universidade federal do rio de janeiro ufrj centro de ... · amanda osÓrio ayres de freitas, ......
TRANSCRIPT
Universidade Federal do Rio de Janeiro – UFRJ
Centro de Ciências da Saúde
Faculdade de Odontologia
ASPECTOS MICROBIOLÓGICOS ASSOCIADOS AOS
MINI-IMPLANTES ORTODÔNTICOS
AMANDA OSÓRIO AYRES DE FREITAS, CD, MO
Tese submetida ao corpo docente da Faculdade de
Odontologia da Universidade Federal do Rio de Janeiro -
UFRJ, como parte dos requisitos, para a obtenção do Título
de Doutor em Odontologia (Ortodontia).
Rio de Janeiro
2014

ii
ASPECTOS MICROBIOLÓGICOS ASSOCIADOS AOS
MINI-IMPLANTES ORTODÔNTICOS
AMANDA OSÓRIO AYRES DE FREITAS, CD
Orientadores: Profª. Drª. MATILDE DA CUNHA GONÇALVES NOJIMA
Profª. Drª. DANIELA SALES ALVIANO MORENO
Tese submetida ao corpo docente da
Faculdade de Odontologia da Universidade do Brasil -
UFRJ, como parte dos requisitos para obtenção do Título
de Doutor em Odontologia (Ortodontia).
Comissão Examinadora:
__________________________ _____________________________
Profª. Drª. Celuta Sales Alviano Profª. Drª. Luciana Rougemont Química CD
__________________________ _____________________________
Profª. Drª. Ana Maria Bolognese Prof. Dr. Eduardo Franzotti Sant’Anna CD CD
_____________________________ Profª. Drª. Matilde da C. G. Nojima CD
Rio de Janeiro
2014

iii
Ficha Catalográfica
FREITAS, Amanda Osório Ayres de
Aspectos microbiológicos associados aos mini-implantes
ortodônticos. Rio de Janeiro: UFRJ/Faculdade de Odontologia, 2014.
xxii, 121f.
Tese: Doutorado em Odontologia (Ortodontia) – Universidade Federal
do Rio de Janeiro, Faculdade de Odontologia, 2014.
1. Ancoragem esquelética 2. Mini-implante
3. Microbiologia 4. Teses
I. Título
II. Tese (Doutorado – UFRJ/ Faculdade de Odontologia)

iv
A Deus, e aos que estiveram sempre ao meu lado, iluminando meu caminho
e me amparando nos momentos de dificuldade. Aos meus queridos avós Dr.
Waldir Ayres e Lúcia Ayres, que com certeza continuam vibrando com minhas
conquistas.
DEDICO

v
HOMENAGEM ESPECIAL
A minha mãe, meu pai e meu irmão, agradeço pelo apoio e incentivo
para que conseguisse progredir na minha carreira profissional e,
principalmente, por entenderem a necessidade da minha ausência durante
este período de muito trabalho.
A minha querida sobrinha Beatriz Knoch Freitas pelo amor verdadeiro
e incondicional.
Muito obrigada!

vi
AGRADECIMENTOS
Aos professores, Drª. Ana Maria Bolognese, Dr. Antônio Carlos de
Oliveira Ruellas, Dr. Eduardo Franzotti Sant’ana, Dr. José Fernando Stangler
Brazzalle, Dr. Lincoln Issamu Nojima, Drª. Margareth Maria Gomes de Souza,
Drª. Matilde da Cunha Gonçalves Nojima, Drª. Mônica Tirre de Souza Araújo,
Drª. Teresa Cristina Moreira (in memoriam), que me apresentaram e me fizeram
apaixonar pela Ortodontia. Cada um contribuiu, de alguma maneira, para a minha
formação e para despertar a vontade de compartilhar meus conhecimentos e
aprender com os estudantes de Odontologia.
Agradeço novamente à orientação e ao carinho da Profª. Drª. Matilde da
Cunha Gonçalves Nojima. E, em especial, pela confiança e incentivo, me
estimulando sempre a seguir em frente, apesar das dificuldades.
Ao querido amigo Waltencir Ferreira e adorável família, por me acolherem
como se fizesse parte dela. Muito obrigada por tudo! Sempre me lembrarei do
carinho, ajuda, do apoio nos momentos difíceis e das boas risadas que demos
juntos. Aos funcionários e amigos do Departamento de Ortodontia.
Aos meus orientadores de iniciação científica no período de graduação,
Profª. Drª Mônica Tirre de Souza Araújo, Dr. Milton Santamaria Jr, Dr. Camilo
Aquino Melgaço, Luiz Felipe Miranda Costa, que me apresentaram ao mundo da
ciência.

vii
Aos colegas e amigos da 43ª turma de mestrado (2007/2008), Bianca Motta,
Carina Rodrigues, Joanna Binato, José Luiz Muñoz, Letícia Felicio, Mariana
Marquezan, Thiago Lau, pela solidariedade e convívio durante os dois anos de
curso.
Aos colegas e amigos da 42ª turma de mestrado (2006/2007), Ângela Dalvi,
Cristiane Machado, Luciana Boaventura, Matheus Pithon, Maurício Guerra,
Paula Nascimento, Raphael Mesquita e Rogério Lacerda, pela dedicação em
tornarem a permanência no curso de mestrado mais prazerosa.
Aos colegas e amigos da 44ª turma de mestrado (2008/2009), Alexandre
Ribeiro, Ana Sabanneff, Cláudia Trindade, Carolina Baratieri, Diego
Lorenzoni, Donizete D’Andrea, Ilana Cruz, Matheus Alves Jr, pelos bons
momentos que passamos juntos.
Aos colegas de turma do doutorado (2009/2013): Giselle Villani, Luiz Felipe
Miranda, Mariana Marquezan e Rodrigo Santiago pela parceria nos trabalhos,
pela ótima convivência e carinho.
Aos colegas da turma 2010/2014: Carolina Baratieri, Claudia Trindade e
Matheus Alves Jr ; da turma 2011/2015: Alline Birra, Dayanne Lopes, Geórgia
Lau, Lígia Claudino e Teresa Cristina Oliveira, pela companhia e especialmente
pela contribuição nos trabalhos realizados.
Aos alunos do curso de mestrado das 45ª, 46ª e 47ª turmas, por colaborarem
nas coletas de material biológico dos pacientes, que estavam sob sua
responsabilidade.
À Déborah Leite, doutoranda em Microbiologia, pela ajuda e orientação na
etapa laboratorial da biologia molecular. Obrigada pela dedicação, pelo carinho e
pela amizade que construímos! Sua gentileza e humildade ao passar seus

viii
conhecimentos farão de você uma professora exemplar e muito querida. Torço
muito pelo seu sucesso!
Às professoras Drª Celuta Sales Alviano e Drª Daniela Sales Alviano
Moreno, pela orientação, dedicação, confiança, carinho, pelos ensinamentos
profissionais e da vida... Faltam palavras para agradecer. Desejo toda felicidade do
mundo a vocês e à família, que vai aumentar em breve. Vocês têm toda a minha
admiração e gratidão.
Querida Fátima Goulart, muito obrigada por continuar fazendo parte da
minha vida. Guardo no coração todo o seu carinho e toda a sua paciência para me
ensinar a trabalhar no laboratório. Você é muito especial!
Aos queridos amigos que fiz no laboratório de Microbiologia Estrutura de
Superfícies. Saibam que tenho carinho muito especial por cada um, pois sempre
foram maravilhosos comigo. Os tenho como grandes amigos, para toda vida.
À brilhante Profa Dra Ana Paula Vieira Colombo, agradeço por aceitar a
colaboração nos meus trabalhos, pela oportunidade de ajudar nas aulas práticas
de Microbiologia Oral, por tudo que me ensinou durante nossas conversas,
contribuindo com minhas pesquisas e minha vida. Acima de tudo, obrigada pela
amizade, carinho, e por me acolher na turma animada do laboratório. Foram
momentos maravilhosos!
Meninas, nem sei por onde começar... Adorei conhecê-las. A amizade de
todas: Bete Brasil, Carina Boghossian, Rachel Miranda, Renata Souto e Talita
Lourenço, foi um presente que recebi durante estes quatro anos. Dividimos muitas
emoções, sem dúvida. Certamente, estaremos sempre juntas! Adoro vocês! Muito
obrigada pela ajuda nos trabalhos, pela generosidade e carinho com que me
receberam no laboratório e em suas vidas.

ix
Durante a vida, algumas pessoas tornam-se essenciais para seguirmos na
nossa caminhada. Felizmente tive o privilégio de fazer grandes amizades desde a
infância. Amigos que se tornam parte da família, por escolha. Queridas amigas:
Ana Carolina Amorim, Clarisse Moreno, Fernanda Alonso, Fernanda
Gorgulho, Michelle Seabra e Monique Cavalcante, muito obrigada por tudo! A
vida não seria tão boa sem vocês.
Cássia Neres e Marcela Rodrigues, não poderia deixar de agradecê-las
pelo carinho, apoio, companheirismo, durante e depois dos nossos quatro anos de
graduação. A amizade sólida durante nossa formação fortaleceu-se com o passar
dos anos e, com certeza, conto com vocês para toda vida!
Aos “guerreiros” e amigos da Turma EAS/EST 2013: Ten Alexandra Braga,
Ten Alexandro, Ten Cecília Pereira, Ten Damyelly, Ten Joyce Gomes, Ten
Guedes, Ten Luiza Garcia, Ten mariana Morais, Ten R. Bittencourt, Ten
Vanessa Nascimento, Ten Viviane Souza. A amizade de vocês foi um presente
inesperado e, principalmente, o apoio que precisei para tornar a adaptação ao meio
militar mais tranquila. Vocês são o verdadeiro “braço forte e mão amiga”!
À CAPES, pela bolsa de estudos concedida.
À Faperj, pelo financiamento dos projetos de pesquisa.
x
RESUMO
FREITAS, Amanda Osório Ayres de. Aspectos microbiológicos associados aos
mini-implantes ortodônticos. Orientadoras: Profª. Drª. Matilde da Cunha
Gonçalves Nojima, Profª. Drª. Daniela Sales Alviano Moreno. Rio de Janeiro: UFRJ/
Faculdade de Odontologia, 2014. Tese (Doutorado em Odontologia- Ortodontia).
xxii, 121f.
Os autores deste estudo avaliaram a topografia do perfil transmucoso de
mini-implantes ortodônticos (MI), a adesão microbiana na superfície destes
dispositivos e o método mais eficaz para o controle microbiano dos mesmos. Para
a análise da topografia da superfície do perfil transmucoso de MI, foram realizadas
fotomicrografias e leituras da rugosidade de três marcas comerciais nacionais, por
meio de microscopia eletrônica de varredura (MEV) e microscopia de força atômica
(MFA). Após a inoculação com placa dental cultivada in vitro, coletada de pacientes
em tratamento ortodôntico, a adesão e formação de biofilme foram avaliadas em
ensaio microbiológico durante sete dias, a partir de MEV e microscopia óptica de
fluorescência (MF) do perfil transmucoso dos MI. Além disso, para detectar a
variedade e quantidade de micro-organismos aderidos, aplicou-se o “Checkerboard
DNA-DNA hybridization”. O estudo in vivo realizado comparou quatro protocolos de
xi
higienização dos MI (mecânico, e mecânico associado aos agentes químicos:
clorexidina, triclosan ou cloreto de cetilpiridínio), após 21 dias de aplicação. O
material biológico coletado do sulco peri-implantar foi submetido à análise
molecular por PCR real-time. Os resultados evidenciaram maior rugosidade na
superfície do perfil transmucoso da marca SIN®. As imagens de MEV e MF
demonstraram adesão, diversidade morfológica e viabilidade celular durante todo o
período experimental. Apesar da variedade de espécies detectadas pelo
“Checkerboard DNA-DNA hybridization”, os níveis bacterianos não apresentaram
diferença ao longo do ensaio. A avaliação dos quatro métodos propostos para
higienização do perfil transmucoso dos mini-implantes comprovou que o controle
microbiano é alcançado com a limpeza mecânica dos dispositivos, sem uso
adicional de agentes químicos.

xii
SUMMARY
FREITAS, Amanda Osório Ayres de. Aspectos microbiológicos associados aos
mini-implantes ortodônticos. Orientadoras: Profª. Drª. Matilde da Cunha
Gonçalves Nojima, Profª. Drª. Daniela Sales Alviano Moreno. Rio de Janeiro: UFRJ/
Faculdade de Odontologia, 2014. Tese (Doutorado em Odontologia- Ortodontia).
xxii, 121f.
The authors of this study evaluated the topography of the transmucosal neck
of orthodontic mini-implants (MI), the microbial adhesion and biofilm formation on
the devices surface and determined the most effective method for their microbial
control. For topography surface analysis of the transmucosal neck of MI,
photomicrographs and roughness scanning of three different brazilian trademarks
were performed by scanning electron microscopy (SEM), and atomic force
microscopy (AFM). After inoculation with dental plaque cultured in vitro, colected
from orthodontic patients, adhesion and biofilm formation were observed during a
seven day microbiological assay, by SEM and optical fluorescence microscopy (FM)
of MI transmucosal neck. Furthermore, to detect the number and the variety of
adhered micro-organisms, Checkerboard DNA-DNA hybridization was applied. The
in vivo study was developed to compare four hygiene protocols for MI, after 21 days
of usage. The biological material collected from peri-implant sulcus was submitted

xiii
to molecular analysis by real-time PCR. Results evidenced greater surface
roughness on transmucosal neck surface of SIN™. Images from SEM e MF showed
adhesion, morphological diversity and cellular viability at all experimental time.
Despite the variety of species detected by Checkerboard DNA-DNA hybridization,
bacterial levels did not present difference during the assay. The evaluation of the
four hygiene methods proposed for transmucosal neck of MI proved that microbial
control is acquired by mechanical cleaning of the devices, without adicional
chemical agents usage.

xiv
RESÚMEN
FREITAS, Amanda Osório Ayres de. Aspectos microbiológicos associados aos
mini-implantes ortodônticos. Orientadoras: Profª. Drª. Matilde da Cunha
Gonçalves Nojima, Profª. Drª. Daniela Sales Alviano Moreno. Rio de Janeiro: UFRJ/
Faculdade de Odontologia, 2014. Tese (Doutorado em Odontologia- Ortodontia).
xxii, 121f.
Los autores de este estudio evaluaron la topografía del perfil transmucoso
de mini-implantes ortodóncicos (MI), la adhesión microbiana en la superficie de
estos dispositivos y el método más eficaz para el control microbiano de los mismos.
Para el análisis de la topografía de la superficie del perfil transmucoso, fueron
realizadas fotomicrografías y lecturas de la rugosidad de tres marcas comerciales,
nacionales, por medio de microscopia electrónica de barrido (MEB) y microscopia
de fuerza atómica (MFA). Luego de la inoculación con placa dental cultivada in vitro,
colectada de pacientes en tratamiento ortodóncico, la adhesión y la formación del
biofilm fueron evaluadas en un ensayo microbiológico durante siete días a partir del

xv
MEV y microscopía óptica de fluorescencia (MF) del perfil transmucoso de los MI.
Además, para detectar la variedad y la cantidad de micro-organismos adheridos, se
aplicó el “Checkerboard DNA-DNA hybridization”. El estudio in vivo realizado
comparó cuatro protocolos de higienización de los MI (mecánico, y mecánico
asociado a los agentes químicos: clorhexidina, triclosán o cloruro de cetilpiridinio),
tras 21 días de aplicación. El material biológico colectado del surco peri-implantal
fue sometido a análisis molecular por medio de PCR real-time. Los resultados
evidenciaron mayor rugosidad en la superficie del perfil transmucoso de la marca
SIN®. Las imágenes de MEV y MF demostraron adhesión, diversidad morfológica
y viabilidad celular durante todo el período experimental. A pesar de la variedad de
especies detectadas por el “Checkerboard DNA-DNA hybridization”, los niveles
bacterianos no presentaron diferencia a lo largo del ensayo. La evaluación de los
cuatro métodos propuestos para higienización del perfil transmucoso de los mini-
implantes comprobó que el control microbiano se alcanza con la limpieza mecánica
de los dispositivos, sin el uso adicional de agentes químicos.

xvi
LISTA DE ILUSTRAÇÕES
DELINEAMENTO DA PESQUISA
Quadro 1 Relação das cepas bacterianas empregadas na confecção das
sondas de DNA………………………………………………...........
DESENVOLVIMENTO DA PESQUISA
ARTIGO 1
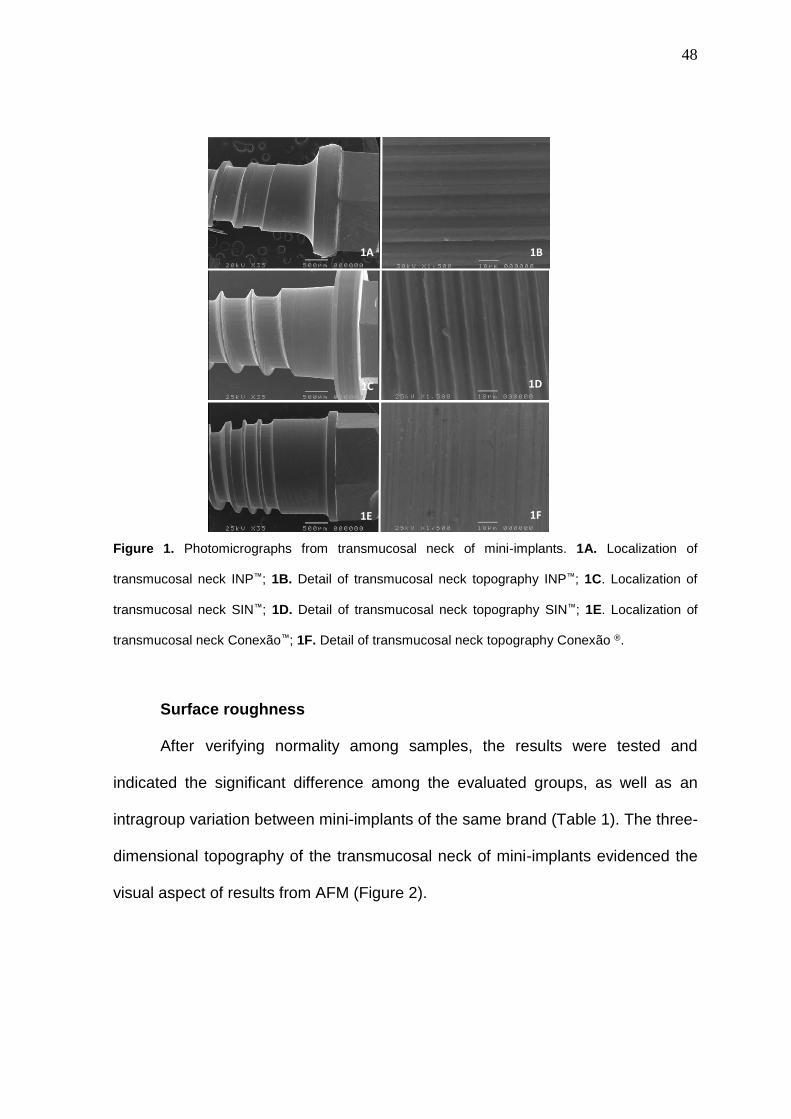
Figure 1 Photomicrographs from transmucosal neck of mini-implants. 1A.
Localization of transmucosal neck INP™; 1B. Detail of
transmucosal neck topography INP®; 1C. Localization of
transmucosal neck SIN™; 1D. Detail of transmucosal neck
topography SIN™; 1E. Localization of transmucosal neck
Conexão™; 1F. Detail of transmucosal neck topography
Conexão™. (a) Collection of the fluids from gingival sulcus (b)
Schematic design……………………………………………………
Página
36
48
Figure 2 Three-dimensional topography of the transmucosal neck of
mini-implants. 3A INPTM; 3B SINTM; CONEXÃOTM……………..
49

xvii
ARTIGO 2
Figure 1 Bacterial strains used for production of DNA probes…………….
Figure 2 Images of microbial adhesion and biofilm formation development
during experimental times. 1. 6h; 2. 12h; 3. 18h; 4. 24h; 5. 48h;
6. 72h; 7. 96h; 8. 120h; 9. 144h; 10. 168h. A. Fluorescence
microscopy 400X; B. Photomicrograph 1.200X; C.
Photomicrograph 5.000X.............................................................
Figure 3 Graphic representing the distribution of bacterial levels at
different experimental times; 0 (not detected); 1 (<105 cells); 2
(approximately 105); 3 (105–106); 4 (approximately 106), and 5
(>106 cells)…………………………………………………………..
62
64
66

xviii
LISTA DE TABELAS
DESENVOLVIMENTO DA PESQUISA Página
Artigo1
Table 1 Comparison of Ra values (nm) intra and between groups after
AFM………………………………………………………………..
49
Artigo 3
Table 1 Intragroup and intergroup comparison regarding changes in
the number of bacterial cells (log 10) detected at baseline (T1)
and final observation time (T2), according to the hygiene
protocol applied in the study……………………………………….
81
xix
LISTA DE ABREVIATURAS, SIGLAS E SÍMBOLOS
MI Mini-implantes / “Mini-implants”
DAT Dispositivo de Ancoragem Temporária
TAD “Temporary Anchorage Device”
MFA Microscopia de Força Atômica
AFM “Atomic Force Microscopy”
Ra média da rugosidade de superfície
MEV Microscopia Eletrônica de Varredura
SEM “Scanning Electron Microscopy”
MF Microscopia de Fluorescência
FM “Fluorescence Microscopy”
BHI “Bovine Brain Heart Infusion”/ Infusão de Cérebro e Coração Bovinos
UFC/mL Unidades Formadoras de Colônia por mililitro
PBS “Phosphate Buffer Solution”/ Solução Tampão de Fosfato
Tris-EDTA Solução tampão à base de EDTA (“Ethylenediamine Tetraacetic Acid”,
Ácido Etilenodiamino Tetra-Acético)
TE Tris-EDTA
Aa Actinomyces actinomycetemcomitans
PCR “Polymerase Chain Reaction”/ Reação em Cadeia da Polimerase
xx
GM Grupo Higienização Mecânica
MG “Mechanical Hygiene Group”
GC Grupo Clorexidina
CG “Chlorhexidine Group”
GT Grupo Triclosan
TG “Triclosan Group”
GCCP Grupo Cloreto de Cetilpiridínio
CPCG “Cetilpiridine Chloride Group”
mix mistura de reagentes
xxi
ÍNDICE
Página
1 INTRODUÇÃO............................................................................................... 23
2 PROPOSIÇÃO............................................................................................... 28
3
DELINEAMENTO DA PESQUISA .................................................................
3.2 METODOLOGIA PARA AVALIAÇÃO DA RUGOSIDADE DE
SUPERFÍCIE E TOPOGRAFIA DO PERFIL TRANSMUCOSO DE MINI-
IMPLANTES...................................................................................................
3.2 METODOLOGIA PARA OBSERVAÇÃO DA ADESÃO MICROBIANA
E FORMAÇÃO DE BIOFILME EM MINI-IMPLANTES................................
3.3 METODOLOGIA PARA DETERMINAÇÃO DO MÉTODO MAIS
EFICAZ NO CONTROLE MICROBIANO DO PERFIL TRANSMUCOSO DE
MINI-IMPLANTES ORTODÔNTICOS............................................................
29
29
31
38
4 DESENVOLVIMENTO DA PESQUISA .........................................................
4.1 ARTIGO 1: OSÓRIO A, SILVA DL, ALVIANO DS, ALVIANO CS,
NOJIMA MCG. Topography of mini-implant’s transmucosal neck: a
preliminary study. Artigo a ser submetido ao Brazilian Oral Research………..
4.2 ARTIGO 2: OSÓRIO A, BOGHOSSIAN C, LOURENÇO TBG,
COLOMBO APV, ALVIANO DS, NOJIMA MCG. Microbial adhesion and
43
44
xxii
biofilm formation in orthodontic mini-implants. Artigo a ser submetido ao
Clinical Oral Implants Research......................................................................
4.1 ARTIGO 3: OSÓRIO A, LEITE D, SOUTO RM, COLOMBO APV,
ALVIANO DS, NOJIMA MCG. Microbial control of orthodontic mini-implants.
Artigo a ser submetido ao American Journal of Orthodontics and Dentofacial
Orthopedics…………………………………………………………………………
55
76
5 DISCUSSÃO .................................................................................................. 93
6 CONCLUSÃO ................................................................................................ 102
7 RECOMENDAÇÕES ..................................................................................... 103
8 REFERÊNCIAS BIBLIOGRÁFICAS .............................................................. 104
9
ANEXOS ........................................................................................................
9.1 ANEXO 1 TERMO DE CONSENTIMENTO LIVRE E ESCLARECIDO
9.2 ANEXO 2 APROVAÇÃO DO COMITÊ DE ÉTICA .............................
9.3 ANEXO 3 PROTOCOLO DE HIGIENIZAÇÃO 1..................................
9.4 ANEXO 4 PROTOCOLO DE HIGIENIZAÇÃO 2..................................
9.5 ANEXO 5 PROTOCOLO DE HIGIENIZAÇÃO 3..................................
9.6 ANEXO 6 PROTOCOLO DE HIGIENIZAÇÃO 4..................................
9.7 ANEXO 7 ARTIGO 2, FIGURA 2 (PARTE 1)......................................
9.8 ANEXO 8 ARTIGO 2, FIGURA 2 (PARTE 2)......................................
112
112
115
116
117
118
119
120
121

23
1 INTRODUÇÃO
A ancoragem representa fator crítico para o sucesso do tratamento
ortodôntico (ALSAMAK et al, 2012; APEL et al, 2009; KYUNG et al, 2003). Diante
da praticidade e eficiência proporcionada pelos mini-implantes ortodônticos, estes
tornaram-se os dispositivos temporários de ancoragem (DTA) de escolha para a
substituição dos métodos tradicionais, como aparelhos extra-bucais, principalmente
em pacientes adultos (ALSAMAK et al, 2012; APEL et al, 2009; ARAÚJO et al,
2006; BAE et al, 2002; CELENZA e HOCKMAN, 2000; CHENG et al, 2004;
FREITAS et al, 2012; KANOMI, 2007; LUZI et al, 2009; MIYAWAKI et al, 2003;
RINALDI e ARANA-CHAVEZ, 2010; SINGH et al, 2010; TORTAMANO et al, 2012;
TSENG et al, 2006; WU e WU, 2009).
Os mini-implantes estão presentes na rotina da clínica ortodôntica (CHENG
et al, 2004; LUZI et al, 2009; LIOU et al, 2004; TORTAMANO et al, 2012; WILMES
et al, 2006). Fatores relacionados ao seu sucesso foram amplamente descritos na
literatura (APEL et al, 2009; CHENG et al, 2004; FREITAS et al, 2012;
TORTAMANO et al, 2012), como (estabilidade primária, definida como a
estabilidade do DTA imediatamente após sua inserção no tecido ósseo; critério do

24
profissional durante o procedimento cirúrgico; qualidade do osso hospedeiro e
região anatômica selecionada para a inserção do dispositivo. Para manutenção do
parafuso na cavidade bucal, destacam-se a influência da magnitude de força
aplicada, a presença de trauma e o controle de placa bacteriana ao redor do mini-
implante (ARAÚJO et al, 2006; LUZI et al, 2009; MAH e BUGSTRAND, 2005;
PITHON et al, 2008; SQUEFF et al, 2008; WILMES et al, 2006). Portanto, , os
fatores biológicos que interferem na estabilidade dos mini-implantes a longo prazo
também devem ser destacados; dentre os quais, ressalta-se a mucosite peri-
implantar (ARAÚJO et al, 2006; CARANO et al, 2005; CELENZA e HOCKMAN,
2000; FERREIRA JR et al, 2009; FREITAS et al, 2012; GRAY e SMITH, 2000;
HEUER et al, 2007; LUZI et al, 2009; MAH e BUGSTRAND, 2005; MELSEN, 2005;
MIYAWAKI et al, 2003; PIER-FRANCESCO et al, 2006; WILMES et al, 2006;
YOSHINARI et al, 2000).
Mini-implantes ortodônticos são usualmente constituídos de ligas de titânio,
visto suas excelentes propriedades mecânicas e de superfície, resistência à
corrosão e biocompatibilidade (ALSAMAK et al, 2012; SUBRAMANI et al, 2009;
STÁJER et al, 2012). Pesquisas comprovam que a rugosidade do material
representa fator importante para a adesão e consequente formação de biofilme
sobre a superfície destes dispositivos, além de interferir na remoção da placa dental
(AL-AHMAD et al, 2013; BURGÜERS et al, 2009; DORKHAN et al, 2012;
SCHMIDLIN et al, 2013; SUBRAMANI et al, 2009; STÁJER et al, 2012). Materiais
com superfícies mais polidas limitam a formação e progressão do biofilme (AL-
AHMAD et al, 2013; BURGÜERS et al, 2009; DORKHAN et al, 2012; SUBRAMANI
et al, 2009; STÁJER et al, 2012). A presença de irregularidades favorece a

25
colonização, pois protege as bactérias da força de limpeza do fluxo salivar, da
mastigação, deglutição e dos procedimentos de higienização, permitindo o
estabelecimento de ligações menos reversíveis entre os micro-organismos
presentes no biofilme (RIMONDINI et al, 1997; THEUGHELS et al, 2006).
Após a inserção do dispositivo transitório de ancoragem e a sua exposição
ao meio bucal, inicia-se a formação da película adquirida, que promove a adesão
entre micro-organismos iniciadores e a superfície do implante. Estas bactérias são
capazes de criar as condições necessárias para a adesão de outros micro-
organismos, inclusive patógenos periodontais (BODET et al, 2007; HEUER et al,
2007; LUZI et al, 2009).
A região peri-implantar, mais especificamente a área de sulco formada entre
o perfil transmucoso dos mini-implantes ortodônticos e a gengiva inserida
adjacente, corresponde à área que permanece em contato justo com os tecidos
moles. Espera-se que ocorra o selamento adequado da mucosa nesta área,
protegendo o sulco peri-implantar do ataque bacteriano e das influências do meio
bucal (LEE e WANG, 2010; STÁJER et al, 2012). Porém, a região do mini-implante
exposta é de fácil acúmulo de placa microbiana e a área peri-implantar, pelo acesso
clínico restrito, oferece maior dificuldade de higienização (APEL et al, 2009;
FREITAS et al, 2012). A evolução na formação de biofilme sobre o mini-implante
pode resultar na inflamação da mucosa adjacente e consequente perda de
estabilidade do dispositivo (ARAÚJO et al, 2006; BODET et al, 2007; CARANO et
al, 2005; CELENZA e HOCKMAN, 2000; DRAKE et al, 1999; FERREIRA JR et al,
2009; GRAY e SMITH, 2000; HEUER et al, 2007; LUZI et al, 2009; MAH e
BUGSTRAND, 2005; MELSEN, 2005; MINEOKA et al; 2008; PIER-FRANCESCO
et al, 2006; YOSHINARI et al, 2000; WILMES et al, 2006).

26
Um dos fatores de risco para inflamação peri-implantar está relacionado à
composição da microbiota constituinte e quantidade de placa bacteriana ao redor
do implante (GERBER et al, 2006; HEUER et al, 2007; MOMBELLI et al, 1993;
PIER-FRANCESCO et al, 2006; POGNARISON et al, 2007; TRAN e RUDNEY,
1996). As bactérias mais comumente associadas à inflamação peri-implantar são
aquelas relacionadas à doença periodontal: Prevotella intermedia, Porphyromonas
gingivalis, Actinobacillus actinomycetemcomitans; Bacteroides forsythus,
Treponema denticola, Prevotella nigrescens e Fusobacterium nucleatum (BOTERO
et al, 2005; FERREIRA JR et al, 2009; GERBER et al, 2006; HEUER et al, 2007;
HARTROTH et al, 1999; KURAMITSU et al, 2005; KAWADA et al, 2004; MINEOKA
et al; 2008; MARTÍNEZ-PABÓN et al, 2008; MOMBELLI et al, 1993; PIER-
FRANCESCO et al, 2006; POGNARISORN et al, 2007; SANTOS et al, 2002; TRAN
e RUDNEY, 1999). Esses micro-organismos são frequentemente detectados em
indivíduos com periodontite, embora também possam ser identificados, com menor
regularidade e em menor quantidade, em pacientes que possuem periodonto
saudável. Sendo assim, a manutenção da integridade dos tecidos adjacentes ao
implante está relacionada ao equilíbrio parasita-hospedeiro (resposta imune do
hospedeiro ao acúmulo de placa bacteriana) e, não somente à presença ou
ausência desses micro-organismos (BASTANCI et al, 2009; BODET et al, 2007;
BOTERO et al, 2005; COLOMBO et al, 2002; CORTELLI et al, 2008; GERBER et
al, 2006; GOSAU et al, 2010; HALLÉN et al, 2008; HEUER et al, 2007; INABA et al,
2008; ISHIGURO et al, 2009; KOLENBRANDER e ANDERSEN, 1989;
KURAMITSU et al, 2005; MARTÍNEZ-PABÓN et al, 2008; MINEOKA et al; 2008;
NAKANO et al, 2004; PASTER et al, 2001; PIER-FRANCESCO et al, 2006;
27
POGNARISORN et al, 2007; RIEP et al, 2009; VERNAL et al, 2009; YOSHINARI et
al, 2000).
Diante das propriedades de superfície dos dispositivos à base de titânio, do
ambiente ao qual estes são submetidos edas características individuais de cada
hospedeiro, alguns métodos de higienização paramini-implantes já foram
propostos, especialmente com a aplicação de agentes químicos (ARAÚJO et al,
2006; APEL et al, 2009; FREITAS et al, 2012; GOSAU et al, 2010; STÁJER et al,
2012). Apesar do consenso sobre a necessidade da redução dos fatores que
podem facilitar a adesão e formação de biofilme, ainda não foi definido pela
comunidade científica qual seria o método mais eficaz para o controle microbiano
dos mini-implantes na clínica ortodôntica.
Evidenciadaa importância dos fatores biológicos na permanência dos MI na
cavidade bucal, sustenta-se a necessidade da investigação destes, antes que haja
prejuízo aos tecidos adjacentes e consequente perda dos dispositivos de
ancoragem temporária.
28
2 PROPOSIÇÃO
Determinar os aspectos microbiológicos influentes na permanência dos mini-
implantes ortodônticos na cavidade bucal através de:
2.1 análise topográfica da superfície do perfil transmucoso de três mini-
implantes de fabricação brasileira;
2.2 acompanhamento do processo de evolução da adesão microbiana e
formação de biofilme, in vitro, na superfície de mini-implantes;
2.3 avaliação, in vivo, de quatro métodos de controle microbiano do perfil
transmucoso de mini-implantes.

29
3 DELINEAMENTO DA PESQUISA
3.1 METODOLOGIA PARA AVALIAÇÃO DA RUGOSIDADE DE SUPERFÍCIE
E TOPOGRAFIA DO PERFIL TRANSMUCOSO DE MINI-IMPLANTES
A avaliação preliminar da rugosidade de superfície e topografia do perfil
transmucoso de marcas comerciais diferenciadas de mini-implantes nacionais
determinou o dispositivo utilizado no experimento in vitro
3.1.1 CARACTERIZAÇÃO DA AMOSTRA
Foram selecionadas três marcas comerciais de mini-implantes nacionais:
SIN® (São Paulo, SP, Brasil); INP® (São Paulo, SP, Brasil) e Conexão® (Arujá, SP,
Brasil), todos constituídos de Ti6 Al4 V, tipo auto perfurante, com 1,0 mm de perfil
transmucoso. Para determinação do número amostral, foi realizado um estudo
piloto, que apontou a necessidade de três mini-implantes de cada fabricante para
que fosse detectada a diferença entre as respectivas marcas em cada análise
realizada na presente investigação.
3.1.2 ANÁLISE DA TOPOGRAFIA DO PERFIL TRANSMUCOSO DE MINI-
IMPLANTES
Fotomicrografias obtidas a partir de microscopia eletrônica de varredura
(MEV) (Equipamento JEOL-JSM, 6460LV, Tóquio, Japão) evidenciaram detalhes
da área de interesse das diferentes marcas utilizadas no estudo.
30
O material avaliado não indicou a necessidade de preparo prévio para a
análise, visto quea composição metálica atendia às demandas exigidas pela
técnica.
3.1.3 ANÁLISE DA RUGOSIDADE DE SUPERFÍCIE DO PERFIL
TRANSMUCOSO DE MINI-IMPLANTES
Os dispositivos utilizados foram fixados em lâminas de vidro com auxílio de
cera utilidade (Wilson, Polidental Indústria e Comércio Ltda., Cotia, SP), de modo
que a superfície do perfil transmucoso permanecesse paralela à lâmina. Para
viabilizar a leitura, foi necessária a remoção do colar entre a cabeça do mini-
implante e o perfil transmucoso.
No microscópio de força atômica (Equipamento JPK Nanowizard, modelo
Nr: H-01-0086, Berlim, Alemanha), com ponta revestida de silício (NanoWorld,
NCLR-20, Neuchâtel, Suíça), em modo não contato, haste de frequência de
ressonância de 190 kHz e constante de força de 48 N/mm (SILVA et al, 2013) foram
realizadas, 27 leituras: três por mini-implante, aproximadamente, a cada 0,3 mm.As
imagens originadas foram processadas a partir do software (JPK Image Processing,
versão 3.0, JPK instruments) para visualização da topografia tridimensional dos
perfis transmucosos, assim como para determinação do valor da rugosidade da
superfície (Ra) dos mesmos (SILVA et al, 2013).
3.1.4 ANÁLISE ESTATÍSTICA
A avaliação das fotomicrografias foi realizada por inspeção visual e descritiva
da superfície do perfil transmucoso dos mini-implantes.
31
Aos resultados obtidos a partir da microscopia de força atômica (MFA) foram
aplicados os métodos de análise estatística descritiva, além da comparação entre
os valores de rugosidade de superfície. Diante da distribuição normal da amostra,
detectada pelo teste Kolmogorov- Smirnov, foram utilizados os testes T-Student
para determinar a diferença intragrupos e ANOVA complementado pelo Post-Hoc
Tukey para diferenças intergrupos. Todo o desenvolvimento estatístico foi realizado
no “software” SPSS 17.0 (Statistical Package for Social Sciences; SPSS Inc.,
Chicago, IL, USA). A significância estatística adotada foi ao nível de 5%.
3.2 METODOLOGIA PARA OBSERVAÇÃO DA ADESÃO MICROBIANA E
FORMAÇÃO DE BIOFILME NOS MINI-IMPLANTES
Quarenta mini-implantesforam submetidos ao ensaio microbiológico in vitro,
desde 6 horas até 7 dias após a inoculação em meio de cultura obtido a partir da
coleta de placa supragengival doada por pacientes em tratamento ortodôntico na
Clínica do Programa de Pós-Graduação em Odontologia (Ortodontia) da
Universidade Federal do Rio de Janeiro. A marca comercial escolhida para este
experimento foi a que apresentou maior rugosidade de superfície no estudo
preliminar: SIN® (São Paulo, SP, Brasil). As observações foram realizadas porMEV,
microscopia de fluorescência (MF) e “Checkerboard DNA-DNA Hybridization”.
Os 40 mini-implantes foram distribuídos em duas placas de 24 poços de
acordo com os tempos de análise. Nas primeiras 24 horas, foram realizadas
análises a cada seis horas e, a partir desse tempo, com intervalo de 24 horas, até
serem completados os sete dias de avaliação. Foram utilizados quatro dispositivos
temporários de ancoragem para cada tempo de observação, sendo dois para
análise molecular, um para visualização em MEV e um para MF.

32
3.2.1 OBTENÇÃO DO INÓCULO
Doze pacientes, adultos jovens, de ambos os gêneros, em tratamento
ortodôntico na Clínica do Programa de Pós-Graduação em Odontologia
(Ortodontia) da Universidade Federal do Rio de Janeiro doaram placa
supragengival. Foram estabelecidos critérios de exclusão, como: presença de
doenças sistêmicas, antibioticoterapia recente (6 meses anteriores ao início do
período de coleta) e mulheres gestantes. Todos os participantes deram ciência ao
Termo de Consentimento Livre e Esclarecido (Anexo 1, página 112), previamente
aprovado pelo Comitê de Ética em Pesquisa do Instituto de Estudos em Saúde
Coletiva da Universidade Federal do Rio de Janeiro (Anexo 2, página 115). A coleta
foi realizada em tempo único, durantea consulta de rotina do tratamento
ortodôntico. Para tal, ambos os arcos foram mantidos em isolamento relativo com
roletes de algodão, secos com jato de ar comprimido emitido por seringa tríplice.
Em seguida, a placa supragengival foi coletada com auxílio de sonda exploradora
# 5esterelizada (ref. 11511, Duflex ®, SS White ®, RJ, Brasil), removendo-se o
material presente na superfície dentária ao redor das margens dos acessórios
colados, constituintes da aparelhagem ortodôntica fixa.
O material obtido foi depositado em tubos Eppendorf® com 1mL de solução
salina redutora estéril, composta por 0,85% de cloreto de sódio e 1% de tioglicolato
de sódio. Os tubos foram pesados antes e após a coleta da placa supragengival
para determinar a massa de material coletado. Em seguida, o material foi
transferido para caldo de BHI (Brain Heart Infusion, Himedia) suplementado com
sacarose 3%, hemina 5 µg/mL e menadione 10 µg/mL, mantendo-o incubado por 7
dias, a 37 ºC, em jarra de anaerobiose.

33
Após a incubação, foi realizada a leitura da densidade óptica do inóculo no
espectrofotômetro (Beckman Coulter DU 530 Spectrophotometer), a qual
correspondeu a 1,5 x 108 UFC/mL, usando os valores da escala de McFarland como
referência.
3.2.2 SENSIBILIZAÇÃO DOS MINI-IMPLANTES
Os mini-implantes foram sensibilizados com 200 µl saliva 10% (PBS),
durante 2h, sob agitação (WALKER et al, 2010). Em seguida, foram acondicionados
nas placas de 24 poços para inoculação.
3.2.3 INOCULAÇÃO DOS MINI-IMPLANTES
Foi respeitada a proporção de 500 µl de meio de cultura (BHI suplementado
com sacarose 3%, hemina 5 µg/mL e menadiona 10 µg/mL) para 500 µl de inóculo
preparado. O meio de cultura foi renovado a cada 48 horas após as primeiras 72
horas de incubação (SÁNCHEZ et al, 2011). Em cada placa havia dois poços
disponíveis para o controle negativo, que possuíam 1mL de meio de cultura puro.
Em cada tempo de avaliação no decorrer do estudo, cada mini-implante foi
preparado de acordo com a técnica de análise empregada.
3.2.4 MICROSCOPIA ELETRÔNICA DE VARREDURA
Para a microscopia eletrônica de varredura, os mini-implantes foram lavados
em PBS, suavemente secos em gaze estéril e fixados com glutaraldeído 2,5% em
tampão cacodilato 0,1 M, por 24h. Em seguida, foram novamente lavados em PBS,
secos e montados em “stubs” de alumínio. Por meio de pulverização catódica, os

34
DTA foram revestidos com ouro e levados ao microscópio (Quanta FEG 400; FEI
Company, Eindhoven, Holanda).
3.2.5 MICROSCOPIA DE FLUORESCÊNCIA
Após a contaminação, cada mini-implante foi lavado com solução salina
redutora estéril, composta por 0,85% de cloreto de sódio e 1% de tioglicolato de
sódio e, em seguida, inserido em tubo Eppendorf® contendo 300 µL da mesma
solução. Os reagentes do “kit” LIVE/DEAD® BacLight (Molecular Probes –
Invitrogen. Eugene, Oregon, EUA), utilizados para avaliar viabilidade bacteriana,
foram preparados pela mistura dos seus dois componentes: SYTO 9 (A) para
células viáveis e Iodeto de propidium (B) para células inviáveis. Alíquotas de 0,5 µL
de cada reagente foram acrescentadas a cada tubo Eppendorf® contendo o mini-
implante e a solução salina. Posteriormente, o conjunto foi mantido no escuro,
durante 15 minutos, à temperatura ambiente.
Em seguida, os mini-implantes foram fixados em lâmina de vidro com
esmalte incolor (Colorama®, São Paulo, SP) e a emissão de fluorescência foi
detectada pelo microscópio (Axiovert® 200M; Carl Zeiss Microlmaging GmbH,
Göttingen, Alemanha). As imagens geradas foram captadas por câmera digital
acoplada (Axiocam MRc5/MRm; Carl Zeiss Microlmaging GmbH) e trabalhadas no
software AxioVision 4.6 (Carl Zeiss Microlmaging GmbH).
35
3.2.6 “CHECKERBOARD DNA-DNA HYBRIDIZATION”
As bactérias aderidas à superfície dos MI foram identificadas e semi-
quantificadas a partir da adaptação da técnica previamente descrita na literatura
(COLOMBO et al, 2002; 2005; LOURENÇO, 2011; SOCRANSKY et al,1994).
Os mini-implantes foram lavados com PBS após a incubação e, em seguida,
inseridos em tubo Eppendorf® contendo 150 µL da solução 10 Mm Tris, 1Mm EDTA
e água destilada (TE) estéril para agitação em vórtex. Após a liberação das células
aderidas aos mini-implantes para a solução, foram acrescidos 150 µL de 0,5 M de
NaOH. Em seguida, aqueceu-se a solução (100°C em banho-maria por 5 min) para
promover lise celular e liberação do material genético presente. O DNA em
suspensão foi neutralizado pela adição de 0,8 mL de 5 M de acetato de amônia. As
amostras foram inseridas nas canaletas do “Minislot” (Immunetics, Cambridge, MA,
EUA), sob o qual encontrava-se a membrana de nylon (15 X 15 cm) com carga
positiva (Hybond-N+, GE Healthcare Life Sciences, Piscataway, NJ, EUA), para
deposição do DNA. Após a remoção do aparato, a membrana foi submetida à
temperatura de 120°C por 20 min em forno (Fanem Ltda., São Paulo, SP), para
fixação do DNA da amostra na mesma. As duas últimas canaletas do “Minislot”
foram preenchidas com a mistura das espécies bacterianas que deram origem às
sondas de DNA de interesse, em concentrações de 105 e 106 células/mL
(LOURENÇO, 2011).
Em seguida, foi realizada a pré-hibridização da membrana em solução de
50% de formamida, 1% de caseína, 5 x SSC, 25 mM de fosfato de sódio (pH 6,5) e
0,5 mg/mL de RNA de levedura, por uma hora, a 42C. A membrana pronta foi
posicionada sob a placa acrílica do “Miniblotter” 45 (Immunetics, Cambridge, MA,

36
EUA) de maneira que o DNA fixado estivesse perpendicular às canaletas do
aparato (LOURENÇO, 2011).
Foram preparadas 40 sondas específicas para 43 espécies bacterianas
(Quadro1, página 33), através do Kit DIG-High Prime (Roche Brasil, São Paulo, SP,
Brasil). Os sorotipos “a”, “b” e “c” da espécie Aa foram agrupados em sonda única
(LOURENÇO, 2011).
As diversas sondas específicas foram diluídas em solução de hibridização,
composta por 45% de formamida, 5 X SSC, 20 mM de fosfato de sódio (pH 6,5),
0,2 mg/mL de RNA de levedura, 10% de sulfato de dextrano, 1% de caseína, e
mantidas na concentração de 20 ng/mL. Deste modo, alíquotas de 135 L das
sondas específicas de DNA foram pipetadas em cada canaleta do “MiniBlotter” 45
(Immunetics, Cambridge, MA, EUA). A hibridização das sondas com o material
genético da amostra foi efetuada a partir da incubação do aparato por 16 horas, a
42 °C (LOURENÇO, 2011).
Espécie Cepa* Espécie Cepa*
Aggregatibacter actinomycetemcomitans a 43718 Leptotrichia buccalis 14201
Aggregatibacter actinomycetemcomitans b 29523 Neisseria mucosa 19696
Aggregatibacter actinomycetemcomitans c 625** Porphyromonas gingivalis 33277
Actinomyces gerensceriae 23860 Prevotella intermedia 25611
Actinomyces israelli 12102 Prevotella melaninogenica 25845
Actinomyces odontolyticus 17929 Prevotella nigrescens 33563
Actinomyces naeslundii 12104 P. micra 33270
Actinomyces viscosus 43146 Propionibacterium acnes I 11827
Capnocytophaga gingivalis 33624 Propionibacterium acnes II 43541
Capnocytophaga ochracea 33596 Streptococcus anginosus 33397
Capnocytophaga sputigena 33612 Streptococcus constellatus 27823
Campylobacter concisus 33237 Streptococcus mitis 49456
Campylobacter rectus 33238 Streptococcus intermedius 27335
Campylobacter showae 51146 Streptococcus noxia 43541
Eubacterium nodatum 33099 Streptococcus oralis 35037
Eubacterium saburreum 33271 Streptococcus sanguinis 10556
Eikenella corrodens 23834 Streptococcus gordonii 10558

37
Fusobacterium periodonticum 33693 Tannerella forsythia 43037
Fusobacterium nucleatum ss. vincentii 49256 Treponema denticola B1**
F. nucleatum ss nucleatum 25586 Treponema socranskii S1**
F. nucleatum ss polymorphum 10953 Veillonella parvula 10790
Gemella morbilorum 27824
*ATCC (American Type Culture Collection, Rockville, MD, EUA), **The Forsyth Institute, (Boston, MA, EUA),
Cores correspondentes aos complexos microbianos da placa supragengival.
Quadro 1. Relação das cepas bacterianas empregadas na confecção das sondas de DNA.
As sondas fracamente hibridizadas foram removidas da membrana após
lavagem em solução adstringente (0,1 X SSC, 0,1% SDS) por 40 min, a 65C.
Postreriormente, a membrana foi mantida em solução bloqueadora durante uma
hora (0,1 M ácido maleico, 3 M NaCl, 0,2 M NaOH, 0,3% Tween 20, 0,5% caseína,
pH 8,0) e mais 30 min nesta solução acrescida de anticorpo anti-digoxigenin-AP
1/25.000 (Roche, São Paulo, SP, Brasil), para manutenção das ligações já
realizadas. Em seguida, a membrana foi lavada duas vezes por 15 min em solução
tampão (0,1 M ácido maleico, 3 M NaCl, 0,2 M NaOH, 0,3% Tween 20, pH 8,0), e
uma vez por 5 min em solução 0,2 M de dietanolamina (pH 9,5) e 2 mM MgCl2. Por
fim, a membrana foi sensibilizada pelo substrato fluorescente da solução detectora
(ECF, GE Healthcare Life Sciences). A membrana foi escaneada e a imagem
captada pelo Sistema de Imagens Storm TM 860 (Molecular Dynamics, GE
Healthcare Life Sciences) (BOGHOSSIAN et al, 2011; LOURENÇO, 2011).
A análise da imagem foi realizada por comparação visual com a intensidade
dos sinais emitidos pelos controles de 105 e 106 células bacterianas das espécies
avaliadas na membrana. Os sinais foram ranqueados como: 0: não detectado; 1:
<105 células; 2: ~105 células; 3: 105-106 células; 4: ~106 células; 5: >106 células. A
ausência de sinal, determinada como zero não caracteriza a inexistência de células

38
bacterianas, as quais poderiam estar presentes no níveis entre 1-1.000, já que a
sensibilidade do ensaio foi ajustada para detecção de 104 células (BOGHOSSIAN
et al, 2011; LOURENÇO, 2011).
3.2.7 ANÁLISE ESTATÍSTICA
No intuito de avaliar se houve diferença estatística significante entre os níveis
de detecção dos micro-organismos (score de 0-5) ao longo do tempo, foi aplicado
o teste de Kruskal-Wallis. A distribuição dos níveis de prevalência de cada micro-
organismo ao longo do tempo foi representada em gráfico.
3.3 METODOLOGIA PARA DETERMINAÇÃO DO MÉTODO MAIS EFICAZ
NO CONTROLE MICROBIANO DO PERFIL TRANSMUCOSO DE MINI-
IMPLANTES ORTODÔNTICOS
O estudo in vivo comparou quatro dos principais procedimentos de
higienização utilizados pelos pacientes, através da análise quantitativa por reação
em cadeia da polimerase (PCR) em tempo real.
Os indivíduos selecionados para esta pesquisa eram adultos e adultos-
jovens, de ambos os gêneros, os quais encontravam-se em tratamento ortodôntico
na Clínica do Programa de Pós-Graduação em Odontologia (Ortodontia) da
Universidade Federal do Rio de Janeiro. Os critérios de exclusão estabelecidos
foram: presença de doenças sistêmicas, antibioticoterapia recente (6 meses
anteriores ao início do período de coleta) e mulheres gestantes. Todos os
participantes deram ciência ao Termo de Consentimento Livre e Esclarecido (Anexo
1, página 112). O projeto de pesquisa foi previamente aprovado pelo Comitê de

39
Ética em Pesquisa do Instituto de Estudos em Saúde Coletiva da Universidade
Federal do Rio de Janeiro, sob parecer n0 149/2011 (Anexo 2, página 115).
Dentre 42 pacientes que possuíam mini-implantes instalados na cavidade
bucal, 39 participaram e contribuíram com 59 dispositivos temporários de
ancoragem, variando em quantidade de um a quatro MI por indivíduo. Estes
pacientes foram divididos, aleatoriamente, em quatro grupos, correspondentes aos
métodos de higienização aplicados: mecânico (GM) e mecânico associado ao
químico, complementado porcolutórios bucais à base de clorexidina (GC), triclosan
(GT) ou cloreto de cetilpiridínio (GCCP). Para padronizar o controle microbiano, os
participantes foram orientados e receberam o protocolo de higienização a ser
seguido por escrito (Anexos 3, 4, 5 e 6, páginas 116, 117, 118 e 119).
3.3.1 COLETA DO MATERIAL BIOLÓGICO
Após isolamento relativo com roletes de algodão, remoção de placa
supragengival com gaze estéril, aplicação de jato de ar ao redor da cabeça dos
mini-implantes e da superfície dentária adjacente, o material de interesse foi
coletado da área de sulco formado pelo perfil transmucoso e a gengiva inserida, a
partir da introdução de quatro cones de papel absorventes # 40 estréreis (ENDO
POINTS®, Manacapuru, AM, Brasil) durante 45 segundos (BOTERO et al, 2005;
FERREIRA JR et al, 2009; FREITAS, 2011; GERBER et al, 2006; HARTROTH et
al, 1999; JERVOE-STORM et al, 2007; MORIKAWA et al, 2008; NARANJO et al,
2006; SAKAMOTO et al, 2001).
Estes procedimentos foram realizados no tempo inicial (“baseline”) e 21 dias
após o início da terapêutica (tempo final).
40
Todo material coletado foi armazenado em tubos do tipo Eppendorf® com
capacidade para 1,5 ml, contendo 50 µl de Tris EDTA e mantido a -20°C até o
processamento laboratorial (ROÇAS et al, 2002).
3.3.2 EXTRAÇÃO DO DNA DO MATERIAL BIOLÓGICO
Após o descongelamento, os tubos foram agitados em vórtex por 60
segundos e os quatro cones de papel foram removidos, restando apenas o material
biológico.
O DNA foi extraído segundo o método da Proteinase K (SMITH et al, 1989).
Após a centrifugação do material, o pellet foi preservado e foram adicionados 44 µL
de TE, 5 µL de Tween 20 5% e 1 mL de 10 mg/mL de Proteinase K. Assim, obteve-
se o volume total de 50 µL de solução para reação. O material extraído foi
quantificado por espectrofotometria a fim de viabilizar a padronização da alíquota
de DNA utilizada na reação (NanoDrop® 2000, Thermo Scientific, Waltham, MA,
EUA).
3.3.3 ANÁLISE QUANTITATIVA POR PCR EM TEMPO REAL
Para avaliar os métodos de higienização indicados anteriormente, foi
realizada a quantificação total de bactérias presentes na área de sulco peri-
implantar nos tempos inicial e final determinados no estudo. O PCR em tempo real
foi conduzido com os reagentes do Power SYBER Green PCR Master Mix (Applied
Biosystems, Foster City, CA, EUA), em 20 µL de reação. Os primers universais
utilizados foram descritos por ASAI e colaboradores (2002) (5’ - GAT TAG ATA
CCC TGG TAG TCC AC – 3’ e 5’ – TAC CTT GTT ACG ACT T – 3’) Deste volume,
as alíquotas para todas as reações foram de 5 µL (3 ng/mL) de DNA da amostra,
10 µL de MIX, 0,4 µL de cada primer, 0,4 µL de ROX (1:10) para correção de
41
variações de volume e evaporação ao longo da reação, assim como 3,8 µL de água
ultra pura para PCR. As reações foram dispostas em placas de 96 poços, seladas,
centrifugadas e inseridas na termocicladora para amplificação. As reações foram
submetidas aos seguintes ciclos: 1 ciclo de 95ºC/10min; 40 ciclos de 95ºC/1min, 40
ciclos de 52ºC/1min e 40 ciclos de 72ºC/1min. As amplificações da PCR foram
medidas a 78 ºC. A cada ciclo, a fluorescência do corante repórter foi monitorada
(PAIVA et al, 2013).
Para que os resultados das reações fossem aferidos, curvas-padrão,
constituíramreferência para interpretação dos dados. As curvas-padrão utilizadas
neste estudo possuíam relação de 1:1 entre o número de cópias obtidas e o número
de células bacterianas presentes na amostra investigada. Essas foram descritas
por PAIVA e colaboradores (2013), apresentando variação na concentração de 102
até 107, tendo, como base, o DNA extraído da cepa de Enterococcus Faecalis
ATCC 29212. Ao mesmo tempo em que a reação ocorreu, os sinais emitidos foram
transcritos em gráficos e os valores numéricos obtidos resultaram de cálculo
matemático realizado pelo software v2.0.4 ABI 7500 (Applied Biosystems, Foster
City, CA, EUA).
3.3.4 ANÁLISE ESTATÍSTICA
O tratamento estatístico dos dados obtidos foi realizado com auxílio do
software SPSS 17.0 (Statistical Package for Social Sciences; SPSS Inc., Chicago,
IL, USA), através da análise descritiva dos resultados, com determinação de
valores de média e desvio-padrão. Diante da normalidade dos dados, evidenciada
pelo teste Kolmogorov-Smirnov, foram aplicados os testes T-Student pareado para

42
avaliação intragrupos e ANOVA com Post-Hoc Tukey para detectar diferença
intergrupos. A significância estatística adotada foi ao nível de 5%.
43
4 DESENVOLVIMENTO DA PESQUISA
4.1 ARTIGO 1
OSÓRIO A, SILVA DL, ALVIANO DS, ALVIANO CS, NOJIMA MCG. Topography
of mini-implant’s transmucosal neck: a preliminary study. Artigo a ser submetido
ao Brazilian Oral Research no American Journal of Orthodontics and Dentofacial
Orthopedics.
4.2 ARTIGO 2
OSÓRIO A, BOGHOSSIAN C, LOURENÇO TBG, COLOMBO APV, ALVIANO
DS, NOJIMA MCG. Microbial adhesion and biofilm formation in orthodontic mini-
implants. Artigo a ser submetido ao Clinical Oral Implants Research.
4.3 ARTIGO 3
OSÓRIO A, LEITE D, SOUTO RM, COLOMBO APV, ALVIANO DS, NOJIMA
MCG. Microbial control of orthodontic mini-implants. Artigo a ser submetido ao
American Journal of Orthodontics and Dentofacial Orthopedics.
44
4.1 ARTIGO 1
OSÓRIO A, SILVA DL, ALVIANO DS, ALVIANO CS, NOJIMA MCG. Topography of
mini-implant’s transmucosal neck: a preliminary study. Artigo a ser submetido ao
Brazilian Oral Research.
Abstract
The authors aimed to analyze the topography of the transmucosal neck of three
different brazilian orthodontic mini-implants. Nine samples were used to evaluate
the surface topography by scanning electron microscopy (SEM). The surface
roughness was determined by atomic force microscopy (AFM). Twenty seven
lectures were made and the results were submitted to descriptive statistics and intra
and inter-group comparisson. The photomicrographs from SEM and the three-
dimensional images produced from AFM were visually analyzed. Results indicated
statistical difference among surface roughness of evaluated groups, as well as the
variation among values from mini-implants of the same brand. Photomicrographs
and three dimensional images also showed the visual difference among mini-
implants of the same and the different brands. According to the transmucosal neck
charactherstics, SIN® (São Paulo, SP, Brazil) presented roughest surface when
compared to Conexão® (Arujá, SP, Brazil) and INP® (São Paulo, SP, Brazil). The
last brand also presented great variation of surface roughness among the mini-
implants studied herein.

45
Keywords
Surface characteristics; surface properties; orthodontic anchorage procedures.
INTRODUCTION
Anchorage control represents a critical factor for successful orthodontic
treatment 1-3. Orthodontic mini-implants became popular due to their simple use,
success rates and independence of patients cooperation. Therefore, these implants
were ellected for substitution of traditional anchorage devices, as headgears,
especially in adult patients 1,2,4-18.
Titanium alloys are widely used in orthodontic mini-implants constitution due
to their excelent mechanical properties, surface characteristics, corrosion resistance
and biocompatibility 1,19, 20. However, recent studies proved that surface roughness
represents an important factor for bacterial adhesion and biofilm formation, thus
interferes with the surface cleaning 19-25. Irregularities on the material surface harbor
microorganisms from forces of salivary flow and clearance, chewing, swallowing and
hygiene procedures 26, 27. For long-term permanence of the temporary anchorage
devices, it is necessary to control biofilm formation around them and the adjacent
mucosa8. Then, rough transmucosal neck of mini-implants facilitate bacterial
colonization in the peri-implant area, and can interfere in its health leading to
mucosal seal failure 8,19-23.
According to this issue, the purpose of the present study was to analyze the
topography of the transmucosal neck of orthodontic mini-implants by scanning
electron microscopy and determine the surface roughness by atomic force
microscopy.

46
MATERIALS AND METHODS
Samples Characterization
Self-drilling Ti6 Al4 V alloy mini-implants from three brazilian brands were
selected for this study: SIN™ (São Paulo, SP, Brazil), INP™ (São Paulo, SP, Brazil),
and Conexão™ (Arujá, SP, Brazil), all with 1.0 mm transmucosal neck. A pilot study
detected the need for three mini-implants from each manufacturer to determine the
statistical difference among the samples.
Surface topography
Three mini-implants from each brand were used to evaluate the surface
topography of their transmucosal neck. Photomicrographs obtained from scanning
electron microscope (SEM; JEOL-JSM, 6460LV, Tokio, Japan) evidenced details
from the interest area.
The samples were observed as-recieved, since they were made of metallic
material and met the criteria required by the applied technique.
Surface roughness
Following the proposed, three mini-implants of each brand were evaluated.
After the removal of the collar, the devices were fixed on a glass slide with segment
of wax, so that the transmucosal neck was parallel to the glass slide 24.
Measures were obtained from atomic force microscopy (AFM; JPK Nano
Wizard, Nr: H-01-0086, Berlin, Germany). In total, nine measurements of each
brand were made (three of each sample). The scanning areas were 20 µm x 20 µm,
with intervals of approximately 0.3 mm, from the limit between the collar and the

47
transmucosal neck to the limit between that and the active portion of the screw.
Values of the arithmetic average roughness (Ra) and the three-dimensional
topography of the transmucosal neck of mini-implants were processed by a specific
software (JPK Image Processing, versão 3.0, JPK instruments) 24.
Data analysis
Topographic analysis of transmucosal neck surface was described after
macroscopic and visual observation of photomicrographs and three-dimensional
images.
Data from AFM were subjected to SPSS 17.0 (Statistical Package for Social
Sciences; SPSS Inc., Chicago, IL, USA). Descriptive statistical analysis was
applied, as well as Kolmogorov- Smirnov test to detect normality among samples.
Then, Ra values were submitted to ANOVA and Tukey post-hoc test to identify the
diferences among the tested variables. The significance level was set at 5%.
Results
Surface Topography
Photomicrographs (Figure 1) showed the visual difference among the mini-
implants. According to the transmucosal neck charactherstics, the SIN™ (São Paulo,
SP, Brazil) presented roughest surface when compared to INP™ (São Paulo, SP,
Brazil) and Conexão™ (Arujá, SP, Brazil).
48
Figure 1. Photomicrographs from transmucosal neck of mini-implants. 1A. Localization of
transmucosal neck INP™; 1B. Detail of transmucosal neck topography INP™; 1C. Localization of
transmucosal neck SIN™; 1D. Detail of transmucosal neck topography SIN™; 1E. Localization of
transmucosal neck Conexão™; 1F. Detail of transmucosal neck topography Conexão ®.
Surface roughness
After verifying normality among samples, the results were tested and
indicated the significant difference among the evaluated groups, as well as an
intragroup variation between mini-implants of the same brand (Table 1). The three-
dimensional topography of the transmucosal neck of mini-implants evidenced the
visual aspect of results from AFM (Figure 2).
1A 1B
1C 1D
1E 1F

49
Table 1. Results regarding intragroup and intergroup comparison of readings (n=9) Ra values (nm)
after AFM.
* (P<0.05).
Figure 2. Three-dimensional topography of the transmucosal neck of mini-implants. 3A INP™; 3B
SIN™; 3C CONEXÃO™.
Discussion
The importance of surface characteristics is largely discussed in scientific
literature, since it can interfere in dental materials behavior 28. This preliminary study
focused on determining in advance a mini-implant that could favor the microbial
adhesion and biofilm formation over the transmucosal neck surface to further
develop an in vitro microbiological assay.
Commercially, mini-implants’ brands are avaialble in T6Al4V. Titanium alloys
offer excellent biocompatibility and surface properties, as polishing, corrosion
resistance, bacteriostatic action, and mechanical strength 1, 19.
The results of the present study agreed with AlSamak et al (2012),
considering the photomicrographs and three-dimensional images that showed
irregular surface topography of mini-implants, with parallel lines along the device,
2A 2B
3A 3B 3C
50
as well as structural defects (Figures 1 and 3). The authors also agreed that
manufactures should prepare materials in order to decrease their adhesion
potential, specially producing smooth surface textures 22, 28, 29. Difference of
structural surface topography was found among mini-implants of the same brand,
evidencing the necessity of better finishing of products.
When exposed to the oral environment, high surface roughness in titanium
devices may promote bacterial adhesion and hamper microbial biofilm removal 23.
Salivary pellicle immediatly covers the titanium surface, and its proteins work as
receptors for micro-organisms binding and subsequent biofilm formation 23. Plaque
accumulation usually follows the sequence of onset: cocci, rods, filamentous,
fusiforms, spirochetes and aggregates as corn-cobs 26, 27. The coccoid forms found
in initial biofilm formation stage are considered nono-pathogenic, unlike the others
associated with mature plaque 26.
Bollen et al (1997) suggested a maximum Ra value of 0.2 µm for better
bacterial adhesion control. The highest mean of Ra value found in this experiment
was 0.25 µm, which could be considered acceptable. Rougher surfaces are
favorable to greater plaque accumulation and retention 27, since they increase the
available area for colonization and the presence of pits and gooves protect bacteria
from removal forces allowing the establishment of less reversible binding to the
surface 21, 26, 28.
The peri-implant area determined by the gingival attachment to the neck of
the implant, which is responsable for mucosal seal and protection of mini-implant
health, should be resistant to bacteria adhesion and retention. Therefore, the
transmucosal neck of mini-implants deserves better polishing and smoother surface
to prevent enviromental injures 8, 19-23.
51
In order to promote bacteria adhesion and biofilm formation, which are
essential for a future in vitro microbiological essay, and considering the aspects
previously described, one can conclude that the mini-implant with greater surface
roughness SIN™ (São Paulo, SP, Brazil) should be the elected to that purpose.
Conclusion
The authors concluded that the transmucosal neck of orthodontic mini-
implants evaluated presented important surface roughness, particularly SIN™.
References
1. AlSamak S, Bitsanis E, Makou M, Eliades G. Morphological and structural
characteristics of orthodontic mini-implants. J Orofac Orthop. 2012
Jan;73:58-71.
2. Apel S, Apel C, Morea C, Tortamano A, Dominguez GC, Conrads G.
Microflora ssociated with succesful and failed orthodontic mini-implants. Clin
Oral Impl Res. 2009;20:1186-1190.
3. Kyung HM, Park HS, Bae SM, Sung JH, Kim IB. Development of orthodontic
micro-implants for intraoral anchorage. JCO. 2003 Jun;37(6):321-323.
4. Araújo TM, Nascimento MHA, Bezerra F, Sobral MC. Skeletal anchorage in
orthodontics with Mini-implants. Dental Press J Orthod. 2006
Jul/Aug;11(4):126-156.
5. Bae S, Park H, Kyung H, Kwon O, Sung J. Clinical Application of Micro-
Implant Anchorage. JCO. 2002 May;36(5):298-302.
6. Celenza F, Hockman MN. Absolute Anchorage in Orthodontics: Direct and
Indirect Implant-Assisted Modalities. JCO. 2000 Jul;34(7):397-402.

52
7. Cheng SJ, Tseng Y, Lee JJ, Kok SH. A Prospective Study of the Risk Factors
Associated with Failure of Mini-implants Used for Orthodontic Anchorage. Int
J Oral Maxillofac Implants. 2004;19(1):100-106.
8. Freitas AOA, Alviano CS, Alviano DS, Siqueira Jr JF, Nojima LI, Nojima
MCG. Microbial colonization in orthodontic mini-implants. Braz Dent J.
2012;23(4):422-427.
9. Kanomi R. Mini-Implant for Orthodontic Anchorage. JCO.1997;31(11):763-
767.
10. Luzi C, Verna C, Melsen B. Guidelines for Success in Placement of
Orthodontic Mini-Implants. JCO. 2009;43(1):39-44.
11. Miyawaki S, Koyama I, Inoue M, Mishima K, Sugahara T, Takano YT. Factors
Associated with the Stability of the Titanium Screws Placed in the Posterior
Region for Orthodontic Anchorage. Am J Orthod Dentofacial Orthop.2003
Oct;124(4):373-378.
12. Phiton MM, Nojima LI, Nojima MCG, Ruellas ACO.
Comparative study of fracture torque for orthodontic mini-implants of different
trademarks. Oral Surgery (Print). 2008;1:84-87.
13. Phiton MM, Nojima MCG, Nojima LI. Primary stability of orthodontic mini-
implants inserted into maxilla and mandible of swine. Oral Surgery, Oral
Medicine, Oral Pathology, Oral Radiology and Endodontics.2012;66, p.in
press.
14. Rinaldi JC, Arana-Chavez V. Ultrastructure of the interface between
periodontal tissues and titanium mini-implants. Angle
Orthod.2010;80(3):459-465.
53
15. Singh K, Kumar D, Jaiswal RK, Bansal A. Temporary anchorage devices-
mini-implants. Natl Maxillofac Surg.2010 Jan/Jun;1(1):30-34.
16. Tortamano A, Dominguez GC, Haddad ACSS, Nunes FD, Nacao M, Morea
C. Periodontopathogens around the surface of mini-implants removed from
orthodontic patients. Angle Orthod.2012;82(4):591-595.
17. Tseng YC, Hsieh CH, Chen CH, Shen YS, Huang IY, Chen CM. The
application of mini-implants for orthodontic anchorage. Int J Oral Maxillofac
Surg. 2006;35:704-707.
18. Wu TY, Kuang SH, Wu CH. Factors associated with the stability of mini-
implants for orthodontic anchorage: a study of 414 samples in Taiwan. Int J
Oral Maxillofac Surg. 2009;67:1595-1599.
19. Subramani K, Jung RE, Molenberg A, Hämmerie CHF. Biofilm on dental
implants: a review of literature. Int J Oral Maxillofac Implants. 2009;24:616-
626.
20. Stájer A, Urbán E, Pelsöczi IK, Mihalik E, Rakonczay Z, Nagy K, Turzó K,
Radnai M. Effect of caries preventive products on the growth of bacterial
biofolm on titanium surface. Acta Microbiol Immunol Hung. 2012;59(1):51-61.
21. Al-Ahmad A, Al-Ahmad MW, Fackler A, Follo M, Hellwig E, Bächle M, Hannig
C, Han JS, Wolkewitz M, Kohal R. In vivo study of the initial bacterial
adhesion on different implant materials. Arch Oral Biol. 2013;58:1139-1147.
22. Bürgers R, Gerlach T, Hahnel S, Schwarz F, Handel G, Gosau M. In vivo and
in vitro biofilm formation on two different titanium implant surfaces. Clin Oral
Impl Res. 2010;21:156-164.

54
23. Dorkhan M, de Paz LEC, Skepö M, Svensäter G, Davies JR. Effects of saliva
or serum coating on adherence of Streptococcus oralis strains to titanium.
Microbiology. 2012;158:390-397.
24. Silva DL, Mattos CT, Simão RA, Ruellas ACO. Coating stability and surface
characteristics of esthetic orthodontic coated archwires. Angle Orthod. 2013
Nov;83(6):994-1001.
25. Schimidlin PR, Müller P, Attin M, Wieland M, Hofer D, Guggenheim B.
Polyspecies biofilm formationon implant surfaces with different surface
characteristics. J Appl Oral Sci. 2013;21(1):48-53.
26. Rimondini L, Farè S, Brambilla, Felloni A, Consonni C, Brossa F, Carassi A.
The effect of surface roughness on early in vivo plaque colonizationon
titanium. J Periodontol.1997;68:556-562.
27. Teughels W, Assche NV, Sliepen I, Quirynen M. Effect of material
characteristics and/or surface topography on biofilm development. Clin Oral
Impl Res. 2006;17(Suppl 2):68-81.
28. Quirynen M, Van Der Mei HC, Bollen CML, Schotte A, Marechal M,
Doornbusch GI, Naert I, Busscher HJ. An in vivo study of the influence of the
surface roughness of implants on the microbiology of supra and subgingival
plaque. J Dent Res. 1993;72:1304-1309.
29. Drake DR, Paul J, Keller JC. Primary bacterial colonization of implant
surfaces. Int J Oral Maxillofac Implants. 1999;14(2):226-232.
30. Bollen CM, Lambrechts P, Quirynen M.Comparison of surface roughness of
oral hard materials to the threshold surface roughness for bacterial plaque
retention: a review of the literature.Dent Mater. 1997 Jul;13(4):258-269.

55
4.2 ARTIGO 2
OSÓRIO A, BOGHOSSIAN C, LOURENÇO TBG, COLOMBO APV, ALVIANO DS,
NOJIMA MCG. Microbial adhesion and biofilm formation in orthodontic mini-
implants. Artigo a ser submetido ao Clinical Oral Implants Research.
Abstract
Objectives: To follow the microbial adhesion and biofilm formation on
orthodontic mini-implants. Material and Methods: Forty mini-implants were
subjected to an in vitro microbiological assay of seven days. The adhesion and
biofilm development were evaluated by scanning electron microscopy (SEM),
fluorescence microscopy (FM) and DNA-DNA checkerboard hybridization. Results:
It was observed a representative microbial adhesion and great variety of micro-
organisms morphology. Images from SEM showed mature bacterial colonies
formation at 96 and 120 hours. The Live/Dead FM showed representative cellular
viability throughout the research time. The six different microbial complexes of
supragingival plaque were detected after 12 hours of incubation. The largest variety
of micro-organisms was observed between six and 48 hours. There was no
significant difference among bacterial levels during experimental times (p=0.2).
Conclusion: The microbial adhesion on the transmucosal neck of mini-implants
was detected after six hours of incubation. Cellular organization similar to biofilm
was observed after 96 hours of experiment. One can conclude that the transmucosal
56
neck of mini-implants represented a propitious site for microbial adhesion and
biofilm formation, and thus confirms the importance to control bacterial colonization
in order to preserve the mucosal seal around implants, preventing inflammation and
devices’s failure.
INTRODUCTION
Mini-implants are routinely used in contemporary orthodontics and have
aroused attention among professionals, since they offer absolute anchorage to
undesirable tooth movement with high levels of clinical success (Tortamano et al,
2012; Wu & Wu, 2009).
The long-term maintenance of mini-implants depends on some factors as
design, diameter, length and primary stability of the temporary anchorage devices
(TAD), host’s bone thickness, orthodontic mechanics, magnitude of applied force,
presence of trauma and plaque control around the device (Araújo et al, 2006; Luzi
et al, 2009; Mah & Bugstrand, 2005; Pithon et al, 2008; Squeff et al, 2008; Wilmes
et al, 2006).
The insertion of a mini-implant in the oral cavity creates a new sulcus by the
contact between the device’s surface and the adjacent mucosa. A proper mucosal
seal guarantees the sulcus health (Lee & Wang, 2010; Stájer et al, 2012).. However,
after exposition to the oral environment, a salivary pellicle readily coats the material
surface, favoring microbial adhesion and biofilm formation. .
Biofilm can grow and establish on several surfaces, as living tissues, teeth,
orthodontic accessories, acrylic resin and implants (Subramani et al, 2009).The
biofilm formation on implants is similar to that on teeth surface and follows a
sequential process (Subramani et al, 2009). After 24 hours, it is observed great

57
bacterial colonization on titanium surface, with several layers of bacteria. The
bacterial count remains similar during 14 days (Rasperinni et al, 1998; Stájer et al,
2010).
As the evolution of biofilm can interfere in the sulcus mucosa seal, cause peri-
implant mucosite and stability loss of the TAD (Araújo et al, 2006; Bodet et al, 2007;
Carano et al, 2005 Celenza & Hockman, 2000; Drake et al, 1999; Ferreira Jr et al,
2009; Gray & Smith, 2000; Heuer et al, 2007; Luzi et al, 2009; Mah & Bugstrand,
2005; Melsen, 2005; Mineoka et al; 2008; Pier-Francesco et al, 2006; Yoshinari et
al, 2000; Wilmes et al, 2006), the authors aimed to better understand the adhesion
and biofilm formation on orthodontic mini-implants.
MATERIALS AND METHODS
In order to observe how adhesion and biofilm formation occur in orthodontic
mini-implants, an in vitro microbiological assay of seven days was developed for
scanning electron microscopy (SEM), fluorescence microscopy (FM) and DNA-DNA
checkerboard hybridization analysis.
Forty mini-implants were used for evaluation from six hours to seven days
after inoculation in culture medium obtained from the collection of supragingival
plaque. The trademark SIN™(São Paulo, SP, Brazil): 8.0 mm long, 1.4 mm
diameter, and 1.0 mm transmucosal neck was sellected for this study, since
presented rougher surface according to a preliminar study. The mini-implants were
distributed on two 24-well tissue culture plates, according to the times of inoculation.
In the first 24 hours, the observation was performed after six hours time intervals.
Then, the observation was done every 24 hours, until completing seven days of

58
incubation. Four anchorage devices were used at each interval time: two for
molecular analysis, one for SEMand one for FM.
Supragingival plaque collection
Twelve patients, young adults, from both genders, under treatment at the
Graduation Clinic of Orthodontics at the School of Dentistry of Federal University of
Rio de Janeiro, Brazil, donated supragingival plaque for this experiment. The
exclusion criteria were the presence of systemic disease, recente antibiotic therapy
(six months before study) and pregnancy. All patients signed a consent form
previously approved by the Research Ethics Committee of IESC/ UFRJ (protocol
#50/2011; report #149/2011).
Collection was performed in a single stage, during routine orthodontic
appointment. Both dental arches were isolated from buccal and labial mucosa with
cotton rolls and teeth were dried with air. Then, supragingival plaque was collected
with sterile explorer #5 (ref. 11511, Duflex ®, SS White ®, RJ, Brazil), removing the
material around the edges of the bonding brackets. The supragingival plaque was
inserted into a Eppendorf™ tube containing 1 mL of 0,85% sterile saline.
Inoculum preparation
After centifugation, the pellet was transferred to three tubes containing 30 mL
of BHI broth (Brain Heart Infusion, Oxoid™, Hampshire, UK) supplemented with 3%
saccharose, 5 µg/mL hemine and 10 µg/mL menadione, incubated for seven days
at 37ºC, in an anaerobic jar, with oxygen restriction.
59
After incubation, the optical density of growing culture was measured
(Beckman Coulter DU 530 Spectrophotometer, Brea, CA). The inoculum presented
1.5 x 108 UFC/mL, using the McFarland standards as reference.
Saliva collection and processing
Unstimulated saliva was collected from the same subjects who donated
supragingival plaque. The saliva samples were diluted to 1:10 in PBS, centrifugated
and supernatant was filter sterilized.
Adhesion and biofilm development assay
The mini-implants were coated with 10% sterile saliva for two hours at room
temperature under agitation (Walker et al, 2010). Next, they were placed in 24-well
tissue culture plates.
Each well was filled with 500 µL of BHI broth (Oxoid™, Hampshire, UK)
supplemented with 3% saccharose, 5 µg/mL hemin and 10 µg/mL menadione, and
500 µL of pooled bacterial culture. The culture medium was renewed every 48 hours
after 72 hours of incubation (Sánchez et al, 2011). On each culture plate, two wells
were used as control, with 1mL of sterile medium.
After incubation, the mini-implants were processed according to the methods
of analysis applied in the study.
Scanning electron microscopy
For scanning electron microscopy, the mini-implants were gently rinsed in
PBS and fixed in 2.5% glutharaldheyde diluted in 0.1 M cacodylate buffer for 24h.
60
Following, they were rinsed in PBS once again, dried, fixed on specific stubs for
metallization and observed by SEM (Quanta FEG 400; FEI Company, Eindhoven,
Netherlands).
Fluorescence microscopy
After contamination, the mini-implants were rinsed in 0,85% sterile saline and
inserted into an Eppendorf™ tube filled with 300 µL of the same solution. Reagents
of LIVE/DEAD™ BacLight (Molecular Probes – Invitrogen. Eugene, Oregon, USA)
viability kit for microscopy assay were prepared by mixing SYTO 9 (A), for live and
active cells (fluorescent green) and propidium iodide (B), for dead and inactive cells
(fluorescent red). Aliquots of 0.5 µL of each reagent were added to each Eppendorf™
tube containing the mini-implant and the saline solution. Then the tubes were
maintained in darkness, at room temperature for 15 minutes.
Following, the mini-implants were fixed on glass slides, so that the
transmucosal neck was parallel to the glass slide. Microscopy images of ten devices
were captured by a digital camera (Axiocam™ MRc5/MRm; Carl Zeiss Microlmaging
GmbH) connected to the microscope (Axiovert™ 200M; Carl Zeiss Microlmaging
GmbH, Göttingen, Germany) and processed by the software AxioVision 4.6 (Carl
Zeiss Microlmaging GmbH).
Checkerboard DNA-DNA hybridization
After incubation, mini-implants were rinsed in PBS and transferred to
Eppendorf™ tubes with 150 µL of 10 Mm Tris, 1Mm EDTA, sterile distilled water
solution (TE) for vortex shaking. The cells adhered to the mini-implants were
61
dispersed and 150 µL of 0.5 M NaOH solution was added to them (Boghossian et
al, 2011).
The cells were lysed and the denatured DNA was neutralized by 0.8 mL of
5M ammonium acetate. The DNA suspension was fixed on a nylon membrane
(Hybond-N+, GE Healthcare Life Sciences, Piscataway, NJ, USA) using the Minislot
device (Immunetics™,Cambridge, MA, USA). After prehybridization against DNA
samples, the membrane was positioned so that the DNA lines were upright to the
Miniblotter 45 slots (Immunetics™, Cambridge, MA, USA). Next, the membrane was
hybridized against genomic DNA probes digoxigenin labelled (Kit Dig-High Prime™,
Roche Applied Science, São Paulo, SP, Brazil). The bacterial species selected to
produce the DNA probes were described in Square 1. After hybridization, the
membrane was washed at high stringency solutions and linked probes were
identified by phosphatase-conjugated antibody against digoxigenin (Roche Applied
Science, São Paulo, SP, Brazil). Finally, the fluorescence was captured by the
Storm™ 860 imaging system (GE™ Healthcare Life Science, São Paulo, SP,
Brazil). Signals were compared to the standards of 105 and 106 bacterial cells for
the evaluated species on the same membrane. They were scored as: (0) not detect;
(1) <105 cells; (2) approximately 105; (3) 105–106; (4) approximately 106, and (5)
>106 cells. The absence of signal, considered as zero, could represent bacterial
ranges between 1–1000, since the sensitivity of the assay was adjusted detect 104
cells of a given species by adjusting the concentration of each DNA probe
(Boghossian et al, 2011).

62
Species Strains* Species Strains*
Aggregatibacter actinomycetemcomitans a 43718 Leptotrichia buccalis 14201
Aggregatibacter actinomycetemcomitans b 29523 Neisseria mucosa 19696
Aggregatibacter actinomycetemcomitans c 625** Porphyromonas gingivalis 33277
Actinomyces gerensceriae 23860 Prevotella intermedia 25611
Actinomyces israelli 12102 Prevotella melaninogenica 25845
Actinomyces odontolyticus 17929 Prevotella nigrescens 33563
Actinomyces naeslundii 12104 P. micra 33270
Actinomyces viscosus 43146 Propionibacterium acnes I 11827
Capnocytophaga gingivalis 33624 Propionibacterium acnes II 43541
Capnocytophaga ochracea 33596 Streptococcus anginosus 33397
Capnocytophaga sputigena 33612 Streptococcus constellatus 27823
Campylobacter concisus 33237 Streptococcus mitis 49456
Campylobacter rectus 33238 Streptococcus intermedius 27335
Campylobacter showae 51146 Streptococcus noxia 43541
Eubacterium nodatum 33099 Streptococcus oralis 35037
Eubacterium saburreum 33271 Streptococcus sanguinis 10556
Eikenella corrodens 23834 Streptococcus gordonii 10558
Fusobacterium periodonticum 33693 Tannerella forsythia 43037
Fusobacterium nucleatum ss. vincentii 49256 Treponema denticola B1**
F. nucleatum ss nucleatum 25586 Treponema socranskii S1**
F. nucleatum ss polymorphum 10953 Veillonella parvula 10790
Gemella morbilorum 27824
*ATCC (American Type Culture Collection, Rockville, MD, USA), **The Forsyth Institute, (Boston, MA, USA),
Colors corresponding to the supragingival plaque microbial complexes.
Figure 1. Bacterial strains used for production of DNA probes.
Data analysis
Data from photomicrographs and digital images were described after
macroscopic and visual observation. Results obtained from checkerboard DNA-
DNA hybridization were submitted to SPSS 17.0 (Statistical Package for Social
Sciences; SPSS Inc., Chicago, IL, USA). Kruskal-Wallis test was applied for
detection of possible statistical difference among the score during interval times.
63
The level of signifficance was set at 5%. The distribution of the prevalence levels
was presented in graphic.
Results
Scanning electron microscopy and fluorescence microscopy
After six hours of incubation, representative microbial adhesion was
observed, and kept relatively constant during the experiment, as well as the quantity
and morphology of micro-organisms found. However, 5.000X magnification images
from SEM showed cellular organization similar to more mature bacterial colonies
formation at 96 and 120 hours. Since the initial experimental times, micro-organisms
with different morphological charcteristics were identified, as coccus, rods, bacilli,
filaments and corn cobs. The live/ dead fluorescence showed cellular viability
throughout the research time. This evidenced that the transmucosal neck of mini-
implants, when submitted to the experimental conditions applied at this study,
represented a propitious site for microbial adhesion and biofilm formation (Figure
1).

64
Figure 2. Images of microbial adhesion and biofilm formation development during experimental times. 1. 6h; 2. 12h; 3. 18h;
4. 24h; 5. 48h; 6. 72h; 7. 96h; 8. 120h; 9. 144h; 10. 168h. A. Fluorescence microscopy 400X; B. SEM photomicrograph
1.200X; C. SEM photomicrograph 5.000X.

65
Checkerboard DNA-DNA hybridization
The six different microbial complexes of supragingival plaque were found
since initial search time, except the red complex, which was detected after 12 hours
of incubation. The largest variety of micro-organisms was observed between six and
48 hours, decreasing within 72 hours and raising again until the 168 hours (Figure
2). However, there was no significant difference among bacterial levels considering
the experimental times evaluated in the study (p=0.2).

66
Figure 3. Graphic representing the bacterial levels distribution at different experimental times; 0 (not detected); 1 (<105 cells); 2 (approximately 105); 3 (105–106); 4 (approximately 106), and
5 (>106 cells).
0
1
2
3
4
5
6h 12h 18h 24h 48h 72h 96h 120h 144h 168h

67
Discussion
A previous study was performed to determine the ideal mini-implant for the
development of bacterial adhesion and biofilm formation assay. Results pointed
SIN™ (São Paulo, SP, Brazil: 8.0 mm long, 1.4 mm diameter, and 1.0 mm
transmucosal neck) mini-implant as the rougher transmucosal neck surface. It is
well known that irregular surfaces promote colonization and mainly reduce
hygiene procedures efficiency, thereby encourages the evolution of biofilm and
its complexity (Quirynen et al, 1993; Rimondini et al, 1997; Schmidlin et al, 2013).
The transmucosal neck of temporary anchorage devices was in focus in
the present study because it remains in contact with the adjacent mucosa,
forming a new sulcus. Depending on the anatomic location of the mini-implant, it
offers difficulty in access and cleaning (Freitas et al, 2012; Lee & Wang, 2010;
Stájer et al, 2012).
After insertion, the mini-implant’s surface exposed to oral cavity is covered
by salivary pellicle, followed by microbial adsortion and adhesion (Gosau et al,
2010), although the adquired pellicle on titanium surfaces presents lower albumin
adsortion capability (Lee & Wang, 2010). The sulcus seal is essential for peri-
implant mucosa health and must be protected from bacteria invasion (Lee &
Wang, 2010; Stájer et al, 2012). The long-term permanence of temporary
anchorage devices depends on microbial control around them, since poor
hygiene can lead to mucosal inflammation and mini-implant’s failure (Apel et al,
2009; Bürgers et al, 2010; Freitas et al, 2012; Hoiby et al, 2010; Tortamano et al,
2012; Tseng et al, 2006).
It is expected that the biofilm formation on implants occurs similar to the
teeth (Dhir et al, 2013; Lee & Wang, 2010). Then, as described in our study, initial
colonizers were observed in the early stage of biofilm formation. Despite most

68
are commensal bacteria, they provide the pre-conditions for the aggregation of
the subsequent colonizers, as gram negative anaerobic bacteria, and influence
the stages of biofilm formation (Li et al, 2004; Kreth et al, 2009; Heuer et al, 2011).
The oral cavity is a complex environment difficult to reproduce (Al-Ahmad
et al, 2013). The supragingival plaque was collected from patients and cultured
in vitro. Although the authors followed previously published methods for biofilm
formation (Sànchez et al, 2011; Walker et al, 2007), our cells culture suffered
selection.
Microscopic images showed microbial adhesion at six hours of incubation,
corroborating with prior studies that described initial colonization after 30 minutes,
among the interval times from zero to four hours, or from two to six hours of oral
exposure (Al-Ahmad et al, 2013; Dhir et al, 2013; Lee & Wang, 2010; Subramani
et al, 2009). The bacterial morphology evidenced cocci, rods, bacilli, short and
long filaments and corn cobs during all experimental times. Stájer et al (2012)
described the presence of early colonizers in the first 24 hours and the
maintenance of stable colonization up to 14 days. Freitas et al (2012) also
evidenced the colonization of Streptococcus on mini-implants’s gingival sulcus
after 24 hours of insertion, which remained stable for three months. Other
authors reported the presence of similar bacterial morphologies, as Dhir et al
(2013), Kreth et al, (2008), Rimondini et al (1997) and Subramani et al (2009).
However, between 96 and 120 hours, SEM and FM images of this study showed
more mature cellular organization. Teughels et al (2006) reported that mature
plaque was present, but only after several days, and showed increased
proportions of rods, motile and spirochets. In almost all our fluorescence
photomicrographs, the oral bacteria colonization on the surface was monolayer

69
or isolated aggregation of cells, as well as previously described by Gosau et al
(2010).
The molecular evaluation showed the diversity of micro-organisms in the
transmucosal neck of mini-implants at interval times. Species of all bacteria
complexes were found at 12 hours of incubation, even those belonging to the red
complex. Similar results were found by Li et al (2004) that analyzed the biofilm
collected from teeth, except for the observation of bacteria from the red complex
even in the early stages from zero to six hours time interval. In spite of the
diversity, the levels of bacteria remained stable in this study, with no significant
statistical difference during the follow-up period.
Results confirmed that different microbial communities of supragingival
complexes could resist and grow on mini-implants surface. The orange and the
red complexes, usually associated with periodontal disease and clinical signs of
inflammation (Haffajee et al, 2008), were detected at initial time and remained in
high levels (3-5) even after six or seven days of incubation. Periodontopathogen
species as P. melaninogenica, F. nucleatum vicentii, G. morbilorum, C. concisus,
C. showae, S. noxia, classified in the orange complex, and E. nodatum, T.
socranskii, P. gingivalis, T. forsythia, from the red complex, when adhered to mini-
implants in the oral cavity, in the same levels evidenced in this study, would
possibly cause peri-implant inflammation and contribute to stability loss. In
contrast, bacteria classified in the purple, green, blue or yellow complexes,
observed in periodontal health, were detected during all experimental times, and
mostly in lower levels (0-2), except for A. naeslundii, Aa a+b+c, A. gerencseria,
V. parvula, C. gingivalis and S. gordonii. Therefore, its was verified that biofilm
composition became more complex over time, with predominance of pathogenic
micro-organims.

70
Conclusion
According to the results, mini-implants represented a propitious site for
microbial adhesion and biofilm formation. Itconfirms the importance to control
bacterial colonization in order to preserve the mucosal seal around implants,
preventing inflammation and devices’s failure.
References
1. Al-Ahmad A, Al-Ahmad MW, Fackler A, Follo M, Hellwig E, Bächle M,
Hannig C, Han JS, Wolkewitz M, Kohal R. In vivo study of the initial
bacterial adhesion on different implant materials. Arch Oral Biol.
2013;58:1139-1147.
2. Apel S, Apel C, Morea C, Tortamano A, Dominguez GC, Conrads G.
Microflora ssociated with succesful and failed orthodontic mini-implants.
Clin Oral Impl Res. 2009;20:1186-190.
3. Araújo TM, Nascimento MHA, Bezerra F, Sobral MC. Skeletal anchorage
in orthodontics with Mini-implants. Dental Press J Orthod. 2006
Jul/Aug;11(4):126-56.
4. Bodet C, Chandad F, Grenier D. Potentiel pathogénique de
Porphyromonas gingivalis, Treponema denticola et Tannerella forsythia,
le Complexe Bacterèrien Rouge Associé à la Parodontite. Pathologie
Biologie. 2007;55:154-162.
5. Boghossian CMS, Souto RM, Luiz RR, Colombo APV. Association of red
complex, A. actinomycetemcomitans and non-oral bacteria with
periodontal diseases. Arch Oral Biol. 2011; 56:899-906.

71
6. Bürgers R, Gerlach T, Hahnel S, Schwarz F, Handel G, Gosau M. In vivo
and in vitro biofilm formation on two different titanium implant surfaces.
Clin Oral Impl Res. 2010;21:156-164.
7. Carano A, Velo S, Leone P, Siciliani G. Clinical Aplications of the
Miniscrew Anchorage System. JCO. 2005Jan;39(1):9-24.
8. Celenza F, Hockman MN. Absolute Anchorage in Orthodontics: Direct and
Indirect Implant-Assisted Modalities. JCO. 2000 Jul;34(7):397-402.
9. Colombo AP, Teles RP, Torres MC, Souto R, Rosalem WJ, Mendes MC,
Uzeda M. Subgingival microbiota of Brazilian subjects with untreated
chronic periodontitis. J Periodontol. 2002;73:360-369.
10. Colombo AP, Teles RP, Torres MC, Souto R, Rosalem WJ, Mendes MC,
Uzeda M. Effects of non-surgical mechanical therapy on the subgingival
microbiota of Brazilians with untreated chronic periodontitis: 9-month
results. J Periodontol. 2005; 76: 778-784.
11. Dhir S. Biofilm and dental implant: the microbial link. J Indian Soc
Periodontol. 2013 Jan-Feb; 17(1):5-11.
12. Drake DR, Paul J, Keller JC. Primary bacterial colonization of implant
surfaces. Int J Oral Maxillofac Implants. 1999;14(2):226-232.
13. Ferreira JR SB, Figueiredo CM, Almeida ALPF, Assis GF, Dionísio TJ,
Santos FC. Clinical, Histological, and Microbiological Finding in Peri-
implant Disease: A Pilot Study. Implant Dentistry. 2009;18(4):334-44.
14. Freitas AOA, Alviano CS, Alviano DS, Siqueira Jr JF, Nojima LI, Nojima
MCG. Microbial colonization in orthodontic mini-implants. Braz Dent J.
2012;23(4):422-27.
72
15. Gosau M, Hahnel S, Schwarz F, Gerlach T, Reichert TE, Bürgers R.
Effects of six different peri-implantitis disinfection methods on in vivo
human oral biofilm. Clin Oral Impl Res. 2010;21:866-72.
16. Gray JB, Smith R. Transitional Implants for Orthodontic Anchorage. JCO.
2000 Nov;34(11):659-66.
17. Heuer W, Elter C, Demling A, Neumann A, Suerbaum S, Hannig M,
Heidenblut T, Bach W, Stiesch-Scholz M. Analysis of Early Biofilm
Formation on Oral Implants in Man. J Oral Rehabil. 2007;34:377-82.
18. Hoiby N, Ciofu, O, Johansen HK, Song Z, Moser C, Jansen PO, Molin S,
Givkov M, Tolker-Nielsen T, Bjamsholt T. The clinical impacto f bacterial
biofilms. Int J O Sci. 2011;3:55-65.
19. Kreth J, Merritt J, Qi F. Bacterial and host interactions of oral streptococci.
DNA and Cell Biology. 2009;28(8):397-403.
20. Lee A, Wang HL. Biofilm related to dental implants. Implant
Dentistry.2010;19(5):387-93
21. Li J, Helmerhorst EJ, Leone CW, Troxler RF, Yaskell T, Haffajee AD,
Socransky SS, Oppenheim FG. Identification of early microbial colonizers
in human dental biofilm. J Appl Microbiol. 2004;97: 1311-1318.
22. Luzi C, Verna C, Melsen B. Guidelines for Success in Placement of
Orthodontic Mini-Implants. JCO. 2009;43(1):39-44.
23. Mah J, Bugstrand F, Graham JW. Temporary Anchorage Devices, a
Status Report. JCO. 2005;39(3):132-36.
24. Melsen B. Mini-implants: Where are we? JCO. 2005 Sept;39(9):539-47.
25. Pier-Francesco A, Adams RJ, Waters MGJ, Wiliams DW. Titanium
Surface Modification and its Effect on the Adherence of Porphyromonas
gingivalis: an in vitro study. Clin Oral Impl Res. 2006;17:633-37.

73
26. Pithon MM, Nojima LI, Nojima MCG, Ruellas ACO. Evaluation of Flexural
Strength and Fracture resistance of Orthodontic Mini-implants. Dental
Press J Orthod. 2008;13(5):128-33.
27. Quirynen M, Teughels W, De Soete M, Van Steenbergh D. Topical
antiseptics and antibioticsin the initial therapy of chronic adult periodontitis:
microbiological aspects. Periodontol 2000. 2002; 28:72-90.
28. Rasperini G, Maglione M, Cocconcelli PS, Simion M. In vivo early plaque
formation on pure titanium and ceramic abutments: a comparative
microbiological and SEM analysis.Clin Oral Impl Res. 1998; 9:357-364.
29. Rimondini L, Farè S, Brambilla, Felloni A, Consonni C, Brossa F, Carassi
A. The effect of surface roughness on early in vivo plaque colonizationon
titanium. J Periodontol.1997;68:556-562.
30. Sánchez MC, Llama-Palacios A, Blanc V, Léon R, Herrera D, Sanz M.
Structure, viability and bacterial kinetics of an in vitro biofilm model using
six bacteria from the subgingival microbiota. J Periodont Res. 2011;
46:252-260.
31. Schimidlin PR, Müller P, Attin M, Wieland M, Hofer D, Guggenheim B.
Polyspecies biofilm formationon implant surfaces with different surface
characteristics. J Appl Oral Sci. 2013;21(1):48-53.
32. Socransky SS, Smith C, Martin L, Paster BJ, Dewhirst FE, Levin
AE.Checkerboard DNA-DNA hybridization. Biotechniques. 1994
Oct;17(4):788-92.
33. Squeff LR, Simonson MBA, Elias CN, Nojima LI. Characterization of mini-
implants used for orthodontic anchorage. Dental Press J Orthod.
2008;13(5):45-56.

74
34. Stájer A, Urbán E, Pelsöczi IK, Mihalik E, Rakonczay Z, Nagy K, Turzó K,
Radnai M. Effect of caries preventive products on the growth of bacterial
biofolm on titanium surface. Acta Microbiol Immunol Hung. 2012;59(1):51-
61.
35. Subramani K, Jung RE, Molenberg A, Hämmerie CHF. Biofilm on dental
implants: a review of literature. Int J Oral Maxillofac Implants. 2009;24:616-
626.
36. Teughels W, Assche NV, Sliepen I, Quirynen M. Effect of material
characteristics and/or surface topography on biofilm development. Clin
Oral Impl Res. 2006;17(Suppl 2):68-81.
37. Tortamano A, Dominguez GC, Haddad ACSS, Nunes FD, Nacao M,
Morea C. Periodontopathogens around the surface of mini-implants
removed from orthodontic patients. Angle Orthod.2012;82(4):591-95.
38. Tseng YC, Hsieh CH, Chen CH, Shen YS, Huang IY, Chen CM. The
application of mini-implants for orthodontic anchorage. Int J Oral
Maxillofac Surg. 2006;35:704-707.
39. Walker C, Borden LC, Zambon JJ, Bonta CY, Devizio W, Volpe AR. The
effects of a 0.3% triclosan-containing dentifrice on the microbial
composition of supragingival plaque. J Clin Periodontol. 1994
May;21(5):334-41.
40. Wilmes B, Rademacher C, Olthoff G, Drescher D. Parameters Affecting
Primary Stability of Orthodontic Mini-implants. J Orofac Orthoped.
2006;3:162-74.
41. Wu TY, Kuang SH, Wu CH. Factors associated with the stability of mini-
implants for orthodontic anchorage: a study of 414 samples in Taiwan. Int
J Oral Maxillofac Surg. 2009;67:1595-99.
75
42. Yoshinari M, Oda Y, Kato T, Okuda K, Hirayama A. Influence of Surface
Modifications to Titanium on Oral Bacterial Adhesion in vitro. J Biomed.
Mater Res. 2000;52(2):388-94.
76
4.3 ARTIGO 3
OSÓRIO A, LEITE D, SOUTO RM, COLOMBO APV, ALVIANO DS, NOJIMA
MCG. Microbial control of orthodontic mini-implants. Artigo a ser submetido ao
American Journal of Orthodontics and Dentofacial Orthopedics.
Abstract
Introduction: Microbial control around mini-implants is considered an important
factor for the temporary anchorage device (TAD) maintainance during orthodontic
treatment, since poor hygiene can lead to inflammation of peri-implant mucosa
and stability loss. Thereby, the authors aimed to evaluate four methods applied
for mini-implant microbial control, and indicate the most suitable hygiene
procedure for cleaning mini-implants. Methods: At baseline and 21 days after
usage of mechanical, chlorexidine, triclosan or cetylpyridinium chloride methods
of oral hygiene, biological material was collected from 59 mini-implants and
processed for real-time PCR molecular investigation of total nonspecific bacteria.
Results: There was significant difference between baseline and 21 days
bacterial total count considering each hygiene method, except for the
cetylpyridinium chloride. However, no statistical difference was detected when all
methods were compared. Conclusions: The mechanical hygiene of orthodontic
mini-implants works well to keep microbial control of the devices.
77
INTRODUCTION
Anchorage in Orthodontics is defined as resistance to undesirable tooth
movement. 1-4 The conventional methods for anchorage are not the best for
critical cases, since they involve structures with potencial mobility as teeth and
depend on patient cooperation. 1-3, 5 The development of skeletal anchorage
methods contributed to difficult tooth movements, as mesiodistal movement of
posterior teeth, individual or mass intrusion, become more easily achieved.6
Thus, mini-implants are replacing anchorage devices as headgears, elastics and
arch bars. 3, 6
Several studies showed clinical applications, mechanical strategies and
properties of these skeletal devices. Nevertheless, the biological factors
associated with long-term success of mini-implants are underexploited. Microbial
control around mini-implants is considered a relevant factor for the device
maintainance, 1, 4, 7, 8 specially because the poor hygiene can lead to inflammation
of peri-implant mucosa and TAD’s stability loss. 3, 9-10
Immediately after intra-oral exposure, the mini-implant’s surface is covered
by adquired pellicle, which promotes the adhesion of early colonizers. These
bacteria create favorable conditions for adhesion of other species, including
periodontophatogens, which are frequently associated with inflammation and
periodontal disease. 21-25
The sulcus formed between the transmucosal neck of mini-implants and
the adjacent gingiva establishes an area of close contact between the material
surface and the mucosa. However, this area can be colonized if dental plaque
accumulation persists and implant hygiene procedures fail. 4, 26, 27

78
Some methods have been proposed for mini-implants’s hygiene,
especially based on chemical agents. 1, 4, 9, 23, 27 Despite the consensus about the
necessity to reduce factors influencing microbial adhesion and biofilm formation,
an efficient method for microbial control around mini-implants is not yet defined.
Therefore, the aim of the present study was to evaluate the efficiency of four
methods indicated for orthodontic mini-implant’s microbial control.
MATERIALS AND METHODS
Among 42 young adults, from both genders, under treatment at the
Graduation Clinic of Orthodontics at the School of Dentistry of Federal University
of Rio de Janeiro, Brazil, 39 individuals were sellected for the present research
and contributed with 59 mini-implants in total. The exclusion criteria were the
presence of systemic diseases, recent antibiotic therapy (six months before the
beginning of the study and/or over the study period) and pregnancy. All patients
signed a consent form previously approved by the Research Ethics Committee
of IESC/ UFRJ (protocol #50/2011; report #149/2011).
Individuals were randomly distributed in four groups according to the
hygiene method applied, comprising: mechanical hygiene (MG), or mechanical
hygiene associated with chemical agent: chlorhexidine 0.12% (CHXG), Triclosan
0.03% (TG), or cetylpyridinium chloride 0.05% (CPCG). To standardize the
hygiene methods, the participants received oral hygiene instructions and a written
protocol to be followed, adapted to each group of the study.
Sample collection

79
Collections were performed in the sulcus formed between the mini-
implants’s transmucosal neck and the attached gingiva at baseline and 21 days
after the use of the therapeutic methods. 4, 11
Previously, supragingival plaque was removed with sterile gauze and
compressed air around dental surface and mini-implant’s head. The anchorage
devices were kept isolated with sterile cotton rolls. 28-31
Four endodontic paper points # 40 (ENDO POINTS®, Manacapuru, AM,
Brasil) were gently inserted in the sulcus formed between the TAD’s
transmucosal neck and the attached gingiva during 45 seconds to collect the
biological material. 11, 32-34
The paper points were stored inside Eppendorf® tubes with 50 µl of Tris
EDTA and maintained at -20°C until laboratorial process.11, 35
DNA extraction
DNA samples were extracted by proteinase K method. 36 After defrosting,
tubes were vortexed for 60 seconds and the four paper points inside each tube
were despised. The biological material was centrifuged, the pellet was preserved
and 44 µL of TE, 5 µL of Tween 20 5% and 1 mL of Proteinase K 10 mg/mL were
added to the tube. A total volume of 50 µL was obtained for reaction. The DNA
concentration was measured (NanoDrop® 2000, Thermo Scientific, Waltham,
MA, USA) and standardized to guarentee the fidelity of the reaction results.
Real-time PCR quantitative analysis
The quantitative analysis of total bacteria was performed at baseline and
21 days after treatment in each group to evaluate the hygiene methods applied
over the study. Total bacteria quantification was made using 16S ribossomal

80
RNA (rRNA) gene targeted real- time PCR. Power SYBER Green PCR Master
Mix (Applied Biosystems, Foster City, CA, USA) was used for a total volume of
20 µL reaction. The universal primers sellected were described by Asai et al
(2002) (5’ - GAT TAG ATA CCC TGG TAG TCC AC – 3’ and 5’ – TAC CTT GTT
ACG ACT T – 3’). Each reaction comprised 5µL DNA(3 ng/µL),10 µL MIX, 0.4 µL
of each primer, 0.4 µL ROX (1:10) to control variation in volume and evaporation
along the reaction, and 3.8 µL of ultrapure water for PCR. The reactions were
distributed to 96-well culture plates, sealed, centrifuged and inserted into the
thermocycler for amplification. The programmed cycles were: 1 cycle
95ºC/10min; 40 cycles 95ºC/1min, 40 cycles 52ºC/1min and 40 cycles 72ºC/1min.
Amplifications were measured at 78 ºC. The fluorescence was monitored in every
cycle.
Standard curves used as reference to acquire the results and assess
bacterial levels presented 1:1 ratio between the number of copies obtained and
the number of bacterial cells evidenced in the analyzed samples.37 The curves
concentration ranged from 102 to 107, based upon DNA extracted from
Enterococcus Faecalis ATCC 29212 strain. While the reaction occured, the
fluorescent signals were input into graphics and numeric values obtained as
results of mathematical calculs carried out on software v2.0.4 ABI 7500 (Applied
Biosystems, Foster City, CA, USA).
Data analysis
Data was analyzed on SPSS 17.0 (Statistical Package for Social Sciences;
SPSS Inc., Chicago, IL, USA). Descriptive analysis of results was performed by
mean values and standard deviation. Data normality was tested by Kolmogorov-
Smirnov. Paired T Student test was applied to verify intragroup difference and

81
ANOVA with Tukey Post-Hoc to detect diferences among groups. The assumed
significance level was 5%.
Results
Real time PCR results revealed that it is important to establish a routine
for mini-implants’s hygiene. The methods applied in the present study showed
significant difference between baseline and final observation times, except for
CPCG with cetylpyridinium chloride 0.05%. Nevertheless, there was no statistical
difference among all hygiene protocols studied herein (Table I). This evidenced
that the mechanical hygiene of orthodontic mini-implants per se is enough to keep
microbial control of the devices.
Table I. Intragroup and intergroup comparison regarding changes in the number of bacterial cells
(log 10) detected at baseline (T1) and final observation time (T2), according to the hygiene
protocol applied in the study.
N= sample number; SD (standard deviation). * Statistical significance level at 5%.. *Paired t test for intragroup comparison. ANOVA with Tukey Post-Hoc for intergroup comparison.
Discussion
Success in skeletal orthodontic anchorage is mainly dependent on TAD’s
primary stability. It is defined as implant fixation immediately after insertion. Mini-
implant’s stability is influenced by operator skill during surgical procedure, quality
of the host bone and anatomical region sellected for insertion. Titanium alloys are
82
biocompatible materials, which offer corrosion resistance,mechanical resistance
and great surface topography. 6, 9, 12, 24, 27, 38- 40 For implants’s long-term stability,
it is also important to consider the magnitude of the applied force, presence of
trauma and plaque control around the screw. 9, 14, 15, 19, 40, 41
An adquired pellicle readly covers the mini-implant’s surface after oral
exposure and the early colonizers begin the biofilm formation process, promoting
the attachment of virulent species responsable for tissue inflammation and
periodontal disease. 13, 21-25When implant hygiene fails, the peri-implant gingival
sulcus is colonized by dental plaque constituted by micro-organisms with different
levels of virulence and loses the natural seal, compromising device permanence
in the oral cavity.1, 4, 9, 27, 39, 43.
The mouthwash rinses are products used for oral hygiene since they help
maintain oral health and improve the quality of life for patients, as well as their
general health. 44 However, some authors reported that brushing the teeth with
fluoride dentifrice is enough to reduce clinical periodontal index and the quantity
of 40 species from oral microbiota 45
Gosau et al (2010) described that mechanical debridment on implants
surfaces does not remove all adhering micro-organisms, and should be
complemented with other peri-implant therapies as use of antiseptics. The
combined use of chemical agentes and mechanical theraphy should be preferred.
Our results revealed significant difference among the therapies applied
between baseline and final observation times over the study, except for the
Cetylpyridinium Chloride 0.05% mouthwash. Results were favorable to mini-
implants microbial control maintenance, since reduced non-specific total bacteria
colonization, which is considered an important factor to restore the equilibrium
between peri-implant microbiota and host defense. 23
83
Prior studies have shown that Chlorhexidine 0.12% presents wide-
spectrum antibacterial activity. 46, 47It acts by altering the bacterial cell membrane
and causing subsequent leakage and destruction of the cell. 21, 47 Chlorhexidine
also reveals great substantivity, defined as the ability to bind to tissues with slow
release.48 The efficacy of chlorhexidine is comproved by several results
described in the literature.49 Chlorhexidine gluconate inhibit plaque formation
around natural teeth and implants.21, 23
Other chemicals, as triclosan, are reported as plaque-reducing mouth
rinses. Triclosan 0.03% was searched by several authors and defined as high
antibacterial potente agent, capable to reduce the attached bacteria, including
gram-positive, gram-negative and anaerobic bacteria. 50, 51 However, among the
studies evaluated by Gosau et al (2010), none of them evidenced that triclosan
was as efficient as chlorexidine.
Cetylpyridinium chloride 0.05% exhibited reduction in gingivitis and
supragingival plaque index, overall score of bacteria in gingival sulcus and saliva,
as significant decrease in anaerobic bacteria of supragingival plaque after 14
days of use. 52-54
The present study did not reveal statistical difference among the hygiene
methods tested. Previous researches comparing Chlorexidine 0.12%, Triclosan
0.03% and Cetylpyridinium Chloride 0.05% showed greater efficacy of
chlorexidine or triclosan based mouth rinses in bacteria recolonization control as
well as supragingival plaque and gingivitis clinical index after five days use.55, 56
Nevertheless Lang et al (2012) described that products as Triclosan 0.03% and
Chlorexidine 0.12% offer modest efficacy in plaque acumulation and gingivitis
reduction when conventional oral hygiene is not applied (Lang et al, 2012).

84
However, based on our data, it was evidenced that only the mechanical
hygiene of mini-implants maintains microbial control of orthodontic mini-implants.
Our results are similar to studies which pointed that mouth rinses based on
triclosan or chlorexidine in addition to toothbrushing with dentifrice containing
triclosan 0,03% did not bring better benefit to the oral microbial control.57, 58
Toothbrushing with triclosan 0.03% dentifrice has greater efficacy when
compared with the conventional fluoride ones.51, 59 Peri-implant microbial control
is achieved by brushing with triclosan 0.03% and copolymer dentifrice. Those
dentifrices reduce supragingival plaque index and gingivitis, besides the mainly
periodontopathogens.60 It is also important to emphasize that even in low
concentrations of NaF, in an acidic environment, the reaction between Ti and the
proton of HF in solution, destroy the titanium oxide layer, which is responsable
for corrosion resistance of titanium alloys. Treatment with these solutions causes
significant changes on Ti surface roughness, favoring the development of more
mature plaque and hampering biofilm removal.27 Thus, mechanical hygiene of
peri-implant area should be better applied in oral hygiene routine.
CONCLUSION
The mechanical hygiene of orthodontic mini-implants by itself maintains
microbial control of the devices. The different methods applied in this study were
capable to control microbial colonization around TADs, except for the
Cetylpyridinium Chloride 0.05% mouthwash.

85
REFERENCES
1. Apel S, Apel C, Morea C, Tortamano A, Dominguez GC, Conrads G.
Microflora ssociated with succesful and failed orthodontic mini-implants.
Clin Oral Impl Res. 2009;20:1186-190.
2. Bae S, Park H, Kyung H, Kwon O, Sung J. Clinical Application of Micro-
Implant Anchorage. JCO. 2002 May;36(5):298-302.
3. Celenza F, Hockman MN. Absolute Anchorage in Orthodontics: Direct and
Indirect Implant-Assisted Modalities. JCO. 2000 Jul;34(7):397-402.
4. Freitas AOA, Alviano CS, Alviano DS, Siqueira Jr JF, Nojima LI, Nojima
MCG. Microbial colonization in orthodontic mini-implants. Braz Dent J.
2012;23(4):422-27.
5. Wu TY, Kuang SH, Wu CH. Factors associated with the stability of mini-
implants for orthodontic anchorage: a study of 414 samples in Taiwan. Int
J Oral Maxillofac Surg. 2009;67:1595-99.
6. AlSamak S, Bitsanis E, Makou M, Eliades G. Morphological and structural
characteristics of orthodontic mini-implants. J Orofac Orthop. 2012
Jan;73:58-71.
7. Tortamano A, Dominguez GC, Haddad ACSS, Nunes FD, Nacao M,
Morea C. Periodontopathogens around the surface of mini-implants
removed from orthodontic patients. Angle Orthod.2012;82(4):591-95.
8. Tseng YC, Hsieh CH, Chen CH, Shen YS, Huang IY, Chen CM. The
application of mini-implants for orthodontic anchorage. Int J Oral
Maxillofac Surg. 2006;35:704-707.
9. Araújo TM, Nascimento MHA, Bezerra F, Sobral MC. Skeletal anchorage
in orthodontics with Mini-implants. Dental Press J Orthod. 2006
Jul/Aug;11(4):126-56.

86
10. Carano A, Velo S, Leone P, Siciliani G. Clinical Aplications of the
Miniscrew Anchorage System. JCO. 2005Jan;39(1):9-24.
11. Ferreira JR SB, Figueiredo CM, Almeida ALPF, Assis GF, Dionísio TJ,
Santos FC. Clinical, Histological, and Microbiological Finding in Peri-
implant Disease: A Pilot Study. Implant Dentistry. 2009;18(4):334-44.
12. Gray JB, Smith R. Transitional Implants for Orthodontic Anchorage. JCO.
2000 Nov;34(11):659-66.
13. Heuer W, Elter C, Demling A, Neumann A, Suerbaum S, Hannig M,
Heidenblut T, Bach W, Stiesch-Scholz M. Analysis of Early Biofilm
Formation on Oral Implants in Man. J Oral Rehabil. 2007;34:377-82.
14. Luzi C, Verna C, Melsen B. Guidelines for Success in Placement of
Orthodontic Mini-Implants. JCO. 2009;43(1):39-44.
15. Mah J, Bugstrand F, Graham JW. Temporary Anchorage Devices, a
Status Report. JCO. 2005;39(3):132-36.
16. Melsen B. Mini-implants: Where are we? JCO. 2005 Sept;39(9):539-47.
17. Miyawaki S, Koyama I, Inoue M, Mishima K, Sugahara T, Takano YT.
Factors Associated with the Stability of the Titanium Screws Placed in the
Posterior Region for Orthodontic Anchorage. Am J Orthod Dentofacial
Orthop.2003 Oct;124(4):373-378.
18. Pier-Francesco A, Adams RJ, Waters MGJ, Wiliams DW. Titanium
Surface Modification and its Effect on the Adherence of Porphyromonas
gingivalis: an in vitro study. Clin Oral Impl Res. 2006;17:633-37.
19. Wilmes B, Rademacher C, Olthoff G, Drescher D. Parameters Affecting
Primary Stability of Orthodontic Mini-implants. J Orofac Orthoped. 2006
Mar;3:162-74.
87
20. Yoshinari M, Oda Y, Kato T, Okuda K, Hirayama A. Influence of Surface
Modifications to Titanium on Oral Bacterial Adhesion in vitro. J Biomed.
Mater Res. 2000;52(2):388-94.
21. Bürgers R, Gerlach T, Hahnel S, Schwarz F, Handel G, Gosau M. In vivo
and in vitro biofilm formation on two different titanium implant surfaces.
Clin Oral Impl Res. 2010;21:156-164.
22. Dorkhan M, de Paz LEC, Skepö M, Svensäter G, Davies JR. Effects of
saliva or serum coating on adherence of Streptococcus oralis strains to
titanium. Microbiology.2012;158:390-397.
23. Gosau M, Hahnel S, Schwarz F, Gerlach T, Reichert TE, Bürgers R.
Effects of six different peri-implantitis disinfection methods on in vivo
human oral biofilm. Clin Oral Impl Res. 2010;21:866-72.
24. Subramani K, Jung RE, Molenberg A, Hämmerie CHF. Biofilm on dental
implants: a review of literature. Int J Oral Maxillofac Implants. 2009;24:616-
626.
25. Teughels W, Assche NV, Sliepen I, Quirynen M. Effect of material
characteristics and/or surface topography on biofilm development. Clin
Oral Impl Res. 2006;17(Suppl 2):68-81.
26. Lee A, Wang HL. Biofilm related to dental implants. Implant Dentistry.
2010;19(5):387-93.
27. Stájer A, Urbán E, Pelsöczi IK, Mihalik E, Rakonczay Z, Nagy K, Turzó K,
Radnai M. Effect of caries preventive products on the growth of bacterial
biofolm on titanium surface. Acta Microbiol Immunol Hung. 2012;59(1):51-
61.

88
28. Gerber J, Wenaweser D, Heitz-Mayfield L, Lang PL, Person GR.
Comparison of Bacterial Plaque Samples from Titanium Implant and Tooth
Surfaces by Different Methods. Clin Oral Impl Res. 2006;17:1-6.
29. Jervöe-Storm PM, Alahdab H, Koltzscher M, Fimmers R, Jepsen S.
Comparison of Curet and Paper Point Sampling of Subgingival Bacteria
as Analyzed by Real-Time Polymerase Chain Reaction. J Periodontol.
2007;78(5):909-17.
30. Morikawa M, Chiba T, Tomii N, Sato S, Takahashi Y, Konishi K, Numabe
Y, Iwata K, Imai K. Comparative Analysis of Putative Pariodontopathic
Bacteria by Multiplex Polymerase Chain Reaction. J Periodont Res.
2008;43:268-74.
31. Naranjo AA, Triviño ML, Jaramillo A, Betancourth M, Botero JH. Changes
in the Subgingival Microbiota and Periodontal Parameters Before and 3
Months after Bracket Placement. Am J Orthod Dentofacial Orthop.
2006;130(3):275.e17-275.e22.
32. Botero JE, González AM, Mercado RA, Olave G, Contreras A. Subgingival
Microbiota in Peri-Implant Mucosa Lesions and Adjacent Teeth in Partially
Edentulous Patients. J Periodontol. 2005;76(9):1490-1495.
33. Hartroth B, Seyfahrt I, Conrads G. Sampling of Periodontal Pathogens by
Paper Points: Evaluation of Basic Parameters. Oral Microbiol Immunol.
1990;(14):326-30.
34. Sakamoto M, Takeuchi Y, Umeda M, Ishikawa I, Benno Y. Rapid Detection
and Quantification of Five Periodontopathic Bacteria by Real-Time PCR.
Microbiol Immunol. 2001;45(1):39-44.

89
35. Roças IN, Siqueira JR JF, Andrade AFB, Uzeda M. Identification of
Selected Putative Oral Pathogens in Primary Root Canal Infections
Associated with Symptoms. Anaerobe. 2002;(8): 200-8.
36. Smith GLF, Socransky SS, Smith CM. Rapid method for the purification of
DNA from subgingival microorganisms Oral Microbiol Immunol. 1989;4:47-
51.
37. Paiva SSM, Siqueira Jr JF, Rôças IN, Carmo FL, Leite DCA, Ferreira DC,
Rachid CTC, Rosado AS. Molecular microbiological evaluation of passive
ultrassonic activation as a supplemantary disinfecting step: A clinica study.
J Endod. 2013; 39(2):190-194.
38. Huang R, Li M, Gregory RL. Bacterial interactions in dental biofilm.
Virulence. 2011 Sept/Oct; 2(5):435-44.
39. Sato R, Sato T, Takahashi I, Sugawara I, Takahashi N. Profiling of
Bacterial Flora in Crevices around Titanium Orthodontic Anchor Plates,
Clin Oral Impl Res. 2007;18:21-6.
40. Squeff LR, Simonson MBA, Elias CN, Nojima LI. Characterization of mini-
implants used for orthodontic anchorage. Dental Press J Orthod.
2008;13(5):45-56.
41. Pithon MM, NOJIMA LI, NOJIMA MCG, Ruellas ACO. Evaluation of
Flexural Strength and Fracture resistance of Orthodontic Mini-implants.
Dental Press J Orthod. 2008;13(5):128-33.
42. Mineoka T, Awano S, Rikimaru T, Kurata H, Yoshida A, Ansai T, Takehara,
T. Site-Specific Development of Periodontal Disease is Associated with
Increase levels of Porphyromonas gingivalis, Treponema denticola and
Tannerella forsythia in Subgingival Plaque. J Periodontol. 2008;79(4):670-
676.

90
43. Lee A, Wang HL. Biofilm related to dental implants. 2010;19(5):387-93
44. Cortelli JR, Aquino DR, Cortelli SC, Fernandes CB, Carvalho-Filho J,
Franco GC et al. Etiological Analysis of Initial Colonization of Periodontal
Pathogens in Oral Cavity. J Clin Microbiol. 2008;46(10):1322-29.
45. Bogren A, Teles RP, Torresyap G, Haffajee AD, Socransky SS,
Wennström JL. Clinical and microbiologic changes associated with the
combined use of a powered toothbrush and a triclosan/copolymer
dentifrice: a 3-year prospective study. J Periodontol. 2007
Sep;78(9):1708-17.
46. Slots J, Rams TE, Schonfeld SE. In vitro activity of chlorhexidine against
enteric rods, pseudomonads and acinetobacter from human periodontitis.
Oral Microbiol Immunol. 1991 Feb;6(1):62-4.
47. Quirynen M, Teughels W, De Soete M, Van Steenbergh D. Topical
antiseptics and antibioticsin the initial therapy of chronic adult periodontitis:
microbiological aspects. Periodontol 2000. 2002; 28:72-90.
48. Mandel ID. Antimicrobial mouthrinses: overview and update. JADA.
1994;125:2-10.
49. Gusberti FA, Sampathkumar P, Siegrist BE, Lang NP. Microbiological and
clinical effects of chlorhexidine digluconate and hydrogenperoxide
mouthrinses on developing plaque and gingivitis. J Clin Periodontol. 1988
Jan;15(1):60-7.
91
50. Haroszthy VI, Zambon JJ, Sreenivasan PK. Evaluation of the
antimicrobial activity of dentifrices on human oral bacteria. J Clin Dent.
2010;21(4):96-100.
51. Walker C, Borden LC, Zambon JJ, Bonta CY, Devizio W, Volpe AR. The
effects of a 0.3% triclosan-containing dentifrice on the microbial
composition of supragingival plaque. J Clin Periodontol. 1994
May;21(5):334-41.
52. Allen DR, Davies R, Bradshaw B, Ellwood R, Simone AJ, Robinson R et
al. Efficacy of a mouthrinse containing 0.05% cetylpyridinium chloride for
the control of plaque and gingivitis: a 6-month clinical study in adults.
Compend Contin Educ Dent. 1998;19(2 Suppl):20-6.
53. Escribano M, Herrera D, Morante S, Teughels W, Quirynen M, Sanz M.
Efficacy of a low-concentration chlorhexidine mouth rinse in non-compliant
periodontitis patients attending a supportive periodontal care programme:
a randomized clinical trial. J Clin Periodontol. 2010 Mar;37(3):266-75.
54. Hu D, Li X, Sreenivasan PK, Devizio W. A randomized, double-blind
clinical study to assess the antimicrobial effects of a cetylpyridinium
chloride mouth rinse on dental plaque bacteria. Clin Ther. 2009
Nov;31(11):2540-8.
55. Pizzo G, Guiglia R, Imburgia M, Pizzo I, D'angelo M, Giuliana G. The
effects of antimicrobial sprays and mouthrinses on supragingival plaque
regrowth: a comparative study. J Periodontol. 2006 Feb;77(2):248-56.
56. Shim JY, Yim SB, Chung JH, Hong KS. Antiplaque and antigingivitis
effects of a mouthrinse containing cetylpyridinium chloride, triclosan and
dipotassium glycyrrhizinate. J Periodontal Implant Sci. 2012 Apr;42(2):33-
8. Epub 2012 Apr 30.

92
57. Lang NP, Sander L, Barlow A, Brennan K, White DJ, Bacca L et al.
Experimental gingivitis studies: effects of triclosan and triclosan-containing
dentifrices on dental plaque and gingivitis in three-week randomized
controlled clinical trials. J Clin Dent. 2002;13(4):158-66.
58. Andrade AR, Machón L, Chávez N. Effectiveness of a mouthwash
containing Triclosan and Gantrez in the reduction of biofilm and gingivitis:
a clinical pilot study.J Contemp Dent Pract. 2009 Nov 1;10(6):E033-40.
59. Ciancio SG. Controlling biofilm with evidence-based dentifrices. Compend
Contin Educ Dent. 2011 Jan-Feb;32(1):70-6.
60. Sreenivasan PK, Vered Y, Zini A, Mann J, Kolog H, Steinberg D, Zambon
JJ. A 6-month study of the effects of 0.3% triclosan/copolymer dentifrice
on dental implants. J Clin Periodontol. 2011 Jan;38(1):33-42.
93
5 DISCUSSÃO
A influência dos fatores biológicos associados ao sucesso dos mini-
implantes ortodônticos é um aspecto ainda pouco explorado a despeito da sua
importância. Apesar do pouco tempo de permanência destes dispositivos
transitórios de ancoragem, quando comparado ao período total do tratamento
ortodôntico ou ao tempo de permanência de um elemento dentário ou implante,
não se justifica a escassez de pesquisas sobre o assunto. A inflamação do tecido
adjacente ao parafuso gera desconforto e pode causar perda de estabilidade do
mesmo, na ausência de terapia adequada.
A área peri-implantar, que corresponde à área de contato entre o perfil
transmucoso do mini-implante e a gengiva inserida adjacente é responsável pelo
selamento mucoso e proteção do dispositivo contra adesão e retenção
microbiana (AL-AHMAD et al, 2013; BURGÜERS et al, 2009; DORKHAN et al,
2012; FREITAS et al, 2012; STÁJER et al, 2012; SUBRAMANI et al, 2009). Ao
ser inserido na cavidade bucal, a superfície do mini-implante e a mucosa definem
um novo sulco, o qual, dependendo da localização, pode oferecer dificuldades
para o acesso clínico e a higienização (FREITAS et al, 2012; LEE e WANG,
2010; STÁJER et al, 2012). Portanto, o perfil transmucoso foi eleito como região
de interesse para os experimentos in vitro e in vivo que têm sido desenvolvidos.
A literatura apresenta estudos prévios abordando alguns fatores que
podem interferir no controle microbiano dos mini-implantes, como as

94
propriedades do material do dispositivo, os métodos de higienização aplicados,
a colaboração e as características individuais dos pacientes.
A importância das características da superfície dos materiais
odontológicos é bastante discutida na literatura científica, visto que interferem no
seu comportamento na cavidade bucal (QUIRYNEN et al, 2009). Os mini-
implantes são constituídos de ligas de titânio T6Al4V, pois este material apresenta
excelentes características de superfície e biocompatibilidade, além de
resistência mecânica, resistência à corrosão (ALSAMAK et al, 2012;
SUBRAMANI et al, 2009).
Com o objetivo de determinar a topografia do material de maior
rugosidade de superfície, para o desenvolvimento do experimento in vitro, foi
desenvolvido o estudo preliminar com três marcas comerciais de mini-implantes
nacionais (página 44). Para tal, estes foram submetidos à microscopia eletrônica
de varredura (MEV) e microscopia de força atômica (MFA).
Os resultados apresentados nas fotomicrografias e nas imagens
tridimensionais da superfície do perfil transmucoso dos mini-implantes
analisados encontram-se expostos nas Figuras 1 e 2 (páginas 48 e 49), e
corroboram com estudo já publicado, evidenciando a irregularidade na topografia
dos DTA, com estrias paralelas entre si e defeitos estruturais ao longo do perfil
transmucoso (ALSAMAK et al, 2012). Os autores também concordam que
fabricantes deveriam produzir materiais com superfície mais lisa e homogênea,
no intuito de diminuir o potencial de adesão microbiana nos mini-implantes
ortodônticos (BÜRGERS et al, 2009; DRAKE et al, 1999; QUIRYNEN et al,
1993). Além da diferença entre as marcas avaliadas, observou-se, também, a
diferença visual importante entre dispositivos de um mesmo fabricante,
95
ratificando a necessidade de melhor acabamento das peças (Tabela 1, página
49).
BOLLEN et al (1997) sugeriram o valor de 0,2 µm Ra como valor máximo
de rugosidade de superfície para o controle da adesão bacteriana. Os valores
encontrados no presente estudo mostraram a marca SIN® (São Paulo, SP,
Brasil) com os maiores valores de rugosidade de superfície do perfil
transmucoso, apresentando diferença estatística em relação aos demais mini-
implantes avaliados (Tabela 1, página 49). Os dispositivos da marca SIN®
revelaram média de rugosidade maior em relação àquela considerada ideal para
o controle microbiano, determinada em 0,25 µm. No entanto, transpondo os
resultados para a aplicação clínica de fato, os autores deste estudo não
acreditam que 0,05 µm comprometam sua utilização na prática ortodôntica,
quando realizada higienização adequada.
Após a exposição do titânio à cavidade bucal, forma-se imediatamente
uma película salivar, apesar desta apresentar menor capacidade de adsorção da
albumina sobre o material considerado (LEE e WANG, 2010). As proteínas da
película salivar agem como receptores para adesão de micro-organismos sobre
a superfície do titânio, com subsequente formação de biofilme (DORKHAN et al,
2012).
Superfícies rugosas favorecem o acúmulo e a retenção de placa
bacteriana (TEUGHELS et al, 2006). A rugosidade aumenta a área de superfície
disponível para colonização, com a formação de picos e vales, além de permitir
estabelecimento de ligações mais fortes entre as mesmas e a superfície do
titânio (AL-AHMAD et al, 2013; QUIRYNEN et al, 1993; RIMONDINI et al, 1997).
Portanto, o perfil transmucoso dos mini-implantes merece acabamento mais
refinado e superfície mais polida, a fim de reduzir injúrias do ambiente bucal (AL-

96
AHMAD et al, 2013; BURGÜERS et al, 2009; DORKHAN et al, 2012; FREITAS
et al, 2012; STÁJER et al, 2012; SUBRAMANI et al, 2009).
É constatado que superfícies irregulares reduzem a eficiência dos
procedimentos de higiene e, por consequência, facilitam a formação, a evolução
e o aumento da complexidade do biofilme (QUIRYNEN et al, 1993; RIMONDINI
et al, 1997; SCHMIDLIN et al, 2013). Como o selamento do sulco entre a
superfície do titânio e a mucosa adjacente é essencial para manutenção da
saúde peri-implantar, este deve ser protegido da invasão bacteriana (LEE e
WANG, 2010; STÁJER et al, 2012).
A formação do biofilme em implantes constituídos de titânio ocorre de
modo semelhante à superfície dentária (DHIR et al, 2013; LEE e WANG, 2010).
Logo, os colonizadores iniciais são semalhantes e são observados no estágio
inicial da formação do biofilme. A maioria das bactérias colonizadoras iniciais são
comensais, porém fornecem as condições necessárias para agregação dos
colonizadores subsequentes, como anaeróbios gram-negativos e influenciam
nos estágios de formação do biofilme (LI et al, 2004; KRETH et al, 2009; HEUER
et al, 2011).
O meio bucal é um ambiente complexo que apresenta condições
especiais, sendo de difícil reprodução em laboratório (AL-AHMAD et al, 2013).
Para observar a adesão e a formação de biofilme na superfície do perfil
transmucoso de mini-implantes ortodônticos, foi realizado o ensaio
microbiológico in vitro. Utilizou-se inóculo cultivado em laboratório, a partir da
placa supragengival coletada de pacientes ortodônticos, sob restrição de
oxigênio. Com isso, o inóculo sofreu, portanto, sua primeira seleção. Os autores
seguiram os modelos de desenvolvimento de biofilme in vitro publicados por
SÀNCHEZ et al (2011) e WALKER et al (2007). Os métodos aplicados podem

97
ter influenciado os resultados obtidos na presente pesquisa, principalmente, no
que diz respeito aos resultados nas primeiras 72 horas de experimento, pois a
renovação do meio de cultura foi realizada de 48 em 48 horas após as primeiras
72 horas de incubação (Figura 2, página 64; Anexos 7 e 8, páginas 120 e 121).
A viabilidade e a diversidade decresceram nos tempos iniciais, e aumentaram
com a renovação do meio de cultura (Figura 2, página 64; Anexos 7 e 8, págnas
120 e 121).
As imagens obtidas em MEV, neste estudo, evidenciaram adesão
microbiana após seis horas de experimento, corroborando com resultados já
descritos em estudos prévios (Figura 2, página 64; Anexos 7 e 8, páginas 120 e
121). Estes mostraram a colonização inicial após 30 minutos de inoculação; entre
intervalos de zero e duas horas assim como intervalos entre duas e seis horas
de exposição à cavidade bucal (AL-AHMAD et al, 2013; DHIR et al, 2013; LEE e
WANG, 2010; SUBRAMANI et al, 2009). STÁJER et al (2012) descreveram a
presença de colonizadores iniciais nas primeiras 24 horas de experimento, com
manutenção da colonização de modo estável até 14 dias. FREITAS et al (2012)
também detectaram a colonização inicial de streptococcus spp nas primeiras 24
horas, a qual permaneceu estável por três meses. A morfologia bacteriana
observada nas imagens de MEV (Figura 2, página 64; Anexos 7 e 8, páginas 120
e 121) mostrou variação desde os tempos iniciais, com a presença de cocos,
bastões, bacilos, filamentos curtos e longos, concordando com formas descritas
por autores em estudos anteriores, como DHIR et al (2013), KRETH et al, (2008),
RIMONDINI et al (1997) e SUBRAMANI et al (2009). Nas fotomicrografias entre
96 e 120 horas, ou seja após 4 e 5 dias do início do experimento, observou-se
organização celular mais madura (Figura 2, página 64; Anexos 7 e 8, páginas
120 e 121). Nossos achados diferem de TEUGHELS et al (2006), os quais
98
reportaram a presença de placa madura entre sete e 10 dias, aproximadamente,
com a constatação de bastões e espiroquetas. Nas fotomicrografias por
fluorescência, a colonização bacteriana na superfície do titânio dos DTA da
marca SIN® mostrou-se em camada única, com micro-colônias ou células
isoladas durante todo o tempo experimental (Figura 2, página 64; Anexos 7 e 8,
págs. 120 e 121), conforme descrito por GOSAU et al (2010).
Os resultados obtidos a partir do Checkerboard DNA-DNA hybridization
confirmaram a diversidade microbiana durante todos os tempos de avaliação
investigados no estudo in vitro aqui discutido (Figura 3, página 66). Todos os
complexos microbianos da placa supragengival descritos por HAFFAJEE et al
(2008) foram detectados nas primeiras 12 horas de incubação, inclusive os dos
complexos laranja e vermelho, que estão associados às doenças periodontais
(Figura 3, página 66). Resultados semelhantes foram descritos por LI et al (2004)
a partir da coleta de placa bacteriana da superfície dentária, exceto pela
detecção de bactérias do complexo vermelho a partir das primeiras seis horas
de experimento. Apesar da diversidade de micro-organismos observados, os
níveis bacterianos permaneceram estáveis, sem diferença estatística significante
entre os intervalos de tempo estudados (página 65). A sensibilidade da técnica
e os níveis de detecção utilizados podem ter colaborado para os baixos níveis
bactérias evidenciados. O fato de a técnica não ter detectado a presença de
determinadas espécies não significa, obrigatoriamente, que estas não estavam
presentes. Pode-se afirmar somente que não alcançaram o nível mínimo de
detecção do método aplicado.
Diante da evidência da rápida e estável colonização microbiana na
superfície do perfil transmucoso de mini-implantes ortodônticos, justifica-se,
portanto, que o método de controle microbiano adequado do sulco peri-implantar

99
tenha sido investigado nesta pesquisa (página 76). A inflamação do periodonto
ocorre quando a higiene é insatisfatória e não há controle microbiano adequado
da região peri-implantar, prejudicando a permanência dos dispositivos
temporários de ancoragem na cavidade bucal (APEL et al, 2009; BÜRGERS et
al, 2010; FREITAS et al, 2012; HOIBY et al, 2010; TORTAMANO et al, 2012;
TSENG et al, 2006).
Enxaguatórios são amplamente utilizados como produtos auxiliares da
higiene bucal, pois contribuem para a saúde bucal e geral dos pacientes,
influenciando na melhora da qualidade de vida dos mesmos (CORTELLI et al,
2010). Entretanto, autores descreveram que o uso de dentifrício fluoretado na
escovação seria suficiente para reduzir índices clínicos periodontais e diminuir o
nível de micro-organismos na microbiota bucal (BOGREN et al, 2007).
O debridamento mecânico da superfície de implantes dentários foi
descrito, por GOSAU et al (2010), como estratégia insuficiente para remoção de
todos os micro-organismos aderidos. A higiene na região implantar deveria ser
complementada por antissépticos bucais, associando as estratégias mecânica e
química para o controle microbiano (GOSAU et al, 2010).
O estudo in vivo (página 76) revelou a eficácia de todas as terapias de
controle microbiano aplicadas na metodologia, exceto pelo bochecho de cloreto
de cetilpiridínio 0,05% (p > 0,05) (Tabela 1, página 81). A quantidade total de
bactérias inespecíficas detectadas pelo PCR real-time diminuiu nos grupos
avaliados, apesar de a diferença estatística não se apresentar em todos. Este
resultado é considerado favorável ao controle microbiano, visto que a redução
do nível bacteriano é fator importante para manter o equilíbrio entre a microbiota
peri-implantar e a defesa do hospedeiro (GOSAU et al, 2010).
100
A clorexidina possui amplo espectro de atividade antibacteriana (SLOTS
et al. 1991; QUIRYNEN et al; 2002), atua na membrana celular, causando sua
ruptura e, desse modo, a lise celular (QUIRYNEN et al, 2002; BÜRGERS et al,
2008). Além disso, a clorexidina também apresenta substantividade, a qual é
definida pela capacidade de ligar-se aos tecidos e ser lentamente liberada
(MANDEL, 1994). Resultados descritos na literatura comprovam sua eficácia
(GUSBERTI e SAMPATHKURMAR, 1988) e destacam que o gluconato de
clorexidina inibe a formação de placa bacteriana na superfície dentária e ao redor
de implantes (BÜRGERS et al, 2008; GOSAU et al, 2010).
Outras substâncias antissépticas são descritas como enxaguatórios
bucais capazes de reduzir a placa bacteriana. O triclosan 0,03% apresenta alto
potencial antibacteriano, pois reduz a adesão de bactérias gram-positivas, gram-
negativas e anaeróbias (HAROSZTHY et al, 2010; WALKER et al, 1994). Porém,
os estudos avaliados por GOSAU et al (2010) não comprovaram a maior
eficiência do triclosan em relação à clorexidina.
O cloreto de cetilpiridínio 0,05% foi citado, em pesquisas anteriores, como
responsável pela redução da gengivite, do índice de placa supragengival, e do
total de bactérias presentes no sulco gengival e saliva. Constatou-se, também,
a diminuição significativa do número de bactérias anaeróbias na placa
supragengival após 14 dias de sua utilização (ALLEN et al, 1998; ESCRIBANO
et al, 2010; Hu et al, 2009).
Os resultados deste estudo não demonstraram diferença estatística entre
os quatro métodos de higiene estudados (Tabela 1, página 81), caracterizando
a higienização mecânica como método suficiente para o controle de placa nos
DAT. No entanto, estudos prévios compararam bochechos a base de clorexidina
0,12%, triclosan 0,03% e cloreto de cetilpiridínio 0,05%, determinando maior

101
eficácia da clorexidina e do triclosan no controle da recolonização bacteriana,
placa supragengival, gengivite e dos índices clínicos periodontais, após cinco
dias de uso (PIZZO et al, 2006; SHIM et al, 2012).
Considerando os dentifrícios utilizados na escovação, aqueles que
contêm triclosan 0,03% apresentaram melhores resultados quando comparados
aos convencionais, somente fluoretados (CIANCIO et al, 2011; WALKER et al,
1994). O controle microbiano peri-implantar é alcançado através da escovação
com dentifrício contendo triclosan 0,03% e copolímero. Estes dentifrícios
reduzem os índices de placa supragengival e gengivite, assim como os principais
patógenos periodontais (SREENIVASAN et al, 2011). Cabe ressaltar ainda que,
mesmo em baixas concentrações, a presença do fluoreto de sódio em ambiente
ácido estimula a reação entre o Ti e os prótons de HF, destruindo a camada de
óxido de titânio responsável pela resistência à corrosão das ligas de titânio. A
utilização de colutórios bucais, géis fluoretados ou soluções aquosas de NaF
altera a rugosidade de superfície do titânio, favorece o desenvolvimento de placa
bacteriana madura e dificulta a remoção do biofilme (STÁJER et al, 2012).
De acordo com os resultados obtidos nesta pesquisa, fica evidente a
importância da indicação do controle microbiano dos mini-implantes e da região
peri-implantar, visto que os DTA apresentam superfície favorável à adesão e
desenvolvimento de diferentes espécies de micro-organismos desde os estágios
iniciais de contato com os mesmos. A estratégia de higienização mecânica dos
DTA é eficaz e elimina a etapa adicional do controle químico do biofilme aderido,
a qual exige maior colaboração e custo adicional aos pacientes portadores
destes dispositivos. Com isso, a saúde do periodonto adjacente aos mini-
implantes seria mantida e deixaria de ser um fator contribuinte para a perda de
estabilidade dos mesmos.

102
6 CONCLUSÃO
6.1 Os mini-implantes da marca SIN® (São Paulo, SP, Brazil)
apresentaram rugosidade de superfície signicativamente maior quando
comparados aos mini-implantes das marcas INP® (São Paulo, SP, Brasil) e
Conexão® (Arujá, SP, Brasil).
6.2 A adesão microbiana, in vitro, na superfície de mini-implantes
ortodônticos foi evidenciada a partir de seis horas de incubação, com diferentes
morfologias bacterianas e seguiu sem variação importante. A colonização
bacteriana na superfície do titânio ocorreu em camada única, com micro-colônias
ou células isoladas. A quantidade e a qualidade das bactérias detectadas
mantiveram-se sem diferença estatística ao longo do estudo.
6.3 Todas as terapias de controle microbiano peri-implantar investigadas
apresentaram-se eficazes. Não houve diferença estatística entre os quatro
métodos de higiene estudados: mecânica, ou complementada com soluções à
basse de clorexidina, triclosan e cloreto de cetilpiridínio.

103
7 RECOMENDAÇÕES
7.1 Aumentar a variedade de marcas comerciais de mini-implantes
ortodônticos para avaliação topográfica, incluindo os de fabricação estrangeira,
e considerar, também, a avaliação da energia livre de superfície dos DTA;
7.2 Utilizar câmara de anaerobiose para preparar o inóculo e estudar a
adesão de micro-organismos presentes na placa subgengival, bem como a
formação de biofilme in vitro nos mini-implantes ortodônticos;
7.3 Trocar o meio de cultura utilizado no ensaio in vitro com menor
intervalo de tempo;
7.4 Aplicar PCR Real-time com método TaqMan de detecção para
diagnosticar e quantificar os micro-organismos com capacidade de adesão na
superfície de titânio ao longo do tempo;
7.5 Realizar o ensaio microbiológico in vitro com diferentes marcas
comerciais, que apresentem diferentes características de superfície, a fim de
avaliar a influência destas características na adesão e formação de biofilme;
7.6 Estudar a topografia de mini-implantes removidos da cavidade bucal,
de modo a determinar a influência do meio e da colonização microbiana sobre a
mesma.
7.7 Estender o tempo de avaliação dos métodos de higienização dos mini-
implantes ortodônticos, visando maior alcance clínico nos resultados.
104
8 REFERÊNCIAS BIBLIOGRÁFICAS
AL-AHMAD A, AL-AHMAD MW, FACKLER A, FOLLO M, HELLWIG E, BÄCHLE M, HANNIG C, HAN JS, WOLKEWITZ M, KOHAL R. In vivo study of the initial bacterial adhesion on different implant materials. Arch Oral Biol. 2013;58:1139-1147. ALLEN DR, DAVIES R, BRADSHAW B, ELLWOOD R, SIMONE AJ, ROBINSON R et al. Efficacy of a mouthrinse containing 0.05% cetylpyridinium chloride for the control of plaque and gingivitis: a 6-month clinical study in adults. Compend Contin Educ Dent. 1998;19(2 Suppl):20-6. ALSAMAK S, BITSANIS E, MAKOU M, ELIADES G. Morphological and structural characteristics of orthodontic mini-implants. J Orofac Orthop. 2012 Jan;73:58-71. ANDRADE AR, MACHÓN L, CHÁVEZ N. Effectiveness of a mouthwash containing Triclosan and Gantrez in the reduction of biofilm and gingivitis: a clinical pilot study.J Contemp Dent Pract. 2009 Nov 1;10(6):E033-40. APEL S, APEL C, MOREA C, TORTAMANO A, DOMINGUEZ GC, CONRADS G. Microflora ssociated with succesful and failed orthodontic mini-implants. Clin Oral Impl Res. 2009;20:1186-1190. ARAÚJO TM, NASCIMENTO MHA, BEZERRA F, SOBRAL MC. Ancoragem Esquelética em Ortodontia com Miniimplantes. Dental Press J Orthod. 2006 Jul/Aug;11(4):126-56. ASAI Y, JINNO T, IGARASHI H, OHYAMA Y, OGAWA T. Detection and quantification of oral treponemes in subgingival plaque by real-time PCR. J Clin Microbiol. 2002 Sep;40(9):3334-40. BAE S, PARK H, KYUNG H, KWON O, SUNG J. Clinical Application of Micro- Implant Anchorage. JCO. 2002 May;36(5):298-302. BASTANCI, N.; REDDI, D.; RANGARAJAN, M.; CURTIS, M. A.; BELIBASAKIS, G. N., Porphyromonas gingivalis Stimulates TACE Production by T cells. Oral Microbiol Immunol. 2009;24:146-151. BODET C, CHANDAD F, GRENIER D. Potentiel pathogénique de Porphyromonas gingivalis, Treponema denticola et Tannerella forsythia, le Complexe Bacterèrien Rouge Associé à la Parodontite. Pathologie Biologie. 2007;55:154-162. BOGHOSSIAN CMS, SOUTO RM, LUIZ RR, COLOMBO APV. Association of red complex, A. actinomycetemcomitans and non-oral bacteria with periodontal diseases. Arch Oral Biol. 2011; 56:899-906.
105
BOGREN A, TELES RP, TORRESYAP G, HAFFAJEE AD, SOCRANSKY SS, WENNSTRÖM JL. Clinical and microbiologic changes associated with the combined use of a powered toothbrush and a triclosan/copolymer dentifrice: a 3-year prospective study. J Periodontol. 2007 Sep;78(9):1708-17. BOLLEN CM, LAMBRECHTS P, QUIRYNEN M.Comparison of surface roughness of oral hard materials to the threshold surface roughness for bacterial plaque retention: a review of the literature.Dent Mater. 1997 Jul;13(4):258-269. BOTERO JE, GONZÁLEZ AM, MERCADO RA, OLAVE G, CONTRERAS A. Subgingival Microbiota in Peri-Implant Mucosa Lesions and Adjacent Teeth in Partially Edentulous Patients. J Periodontol. 2005;76(9):1490-1495. BÜRGERS R, GERLACH T, HAHNEL S, SCHWARZ F, HANDEL G, GOSAU M. In vivo and in vitro biofilm formation on two different titanium implant surfaces. Clin Oral Impl Res. 2010;21:156-164. CARANO A, VELO S, LEONE P, SICILIANI G. Clinical Aplications of the Miniscrew Anchorage System. JCO. 2005Jan;39(1):9-24. CELENZA F, HOCKMAN MN. Absolute Anchorage in Orthodontics: Direct and Indirect Implant-Assisted Modalities. JCO. 2000 Jul;34(7):397-402. CHENG SJ, TSENG Y, LEE JJ, KOK SH. A Prospective Study of the Risk Factors Associated with Failure of Mini-implants Used for Orthodontic Anchorage. Int J Oral Maxillofac Implants. 2004;19(1):100-106. CIANCIO SG. Controlling biofilm with evidence-based dentifrices. Compend Contin Educ Dent. 2011 Jan-Feb;32(1):70-6.
COLOMBO AP, TELES RP, TORRES MC, SOUTO R, ROSALEM WJ, MENDES MC, UZEDA M. Subgingival microbiota of Brazilian subjects with untreated chronic periodontitis. J Periodontol. 2002;73:360-369.
COLOMBO AP, TELES RP, TORRES MC, SOUTO R, ROSALEM WJ, MENDES MC, UZEDA M. Effects of non-surgical mechanical therapy on the subgingival microbiota of Brazilians with untreated chronic periodontitis: 9-month results. J Periodontol. 2005; 76: 778-784. CORTELLI JR, AQUINO DR, CORTELLI SC, FERNANDES CB, CARVALHO-FILHO J, FRANCO GC et al. Etiological Analysis of Initial Colonization of Periodontal Pathogens in Oral Cavity. J Clin Microbiol. 2008;46(10):1322-29. DHIR S. Biofilm and dental implant: the microbial link. J Indian Soc Periodontol. 2013 Jan-Feb; 17(1):5-11. DORKHAN M, DE PAZ LEC, SKEPÖ M, SVENSÄTER G, DAVIES JR. Effects of saliva or serum coating on adherence of Streptococcus oralis strains to titanium. Microbiology. 2012;158:390-397. DRAKE DR, PAUL J, KELLER JC. Primary bacterial colonization of implant surfaces. Int J Oral Maxillofac Implants. 1999;14(2):226-232.
106
ESCRIBANO M, HERRERA D, MORANTE S, TEUGHELS W, QUIRYNEN M, SANZ M. Efficacy of a low-concentration chlorhexidine mouth rinse in non-compliant periodontitis patients attending a supportive periodontal care programme: a randomized clinical trial. J Clin Periodontol. 2010 Mar;37(3):266-75. Epub 2010 Jan 19. FERREIRA JR SB, FIGUEIREDO CM, ALMEIDA ALPF, ASSIS GF, DIONÍSIO TJ, SANTOS FC. Clinical, Histological, and Microbiological Finding in Peri-implant Disease: A Pilot Study. Implant Dentistry. 2009;18(4):334-44. FREITAS AOA, ALVIANO CS, ALVIANO DS, SIQUEIRA JR JF, NOJIMA LI, NOJIMA MCG. Microbial colonization in orthodontic mini-implants. Braz Dent J. 2012;23(4):422-427. GERBER J, WENAWESER D, HEITZ-MAYFIELD L, LANG PL, PERSON GR. Comparison of Bacterial Plaque Samples from Titanium Implant and Tooth Surfaces by Different Methods. Clin Oral Impl Res. 2006;17:1-6. GOSAU M, HAHNEL S, SCHWARZ F, GERLACH T, REICHERT TE, BÜRGERS R. Effects of six different peri-implantitis disinfection methods on in vivo human oral biofilm. Clin Oral Impl Res. 2010;21:866-72. GRAY JB, SMITH R. Transitional Implants for Orthodontic Anchorage. JCO. 2000 Nov;34(11):659-66. GUSBERTI FA, SAMPATHKUMAR P, SIEGRIST BE, LANG NP. Microbiological and clinical effects of chlorhexidine digluconate and hydrogenperoxide mouthrinses on developing plaque and gingivitis. J Clin Periodontol. 1988 Jan;15(1):60-7. HALLÉN U, BJÖRKNER AE, HALLBERG EC. Binding of the periodontitis associated bacterium Porphyromonas gingivalis to glycoproteins from human epithelial cells.Oral Microbiol Immunol. 2008 Oct;23(5):367-71. HAROSZTHY VI, ZAMBON JJ, SREENIVASAN PK. Evaluation of the antimicrobial activity of dentifrices on human oral bacteria. J Clin Dent. 2010;21(4):96-100. HARTROTH B, SEYFAHRT I, CONRADS G. Sampling of Periodontal Pathogens by Paper Points: Evaluation of Basic Parameters. Oral Microbiol Immunol. 1990;(14):326-30. HEUER W, ELTER C, DEMLING A, NEUMANN A, SUERBAUM S, HANNIG M, HEIDENBLUT T, BACH W, STIESCH-SCHOLZ M. Analysis of Early Biofilm Formation on Oral Implants in Man. J Oral Rehabil. 2007;34:377-82. HOIBY N, CIOFU, O, JOHANSEN HK, SONG Z, MOSER C, JANSEN PO, MOLIN S, GIVKOV M, TOLKER-NIELSEN T, BJAMSHOLT T. The clinical impacto f bacterial biofilms. Int J O Sci. 2011;3:55-65. HU D, LI X, SREENIVASAN PK, DEVIZIO W. A randomized, double-blind clinical study to assess the antimicrobial effects of a cetylpyridinium chloride mouth rinse on dental plaque bacteria. Clin Ther. 2009 Nov;31(11):2540-8.

107
HUANG R, LI M, GREGORY RL. Bacterial interactions in dental biofilm. Virulence. 2011 Sept/Oct; 2(5):435-44. INABA H, NAKANO K, KATO T, NOMURA R, KAWAI S, KUBONIWA M, ISHIHARA K, OOSHIMA T, AMANO A. Heterogenic Virulence and Related Factors among Clinical Isolates of Porphyromonas gingivalis with Type II Fimbriae. Oral Microbiol Immunol. 2008;23:29-35. ISHIGURO I, SAIKI K, KONISHI K. PG27 is a Novel Membrane Protein Essential for a Porphyromonas gingivalis Protease Secretion System. FEMS Microbiol Lett. 2009;292:261-267.
JERVÖE-STORM PM, ALAHDAB H, KOLTZSCHER M, FIMMERS R, JEPSEN S. Comparison of Curet and Paper Point Sampling of Subgingival Bacteria as Analyzed by Real-Time Polymerase Chain Reaction. J Periodontol. 2007;78(5):909-17. KANOMI R. Mini-Implant for Orthodontic Anchorage. JCO.1997;31(11):763-767. KAWADA M, YOSHIDA A, SUZUKI N, NAKANO Y, SAITO T, OHO T, KOGA T. Prevalence of Porphyromonas gingivalis in Relation to Periodontal Status assessed by Real-Time PCR. Oral Microbiol Immunol. 2004;19: 289-292. KOLENBRANDER PE, ANDERSEN RN. Inhibition of Coaggregation Between Fusobacterium nucleatum and Porphyromonas gingivalis by Lactose and Related Sugars. Infection and Immunity. 1989;57(10):3204-3209. KRETH J, MERRITT J, QI F. Bacterial and host interactions of oral streptococci. DNA and Cell Biology. 2009;28(8):397-403. KURAMITSU HK, CHEN W, IKEGAMI A. Biofilm Formation by the Periodontopathic Bacteria Treponema denticola and Porphyromonas gingivalis. J Periodontol.2005;76(11):2047-2051. KYUNG HM, PARK HS, BAE SM, SUNG JH, KIM IB. Development of orthodontic micro-implants for intraoral anchorage. JCO. 2003 Jun;37(6):321-323. LANG NP, SANDER L, BARLOW A, BRENNAN K, WHITE DJ, BACCA L et al. Experimental gingivitis studies: effects of triclosan and triclosan-containing dentifrices on dental plaque and gingivitis in three-week randomized controlled clinical trials. J Clin Dent. 2002;13(4):158-66. LEE A, WANG HL. Biofilm related to dental implants. Implant Dentistry. 2010;19(5):387-93. LI J, HELMERHORST EJ, LEONE CW, TROXLER RF, YASKELL T, HAFFAJEE AD, SOCRANSKY SS, OPPENHEIM FG. Identification of early microbial colonizers in human dental biofilm. J Appl Microbiol. 2004;97: 1311-1318. LIOU EJW, PAI BCJ, LIN JCY. Do Miniscrews Remain Stationary Under Orthodontic Forces? Am J Orthod Dentofacial Orthoped. 2004 July;126(1):42-47. LOURENÇO TGB. Avaliação longitudinal do perfil microbiológico e da resistência do biofilme subgengival de pacientes com periodontite agressiva generalizada aos

108
antimicrobianos clorexidina, amoxicilina e metronidazol. 2011; Monografia (Bacharelado em Ciências Biológicas: Microbiologia e Imunologia) xviii; 68f. - Rio de Janeiro: UFRJ/Instituto de Microbiologia Paulo de Góes. LUZI C, VERNA C, MELSEN B. Guidelines for Success in Placement of Orthodontic Mini-Implants. JCO. 2009;43(1):39-44. Mah J, Bugstrand F, Graham JW. Temporary Anchorage Devices, a Status Report. JCO. 2005;39(3):132-36. MANDEL ID. Antimicrobial mouthrinses: overview and update. JADA. 1994;125:2-10. MARTÍNEZ-PABÓN MC, RESTREPO-OSPINA DP, ISAZA G, OROZCO-ROJAS LM, TOBÓN-ÁRROYAVE SI. Detection of Treponema denticola em Saliva Obtained from Patients with Various Periodontal Conditions. Clin Oral Invest. 2008;12:73-81. MELSEN B. Mini-implants: Where are we? JCO. 2005 Sept;39(9):539-47. MINEOKA T, AWANO S, RIKIMARU T, KURATA H, YOSHIDA A, ANSAI T, TAKEHARA, T. Site-Specific Development of Periodontal Disease is Associated with Increase levels of Porphyromonas gingivalis, Treponema denticola e Tannerella forsythia in Subgingival Plaque. J Periodontol. 2008;79(4):670-676. MIYAWAKI S, KOYAMA I, INOUE M, MISHIMA K, SUGAHARA T, TAKANO YT. Factors Associated with the Stability of the Titanium Screws Placed in the Posterior Region for Orthodontic Anchorage. Am J Orthod Dentofacial Orthop.2003 Oct;124(4):373-378. MORIKAWA M, CHIBA T, TOMII N, SATO S, TAKAHASHI Y, KONISHI K, NUMABE Y, IWATA K, IMAI K. Comparative Analysis of Putative Pariodontopathic Bacteria by Multiplex Polymerase Chain Reaction. J Periodont Res. 2008;43:268-74. NAKANO, K.; KUBONIVA, M.; NAKAGAWA, I.; YAMAMURA, T.; NOMURA, R.; OKAHASHI, N.; OOSHIMA, T.; AMANO, A., Comparison of Inflammatory Changes caused by Porphyromonas gingivalis with Distinct fimA Genotypes in Mouse Abscess Model. Oral Microbiol Immunol. 2004;19:205-209. NARANJO AA, TRIVIÑO ML, JARAMILLO A, BETANCOURTH M, BOTERO JH. Changes in the Subgingival Microbiota and Periodontal Parameters Before and 3 Months after Bracket Placement. Am J Orthod Dentofacial Orthop. 2006;130(3):275.e17-275.e22. PAIVA SSM, SIQUEIRA JR JF, RÔÇAS IN, CARMO FL, LEITE DCA, FERREIRA DC, RACHID CTC, ROSADO AS. Molecular microbiological evaluation of passive ultrassonic activation as a supplemantary disinfecting step: A clinica study. J Endod. 2013; 39(2):190-194. PASTER BJ, BOCHES SK, GALVIN JL, ERICSON RE, LAU CN, LEVANOS VA, SAHASRABUDHE A, DEWHIRST F. Bacterial Diversity in Human Subgingival Plaque. J Bacteriol. 2001;183(12):3770-3783.

109
PIER-FRANCESCO A, ADAMS RJ, WATERS MGJ, WILIAMS DW. Titanium Surface Modification and its Effect on the Adherence of Porphyromonas gingivalis: an in vitro study. Clin Oral Impl Res. 2006;17:633-37. PITHON MM, NOJIMA LI, NOJIMA MCG, RUELLAS ACO. Avaliação da Resistência à Flexão e Fratura de Mini-implantes Ortodônticos. Dental Press J Orthod. 2008;13(5):128-33. PHITON MM, NOJIMA MCG, NOJIMA LI. Primary stability of orthodontic mini-implants inserted into maxilla and mandible of swine. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics. 2012;66:p.in press.
PHITON MM, NOJIMA LI, NOJIMA MCG, RUELLAS ACO. Comparative study of fracture torque for orthodontic mini-implants of different trademarks. Oral Surgery. 2008;1:84-87.
PIZZO G, GUIGLIA R, IMBURGIA M, PIZZO I, D'ANGELO M, GIULIANA G. The effects of antimicrobial sprays and mouthrinses on supragingival plaque regrowth: a comparative study. J Periodontol. 2006 Feb;77(2):248-56. POGNARISORN NJ, GEMMELL E, TAN AES, HENRY PJ, MARSHALL RI,; SEYMOUR GJ. Inflammation Associated with Implants with Different Surface Types. Clin Oral Impl Res. 2007;18:114-125. QUIRYNEN M, TEUGHELS W, DE SOETE M, VAN STEENBERGH D. Topical antiseptics and antibioticsin the initial therapy of chronic adult periodontitis: microbiological aspects. Periodontol 2000. 2002; 28:72-90. QUIRYNEN M, VAN DER MEI HC, BOLLEN CML, SCHOTTE A, MARECHAL M, DOORNBUSCH GI, NAERT I, BUSSCHER HJ. An in vivo study of the influence of the surface roughness of implants on the microbiology of supra and subgingival plaque. J Dent Res. 1993;72:1304-1309. RASPERINI G, MAGLIONE M, COCCONCELLI PS, SIMION M. In vivo early plaque formation on pure titanium and ceramic abutments: a comparative microbiological and SEM analysis.Clin Oral Impl Res. 1998; 9:357-364. RIEP B, EDESI-NEUB L, CLAESSEN F, SKARABIS H, EHMKE B, FLEMMIG TF, BERNIMOULIN JP, GÖBEL UB, MOTER A. Are Putative Periodontal Pathogens Reliable Diagnostic Markers? J Clin Microbiol. 2009; 47(6):434-442. RIMONDINI L, FARÈ S, BRAMBILLA, FELLONI A, CONSONNI C, BROSSA F, CARASSI A. The effect of surface roughness on early in vivo plaque colonizationon titanium. J Periodontol.1997;68:556-562. RINALDI JC, ARANA-CHAVEZ V. Ultrastructure of the interface between periodontal tissues and titanium mini-implants. Angle Orthod.2010;80(3):459-465. ROÇAS IN, SIQUEIRA JR JF, ANDRADE AFB, UZEDA M. Identification of Selected Putative Oral Pathogens in Primary Root Canal Infections Associated with Symptoms. Anaerobe. 2002;(8): 200-8. SAKAMOTO M, TAKEUCHI Y, UMEDA M, ISHIKAWA I, BENNO Y. Rapid Detection and Quantification of Five Periodontopathic Bacteria by Real-Time PCR. Microbiol Immunol. 2001;45(1):39-44.
110
SÁNCHEZ MC, LLAMA-PALACIOS A, BLANC V, LÉON R, HERRERA D, SANZ M. Structure, viability and bacterial kinetics of an in vitro biofilm model using six bacteria from the subgingival microbiota. J Periodont Res. 2011; 46:252-260. SANTOS FA, BASTOS EMA, RODRIGUES PH, UZEDA M, CARVALHO MAR, FARIAS LM, MOREIRA ESA. Susceptibility of Prevotella intermedia / Prevotella nigrescens (and Porphyromonas gingivalis) to Propolis (Bee Glue) and other Antimicrobial Agents. Anaerobe. 2002;8:9-15. SATO R, SATO T, TAKAHASHI I, SUGAWARA I, TAKAHASHI N. Profiling of Bacterial Flora in Crevices around Titanium Orthodontic Anchor Plates, Clin Oral Impl Res. 2007;18:21-6. SCHIMIDLIN PR, MÜLLER P, ATTIN M, WIELAND M, HOFER D, GUGGENHEIM B. Polyspecies biofilm formationon implant surfaces with different surface characteristics. J Appl Oral Sci. 2013;21(1):48-53. SHIM JY, YIM SB, CHUNG JH, HONG KS. Antiplaque and antigingivitis effects of a mouthrinse containing cetylpyridinium chloride, triclosan and dipotassium glycyrrhizinate. J Periodontal Implant Sci. 2012 Apr;42(2):33-8. Epub 2012 Apr 30. SILVA DL, MATTOS CT, SIMÃO RA, RUELLAS ACO. Coating stability and surface characteristics of esthetic orthodontic coated archwires. Angle Orthod. 2013 Nov;83(6):994-1001. SINGH K, KUMAR D, JAISWAL RK, BANSAL A. Temporary anchorage devices- mini-implants. Natl Maxillofac Surg.2010 Jan/Jun;1(1):30-34.
SLOTS J, RAMS TE, SCHONFELD SE. In vitro activity of chlorhexidine against enteric
rods, pseudomonads and acinetobacter from human periodontitis. Oral Microbiol Immunol.
1991 Feb;6(1):62-4.
SMITH GLF, SOCRANSKY SS, SMITH CM. Rapid method for the purification of DNA from subgingival microorganisms Oral Microbiol Immunol. 1989;4:47-51.
SOCRANSKY SS, SMITH C, MARTIN L, PASTER BJ, DEWHIRST FE, LEVIN AE. Checkerboard DNA-DNA hybridization.Biotechniques. 1994 Oct;17(4):788-92.
SQUEFF LR, SIMONSON MBA, ELIAS CN, NOJIMA LI. Caracterização de mini-implantes utilizados na ancoragem ortodôntica. Dental Press J Orthod. 2008;13(5):45-56. SREENIVASAN PK, VERED Y, ZINI A, MANN J, KOLOG H, STEINBERG D, ZAMBON JJ. A 6-month study of the effects of 0.3% triclosan/copolymer dentifrice on dental implants. J Clin Periodontol. 2011 Jan;38(1):33-42 STÁJER A, URBÁN E, PELSÖCZI IK, MIHALIK E, RAKONCZAY Z, NAGY K, TURZÓ K, RADNAI M. Effect of caries preventive products on the growth of bacterial biofolm on titanium surface. Acta Microbiol Immunol Hung. 2012;59(1):51-61.
111
SUBRAMANI K, JUNG RE, MOLENBERG A, HÄMMERIE CHF. Biofilm on dental implants: a review of literature. Int J Oral Maxillofac Implants. 2009;24:616-626. TEUGHELS W, ASSCHE NV, SLIEPEN I, QUIRYNEN M. Effect of material characteristics and/or surface topography on biofilm development. Clin Oral Impl Res. 2006;17(Suppl 2):68-81. TORTAMANO A, DOMINGUEZ GC, HADDAD ACSS, NUNES FD, NACAO M, MOREA C. Periodontopathogens around the surface of mini-implants removed from orthodontic patients. Angle Orthod.2012;82(4):591-595. TRAN SD, RUDNEY JD. Multiplex PCR Using Conserved and Species-Specific 16S rRNA Gene Primers for Simultaneous Detection of Actinobacillus Actinomycetemcomitans and Porphyromonas gingivalis. J Clin Microbiol.1996;34(10):443-452. TSENG YC, HSIEH CH, CHEN CH, SHEN YS, HUANG IY, CHEN CM. The application of mini-implants for orthodontic anchorage. Int J Oral Maxillofac Surg. 2006;35:704-707. VERNAL R, LEÓN R, SILVA A, VAN WINKELHOFF AJ, GARCIA-SANZ JA, SANZ M. Differential cytokine expression by human dendritic cells in response to different Porphyromonas gingivalis capsular serotypes. J Clin Periodontol. 2009 Oct;36(10):823-9. WALKER C, BORDEN LC, ZAMBON JJ, BONTA CY, DEVIZIO W, VOLPE AR. The effects of a 0.3% triclosan-containing dentifrice on the microbial composition of supragingival plaque. J Clin Periodontol. 1994 May;21(5):334-41. WILMES B, RADEMACHER C, OLTHOFF G, DRESCHER D. Parameters Affecting Primary Stability of Orthodontic Mini-implants. J Orofac Orthoped. 2006 Mar;3:162-74. WU TY, KUANG SH, WU CH. Factors associated with the stability of mini-implants for orthodontic anchorage: a study of 414 samples in Taiwan. Int J Oral Maxillofac Surg. 2009;67:1595-1599.
YOSHINARI M, ODA Y, KATO T, OKUDA K, HIRAYAMA A. Influence of Surface Modifications to Titanium on Oral Bacterial Adhesion in vitro. J Biomed. Mater Res. 2000;52(2):388-94.
112
9 ANEXOS
9.1 ANEXO 1: TERMO DE CONSENTIMENTO LIVRE E ESCLARECIDO
TERMO DE CONSENTIMENTO LIVRE E ESCLARECIDO
Essas informações estão sendo fornecidas de modo a convidá-lo (a) a
participar de maneira voluntária na pesquisa denominada: Caracterização de
aspectos biológicos associados aos mini-implantes ortodônticos, que tem
como objetivo verificar os microorganismos que vivem ao redor dos mini-
implantes, determinar o melhor método de mantê-los limpos e combater esses
microorganismos.
Essa pesquisa justifica-se pela grande indicação e utilização destes
dispositivos como auxiliares de ancoragem no tratamento ortodôntico. Além
disso, a inflamação na região de inserção dos mini-implantes corresponde a uma
das principais causas da perda clínica desses dispositivos, e conseqüente
prejuízo no andamento do tratamento.
Você deverá estar matriculado e encontrar-se em tratamento na Clínica
de Ortodontia do Departamento de Odontopediatria e Ortodontia da Faculdade
de Odontologia da UFRJ, além de apresentar indicação da utilização de mini-
implantes no seu plano de tratamento. Será orientado a seguir as instruções de
higiene bucal determinadas por um protocolo, de modo a não haver prejuízos
quanto à saúde bucal durante o seu período de realização. Com a finalidade de
pesquisa, será realizado o seguinte procedimento, além do tratamento de rotina:
Universidade Federal do Rio de Janeiro Faculdade de Odontologia Departamento de Odontopediatria e Ortodontia Curso de Pós-Graduação em Odontologia - Ortodontia
113
Coleta de fluido no sulco entre o mini-implante e a gengiva adjacente,
em dois dias diferentes: um inicial e outro 21 dias após o início da
higienização indicada pelo pesquisador.
Coleta de placa bacteriana ao redor dos bráquetes que compõem o
aparelho ortodôntico fixo e nos dentes.
A participação nesta pesquisa é voluntária e, em caso de desistência, o
você poderá retirar o consentimento, com a certeza de que não haverá prejuízos
em relação à sua assistência, e seus dados não serão utilizados na pesquisa.
Os resultados obtidos, na totalidade, serão publicados sob forma de
artigo, em revista de caráter científico e estarão disponíveis também no serviço.
Os dados pessoais dos participantes serão mantidos em absoluto sigilo. Os
resultados individuais do experimento serão de competência dos pesquisadores
envolvidos no projeto. Não será permitido o acesso a terceiros, garantindo
proteção contra qualquer tipo de discriminação ou estigmatização. Esta pesquisa
não resultará em prejuízos biológicos, psicológicos ou sociais dos seus
participantes. Qualquer dúvida ou informação adicional poderá ser respondida
pelas pesquisadoras envolvidas: Drª Amanda Osório Ayres de Freitas e Profª Drª
Matilde da Cunha Gonçalves Nojima, pelo telefone 2590-2727, sempre que
solicitadas.Caso você tenha dificuldade de entrar em contato com o pesquisador
responsável, comunique o fato à Comissão de Ética em Pesquisa do Instituto de
Estudos em Saúde Coletiva pelo telefone (21) 2598-9328 ou pelo e-mail
Acredito ter sido informado(a) de maneira satisfatória a respeito do estudo
citado acima. Eu discuti com a Dra. Amanda Osório Ayres de Freitas sobre a
minha decisão em participar desse estudo. Ficaram claros para mim quais são
os propósitos do estudo, os procedimentos a serem realizados, seus
desconfortos e riscos; as garantias de confidencialidade, e de esclarecimento
permanentes. Ficou claro também que a minha participação é isenta de
despesas e que tenho garantido o acesso ao tratamento ortodôntico durante a
pesquisa. Concordo em participar deste estudo e poderei retirar o meu
consentimento a qualquer momento, sem penalidades ou prejuízos no meu
atendimento na Instituição.
_________________________________ Data ____/____/______.
Participante da pesquisa/ Responsável

114
_________________________________ Data ____/____/______.
Profª Drª Matilde da Cunha Gonçalves Nojima
_________________________________ Data ____/____/______.
Drª Amanda Osório Ayres de Freitas

115
9.2 ANEXO 2: APROVAÇÃO DO COMITÊ DE ÉTICA
116
9.3 ANEXO 3: PROTOCOLO DE HIGIENIZAÇÃO 1
Protocolo de Higienização Controle para Grupo Mecânico
1) Higienizar sempre após as refeições;
2) Realizar higiene bucal com fio dental, escovação com pasta
fluoretada, escova interdental.
3) Higienizar isoladamente a região do mini-implante, delicadamente,
com o auxílio de escova interdental e pasta fluoretada.
Universidade Federal do Rio de Janeiro Faculdade de Odontologia Departamento de Odontopediatria e Ortodontia Curso de Pós-graduação em Odontologia - Ortodontia

117
9.4 ANEXO 4: PROTOCOLO DE HIGIENIZAÇÃO 2
Protocolo de Higienização para Grupo Clorexidina
1) Higienizar sempre após as refeições;
2) Realizar higiene bucal com fio dental, escovação com pasta
fluoretada, escova interdental.
3) Após higienizar isoladamente a região do mini-implante,
delicadamente, com o auxílio de escova dental e pasta fluoretada,
complementar a limpeza com o auxílio de escova interdental
umedecida com a solução fornecida.
Universidade Federal do Rio de Janeiro Faculdade de Odontologia Departamento de Odontopediatria e Ortodontia Curso de Pós-graduação em Odontologia - Ortodontia

118
9.5 ANEXO 5: PROTOCOLO DE HIGIENIZAÇÃO 3
Protocolo de Higienização para Grupo Triclosan
1) Higienizar sempre após as refeições;
2) Realizar higiene bucal com fio dental, escovação com pasta
fluoretada, escova interdental.
3) Após higienizar isoladamente a região do mini-implante,
delicadamente, com o auxílio de escova dental e pasta fluoretada,
complementar a limpeza com o auxílio de escova interdental
umedecida com a solução fornecida.
Universidade Federal do Rio de Janeiro Faculdade de Odontologia Departamento de Odontopediatria e Ortodontia Curso de Pós-graduação em Odontologia - Ortodontia
119
9.6 ANEXO 6: PROTOCOLO DE HIGIENIZAÇÃO 4
Protocolo de Higienização para Grupo Cloreto de Cetilpiridínio
1) Higienizar sempre após as refeições;
2) Realizar higiene bucal com fio dental, escovação com pasta
fluoretada, escova interdental.
3) Após higienizar isoladamente a região do mini-implante,
delicadamente, com o auxílio de escova dental e pasta fluoretada,
complementar a limpeza com o auxílio de escova interdental
umedecida com a solução fornecida.
Universidade Federal do Rio de Janeiro Faculdade de Odontologia Departamento de Odontopediatria e Ortodontia Curso de Pós-graduação em Odontologia - Ortodontia
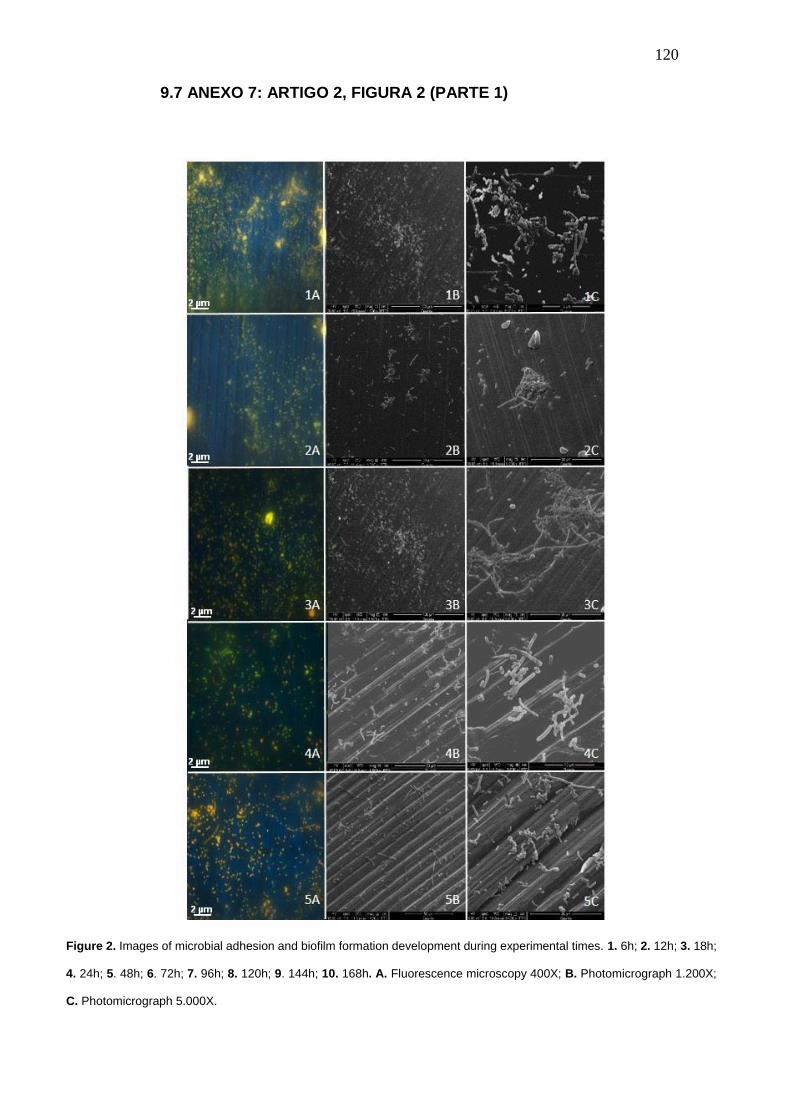
120
9.7 ANEXO 7: ARTIGO 2, FIGURA 2 (PARTE 1)
Figure 2. Images of microbial adhesion and biofilm formation development during experimental times. 1. 6h; 2. 12h; 3. 18h;
4. 24h; 5. 48h; 6. 72h; 7. 96h; 8. 120h; 9. 144h; 10. 168h. A. Fluorescence microscopy 400X; B. Photomicrograph 1.200X;
C. Photomicrograph 5.000X.

121
9.8 ANEXO 8: ARTIGO 2, FIGURA 2 (PARTE 2)
Figure 2. Images of microbial adhesion and biofilm formation development during experimental times. 1. 6h; 2. 12h; 3. 18h;
4. 24h; 5. 48h; 6. 72h; 7. 96h; 8. 120h; 9. 144h; 10. 168h. A. Fluorescence microscopy 400X; B. Photomicrograph 1.200X;
C. Photomicrograph 5.000X.