valor diagnóstico do achado endoscópico “mucosa nacarada...
TRANSCRIPT
PROGRAMA DE PÓSPROGRAMA DE PÓSPROGRAMA DE PÓSPROGRAMA DE PÓS----GRADUAÇÃO EM CIENCIAS MEDICAS GRADUAÇÃO EM CIENCIAS MEDICAS GRADUAÇÃO EM CIENCIAS MEDICAS GRADUAÇÃO EM CIENCIAS MEDICAS
Dissertação de Mestrado
Valor Diagnóstico do Achado Endoscópico “Mucosa Nacarada” na Esofagite de
Refluxo
Autor: José Salomão JR. Orientador: Júlio C. Pereira Lima Co-orientador: Raul Mendoza Sassi.
Dissertação de Mestrado
Biblioteca Paulo Lacerda de Azevedo
Ano 2007
Diagnóstico

Livros Grátis
http://www.livrosgratis.com.br
Milhares de livros grátis para download.
AGRADECIMENTOS Tivemos o privilégio de trabalhar durante este período de mestrado com a equipe
de pós-graduação da Fundação Faculdade Federal de Ciências Médicas de Porto Alegre
aonde somamos verdadeiro aprendizado e conhecimento.
Agradeço ao orientador, co-orientador e todos os colaboradores pela paciência,
oportunidade, credibilidade e aprendizado.
Por fim agradeço e dedico aos pacientes que além de seus problemas de saúde
ainda se disponibilizaram a participar deste projeto de pesquisa.
3
SUMÁRIO
1 INTRODUÇÃO........................................................................................................... 4
1.1 REFERÊNCIAS.................................................................................................... 12
2 ARTIGO CIENTÍFICO............................................................................................ 14
2.1 ABSTRACT ……………………………..........………………………………... 15
2.2 INTRODUCTION................................................................................................. 16
2.3 MATERIAL AND METHODS............................................................................. 17
2.3.1 Type of study and sampling.......................................................................…. 17
2.3.2 Patients............................................................................................................ 17
2.3.3 Instruments and definition of variables......................................................… 18
2.3.4 Data analysis................................................................................................... 19
2.3.5 Ethical aspects................................................................................................ 20
2.4 RESULTS……….................................................................................................. 20
2.5 DISCUSSION ....................................................................................................... 25
2.6 ACKNOWLEDGEMENTS................................................................................... 28
2.7 REFERENCES...................................................................................................... 29
ANEXOS
4
1. INTRODUÇÃO
A endoscopia digestiva alta é o procedimento de primeira escolha para o
diagnóstico de afecções do trato digestório superior. Através deste procedimento
consegue-se estabelecer uma correlação entre sintomas dos pacientes e achados
endoscópicos. Nem sempre esta correlação é bem estabelecida. Por exemplo, a esofagite
erosiva achado comum na Doença do Refluxo Gastroesofágico (DRGE) está presente
apenas na metade dos pacientes com esta afecção. A grande questão é que as
classificações endoscópicas para esofagite contemplam apenas a partir de erosões, não
incluindo pequenas alterações macroscópicas. Um achado comum durante o
procedimento endoscópico é o desaparecimento do padrão vascular e a substituição por
uma mucosa esbranquiçada próxima a transição esofagogástrica, que denominamos de
mucosa nacarada.
Em revisão da literatura os trabalhos relacionados a achados endoscópicos
mínimos de esofagite são poucos e não estabeleceram os verdadeiros valores destas
pequenas alterações. Trabalho na década de 80 valoriza este achado, mas não estabelece
a verdadeira acurácia deste teste, e os atuais estão relacionados às novas tecnologias,
como magnificação de imagem, imagem digital e imunohistoquímica.
Justificamos a realização deste trabalho, para validar o valor diagnóstico do
achado endoscópico mucosa nacarada, como critério de esofagite macroscópica.
Comparando em um grupo de pacientes com mucosa nacarada e outro sem mucosa
nacarada, a presença de alterações microscópicas ou histológicas (padrão ouro)
sugestivas de esofagite microscópica.
Várias são as classificações existentes para esofagite de refluxo, a mais
tradicional é a de Savary-Miller, desde 1977, que apresenta quatro níveis de graduação e
se baseia na extensão das erosões da mucosa, sem valorizar alterações mínimas. Na
tentativa de se aproximar da classificação ideal em 1994 um grupo financiado pela
Organização Mundial de Gastroenterologia propôs a classificação de Los Angeles, que
recebeu este nome por ter sido apresentada no Congresso Mundial, na cidade de Los
Angeles. Nesta nova classificação os termos erosão e ulceração foram substituídos por
“quebra de mucosa” como também as complicações relacionadas à DRGE, como Barret
e estenoses, que deveriam ser citadas separadamente. Nenhumas destas duas
classificações contemplam pequenas alterações endoscópicas, como mucosa nacarada.
Talvez este aspecto nos leve a números tão baixos de sensibilidade global nas
5
endoscopias digestivas altas para DRGE, em torno de 40 a 60%. Quando considerado a
presença de erosões as endoscopias diagnósticas apresentam especificidade de 95% para
o diagnóstico de DRGE (10).
Quando pensamos em utilizarmos a biópsia para aumentar a sensibilidade do
teste, endoscopia digestiva na DRGE, e por fim a qualquer dúvida diagnóstica
encontramos na literatura o trabalho clássico de ISMAIL-BEIJI que determina os
achados histológicos de esofagite de refluxo. Trabalho que foi realizado através da
sucção da mucosa esofágica com auxílio da manometria. Determinaram-se os critérios
histológicos utilizando como parâmetros o espessamento da camada basal em 15% em
relação à espessura do epiltélio, a extensão das papilas até 2/3 da camada epitelial e a
presença de neutrófilos na lâmina própria. Em nosso estudo ainda acrescentou-se a
congestão vascular, a presença de neutrófilos e eosinófilos na camada epitelial
(exocitose) e a presença de glicogênio. Este último controverso em relação à presença
na esofagite, mas alguns autores consideram a sua presença, embora não esteja
estabelecido (3). WEINSTEIN e cols em trabalho publicado 1975 realizaram biópsia
por sucção em pacientes assintomáticos para doença de refluxo, e questionaram os
achados de ISMAIL-BEIJI. Pois encontraram alterações histológicas em 55% dos
pacientes biopsiados a 2,5cm distais e 19% dos biopsiados acima de 2,5cm. Mesmo com
este impasse os achados de ISMAIL-BEIJI permanecem até hoje como parâmetros
histológicos de DRGE.
Em trabalho nacional publicado no livro da Sociedade Brasileira de Endoscopia
(SOBED) em 1984 o professor CELSO AFFONSO DE OLIVEIRA já valorizava o
achado endoscópico mucosa nacarada e denominava de esofagite edematosa,
considerando como primeiro estádio da esofagite de refluxo e, nesta fase, a biópsia
indispensável. Analisou 147 casos de hérnia hiatal e avaliou as alterações histológicas
em indivíduos com mucosa nacarada e mucosa normal. Encontrou 57,1% de alterações
histológicas em mucosa nacarada e 32,5% de alterações em mucosa endoscopicamente
normal. Na época não se calculou a sensibilidade, especificidade, os valores preditivos,
a acurácia e o verdadeiro p destes dois achados. Parece que não houve grande diferença
nestes dois grupos.
KIESSLICH R. et al em trabalho publicado em 2004 com o objetivo de
estabelecer alterações mínimas vistas através de endoscopia com magnificação em
pacientes sem esofagite erosiva, correlacionou grupos de pacientes com sintomas e sem
sintomas de DRGE. Concluiu que nos pacientes com sintomas sem esofagite erosiva, a
6
combinação de alterações mínimas à magnificação e as alterações histológicas
apresentaram uma sensibilidade de 62%, especificidade de 74%, valor preditivo positivo
67%, valor preditivo negativo de 67% com acurácia global de 68%. Apresentando um p
significativo quando comparado com grupo controle. Embora o p significativo quando
em comparação entre os grupos, a acurácia do teste deixou a desejar.
FLORA-FILHO em trabalho publicado em 2000, em pacientes com sintomas de
refluxo, com o objetivo de reavaliar a sensibilidade da pHM-24h a partir de achados
histológicos compatíveis com esofagite, segundo os critérios de ISMAIL-BEIJI,
demonstrou uma sensibilidade de 60% para o método. Neste estudo também verificou
uma sensibilidade de 65,7% para as endoscopias quando considerado a presença de
erosões.
JOHNSSON F. publicou em 1987 trabalho com o objetivo de validar sintomas e
achados endoscópicos que confirmassem o diagnóstico de DRGE, comparando estes
achados com pHM 24h. Avaliou 220 pacientes, e no grupo de pacientes sem erosões
pela endoscopia (n=53), com alterações mínimas (eritema), encontrou uma sensibilidade
de 22%, especificidade 74% e valor preditivo de 43%. Quando avaliou o grupo de
pacientes com hérnia hiatal para o diagnóstico de DRGE (n=138) teve uma
sensibilidade de 75%, especificidade de 49% e valor preditivo positivo de 57%.
VIETH M. and cols em trabalho publicado em 2004 estudou pacientes com
DRGE, com erosões e sem erosões à endoscopia, com objetivo de validar os achados
histológicos descritos na literatura. Realizou biópsia em todos os pacientes na linha Z e
2cm acima da linha de transição(Z). Os critérios histológicos estudados foram
hiperplasia de camada basal, projeção de papilas, infiltrados de neutrófilos, eosinófilos,
linfócitos, ectasia e congestão capilar, acantose glicogênica, presença de células em
balão e espongiose. Concluiu que os melhores parâmetros histológicos para o
diagnóstico de DRGE são hiperplasia da camada basal e projeção de papilas. Encontrou
um p < 0,001 quando comparou estes dois resultados nos grupos com erosões e sem
erosões, acrescentando a suas conclusões que quanto mais esofagite (erosões) à
endoscopia maior a sensibilidade e especificidade da biópsia.
PATRIZIA ZENTILIN and cols publicou em 2005 no American Journal of
Gastroenterology uma reavaliação do valor diagnóstico da histologia nos pacientes com
DRGE. Analisou 135 pacientes com sintomas de refluxo e endoscopias com erosões e
sem erosões e comparou com grupo controle de vinte pacientes sem sintomas e com
endoscopias normais. Usou como critério histológico necrose/erosão, infiltração
7
intraepitelial de eosinófilos e neutrófilos, hiperplasia da camada basal, projeção de
papilas e dilatação dos espaços intercelulares. Encontrou alterações histológicas em 100
de 119 pacientes com DRGE (84%) e 3 de 20 do grupo controle(15%), p<0,00001. Nos
pacientes com esofagite erosiva, segundo os critérios de Los Angeles, 96% tinham
alterações histológicas e nos pacientes sem esofagite erosiva, endoscopias normais ou
minimamente alteradas, 76% tinham alterações histológicas.
DAVID ARMSTRONG em publicação na revista Yale Journal of Biology and
Medicine-2000, artigo de revisão sobre avaliação endoscópica na DRGE considera a
endoscopia como a primeira escolha na investigação, mas não é o arbitro final para o
diagnóstico. Também considera o exame altamente especifico quando a presença de
erosões, mas de baixa sensibilidade. Refere que o papel da biópsia na DRGE continua
indefinido, exceto na suspeita de Barret, e alterações mínimas a endoscopia não devem
ser consideradas até o momento.
H. WORTH BOYCE em edital publicado na Gastrointestinal Endoscopy em
2002 questiona a endoscopia diagnóstica e as classificações para esofagite de refluxo.
Em meio a comentários a respeito das classificações existentes para esofagite conclui
que a endoscopia digestiva não é o arbitro final para o diagnóstico de DRGE, podendo o
paciente apresentar sintomas relacionados ao refluxo, endoscopia normal e às vezes
histologias alteradas ou mesmo normais. Considera que alterações mínimas a
endoscopia (ausência de erosões) não devam ser consideradas, mas acredita que a
biópsias nestes casos pode ser interessante para complementação diagnóstica. Por fim
considera as novas tecnologias agregadas à endoscopia, como magnificação de imagem
e uso de corantes, novas ferramentas para melhorarem os critérios diagnósticos em
endoscopia.
HATLEBAKK and BERSTAD publicaram em 1997 na revista Scand J
Gastroenterol um trabalho com o objetivo de determinar os achados endoscópicos que
tinham a melhor relação com a esofagite de refluxo. Para isto usaram a classificação
endoscópica de Berstad, que contempla a partir de linhas avermelhadas sem exsudato
fibrinoso(erosão) até erosões, como achado endoscópico de esofagite. Usou como
padrão ouro a pH-metria de 24hs. Encontrou como melhor parâmetro endoscópico de
esofagite endoscópica o exsudato fibrinoso brancacento e o tamanho das erosões, sendo
que nestes dois achados os pacientes apresentavam um período de refluxo a pH-metria
significativamente maior. Concluíram que apenas linhas avermelhadas, embora sem
exsudato e de qualquer tamanho, são marcadores de esofagite quando comparados a
8
controles normais e acreditam que a endoscopia isoladamente não reflete as alterações
teciduais.
RONNIE FASS em recente edital expõe algumas controvérsias em DRGE.
Nesta publicação relata que a DRGE inclui três grupos, os com DRGE sem erosões
(60%-70%), os com DRGE com erosões (20%-30%) e os com Barret (6%-10%). Refere
que os pacientes sem erosões podem ter pH-metria de 24hs normais em metade dos
casos, e também respondem pior ao tratamento com inibidores de bomba de prótons.
Este fato reforça a importância de estudos para melhorar a sensibilidade e especificidade
da endoscopia na DRGE.
Publicações de autores Japoneses, que utilizam à classificação de Los Angeles,
demonstraram que pacientes Japoneses com sintomas de DRGE, apenas 14,3% destes
apresentam endoscopias com esofagite erosiva. Consideram a classificação de Los
Angeles insuficiente para o Japão, e advoga a inclusão de alterações mínimas a
classificação de Los Angeles determinando os graus N e M. Também alguns autores
consideram as alterações histológicas clássicas, como dilatação capilar, projeção de
papilas, hiperplasia de camada basal e infiltração de células inflamatórias, pouco claras
nos pacientes com DRGE e endoscopias sem esofagite erosiva.
FUJITA M. and cols e NISHIYAMA and cols tem estudado, através de
imunohistoquímica, a expressão de proteínas do processo inflamatório em pacientes
com sintomas de DRGE e endoscopias sem erosões. Este estudo tem demonstrado que o
processo inicial é a infiltração de células inflamatórias na lámina própria, e sugerindo
que estas alterações não são observadas em critérios histológicos na fase inicial da
DRGE, onde as endoscopias são normais ou minimamente alteradas.
Os métodos diagnósticos presentes até o momento ainda apresentam acurácia
inadequados para o diagnósico de DRGE, embora a especificidade da endoscopia no
diagnóstico de esofagite de refluxo é alta (95%) quando presente a forma erosiva ela é
de baixa sensibilidade global. Acreditamos que as técnicas de magnificação de imagem
associado à histologia com imunohistoquímica vão auxiliar no diagnóstico de pequenas
alterações endoscópicas, aumentando a acurácia do teste.
9
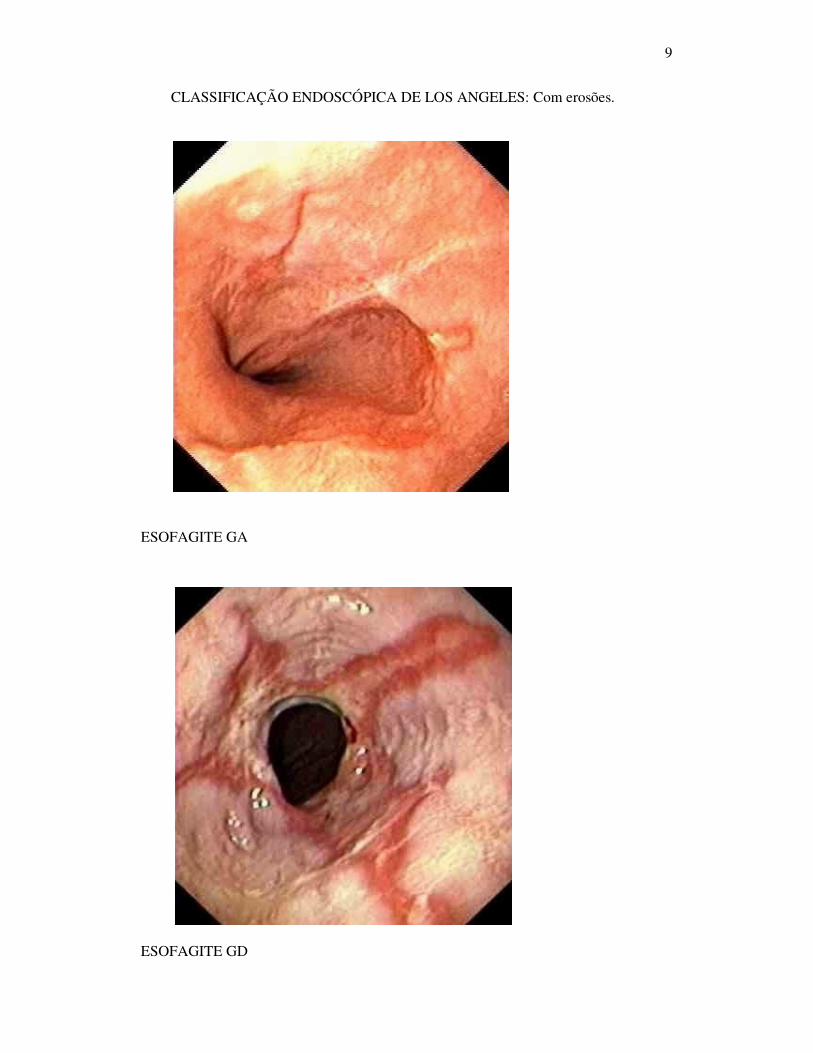
CLASSIFICAÇÃO ENDOSCÓPICA DE LOS ANGELES: Com erosões.
ESOFAGITE GA
ESOFAGITE GD
10
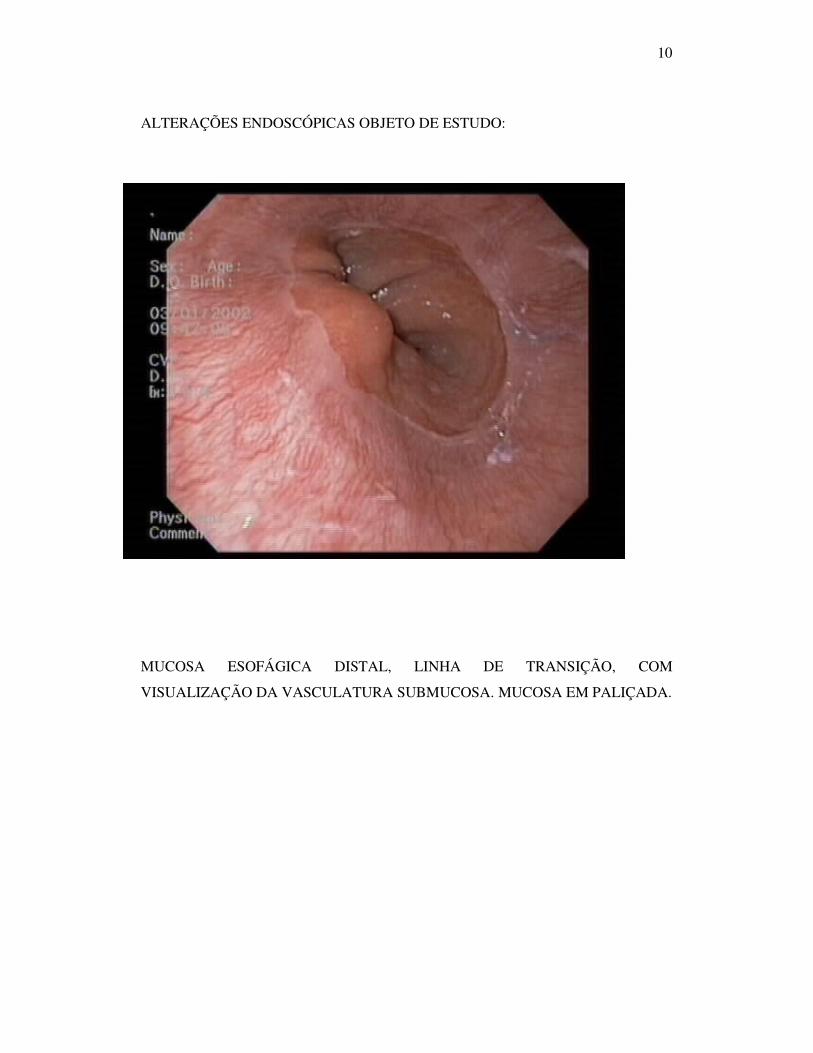
ALTERAÇÕES ENDOSCÓPICAS OBJETO DE ESTUDO:
MUCOSA ESOFÁGICA DISTAL, LINHA DE TRANSIÇÃO, COM
VISUALIZAÇÃO DA VASCULATURA SUBMUCOSA. MUCOSA EM PALIÇADA.
11
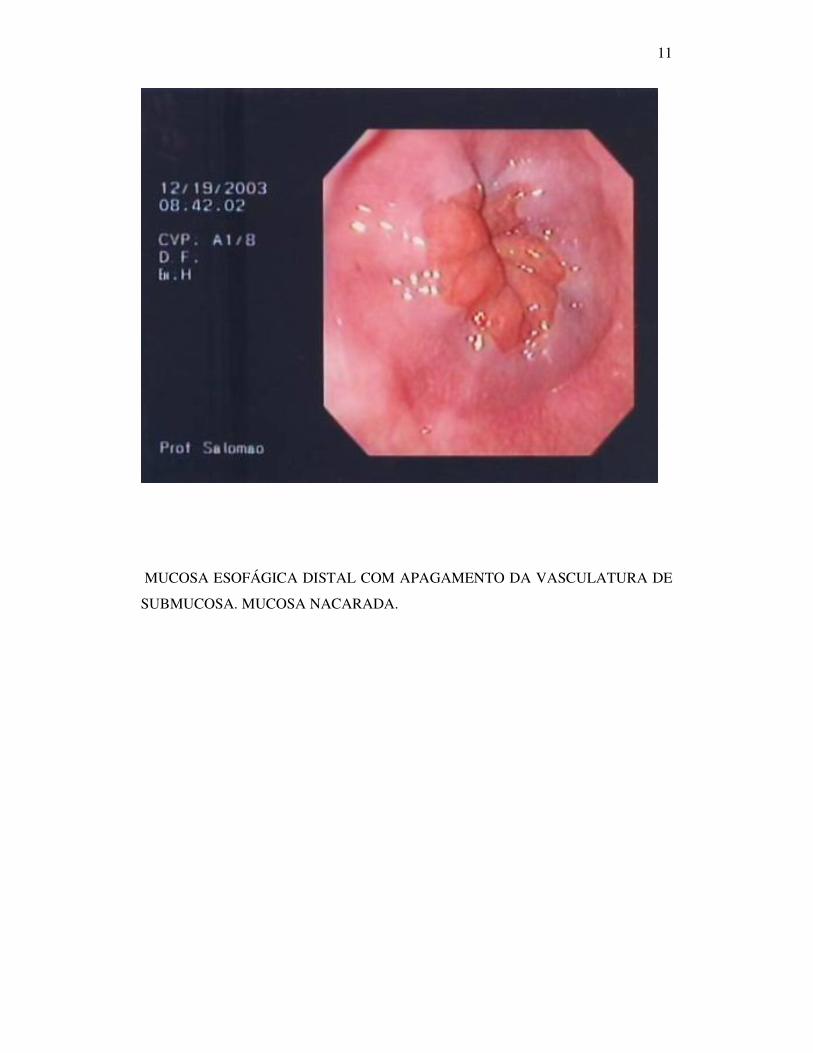
MUCOSA ESOFÁGICA DISTAL COM APAGAMENTO DA VASCULATURA DE
SUBMUCOSA. MUCOSA NACARADA.
12
1.2 REFERÊNCIAS BIBLIOGRÁFICAS. 1) AMANO Y, ISHIMURA N, FUTURA K. Interobserver agreement on classifying diagnoses of nonerosive esophagitis. Endoscopy, 38: 1032-5, oct. 2006. 2) ARMSTRONG D. Endoscopic Evaluation of Gastro-Esophageal Reflux Disease. Yale J Biol MED, 72: 93-100, 1999. 3) BOYCE HW. Endoscopic diagnosis and classification of reflux esophagitis: Are we there yet? Gastrointestinal Endoscopy, 56:775-778, 2002. 4) FASS RONIE. Doença do Refluxo Gastroesofágico: Questões e conceitos atuais. 5) FLORA-FILHO R, CÂMARA-LOPES LH, ZILBERSTEIN B. Critérios histológicos de esofagite na doença do refluxo gastroesofágico. Reavaliação da sensibilidade da pHmetria esofágica de 24hs. Arq. Gastroenterologia 37: 197-202, 2000. 6) GOLDMAN, H. Inflammatory Disorders of the Esophagus.Gastrointestinal mucosal biopsy.1996,p.11-49. 7) HATLEBAKK JG, BERSTAD A. Endoscopic Grading of Reflux Oesophagitis: What Observations Correlate with Gastro-Oesophageal Reflux? Scand J Gastroenterol 32: 760-65,1997. 8) ISMAIL-BEIGI F, HORTON PF, POPE II CE. Histological consequences of gastroesophageal reflux in man. Gastroenterology 58: 163-74, 1970. 9) JOHNSSON F et al. Symptoms and Endoscopic Finding in the Diagnosis of Gastroesophageal Reflux Disease. Scand J Gastroenterol 22: 714-718, 1987. 10) KAHRILAS JP, PANDOLFINO JE. Gastroesophageal Reflux Disease. In: Sleisenger F. Gastrointestinal Disease. 2004, p.599-622. 11) KIESSLICH R et al. Minimal Change Esophagitis: Prospective Comparison of Endoscopic and Histological Markers between Patients with Non-erosive Reflux Disease and Normal Controls Using Magnifying Endoscopy. Dig Dis 22: 221-227, 2004. 12) NADER F et al. Prevalência de pirose em Pelotas, RS, Brasil. Estudo de base populacional. Arquivos de Gastroenterologia. 2003. 13) OLIVEIRA CA, LIMA Jr GF. Contribuição da Endoscopia para o Diagnóstico da Hérnia Hiatal e da Esofagite de Refluxo. In: SOBED. Endoscopia Digestiva. Rio de Janeiro: Fundação SmithKline, julho de1984, p.77-95. 14) PEREIRA-LIMA J. et al. Prevalência da doença do refluxo gastroesofágico: estudo populacional em Porto Alegre, RS. GED 19: 73-78, 2000.
13
15) PIRES C et al. Comparação do diagnóstico endoscópico com o histopatológico em crianças portadoras de esofagite. R.Ci.méd. biol., 2:155-162, 2003. 16) TÉNAIOVÁ J et al. Incidence of hiatal hernias in the current endoscopic praxis. Cas Lek Cesk 146:74-76, 2007. 17) VIETH M et al. What Parameters Are Relevant for the Histological Diagnosis of Gastroesophageal Reflux Disease without Barrett’s Mucosa? Dig Dis 22: 196-201,2004. 18) WEINSTEIN WM, BOGOCH ER, BOWES KL. The normal human esophageal mucosa: a histological reappraisal. Gastroenterology 68: 40-4, 1975. 19) ZENTILIN P. et al. Reassessment of the diagnostic Value of Histology in Patients with GERD, Using Multiple Biopsy Sites and na Appropriate Control Group. American Journal of gastroenterology 2299-2305, 2005.
14
Artigo Científico
Valor Diagnóstico do Achado Endoscópico “Mucosa Nacarada” na
Esofagite de Refluxo
Autor: José Salomão JR. Orientador: Júlio C. Pereira Lima. Co-orientador: Raul ª Mendoza Sassi. Patologista colaborador: Dr.Renan Juliano.
Trabalho realizado no Hospital Universitário da Fundação
Universidade Federal de Rio Grande (FURG), no Serviço de
Endoscopia Digestiva da Santa Casa de Rio Grande e Serviço de
Gastroenterologia da FFFCMPA/Santa Casa de Porto Alegre.
Endereço para correspondência: [email protected]
15
DIAGNOSTIC VALUE OF THE ENDOSCOPIC FINDING OF THE NACRED MUCOSA FOR THE REFLUX ESOPHAGITIS
ABSTRACT Objectives: This study had as aim the validation of the nacred mucosa presence in the
endoscopy for the esophagitis diagnosis. Experimental design: A study of transversal
type was designed to calculate the sensitivity and specificity of the nacred mucosa.
Place of Study: It was performed at two Digestive Endoscopy Units in the city of Rio
Grande, RS. Patient selection: All patients submitted to the digestive endoscopy during
the time period of January 2005 and July 2006 that fulfilled the inclusion and exclusion
criteria. Results: The sensitivity and specificity of nacred mucosa from the 118 studied
patients were 68.1% and 37.5%, respectively. When the group with hiatal hernia was
analyzed the sensitivity was of 95.7% and specificity 0%. When studying the validity of
the double criterion (nacred mucosa plus hiatal hernia) the sensitivity was 24.2% and
specificity 63%. Conclusions: The validation of the nacred mucosa for the diagnosis of
the esophagitis is low. The presence of nacred mucosa and hiatal hernia increased the
specificity of the test.
Keywords: esophagitis, nacred mucosa, edematous esophagitis, Reflux Disease,
validation.
16
INTRODUCTION The normal endoscopic aspect of the distal esophagus must present the
visualization of the submucosa vessels. The nacred mucosa is characterized by a more
whitish coloration of the distal esophagus and the vanishing of the visualization of this
submucosa vasculature.
The organic complaints of the Gastroesophageal Reflux Disease (GERD) are
very frequent in gastroenterology units. In studies performed in the State of Rio Grande
do Sul, in the cities of Pelotas and Porto Alegre, the prevalence is of about 20% of the
population (12-14).
The upper digestive endoscopy is the first diagnostic method for this injury. The
endoscopic classification for the reflux esophagitis, by Savary-Miller and Los Angeles,
contemplate only erosive lesions, not considering the nacred mucosa as esophagitis,
resulting in a sensitivity of about 50% for this method (2).
OLIVEIRA and LIMA (13) considered the nacred mucosa as edematous
esophagitis supporting that it was an initial phase of the endoscopic esophagitis, and
biopsies were indicated. Patients with Non-Erosive Reflux Disease (NERD) that would
may have nacred mucosa are of 60 to 70% of the patients with GERD (4) and any
diagnose method presents low sensitivity in this situation. The majority of the studies
exclude esophageal minimal alterations, including the nacred mucosa.
In this way, the presence of this endoscopic alteration as a criterion of
esophagitis was not completely evaluated. This study evaluate this common alteration in
the endoscopy and has as main objective to validate the nacred mucosa as a diagnose
test for esophagitis, using the histological criteria of ISMAIL-BEIGI et al. (8) as gold
standard in the esophagitis diagnostics.
17
MATERIAL AND METHODS
Type of study and sampling
The study was of the transversal type, adequate for the research objective and
carried out in the Digestive Endoscopy Unit of the University Hospital from Fundação
Universidade Federal de Rio Grande (FURG) and in the Digestive Endoscopy Unit of
the Santa Casa de Rio Grande, during the period of January 2005 to July 2006.
The sampling was non-randomized since the objective was the validation of the
nacred mucosa presence in relation to esophagitis confirmed by histopathological
examination. The size of the sample was calculated using the necessary parameters for
this kind of study. It was expected a sensitivity and specificity of 90% with 10% error, a
confidence level of 95%, and a ratio of ill people without/with esophagitis of 3:7. These
numbers rendered a sample of 117 patients. To this value it was accreted 10% for
possible losses, reaching a total of 129 persons.
Patients
The patients submitted to upper digestive endoscopy were evaluated
consecutively. All of them had indications to perform upper digestive endoscopy due to
superior abdominal symptoms, as dyspepsia, pyrosis, epigastric pain and post-prandial
plenitude. Before the examination the patients filled a formulary with their personal data
(name, age, sex, and address) and examination motive. It was excluded from this study
patients that presented erosive esophagitis, esophagus ulcerations, suspect of Barrett’s
esophagus, esophagic neoplasia, gastric neoplasia, and gastric and duodenal ulcerations.
18
Instruments and definition of variables
In the endoscopic examination it was used a Pentax 3300 equipment, EG 2930
and Olympus Exera CV 145 GIF with Olympus and Endoflex biopsy forceps. During
the esophagoscopy the esophagogastric junction (E-G) was carefully examined for the
presence or absence of hiatal hernia. This endoscopic diagnosis was considered when
the Z-line was above 2.0 cm of the diaphragmatic clamping.
From the endoscopic viewpoint, it was defined as palisade mucosa (normal
esophagic mucosa) when it was observed the distal submucosa vasculature, in addition
to almost the transparency of it. The presence of nacred mucosa was considered when
there was the vanishing of the vasculature of the distal submucosa, and the mucosa was
whitish pearly.
From each patient it was removed four fragments – one from each quadrant of
the inferior esophagus – located about 2.5 to 5 cm above Z line. The four removed
fragments were preserved in formalin until its inclusion in paraffin blocks, after alcohol
dehydration and xylol clarification, in OMA histotechnique. The fragments were
included always in two blocks to facilitate the posterior microtomy and staining. The 5-
µm cuts were performed in Spencer 820 microtome, followed by Hematoxylin-Eosin
(HE), Giemsa and Alcian Blue staining techniques. It was selected three HE slides for
evaluation, and the Giemsa and Alcian Blue were used for eventual intestinal
metaplasia, as part of the routine study of the cases and diagnostic formulation. From
the HE slides it was selected three sections with the incidence perfectly transversal for
the epithelial thickness, basal layer and papillae height analysis (if necessary, new cuts
were performed). The other variables were also analyzed in other representative
sections, once they were representative of the total.
19
All slides were analyzed by the same pathologist, without the knowledge of the
endoscopic finds of the patients.
Before the observations start it was established the following parameters for the
histopathological identification:
a) Hyperplasia of basal layer: considered present when it fills 15% or more of the
scaly epithelium thickness.
b) Papillae projection: considered when these structures fill more than 50% of the
mucosa layer.
c) Granulocyte infiltration: considered when observed the presence or absence of
neutrophils and/or eosinophils in the thickness of the epithelial layer
(exocytose).
d) Vascular congestion: considered present or absent, taking into account mainly
the papillary vessel dilatations.
e) Glycogen: considered the presence of thickness enlargement of the layer
containing glycogen in the study with HE (acanthosis).
It was considered alterations compatible with esophagitis when there was
present any one of the lesions described above.
Data analysis
The data were imputed in the program Stata 9.0 for the statistical analysis. First
it was carried out the description of the data. At this phase it was calculated the averages
and standard deviations of the continuous variables and the proportions for the case of
categorical variables. The frequencies of the nacred mucosa and of the different
histopatological categories were identified. Following, it was carried out the bivariate
20
analysis among the presence of the nacred mucosa and the demographical data and
histopathological finds, by using the chi-square test. In case of impossibility of using
this test it was applied the Fisher’s Exact Test. The fixed value for p was 0.05 of a two-
tailored test.
The validation study was carried out by the calculation of the test accuracy,
sensitivity, specificity, and also the predictive values (positive and negative) for the
presence of the nacred mucosa, having as gold standard the histopathological presence
of esophagitis. It was also performed calculations for any one of the histopathological
categories.
Ethical aspects
The study was submitted and approved by the Ethical Commission of the
University Hospital of the Fundação Universidade Federal do Rio Grande (Process
Number 23116.6775/5.18). It was applied a term of free and clarified commitment, at
the moment in which the patients were invited to participate. Independently of the
project participation, all individuals have received the adequate treatment for their
diagnosis.
RESULTS
From the 124 patients identified, six were excluded by presenting inadequate
material. So the final sample was of 118 patients.
The age distribution varied from 16 to 80 years old, with an average of 47.8
years old (SD 12.5). The sex distribution was 75 females (63.7%) and 43 males
(36.3%). The most frequent age was the category of 40-49 years old (36%).
The frequency of the nacred mucosa in the sample was 67%. The distribution of
this finding by sex or age did not show important differences (Table 1).
21
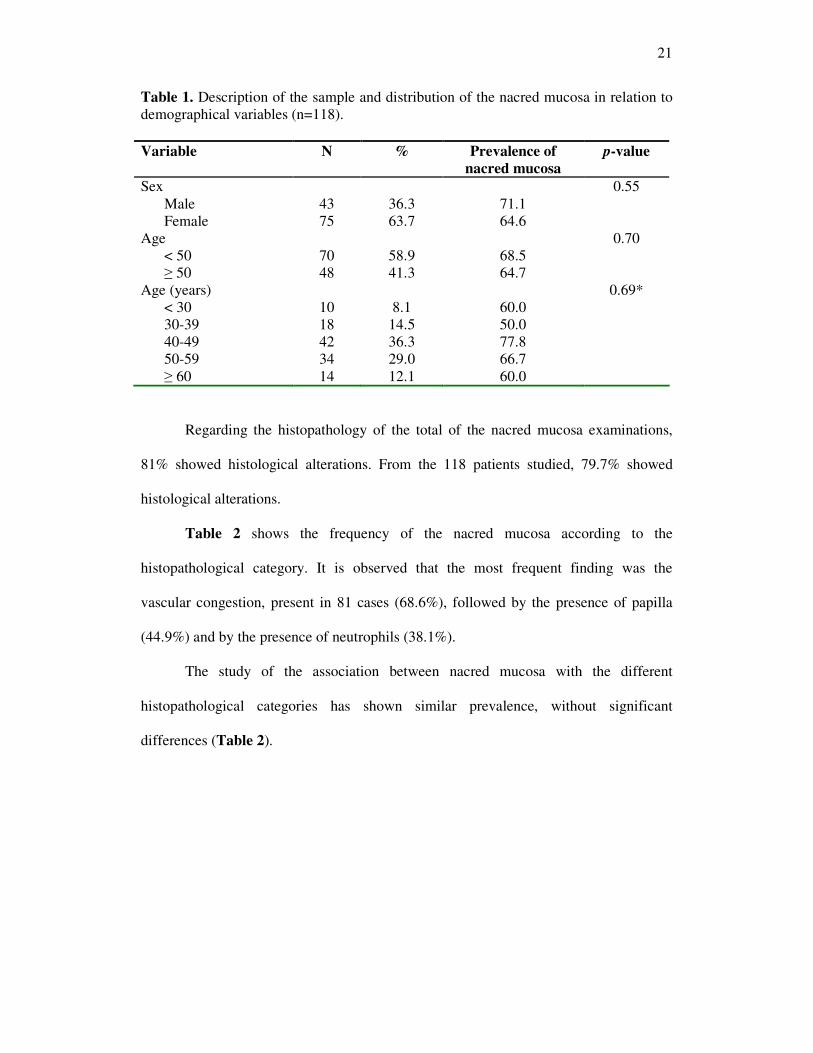
Table 1. Description of the sample and distribution of the nacred mucosa in relation to demographical variables (n=118). Variable N % Prevalence of
nacred mucosa p-value
Sex 0.55 Male 43 36.3 71.1 Female 75 63.7 64.6
Age 0.70 < 50 70 58.9 68.5 ≥ 50 48 41.3 64.7
Age (years) 0.69* < 30 10 8.1 60.0 30-39 18 14.5 50.0 40-49 42 36.3 77.8 50-59 34 29.0 66.7 ≥ 60 14 12.1 60.0
Regarding the histopathology of the total of the nacred mucosa examinations,
81% showed histological alterations. From the 118 patients studied, 79.7% showed
histological alterations.
Table 2 shows the frequency of the nacred mucosa according to the
histopathological category. It is observed that the most frequent finding was the
vascular congestion, present in 81 cases (68.6%), followed by the presence of papilla
(44.9%) and by the presence of neutrophils (38.1%).
The study of the association between nacred mucosa with the different
histopathological categories has shown similar prevalence, without significant
differences (Table 2).
22
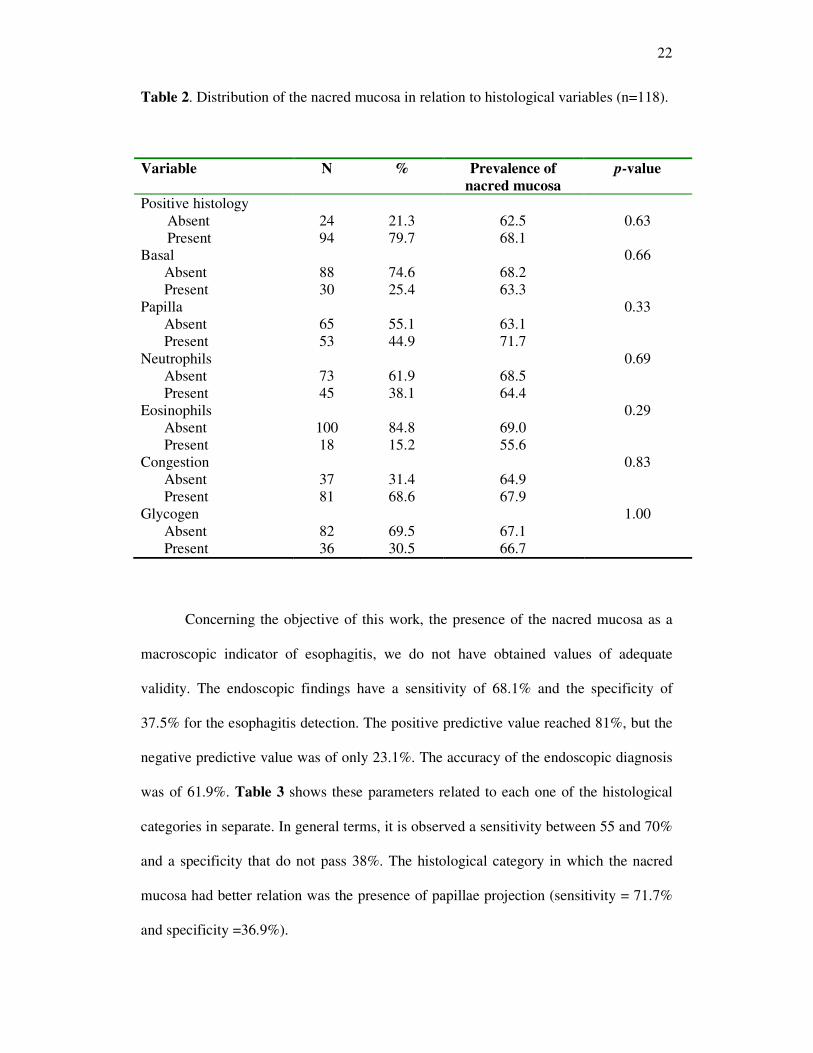
Table 2. Distribution of the nacred mucosa in relation to histological variables (n=118).
Variable N % Prevalence of nacred mucosa
p-value
Positive histology Absent 24 21.3 62.5 0.63 Present 94 79.7 68.1 Basal 0.66
Absent 88 74.6 68.2 Present 30 25.4 63.3
Papilla 0.33 Absent 65 55.1 63.1 Present 53 44.9 71.7
Neutrophils 0.69 Absent 73 61.9 68.5 Present 45 38.1 64.4
Eosinophils 0.29 Absent 100 84.8 69.0 Present 18 15.2 55.6
Congestion 0.83 Absent 37 31.4 64.9 Present 81 68.6 67.9
Glycogen 1.00 Absent 82 69.5 67.1 Present 36 30.5 66.7
Concerning the objective of this work, the presence of the nacred mucosa as a
macroscopic indicator of esophagitis, we do not have obtained values of adequate
validity. The endoscopic findings have a sensitivity of 68.1% and the specificity of
37.5% for the esophagitis detection. The positive predictive value reached 81%, but the
negative predictive value was of only 23.1%. The accuracy of the endoscopic diagnosis
was of 61.9%. Table 3 shows these parameters related to each one of the histological
categories in separate. In general terms, it is observed a sensitivity between 55 and 70%
and a specificity that do not pass 38%. The histological category in which the nacred
mucosa had better relation was the presence of papillae projection (sensitivity = 71.7%
and specificity =36.9%).
23
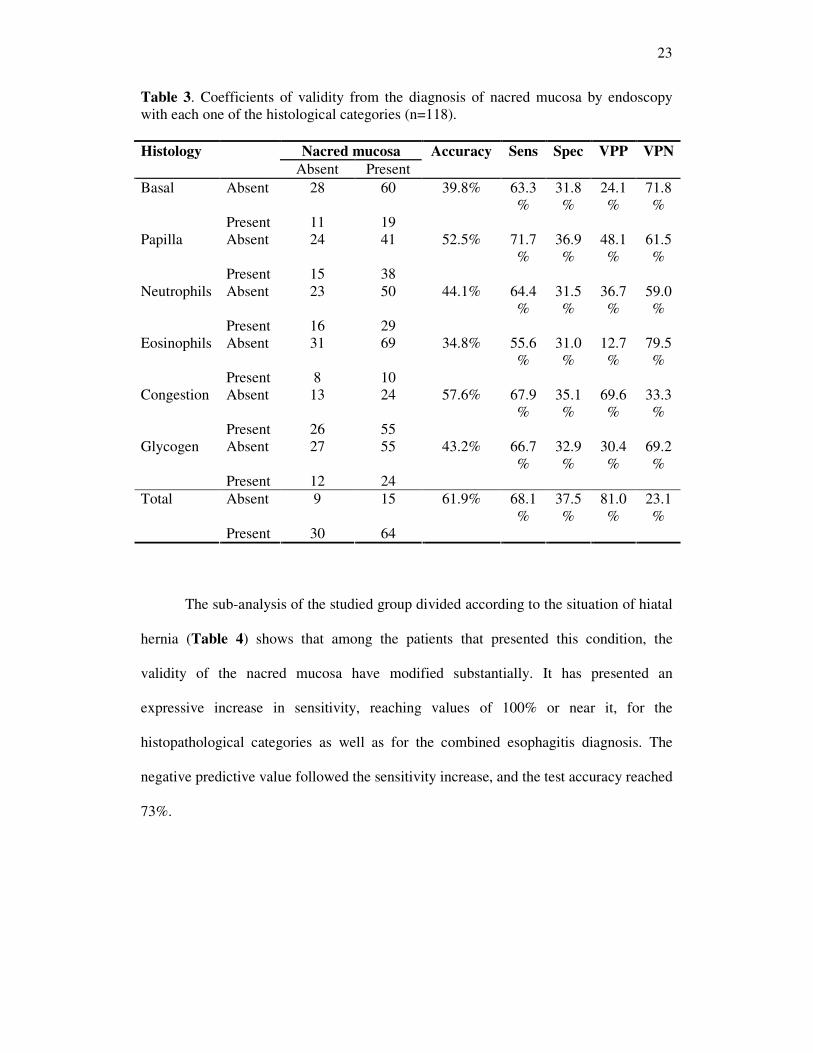
Table 3. Coefficients of validity from the diagnosis of nacred mucosa by endoscopy with each one of the histological categories (n=118). Histology Nacred mucosa Accuracy Sens Spec VPP VPN Absent Present
Absent 28 60 39.8% 63.3%
31.8%
24.1%
71.8%
Basal
Present 11 19 Absent 24 41 52.5% 71.7
% 36.9%
48.1%
61.5%
Papilla
Present 15 38 Absent 23 50 44.1% 64.4
% 31.5%
36.7%
59.0%
Neutrophils
Present 16 29 Absent 31 69 34.8% 55.6
% 31.0%
12.7%
79.5%
Eosinophils
Present 8 10 Absent 13 24 57.6% 67.9
% 35.1%
69.6%
33.3%
Congestion
Present 26 55 Absent 27 55 43.2% 66.7
% 32.9%
30.4%
69.2%
Glycogen
Present 12 24 Absent 9 15 61.9% 68.1
% 37.5%
81.0%
23.1%
Total
Present 30 64
The sub-analysis of the studied group divided according to the situation of hiatal
hernia (Table 4) shows that among the patients that presented this condition, the
validity of the nacred mucosa have modified substantially. It has presented an
expressive increase in sensitivity, reaching values of 100% or near it, for the
histopathological categories as well as for the combined esophagitis diagnosis. The
negative predictive value followed the sensitivity increase, and the test accuracy reached
73%.
24
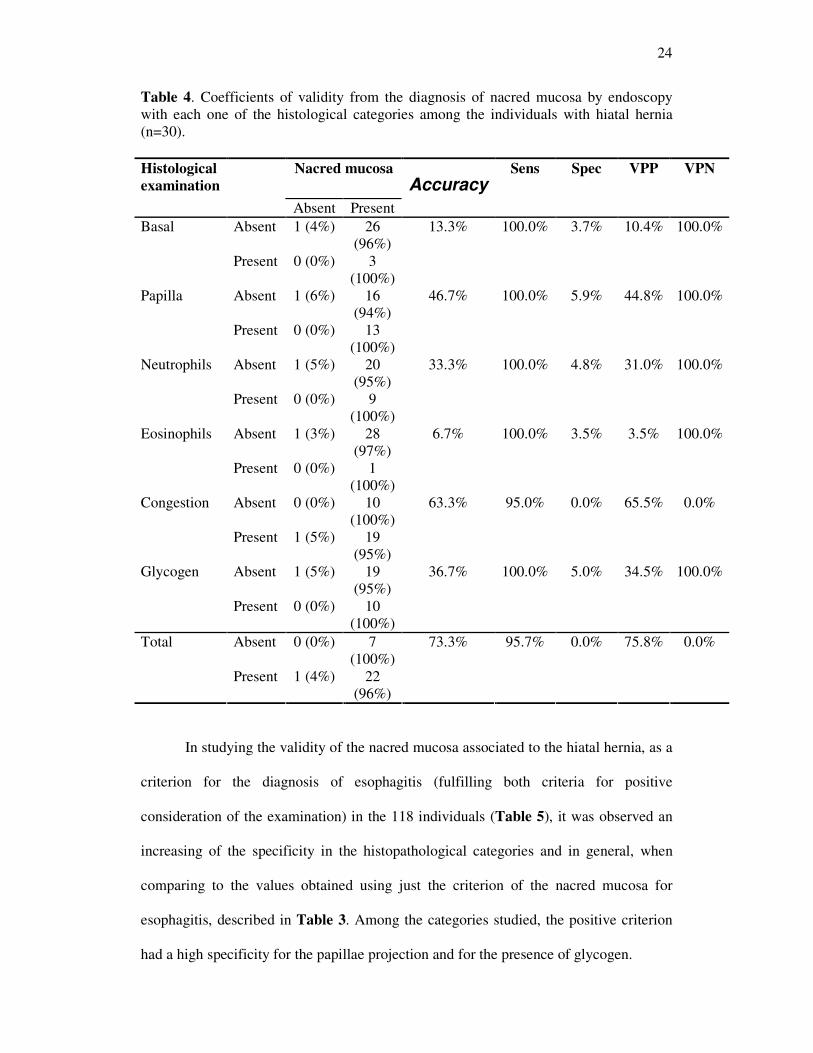
Table 4. Coefficients of validity from the diagnosis of nacred mucosa by endoscopy with each one of the histological categories among the individuals with hiatal hernia (n=30).
Nacred mucosa Accuracy
Sens Spec VPP VPN Histological examination
Absent Present Absent 1 (4%) 26
(96%) 13.3% 100.0% 3.7% 10.4% 100.0% Basal
Present 0 (0%) 3 (100%)
Absent 1 (6%) 16 (94%)
46.7% 100.0% 5.9% 44.8% 100.0% Papilla
Present 0 (0%) 13 (100%)
Absent 1 (5%) 20 (95%)
33.3% 100.0% 4.8% 31.0% 100.0% Neutrophils
Present 0 (0%) 9 (100%)
Absent 1 (3%) 28 (97%)
6.7% 100.0% 3.5% 3.5% 100.0% Eosinophils
Present 0 (0%) 1 (100%)
Absent 0 (0%) 10 (100%)
63.3% 95.0% 0.0% 65.5% 0.0% Congestion
Present 1 (5%) 19 (95%)
Absent 1 (5%) 19 (95%)
36.7% 100.0% 5.0% 34.5% 100.0% Glycogen
Present 0 (0%) 10 (100%)
Absent 0 (0%) 7 (100%)
73.3% 95.7% 0.0% 75.8% 0.0% Total
Present 1 (4%) 22 (96%)
In studying the validity of the nacred mucosa associated to the hiatal hernia, as a
criterion for the diagnosis of esophagitis (fulfilling both criteria for positive
consideration of the examination) in the 118 individuals (Table 5), it was observed an
increasing of the specificity in the histopathological categories and in general, when
comparing to the values obtained using just the criterion of the nacred mucosa for
esophagitis, described in Table 3. Among the categories studied, the positive criterion
had a high specificity for the papillae projection and for the presence of glycogen.
25
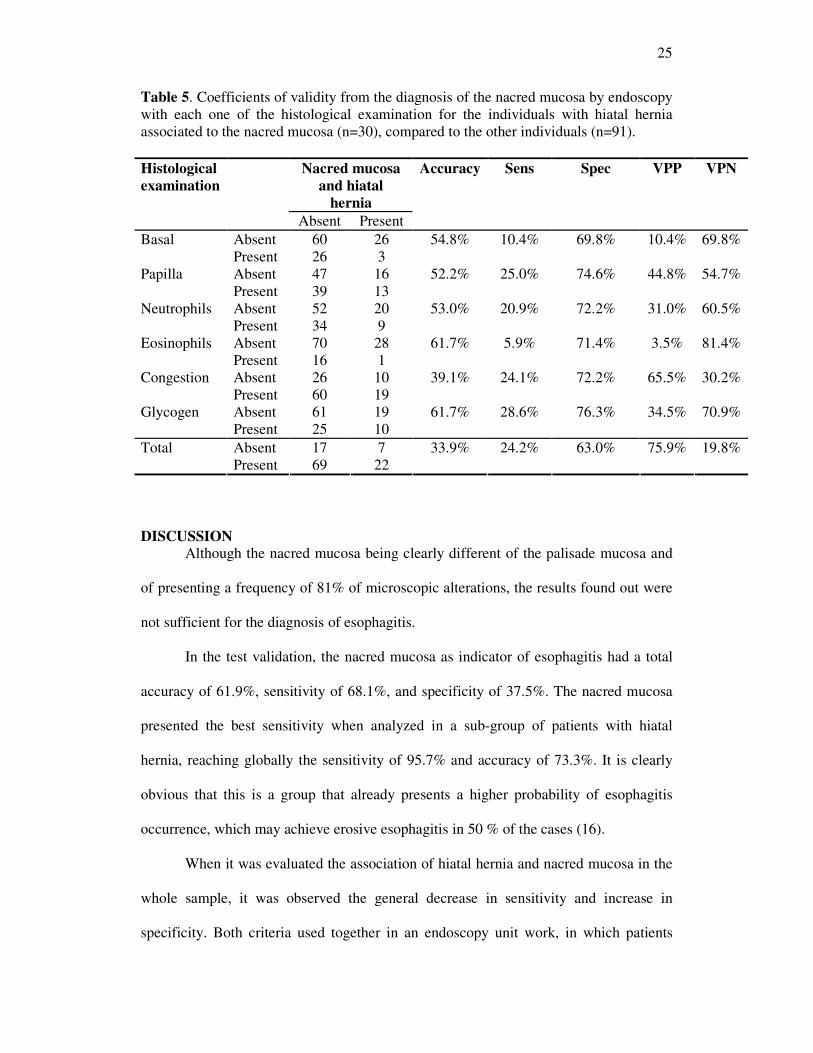
Table 5. Coefficients of validity from the diagnosis of the nacred mucosa by endoscopy with each one of the histological examination for the individuals with hiatal hernia associated to the nacred mucosa (n=30), compared to the other individuals (n=91).
Nacred mucosa and hiatal
hernia
Accuracy Sens Spec VPP VPN Histological examination
Absent Present Absent 60 26 54.8% 10.4% 69.8% 10.4% 69.8% Basal Present 26 3 Absent 47 16 52.2% 25.0% 74.6% 44.8% 54.7% Papilla Present 39 13 Absent 52 20 53.0% 20.9% 72.2% 31.0% 60.5% Neutrophils Present 34 9 Absent 70 28 61.7% 5.9% 71.4% 3.5% 81.4% Eosinophils Present 16 1 Absent 26 10 39.1% 24.1% 72.2% 65.5% 30.2% Congestion Present 60 19 Absent 61 19 61.7% 28.6% 76.3% 34.5% 70.9% Glycogen Present 25 10 Absent 17 7 33.9% 24.2% 63.0% 75.9% 19.8% Total Present 69 22
DISCUSSION
Although the nacred mucosa being clearly different of the palisade mucosa and
of presenting a frequency of 81% of microscopic alterations, the results found out were
not sufficient for the diagnosis of esophagitis.
In the test validation, the nacred mucosa as indicator of esophagitis had a total
accuracy of 61.9%, sensitivity of 68.1%, and specificity of 37.5%. The nacred mucosa
presented the best sensitivity when analyzed in a sub-group of patients with hiatal
hernia, reaching globally the sensitivity of 95.7% and accuracy of 73.3%. It is clearly
obvious that this is a group that already presents a higher probability of esophagitis
occurrence, which may achieve erosive esophagitis in 50 % of the cases (16).
When it was evaluated the association of hiatal hernia and nacred mucosa in the
whole sample, it was observed the general decrease in sensitivity and increase in
specificity. Both criteria used together in an endoscopy unit work, in which patients
26
arrive with several complaints, result in a better specificity for the diagnosis of
esophagitis, but very low sensitivity.
The study did not select patients by symptoms of gastroesophagic reflux. Maybe
this selection would show a higher association of the nacred mucosa and microscopic
esophagitis. The majority of the studies for the validation of diagnostic methods in the
GERD are carried out in patients with symptoms of this illness (5-7-9-11). The
histological criteria used were determined by ISMAIL-BEIJI et al. (8), except by the
presence of glycogen, which is not well-established its relation with esophagitis, but it
was considered in this study according to some authors (10-17). This alteration
presented the same results of the other histological findings. The histological evidence
of better result was the papillae projections, according to the findings of other studies
(8-17).
The diagnostic method of first choice in the GERD is the endoscopy, being
known that the sensitivity of the method is about 50%, i.e., the patients with GERD
have endoscopy without erosions in half of the cases. These patients consider
themselves as carriers of the NERD, and can attain even 60 to 70% of the GERD
patients (4). The small endoscopic alterations have not been defined (7) nor valorized in
the majority of the service units. Some Japanese authors sustain that the Los Angeles
classification should contemplate minimal alterations, but concluded that it has low
clinical value (1). KIESSLICH et al. (11), in a study with NERD using magnification
equipment and histology combination, could predict with a sensitivity of 62% and
specificity of 74% the presence of esophagitis. In the present study it was found similar
sensitivity, but the specificity was very low, maybe because the patients were not pre-
selected as GERD symptomatic. Celso Affonso de Oliveira already valorized the
finding of nacred mucosa and called it edematous esophagitis, considering it as the first
27
stage of the reflux esophagitis and, at this phase, suggested biopsy as indispensable.
This author, in 1984, published a work in a book of the Brazilian Society of Endoscopy
(Sociedade Brasileira de Endoscopia – SOBED) in which he analyzed 147 cases of
hiatal hernia and evaluated the histological alterations in individuals with normal
mucosa and other with nacred mucosa. He found out 57.1% of histological alterations in
patients with edematous esophagitis and 32.5% without this condition.
Also, it was analyzed 699 patients with hiatal hernia and found out 23.2% of
edematous esophagitis (8). The findings of the present study show 96.8% of nacred
mucosa in the group with hiatal hernia, and the histological alterations in this group
were present in 96% of the cases. These differences occurred due to the design of the
study, once it was planned to evaluate the validity.
WEINSTEIN et al. (18) performed biopsies in asymptomatic patients for GERD
and found out histological alterations in a significant number of cases, i.e., the
histological alterations may be present in individuals with normal endoscopy (9). Other
studies have evaluated the validation of pHmetry. One of them, looking for the analysis
of the 24 h esophagical pHmetry in patients with histologically confirmed esophagitis
resulted in 60% of sensitivity for this method (5). The low sensitivity of this test
confirms the necessity of a new valid examination for the GERD presence.
The nacred mucosa is a minimal alteration and its correlation with histology is
poorly studied and defined. There are no data that supports the nacred mucosa and
biopsy as diagnostic methods, not even well-established data regarding its sensitivity
and specificity.
We conclude that the nacred mucosa presents inadequate sensitivity and
specificity for the diagnosis of the reflux esophagitis. In the sub-group presenting hiatal
hernia the nacred mucosa may be used as a good indicator of esophagitis.
28
This study was the first to evaluate the validity of the nacred mucosa role in the
diagnosis of esophagitis. New technologies, such as stained image magnifications,
digitalization process and immunohistochemistry, should contribute for a better
elucidation of this mucosa alteration, as well its histological changes.
ACKNOWLEDGEMENTS During the period of this Master Degree we have the privilege of working with
the team from the Post-graduation Program of Fundação Faculdade Federal de Ciências
Médicas, of Porto Alegre, which we have summed up true learning and knowledge.
I would like to thank my supervisor, co-supervisor, and all persons that have
collaborated, for the patience, opportunity, credibility and learning.
Finally, I would like to thank and dedicate this work to the patients that, despite
their health problems, still were able to participate of this research project.
29
REFERENCES
1) AMANO Y, ISHIMURA N, FUTURA K. Interobserver agreement on classifying diagnoses of nonerosive esophagitis. Endoscopy, 38: 1032-5, oct. 2006. 2) ARMSTRONG D. Endoscopic Evaluation of Gastro-Esophageal Reflux Disease. Yale J Biol MED, 72: 93-100, 1999. 3) BOYCE HW. Endoscopic diagnosis and classification of reflux esophagitis: Are we there yet? Gastrointestinal Endoscopy, 56:775-778, 2002. 4) FASS RONIE. Doença do Refluxo Gastroesofágico: Questões e conceitos atuais. 5) FLORA-FILHO R, CÂMARA-LOPES LH, ZILBERSTEIN B. Critérios histológicos de esofagite na doença do refluxo gastroesofágico. Reavaliação da sensibilidade da pHmetria esofágica de 24hs. Arq. Gastroenterologia 37: 197-202, 2000. 6) GOLDMAN, H. Inflammatory Disorders of the Esophagus.Gastrointestinal mucosal biopsy.1996,p.11-49. 7) HATLEBAKK JG, BERSTAD A. Endoscopic Grading of Reflux Oesophagitis: What Observations Correlate with Gastro-Oesophageal Reflux? Scand J Gastroenterol 32: 760-65, 1997. 8) ISMAIL-BEIGI F, HORTON PF, POPE II CE. Histological consequences of gastroesophageal reflux in man. Gastroenterology 58: 163-74, 1970. 9) JOHNSSON F et al. Symptoms and Endoscopic Finding in the Diagnosis of Gastroesophageal Reflux Disease. Scand J Gastroenterol 22: 714-718, 1987. 10) KAHRILAS JP, PANDOLFINO JE. Gastroesophageal Reflux Disease. In: Sleisenger F. Gastrointestinal Disease. 2004, p.599-622. 11) KIESSLICH R et al. Minimal Change Esophagitis: Prospective Comparison of Endoscopic and Histological Markers between Patients with Non-erosive Reflux Disease and Normal Controls Using Magnifying Endoscopy. Dig Dis 22: 221-227, 2004. 12) NADER F et al. Prevalência de pirose em Pelotas,RS, Brasil. Estudo de base populacional. Arquivos de Gastroenterologia. 2003. 13) OLIVEIRA CA, LIMA Jr GF. Contribuição da Endoscopia para o Diagnóstico da Hérnia Hiatal e da Esofagite de Refluxo. In: SOBED. Endoscopia Digestiva. Rio de Janeiro: Fundação SmithKline, julho de1984, p.77-95. 14) PEREIRA-LIMA J. et al. Prevalência da doença do refluxo gastroesofágico: estudo populacional em Porto Alegre, RS. GED 19: 73-78, 2000.
30
15) PIRES C et al. Comparação do diagnóstico endoscópico com o histopatológico em crianças portadoras de esofagite. R.Ci.méd. biol., 2:155-162, 2003. 16) TÉNAIOVÁ J et al. Incidence of hiatal hernias in the current endoscopic praxis. Cas Lek Cesk 146:74-76, 2007. 17) VIETH M et al. What Parameters Are Relevant for the Histological Diagnosis of Gastroesophageal Reflux Disease without Barrett’s Mucosa? Dig Dis 22: 196-201, 2004. 18) WEINSTEIN WM, BOGOCH ER, BOWES KL. The normal human esophageal mucosa: a histological reappraisal. Gastroenterology 68: 40-4, 1975. 19) ZENTILIN P. et al. Reassessment of the diagnostic Value of Histology in Patients with GERD, Using Multiple Biopsy Sites and na Appropriate Control Group. American Journal of gastroenterology 2299-2305, 2005.
Livros Grátis( http://www.livrosgratis.com.br )
Milhares de Livros para Download: Baixar livros de AdministraçãoBaixar livros de AgronomiaBaixar livros de ArquiteturaBaixar livros de ArtesBaixar livros de AstronomiaBaixar livros de Biologia GeralBaixar livros de Ciência da ComputaçãoBaixar livros de Ciência da InformaçãoBaixar livros de Ciência PolíticaBaixar livros de Ciências da SaúdeBaixar livros de ComunicaçãoBaixar livros do Conselho Nacional de Educação - CNEBaixar livros de Defesa civilBaixar livros de DireitoBaixar livros de Direitos humanosBaixar livros de EconomiaBaixar livros de Economia DomésticaBaixar livros de EducaçãoBaixar livros de Educação - TrânsitoBaixar livros de Educação FísicaBaixar livros de Engenharia AeroespacialBaixar livros de FarmáciaBaixar livros de FilosofiaBaixar livros de FísicaBaixar livros de GeociênciasBaixar livros de GeografiaBaixar livros de HistóriaBaixar livros de Línguas
Baixar livros de LiteraturaBaixar livros de Literatura de CordelBaixar livros de Literatura InfantilBaixar livros de MatemáticaBaixar livros de MedicinaBaixar livros de Medicina VeterináriaBaixar livros de Meio AmbienteBaixar livros de MeteorologiaBaixar Monografias e TCCBaixar livros MultidisciplinarBaixar livros de MúsicaBaixar livros de PsicologiaBaixar livros de QuímicaBaixar livros de Saúde ColetivaBaixar livros de Serviço SocialBaixar livros de SociologiaBaixar livros de TeologiaBaixar livros de TrabalhoBaixar livros de Turismo