fígado gordo e síndrome metabólicoworkshops-endoscopia.pt/.../figado-gordo-e-sindrome... · •...
TRANSCRIPT

PedroMarquesdaCosta,MarianaVerdelhoMachado 2017
Fígadogordoesíndromemetabólico
Casoclínico- 1
ID: sexo feminino, raça caucasiana, 72 anos.
Motivo:Dor abdominal
HDA: Queixas crónicas, com agravamento das queixas nos últimos 3 meses, com dor abdominalsobretudo no quadrante inferior direito, tipo moinha, constante, associado a distensão abdominalnocturna e flatulência. Sem alterações do transito intestinal, queixas GI ou perda ponderal.
Antecedentes Pessoais- Angina instável, efectuou coronariografia com colocação de stent há 3 meses- Histerectomia com ooforectomia bilateral (aos 44 anos)- Oclusão intestinal por bridas- Hipertensão arterial, controlada- Arritmia cardíaca (FA paroxística?)
Hábitos:Æ hábitos alcoólicos, tabágicos ou toxifílicos.Medicação : carvedilol, aspirina, clopidogrel, candesartan
Antecedentes Familiares:- pais faleceram de patologia cardíaca (pai aos 50 e mãe aos 60 anos)- 2 irmãos faleceram com 50 anos, com patologia cardiovascular

Casoclínico- 1
ExameObjectivo:• Altura 167 cm• Peso 85 kg• IMC 30.1 kg/m2• Abdómen: cicatriz linear, sem sinais
inflamatórios, dor à palpação da FI direita;hérnia inguinal direita?
Exames:• EDA (2009) - esofagite grau A de Los Angeles
• Colonoscopia (2011) - micropólipo séssil de 3mm no cólon transverso, diverticulose docólon.
• Ecografia abdominal (2016): fígado decontornos regulares, hepatomegália, comesteatose; sem litíase vesícula ou outraslesões.
Análise ValorHb 11,5 g/dL
VGM 95,4 fL
Plaq 154000 109/L
INR 1,02
Glucose 86 mg/dL
HbA1C 5,6 %
Insulina 6,3 uU/mL
Col. Total 170 mg/dL
LDL/HDL 103/53 mg/dL
TAG 71 mg/dL
AST/ALT 17/11 U/L
FA 76 U/L
BT 0,69 mg/dL

FígadoGordoNãoAlcoólico(FGNA)

DoençaHepáticaNãoAlcoólica- definição
Acumulaçãoexcessivadetecidoadiposohepático,estáassociadaa
insulinorresistência(IR)eédefinidapelapresençadeesteatose
em>5%doshepatócitos.
FígadoGordonãoalcoólico(FGNA)
Esteatohepatitenãoalcoólica
(EHNA)
Exclusãodascausassecundáriasedeumconsumodiáriodeálcool>30gparaosexo
masculinoe>20gparaosexofeminino.
e…
EASLGuidelines.JHepatol.2016PMID: 27062661

FígadoGordoNãoAlcoólico
• FígadogordoéapatologiahepáticamaisfrequentenoOcidente.• Prevalênciaglobal:6-35%(mediana20%)• PrevalênciaEuropa:25-26%.
Younossi Z,Gastroenterology. 2016- PMID26980624

Fiuza Met al.Rev PorCardiol 2008;PMID:19280993
30,33%27,06%
SíndromeMetabólico- epidemiologia

SíndromeMetabólico- fisiopatologia
Eckel RH.Lancet 2005;PMID: 15836891

Fígadogordo- fisiopatologia
MachadoMVGastroenterology.2016;PMID: 26928243

Esteatohepatitenãoalcoólica- fisiopatologia
MachadoMVGastroenterology.2016;PMID: 26928243

DoençaHepáticaNãoAlcoólica– histórianatural
!! !!
Death/OLT/*complica1ons*
Slow*Progressors*
Rapid*Progressors*
?7yrs! !?5(6yrs!
Simple*steatosis*Steatosis*+*Lobular*Inflamma1on*
NASH*+/C*Portal*Inflamma1on*
Advanced*fibrosis*(Cirrhosis)*
Early*fibrosis*
!! !!
Característica (% população)
FGNA 25-35%
EHNA 5-10,5%
Cirrose 1,25-3,75%
20-30%
20-30%

DoençaHepáticaNãoAlcoólica
COMOAVALIARODOENTE?MÉTODOSNÃOINVASIVOS
Osmarcadoresnãoinvasivosdeverão:i) noscuidadosdesaúdeprimários, identificaroriscodeDHNAentre
osindivíduos comriscometabólicoaumentado;ii) noscuidadosdesaúdesecundárioseterciários,identificaros
indivíduos compiorprognóstico (p.ex.:EHNAgrave);iii) avaliaraprogressãodadoença;iv) preverarespostaaintervençõesterapêuticas.
EASLGuidelines.JHepatol.2016PMID: 27062661

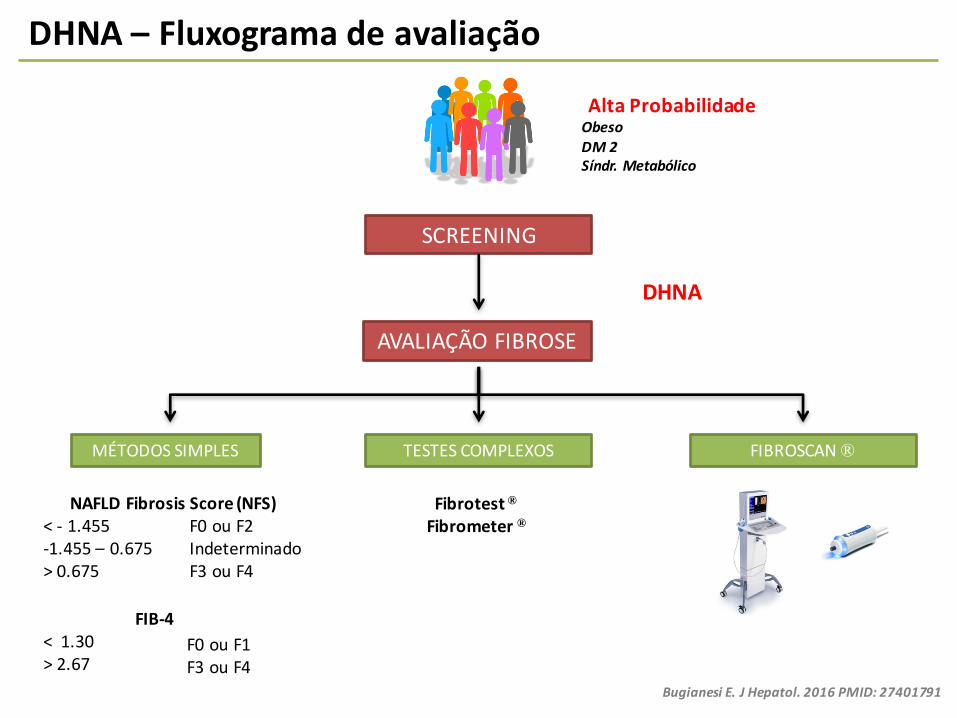
DHNA– Fluxogramadeavaliação
AltaProbabilidadeObesoDM2Síndr.Metabólico
1ºPASSO!
Bugianesi E.JHepatol. 2016PMID: 27401791

DoençaHepáticaNãoAlcoólica- factoresmoduladores
A.Lonardo et alDig Liver Dis.2015PMID:26454786
Moduladoresfisiológicos
Moduladoresmetabólico

DHNA– Fluxogramadeavaliação
AltaProbabilidadeObesoDM2Síndr.Metabólico
Bugianesi E.JHepatol. 2016PMID: 27401791
SCREENING
ECOGRAFIAABDOMINAL
TRANSAMINASES(ALT)
FATTYLIVERINDEX(FLI)
Sensibilidadesópara>20/30%deesteatose
<30– BAIXORISCO>60– ALTORISCO
•IMC,•Perímetro abdominal•Triglicéridos•GGT
Homens>30U/LMulheres>19U/L

DHNA– Fluxogramadeavaliação
SCREENING
ECOGRAFIAABDOMINAL
TRANSAMINASES(ALT)
FATTYLIVERINDEX(FLI)
AltaProbabilidadeObesoDM2Síndr.Metabólico
<30– BAIXORISCO>60– ALTORISCO
Homens>30U/LMulheres>19U/L
AVALIAÇÃOFIBROSE
Sensibilidadesópara>20/30%deesteatose
Bugianesi E.JHepatol. 2016PMID: 27401791

DoençaHepáticaNãoAlcoólica- Fibrose
Fibroseéofactordemaiorimpactoprognóstico
Fibrose3- 4
Fibrose1- 2
Controlos
Ekstedt M,Hepatol 2015–PMID:25125077AnguloP,Gastroenterol 2015–PMID:25936633
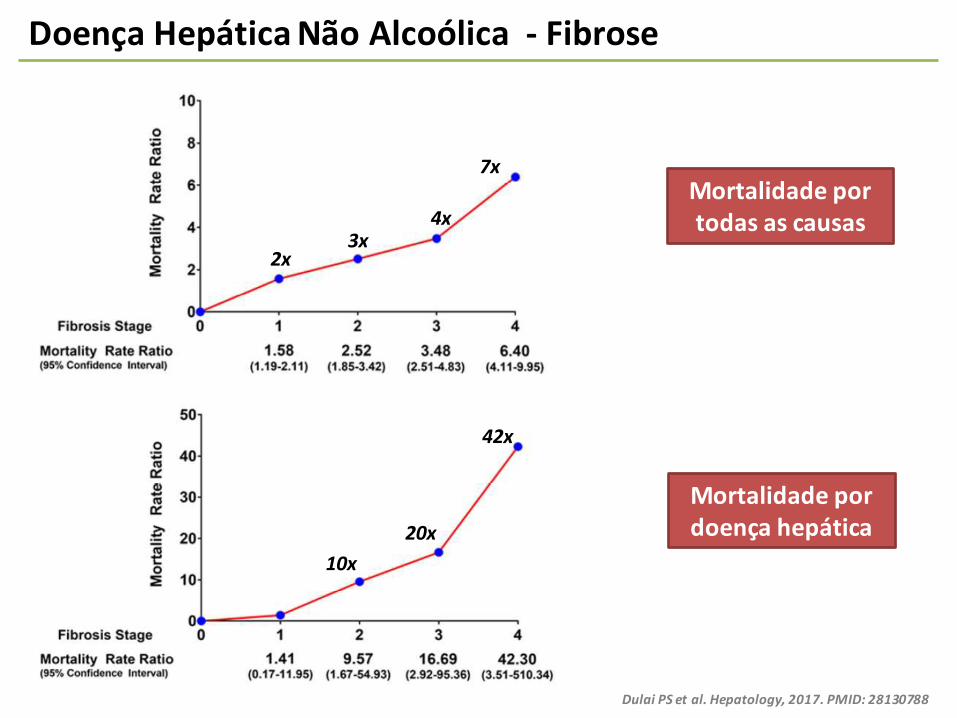
Mortalidadeportodasascausas
DoençaHepáticaNãoAlcoólica- Fibrose
Mortalidadepordoençahepática
Dulai PSetal.Hepatology,2017.PMID: 28130788
7x
4x3x
2x
42x
20x10x

DoençaHepáticaNãoAlcoólica- Factoresderisco
Podemospreverquemevoluicomfibrose?
SinghSet al.Clin Gastroenterol Hepatol.2015PMID: 24768810
DHNA– Fluxogramadeavaliação
SCREENING
AltaProbabilidadeObesoDM2Síndr.Metabólico
AVALIAÇÃOFIBROSE
DHNA
FIBROSCAN®TESTESCOMPLEXOSMÉTODOSSIMPLES
NAFLDFibrosis Score(NFS)<- 1.455-1.455– 0.675>0.675
F0ouF2IndeterminadoF3ouF4
FIB-4<1.30>2.67
F0ouF1F3ouF4
Fibrotest ®Fibrometer ®
Bugianesi E.JHepatol. 2016PMID: 27401791

NAFLDFibrosisscore• BMI• Age• Hyperglycemia• AST/ALTratio• Platelets• Albumin
BARDScore• BMI>28• AST/ALT>0.8• Diabetes• Femalesex
APRI• AST• Platelets
FIB-4• Age• AST• ALT• Platelets
DoençaHepáticaNãoAlcoólica– métodosnãoinvasivos
WaiCT,Hepatology.2003PMID: 12883497Sterling RKet al.Hepatology.2006PMID: 16729309
Anguloetal,Hepatology.2007PMID: 17393509Harrison SAet al.Gut. 2008PMID: 18390575
McPherson S.Gut. 2010PMID: 20801772

DoençaHepáticaNãoAlcoólica– FIBROSCAN®
CassinottoC.Hepatology.2016PMID:26659452F.Contietal.DigestiveandLiverDisease. 2016- PMID: 27522549
F2 F3 F4
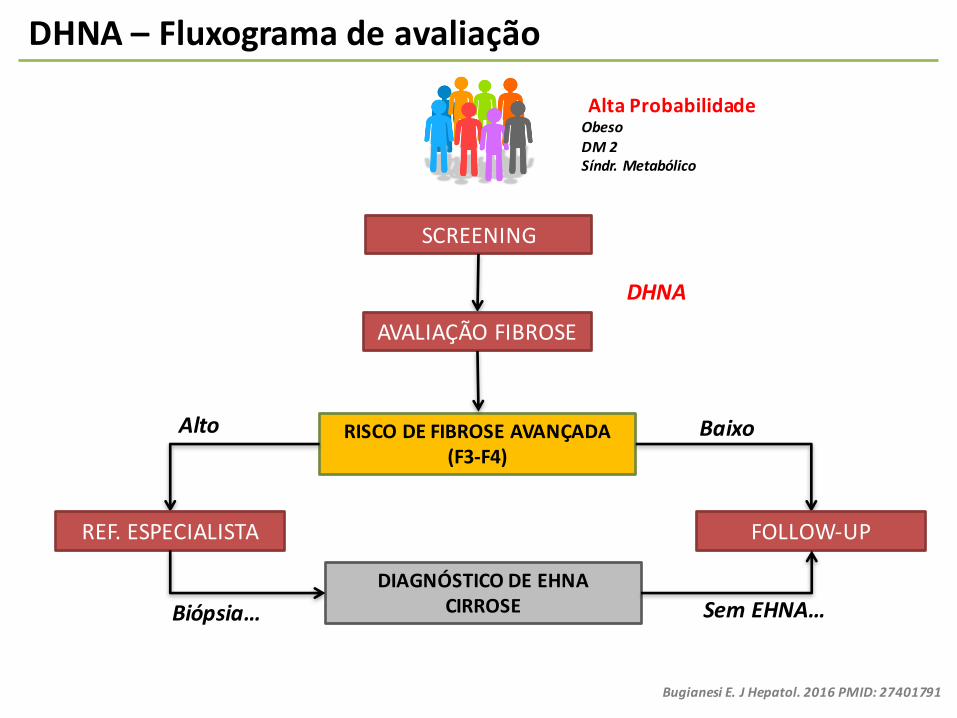
DHNA– Fluxogramadeavaliação
SCREENING
AltaProbabilidadeObesoDM2Síndr.Metabólico
AVALIAÇÃOFIBROSE
DIAGNÓSTICODEEHNACIRROSE
RISCODEFIBROSEAVANÇADA(F3-F4)
DHNA
REF.ESPECIALISTA FOLLOW-UP
Alto Baixo
Biópsia… SemEHNA…
Bugianesi E.JHepatol. 2016PMID: 27401791

Casoclínico- 1
ExameObjectivo:• Altura 167 cm• Peso 85 kg• IMC 30.1 kg/m2
Análise Valor
Hb 11,5 g/dL
VGM 95,4 fL
Plaq 154000 106/L
INR 1,02
Glucose 86 mg/dL
HbA1C 5,6 %
Insulina 6,3 uU/mL
Col. Total 170 mg/dL
LDL/HDL 103/53 mg/dL
TAG 71 mg/dL
AST/ALT 17/11 U/L
FA 76 U/L
BT 0,69 mg/dL
albumina 3,9 g/dL
NAFLDFibrosisscore- 1,996
<- 1.455 - F0ou F2
ID:sexofeminino, raçacaucasiana,72anos.
FIB-42,4
1,3-2,6- indeterminado
VIGIAR+/-
FIBROSCAN
RISCOCARDIOVASCULAR

Nature Reviews | Gastroenterology & Hepatology
Early-stage NAFLD Late-stage NAFLDIntermediate
Lifestyle intervention such as diet and exercise changes
Bariatric surgery such as gastric bypass or sleeve gastrectomy*
Current therapies• Vitamin E• Pentoxifylline• Insulin sensitizers
Therapies in development• Obeticholic acid• GFT505
Pharmacological therapy
Screening for HCCand oesophageal varices
NASH stage 1–��ȮDTQUKU� NASH with cirrhosisSteatosis alone
fibrosis (an unexpectedly high proportion given the short trial duration), which might have therefore overestimated the antifibrotic effect of liraglutide. It is also unclear to what degree the liraglutide-associated weight loss con-tributed to the histological improvement, compared with the contribution of the direct effects of liraglutide independent of weight loss. A full publication and further validation of the data in larger trials are awaited110.
Management of high-risk NAFLDIn patients with advanced fibrosis (bridging fibrosis or cirrhosis), the risk of adverse clinical outcomes is more imminent. On the basis of existing evidence, the goals of therapy in patients with advanced liver disease include the reversal of the fibrogenic process that is driving the progression of liver fibrosis, correction of the underlying metabolic and inflammatory drivers of the disease and prevention or treatment of the complications of cirrho-sis. Patients with cirrhosis should be screened for HCC and undergo screening for oesophageal varices as recom-mended by American Association for the Study of Liver Diseases practice guidelines24.
A study published in 2013 indicated that rifaximin in patients with alcoholic cirrhosis reduced the risk of all complications of cirrhosis and hepatic decompensa-tion following an initial bout of variceal haemorrhage111. If validated in future trials, rifaximin might provide an aetiology-agnostic method to reduce the risk of decompensation in patients with cirrhosis.
Until the past few years cirrhosis was not thought to be a reversible process. However, studies in patients infected with HBV have illustrated that fibrosis could be reversed with effective treatment of the underlying disease, even in the setting of cirrhosis112. Since these initial pub-lications, substantial research has illustrated the dynamic nature of hepatic fibrogenesis and dissolution, leading to the development of multiple new antifibrotic com-pounds113. Currently, no approved therapy is available to specifically reverse advanced fibrosis and tissue remodel-ling in NASH. However, three major antifibrotic therapies are currently in phase IIb trials and the results of these are eagerly anticipated. The first trial involves a monoclonal antibody against lysyl oxidase, an enzyme critical for col-lagen crosslinking. Lysyl oxidase has also been implicated in the trafficking of stem cells to the liver and modulation of the microenvironment to promote hepatic carcino-genesis114. The second therapy, cenciviroc, is a CCR2 and CCR5 antagonist. Although it primarily targets inflamma-tion, inhibiting CCR2 and CCR5 also improves fibrosis and insulin sensitivity. Additionally, evidence suggests that macrophage infiltration in adipose tissue is CCR2 medi-ated, hence the rationale for the use of this agent in diabe-tes mellitus115,116. The third agent is an antibody against the profibrogenic galectin family of lectin proteins. Treatment with a galectin-binding complex carbohydrate markedly reduced fibrosis in an animal model of NASH117.
ConclusionsThe treatment of NAFLD and NASH is rapidly evolv-ing, yet not all patients with NAFLD need pharmaco-logical treatment. In order to recommend the most appropriate treatment approach, it is important for the clinician to be able to identify those patients at greatest risk of disease progression and to risk stratify them by the severity of their liver disease. The evidence base for treatment is growing and proof of short-term efficacy on the basis of surrogate histological end points for several agents is already available. Some concerns remain about the long-term safety of available agents, necessitating thoughtful consideration of the potential risks and bene-fits. Multiple new drugs are in development and the path-ways for drug approval are being clarified. A variety of therapies will probably emerge over the next 5–7 years, permitting a stage-based approach (FIG. 2) and/or greater personalization of drug selection.
Figure 2 | #�UVCIG�DCUGF�CRRTQCEJ�VQ�VJG�VTGCVOGPV�QH�0#(.&��Lifestyle modifications should be pursued throughout the disease course. Pharmacological therapy is not advised for patients with early-stage NAFLD as a result of their low risk of disease progression; however, in patients with intermediate to late stage NAFLD drugs can be a prescribed based on a risk-benefit analysis. Patients with cirrhosis should be screened for HCC and oesophageal varices. Bariatric surgery can be considered for any patient that meets selection criteria��, and can be safe and effective in carefully selected individuals with advanced fibrosis and cirrhosis, although patients with cirrhosis should only by treated in centres with extensive experience with patients with liver disease. �0#5*�UVCIG��s��HKDTQUKU�EQPHKTOGF�D[�DKQRU[��*%%��JGRCVQEGNNWNCT|ECTEKPQOC�
1. Matteoni, C. A. et al. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology 116, 1413–1419 (1999).
2. Wong, R. J., Cheung, R. & Ahmed, A. Nonalcoholic steatohepatitis is the most rapidly growing indication for liver transplantation in patients with hepatocellular carcinoma in the U.S. Hepatology 59, 2188–2195 (2014).
3. Pais, R. et al. A systematic review of follow-up biopsies reveals disease progression in patients with non-alcoholic fatty liver. J. Hepatol. 59, 550–556 (2013).
4. Pais, R. et al. Progression from isolated steatosis to steatohepatitis and fibrosis in nonalcoholic fatty liver disease. Clin. Res. Hepatol. Gastroenterol. 35, 23–28 (2011).
5. McPherson, S. et al. Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using
paired biopsies: implications for prognosis and clinical management. J. Hepatol. 62, 1148–1155 (2015).
6. Ratziu, V. et al. Liver fibrosis in overweight patients. Gastroenterology 118, 1117–1123 (2000).
7. Angulo, P., Keach, J. C., Batts, K. P. & Lindor, K. D. Independent predictors of liver fibrosis in patients with nonalcoholic steatohepatitis. Hepatology 30, 1356–1362 (1999).
REV IEWS
8 | ADVANCE ONLINE PUBLICATION www.nature.com/nrgastro
© 2016 Macmillan Publishers Limited. All rights reserved
Tratamento
RinellaME,NRGH2016–PMID26907882
DHNA– TRATAMENTO

Casoclínico- 2
ID:sexomasculino,raçabranca,65anos.
Motivo: Esteatohepatite nãoalcoólica(EHNA)
HDA: Dador de sangue de 1983-1995 (A Rh+), altura em que se detectam alterações das provashepáticas (aminotransferases flutuantes de 2-5x LSN, sem colestase). Antecedentes de contacto comtricloroetileno inalado (na fábrica) de 1980-1997. Restante investigação, sem outra causa etiológica quenão FGNA (teve um AMA positivo transitório).
AntecedentesPessoais- dislipidémia mistahámaisde15anos- HTAdesdehácercade20anos- Excessodepesodesdejovem
Hábitos:hábitosalcoólicos(1U/d)– abstinentedesde1997,ex-tabagista (10UMA)– 1980. Medicação: sinvastatina,copalia (amlodipina+valsartan),alfuzosina,omeprazol
AntecedentesFamiliares:- paifaleceucom87anosporcarcinomahepatocelular(semhistóriadeconsumodeálcool)- 2filhos(37e42anos),saudáveis;3netas(saudáveis)

Casoclínico- 2
ExameObjectivo:• Altura 172 cm• Peso 94 kg• IMC 31.8 kg/m2• sem estigmas de DHC
Análise ValorHb 14,6 14,3 g/dL
Plaq 206 178 109/L
INR 0,98 1,05
Glucose 95 92 mg/dL
Col. Total 191 179 mg/dL
LDL/HDL 109/44 112/38 mg/dL
TAG 190 146 mg/dL
AST/ALT 73/139 23/34 U/L
FA 94 67 U/L
BT 0,66 0,5 mg/dL
Albumina 4,7 4,2 g/dL
Exames:• Eco abdominal (2016): contornos regulares, com
esteatose moderada.• BH (2006): NASH com inflamação ligeira e fibrose
moderada
PERDADEPESO9Kg
10cmPer.ABD
C.DIET.NUTRIÇÃO
16,8»5.8kPaFIBROSCAN:
↓TRANSAMINASES
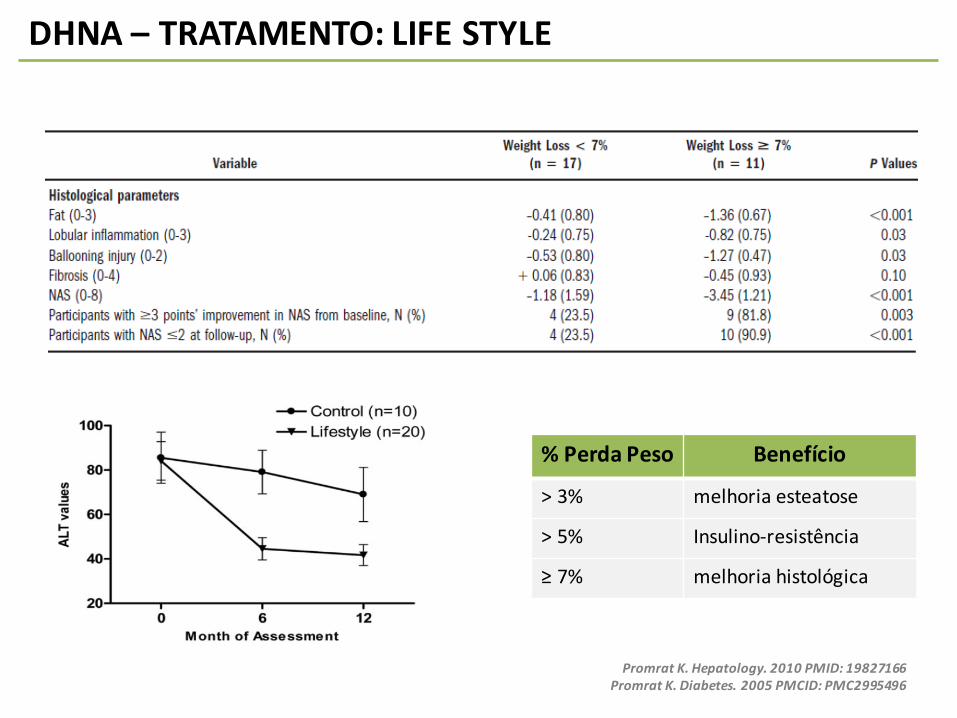
DHNA– TRATAMENTO:LIFESTYLE
%Perda Peso Benefício
>3% melhoriaesteatose
>5% Insulino-resistência
≥7% melhoriahistológica
Promrat K.Hepatology.2010PMID: 19827166Promrat K.Diabetes.2005PMCID: PMC2995496

DHNA– TRATAMENTO:LIFESTYLE
ALT
NAS(histologia)
EXERCÍCIOTEMBENEFÍCIOINDEPENDENTEDAPERDADEPESO
Katsagoni CN;Metabolism. 2017.PMID: 28183444

Casoclínico- 3
ID:sexofeminino,raçabranca,33anos.
Motivo: Esteatohepatite nãoalcoólica(EHNA)
AntecedentesPessoais• Dislipidémia• HTA• Obesidade(IMC33kg/m2)• DMtipo2NIT• DoençadeBeçhet• Tiroidide deHashimoto
Exames:• BH de 2011 - NASH + fibrose moderada• Fibroscan de 2015 de 18 kPa (F4)
• Fibroscan de 2016 de 26.3 kPa (F4)• Padrão flutuante das transaminases
Peso:82Kg »80Kg»82Kg»84Kg»83Kg
Life Style
Terap.Farmacologica

Nature Reviews | Gastroenterology & Hepatology
Early-stage NAFLD Late-stage NAFLDIntermediate
Lifestyle intervention such as diet and exercise changes
Bariatric surgery such as gastric bypass or sleeve gastrectomy*
Current therapies• Vitamin E• Pentoxifylline• Insulin sensitizers
Therapies in development• Obeticholic acid• GFT505
Pharmacological therapy
Screening for HCCand oesophageal varices
NASH stage 1–��ȮDTQUKU� NASH with cirrhosisSteatosis alone
fibrosis (an unexpectedly high proportion given the short trial duration), which might have therefore overestimated the antifibrotic effect of liraglutide. It is also unclear to what degree the liraglutide-associated weight loss con-tributed to the histological improvement, compared with the contribution of the direct effects of liraglutide independent of weight loss. A full publication and further validation of the data in larger trials are awaited110.
Management of high-risk NAFLDIn patients with advanced fibrosis (bridging fibrosis or cirrhosis), the risk of adverse clinical outcomes is more imminent. On the basis of existing evidence, the goals of therapy in patients with advanced liver disease include the reversal of the fibrogenic process that is driving the progression of liver fibrosis, correction of the underlying metabolic and inflammatory drivers of the disease and prevention or treatment of the complications of cirrho-sis. Patients with cirrhosis should be screened for HCC and undergo screening for oesophageal varices as recom-mended by American Association for the Study of Liver Diseases practice guidelines24.
A study published in 2013 indicated that rifaximin in patients with alcoholic cirrhosis reduced the risk of all complications of cirrhosis and hepatic decompensa-tion following an initial bout of variceal haemorrhage111. If validated in future trials, rifaximin might provide an aetiology-agnostic method to reduce the risk of decompensation in patients with cirrhosis.
Until the past few years cirrhosis was not thought to be a reversible process. However, studies in patients infected with HBV have illustrated that fibrosis could be reversed with effective treatment of the underlying disease, even in the setting of cirrhosis112. Since these initial pub-lications, substantial research has illustrated the dynamic nature of hepatic fibrogenesis and dissolution, leading to the development of multiple new antifibrotic com-pounds113. Currently, no approved therapy is available to specifically reverse advanced fibrosis and tissue remodel-ling in NASH. However, three major antifibrotic therapies are currently in phase IIb trials and the results of these are eagerly anticipated. The first trial involves a monoclonal antibody against lysyl oxidase, an enzyme critical for col-lagen crosslinking. Lysyl oxidase has also been implicated in the trafficking of stem cells to the liver and modulation of the microenvironment to promote hepatic carcino-genesis114. The second therapy, cenciviroc, is a CCR2 and CCR5 antagonist. Although it primarily targets inflamma-tion, inhibiting CCR2 and CCR5 also improves fibrosis and insulin sensitivity. Additionally, evidence suggests that macrophage infiltration in adipose tissue is CCR2 medi-ated, hence the rationale for the use of this agent in diabe-tes mellitus115,116. The third agent is an antibody against the profibrogenic galectin family of lectin proteins. Treatment with a galectin-binding complex carbohydrate markedly reduced fibrosis in an animal model of NASH117.
ConclusionsThe treatment of NAFLD and NASH is rapidly evolv-ing, yet not all patients with NAFLD need pharmaco-logical treatment. In order to recommend the most appropriate treatment approach, it is important for the clinician to be able to identify those patients at greatest risk of disease progression and to risk stratify them by the severity of their liver disease. The evidence base for treatment is growing and proof of short-term efficacy on the basis of surrogate histological end points for several agents is already available. Some concerns remain about the long-term safety of available agents, necessitating thoughtful consideration of the potential risks and bene-fits. Multiple new drugs are in development and the path-ways for drug approval are being clarified. A variety of therapies will probably emerge over the next 5–7 years, permitting a stage-based approach (FIG. 2) and/or greater personalization of drug selection.
Figure 2 | #�UVCIG�DCUGF�CRRTQCEJ�VQ�VJG�VTGCVOGPV�QH�0#(.&��Lifestyle modifications should be pursued throughout the disease course. Pharmacological therapy is not advised for patients with early-stage NAFLD as a result of their low risk of disease progression; however, in patients with intermediate to late stage NAFLD drugs can be a prescribed based on a risk-benefit analysis. Patients with cirrhosis should be screened for HCC and oesophageal varices. Bariatric surgery can be considered for any patient that meets selection criteria��, and can be safe and effective in carefully selected individuals with advanced fibrosis and cirrhosis, although patients with cirrhosis should only by treated in centres with extensive experience with patients with liver disease. �0#5*�UVCIG��s��HKDTQUKU�EQPHKTOGF�D[�DKQRU[��*%%��JGRCVQEGNNWNCT|ECTEKPQOC�
1. Matteoni, C. A. et al. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology 116, 1413–1419 (1999).
2. Wong, R. J., Cheung, R. & Ahmed, A. Nonalcoholic steatohepatitis is the most rapidly growing indication for liver transplantation in patients with hepatocellular carcinoma in the U.S. Hepatology 59, 2188–2195 (2014).
3. Pais, R. et al. A systematic review of follow-up biopsies reveals disease progression in patients with non-alcoholic fatty liver. J. Hepatol. 59, 550–556 (2013).
4. Pais, R. et al. Progression from isolated steatosis to steatohepatitis and fibrosis in nonalcoholic fatty liver disease. Clin. Res. Hepatol. Gastroenterol. 35, 23–28 (2011).
5. McPherson, S. et al. Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using
paired biopsies: implications for prognosis and clinical management. J. Hepatol. 62, 1148–1155 (2015).
6. Ratziu, V. et al. Liver fibrosis in overweight patients. Gastroenterology 118, 1117–1123 (2000).
7. Angulo, P., Keach, J. C., Batts, K. P. & Lindor, K. D. Independent predictors of liver fibrosis in patients with nonalcoholic steatohepatitis. Hepatology 30, 1356–1362 (1999).
REV IEWS
8 | ADVANCE ONLINE PUBLICATION www.nature.com/nrgastro
© 2016 Macmillan Publishers Limited. All rights reserved
Tratamento
RinellaME,NRGH2016–PMID26907882
DHNA– TRATAMENTO

DHNA– TRATAMENTOArticles
6 www.thelancet.com Published online November 7, 2014 http://dx.doi.org/10.1016/S0140-6736(14)61933-4
p=0·0002) (table 2). These results did not change after prespecifi ed sensitivity analyses with adjustment for confounders (including weight loss) and multiple imputation for eight patients treated with obeticholic acid and 11 treated with placebo who had missing data on the primary outcome (appendix). Post-hoc subgroup analysis showed no diff erence in the treatment eff ect for the primary outcome between baseline demographic, clinical, or previous treatment subgroups (appendix).
More patients assigned to obeticholic acid compared with placebo had improvement in fi brosis, hepato cellular ballooning, steatosis, and lobular infl ammation (table 2). The mean change in the NAFLD activity score was greater in patients treated with obeticholic acid than placebo (change from baseline=–1·7 vs –0·7; p<0·0001). Despite these improvements in the individual histological features of non-alcoholic steatohepatitis, the proportion of patients with resolution of non-alcoholic steatohepatitis (ie, change from baseline diagnosis to not non-alcoholic steatohepatitis) did not diff er in patients treated with obeticholic acid compared with placebo (22 [22%] of 102 vs 13 [13%] of 98; p=0·08) (table 2).
All patients who completed their fi nal on-treatment study visit and the visit 24 weeks after stopping treatment
(including those without a fi nal biopsy due to early treatment termination) were included in the group comparisons of non-histological secondary outcomes. Signifi cant reductions in serum alanine aminotransferase and aspartate aminotransferase concentrations developed over the fi rst 36 weeks of treatment with obeticholic acid and were sustained for the duration of treatment (fi gure 2, appendix). By contrast, serum alkaline phos-phatase concentrations increased, although γ-glutamyl transpeptidase concentrations (another indicator of cholestasis) decreased. These changes in liver enzyme concentrations reversed after obeticholic acid was stopped and at 24 weeks after treatment discontinuation there were no signifi cant diff erences between the two groups (fi gure 2, appendix).
Compared with placebo, treatment with obeticholic acid was associated with weight loss and a small decrease in systolic blood pressure (fi gure 2, table 3). Fasting serum insulin concentrations were higher and the homoeostasis model of assessment (HOMA) indicated greater hepatic insulin resistance with obeticholic acid treatment compared with placebo at week 72 (table 3). The changes in HOMA and weight reverted towards baseline after treatment was stopped
Figure 2: Changes from baseline in liver enzymes and bodyweight according to treatment groupMean values of changes from baseline during treatment with obeticholic acid (141 patients) or placebo (142 patients) for up to 72 weeks followed by a 24-week post-treatment period are shown. Error bars show 95% CIs. *p<0·05; p values were derived from linear regression modelling change as a function of treatment group and the baseline value of the outcome. Data are included from patients whose treatment was terminated early according to protoc ol design and their serum biochemical test results obtained 24 weeks after stopping treatment are included with the 96-week mean values. (A) Alanine aminotransferase concentrations decreased during treatment with obeticholic acid, reaching a reduced baseline 36 weeks after initiating treatment, whereas concentrations in patients treated with placebo remained unchanged. Alanine aminotransferase concentrations in the obeticholic acid group reverted back to being indistinguishable from placebo 24 weeks after treatment discontinuation. (B) Serum alkaline phosphatase concentrations increased whereas (C) serum γ-glutamyl transpeptidase decreased early in the course of treatment with obeticholic acid. (D) Bodyweight decreased throughout treatment with a rebound back toward baseline after treatment discontinuation.
* **
**
*
–40
–30
–20
–10
0
Alan
ine a
min
otra
nsfe
rase
(U/L
)
A
–10
0
10
20
Alka
line p
hosp
hata
se (U
/L)
B
* ** * *
*
* **
* **
0 12 24 36 48 60 72 96
–40
–60
–20
0
γ-gl
utam
yl tr
ansp
eptid
ase (
U/L)
Weeks
C
0 12 24 36 48 60 72 96
–4
–2
0
2
Wei
ght (
kg)
Weeks
D
* **
* *
PlaceboObeticholic acid
Neuschwander-Tetri BA,Lancet2015– PMID:25468160
FLINTTRIAL– ÁcidoObeticólico

Casoclínico- 4
ID:sexofeminino,raçabranca,62anos.
Motivo: Cirrose(EHNA)
AntecedentesPessoais• CirroseHepáticaaNASH
- Child A(6pontos),MELD11- Hiperesplenismo- DMtipo2 NIT
• Excessodepeso• Dislipidémia
Históriadoençaactual:• Varizesesofágica»RoturadeVE»programadeLEVE
Ecografiaabdominal(09.2016):hepatomegália comcontornoirregular,semlesõesfocais,esplenomegália (17,2cm),semascite.
Análisescomalfa-fetoproteína normal
Ecografiaabdominal(02.2017):nódulohepáticode17mm
!! !!
Death/OLT/*complica1ons*
Slow*Progressors*
Rapid*Progressors*
?7yrs! !?5(6yrs!
Simple*steatosis*Steatosis*+*Lobular*Inflamma1on*
NASH*+/C*Portal*Inflamma1on*
Advanced*fibrosis*(Cirrhosis)*
Early*fibrosis*
!! !!

CONCLUSÕES
• A DHNA É MUITOPREVALENTE NOMUNDO OCIDENTAL.
• A DHNA ASSOCIA-SE A FACTORES DE RISCOMETABÓLICOS (obesidade, DM, IR…).
• É IMPORTANTE:1. IDENTIFICARPOPULAÇÃOEMRISCO2. RASTREARPARAA DHNA REFERENCIARVs VIGIAR3. AVALIARO RISCO/PRESENÇADE FIBROSE
• A DHNA ASSOCIA-SEAUMAUMENTODAMORTALIDADE POR TODAS AS CAUSAS
• A INTERVENÇÃONOESTILODE VIDA – PERDADE PESO– ESSÊNCIAL.
• NOVAS TERAPÊUTICAS PODERÃO ACTUAR NA PROGRESSÃO/REGRESSÃO DAFIBROSE.