四回目aamam--ea----- a eginmu.naramed-u.ac.jp/dspace/bitstream/10564/2698/3/03... ·...
TRANSCRIPT
Hepatology Research
個目掴'a園田町- - E a - - - - -am
価'
a ....
‘ aam
司
自UHF
- 田
h曹
四回目"厳司
BLue
-}, 引一 一t
ate-- ,BEa--z
節Ba'z J.e
The ADAMTS13 activity may predict the cumulative survival
of patients with liver cirrhosis 四 in comparison with the
Child-Turcotte-Pugh score and the MELD score
「-て二 玉E弓亙亙豆E E7二二二て二二二三二コ!一一一一竺竺竺10: D竺 一一一一一---ーー一一一一一一一一一一一一一 Ji Manuscript Type: I Original A代icle I
一一ムーj 一一 一一一一 一ー ーー句ーーーー一町一一一一ー ーー一一時一一一一一一一一一ー」「一一一一一一一一ー一一一一一一一一一一ー一一 丁
Date Submitted by the I _ ,_ ! I n/a :
Author: I '" ~ I
「下両lete List of Authors: r~-;k;料 Hiro出i; NARA MEDICAL U附 ERふ石示両日OF -ー
I INTERNAL MEDICINE i Uemura , Masahito; NARA MEDICAL UNIVERSITY , 3RD DEPT OF
Fujimura , Yosh ihiro; NARA MEDICAL UNIVERSITY , DEPARTMENT of BLOOD TRANSFUSIOIN MEDICINE Matsumoto , Masanori ; NARA MEDICAL UNIVERSITY , DEPARTMENT of BLOOD TRANSFUSIOIN MEDICINE Matsuyama , Tomomi; NARA MEDICAL UNIVERSITY , 3RD DEPT OF INTERNAL MEDICINE ikato ,S巴iji; NARA MEDICAL UNIVERSITY , DEPARTMENT of BLOOD TRANSFUSIOIN MEDICINE Morioka , Chie ; NARA MEDICAL UNIVERSITY , 3RD DEPT OF INTERNAL MEDICINE Ishizashi , Hiromichi; NARA MEDICAL UNIVERSITY , DEPARTMENT of
i … TRANS … N 悶旧叩………D凹閃m叩IC悶ICIN口捌I刑NHori , Yuji; NARA MEDICAL UNIVERSITY , DEPARTMENT of BLOOD TRANSFUSIOIN MEDICINE Fujimoto ,問asao; NARA MEDICAL UNIVERSITY , 3RD DEPT OF INTERNAL MEDICINE Tsujimoto , Tatsuhiro; NARA MEDICAL UNIVERSITY , 3RD DEPT OF INTERNAL MEDICINE Kawaratani , Hideto; NARA MEDICAL UNIVERSITY , 3RD DEPT OF INTERNAL MEDICINE Kurumatani , Norio; NARA MEDICAL UNIVERSITY , DEPARTMENT OF HEAL TH AND EPIOEMIOLOGY Fukui , Hiroshi; NARA MEDICAL UNIVERSITY , 3RD DEPT OF
: 一一一一一一一一一 一一寸一一幅一一一一一一一一一一一一Category: ' 10, Liver failure , 8, Fibrosis and cirrhosis
The Japan Society of Hepatology , Tokyo , Japan
Page 1 of 23 Hepatology Research
5心10LARMJnus 亡ripts
The Japan Society of Hepatology. Tokyo ‘Japan
Hepatology Research
A Takaya , et al. ADAMTS 13 and prognosis of liver cirrhosis
The ADAMTS13 acti 吋tymay predict the cumulative survival of patients with liver
cirrhosis -in comparison with the Child 回Tu rcott ←Pughsco 問 and the MELD sco 問
Running tit1e: ADAMTS 13 and prognosis of1iver cirrhosis
回roaki Takaya 1, M部油ito Uemura 1, Yoshihiro F司加問t,M出anori Matsumotcf ,
Tomomi Matsuyama 1, Seiji Kat0 2, Chie Morioka 1,回romichi Ishiz 田:h i2,Yuji Horf ,
MasaoF 吋imoto 1,Tatsuhiro Ts吋imo 旬l,回detoKawara 路ni¥ Norio Kurumatani 3,回roshi Fukui 1
ln世dDepar 伽1ent ofIntem a1 Medicine , 2Dep 紅白1ent ofBlood Transfusion Medicine , 3Department
of Community Health and Epidemiology , Nara Medic a1 University , K郎副har a, Nara, 634 ・8522 ,
Japan
Ad世田scorrespondence to M出d世加Uem 四百,M.D. 百世dDep ぽ伽1ent ofIntem a1 Medicine , Nara
Medic a1 Universi 臥 K組曲四百, Nara , 634 ・8522 ,Japan. Tel +81 ・744 ・22・3051 ,ext. 3415; F砿:
+81 ・744 ・24-7122; E圃mail:muemura @naram 時 u.acjp
Abbreviations used in this paper: LC, liver cirrhosis; CτP score , Child- Turco 枕.e- Pughs ∞re,MELDscore , Model 伽 End-Stage Liver Disease score; TIPS ,仕組sjug 叫ar intrahepatic portosystemic shunt; ADAMTS , a disintegrin ・l匙eand meta l1oproteinase domain with 吐rrombospondin typ e-l motif; VWF , von Willebrand 血ctor; UL- V京高'M, unusu a11y large von Wulebrand 晶ωrm 叫也ner;HSC , hepatic stellate cells; VWF:AG , von Willebrand 晶ctor antigen; ADAMTS13:AC , ADAMTS13 activity; TTP,吐 lfombotic 由rombocytopenic purp 四百; HCV, hepatitis C virus; HBV, hepatitis B v加s; PBC , P出nary biliary cirrhosis; RS, risk score; SBP , spon 旬neous bacteri a1 perito 凶出;HCC ,hepa 加cellular carcinoma; ns, Japan Integrated Staging; VWFM , VWF m叫timer;VWF:RCo , VWF ristocetin cofactor activity; ELISA , e回戸ne-linked immunosorbent 出say;ADAMTSI3:INH , ADAMTS13 inhibitor.
Total word count; in abstract 250; and text 3549 (excluding the figures , legends and referen ∞s). The number oftables; 2,τhe number of figures; 3
The Japan Society of Hepatology , Tokyo , Japan
Page 2of23
1
Page 3 of 23 Hepatology Research
A Tak: aya , et al. ADAMTS 13 and prognosis of liver cirrhosis
Abstract
Aims: Decre 田ed plasma ADAMTS13 activity (ADAMTS13:A C) res 凶ts in the accumulation of
unus 聞 lly large von Willebrand 恥 tor multimers and platelet 世lfombi fonnation. our aim wasω
evaluate wheth 町ADAMTSI3:AC is a prognostic marker in patients wi也liver cirrhosis.
Method 旨: Plasma ADAMTSI3:AC and its related parameters WI町eexamined 企om 108 cirrhotic
patients.
Results: ADAMTSI3:AC decreased 回出eseverity of liver disease increased (means: controls
100% , Child A-cirrhotics 79% , Child ,B-cirrhotics 63% ,組dChild C-cirrhotics 31 %).
ADAMTS 13 :AC markedly decreased in也ecirrhotics with hepatorenal syndrome , re企actory ascites
and hepatic encephalopathy. 百lecumulative survival time w出 the shortest (median 4.5 mon 血s)血
cinhotics wi血asev ,ぽ'eto moderate ADAMTSI3:AC deficiency (<3~25%), followed bythose with
a mild ADAMTSI3:AC deficiency (2仰い50%) ,and W:出世lelongest in those wi也anonnal r,佃ge
of activity (>50%). In con 仕'ast ,based on the Child~司郎0社e-Pugh (C1P) score , Child C-cirrhotics
had the worst survival , but the survival probabilities did not di晶:rbetween Child A and B cirrhotics.
Based on the Model for End-Stage Liver Disease (ME LD) s∞re, the survival w:回世leworst for
cirrhotics 白血efOUl也 quartile ,while it W:出 notdi 自己:rent 釘nong cirrhotics in由efirstthr 田 q田 rtiles.
In cirrhotics in也esequential s加dy,ADAMTS13:AC significantly decreased wi也白eprogression of
liverdi 尻町ban ∞.
Conclusions: ADAMTSI3:AC concomitantly decreases as the functionalliver capacity decre 出es.
百由activity may be a use 白1prognostic marker that is equal or superior to血e C1P score and 由e
MELDs ∞reωp 問dict not only 吐leshort 圃tenn prognosis but also the long 北 rmsurvival of cirrhotic
patients.
Key words: AD品灯S13 activi 臥C1Ps∞lre ,liver cirrhosis , ~伍LDscore , prognosis
The Japan Society of Hepatology , Tokyo , Japan
2
Hepatology Research
A Takaya , et al. ADAMTS 13 and prognosis of liver cirrhosis 3
INTRODUCTION
Once patients with liver cirrhosis (LC) develop a decompensated condition , the risk of early mortality
sharply increases 1. Any patient with LC is at risk for specific life 血rea 匂ning complications such as
variceal bleeding , sepsis , or hepatorenal syndrome , and hepatopulmonary s戸ldrome. Many studies
have examined factors that predict the survival of patients wi出LC1・7 百leChild score was originally
designed 加国sess the prognosis of cirrhotic patients undergoing surgical 悦 atment for portal
hypertension in 1964 2,組dthereafter its modified form , the Child- l1町 'co 町-Pugh (CTP) score 3, has
been widely used to prognosticate patients with LC 1. However , this sc町eincludes some subjective
components and does not estimate other 血ctors ,such as renal and pulmonary dys 白nction ,that are
commonly associated with decompensated c耐hosi~' 3. Furthermore , the CTP score is not always
su血cient ,partiωlarly when predicting 由eshort-term prognosis of patients4• 百le Model for
End-Stage Liver Disease (ME LD) score w出 designed 白出sess 白eprognosis of cirrhotics who receive
a仕組司ugular intrahepatic portosystemic shunt (TIPS) and has been used as a disease severity index
and a new liver organ allocation syst 怠:m for liver transpl 加 tほion since 2002 5. However , the main
causes of death , including variceal bleeding , ascites ラ hepatorenal s戸ldrome and hepatop u1m onary
syndrome , in advanced cirrhotics are not included in the 恥1E LDscore 6. Patients with advanced liver
dise 回目 tend to bl∞d because of reduced plasma levels of several clotting 白ctors and
thrombocytope 凶a, but they also exhibit せrrombotic ∞mplications 7. Portal or hepatic vein thrombosis
is often observed 加advanced cirrhosis 8,9, and microthrombi formation w部品und in one or multiple
organs in half of autopsied cirrhotics lO.百lI shypercoagulable state may not only a島ct hepatic
parench 戸nal extinction , the acceleration ofliver 日brosis ,and disease progression but also impact other
organs and potentially lead to multi-organ failure.
AD品1TS13 但昼isintegrin・like~d旦etalloproteinase with !hrombo~pondin type-l motifs .ll) is a
metalloproteinase 白紙 specifically cleaves multimeric von Willebrand 白c加r(¥ 崎町 between the
Tyr1605 and Metl606 residues in the A2 domain ll, 12. An ADAMTS13 deficiency , caused either by
mutations in theADA MI'S13 gene l1-14 or by inllibit Oly autoantibodies against ADAMTS13 15, 16, results
in the accumulation of "unusually large" VWF multimers 収正圃VWFM) in the plasma. 百lI s
accumulation leads 加 platelet clumping and/or thrombi under high shear 跡目sand subsequent
Tl1e Japan Society of Hepatology , Tokyo , Japan
Page 4 of23
Page 5 of23 Hepatology Research
A Takaya , et al. ADAMTS13 and prognosis ofliver cirrhosis 4
microcirculatory disturbances. ADAMTS13 is produced exc1usively 担hepatic stellate cells (HSCi 7,
although platelets 18, vascular endothelial cells 19, and kidney podocyte;O have been 加plicated 出
ADAMTS13 ・producing cells. 百le pl硲ma levels of VWF:Ag ,也esubs 回te for ADAMTSI3 ,
substan 世ally increases as liver disease progresse;l ・22,組d白rombocytopenia is commonly s閃 nin
patients wi也 advanced LC23-25. Previous studies reported a significant reduction in ADAMTS 13
activity (AD 馴 TS13:A C) in advanced LC26 , 27, while AD馴 TS13 activity 棚田changed in
another s加が. Sub 叫醐tly ,we demons 仕ated 刷 bo白血epl出maAD 馴 TS13 訓吻削
antigen levels decreased 田也eseverity of cirrhosis increase d, and an imbalance between the decreased
ADAMTS 13 :AC and increased levels of its substrate may reflect a期総that predisposes patients wi由
advanced LC to pla 印刷世rrombus formatio~9. In addition , we have shown 由atADAMTSI3 :AC is
reduced in patients wi出hepatic veno ・occlusive disease 30, alcoholic hepatitis 3I, and those undergoing
living 圃donor-related liver transplantation 32. 百lU S,ADAMTS13:AC likely decreases as 由e
functionalliver capacity also declines in advanced liver diseases.
h也is study , we investigated the relationship betw ∞:n ADAMTS13:AC and 血eprognosis of
patients with LC and examined whether 也eADAMTS13:AC is a use 白1prognostic 晶ctor for
cirrhotic patients compared to也eCTP score and the MELD sco 悶.
MATE RlAL SAND METHODS
Patients
百世sstudy examined a total of 108 LC patients , including one patient with 仕lfombotic
出rombocytopenic purp 町 aστpi 3σhble 1). Patients with a known history of coagulopathies ,
platelet disorders , or liver transplantation at basal evaluation were excluded. 百le origin of liver
disease w,出 hepatitis C virus (HCV) in 67 cases , hepatitis B virus (HBV) in 16 patients , alcohol
abuse in 10 patients , p血nary biliary cirrhosis (PBC) in 4 cases , and cryptogenic in 11 patients.
Cirrhosis w,田 diagnosed based on physical 曲ldings and labora 旬ryteはs,加dinm 佃 yc出es w,出
confirmed by histological criteria. Ofthe LC patients , 35 were Child A, 33 were Child B, and 40
were Child C acco 吋ing to Child- Pugh's criteria 3. The MELD risk s∞re 侭S) w,出 calculated
according to the following formula: RS=0.957 x logc (cre 旭町 mg/dl) + 0.378 x .logc (bilirubin
The Japan Society of Hepatology , Tokyo , Japan
Hepatology Research
A Takaya , et al. ADAMTS 13 and prognosis of liver cirrhosis
mg/dl) + 1.1 20 x 10& (INR) + 0.643 x (cause of cirrhosis) in which the value for 白ecause of
cirrhosis w出 ofor an alcoholic or cholestatic etiology and 1 for viral or other etiologies 5. The
恥ffiLD scω 芯 progressively increased 企om Child A to C. 百leplatelet counts decreased with the
severity of chronic liver diseases. 百lespleen volume determined by computed tomography scans 34
increased as liver disease progressed. The diagnosis of ascites , spontaneous bacterial peritonitis
(SBP) , and hepatorenal syndrome w出 made according to 出ecriteria previously described35•
Ascites w出 easily mobilized in 16 patients and re:fr actory in 28. Ten out of26 Child C-LC with
re:fr actory ascites finally progressed to hepatorenal s戸ldrome. SBP occurred in 10 Child C-LC wi也
re企actory ascites , and 由iswas complicated by hepatorenal syndrome in 7 patients. Forty-one LC
patients developed hepatic encephalopathy grade II or higher 回 described by the classification of
Trey et a1.. 37 Sixty 圃seven LC patients had endoscopic signs of 組 impending variceal rupture
according to the criteria of Japanese Research Society for Portal Hypertension 36. 百leincidence of
endoscopic signs of an impending variceal rupture w:拙 higher in LC patients with Child B加 dChild
C血an in Child A. Hepatocellular carcinoma (HCC) w出 detected in 22 patients (62.9%) with
Child A, 16 patients (48.5%) with Child B, and 19 patients (47.5%) with in Child C.百 leincidence
ofHCC did not di島ramongthr ∞groups ,but the Japan Integrated Staging (ns) score 380btained by
adding the 加mor stage score ofHCC and the CTP score progressively increased :fr om Child A to C.
百leportal thrombosis examined by Doppler-ultr 出onography (US) was detected in 3 patients with
Child B and 3 with Child C (Table 1). 白lce patients were discharged , they were care :ful ly followed
up by conventional liver function tests and tumor markers including αイetoprotein and des 岡 γ
-carboxy prothrombin every mon 由回 outpatients until death , which was the primary end-point to
estimate survival probabilities by the CTP score ,出eMELD score and ADAMTS13:AC. Patients
with liver transplantation were , therefore , excluded. Image diagnosis by US, dynamic enhanced
computed tomography (CT), or dynamic enhanced magnetic resonance imaging (J¥依り was
performed every three months to evalu 蹴 presence or absence of HCC or ascites. All subjects
provided informed consent to participate in the s刷dy. 百le study protocol was approved by the
Nara Medical University Hospital Ethics Committee.
The Japan Society of Hepatology , Tokyo , Japan
Page 6 of 23
5
Page 70f23 Hepatology Research
A Takaya , et al. ADAMTS13 and prognosis ofliver cirrhosis
Determina 姐on of ADAMTS13:AC , VWF:Ag , VWF:RCo , UL- VWFMs細 d
ADAMTS13:INH
Blood was ob凶ned 企'om patients at也et加leof admission or dmセ19their hospital s旬y. Samples
were stored 恒例出tic tubes containing 1/10 白血evolmne of 3.8% sodimn ci回te. Platelet-poor
pl田:m aw:出 prepared by c即位ifuging at 3000 x g at 40C for 15 minutes and stored in aliquots at
-80 0C unti1 analysis. For 7 patients wi血LC,a second pl出:m a訓 nple w:回 tak: enbetween days 120
and 630 (mean: 345 days) during their second hospitalization because ofhepatic encephalopathy in 3
patients , ascites au伊len 匂ltion in 4 patients , and variceal rup 加re in 1 patien t. Plasma
AD品目13:AC was determined by ba血acl伽a
e胞回戸yme-凶eか吋-li肱n肱1虫ke吋d i凶I宜mm宜muno 凶so仙r巾be倒n凶t出蹴sa"可iy (但E凹ロS鮎,A,AD品 ITS13-act-ELISA: Kain os Inc., Tokyoll.
The normal values WI的 102 土23% in the VWFM assa y'9 and 99土22%in 世leact ,回ELISA 41.Plasma
VWF:Ag was measured using a rabbit polyclonal sandwich ELISAρ ak: o, Denmark) , and its
normal level was 100 土53% (n=60, 20-39 years of age). VWF ristocetin cofactor activity
れ市1F:RCo) was determined 出 describecf 2,組dits normal value was 100 土15%. In 49 LC patients
wi血 lowl 町 ADAMTS13:AC (1ess 也an 50% of the normal control) , plasma UL- VWFMs were
analyzed by a vertical SDS- l.O% agarose ge1 electrophoresis system 43 and evaluated using Nlli
image J. ADAMTS13 inhibitor (AD AMTS13: INH) was evaluatβd using plasma that was
heat-inactivated at 560C品if 30 minu 旬SI5 ,16.αle Bethesda unit of inhibitor was de曲led 出 the
amount ofplasma that reduces ADAMTSI3:AC to 50% ofthe control 44, and its titer was de:fin ed加
be signi :fi c佃 tat >0.5 Bethesda Units (BU) /ml.
S旬白tical Analysis
Differenc 邸 among cirrhotics wi由 Child A, B and C, and healthy subj 切tswere analyzed wi由也e
Krus kal ・,Wa11 isrank test before pair 圃,wise comparisons (Table 1 & Table 2). If the Krus kaト,Wallis
rank test showed signi :fi cant differences in each parame 町 among groups , pair-wise ∞mparison in
eachpar ,出neter was evalua 飽dby Mann- whi 也eyU test for continuous variable. 百1e X2.t 回twas
used for categorical data. Differenc 図面白eADAMTS13:AC and CτP scores ob旬ined by由e
sequential s加dy 也 identical patien ぉwere estimated by Wilcoxon signed 圃ifanks test. Correlations
The Japan Society of Hepatology , Tokyo , Japan
6
Hepatology Research
A Takaya , et al. ADAMTS13 and pr'Ogn'Osis 'Ofliver cirrh 'Osis
were calculated by the Sperman rank tes t.百 leanalyses w<抑制 ried 'Out山加gStatview statistical
s'O立 ware (versi 'On 5.0; SAS In副知 te,C町~ NC, USA). 百leKaplan 一Meier analysis was used 旬
evaluate the progn 'Osis 'Of cirrh 'Otic patients acc 'Ording t'O白 edegr 田'O fthe plasma ADAMTS13
acti 吋臥批C1Psc'Ore, and 勧 MELD sc'Oreσigure 1,2, and 3) by a l'Og-rank test using Sta tM蹴
N f'Or Wind 'Ows (AT0484 , Advanced Techn 'Ol'Ogy f'Or Medicine & Science , T'O勾 1'0, Japan). A
tw'O周回 led p-value less 也an0.05 w出 c'Onsidered significan t. All data are presented 出 themean 士
S伽 dard deviati 'On (SD).
RESULTS
Clinical outcome σable 1)
D田恒g a medi 佃 f'Oll'Ow-up 'Of 475 days (range; 5旬 2406 days) , 42 LC patients died wi也恒 5 t'O
1161 da戸 after they had provided samples. Of these , 5 cirrh 'Otic patients were classified 田 Chi1 dA,
6出 Child B, and 31 部 Child Cσable 1). 百le 伺lU se 'Of death in Child A patients W:回 HCC 担4
patients and acute my'Ocardial infarcti 'On血 1patien t,也atin Chi1 d B patien 臼W出 HCC in 5 patients
and ga甜ointestinal bleeding in 1 patient , and 由at in Child C patients was HCC in 17 patients ,
hepatic 白ilure in 7 patien 民hepat 'Orenal syn 世ome in 6 patients , and T1P in 1 patientσable 1).
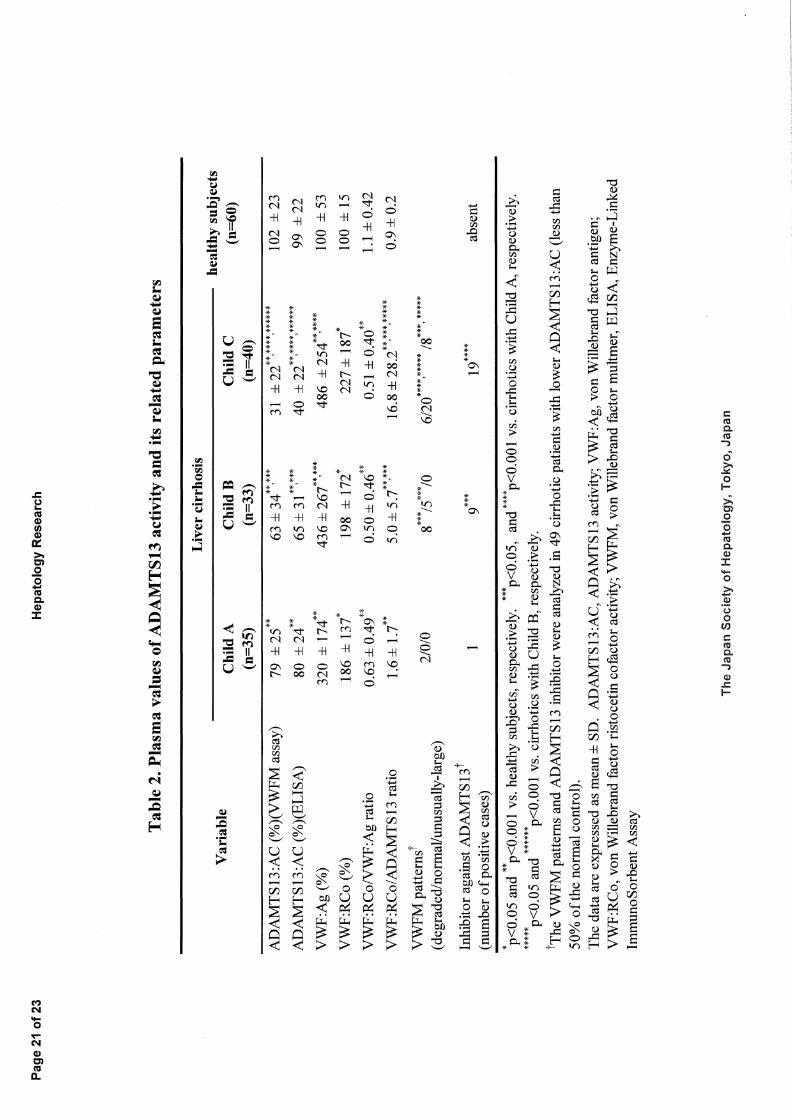
Determination ofADAMTS13:AC and 地問:latedpar. 創neters (Table 2)
Based 'On也eVWFM 田say ,也epl田maADAMTS13:AC w出 56土34% in LC patients , which w出
significantly l'Ower 白an由atin healthy subjects (p<0.001). 百世sactivity progressively decre 田ed出
cirrh 'Osis advanced fr'Om Child A t'O Cσable 2). 百le ADAMTS 13 :AC determined by 吐le
act-ELISA als 'O decreased 郎社lecirrh 'Osis severity incre 出edand w,出 c'Onsistent w抽出eresults 'Of
也eVWFM 出say (1- 0.831 , p<O.OOI). VWF:Ag was significantly high 町泊LCpatients than in
healthy su対ec包,組dw,出higher in patients with Child B and C也anin th'Ose with Child A, but there
W出 n'Odi宜:erence between Child B and Child C patients. The VWF:RC 'O values were higher in LC
patie 凶 than in healthy subjects but did n'Ot differ 翻'Ongthe subgroups 'OfLC patients from Child A
t'OC. 百lerati 'O 'OfVWF:RC 'O加 VWF:Ag was l'Ower in patients with LC (0.54 土0.45,p<0.001) 世lan
in healthy subjects , but 由ere were n'O di能:rences am'Ong LC patients wi由Child A, B, and C. In
The Japan Society of Hepatology , Tokyo , Japan
Page 80f23
7
Page 9 of23 Hepatology Research
A Takaya , et al. ADA 乱1TS 13 and prognosis of liver cirrhosis
con 回st,也eratio ofVWF:RCo to ADAMTSI3:AC signi :fi cantly increased wi血也eprogression of
liver disease. Wi也r田pectto 血eVWFMat 叫yses ,2 Child A cirrhotics had only degraded 園VWFM ,
8 and 5 Child B cirrhotics had degraded 圃.VWFM and normal- VWFM , respectively , and 6, 20, and 8
Child C cirrhotics had degraded 幽.VWFM ,normal- VV¥哩 M,and UL- VWFM , respectively. The
incidence of ADAMTSI3:INH was increased 宜um cirrhotic patients wi也Child A to C (Table 2).
百le凶曲itory activity was 2.0 BU/m t33 in one LC patient wi血1TP and 3.0 BU/ml in a patient with
a severe ADAMTSI3:AC de:fi ciency , but w.出血血emarginal zone between 0.5 and 1.0 BU/ml in
曲目印凶ning patients.
Rela 姐onship ofplasmaADAMTS13:AC to clinical variabl 回
Regarding 血einfluence of HCC ∞mplicated wi也LC on the plasma levels of ADAMTS13:AC ,
ChildALC pa世田tswi 血HCC had a signi :fi cantly lower ADAMTS13:AC 也anthose wi吐loutHCC
(69 土22% vs. 103 土11%, p<O.OOI) , but there were no differences between wi仕1and without HCC
both in LC patients with Child B and Child C. Furthermore , the plasma ADAMTSI3:AC levels
W的 lower in patients with a ns s∞,re of4 (32 土28% ,p<0.05) and ns s∞re of5 (26 土29% ,pく0.05)
由anin patients with a ns score of 0 (67 土24%) ,score of 1 (65 土37%) ,and score of2 (69 土22%). In
addition ,也eADAMTS13:AC levels were signi :fi cantly lower 加 LC patients wi出世le following
clinical conditions than in those without; hepatic encephalopathy (28 土24% vs. 71土29% ,pく0.001) ,
hepatorenal syndrome (13土12%vs.61 土33% ,p<O.OOI) , and severe esophageal varices (46 土33%vs.
75土34% ,p<0.05). Mo悶over ,patients with refractory ascites had a lower ADAMTS13:AC
ο5土17%) than 吐lO se without ascites (70:士30% ,pく0.001) or 由ose wi也 easily mobilized ascites
(56 士37% ,p<O.OOI). 百leADAMTS13:AC w出 lower in cirrhotic patients with po此d世rrombosis
than those without (18土19% vs. 58土34% ,p<0.005). In 7 cirrhotics in 血esequential stud y, the
ADAMTS13:AC signi :fi cantly decreased with 血e progression of liver disturbance
(ADAMTS13:AC 67+23% → 47+29% ,pく0.02 ,Child score 7.7+2 .3→ 8.9+2.η.
The Japan Society of Hepatology , Tokyo , Japan
8

Hepatology Research
A Takaya , et al. ADAMTS13 and prognosis of1iver cirrhosis
Relationship of p"噌 10S Isto曲eCTP score , MELD score 加 dpl制maADAMTS13:AC (Fig.
1,2 &3)
Figures 1 to 3 show the actuarial curves calculated for the survival of the di自主rent patient subgroups ,
according 白血e白reeCτPcl 出ses ,血equartiles of血eMELD risk score (血"5 tqu訂tile ,RS: (ト0.36,
second qu紅白e,RS: 0.37-0.73 ,出廿dqu 紅tile ,RS: 0.7←1.37, and four 由quartile ,RS: 1.38-4.3 2), or
the three ADAMTS13:AC classes (severe to mod 悶 tedeficiency: <25% of the nonnal control , mild
deficiency: 25-50% ofthe nonnal control , and nonnal range: > 5似,). Child C patients had worse
捌 vival 由an Child A and B patients (Figure 1)仔勾rank test among 御伽田 groups ,pく0.0001;
Child C vs. Child A, p<O.OOOI; Child C vs. Child B, p<O.OOOI) , but the survival probabilities were
not di宜erent between Child A and Child B patients. In addition , the survival of patients
corresponding to也efo 町血quartile of the MEill RS w;出 worse 血組曲atof patients corresponding
to the first three RS quぽtiles ,while 吐lesurvival of吐lepatients in也efirst 白ree RS quartiles did not
differ among them 仏og rank test among 由efour groups , p<0.0001; fo町血 quぽtile vs. 0出ers ,
p<O.OOOI). In∞ n回st, the cumulative survival w:出 clearly di民:rent among patients wi血asevere
to moderate AD品汀S13 :ACdeficienc y, mild ADAMTS13 :AC deficienc y, and nonnal range of
ADAMTS13:AC (Log rank test among 批由ree groups , p<O.OOOI; sev 的 tomoderate deficiency
vs. mild deficienc y, p=0.0219; mild deficiency vs. nonnal range , p=0.0287; severe to moderate
deficiency vs. nonnal range , pく0.0001)σigure 3). 百lemedian survival time w;田 the lowest (4.5
months) in cirrhotic patients wi也asevere to moderate ADAMTS 13 :AC deficiency.
DISCUSSION
In this ほudy, we demonstrated 世Ia tcumulative survival di能red according to the levels of plasma
ADAMTS 13 :AC in patients with LC; 吐lesur 吋val timewas 也eshortest in cirrhotics with a severe to
moderate ADAMTS13:AC deficiency , followed by those with a mild ADAMTSI3:AC deficienc ぉ
andw: 出血elongest 白血ose wi由anonnal range of activityσigure 3). In corr 蜘1, based on也e
CTP score , Child C patients had the worst survival , but 世le survival probabilities of Child A and
Child B patients did not d国語rσigure 1). Based on也eMELD score , survival w創出epoorest in
cirrhotics 也血efourth quぽtile ,while it did not di低:r among cirrhotics in the first 由ree quartiles
The Japan Society of Hepatology ,γokyo ,Japan
Page 10 of23
9
Page 11 of 23 Hepatology Research
A Takaya , et al. ADAMTS 13 and prognosis of liver cirrhosis 10
σigure 2). 百leCτP score is not a1ways su血cient to predict short-tenn prognosis 4, and 廿le1¥在 ELD
score has been applied as a disease severity index to peぽonn organ a110cation for liver
仕組splan 匂ition in patients with signi :fi cantly advanced liver diseases. R四latkably ,the median
surviv a1 time was the lowest (4.5 mon 由吟incirrhotics with a severe 旬 modera 旬 ADAMTS13:AC
de:fi ciency , and 也e郎刷出a1 c田vew: 回 very similar or a1m ost identic a1白血 atof patients belonging
to也efour 曲quartile 由eMELD scoreσi 思町田 2& 3). Moreover ,血ethree cumulative surviv a1
curv 回 S仕組:fi edby the degree of deα 右剖ein 也eADAMTS13:AC were clearly di位向ntdur 恒ga
median follow-up of 475 days (企om 5 to 2406 days). Based on previous 問ports and 0町s,也e
degree of deぽ回se in plasma ADAMTS13:AC may be a useful mark ,ぽ加 predict not only 血e
short-tenn prognosis , but a1so the long-tenn surviv a1 ofpatients with LC. It is impo 此ant to be able
to evaluate 也eprognosis of cirrhotic patients using only one p釘amet 民 such 出 ADAMTS13:AC ,
because bo由 the C1P score and the 乱ffiLD score are ca1culated based on a sco 出19 system 也at
encomp 出S回 seve ra1 parameters (bilirubin , a1bumin , prothrombin time , ascites , and encephalopathy
血血e島nner ,and creatinine , bilirubin , pro 血romb 面白ne,and cause of cirrhosis in the la仕er).
Interes 曲19ly ,AD品灯S13:AC signi :fi cantly decreased wi出世leprogression of liver dis 加rbance
m也e 7 LC patients with the sequenti a1 study. These patients were admitted to the hospi ta1 for a
second 由nebecause ofhepatic enceph a10pathy 血3patients , ascites au伊len 旬tion in 4 patients ,組d
variceal rupture in 1 patien t. We p四viously demonstrated that plasma ADAMTS13:AC was
remarkably low in LC patients with hepatic enc 叩ha1opath y, hepator 百la1 syndrome and re企actory
出cites 29. Amultivariate ana1ysis identi 宣edblood anlffioni a, serum creatinine and spleen volume 出
independent 白ctors 伽 tcon 仕ibute to 也edecrease in AD. 品,1TSI3:AC ,indica 曲19 也at
ADAMTSI3:AC is closely related to the severity ofhepatic enceph a1opath y, renal dysfunction and
splenomegaly in LC patients29• These selected parameters ぽeintimately related to 白.ct ors 也at
comprise 血eCτP score or 由eMELD score and predict 吐le prognosis of cirrhotic patients.
Alternatively ,由eAD 品,1TS13:AC w回 lower in 3 Child B and 3 Child C LC patients wi出抑制
thrombosis 也an those wi吐10ut ,but further studies will be needed to elucidate the signi :fi cance of
lower ADAMTS13:AC associated wi血 portal 吐lfO mbus fonnation 企om 也epoint of decreased
白nctionalliver capacity in more LC patients with portal 世lfombosis.
The Japan Society of Hepatology , Tokyo , Japan
Hepatology Research
A Takaya , et al. ADAMTS 13 and prognosis of liver cirrhosis 11
The levels ofVWF:Ag ,血esubs 仕ate of ADAMTSI3 , progressively increased 白血e:fun ctional
liver capacity decreased , probably due to也eneocapilarization of hepatic endothelial cells 由atleads
to liver fibrosis , increased endothelial production induced by endotoxin 21,45 and/or increased
S戸thesis byex 回hepatic endothelial cells 46. VWF:RCo relativeωADAMTS13:AC increased 出
chronic liv ,ぽ disease progressed , and VWF multimers appear 吋加 shi 貴企om a degraded- to
normal 圃,VWFM and 血lally to UL- VWFM 節也e:fun ctional liver capacity and renal :fun ction
deteriorated , indicating 也at advanc 吋 cinhosis may predispose patients to platelet micro 仕rrombi
form 副on29.百lemarked impairment in由een司直le旬 subs 回ieratio , i.e. , decre 出edADAMTS13
to increased VWF:Ag , may lead to platelet hyperaggregability and subsequent microcirculatory
disturbances not only 面白eliver but also in oth ぽ O屯叩s,leading to multi-organ 血ilUI ・e. Indeed ,
portal or hepatic vein 由rombosis is 0宜enobserved in advanced LC patients routinely screened wi血
Doppler ul回sound 8,and in cirrhotic liver tissue removed at 仕組splantatio J>. Moreover ,
microthrombi were found in one or more 0騨 sin half of cirrhotic livers at autopsy lO.
Plasma ADAMTS13:AC may decrease in advanced 伽 hosis due to reduced AD品t1 TS13
pro 山ction in HSCS 47, enhanced consumption to de,伊de1訂gequant 耐田 ofVWF:Ai 6,and/or its
plasma inhibiωIr 15,16. We detected plasma ADAMTS13:INH in 83% of P副ents with a severe 加
moderate ADAMTSI3:AC deficiency , but the AD品汀S13 i曲ibi 加ryactivity Wi制面白emarginal
zone between 0.5 and 1.0 BU/ml in most c田町依田ptone TTP patientο.0 BU/mli 3 and one patient
M血 asevere AD刷 TS13:AC deficiency (3.0 BU/mlf9. We could d制 IgG 圃type
autoantibodies in 5 end-stage cirrhotic patients with a seve 問 ADAMTS13:AC de宣ciency
(く3%f9. 臼le patient had charact 出stic clinical features of TTP. However , the rlαnaining 4
patients did not show any apparent clinical features of TτP, but were indistinguishable 量。m也e
typical 百Ppatient based on AD品t1 TS13:AC and thepresence ofanti-ADAMTS13 autoantibodies.
百lese results indicate that some end-stage cirrhotic patients wi也extremely low ADAMTS 13:AC
and the IgG ADAMTS 13 inhibitor might have a condition similar to TTP or have “subclinical" TTP.
Together wi由 our p問sent results , these findings suggest 也at 也edegree of decrease in plasma
ADAMTS13:AC may be a useful predictor 由at is closely related 白白epa血ogen 回is of hepatic
血ilure ,including encephalopathy and/or renal dis 加rbance ,in patients with advanced LC.
The Japan Society of Hepatology , Tokyo , Japan
Page 12 of 23
Page 13 of 23 Hepatology Research
A Takaya , et al. ADAMTS13 and prognosis ofliver cirrhosis 12
Altematively , various c面白al∞nditions ,including infection , malignancies ,叩dcertain 世ugs ,
C組 lead to a叫uired 百p4 8. In addition , some p飢ien 白川世1congenital 百P油田e
ADAMTSI3:AC is extremely low (<0.5%) due to mutations in theAD AMr S13 gene showed no
appare 国 clinical fea 加res during 世間irchildhood except mild 旬 moderate 白rombocytope 叫aduring
s加 ssful ∞nditions such 出 infection ,but apparently developed “πP" during the 也凶制mester of
pregnancy when VWF production 企'O mpla ∞:n tal endothelial ∞l1 s markedly increas 回49. 百lI s
condition is called “m出queraded TIP in congenital Upsha w-Schulman 明批ome". Furthermore ,
recently , sepsis 圃induced multi-organ failure was shown to be closely related to the decrease in
AD馴 TS13:AC and increase in VWF:Ag50• This 血lding indicates 制 the 四 yme to subs 回Ite
ratio is ex仕'emely impo 蜘 1t in 血eformation of pla 印刷 microthrombi and subsequent
microcirculatory disturbances that lead to multi-organ failure. In advanced cirrhotics , endotoxemia
is frequently detec 旬d2I, and SBP sometimes occurs35• HCC becomes highly complicated 出白e
cirrhotic stage progresses 51, which suggests that these patients 訂eat high ri虫色rplatelet
microthrombi form 組on. 百1erefore ,LC patients wi吐1 a moderate ADAMTS13:AC deficiency
(3-25%) who have no apparent IgG ADAMTS13 inhibitor and whose inhibitory acti 吋tyis in the
marginal zone (0.5-1.0 BU/m りmay be especially prone to a poor ,ぽprognosis when infection and
endo 旬Ixemia to au伊1ent VWF production 企'O mendothelial cell precipitates , ultimately resulting in
由eshortest survival.
In summary , the plasma ADAMTS 13 :AC concomitantly dec 問ases 出血efunctional liver
capacity declines , and 由edegree of activity is closely rela 附加the prognosis of patie 臨 wi由LC.
Therefore , AD品,fT S13 activity may be a use 品1marker to predict the clinical ouぉome in advanced
cinhosis.
ACKNOWLEDGMENTS
百世swork w,出 suppor ぉdinp 紅tby Grants 田祖国Aid for Scien 甘fic Research from 世1e Japanese
Min istry ofEducation , C凶旬re,Sports , Science , and Technology (1¥征 J,YF) and from 吐1e乱伽is町of
Health and Welfare of Japan for Blood Coagulation Abnormalities σF). 百1e au也ors sincerely
出獄lkAyami Isonishi for her great help 出血C出say ofADAMTS13 activity and VWF antigen.
The Japan Society of Hepatology , Tokyo , Japan
Hepatology Research Page 14 of 23
A Takaya , et al. ADAMTS 13 and prognosis of liver ci汀hosis 13
REFERENCES
1. Durand F, ¥匂lla D. Assessment of prognosis of cirrhosis. Semin Liver Dis 2008; 28: 11 0-22.
2. Child CG, Turcotte JG. The liver and portal hypertension. In Child CI, ed. Surgery and
portalHypertension. Philadelphi a, USA: W.B. Saunders , 1964; 50・8.
3. Pugh RN, Murray 圃Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the
esophagus for bleeding oesophageal varices. Br J Surg 1973; 60:646-9.
4. Salemo F, Merli M, C但 za凶ga M, et al. MELD score is better 由姐 Child-Pugh s∞re in
predicting 3酬month survival of patients undergoing transjugular intr ,油epatic portosystemic shun t.
J Hepato12002; 36: 494 ・500.
5. Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predict survival in patients with
end-stage liver disease. Hepatology 2001; 33:464 剛70.
6. Yoo HY, Edwin D, Thuluvath PJ. Relationship ofthe model for end-stage liver disease (ME LD)
scale to hepatic encephalopathy , as defined by electroencephalography and neuropsychometric
testing , and ascites. Am J Gastroentero12003; 98: 1395-9.
7. Northup PG, S叩 daram V, Fallon 1¥侶, et al. Coagulation in Liver Disease Group.
Hypercoagulation and thrombophilia in liver disease. J百1f omb Haemost 2008; 6:2 幽9.
8. Amitrano L, Guardascione MAラBrancaccio V, et al. Risk factors and clinical presentation of portal
vein thrombosis in patients with liver cirrhosis. J Hepato12004; 40:736 ・41.
9. Wanless IR, Wong F, Blendis LM, Greig P, Heathcote EJ, Levy G. Hepatic and portal vein
thrombosis in cirrhosis: possible role in development of parenchymal extinction and portal
hypertension. Hepatology 1995; 21:1238 -47.
10. Oka K, Tanal 但K. Intravascular coagulation in autopsy cases wi出 liver diseases. Thr omb
Haemost 1979; 42:564-70.
11. Moake JL. Thr ombotic microangiopa 由ies. NEngl JMed 2002; 347:589 ・99.
12. F吋加lura Y, Matsumoto M, Yagi H, Yoshioka Aラ Matsui T,百tani K.油 nWillebrand
factor ・'-cleaving protease and Upshaw 圃Sch u1m ans 戸ldrome. Int J Hematol2002; 75:25 ・34.
13.LeηGG , Nichols WC, Lian EC, et al. Mutations in a member ofthe ADAMTS13 gene 白mily
cause thrombotic thrombocytopenic p山pura. Nature 2001; 413: 488 ・94.
The Japan Society of Hepatology , Tokyo , Japan
Page 15 of 23 Hepatology Research
A Takaya , et al. ADAMTS 13 and prognosis of liver cirrhosis 14
14. Kokame K, Matsumoto M, Soejima K, et al. Mutations and common poゆno中hisms in
ADAMTS 13 gene responsible for von Willebrand 血cto r-田 cleaving pr,叫ease activity. Proc Nat1
Acad Sci USA 2002; 99: 11902-7.
15. Furlan M, Robles R, Galbusera M, et al. von Willebrand factor-cleaving protease in thrombotic
thrombocytopenic pu叩ura 姐 dthe hemolytic-uremic syndrome. N Engl J Med 1998;
339:1578 開84.
16. Tsai HM, Lian EC. Antibodies to von Willebrand factor-cleaving protease in acute thrombotic
thrombocytopenic pu中ura. N Engl J Med 1998; 339:1585 ・94.
17. Uemura M, Tatsumi K, Matsumoto M, et al. Localization of ADAMTS13 to由estellate cells of
human liver. Blood 2005; 106:922 -4.
18. Suzuki M, Murata M, Matsubara Y, et al. Det 怠ction of von Wi11 ebrand 血ctor-cleaving protease
(ADAMTS ・13) in human platelets. Biochem Biophys Res Commun 2004; 313:212 ・6.
19. 百lffier N, Nolasco L, Tao Z, Dong JF, Moake 1. Human endothelial cells syn 血esize and release
ADAMTS-13. J Thr omb Haemost 2006; 4:1396 ・404.
20. Manea M, Kristoffersson A, Schneppenheim Rラetal. Podocytes express ADAMTS 13 in normal
renal ∞rtex and in patients with thrombotic thrombocytopenic pu中ura. Br J Haemato12007;
138:651 嗣62.
21. Ferro D, Quintarelli C, Lattuada A, et al.回出 plasma levels of von Willebrand 白ctor 出 a
marker of endothelial per 加rbation in cirrhosis: relationship to endotoxemia. Hepatology
1996; 23:1377 ・83.
22. Albornoz L, Alvarez D, Otaso JC, et al.丸 TonWillebrand 白.c tor could be an index of endothelial
dys :fun ction in patie 国swl血 cirrhosis: relationship to degree of liver 白ilure and nitric oxide
levels. J Hepatoll999; 30:45 ト5.
23. Aster RH. Pooling of platelets 副社le spleen: role in the pathogenesis of “hypersplenic"
由rombocytopenia. J Clin Invest 1966; 45:645 ・57.
24. Peck-Radosavljevic M, Wichlas M, Zacherl J, et al. Thr ombopoietin induces rapid resolution of
thrombocytopenia after orthotopic liver 回nspl 組 tation 伽 ough increased platelet production.
Blood 2000; 95: 795 剛801.
The Japan Society of Hepatology , Tokyo , Japan
Hepatology Research Page 16 of 23
A Takaya , et al. ADAMTS 13 and prognosis of liver cirrhosis 15
25.Schh 宜ski P, Tacke F, Trautwein C, et al. Thro mbopoietin s町umlevels are elevated in patients
hepatitis B/C infection compared to other caus 回 of chronic liver diseases. Liver 2002;
22:114 ・20.
26. Mannucci PM, Canciani MT, Forza 1, Lussana F, La伽 ada A, Rossi E. Changes in health and
disease of血eme 匂1l 0proteinase 也atcleaves von Willebrand 白.ctor. Blood2001; 98:2730 ・1
27. Feys HB, Canciani MT, Peyvandi F, Dec 加1戸1H, Vanhoorelbeke K, Mannucci PM.
ADAMTS13 acti 吋tyto antigen ratio in physiological and pathological conditions associated
with an increased risk ofthrombosis. Br J Haemato12007; 138:534 -40.
28. Lisman T, Bongers 1N, Adelmeijer J, et al. Elev 蹴 dlevels of von Willebrand factor in cirrhosis
support platelet adhesion despite 問duced functional c叩acity. Hepa 加logy 2006; 44:53 田61.
29. Uem 町aM,F吋加1U ra Y, Matsumoto M, et al. Comprehensive 佃 alysis of ADAMTS13 in
patients wi血liv ぽ cirrhosis. Thro mbHaemost2008; 99:1019-29.
30. Park YD, Yoshioka A, Kawa K, et al. Impair 吋 activity of plasma von Willebrand
白c旬if-clea 吋ngprote 邸 emay predict 血eoccurrence ofhepatic veno ・occlusive disease after stem
cell transplantation. Bone Marrow Transplant 2002; 29:789 ・94.
31. U回1U raM, Matsuyama T, Ishikawa M, et al. Decreased Activity of pl部maADAMTS13 may
con 仕ibute to 由edevelopment of liver disturban ∞and multiorgan 晶ilure in patients with
al∞holic hepatitis. A1cohol Clin Exp Res 2005; 29: 264S ・71S.
32. Ko S, Okano E, Kan ehiro H, et al. Plasma ADAMTS13 activity may predict early adverse
events in living donor liver transplantation: obs 町vations in 3 c回目. Liver Tran 甲12006; 12:
859 ・69.
33. YagitaM , UemuraM , N北佃lura T, Kunitomi A, Matsumoto M, Fujimura Y Development of
AD品.rr S-13 inhibitor in a patient wi血 hepatitis C virus 叩 lated liver cirrhosis ca山田
由rombotic 血rombocytope 凶cpu 中ma. JHepa 加12005; 42:420 ・1.
34. Henderson 品,1, Heymsfield SB, Horowitz J, Kutner :t¥柾I. Measurement of liver and spleen
volumeby ∞mputed tomography. Radiology 1981; 141:525 圃7.
The Japan Society of Hepatology , Tokyo , Japan
Page 17 of23 Hepatology Research
A Takaya , et al. ADAMTS 13 and prognosis of liver cirrhosis 16
35. Arr oyo V, G加PERL ,Gerbes AL, et a1. Definition and diagnostic criteria of refractory ascites
加 dhepatoren a1 syndrome in cirrhosis. Intemational ascites club. Hepatology 1996; 23:
164-76.
36. Japanese Research Society for Portal Hypertension. 百le genα ョ1rules for recording
endoscopic 血ldings on esophage a1 varices. Jpn J Surg 1980; 10:329-37.
37. Trey C, Bums DG, and Saunders SJ. Treatment of hepatic coma by exchange blood
trans 血sion. N Engl J Med 1966; 274:473 幽81.
38. Kudo M, Chung H, H司i S, et a1. ぬlidation of a new prognostic 由回ng s戸tem for
hepatocellular carcinoma: the JIS score compared with the CLIP sco 問. Hepatology 2004;
40:1396-1405.
39. Mori Y, Wada H, Gabazza EC, et a1.昨 edicting response to plasma exchange in patients wi也
世rrombotic 由romboc 戸openic pu中ma wi世1me出urement of vWF-cleaving prote 部eactivity.
Transfusion 2002; 42: 572-80.
40. Furlan 悶 Robles R, Solen 吐la1erM, Wassmer M, Sandoz P, Lammle B. Deficiency activity of
von Wi11 ebrand 血ctor-cleaving protease in chronic relapsing thrombotic 白rombocytopenic
purpura. Blood 1997; 89:3097 ・103.
41. Kato S, Matsumoto M, Matsuyama T, Isonishi A,団ura H,町並lura Y Novel monoclon a1
antibody-based e回 yme 加盟1unO 出say for detemlinig pl出ma levels of AD品,ff S13 activity.
Transfusion 2006; 46:1444 圃52.
42. Mac 白rlane DE, Stibbe J, K主by Ep, Zucker l¥侶, Grant RA, McPherson J. A method for
assaying von Willebrand 白ctor( 由加cetin co晶ctor). Thr omb Diath Haemorrh 1975; 34:306 ・8.
43. Warren CM, Krz図面 ski PR, Greas ぽ ML.Ve 耐ca1agarose gel electrophoresis and elec 加 blo 性同
ofhigl トmol ∞叫ar-wei glI tproteins. Electrophoresis 2003; 24: 1695 圃1702.
44. Kasper CK, A1edort L, Aronson D, et a1. Amore uniform me制 rement of factor VIII inhibitors.
Thro mb Diath Haemorrh 1975; 34:869 ・72.
45. Schorer AE, Moldow CF, Rick ME. Interleukin 1 or endotoxin mcreases the release of von
Willebrand factor from human endo 帥 lia1cells. Brit J Haemaω11987; 67:193-7.
The Japan Society of Hepatology ,γokyo ,Japan
Hepatology Research Page 18 of 23
A Tak: aya , et al. ADAMTS13 and prognosis ofliver cirrhosis 17
46. Tomai 1, 1面3白l吋J,Boda Z, Udvardy M, Ptliegler G, Rak K. Endothelium releases more von
Willebrand 恥tor and tissue 吻pe plasmionogen activator upon venous occlusion in patients
with liver cirrhosis than in normals. Haemos 回.is 1993; 23: 58圃64.
47. Kume Y, Ikeda H, Inoue M, et al. Hepatic s旬llate cell damage may lead to decreased plasma
ADAMTS 13 activity in rats. FEBS Lett. 2007; 581: 1631 圃4.
48. Matsumoto M, Yagi H, Ishiz 出hiH, Wada H, F吋imura Y.百 leJapanese 既perience with
thrombotic 也rombocytope 凶cpu 中ura-hemolytic ul芯mic syndrome. Semin Hemato12004;
41:68 ・74.
49.F 吋加1町aY, Matsumoto M, Kokame K, et al. Pregnancy-induωd 也rombocytopenia and T四,
and 也eriskof たtal dea 出,in Upshaw-Schulman syndrome: a series of 15 pregnancies in 9
genotyped patients. Br J Haemato12009; 144:742 圃54.
50. Claus RA, Bockmeyer CL, Budde U, et al. Variations in the ratio between von Willebrand factor
and its cleaving prote 出e d山恒gsystemic intlantmation and association wi也 severity and
prognosis of organ 血il田右.百lfO mbHaemost 2009; 101 :239 -47.
51. Sala M, Fomer A, Varela M, Bruix 1. Prognostic prediction 担 patie 臨 wi白 hepatocellular
伺rcinoma. Semin Liver Dis 2005; 25: 171 ・80.
The Japan Society of Hepatology , Tokyo , Japan
page 19 of23 Hepatology Research
A Takaya , et al. ADAMTS13 and prognosis ofliver cirrhosis 18
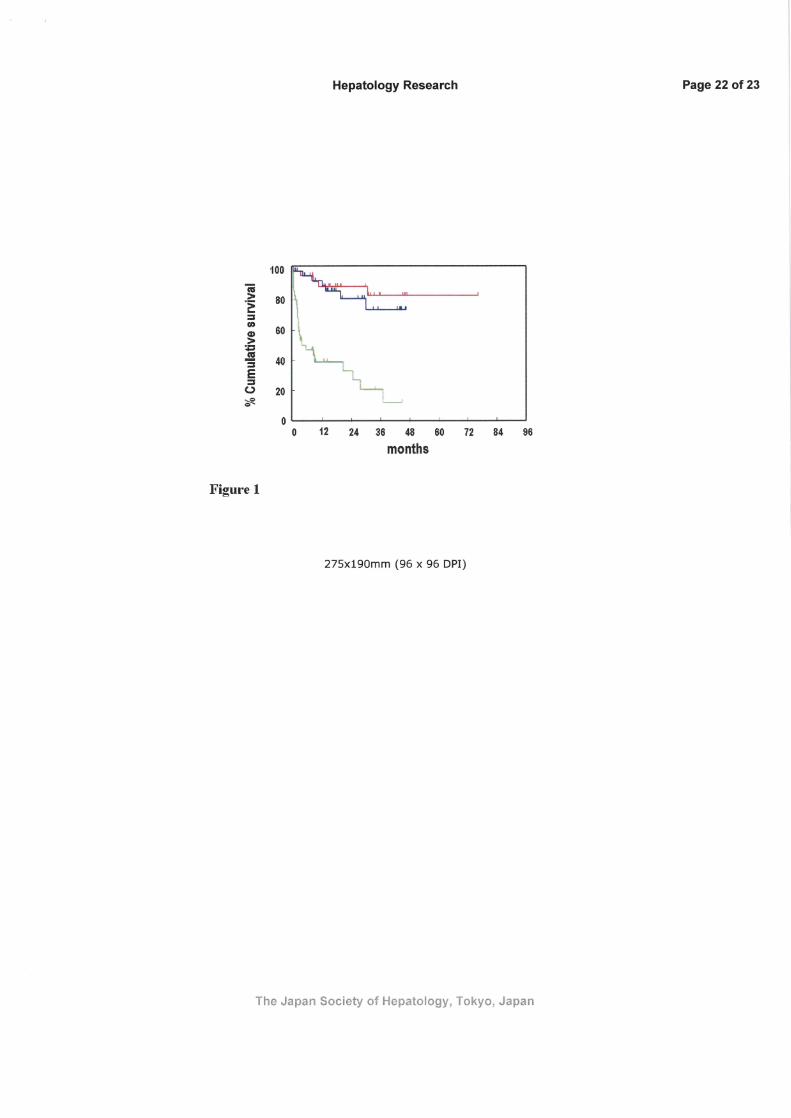
Figure legends
Figu四 1 Cumulative survival rate of 108 patients with liver cirrhosis according to 也eChild
classi :fi cation. Child C patients had worse survival 由組 Child A and B patients , but the survival
probabilities were not di宜erent between Child A and Child B patients (Log rank test among 也et加国
groups , p<O.OOOl; Child C vs. Child A, p<O.OOOl; Child C vs. Child B, p<O.OOOl).τhe red , blue ,
and green lines indicate cirrhotic patients wi也Child A, Child B, and Chi1d C, respectively.
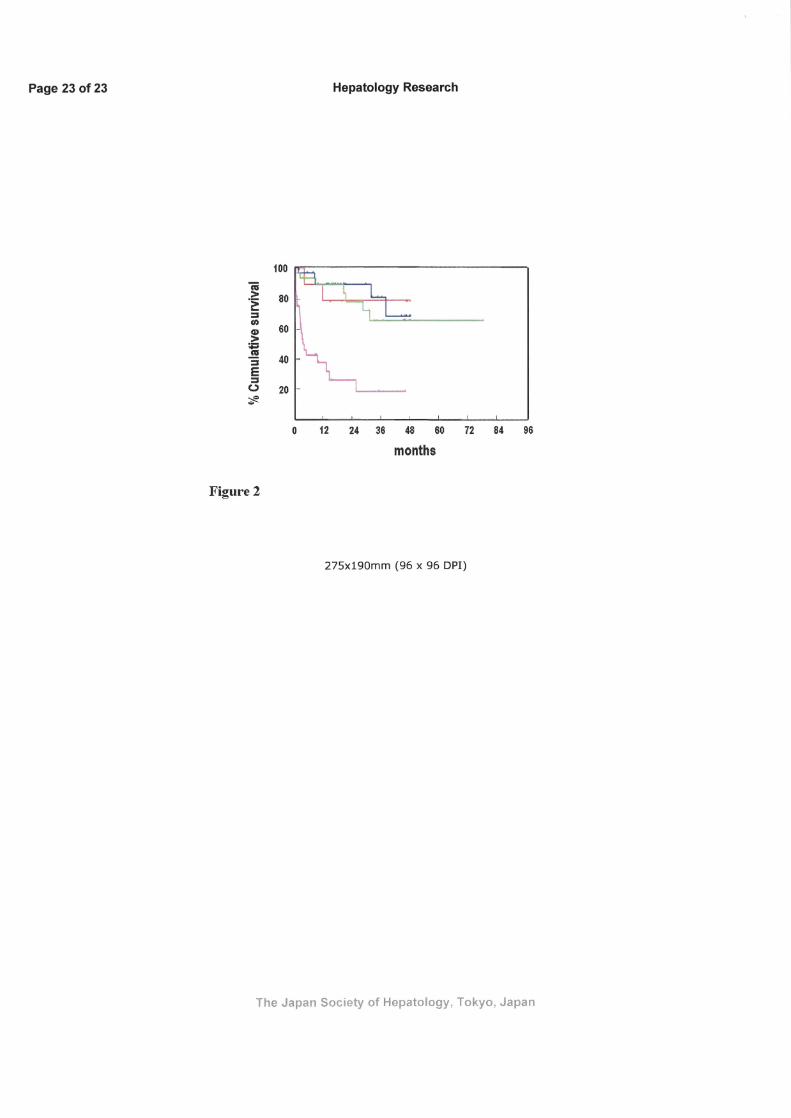
日伊問2 Cum u1ative survival rate of 108 patients wi血liver cirrhosis according to the Model 品r
End 圃Stage Liver Disease (ME LD) score. 百le s町vival of patients corresponding 加出e島町出
quartile of吐leMELD risk score (RS) calculated by也eform 叫a5was worse 白組曲at of patients
corresponding 旬世le 曲"5 t由ree RS quartiles , while 社le survival of the patients in the :fir st由reeRS
quartiles did not diffi 町 among them (lρgra 叫ctest among 由efour groups , p<O.OOOl; 白山由quartile
vs.o 血ers ,pく0.0001). 百lered , blue , grl 悶 1,加dpink lines indicate cirrhotic patients wi由自rst RS
q田氏ile ,second RS quartile ,出ird RS quartile ,組dfourth RS qu釘幽e,respectively.
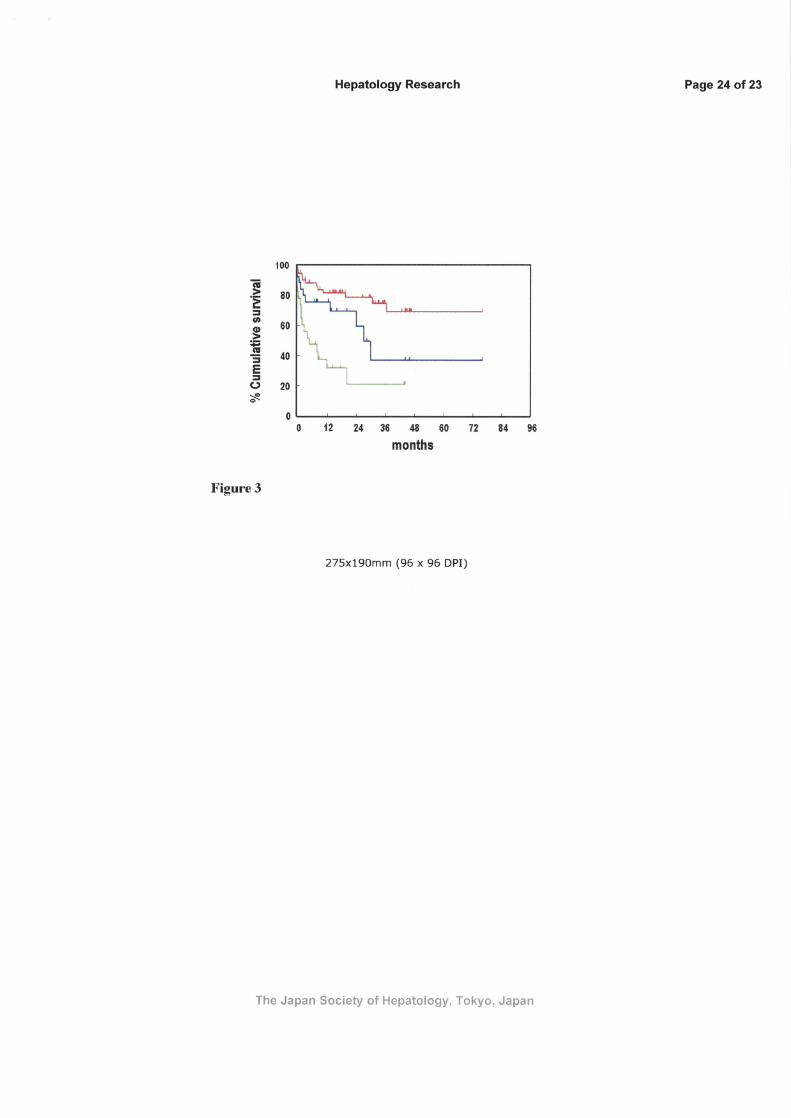
Figure 3 Cumulative survival rate of 108 patients with liver cirrhosis according to ADAMTS 13
acti 吋ザ (AD 品r1 TS13 :AC). 百le survival 則 .ew 出 clearly differentiated among patients wi也 a
seve 問 to moderate ADAMTS 13:AC de:fi ciency , mild ADAMTS 13:AC de:fi ciency , and normal
range of ADAMTS13: AC (lρg rank test among 世1e血ree groups , p<O.OOOI; severe to mod ぽate
de:fi ciency vs. mild deficiency , p=0.0219; mild de:fi ciency vs. normal range , p=0.0287; severe to
moderate deficiency vs. normal r加 ge,p<O.OOOI). 百lemedian survival time was 由elowest (4.5
months) in cirrhotic patients wi血asevere to moderate ADAMTS13:AC de:fi ciency. 百lered , blue ,
and green lines indicate cirrhotic patie 臨 with normal range of ADAMTS13 :AC (> 50%) , mild
ADAMTS13:AC de:fi ciency (25-50% of 吐le normal control) , a sev 関白 moderate
ADAMTS13:AC de:fi ciency (<2 5% of吐lenormal contro り,respectively.
The Japan Society of Hepatology , Tokyo , Japan
Page 20 of23
Hepatology Research
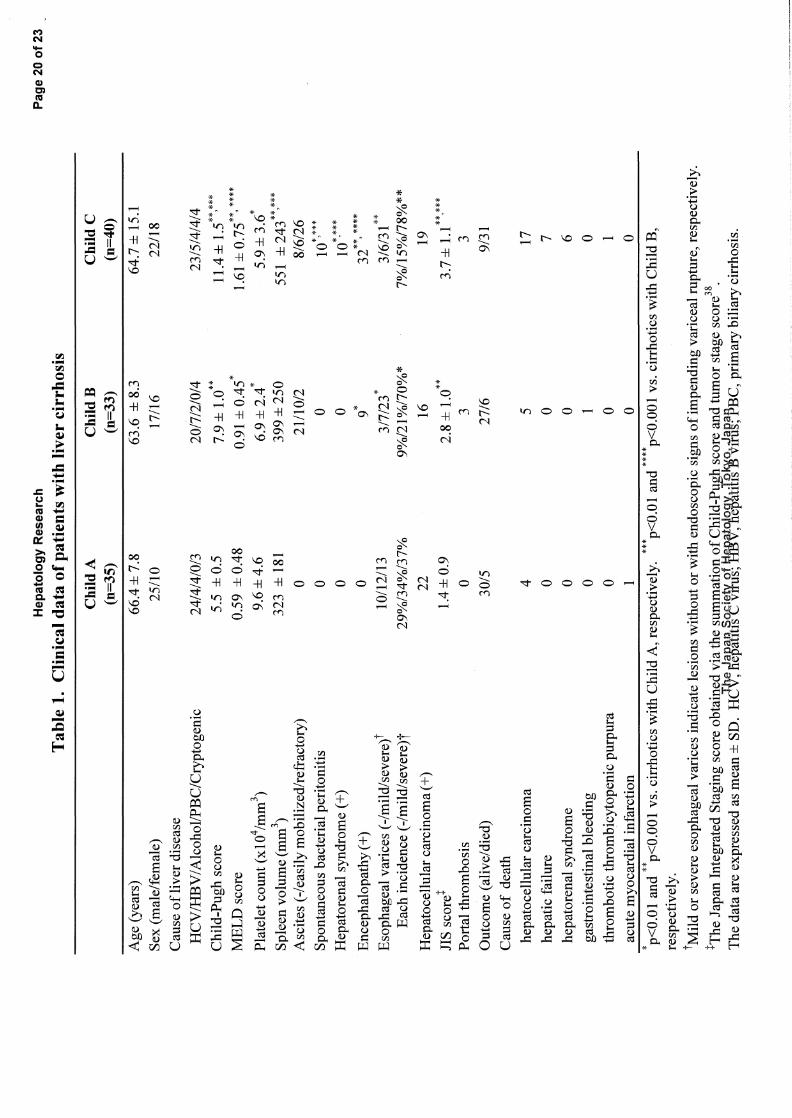
Table 1. Clinical
data of patients
with liver
cirrhosis
Child C
(n=40)
Child B
(n=33)
ChildA (n=35)
64.7土15.1
22/18
63.6士8.3
17/16
66.4土7.8
25/10
Platelet count
(x104 /mm3 )
Spleen volume
(mm3 )
Ascites (-/easily
mobi1ized/refractory)
Spontaneous bacterial
peritonitis
Hepator・enal
s戸ldrome
(+)
Encephalopathy (+)
Esophageal varices
(・/mil
d/severe)
t
Each incidence
(ー/mil
d/severe
)t
Hepatocellular伺rcinoma(+)
JIS score
t
Portal thrombosis
Outcome (alive/died)
Cause of death
hepatocellular carcinoma
hepatic failure
hepatorenal s 戸1曲。me
gastrointestinal bleeding
thrombotic thrombicytopenic
pu中町a
a.cutemyoc訂dialinfarction
1
*p<0.0land紳p<O.OOI
vs. cirrhotics
with Child
A, respectively.
料*p<OMmd
材料p<O.OOI
vs. cirrhotics
wi由Child
B,
respectively.
tMild or severe
esophageal varices
indicate lesions
without or with
endoscopic signs
of impending
variceal rup同re,respectively.
t The Japan
Integrated
Staging score
obtaiI!cd v.ia the
~llIl1
Il).ati
91J.ofÇhjld-Pl
!,gq sc
or~ and tumor
stage sc町e38.
Thed制的低pres
田d出mean
土SD.
HC寺?部諮
t紙幣品1憎軒瀧積:t
i儲%鵡押BC,prim
町bili町ci曲osis.23/5/4/4/4 11.4士1.
51.61土0.75
紳,紳紳
5.9土3.6
傘
551土243
8/6/26
10 '
10司
32*,
20/7/2/0/4
7.9土1.0
0.91土0.45*
6.9土2.4*
399士250
21/10/2 0 0 9
24/4/4/0/3
5.5土0.5
0.59土0.48
9.6土4.6
323土181 。
Age (years)
Sex (male/female)
Cause of liver
disease
HCV IHBV / Alcoho
llPBC/Cryptogenic
Child-Pugh score
恥1ELDscore
。 。3/6/31
紳
7%/15%
/78%**
19
3.7::l: 1.1**'*
紳
3
9/31
ロ 7601 。
3/7/23*
9%/21 %/70%*
16
2.8士1.0
3
27/6
ZJnunu'IAU
。
。10/12/13
29%/34%/37%
22
1.4土0.9
0
30/5
。4 。 。 。
Page 21 of23
Hepatology Research
Table
2. Plasma
values of ADAMTS13
activity and its related
parameters
Variable
ADAMTS13:AC
(%)れ司
IFMassay)
ADAMTS13:AC
(%)(ELISA)
VWF:Ag(%)
VWF:RCo
(%)
VWF:RCo
/VWF
:Ag ratio
VWF:RCo/ADAMTS13
ratio
VWFM pattems
t
( degraded/normaVunusually
圃large)
Inhibitor against
ADAお1TS13
↑
(n町nb町ofpositive
cases)
ChildA (n=35) 79土25
材
80士24
紳
320土174
材
186土137*
0.63土0.49
1.6土1.7肺
2/0/0
Liver cirrhosis Child B
Child C
(n=33) (n=40)
63 :f: 34料開
3土3
1 :f: 22材料材料材料
3土2
牢牢申事牢
キキ百ドキ申ヨドキキ申*申*
65士31
40土22
436土267
紳y林
486土254
特,紳柿
198士172
事227
土187
0.50土0.46紳
0.51土0.40キ
*
5.0士5.7
材戸*
16.8土28.2
事寧寧申申申*申申事
8***/5問/0
6/20'問*材料/8*紳*
9 19問*
healthy subjecfs
(n=60) 102土23
99土22
100土53
100土15
1.1士0.42
0.9士0.2
absent
宇pく0.05
and柿p<O.OOI
vs. healthy
subjects, respectively.
判事pく0.05,and
*帥*p<O.OOI
vs. cirrhotics
with Chi1d A, respectively.
材開p<0.05
and閉山p<O.OOI
vs. cirrhotics
with Child
B, respectively.
tTheVWFMpa
仕emsand ADAMTS
13 inhibitor
were analyzed
in 49 c註rhotic
patients with
lower ADAMTS
13 :AC (1ess than
50% ofthe
normal control).
The data
町e ex:pressed
as mean
土SD.
ADAMTS13:AC
, ADAMTS13
activity; VWF:Ag
, von Wi11ebrand
晶.ctor
antigen;
VWF:RCo
, von Willebrand
晶ctorristocetin
cofactor activity;
VWFM
, von Wi11ebrand
晶ctormultmer
, ELIS
A, En勾喧le-Link:ed
ImmunoSorbent Assay
The Japan
Society of Hepatology
, Tokyo, Japan
Hepatology Research Page 22 of 23
100
何〉E 80
ヨrn
60 -s@ 〉帽=
:|ヘ」し= ts E J 、、,¥ ,.、
。。12 24 36 48 60 72 84 96
months
Figure 1
275x190mm (96 x 96 DPI)
The Japan Society of Hepatology , Tokyo , Japan
Page 23 of 23 Hepatology Research
100
コ帥
3。〉eコ= 冒60
tE 2 JE
~
o 12 24 36 48 60 72 84 96
months
Figure 2
275x190mm (96 x 96 DPI)
The Japan Society of Hepatology , Tokyo , Japan
Hepatology Research Page 24 of 23
100
80
2 的
60
苫。>偲= 40 2
ε ::J (.) 20 、』d52
。。12 24 36 48 60 72 84 96
months
Figure 3
275x190mm (96 x 96 DPI)
The Japan Society of Hepatology , Tokyo , Japan