soniza vieira alves-leon professora associada de ... · • identificar etapas da fisiopatologia da...
TRANSCRIPT

SONIZA VIEIRA ALVES-LEON Professora Associada de Neurologia da
Universidade Federal do Estado do Rio de Janeiro Docente Livre em Neurologia
14:00 às 14:30 h Local: Hotel Blue Tree
CONFLITO DE INTERESSES
• Pesquisadora CNPq: Bolsista de produtividade
• Suporte FAPERJ para pesquisa e apoio a instituição
universitária
• Membro de comitê Ad Hoc CNPq e FAPERJ
• Recebeu suporte educacional e de pesquisa: Biogen Idec,
Teva, Novartis, Genzyme
• Recebeu honorários de consultoria: Novartis, Biogem Idec,
Genzyme
• Membro de Advisory Board: Novartis, Biogen Idec, Genzyme

OBJETIVOS
• Identificar etapas da fisiopatologia da Esclerose Múltipla
e alvos terapêuticos em potencial
• Identificar o papel dos Fármacos Modificadores do curso
da Doença (FMCD) que têm no seu racional diferentes
alvos terapêuticos e vêm mudando os paradigmas de
tratamento da EM

• O SNC é dotado de um repertório de resposta elaborada denominado 'neuroinflamação', que lhe permite lidar com patógenos, toxinas, traumas e degeneração.
• Ações orquestradas por células do sistema imunológico, células vasculares e neurônios, que constituem a neuroinflamação, não são apenas provocados por condições patológicas, mas podem também ser induzidas pelo aumento da atividade neuronal.
• A neuroinflamação mantém a homeostase, para permitir que o SNC possa lidar com maiores demandas metabólicas e aumenta o poder computacional e plasticidade das redes neurais.
• Esclerose Múltipla é uma doença dual, neuroinflamatória e neurodegenerativa, com diferentes gatilhos agindo em indivíduos geneticamente susceptíveis.
NEUROINFLAMAÇÃO: QUAIS AS
IMPLICAÇÕES TERAPÊUTICAS?
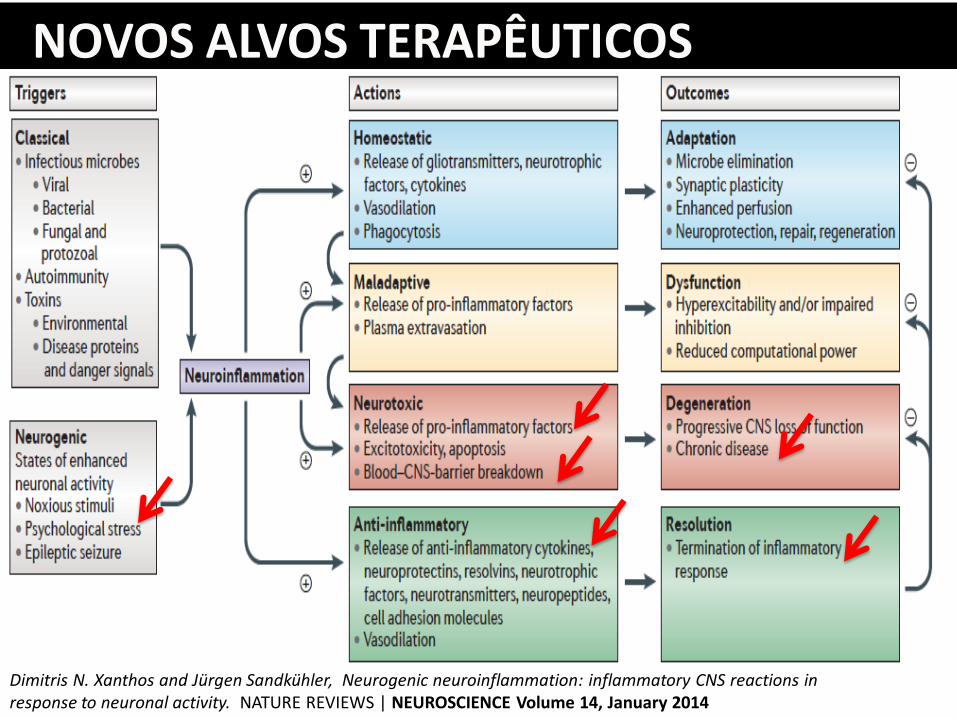
Dimitris N. Xanthos and Jurgen Sandkuhler, Neurogenic neuroinflammation: inflammatory CNS reactions in response to neuronal activity. NATURE REVIEWS | NEUROSCIENCE Volume 14, January 2014
NOVOS ALVOS TERAPÊUTICOS

NEUROINFLAMAÇÃO NEUROGÊNICA
Dimitris N. Xanthos and Jurgen Sandkuhler, Neurogenic neuroinflammation: inflammatory CNS reactions in response to neuronal activity. NATURE REVIEWS | NEUROSCIENCE Volume 14, January 2014

MUDANÇA DA INCIDÊNCIA DE
DOENÇAS AUTOIMUNES EM 50 ANOS

In humans, more than 100 trillion
microorganisms, mostly bacteria, colonize the oral–gastrointestinal tract, and most of these microorganisms reside in the distal intestine.
The microbiota enhances innate immunity to
pathogens. The microbiota promotes adaptive immunity
Segmented filamentous bacteria (SFB) and
other commensal microorganisms activate lamina propria dendritic cells (DCs) and macrophages to induce T helper 17 (TH17) cells and TH1 cells through the production of interleukin-1β ?(IL-1β)?, IL-6 and IL-23 in the case of TH17 cells, and possibly IL-12 in the case of TH1 cells
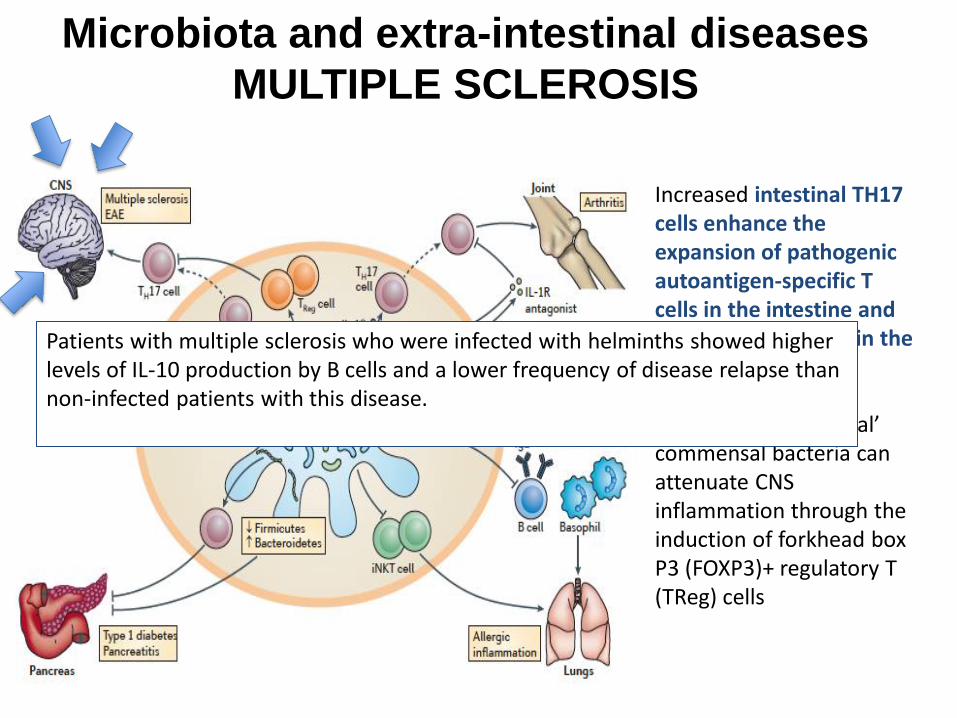
Microbiota and extra-intestinal diseases
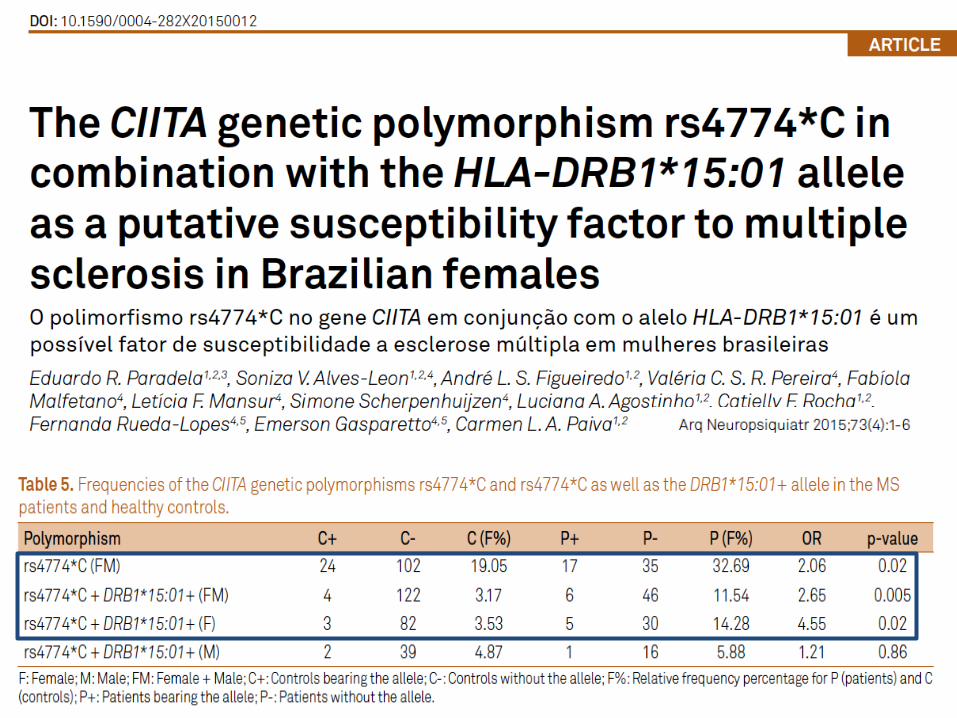
MULTIPLE SCLEROSIS
Increased intestinal TH17 cells enhance the expansion of pathogenic autoantigen-specific T cells in the intestine and cause inflammation in the CNS. By contrast, ‘beneficial’ commensal bacteria can attenuate CNS inflammation through the induction of forkhead box P3 (FOXP3)+ regulatory T (TReg) cells
Patients with multiple sclerosis who were infected with helminths showed higher levels of IL-10 production by B cells and a lower frequency of disease relapse than non-infected patients with this disease.

B
T
APC
IL-4
IL-6
B
MF TH1
TH 2
-
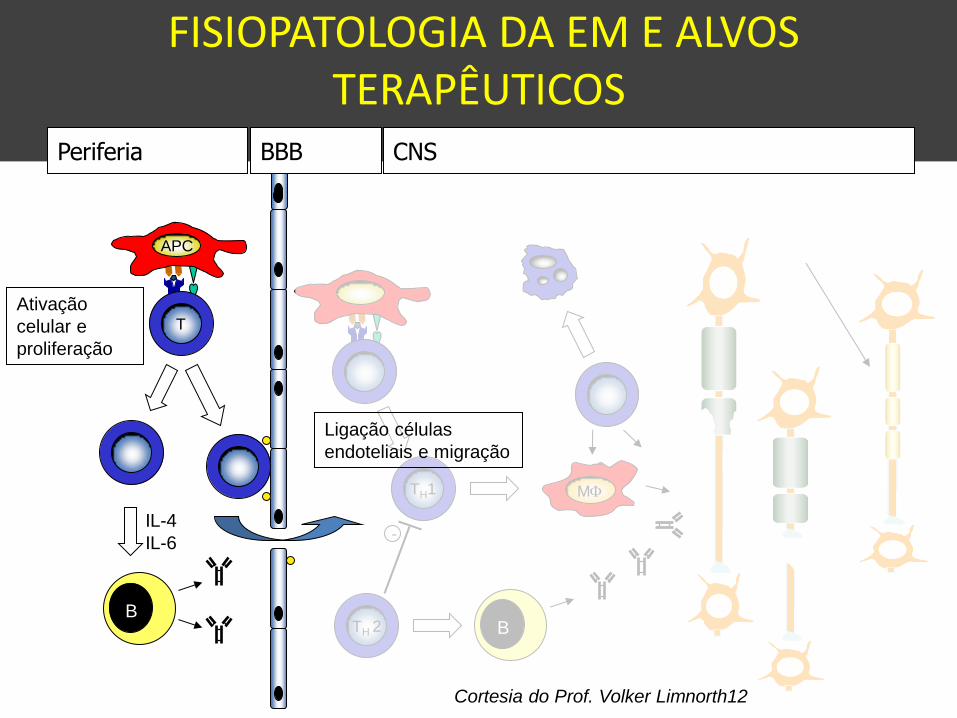
Periferia BBB CNS
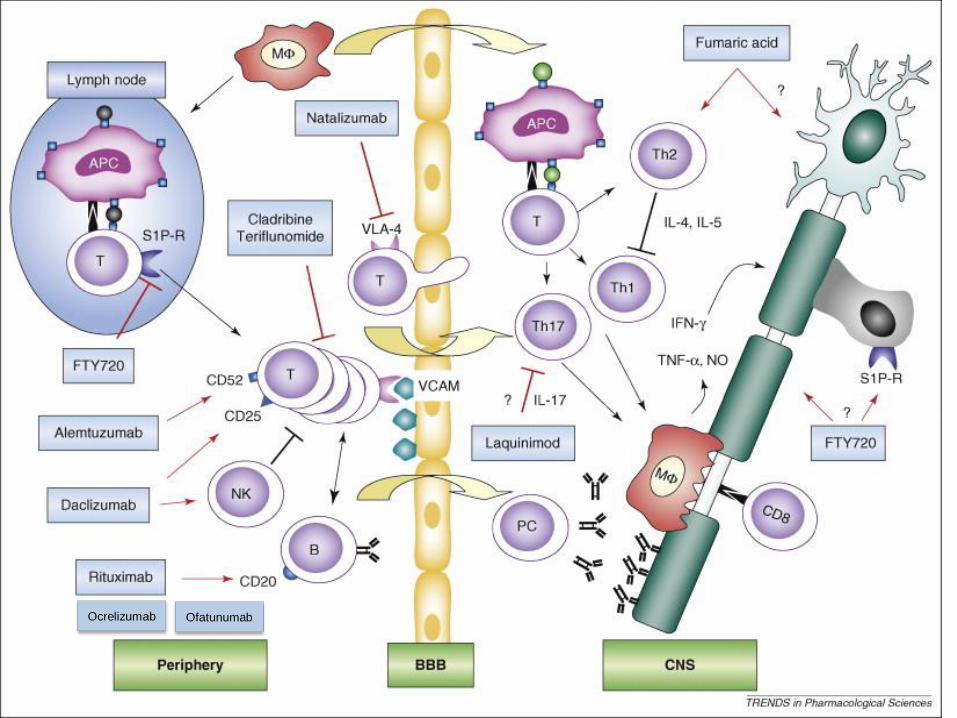
FISIOPATOLOGIA DA EM E ALVOS TERAPÊUTICOS
Ativação
celular e
proliferação
Ligação células
endoteliais e migração
Cortesia do Prof. Volker Limnorth12
13
B
T
APC
IL-4
IL-6
B
MF
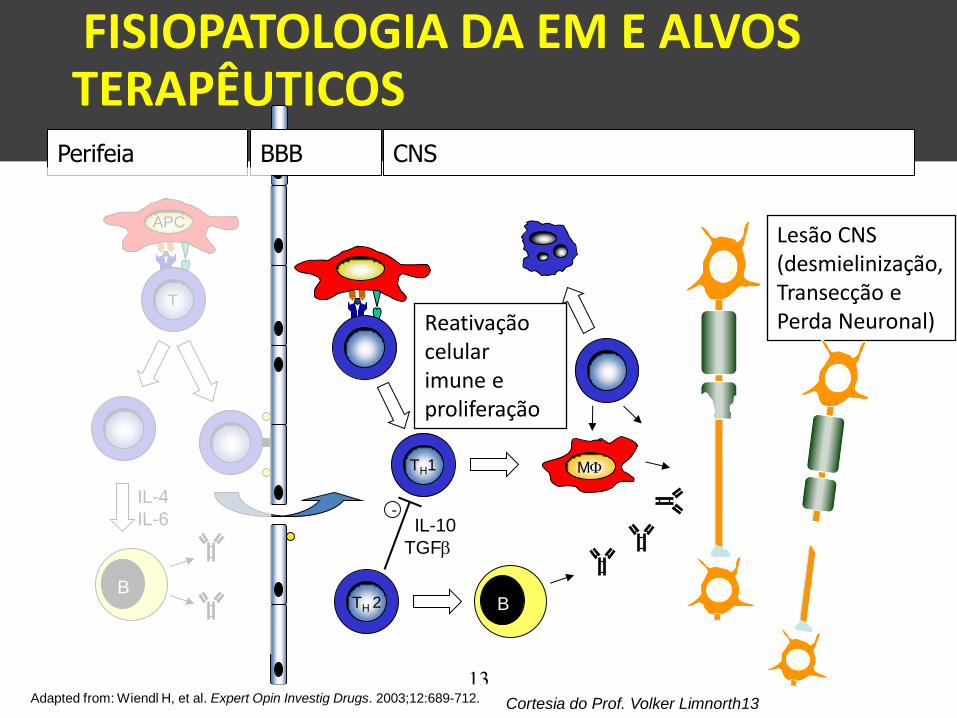
Reativação celular imune e proliferação
TH1
TH 2
IL-10
TGFb
-
Perifeia BBB CNS
Adapted from: Wiendl H, et al. Expert Opin Investig Drugs. 2003;12:689-712.
Lesão CNS (desmielinização, Transecção e Perda Neuronal)
FISIOPATOLOGIA DA EM E ALVOS TERAPÊUTICOS
Cortesia do Prof. Volker Limnorth13
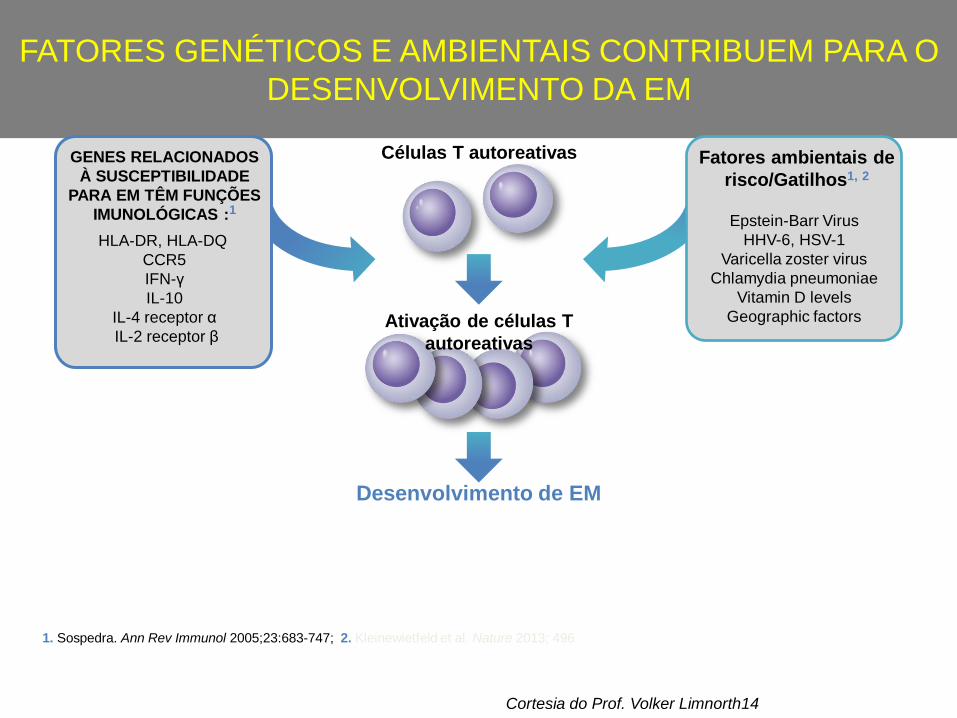
FATORES GENÉTICOS E AMBIENTAIS CONTRIBUEM PARA O
DESENVOLVIMENTO DA EM
1. Sospedra. Ann Rev Immunol 2005;23:683-747; 2. Kleinewietfeld et al. Nature 2013; 496
Células T autoreativas
Ativação de células T
autoreativas
Desenvolvimento de EM
Fatores ambientais de
risco/Gatilhos1, 2
GENES RELACIONADOS
À SUSCEPTIBILIDADE
PARA EM TÊM FUNÇÕES
IMUNOLÓGICAS :1
HLA-DR, HLA-DQ
CCR5
IFN-γ
IL-10
IL-4 receptor α
IL-2 receptor β
Epstein-Barr Virus
HHV-6, HSV-1
Varicella zoster virus
Chlamydia pneumoniae
Vitamin D levels
Geographic factors
Cortesia do Prof. Volker Limnorth14

000

1950 2000 2010 2020
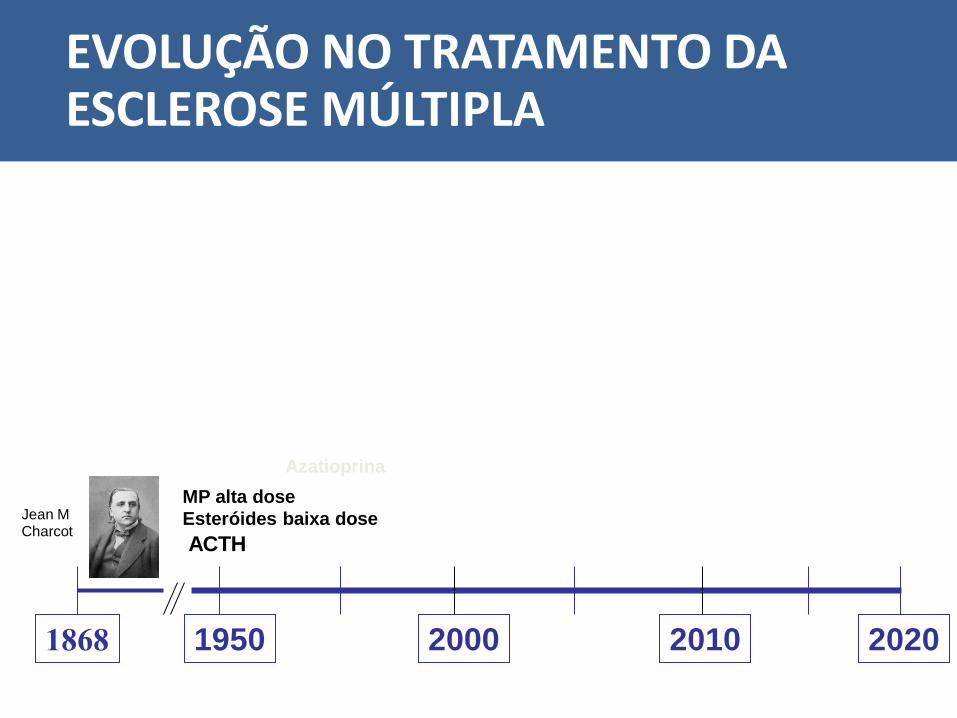
ACTH
1868
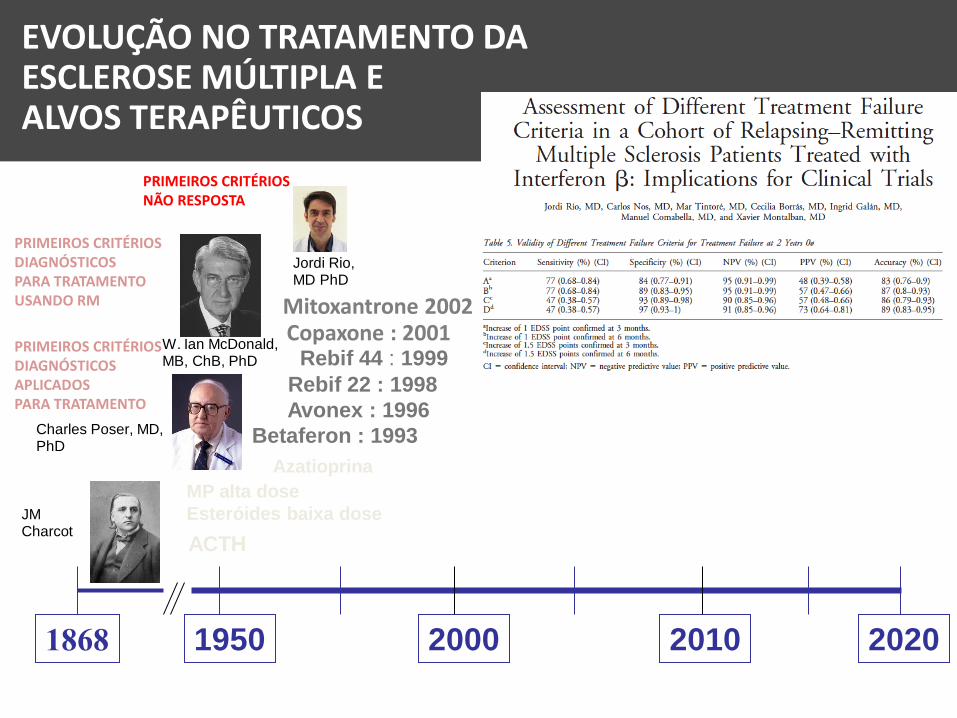
EVOLUÇÃO NO TRATAMENTO DA ESCLEROSE MÚLTIPLA
Jean M Charcot
Azatioprina
MP alta dose
Esteróides baixa dose
1950 2000 2010 2020
ACTH
Azatioprina
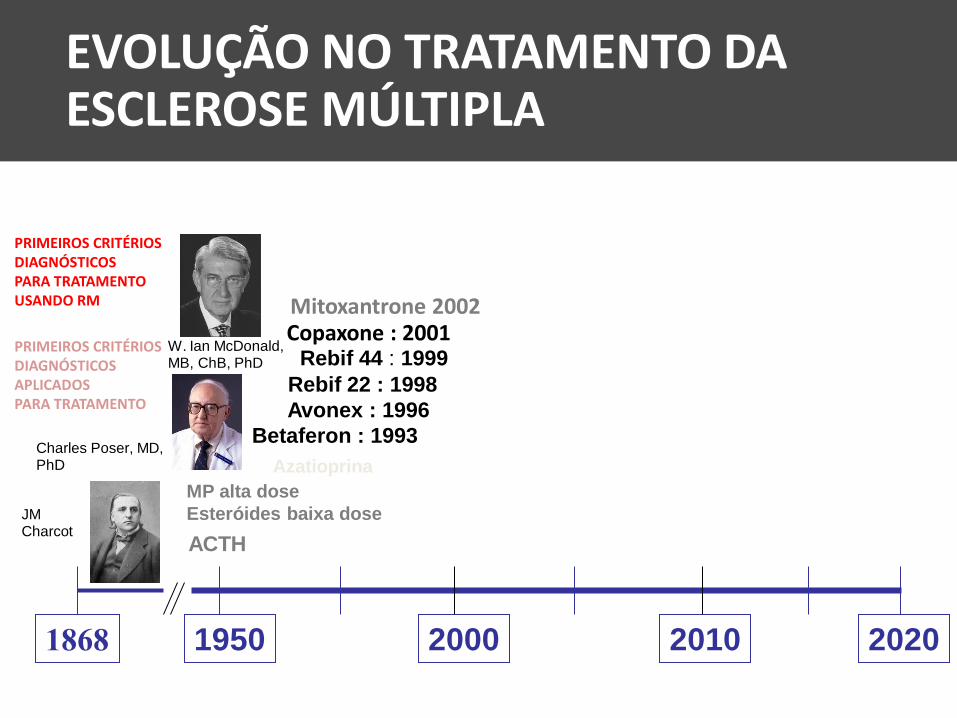
Avonex : 1996
Betaferon : 1993
Rebif 22 : 1998
Rebif 44 : 1999
1868
MP alta dose
Esteróides baixa dose
Mitoxantrone 2002 Copaxone : 2001
W. Ian McDonald, MB, ChB, PhD
EVOLUÇÃO NO TRATAMENTO DA ESCLEROSE MÚLTIPLA
Charles Poser, MD, PhD
JM Charcot
PRIMEIROS CRITÉRIOS DIAGNÓSTICOS PARA TRATAMENTO USANDO RM
PRIMEIROS CRITÉRIOS DIAGNÓSTICOS APLICADOS PARA TRATAMENTO

21
B
T
APC
IL-4
IL-6
B
MF TH1
TH 2
-
Periferia BBB CNS
IFNβ pode diminuir a migração de
leucócitos na BBB
1Muraro PA, et al. J Neuroimmunol. 2000;111:186-194; 2Avolio C, et al. J Neurol Sci. 2001;186:65-73; 3Defazio G, et al. J Interferon Cytokine Res. 2001;21:267-272; 4Defazio G, et al.
J Neuroimmunol.1998; 88:13-20; 5Floris S, et al. J Neuroimmunol. 2002;127:69-79; 6Muraro PA, et al. J Neuroimmunol. 2004;150:123-131; 7Soilu-Hanninen M, et al. J Neuroimmunol.
2005;167:175-182; 8Gelati M, et al. J Neurol.1999;246:569-573; 9Avolio C, et al. Mult Scler. 2005;11:441-446; 10Waubant E, et al. J Interferon Cytokine Res. 2001 ;21:181-185; 11Boz
C, et al. Clin Neurol Neurosurg. 2006;108:124-128; figure adapted from: Wiendl H, et al. Expert Opin Investig Drugs. 2003;12:689-712.
• IFNβ diminui a expressão de moléculas de adesão na
superfície celular 1-8
• IFNβ inibe atividade de MMP 9-11
• Glatiramer in vitro atua provavelmente substituindo
MBP no complexo trimolecuar
IFNβ-1a
Cortesia do Prof. Volker Limnorth21

22
B
T
APC
IL-4
IL-6
B
MF TH1
TH 2
IL-10
TGF-b
-
Periferia BBB CNS
IFNb e GA podem reataurar o balanço do sistema imune em pacientes com EM
Adapted from Wiendl H, et al. Expert Opin Investig Drugs. 2003;12:689-712
• IFNb-1e GA aumentam ação de IL-10 1-4 e
suprimem IL-121,5,6 e atividade de IL-231
1Krakauer M, et al. Mult Scler. 2008;14:622-630; 2Kozovska ME, et al. Neurology. 1999;53:1692-1697; 3Liu Z, et al. J Neuroimmunol. 2001;112:153-162; 4Rudick RA, et al. Neurology. 1998;50:1294-1300; 5Huang Y-M, et al. Clin Exp Immunol. 2001;124:306-314; 6Byrnes AA, et al. Ann Neurol. 2002;51:165-174; figure adapted from: Wiendl H, et al. Expert Opin Investig Drugs. 2003;12:689-712.
Lesão CNS (desmielinização, Transecção e Perda Neuronal)
Cortesia do Prof. Volker Limnorth22

• Glatiramer parece ter como alvo o
complexo trimolecular atuando no SNC
e na periferia 7-11
Miller A, et al. J Neuroimmunol. 1998;92:113-121.7
Duda PW, et al. J Immunol. 2000;165:7300-7307.8
Aharoni R, et al. Proc Natl Acad Sci. 1997;94:10821-10826.9 Bradl M, et al. J Neurol Neurosurg Psychiatry. 2003;74:1364-1370.10 Raivich G, et al. J Neurosci. 1998:18:5804-5816.11
IFNb e GA podem reataurar o balanço do sistema imune em pacientes com EM
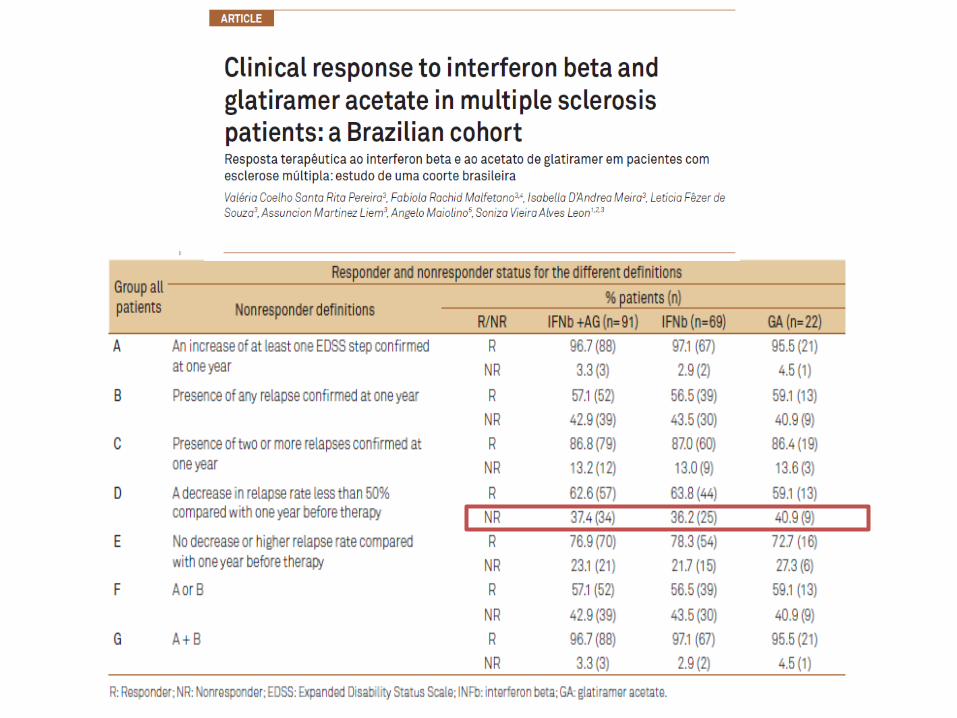
MAS NEM TODOS OS PACIENTES RESPONDIAM AOS INTERFERONS E AO
GLATIRAMER…
1950 2000 2010 2020
ACTH
Avonex : 1996
Betaferon : 1993
Rebif 22 : 1998
Rebif 44 : 1999
1868
Mitoxantrone 2002 Copaxone : 2001
W. Ian McDonald, MB, ChB, PhD
EVOLUÇÃO NO TRATAMENTO DA ESCLEROSE MÚLTIPLA E ALVOS TERAPÊUTICOS
Charles Poser, MD, PhD
JM Charcot
Jordi Rio, MD PhD
Azatioprina
MP alta dose
Esteróides baixa dose
PRIMEIROS CRITÉRIOS DIAGNÓSTICOS PARA TRATAMENTO USANDO RM
PRIMEIROS CRITÉRIOS DIAGNÓSTICOS APLICADOS PARA TRATAMENTO
PRIMEIROS CRITÉRIOS NÃO RESPOSTA

1950 2000 2010 2020
ACTH
Avonex : 1996
Betaferon : 1993
Rebif 22 : 1998
Rebif 44 : 1999
1868
Mitoxantron 2002 Copaxone : 2001
Natalizumabe 2006 Cladribin 2011
Fumarate 2013
Fingolimod 2011
Teriflunomide 2013
Alemtuzumabe 2013
W. Ian McDonald, MB, ChB, PhD
Chris Polman, MD PhD
EVOLUÇÃO NO TRATAMENTO DA ESCLEROSE MÚLTIPLA E ALVOS TERAPÊUTICOS
Charles Poser, MD, PhD
JM Charcot
Azatioprina
MP alta dose
Esteróides baixa dose
PRIMEIROS CRITÉRIOS DIAGNÓSTICOS PARA TRATAMENTO USANDO RM
PRIMEIROS CRITÉRIOS DIAGNÓSTICOS APLICADOS PARA TRATAMENTO
PRIMEIROS CRITÉRIOS PARA DIAGNÓSTICO PRECOCE COM DIS E DIT RM
E O CONCEITO DE TRATAMENTO ALTAMENTE EFICAZ -
NEDA

NATALIZUMABE
• Natalizumab is a humanized recombinant monoclonal antibody against α4-integrin.
• It diminishes leukocyte migration from the peripheral blood into the CNS by preventing its binding via α4-integrin to the ligand vascular cell adhesion molecule (VCAM) found on endothelial surfaces.
• This blocks the adhesion and subsequent migration of lymphocytes lymphocytes across the blood–brain barrier (BBB), attenuating CNS inflammation

30
B
T
APC
IL-4
IL-6
B
MF TH1
TH 2
IL-10
TGFb
-
Periferia BBB CNS
NATALIZUMABE
Lesão CNS (desmielinização, Transecção e Perda Neuronal)
Cortesia do Prof. Volker Limnorth30

Oral, uma vez ao dia (0,5 mg)1
Primeiro em uma nova classe de compostos
terapêuticos1
Liga-se as S1P-Rs expressos nos linfócitos e células
neurais do SNC1-8
Retenção seletiva e reversível de linfócitos circulantes
dos linfonodos1,3,9
linfócitos T de memória centrais e virgens retidas
linfócitos T de memória efetora de vigilância imune
poupadas
Age no interior do SNC2,10-13
atravessa a BHE para o SNC10
reduz astrogliose e ativação de astrócitos lesionais
(receptores S1P estão presentes nos astrócitos)11,12
Alvo / princípio: sistema imune e outros (SNC)
APC
Linfonodo
S1P-R
T
Gliose S1P-R
Fingolimode
Fingolimode
SNC / Sistema Imune e Neural
Sistema Periférico / Imune
OGD
1. Chun J, Hartung HP. Mechanism of action of oral fingolimod (FTY720) in multiple sclerosis. Clin Neuropharmacol. 2010 Mar-Apr;33(2):91-101. 2. Brinkmann V. FTY720 (fingolimod) in Multiple Sclerosis: therapeutic effects in the immune and the central nervous system. Br J Pharmacol. 2009 Nov;158(5):1173-82. 3. Matloubian M, Lo CG, Cinamon G et al. Lymphocyte egress from thymus and peripheral lymphoid organs is dependent on S1P receptor 1. Nature. 2004 Jan 22;427(6972):355-60. 4. Kimura A, Ohmori T, Ohkawa R et al. Essential roles of sphingosine 1-phosphate/S1P1 receptor axis in the migration of neural stem cells toward a site of spinal cord injury. Stem Cells. 2007 Jan;25(1):115-24. 5. Mandala S, Hajdu R, Bergstrom J et al. Alteration of lymphocyte trafficking by sphingosine-1-phosphate receptor agonists. Science. 2002 Apr 12;296(5566):346-9. 6. Brinkmann V. Sphingosine 1-phosphate receptors in health and disease: mechanistic insights from gene deletion studies and reverse pharmacology. Pharmacol Ther. 2007 Jul;115(1):84-105. 7. Baumruker T, Billich A, Brinkmann V et al. FTY720, an immunomodulatory sphingolipid mimetic: translation of a novel mechanism into clinical benefit in multiple sclerosis. Expert Opin Investig Drugs. 2007 Mar;16(3):283-9. 8. Massberg S, von Andrian UH. Fingolimod and sphingosine-1-phosphate--modifiers of lymphocyte migration. N Engl J Med. 2006 Sep 14;355(11):1088-91. 9. Mehling M1, Brinkmann V, Antel J et al. FTY720 therapy exerts differential effects on T cell subsets in multiple sclerosis. Neurology. 2008 Oct 14;71(16):1261-7. 10. Tamagnan GD et al. Pôster P839 apresentado em ECTRIMS 2012. 11. Choi JW, Gardell SE, Herr DR et al. FTY720 (fingolimod) efficacy in an animal model of multiple sclerosis requires astrocyte sphingosine 1-phosphate receptor 1 (S1P1) modulation. Proc Natl Acad Sci U S A. 2011 Jan 11;108(2):751-6. 12. Mehling M, Lindberg R, Raulf F et al. Th17 central memory T cells are reduced by FTY720 in patients with multiple sclerosis. Neurology. 2010 Aug 3;75(5):403-10. 13. Anthony DC, Sibson NR et al. Investigation of immune and CNS-mediated effects of fingolimod in the focal delayed-type hypersensitivity multiple sclerosis model. Neuropharmacology. 2014 Apr;79:534-41. Imagens de mecanismo adaptadas de: Linker RA, Kieseier BC, Gold R. Identification and development of new therapeutics for multiple sclerosis. Trends Pharmacol Sci. 2008 Nov;29(11):558-65.
FINGOLIMODE

Evidâncias sugerem alteração na biologia do S1P no SNC de pacientes com EM1
• Concentração de S1P está significantemente maior no LCR de pacientes com EM (n = 40)2
• Correlação positiva entre concentração de S1P e escore de EDSS 2
**p<0.01 vs control; CSF, cerebrospinal fluid; EDSS, Expanded Disability Status Scale; NAWM, normal appearing white matter 1. Wheeler et al. Brain 2008; 2. Kulakowska A et al. Neurosci Lett 2010; 3. Van Doorn R et al. Glia 2010; 4. Van Doorn R et al. Poster P662 presented at ECTRIMS 2010
15
10
5
0 Control MS
**
(S1
P)
nM
12
8
4
0
EDSS
(S1
P)
nM
2
6
10
5 4 3 2 1 0
R = 0.5867 p<0.001
• Receptores S1P (S1P1 e S1P3) estão up-regulados nos astrocitos das lesões de EM 3,4
Control brain tissue Active MS lesion NAWM
Immunohistochemical staining for S1P1
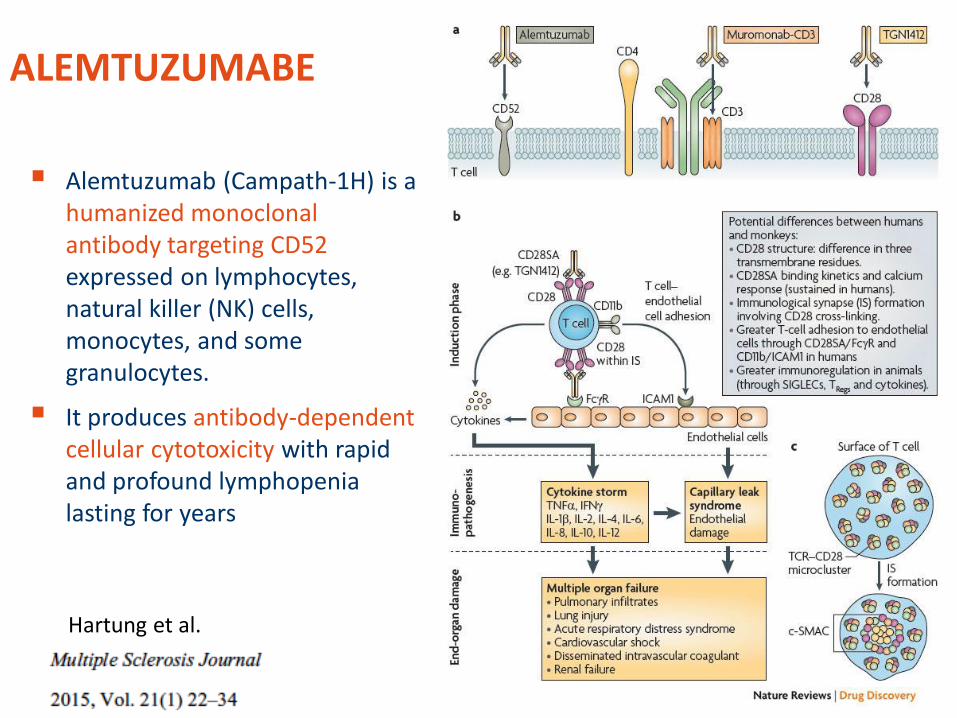
ALEMTUZUMABE
Alemtuzumab (Campath-1H) is a humanized monoclonal antibody targeting CD52 expressed on lymphocytes, natural killer (NK) cells, monocytes, and some granulocytes.
It produces antibody-dependent cellular cytotoxicity with rapid and profound lymphopenia lasting for years
Hartung et al.

ALEMTUZUMABE
Minagar et al. Expert Opin Biol Ther 2010;10:421-9.
Lymphocyte
CD52
Alemtuzumab Dead lymphocyte
Complement binding and
activation
Membrane attack complex
Fc Receptor
Immune cells (eg, NK cells or neutrophils)
Dead lymphocyte
Antibody-dependent Cellular Cytolysis (ADCC)
Complement-dependent Cytolysis (CDC)
Fc region
• Reconstituição subsequente do sistema imune com preservação relativa de células Treg e células B naive
• Linfócitos B – 6 meses • Linfócitos T – 12 meses
1. Fox. Expert Rev Neurother 2010;10:1789-97;
2. Coles et al. J Neurol 2006;253:98-108;
3. Rudick et al. Ann Neurol 2004;56:548–55;
4. Jones et al. Brain 2010:133;2232-47; 5. Cox et al. Eur J Immunol. 2005;35:3332-42.
Alemtuzumabe depleta rapidamente células B e T por meio de 2 principais mecanismos:
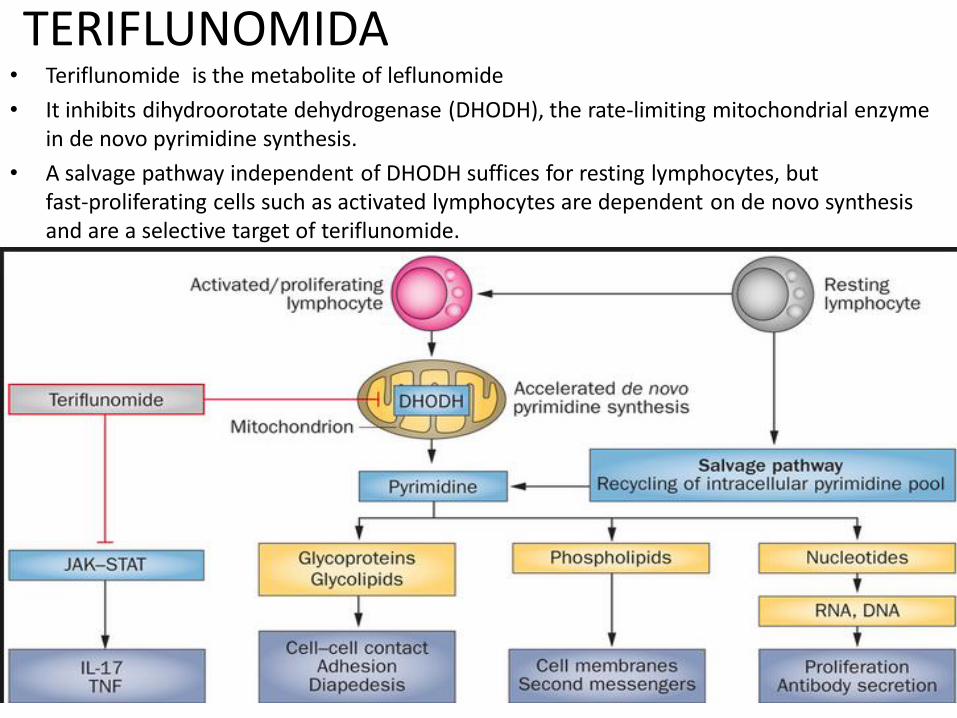
TERIFLUNOMIDA • Teriflunomide is the metabolite of leflunomide
• It inhibits dihydroorotate dehydrogenase (DHODH), the rate-limiting mitochondrial enzyme in de novo pyrimidine synthesis.
• A salvage pathway independent of DHODH suffices for resting lymphocytes, but fast-proliferating cells such as activated lymphocytes are dependent on de novo synthesis and are a selective target of teriflunomide.
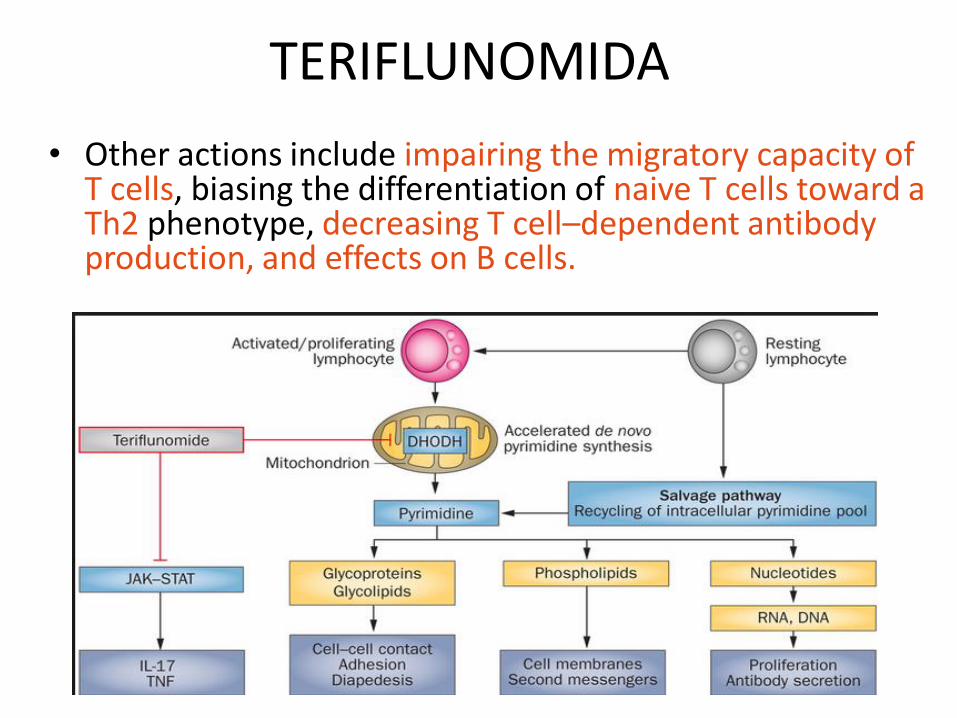
TERIFLUNOMIDA
• Other actions include impairing the migratory capacity of T cells, biasing the differentiation of naive T cells toward a Th2 phenotype, decreasing T cell–dependent antibody production, and effects on B cells.

DIMETILFUMARATO (BG12)
• BG12 (dimethyl fumarate) is an ester of dimethyl fumaric acid, already licensed as a second-line agent in severe psoriasis.
• The exact mode of action of BG12 is not completely understood:
• It may polarize the immune system toward a Th2 phenotype, increase the production of the anti-inflammatory cytokines interleukin (IL)-10 and IL-1 receptor antagonist (IL-1RA), attenuate lipopolysaccharide-induced production of tumor necrosis factor-alpha (TNFα), IL-1β, IL-6, and nitric oxide (NO).
• BG12 may have neuroprotective effects via activation of the NF-E2-related factor 2 (Nrf-2) antioxidant pathway

ARE
Nukleus
Zytoplasma
DMF or MMF
Nrf2
Nrf2
Oxidative
Stress
Nrf2
Nrf2
Nrf2
Nrf2
Nrf2
Nuclear factor (erythroid-derived 2)-like 2 =NFE2L2 or Nrf2, van Horssen J et al. Biochim Biophys Acta. 2011; 1812:141-150 | Linker RA et al. Brain. 2011; 134:678-692
DIMETILFUMARATO (BG12)
DIMETILFUMARATO e seu metabólito ativo (monometil fumarato) agem ativando o Nrf2 (simulando o excesso de Ros). Nrf2 age no DNA ativando genes que levam a produção de Enzimas AntioxidanteS
1950 2000 2010 2020
ACTH
Azathioprin
Avonex : 1996
Betaseron : 1993
Rebif 22 : 1998
Rebif 44 : 1999
1868
steroids, low dose MP - high dose
Mitoxantron 2002 Copaxone : 2001
Natalizumab 2006 Cladribin 2011
Fumarate 2013
Fingolimod 2011
Teriflunomide 2013
Laquinimod 2014
Alemtuzumab 2013
Siponimod / ONO 2015
Daclizumab 2015
Ocrelizumab 2016
PegInterferon 2014
W. Ian McDonald, MB, ChB, PhD
Chris Polman, MD PhD
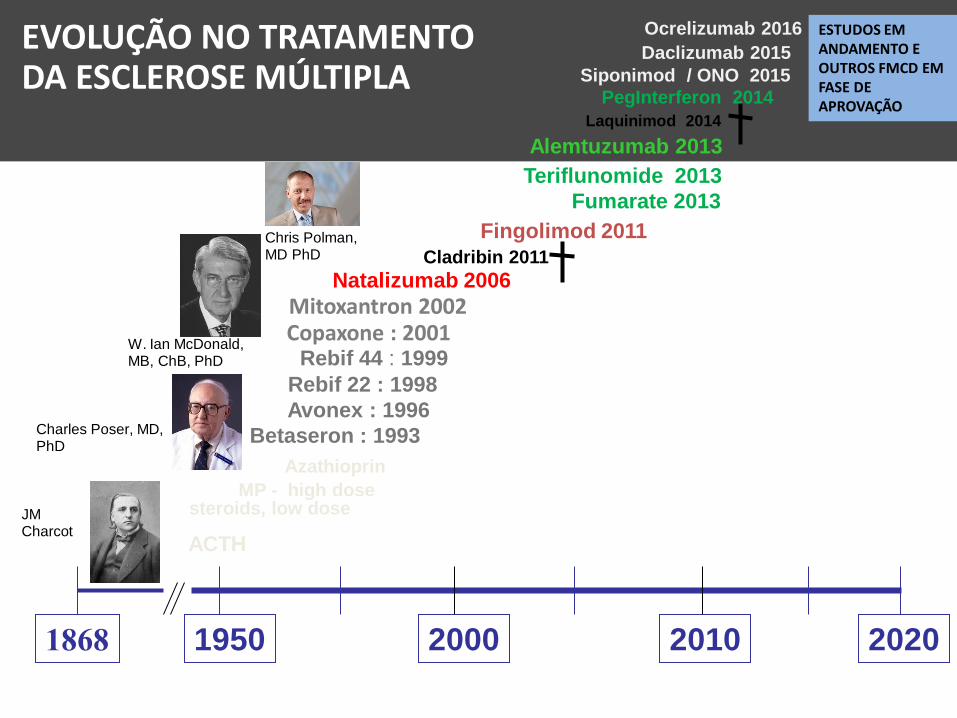
EVOLUÇÃO NO TRATAMENTO DA ESCLEROSE MÚLTIPLA
Charles Poser, MD, PhD
JM Charcot
ESTUDOS EM ANDAMENTO E OUTROS FMCD EM FASE DE APROVAÇÃO

OCRELIZUMABE
• Ocrelizumab is a recombinant humanized antibody that binds to CD20 at a different epitope but partly overlapping with rituximab.
• Ocrelizumab has a half-life of 23-28 days and induces a rapid B cell depletion after infusion, with a recovery of B cell numbers at 3 months

DACLIZUMABE • Daclizumab is a humanized mouse monoclonal antibody. It
antagonizes CD25 which is otherwise up-regulated on activated T cells and allows them to receive the IL-2 signal.
• Daclizumab has a high specificity for IL-2R, with a capacity of saturating IL-2R for 43 days after a single dose of 2 mg/kg.

Hypothesized Immunomodulatory
Effect of Daclizumab Treatment
47
• DAC treatment reduces activated T-cells and increases CD56bright NK cell proliferation via intermediate affinity IL-2 signaling1
1. Martin J, et al. J Immunol 2010;185:1311–1320.
Giovannoni G et al. Presented at ECTRIMS-ACTRIMS; October 19 – 22, 2011, Amsterdam, The Netherlands. Oral presentation 149.

MAIS ALVOS TERAPÊUTICOS…

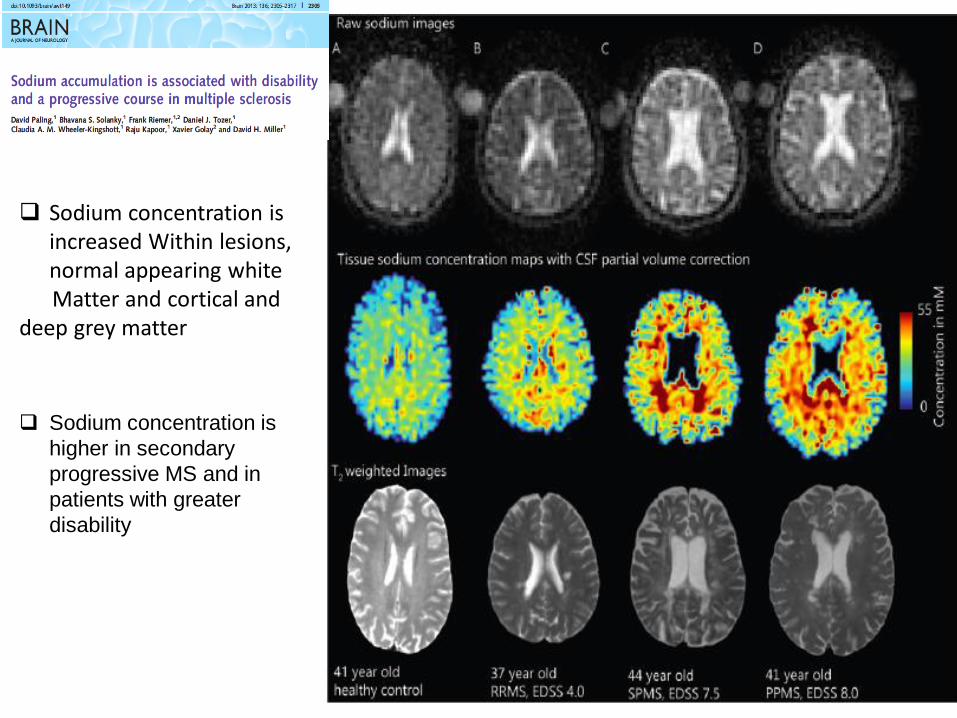
Sodium concentration is increased Within lesions, normal appearing white
Matter and cortical and deep grey matter
Sodium concentration is
higher in secondary
progressive MS and in
patients with greater
disability

Ocrelizumab Ofatunumab

FARMACOTERAPIA
(aguda e imunomoduladora)
EDUCAÇÃO
Fatores de risco
TRATAMENTO
SINTOMÁTICO
Fisioterapia, suporte
ALVOS TERAPÊUTICOS NA ESCLEROSE MÚLTIPLA

N=895 (270 males and 625
females), mean disease 17 years
Risk of reaching EDSS 4 and6
Regular smoking is associated with
more severe disease and faster
disability progression
Smoking cessation, whether before
or after onset of the disease is
associated with a slower
progression of disability
EDSS 4
EDSS 6


Adaptado de: Ingwersen J, Aktas O, Hartung HP. Advances in and Algorithms for the Treatment of Relapsing-Remitting Multiple Sclerosis. Neurotherapeutics. 2016 Jan;13(1):47-57.
CONCLUSÕES
• OS NOVOS ALVOS TERAPÊUTICOS MOSTRAM A NECESSIDADE DE UM MANEJO CADA VEZ MAIS INDIVIDUALIZADO DE DOENÇAS
• O RECONHECIMENTO DE NOVOS ASPECTOS FISIOPATOLÓGICOS É SEGUIDO DE NOVOS ALVOS TERAPÊUTICOS
• A ESCOLHA DOS FMCD DEVE CONSIDERAR A ATIVIDADE DA EM E ABOLIR O CONCEITO DE 1a, 2a., 3a. LINHA SOB PENA DE SE PERDER A MELHOR JANELA TERAPÊUTICA PARA IMPACTAR A MORBIDADE DA DOENÇA
RISCO BENEFÍCIO É INDIVIDUALIZADO!!!