II Grau IV
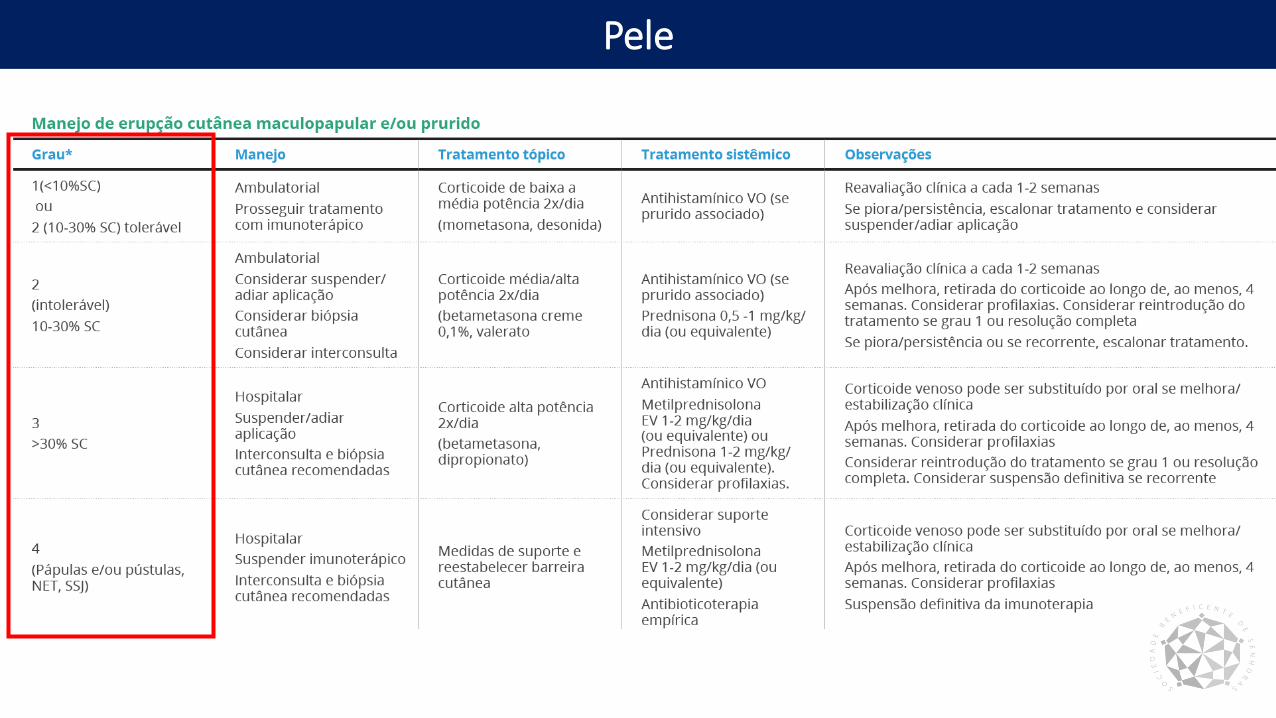
Pele
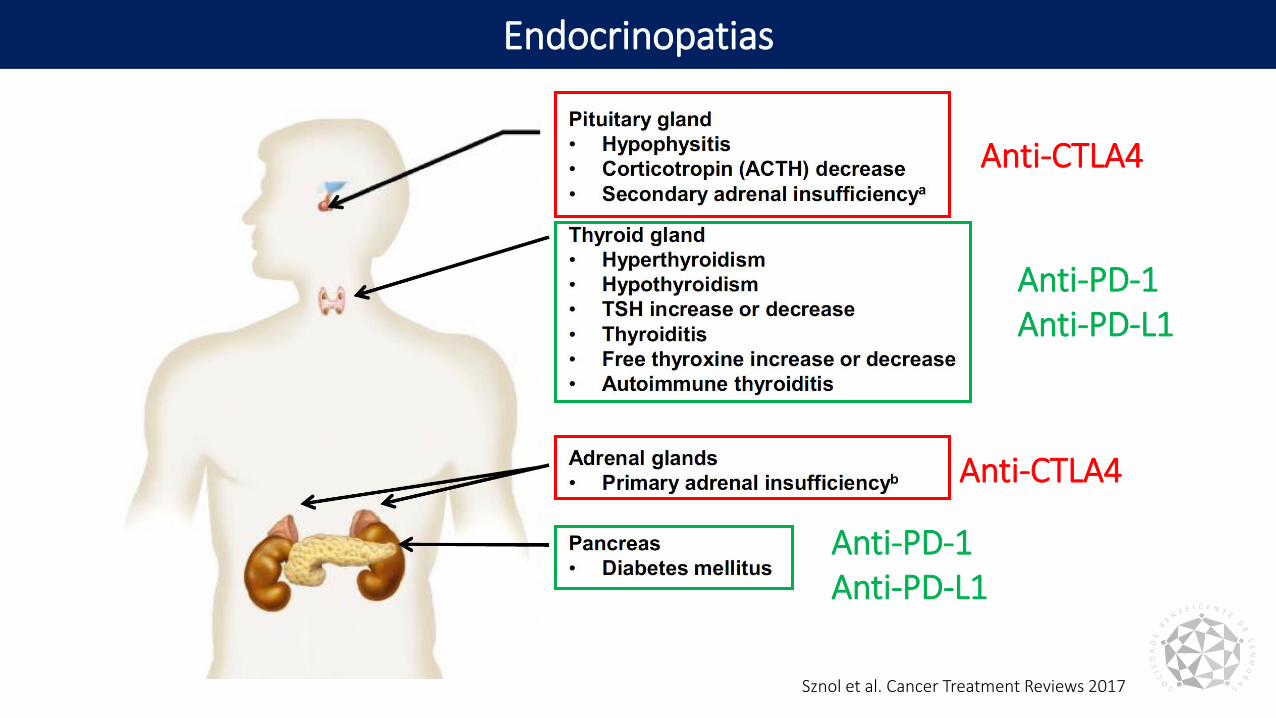
Endocrinopatias
Sznol et al. Cancer Treatment Reviews 2017
Anti-CTLA4
Anti-PD-1Anti-PD-L1
Anti-PD-1Anti-PD-L1
Anti-CTLA4
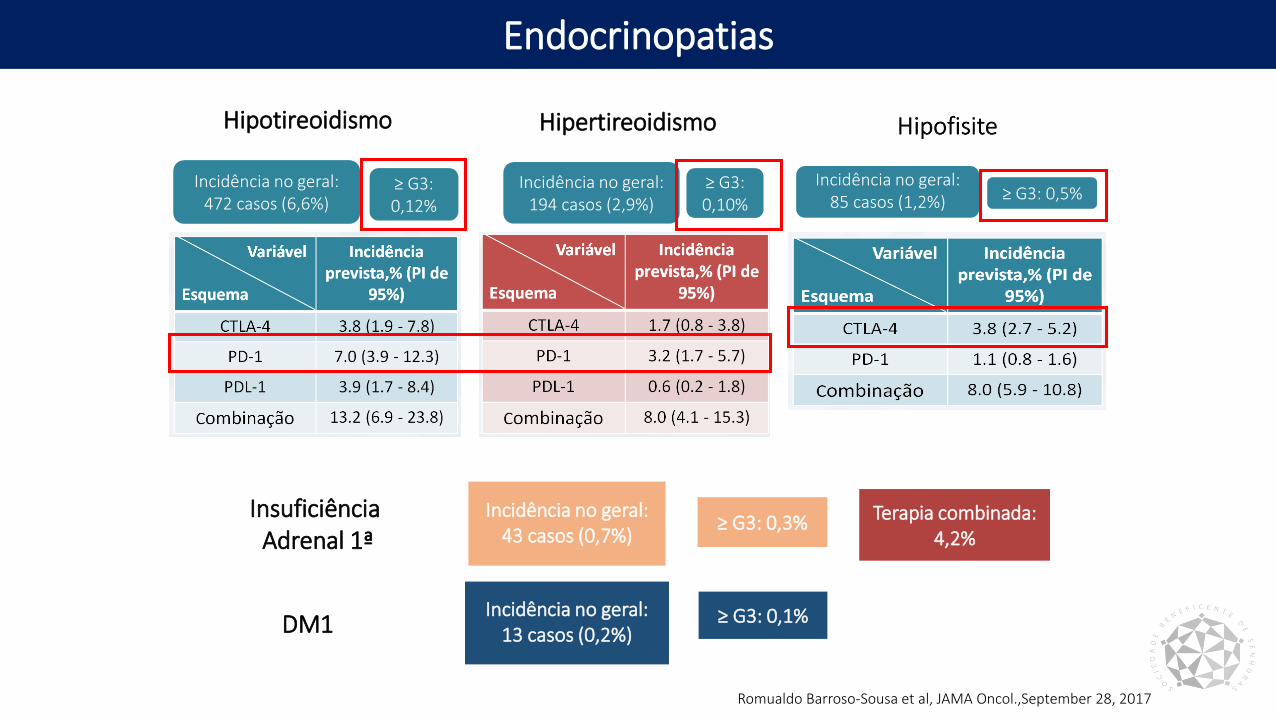
Endocrinopatias
Incidência no geral:472 casos (6,6%)
≥ G3: 0,12%
Hipotireoidismo Hipertireoidismo
Incidência no geral:194 casos (2,9%)
≥ G3: 0,10%
Incidência no geral:85 casos (1,2%) ≥ G3: 0,5%
InsuficiênciaAdrenal 1ª
Incidência no geral:43 casos (0,7%)
Terapia combinada: 4,2%
≥ G3: 0,3%
Incidência no geral:13 casos (0,2%)
≥ G3: 0,1%DM1
Romualdo Barroso-Sousa et al, JAMA Oncol.,September 28, 2017
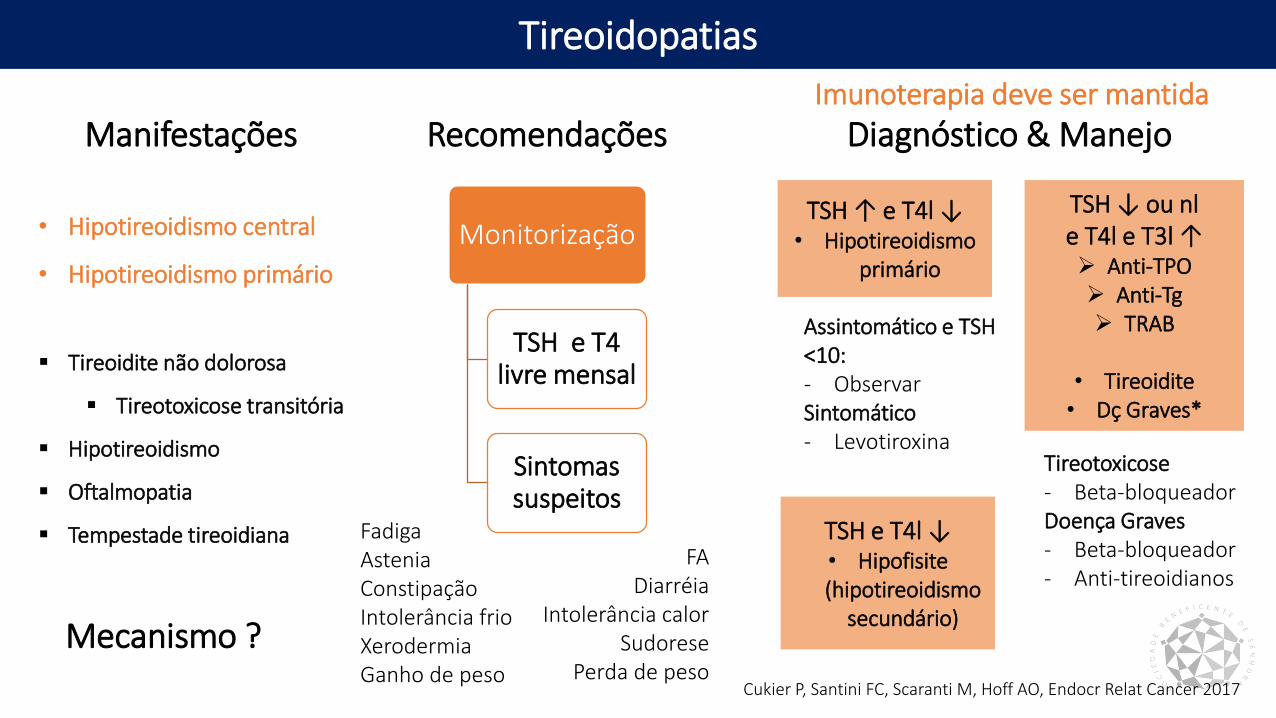
Tireoidopatias
Monitorização
TSH e T4 livre mensal
Sintomas suspeitos
Recomendações
TSH e T4l ↓• Hipofisite(hipotireoidismo
secundário)
Manifestações
Cukier P, Santini FC, Scaranti M, Hoff AO, Endocr Relat Cancer 2017
TSH ↑ e T4l ↓• Hipotireoidismo
primário
TSH ↓ ou nle T4l e T3l ↑ Anti-TPO Anti-Tg TRAB
• Tireoidite• Dç Graves*
Diagnóstico & Manejo
• Hipotireoidismo central
• Hipotireoidismo primário
Tireoidite não dolorosa
Tireotoxicose transitória
Hipotireoidismo
Oftalmopatia
Tempestade tireoidiana FadigaAsteniaConstipaçãoIntolerância frioXerodermiaGanho de peso
FADiarréia
Intolerância calorSudorese
Perda de peso
Mecanismo ?
Assintomático e TSH <10:- ObservarSintomático- Levotiroxina
Tireotoxicose- Beta-bloqueadorDoença Graves- Beta-bloqueador- Anti-tireoidianos
Imunoterapia deve ser mantida
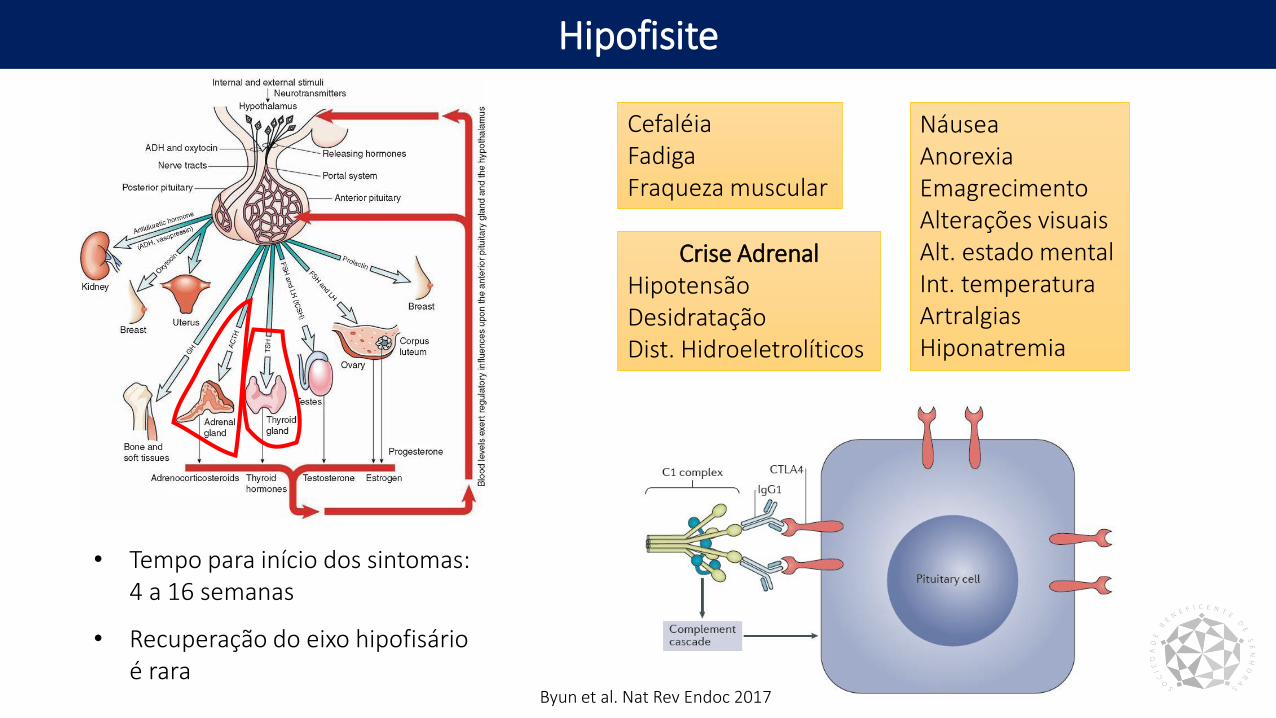
Hipofisite
• Tempo para início dos sintomas: 4 a 16 semanas
CefaléiaFadigaFraqueza muscular
NáuseaAnorexiaEmagrecimentoAlterações visuaisAlt. estado mentalInt. temperaturaArtralgiasHiponatremia
Crise AdrenalHipotensãoDesidrataçãoDist. Hidroeletrolíticos
• Recuperação do eixo hipofisário é rara
Byun et al. Nat Rev Endoc 2017
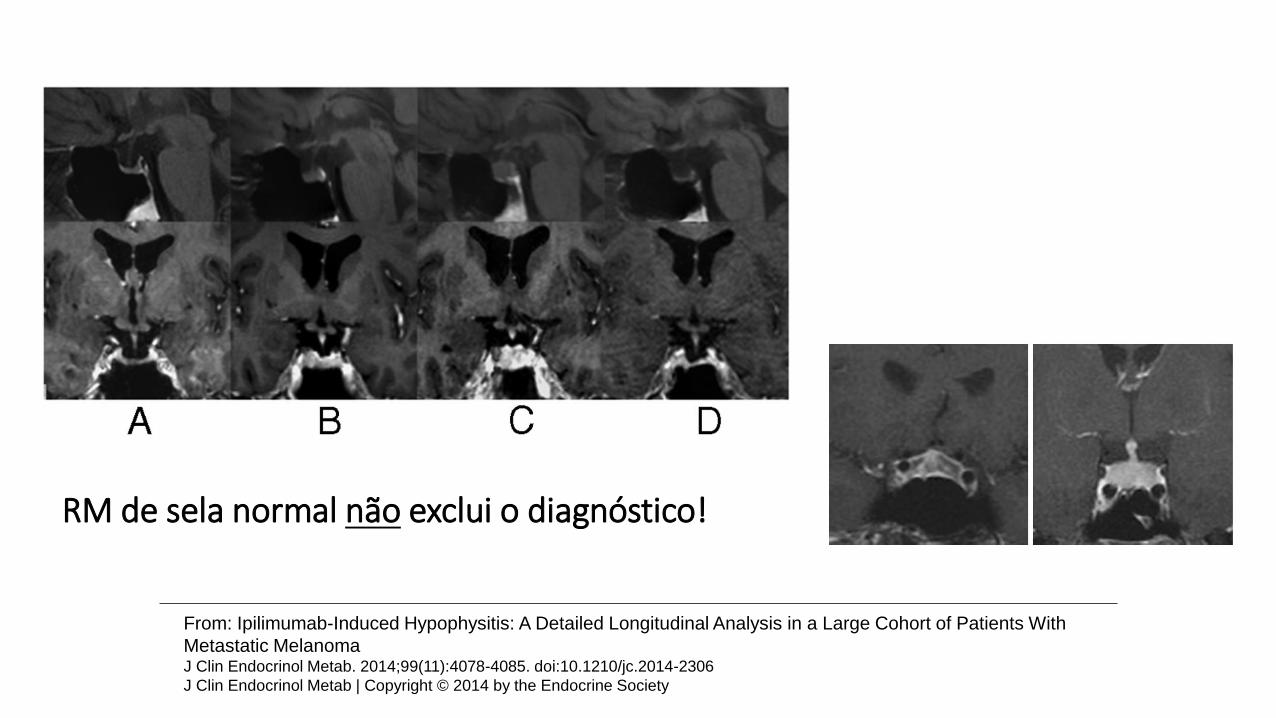
From: Ipilimumab-Induced Hypophysitis: A Detailed Longitudinal Analysis in a Large Cohort of Patients With
Metastatic MelanomaJ Clin Endocrinol Metab. 2014;99(11):4078-4085. doi:10.1210/jc.2014-2306
J Clin Endocrinol Metab | Copyright © 2014 by the Endocrine Society
RM de sela normal não exclui o diagnóstico!
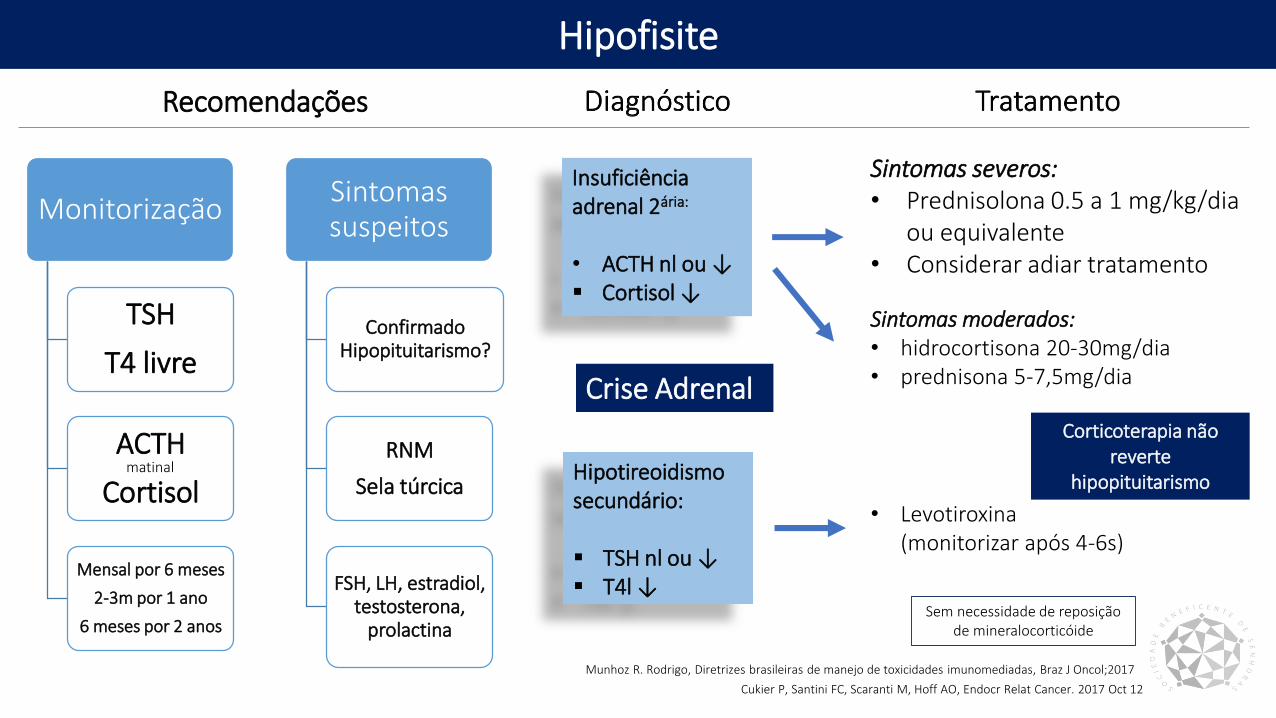
Hipofisite
Monitorização
TSH
T4 livre
ACTH
Cortisol
Mensal por 6 meses
2-3m por 1 ano
6 meses por 2 anos
Sintomas suspeitos
Confirmado Hipopituitarismo?
RNM
Sela túrcica
FSH, LH, estradiol, testosterona,
prolactina
Insuficiência adrenal 2ária:
• ACTH nl ou ↓ Cortisol ↓
Hipotireoidismo secundário:
TSH nl ou ↓ T4l ↓
Recomendações
Cukier P, Santini FC, Scaranti M, Hoff AO, Endocr Relat Cancer. 2017 Oct 12
Munhoz R. Rodrigo, Diretrizes brasileiras de manejo de toxicidades imunomediadas, Braz J Oncol;2017
matinal
Sintomas severos:• Prednisolona 0.5 a 1 mg/kg/dia
ou equivalente• Considerar adiar tratamento
Sintomas moderados:• hidrocortisona 20-30mg/dia • prednisona 5-7,5mg/dia
Sem necessidade de reposição de mineralocorticóide
• Levotiroxina (monitorizar após 4-6s)
Corticoterapia não reverte
hipopituitarismo
Crise Adrenal
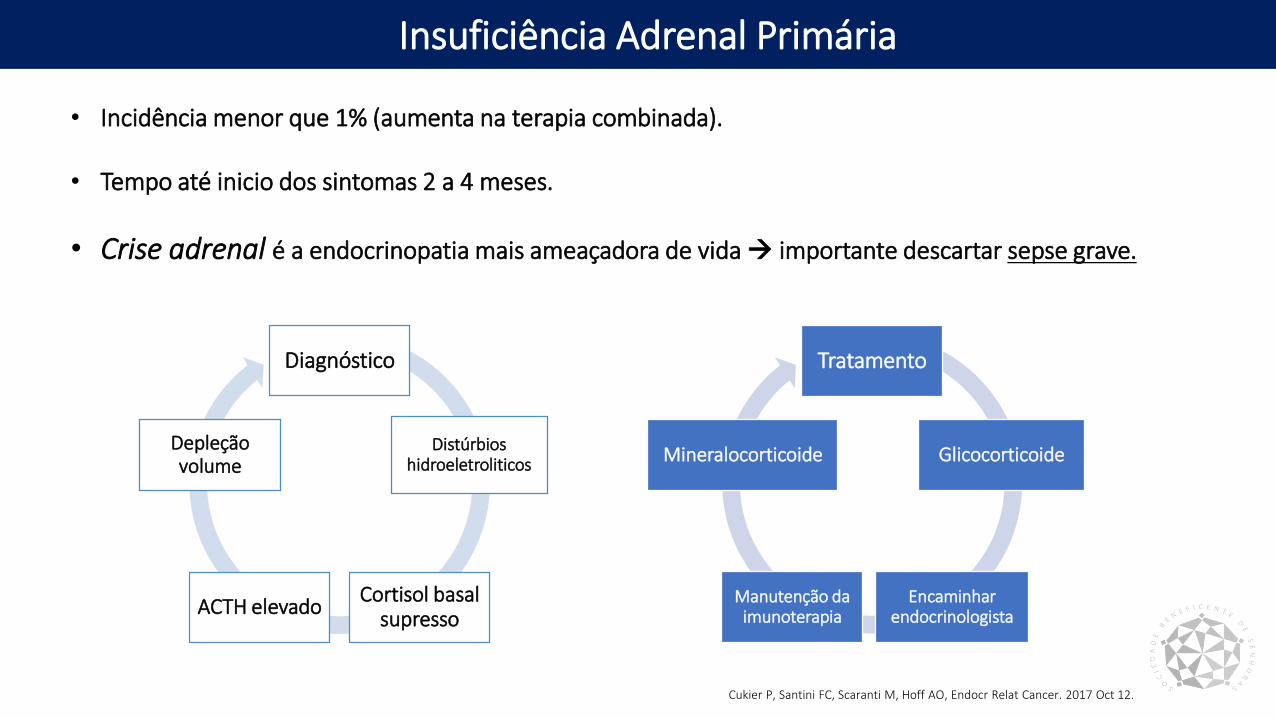
Insuficiência Adrenal Primária
• Incidência menor que 1% (aumenta na terapia combinada).
• Tempo até inicio dos sintomas 2 a 4 meses.
• Crise adrenal é a endocrinopatia mais ameaçadora de vida importante descartar sepse grave.
Diagnóstico
Distúrbios hidroeletroliticos
Cortisol basal supresso
ACTH elevado
Depleção volume
Tratamento
Glicocorticoide
Encaminhar endocrinologista
Manutenção da imunoterapia
Mineralocorticoide
Cukier P, Santini FC, Scaranti M, Hoff AO, Endocr Relat Cancer. 2017 Oct 12.
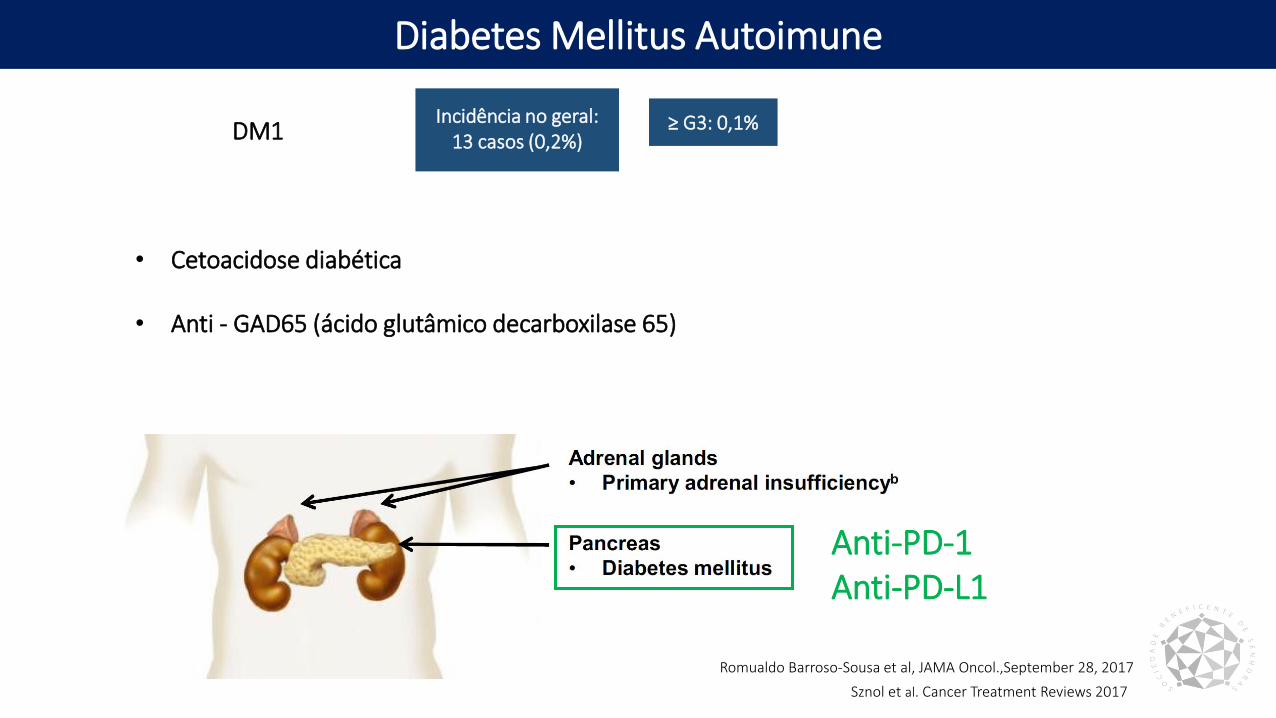
Diabetes Mellitus Autoimune
Sznol et al. Cancer Treatment Reviews 2017
Anti-PD-1Anti-PD-L1
• Cetoacidose diabética
• Anti - GAD65 (ácido glutâmico decarboxilase 65)
Incidência no geral:13 casos (0,2%)
≥ G3: 0,1%DM1
Romualdo Barroso-Sousa et al, JAMA Oncol.,September 28, 2017
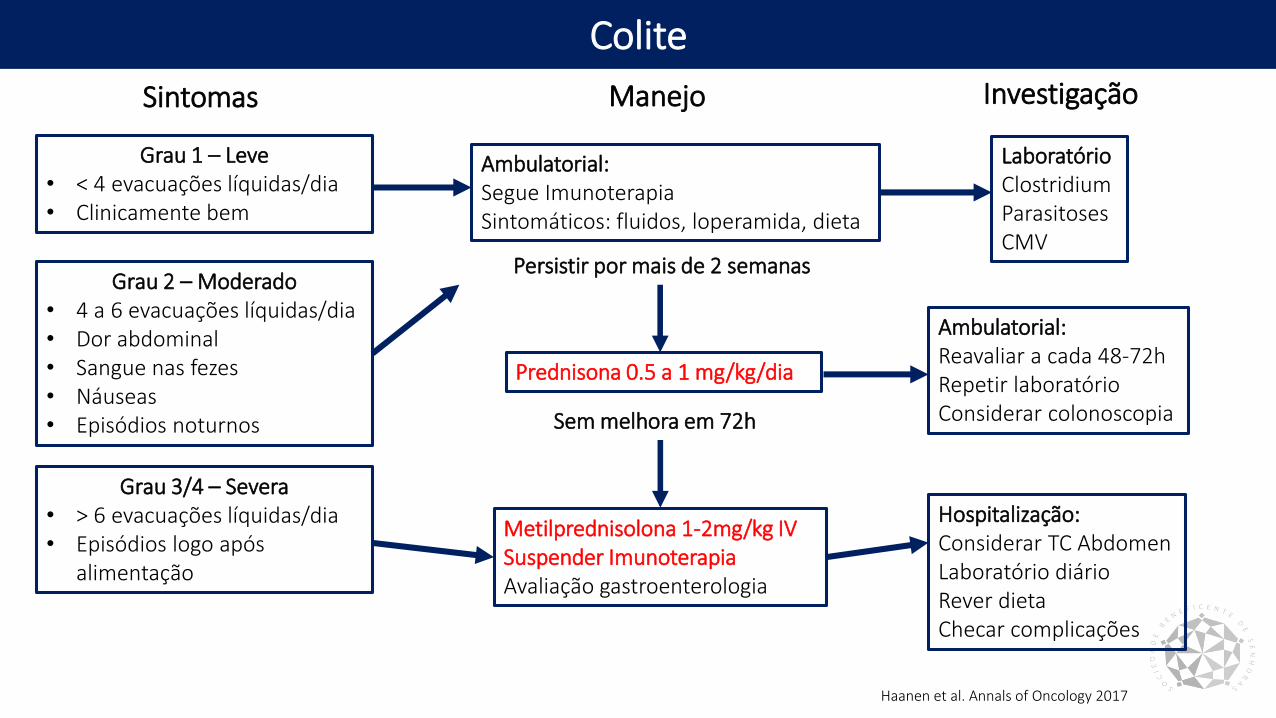
Colite
Grau 1 – Leve• < 4 evacuações líquidas/dia• Clinicamente bem
Ambulatorial:Segue ImunoterapiaSintomáticos: fluidos, loperamida, dieta
LaboratórioClostridiumParasitosesCMV
Grau 2 – Moderado• 4 a 6 evacuações líquidas/dia• Dor abdominal• Sangue nas fezes• Náuseas• Episódios noturnos
Prednisona 0.5 a 1 mg/kg/dia
Ambulatorial:Reavaliar a cada 48-72hRepetir laboratórioConsiderar colonoscopia
Grau 3/4 – Severa• > 6 evacuações líquidas/dia• Episódios logo após
alimentação
Metilprednisolona 1-2mg/kg IVSuspender ImunoterapiaAvaliação gastroenterologia
Hospitalização: Considerar TC AbdomenLaboratório diárioRever dietaChecar complicações
Sintomas Manejo Investigação
Persistir por mais de 2 semanas
Sem melhora em 72h
Haanen et al. Annals of Oncology 2017
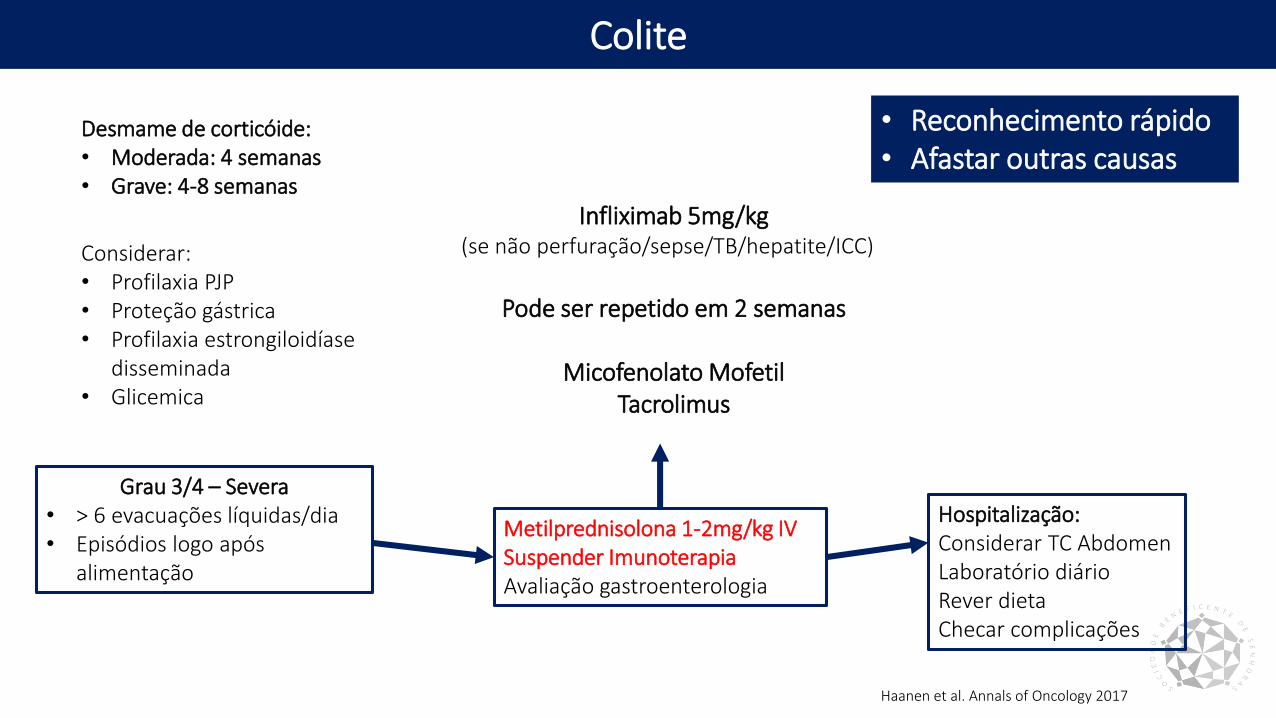
Colite
Grau 3/4 – Severa• > 6 evacuações líquidas/dia• Episódios logo após
alimentação
Metilprednisolona 1-2mg/kg IVSuspender ImunoterapiaAvaliação gastroenterologia
Hospitalização: Considerar TC AbdomenLaboratório diárioRever dietaChecar complicações
Desmame de corticóide:• Moderada: 4 semanas• Grave: 4-8 semanas
Considerar:• Profilaxia PJP• Proteção gástrica• Profilaxia estrongiloidíase
disseminada• Glicemica
Infliximab 5mg/kg(se não perfuração/sepse/TB/hepatite/ICC)
Pode ser repetido em 2 semanas
Micofenolato MofetilTacrolimus
Haanen et al. Annals of Oncology 2017
• Reconhecimento rápido• Afastar outras causas
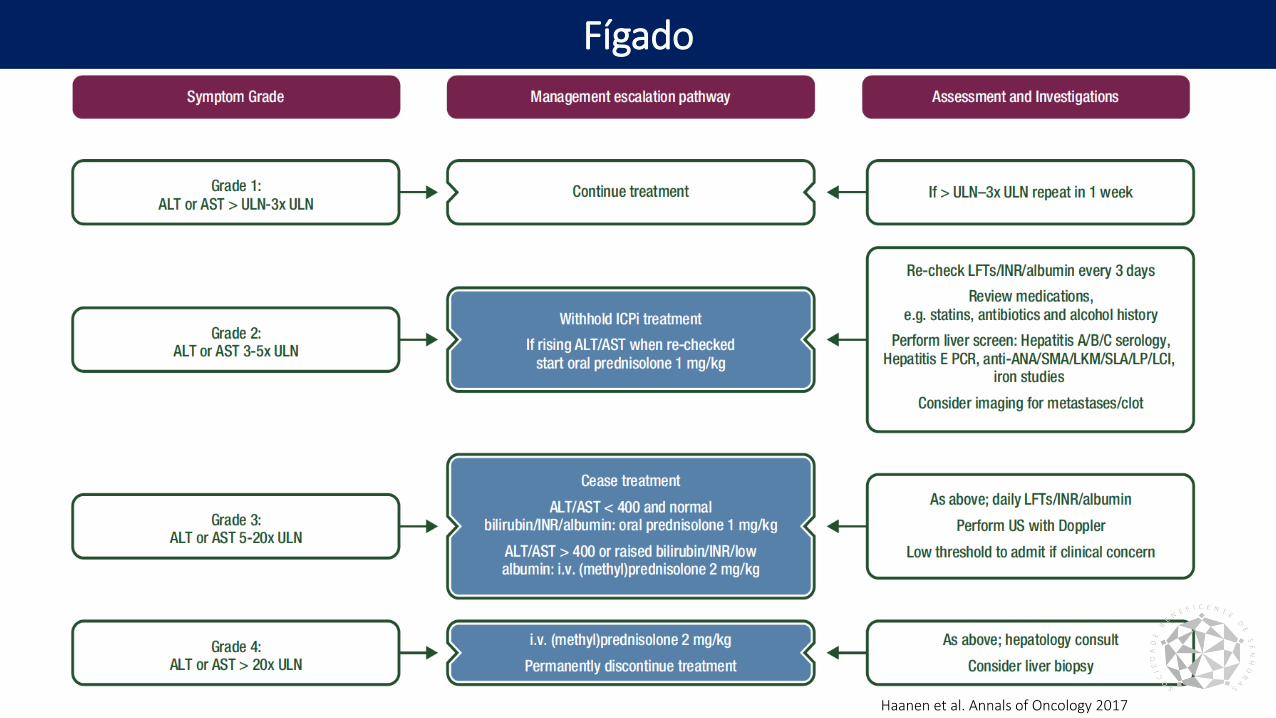
Fígado
Haanen et al. Annals of Oncology 2017
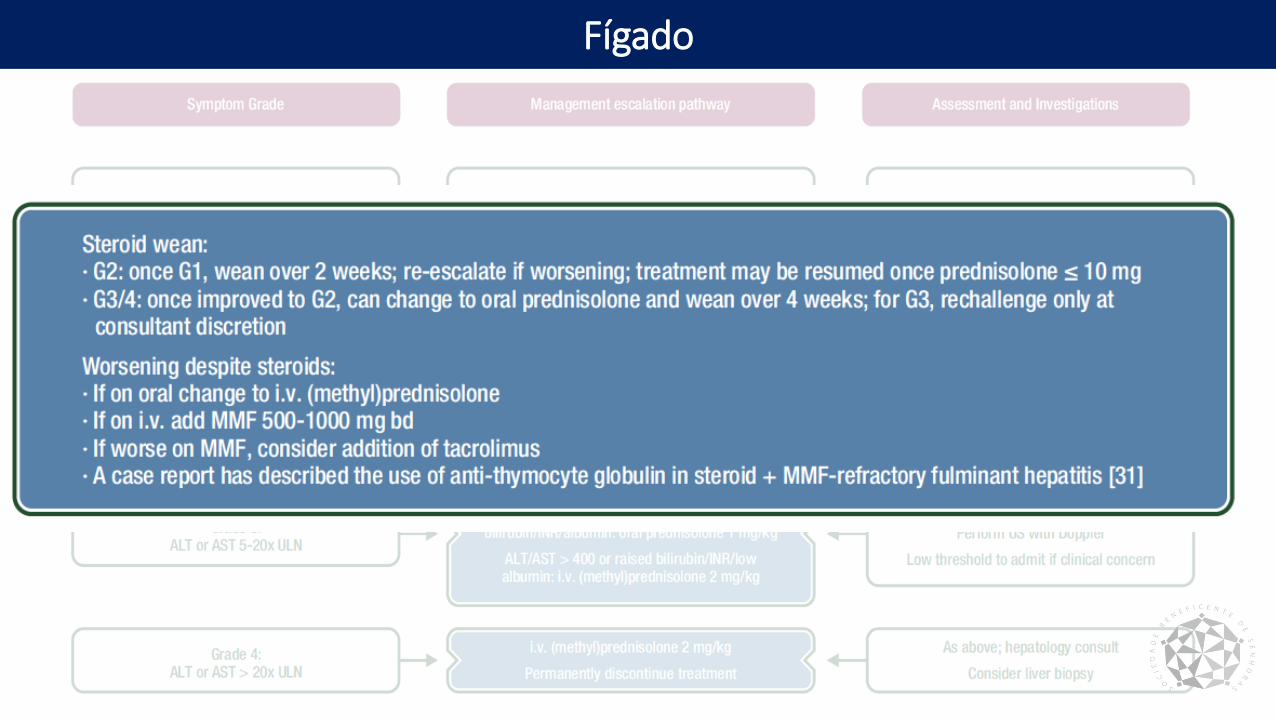
Fígado
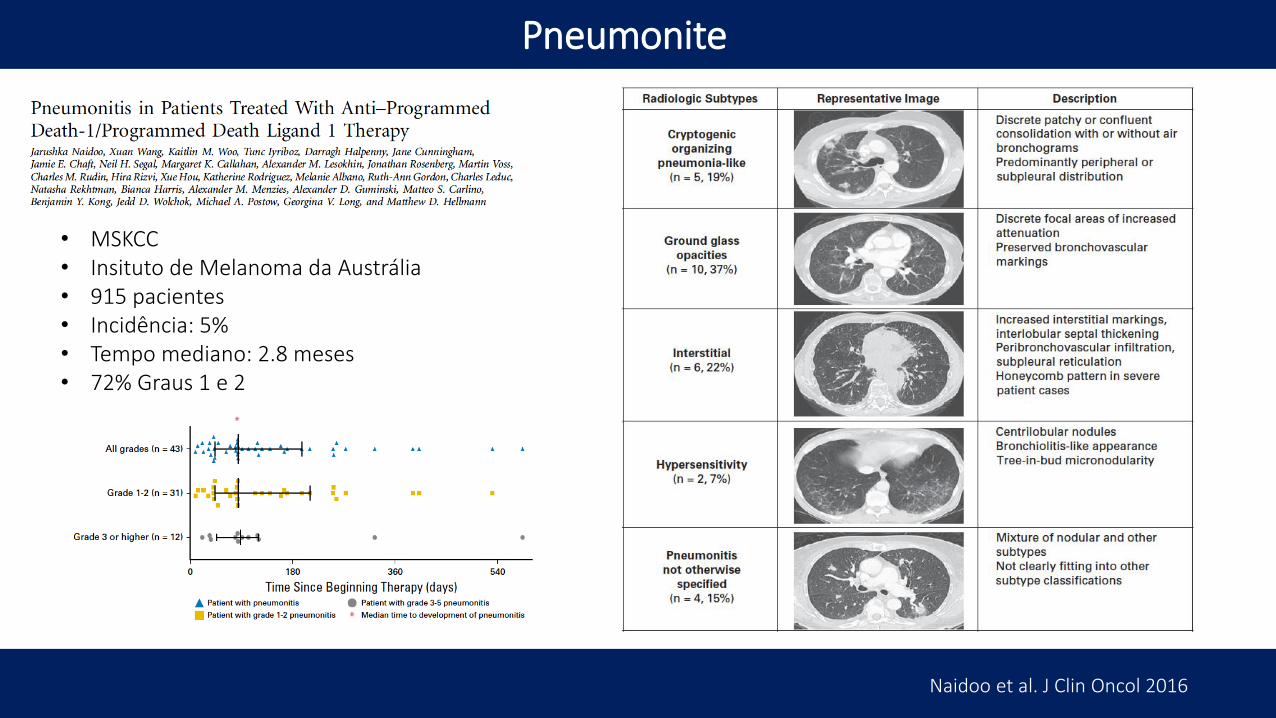
Pneumonite
Naidoo et al. J Clin Oncol 2016
• MSKCC• Insituto de Melanoma da Austrália• 915 pacientes• Incidência: 5%• Tempo mediano: 2.8 meses• 72% Graus 1 e 2
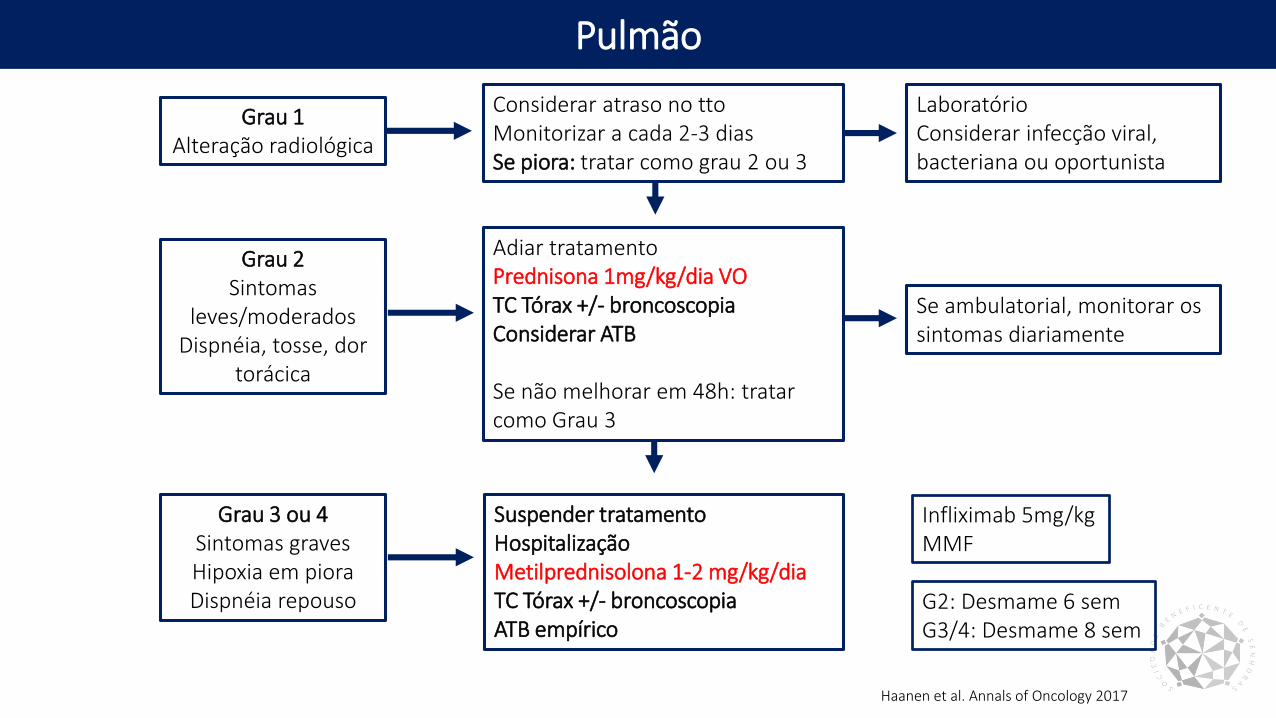
Pulmão
Grau 1Alteração radiológica
Considerar atraso no ttoMonitorizar a cada 2-3 diasSe piora: tratar como grau 2 ou 3
Laboratório Considerar infecção viral, bacteriana ou oportunista
Grau 2 Sintomas
leves/moderadosDispnéia, tosse, dor
torácica
Adiar tratamentoPrednisona 1mg/kg/dia VOTC Tórax +/- broncoscopiaConsiderar ATB
Se não melhorar em 48h: tratar como Grau 3
Se ambulatorial, monitorar os sintomas diariamente
Grau 3 ou 4Sintomas gravesHipoxia em pioraDispnéia repouso
Suspender tratamentoHospitalizaçãoMetilprednisolona 1-2 mg/kg/diaTC Tórax +/- broncoscopiaATB empírico
Infliximab 5mg/kgMMF
G2: Desmame 6 semG3/4: Desmame 8 sem
Haanen et al. Annals of Oncology 2017
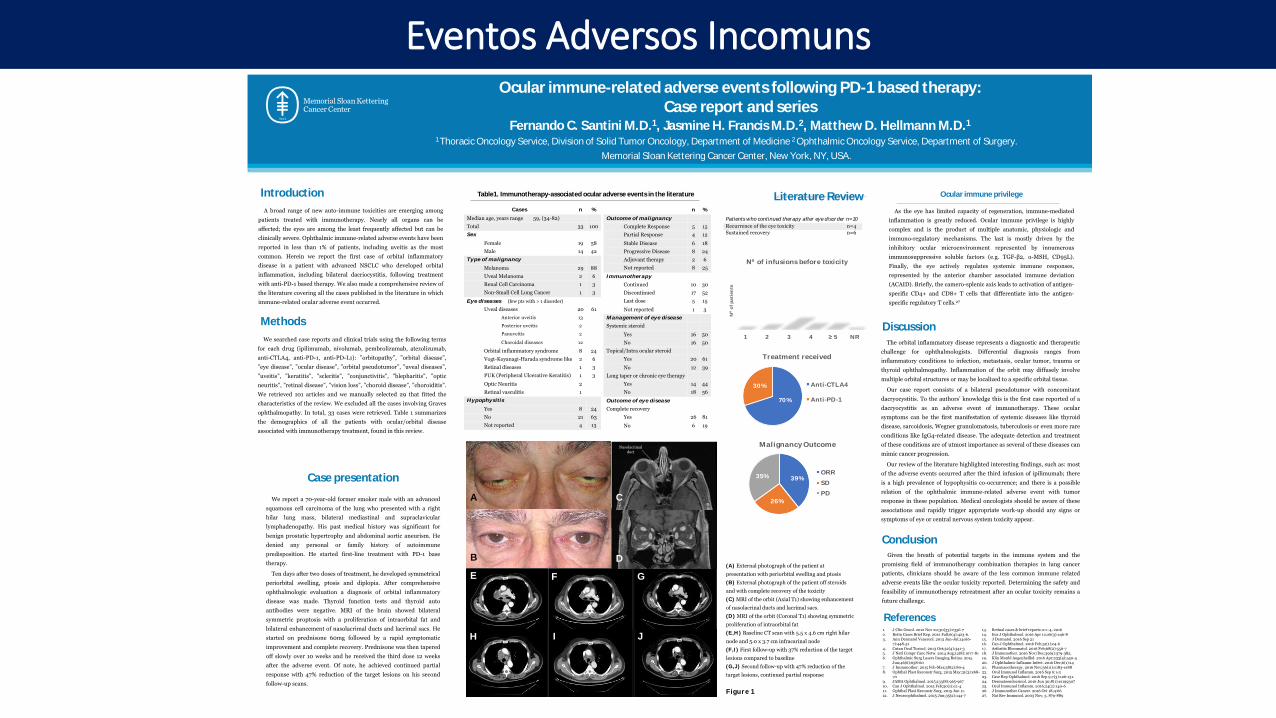
Ocular immune-related adverse events following PD-1 based therapy:
Case report and seriesFernando C. Santini M.D.1, Jasmine H. Francis M.D.2, Matthew D. Hellmann M.D.1
1 Thoracic Oncology Service, Division of Solid Tumor Oncology, Department of Medicine 2 Ophthalmic Oncology Service, Department of Surgery.
Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Introduction
Case presentation
We report a 70-year-old former smoker male with an advanced
squamous cell carcinoma of the lung who presented with a right
hilar lung mass, bilateral mediastinal and supraclavicular
lymphadenopathy. His past medical history was significant for
benign prostatic hypertrophy and abdominal aortic aneurism. He
denied any personal or family history of autoimmune
predisposition. He started first-line treatment with PD-1 base
therapy.
Ten days after two doses of treatment, he developed symmetrical
periorbital swelling, ptosis and diplopia. After comprehensive
ophthalmologic evaluation a diagnosis of orbital inflammatory
disease was made. Thyroid function tests and thyroid auto
antibodies were negative. MRI of the brain showed bilateral
symmetric proptosis with a proliferation of intraorbital fat and
bilateral enhancement of nasolacrimal ducts and lacrimal sacs. He
started on prednisone 60mg followed by a rapid symptomatic
improvement and complete recovery. Prednisone was then tapered
off slowly over 10 weeks and he received the third dose 12 weeks
after the adverse event. Of note, he achieved continued partial
response with 47% reduction of the target lesions on his second
follow-up scans.
The orbital inflammatory disease represents a diagnostic and therapeutic
challenge for ophthalmologists. Differential diagnosis ranges from
inflammatory conditions to infection, metastasis, ocular tumor, trauma or
thyroid ophthalmopathy. Inflammation of the orbit may diffusely involve
multiple orbital structures or may be localized to a specific orbital tissue.
Our case report consists of a bilateral pseudotumor with concomitant
dacryocystitis. To the authors’ knowledge this is the first case reported of a
dacryocystitis as an adverse event of immunotherapy. These ocular
symptoms can be the first manifestation of systemic diseases like thyroid
disease, sarcoidosis, Wegner granulomatosis, tuberculosis or even more rare
conditions like IgG4-related disease. The adequate detection and treatment
of these conditions are of utmost importance as several of these diseases can
mimic cancer progression.
Our review of the literature highlighted interesting findings, such as: most
of the adverse events occurred after the third infusion of ipilimumab; there
is a high prevalence of hypophysitis co-occurrence; and there is a possible
relation of the ophthalmic immune-related adverse event with tumor
response in these population. Medical oncologists should be aware of these
associations and rapidly trigger appropriate work-up should any signs or
symptoms of eye or central nervous system toxicity appear.
ConclusionGiven the breath of potential targets in the immune system and the
promising field of immunotherapy combination therapies in lung cancer
patients, clinicians should be aware of the less common immune related
adverse events like the ocular toxicity reported. Determining the safety and
feasibility of immunotherapy retreatment after an ocular toxicity remains a
future challenge.
References1. J Clin Oncol. 2012 Nov 20;30(33):e356-72. Retin Cases Brief Rep. 2012 Fall;6(4):423-6.3. Ann Dermatol Venereol. 2013 Jun-Jul;140(6-
7):448-514. Cutan Ocul Toxicol. 2013 Oct;32(4):341-35. J Natl Compr Canc Netw. 2014 Aug;12(8):1077-816. Ophthalmic Surg Lasers Imaging Retina. 2015
Jun;46(6):658-607. J Immunother. 2015 Feb-Mar;38(2):80-48. Ophthal Plast Reconstr Surg. 2015 May;31(3):e68-
709. JAMA Ophthalmol. 2015;133(8):965-96710. Can J Ophthalmol. 2015 Feb;50(1):e2-411. Ophthal Plast Reconstr Surg. 2015 Jun 11.12. J Neuroophthalmol. 2015 Jun;35(2):144-7
13. Retinal cases & brief reports 0:1–4, 201614. Eur J Ophthalmol. 2016 Apr 12;26(3):e46-815. J Dermatol. 2016 Sep 2116. Can J Ophthalmol. 2016 Feb;51(1):e4-617. Arthritis Rheumatol. 2016 Feb;68(2):556-718. J Immunother. 2016 Nov/Dec;39(9):379-382.19. Klin Monbl Augenheilkd. 2016 Apr;233(4):540-420. J Ophthalmic Inflamm Infect. 2016 Dec;6(1):1421. Pharmacotherapy. 2016 Nov;36(11):e183-e18822. Ocul Immunol Inflamm. 2016 Sep 6:1-323. Case Rep Ophthalmol. 2016 Sep 9;7(3):126-131.24. Dermatoendocrinol. 2016 Jun 30;8(1):e119930725. Ocul Immunol Inflamm. 2016;24(2):140-626. J Immunother Cancer. 2016 Oct 18;4:6627. Nat Rev Immunol. 2003 Nov; 3, 879-889
Methods
We searched case reports and clinical trials using the following terms
for each drug (ipilimumab, nivolumab, pembrolizumab, atezolizumab,
anti-CTLA4, anti-PD-1, anti-PD-L1): ”orbitopathy”, ”orbital disease”,
”eye disease”, ”ocular disease”, ”orbital pseudotumor”, ”uveal diseases”,
”uveitis”, ”keratitis”, ”scleritis”, ”conjunctivitis”, ”blepharitis”, ”optic
neuritis”, ”retinal disease”, ”vision loss”, ”choroid disease”, ”choroiditis”.
We retrieved 101 articles and we manually selected 29 that fitted the
characteristics of the review. We excluded all the cases involving Graves
ophthalmopathy. In total, 33 cases were retrieved. Table 1 summarizes
the demographics of all the patients with ocular/orbital disease
associated with immunotherapy treatment, found in this review.
Discussion
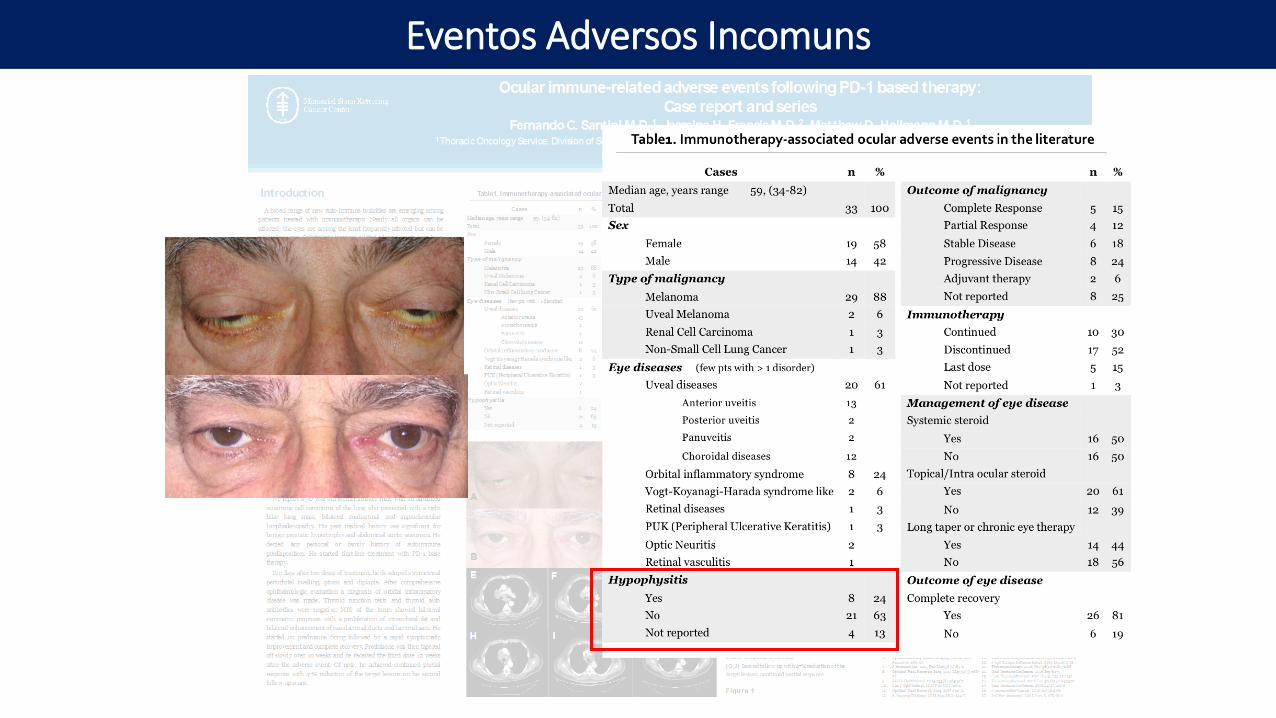
Table1. Immunotherapy-associated ocular adverse events in the literature Ocular immune privilege
As the eye has limited capacity of regeneration, immune-mediated
inflammation is greatly reduced. Ocular immune privilege is highly
complex and is the product of multiple anatomic, physiologic and
immuno-regulatory mechanisms. The last is mostly driven by the
inhibitory ocular microenvironment represented by innumerous
immunosuppressive soluble factors (e.g. TGF-β2, ⍺-MSH, CD95L).
Finally, the eye actively regulates systemic immune responses,
represented by the anterior chamber associated immune deviation
(ACAID). Briefly, the camero-splenic axis leads to activation of antigen-
specific CD4+ and CD8+ T cells that differentiate into the antigen-
specific regulatory T cells.27
39%
26%
35%
Malignancy Outcome
ORR
SD
PD
3
5
11
6 6
2
1 2 3 4 ≥ 5 NR
Nº o
f p
ati
en
ts
Nº of infusions before toxicity
Cases n %
Median age, years range 59, (34-82)
Total 33 100
Sex
Female 19 58
Male 14 42
Type of malignancy
Melanoma 29 88
Uveal Melanoma 2 6
Renal Cell Carcinoma 1 3
Non-Small Cell Lung Cancer 1 3
Eye diseases (few pts with > 1 disorder)
Uveal diseases 20 61
Anterior uveitis 13
Posterior uveitis 2
Panuveitis 2
Choroidal diseases 12
Orbital inflammatory syndrome 8 24
Vogt-Koyanagi-Harada syndrome like 2 6
Retinal diseases 1 3
PUK (Peripheral Ulcerative Keratitis) 1 3
Optic Neuritis 2
Retinal vasculitis 1
Hypophysitis
Yes 8 24
No 21 63
Not reported 4 13
Nasolacrimalduct
A
B
C
D
E F G
H I J
(A) External photograph of the patient at
presentation with periorbital swelling and ptosis
(B) External photograph of the patient off steroids
and with complete recovery of the toxicity
(C) MRI of the orbit (Axial T1) showing enhancement
of nasolacrinal ducts and lacrimal sacs.
(D) MRI of the orbit (Coronal T1) showing symmetric
proliferation of intraorbital fat
(E,H ) Baseline CT scan with 5.5 x 4.6 cm right hilar
node and 5.0 x 3.7 cm infracarinal node
(F,I ) First follow-up with 37% reduction of the target
lesions compared to baseline
(G,J) Second follow-up with 47% reduction of the
target lesions, continued partial response
Figure 1
n %
Outcome of malignancy
Complete Response 5 15
Partial Response 4 12
Stable Disease 6 18
Progressive Disease 8 24
Adjuvant therapy 2 6
Not reported 8 25
Immunotherapy
Continued 10 30
Discontinued 17 52
Last dose 5 15
Not reported 1 3
Management of eye disease
Systemic steroid
Yes 16 50
No 16 50
Topical/Intra ocular steroid
Yes 20 61
No 12 39
Long taper or chronic eye therapy
Yes 14 44
No 18 56
Outcome of eye disease
Complete recovery
Yes 26 81
No 6 19
Literature ReviewA broad range of new auto-immune toxicities are emerging among
patients treated with immunotherapy. Nearly all organs can be
affected; the eyes are among the least frequently affected but can be
clinically severe. Ophthalmic immune-related adverse events have been
reported in less than 1% of patients, including uveitis as the most
common. Herein we report the first case of orbital inflammatory
disease in a patient with advanced NSCLC who developed orbital
inflammation, including bilateral dacriocystitis, following treatment
with anti-PD-1 based therapy. We also made a comprehensive review of
the literature covering all the cases published in the literature in which
immune-related ocular adverse event occurred.
Patients who continued therapy after eye disorder n=10
Recurrence of the eye toxicity n=4
Sustained recovery n=6
70%
30%
Treatment received
Anti-CTLA4
Anti-PD-1
Eventos Adversos Incomuns
Eventos Adversos Incomuns
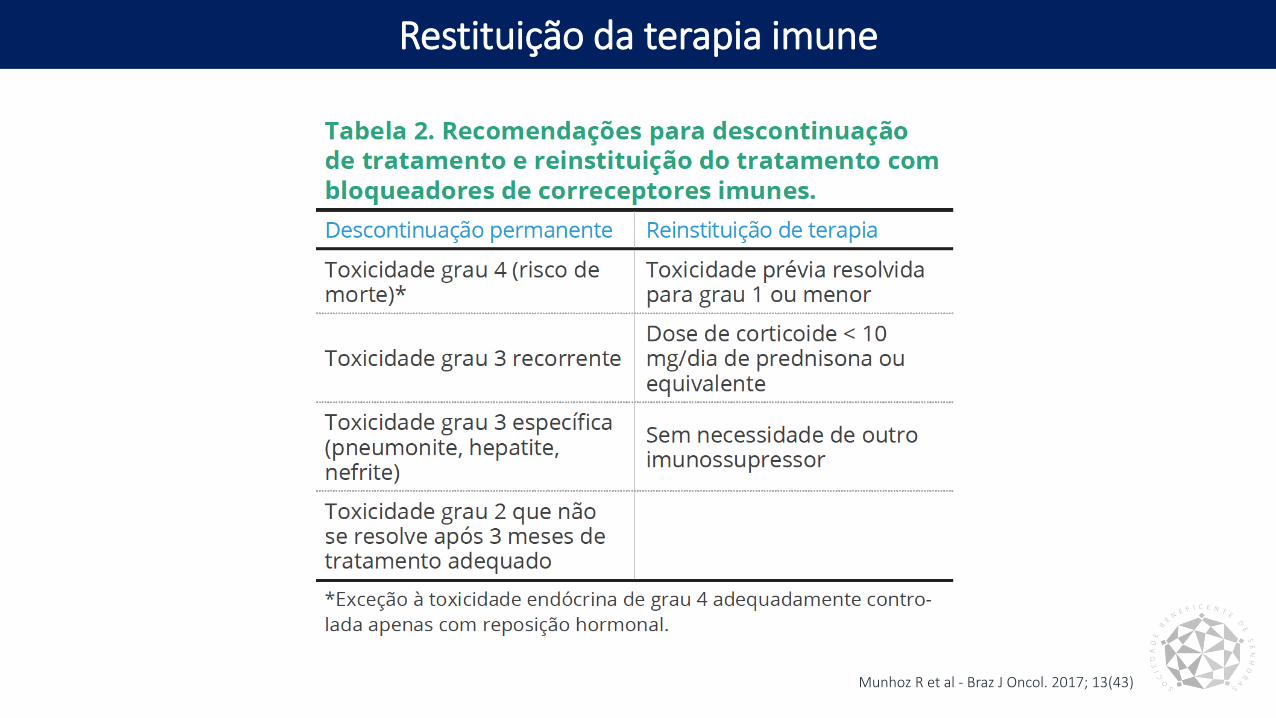
Restituição da terapia imune
Munhoz R et al - Braz J Oncol. 2017; 13(43)

Safety of retreatment with immunotherapy after immune-
related toxicity in patients with lung cancers treated with anti-
PD-(L)1 therapy
Fernando C. Santini, Hira Rizvi, Olivia Wilkins, Martine van Voorthuysen, Elizabeth Panora, Darragh
Halpenny, Mark G. Kris, Charles M. Rudin, Jamie E. Chaft, Matthew D. Hellmann;
Memorial Sloan Kettering Cancer Center, New York, NY
Abstract #9012
Lung Cancer—Non-Small Cell Metastatic
Em revisão pela Cancer Immunology Research
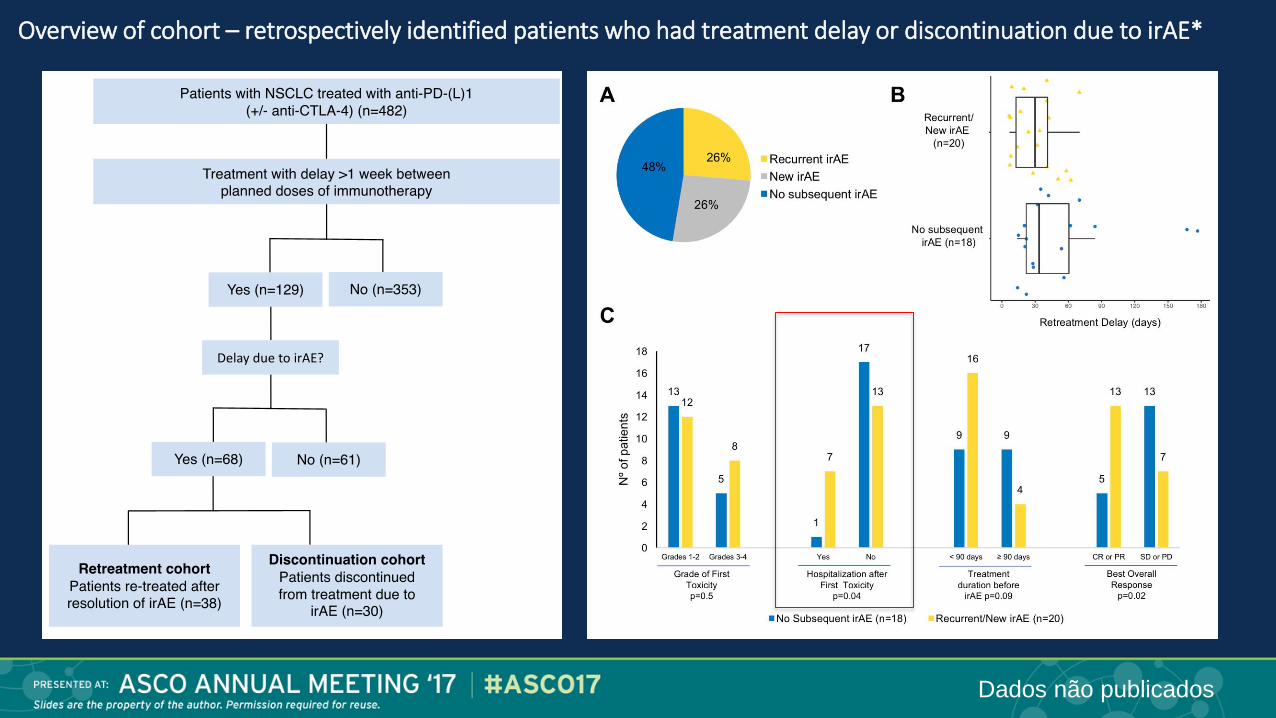
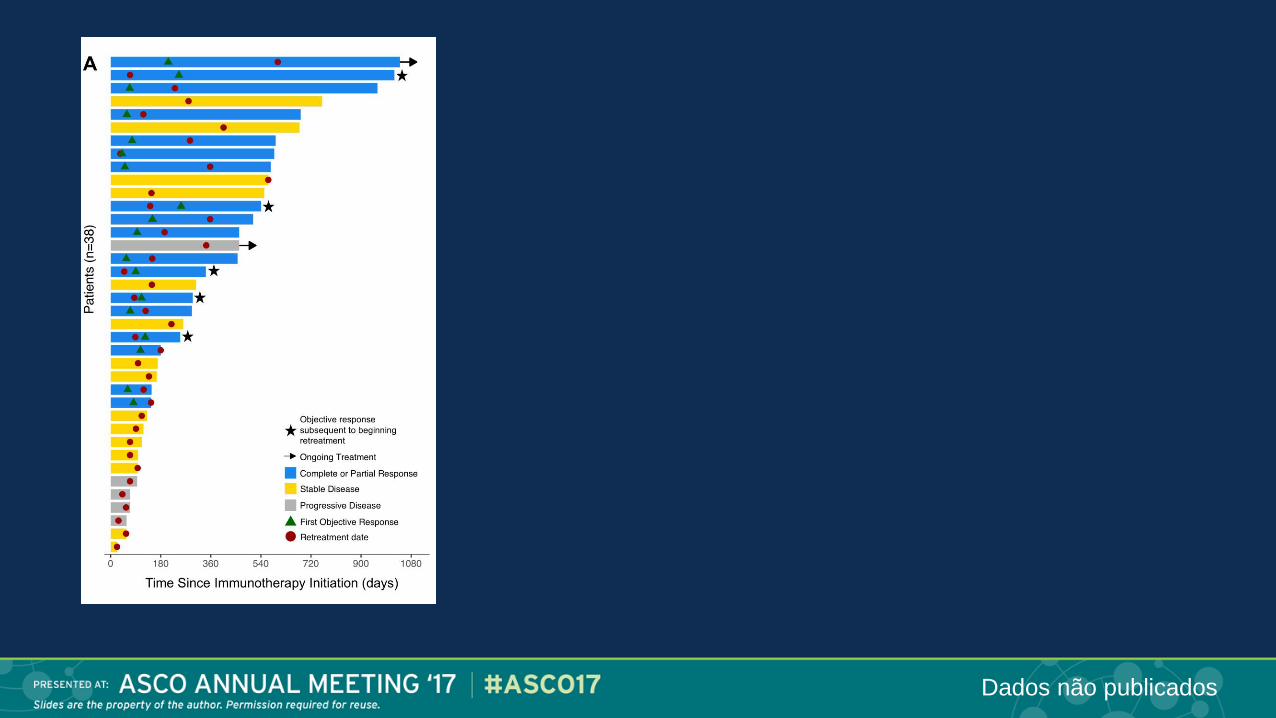
Overview of cohort – retrospectively identified patients who had treatment delay or discontinuation due to irAE*
Dados não publicados
Dados não publicados
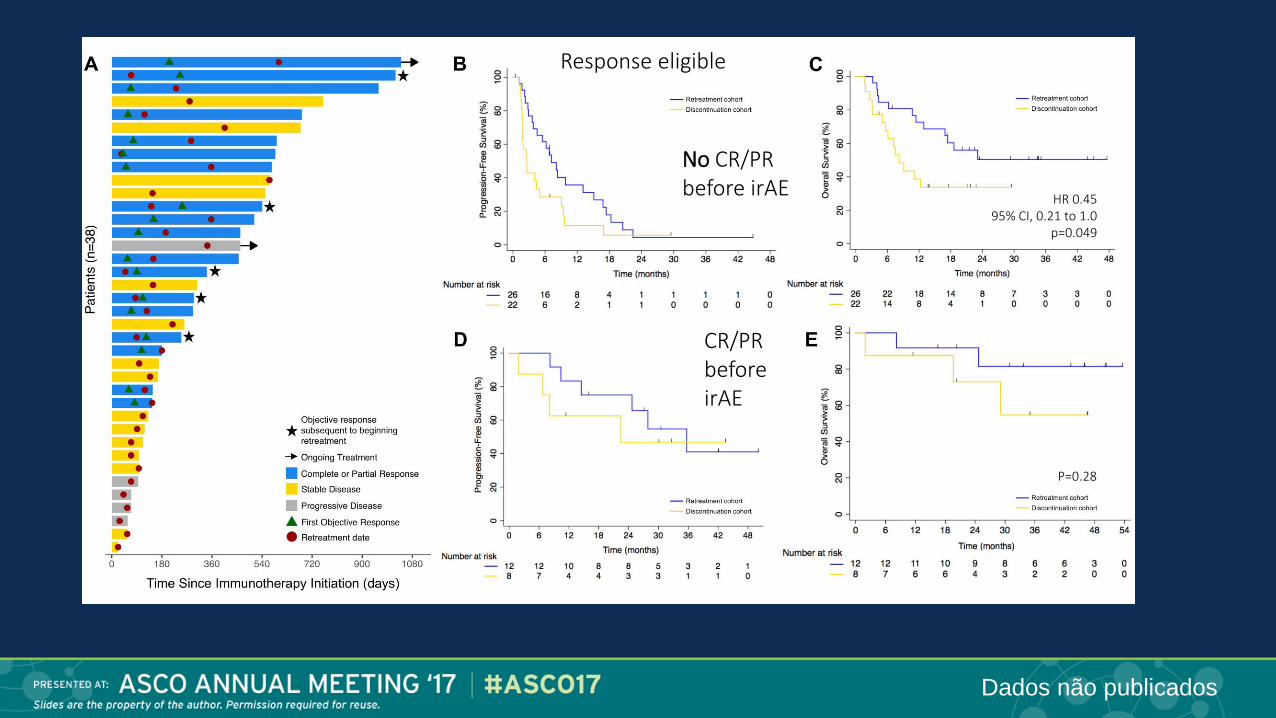
CR/PR before irAE
No CR/PR before irAE
Response eligible
HR 0.4595% CI, 0.21 to 1.0
p=0.049
P=0.28
Dados não publicados
Conclusões:
• Nos pacientes após EAIR, retratamento com terapia anti-PD-(L)1 resultou
em novos/recorrentes EAIR em metare dos pacientes
• Entre os pacientes retratados, necessidade de hospitalização está
associado com maior risco de recorrência ou nova toxicidade
• Maioria das toxicidades foi resolvida, porém dois óbitos ocorreram
• Algumas respostas ocorreram após o retratamento
• No grupo de pacientes que atingiram RC/RP antes da detecção do evento
adverso imuno relacionado, SLP e SG são iguais quando retratado ou
discontinuados
Santini et al, 2017
Safety of retreatment with immunotherapy after immune-related toxicity in patients with lung cancers treated with anti-PD-(L)1 therapy
Dados não publicados
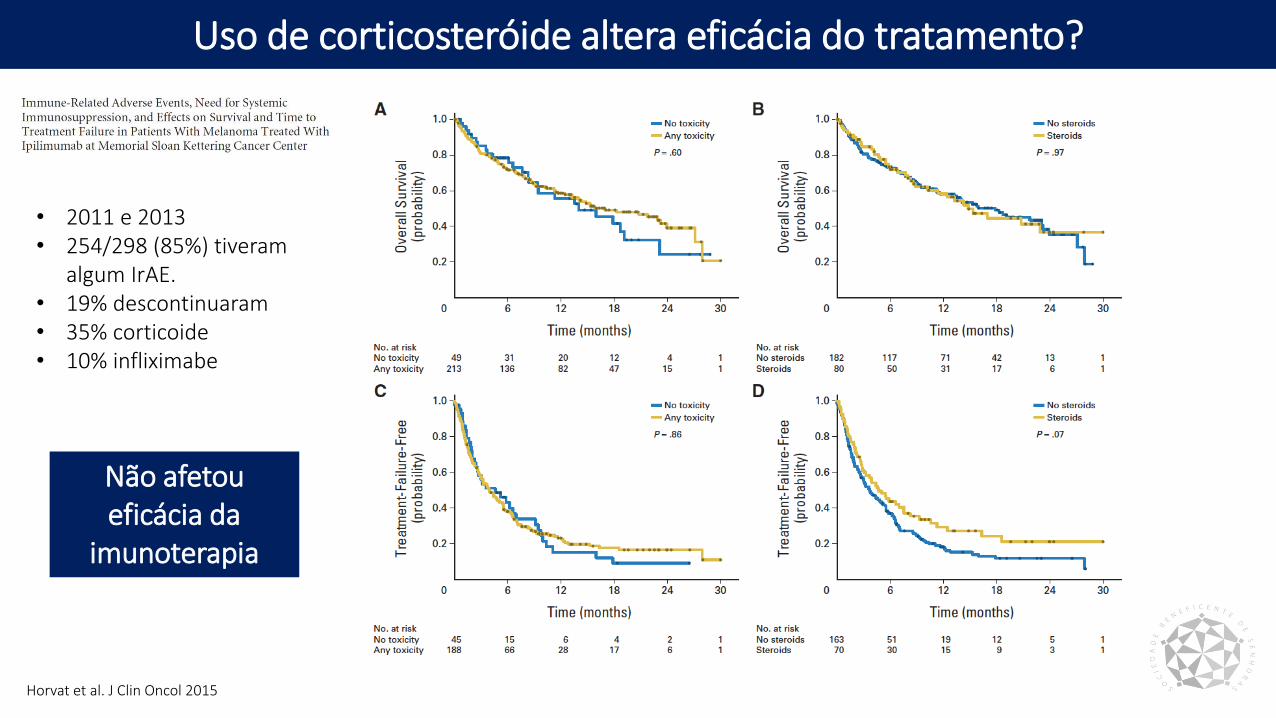
Uso de corticosteróide altera eficácia do tratamento?
Horvat et al. J Clin Oncol 2015
• 2011 e 2013• 254/298 (85%) tiveram
algum IrAE. • 19% descontinuaram • 35% corticoide• 10% infliximabe
Não afetou eficácia da
imunoterapia
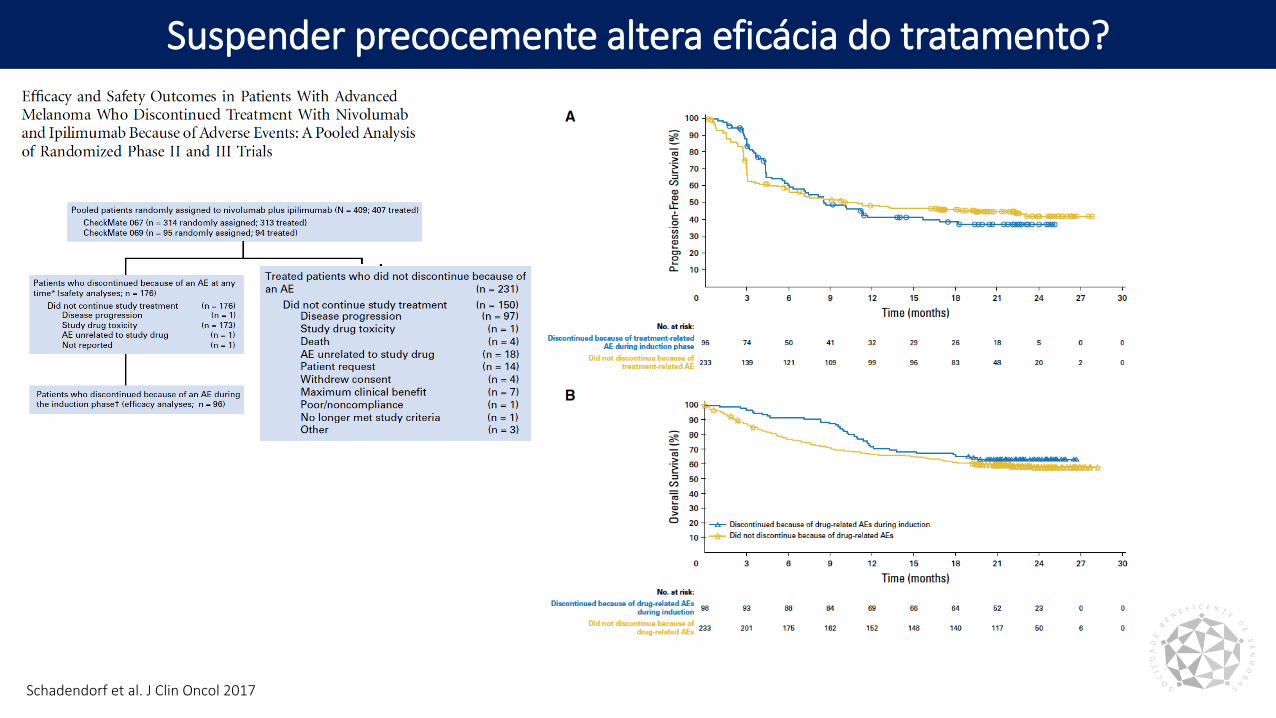
Suspender precocemente altera eficácia do tratamento?
Schadendorf et al. J Clin Oncol 2017
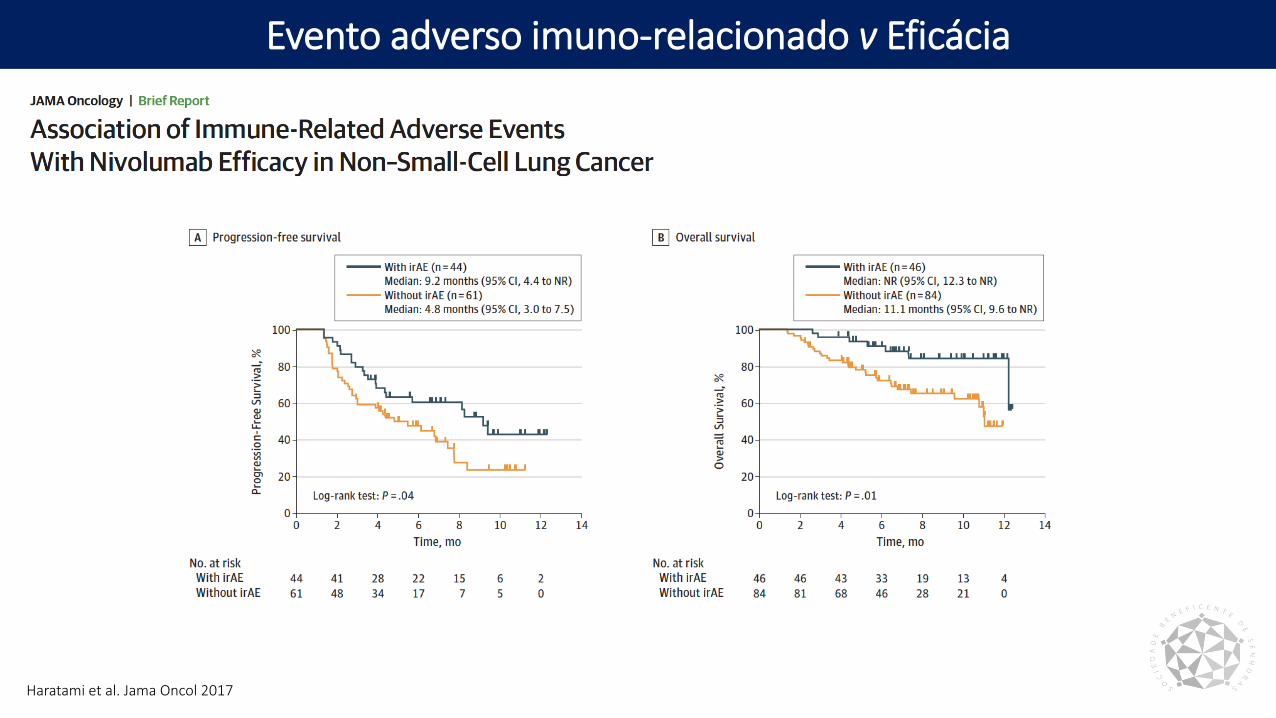
Evento adverso imuno-relacionado v Eficácia
Haratami et al. Jama Oncol 2017
Take home messages
• Monitorização e orientação do paciente
• Uso do corticosteróide quando indicado
• Desmame lento e cuidadoso!
• Suspender/adiar tratamento se > grau 2
• Retratamento?
• Consultar guias de manejo
