programas de exercício físico em indivíduos com ... · ii lopes, s. (2016). programas de...
TRANSCRIPT
Universidade do Porto
Faculdade de Desporto
_______________________________________________________________
Programas de exercício físico em indivíduos com Espondilite
Anquilosante: Determinantes de Qualidade de vida.
_______________________________________________________________
Dissertação submetida às provas para
obtenção do grau de Doutor em Fisioterapia,
pela Faculdade de Deporto da Universidade
do Porto, segundo o Decreto-Lei 74/2006 de
24 março.
Orientador: Professora Doutora Cristina Teresa Torrão Carvalho Mesquita
Escola Superior de Saúde do Porto e Instituto Politécnico do Porto
Coorientador: Doutor José Alberto Ramos Duarte
Professor Catedrático da Faculdade de Desporto da Universidade do Porto.
Sofia Lopes
Porto, 2016
II
Lopes, S. (2016). Programas de exercício físico em indivíduos com Espondilite
Anquilosante: Determinantes de Qualidade de vida. Porto: Lopes, S.
Dissertação de Doutoramento em Fisioterapia apresentada à Faculdade de
Desporto da Universidade do Porto.
Palavras-chave: ESPONDILOARTRITES; FISIOTERAPIA; FUNCIONALIDADE;
BIOMARCADORES; EDUCAÇÃO PARA A SAÚDE

III
“A tarefa não é tanto ver aquilo que ninguém viu, mas pensar o que
ninguém ainda pensou sobre aquilo que todo mundo vê”.
Arthur Schopenhauer

V
Agradecimentos
No decorrer de todo este processo muitas pessoas cruzaram-se no meu
caminho, às quais eu gostaria aqui de deixar uma palavra de amizade e
gratidão, pois sem elas esta tese não seria possível.
Em primeiro lugar, gostaria de agradecer a todos os indivíduos com Espondilite
Anquilosante que participaram neste estudo, em especial ao Dr. Sardoeira
Pinto, enquanto Presidente do Núcleo Regional do Porto da Associação
Nacional de Espondilite Anquilosante, que nos abriu as portas da Associação e
abraçou de imediato este projeto.
Deixo aqui também a minha gratidão à minha orientadora, Prof. Doutora
Cristina Mesquita, pela orientação e apoio em todo este processo. E também
agradeço ao Prof. Doutor José Alberto Duarte como coorientador, pelo apoio
prestado em todo este trabalho.
Retribuo também a todos os colegas e amigos, que sempre me
acompanharam, a amizade o estímulo e o apoio moral em todas etapas desta
tese.
E em último, mas não menos importante, agradeço e dedico à minha família,
este trabalho, por todo o suporte, força, encorajamento e energia prestada,
desde o primeiro momento até ao final, pois só com este apoio tudo o resto foi
exequível.

VII
Índice Geral
Agradecimentos ............................................................................................... V
Índice Geral ..................................................................................................... VII
Índice de Figuras ............................................................................................. XI
Índice de Tabelas .......................................................................................... XIII
Índice de Anexos ........................................................................................... XV
Resumo .........................................................................................................XVII
Abstract ......................................................................................................... XIX
Lista de Abreviaturas ................................................................................... XXI
Capítulo I. Introdução....................................................................................... 1
Capítulo II. Revisão da Literatura .................................................................. 13
Estudo I. Artigo de Revisão. Programas de exercício no domicílio e em grupo
em doentes com espondilite anquilosante: revisão sistemática .................... 15
Resumo ..................................................................................................... 17
Abstract ...................................................................................................... 19
Introdução .................................................................................................. 20
Metodologia ............................................................................................... 21
Resultados ................................................................................................. 24
Discussão .................................................................................................. 27
Conclusão .................................................................................................. 29
Bibliografia ................................................................................................. 30
VIII
Capítulo III. Estudos Originais ...................................................................... 33
Estudo II. Cross-cultural adaptation and validation of the Portuguese version
of “The assessment of knowledge in ankylosing spondylitis patients by a self-
administered questionnaire” .......................................................................... 35
Abstract ...................................................................................................... 38
Introduction ................................................................................................ 39
Methods ..................................................................................................... 40
Results ....................................................................................................... 43
Discussion ................................................................................................. 45
Bibliography ............................................................................................... 48
Estudo III. The relation between functional parameters and C-Reactive
Protein, Erythrocyte Sedimentation Race in Ankylosing Spondylitis: a cross
sectional study .............................................................................................. 51
Abstract ...................................................................................................... 54
Introduction ................................................................................................ 55
Methods ..................................................................................................... 56
Results ....................................................................................................... 59
Discussion ................................................................................................. 62
Conclusion ................................................................................................. 65
Bibliography ............................................................................................... 65
Estudo IV. Effects of group-based vs home-based exercise programs in
patients with ankylosing spondylitis ............................................................... 71
Abstract ...................................................................................................... 73
Introduction ................................................................................................ 75
Methods ..................................................................................................... 76
Results ....................................................................................................... 79
Discussion ................................................................................................. 82
IX
Conclusions ............................................................................................... 85
Bibliography ............................................................................................... 85
Capítulo IV. Discussão ................................................................................... 91
Capitulo V. Conclusões ............................................................................... 103
Capítulo VI. Perspetivas Futuras ................................................................ 107
Capítulo VII. Referências ............................................................................. 111
Anexos .........................................................................................................XXIII


XI
Índice de Figuras
Capítulo II
Estudo I
Figura 1. Flow-Chart alusivo à seleção de artigos a
incluir no estudo………………........................................
22
XIII
Índice de Tabelas
Capítulo II
Capítulo III
Estudo I
Tabela 1. Avaliação da Qualidade Metodológica pela
Escala PEDro………………………………………………
23
Tabela 2. Resumo das Variáveis extraídas dos
artigos……………………………………………………….
24
Estudo II
Tabela 1. . Sample characteristics: socio-demographic
information and history of AS……………………………..
43
Tabela 2. Proportion of correct answers, standardised
for the 1-factor latent trait model and reliability for the
questionnaire……………………………………………….
44
Tabela 3. Test–retest reliability of the questionnaire…. 44
Tabela 4. Questionnaire scores by gender, age,
education level, years since diagnosis and salary……..
45
Estudo III
Tabela 1. Sample characteristics: socio-demographic
information and history of AS……………………………..
59
Tabela 2. Clinical parameters of patients with
ankylosing spondylitis……………………………………..
60
Tabela 3. Spearman’s correlations between functional
and biomarker parameters………………………………..
61
Tabela 4. Association between biomarkers and
functional parameters……………………………………...
61

XIV
Estudo IV
Tabela 1. Sample characteristics: socio-demographic
information and history of AS……………………………..
80
Tabela 2. Intra and intergroup comparison of
functional and biomarker parameters, at baseline and
after 6 months of exercise…………………………….......
81

XV
Índice de Anexos
Anexo I. Aprovação pela Comissão de Ética…………………………………..XXV
Anexo II. Consentimento informado…………………………………………...XXVII

XVII
Resumo
A espondilite anquilosante (EA) é uma doença reumática crónica de
carácter sistémico caraterizada pela inflamação do osso subcondral, cápsulas,
ligamentos e tendões, e proliferação óssea, especialmente na coluna vertebral,
afetando ainda as articulações periaxiais assim como outros órgãos. As
terapias mais comuns na EA são a terapia farmacológica, e a não
farmacológica através da prática de programas de exercícios específicos. O
objetivo principal desta dissertação, foi o de avaliar os efeitos de um programa
de exercícios específicos, em parâmetros funcionais e bioquímicos em
indivíduos com EA. Esta tese é constituída por um artigo de revisão (estudo I) e
três estudos originais (estudos II, III e IV). A revisão sistemática, analisou a
evidência existente sobre a eficácia de programas no domicílio e em grupo,
relativamente ao aumento da funcionalidade em indivíduos com EA. O estudo
II, de natureza observacional descritiva, adaptou e validou um questionário de
conhecimento sobre EA, para a população portuguesa. Já o estudo III, de
caracter observacional analítico, caracterizou indivíduos com EA analisando a
associação de parâmetros funcionais com parâmetros bioquímicos nestes
doentes. O estudo IV, quase-experimental, avaliou o efeito de um programa de
exercícios em grupo e no domicílio na evolução de parâmetros funcionais e
bioquímicos. Os resultados da revisão sistemática permitiram concluir que
parece haver evidência de que os programas realizados em grupo são mais
eficazes do que os realizados no domicílio. Os resultados dos estudos originais
demonstram elevado nível de conhecimento destes indivíduos sobre a sua
doença, nas áreas que abordam a sintomatologia, testes imunológicos e
intervenção. Relativamente à caracterização destes indivíduos, verificou-se a
existência de uma associação entre a velocidade de sedimentação e o índice
de atividade e índice funcional de Bath para a EA. Para além disto, após seis
meses de intervenção, observou-se que o programa realizado em grupo
apresentou melhores resultados, no índice funcional e métrico de Bath, não se
tendo verificado alterações a nível dos parâmetros bioquímicos.
Palavras-chave: ESPONDILOARTRITES; FISIOTERAPIA; FUNCIONALIDADE;
BIOMARCADORES; EDUCAÇÃO PARA A SAÚDE

XIX
Abstract
Keywords Ankylosing spondylitis (AS) is a systemic disease
characterised by chronic inflammation of subchondral bone, capsules,
ligaments and tendons, and bone formation, especially at the spine, also
affecting periaxial joints and other organs. AS standard management consists of
a combination of pharmacological therapy and non-pharmacological treatment
with the adoption of specific exercise programmes. The main objective of this
study was to assess the effects of a specific exercise programme on functional
and biomarker parameters in AS patients. This thesis consists of a review paper
(study I) and three original studies (studies II, III and IV). The systematic review
was undertaken to analyse the existing evidence on the effectiveness of home-
based and group-based exercise programmes to improve functionality in
individuals with AS. Study II had an observational and descriptive nature and
consisted of the analysis and validation of a questionnaire for the Portuguese
population on the knowledge of AS patients regarding the disease. Study III was
an observational analytical study aimed at characterising individuals with AS
and at verifying the association between functional and biomarker parameters in
these patients. Study IV was a quasi-experimental study, and was carried out to
assess the effects of a group-based versus home-based exercise programme in
the evolution of functional and biomarker parameters. The results of the
systematic review have shown evidence that group-based exercise
programmes are more effective than home-based exercise programmes. The
results of the original studies have shown that these individuals have a high
degree of knowledge of the disease, particularly regarding symptoms,
immunological testing and intervention. As far as the characterisation of
individuals with AS is concerned, we found that there is an association between
the sedimentation rate and the Bath functional index for AS. Additionally, after
six months the group-based exercise programme has shown better results in
Bath functional and metric indices, with no changes in the biomarker
parameters.
Key-words: SPONDYLOARTHRITIS; PHYSICAL THERAPY; FUNCTIONALITY;
BIOMARKERS; HEALTH EDUCATION

XXI
Lista de Abreviaturas
ANEA Associação Nacional de Espondilite Anquilosante
ASAS Assessments in Ankylosing Spondylitis International Society
AINES Anti Inflamatórios Não Esteróides
BASDAI Bath Spondylitis Disease Activity Index
BASFI Bath Spondylitis Functional Index
BASMI Bath Spondylitis Metrics Index
EA Espondilite Anquilosante
ESTSP Escola Superior de Tecnologia da Saúde do Porto
EULAR European League against Rheumatism
HLA B27 Antígeno leucocitário humano
IgA Imunoglobulina A
NDI Neck Disability Index
ODI Oswestry Disability Index
PCR Proteína C Reactiva
RPG Reeducação Postural Global
TNF Factor de Necrose Tumoral
vs Versus
VS Velocidade de sedimentação

Capítulo I
Introdução
_____________________________________________________

Capítulo I. Introdução
3
As doenças reumáticas são definidas como alterações funcionais do
sistema músculo-esquelético, de causa não traumática, incluindo as doenças
inflamatórias, degenerativas, metabólicas, alterações dos tecidos moles
periarticulares e doenças de outros sistemas ou órgãos relacionadas com as
anteriores (Lucas, 2010).
Estima-se que em países desenvolvidos, as doenças reumáticas sejam
a principal causa de incapacidade e consumo de cuidados de saúde e recursos
sociais, tendo elevadas repercussões na qualidade de vida e funcionalidade
dos indivíduos (Ramiro, 2010).
Incluída nas doenças reumáticas, existem um grupo de patologias
designadas por espondiloartrites, onde se destacam vários subtipos, tais como
a espondiloartrite psoriátrica, a espondiloartrite reativa, a espondiloartrite
associada com doença intestinal inflamatória, a espondiloartrite indiferenciada
e a espondilite anquilosante (EA), sendo esta última caracterizada como o
principal subtipo deste grupo (Braun & Sieper, 2007).
Atualmente a EA é caracterizada como uma doença reumática
inflamatória e crónica, que afeta primariamente a coluna vertebral, incluindo as
articulações sacroilíacas e, posteriormente, as articulações periféricas (El Tecle
et al., 2015; Schett & Rudwaleit, 2010). Para além do acometimento do
esqueleto axial, podem surgir outras manifestações tais como as enteses,
muitas vezes localizadas nos calcanhares, as uveítes, assim como alterações
noutros órgãos, como por exemplo no coração as cardiomiopatias, as
insuficiências valvulares, defeitos de condução, entre outras, estando
presentes entre 2 a 10% dos indivíduos com EA (Braun & Sieper, 2007;
Momeni et al., 2011; Schett & Rudwaleit, 2010).
Estima-se que a prevalência de EA na população caucasiana seja de
0,5% e que, na Europa, varie entre 0,1% a 1,4%, com uma incidência entre 0,5
a 14 por 100.000 indivíduos por ano, segundo estudos realizados em diferentes
países (Braun & Sieper, 2007). A EA afeta essencialmente jovens adultos, com
cerca de 80% dos indivíduos apresentando os primeiros sintomas antes dos 30
anos, enquanto cerca de 5% dos acometidos pela doença os apresentando
mais tardiamente, por volta dos 45 anos (Braun & Sieper, 2007). Os homens
Capítulo I. Introdução
4
são mais frequentemente atingidos relativamente às mulheres, numa proporção
de 2:1, embora possa existir uma variação geográfica e étnica (Braun & Sieper,
2007; Raychaudhuri & Deodhar, 2014). Nos homens, a coluna vertebral e a
pélvis são mais comumente afetadas, apresentando também algum
acometimento da parede torácica, quadris, ombros e pés e, de uma forma
geral, estas manifestações são mais severas do que nas mulheres. Nestas,
verifica-se que o acometimento da coluna é menor e menos grave, no entanto,
apresentam mais manifestações na pélvis, quadris, joelhos, tornozelos e
punhos (Sieper et al., 2002).
Fazendo uma análise da perspetiva histórica da EA, encontra-se
referências a estudos paleopatológicos no Egipto, em múmias, que sugerem
que esta doença tenha afetado a humanidade desde esta época (Sieper et al.,
2002). Pensa-se que a primeira descrição desta doença tenha surgido em
1559, por Realdo Colombo, através de uma exposição anatómica de
esqueletos com anormalidades características desta doença (Sieper et al.,
2002). Vários estudos e descrições da EA foram realizados ao longo dos anos,
no entanto, com o avanço da ciência e cerca do ano de 1900, através de
relatórios epidemiológicos, radiográficos e clínicos, surgem dados mais
precisos sobre EA e sua relação com outras formas de artrite ou com outras
doenças (Sieper et al., 2002).
A etiologia e a patogénese da EA não são ainda totalmente
compreendidas e entendidas, tornando o seu diagnóstico de difícil execução
(Sieper et al., 2002). Relativamente à sua patogénese, apresentam-se algumas
teorias explicativas que se debruçam sobre mediadores imunológicos, tendo
por base o seu carácter inflamatório, nomeadamente elevados níveis séricos
de Imunoglobulina A (IgA) (Sieper et al., 2002). Outros autores, entretanto,
relatam que a patogénese pode derivar também da inflamação e da formação
do osso novo, especificamente na coluna vertebral. A forte associação entre a
prevalência do antigénio HLA B27 e a incidência e prevalência de EA, é outra
teoria explicativa, uma vez que 90 a 95% dos indivíduos com EA apresenta
este antigénio positivo (Braun & Sieper, 2007). Estima-se que o risco de
desenvolver EA é elevado em indivíduos com HLA B27 positivo e mais elevado
Capítulo I. Introdução
5
ainda em familiares de primeiro grau de indivíduos com HLA B27 positivo,
comparativamente a indivíduos sem história familiar (Braun & Sieper, 2007). As
estruturas cartilaginosas também têm sido alvo de análise, segundo alguns
estudos em indivíduos com esta patologia, verificando-se que as células
mononucleares invadem as estruturas cartilaginosas das articulações
sacroilíacas e discos intervertebrais, levando à sua progressiva destruição e
anquilose (Bardos et al., 2005; Braem & Lories, 2012; Pham, 2008).
A sintomatologia mais frequente na EA inclui a dor articular, rigidez
matinal, astenia com fatigabilidade fácil, afetação da mobilidade vertebral e das
articulações periféricas (Kaya et al., 2007; Zochling et al., 2006). A dor é
normalmente de início insidioso, sentida geralmente na zona lombar e
nádegas, podendo aparecer também na zona cervical, acompanhada de rigidez
matinal, que melhora com a atividade e retoma com a inatividade (El Maghraoui
et al., 2003; Sieper et al., 2002). A astenia com fatigabilidade fácil, muitas
vezes subestimada, é um dos fatores que mais contribui para a morbilidade,
estando classificada como sendo um dos principais problemas, chegando a
atingir 65% destes indivíduos, com um forte impacto nas suas vidas, a nível da
funcionalidade e capacidade física, realização de atividades da vida diária,
relações pessoais e sociais, entre outras (Aissaoui et al., 2012; Zochling et al.,
2006). Atualmente é considerada como um sintoma central na EA, de difícil
avaliação, mas que deve ser tida em conta na abordagem terapêutica nestes
indivíduos (Aissaoui et al., 2012). A limitação da mobilidade vertebral é um dos
principais achados físicos na EA, afetando, nomeadamente, a extensão da
coluna e a expansibilidade torácica, no entanto, também se pode verificar
perda de mobilidade nas articulações periféricas (Sieper et al., 2002).
Relativamente à expansibilidade torácica, esta pode estar comprometida pelo
desenvolvimento da cifose dorsal, afetando as articulações costovertebrais,
esternoclaviculares e esternomanubrial, articulações que levam à diminuição
da expansão da parede torácica com limitação, ventilatória, promovendo assim
uma disfunção pulmonar restritiva (Momeni et al., 2011). Nas articulações
periféricas, a afetação verifica-se em aproximadamente 25% dos indivíduos,
mas com uma apresentação mais assimétrica e com maior acometimento nas
Capítulo I. Introdução
6
grandes articulações dos membros inferiores. Relativamente às enteses, estas
aparecem muitas vezes em locais de difícil acesso, tais como nos discos
intervertebrais, nas facetas articulares, nas inserções ligamentares e também a
nível do trocânter maior do fémur e na tuberosidade isquiática, tornando assim
difícil o seu diagnóstico. Recentemente, com a utilização de ultrassonografia,
têm-se verificado maior facilidade de diagnóstico de enteses nestes indivíduos
(Kaya et al., 2007; Zochling et al., 2006).
Segundo as diretrizes da sociedade internacional de EA (Assessments
in Ankylosing Spondylitis International Society/ European League against
Rheumatism) (ASAS/EULAR) (2010), para a realização de um diagnóstico em
EA, vários aspetos devem ser considerados. Entre eles, contam-se os sinais e
sintomas sugestivos da doença, a história do individuo, os testes clínicos,
laboratoriais e radiológicos, assim como as manifestações extra articulares e a
presença de co-morbilidades (Braun et al., 2011).
Para este diagnóstico, torna-se relevante a realização de exames
laboratoriais potencialmente relevantes, destacando-se entre eles o marcador
HLA B27, a proteína C-reativa (PCR) e a velocidade de sedimentação (VS)
(Braun & Sieper, 2007; Raychaudhuri & Deodhar, 2014; Sieper et al., 2002).
Embora estes marcadores sejam usualmente utilizados, nenhum deles, por si
só, faz o diagnóstico da doença, porque a associação da atividade da doença
com esses marcadores laboratoriais de inflamação é algo limitada. De facto,
têm-se verificado elevadas concentrações de PCR em apenas cerca de 50% a
70% dos doentes, assim como elevação da velocidade de sedimentação e
presença do gene HLA B27 apenas em 90% a 95% dos indivíduos com EA
(Braun & Sieper, 2007; de Vlam, 2010; de Vries et al., 2009; Sieper et al.,
2002). A PCR e a VS são os marcadores mais utilizados no controlo da
doença, em especial na sua fase aguda, pela reprodutibilidade, fiabilidade e
relação custo-eficácia que apresentam (Kisacik et al., 2008). A VS é o
parâmetro laboratorial mais amplamente utilizado para avaliação da atividade
da doença, e continua a ser uma ferramenta útil para monitorização das
doenças inflamatórias como é o caso da EA (Bochen, 2011). A PCR, por si só,
tendo em conta as mudanças rápidas dos seus níveis séricos, reflete uma
Capítulo I. Introdução
7
maior taxa de inflamação (Kisacik et al., 2008). Relativamente à inflamação, é
necessário ter em atenção que tem um carácter dinâmico na EA, ou seja, pode
piorar ou melhorar ao longo do tempo, podendo até desaparecer, pelo que a
avaliação e interpretação destes biomarcadores deve ser ponderada tendo em
conta a evolução clínica do indivíduo (de Vlam, 2010).
Decisivo também para o diagnóstico em EA, juntamente com os
exames laboratoriais, são os exames imagiológicos, pela sua sensibilidade
para detetar alterações estruturais articulares, sendo estas verificadas em mais
de 95% dos indivíduos com EA (Braun & Sieper, 2007). Para a deteção das
alterações estruturais articulares, a radiografia convencional ainda é
considerada como o exame mais fiável, e continua a ser utilizada no
diagnóstico de EA, através dos critérios de New York Modificados (Braun &
Sieper, 2007). Estes critérios são importantes pela sua sensibilidade e
especificidade, não sendo relevantes no diagnóstico precoce da doença, pois
no inicio da doença, as mudanças estruturais podem não ser visíveis na
radiografia convencional, podendo atrasar muitas das vezes o diagnóstico
(Braun & Sieper, 2007; El Tecle et al., 2015). Os critérios de New York
Modificados, compreendem os indicadores clínicos e os radiológicos (El Tecle
et al., 2015). Relativamente aos indicadores clínicos, estes definem-se pela i)
presença de dor lombar de carácter inflamatório, com mais de três meses de
evolução, que melhora com o exercício e não alivia com o repouso; ii) presença
de limitação da mobilidade da coluna lombar em ambos os planos, sagital e
frontal e; iii) presença de limitação da expansibilidade torácica em relação aos
valores normais para a idade e sexo. Os indicadores radiológicos, contemplam
a presença de sacroileíte com grau ≥ 2, bilateralmente, ou grau 3-4,
unilateralmente. O diagnóstico da EA é definido pela presença de um indicador
radiológico e de, pelo menos, um indicador clínico. Um provável diagnóstico da
EA, é definido pela presença de indicadores radiológicos sem indicadores
clínicos ou pela presença de três indicadores clínicos sem presença de
alterações radiológicos (El Tecle et al., 2015).
O diagnóstico de EA pode muitas vezes ser demorado e tardio, no
entanto, a identificação precoce da doença é crucial para estes indivíduos, no

Capítulo I. Introdução
8
sentido de iniciarem uma intervenção adequada. A intervenção e a
monitorização da doença são também determinantes para uma evolução
favorável, com repercussões na qualidade de vida dos sujeitos. A intervenção
na EA contempla a terapia farmacológica, a terapia não farmacológica e a
cirurgia, de acordo com as recomendações da ASAS/EULAR (Braun et al.,
2011).
De facto, no decorrer da doença, pode-se verificar a necessidade de se
efetuar cirurgia (Braun et al., 2011). A cirurgia pode ser benéfica para alguns
indivíduos com uma progressão avançada da doença, nomeadamente, em
indivíduos que apresentem hipercifose cervical, com perda da capacidade de
visão horizontal, instabilidade vertebral e incapacidade funcional (Lazennec et
al., 2015; Sieper et al., 2002). Outra situação onde a cirurgia pode estar
indicada é em casos de baixa densidade mineral óssea, com mudanças
estruturais ósseas, frequentes na articulação coxo femoral, assim como
também no caso de fraturas, muito comuns nestes indivíduos, especialmente
no segmento cervical (Braun & Sieper, 2007; Sieper et al., 2002).
Relativamente à terapia farmacológica, os anti-inflamatórios não
esteroides (AINEs) são recomendados como tratamento farmacológico de
primeira linha (Vastesaeger et al., 2011). A administração contínua de AINEs
em indivíduos com a doença ativa, segundo estudos clínicos, é suficiente para
controlar a dor e a rigidez articular, mas os seus efeitos nocivos, a nível
cardiovascular e gastrointestinal, podem limitar a sua utilização (Braun &
Sieper, 2007). No entanto, alguns destes indivíduos não conseguem controlar a
sintomatologia somente com os AINEs (Braun & Sieper, 2007). Quando estes
são ineficazes e a sintomatologia persiste, as recomendações atuais baseiam-
se na farmacologia biológica. Embora atualmente tenham surgido várias
discussões relativamente à administração deste tipo de fármacos, pela
variabilidade de resultados científicos em indivíduos em diferentes estadios da
doença (Braun et al., 2011). No entanto, são ainda necessárias orientações
sobre que indivíduos devem/podem utilizar esta terapia tendo em conta a
relação custo-efetividade (Braun & Sieper, 2007). Alguns autores sugerem que
se a administração deste tipo de fármacos demonstrar uma redução da

Capítulo I. Introdução
9
incapacidade de trabalho nestes indivíduos, a redução de custo indiretos, vai
compensar de alguma forma o aumento dos custos médicos diretos pela
administração destes fármacos, originando assim uma estimativa mais
favorável no custo-efetividade desta terapia (Reveille et al., 2012; Vastesaeger
et al., 2011).
Quanto à terapia não farmacológica, uma forma de intervenção é
através da fisioterapia, pela prática regular de exercício físico específico, que
pode ser realizado em grupo com supervisão, quer em meio seco, quer em
água (piscina), ou pode ser realizado sem supervisão, no domicílio (Braun et
al., 2011). Os principais objetivos da fisioterapia na EA englobam a redução da
dor, a melhoria da mobilidade e da força muscular, a diminuição da
deformidade da coluna vertebral, a promoção da funcionalidade e da qualidade
de vida destes indivíduos (Passalent, 2011). Como intervenção, a fisioterapia
possui uma panóplia de modalidades que visam alcançar os objetivos acima
referidos, como sendo, a terapia manual, mobilização de tecidos moles, a
hidroterapia e a eletroterapia (Passalent, 2011). A modalidade
preferencialmente descrita em estudos científicos e com maior eficácia tem
sido a prática de exercício físico relativamente à diminuição da dor, atividade
da doença, mobilidade da coluna vertebral, função cardiorrespiratória,
depressão, equilíbrio, fadiga e qualidade de vida (Passalent, 2011). Sabe-se
atualmente que a prática regular de exercício físico apresenta um efeito anti-
inflamatório, associado à redução dos níveis séricos de citocinas pró-
inflamatórias, indicando, assim, ter efeitos relevantes na redução de inflamação
crónica, pelo que o exercício físico regular deve ser tido em conta na EA
(Kisacik et al., 2016; Papini et al., 2014). Ainda relativamente à influência do
exercício físico regular na evolução da EA, este tem-se mostrado crucial pois, a
sua prática regular, promove um aumento, nos vários órgãos e tecidos, da
resistência ao stress oxidativo e, por conseguinte, pode diminuir os danos
oxidativos teciduais associados à evolução da doença (Gunendi et al., 2010).
No entanto, para a prescrição de exercício físico deve ser tida em conta a
frequência, a intensidade, a duração e estratégias de adesão, apesar de ainda
ser escassa a informação existente neste sentido (Dagfinrud et al., 2011;
Capítulo I. Introdução
10
Millner et al., 2015; Zarco et al., 2016). Relativamente à duração dos
programas, a maioria dos estudos publicados apenas fazem um seguimento
dos doentes até um período máximo de 16 semanas, pois em períodos mais
curtos é mais fácil manter a adesão dos doentes aos programas de exercício
físico regular (Millner et al., 2015) Relativamente ao tipo de programa, estes
podem incluir uma combinação de exercícios de fortalecimento muscular,
alongamentos de cadeias musculares, correção postural, reeducação
respiratória, coordenação, equilíbrio, propriocepção e exercícios de
relaxamento (Millner et al., 2015). Os programas de exercício em grupo são
supervisionados e orientados por um fisioterapeuta, permitindo assim a
correção sempre que necessário (Cagliyan, 2007). Em contrapartida, os
programas de exercício no domicílio são considerados mais económicos,
acessíveis, cómodos e eficientes em termos de tempo, pois não há
necessidade de deslocação (Ching-Yi WANG, 2009; Yigit et al., 2013). No
entanto, ainda existe controvérsia relativamente a estes dois tipos de
programas, não existindo consenso sobre qual o mais eficaz (Karapolat et al.,
2008). Outra forma de intervenção, relativamente às medidas não
farmacológicas, é a educação para a saúde, fundamentalmente baseada em
informação dirigida aos doentes, explicando como lidar com determinados
sinais e sintomas, nomeadamente, a dor, tensão muscular, o stress e a
depressão. Relativamente à educação dos doentes, esta é entendida como
qualquer tipo de atividade com vista a potenciar e melhorar o comportamento e
o papel ativo destes indivíduos em relação à sua doença, promovendo a
adesão aos tratamentos, a perceção do seu estado de saúde, um melhor
conhecimento sobre a doença, beneficiando de resultados a longo prazo de
uma forma mais económica e eficaz (Kaya et al., 2007; Marcelo Cardozo de
Souza, 2012). A educação para a saúde contempla também informação acerca
de métodos de relaxamento e técnicas de autogestão na EA (Braun et al.,
2011; Masiero et al., 2011). O nível de educação encontra-se diretamente
relacionado com o nível de conhecimento dos indivíduos, sendo que quanto
maior for o nível de educação, maior será o conhecimento, promovendo desta
forma uma maior responsabilização e controlo por parte dos indivíduos
Capítulo I. Introdução
11
relativamente à sua doença, o que em doenças crónicas, nomeadamente na
EA, é importante, para fazer frente à incapacidade funcional, à dor, à
desmotivação e baixa qualidade de vida destes indivíduos (Claudepierre et al.,
2004; E. Lubrano, 1998)
Todas as intervenções descritas, acarretam custos para estes
indivíduos, suas famílias e para o sistema de saúde onde estão envolvidos,
dependendo essencialmente da duração e da atividade da doença (Younes et
al., 2010). Se se associar a estes custos a (in)capacidade de continuar num
trabalho com remuneração e a (in)capacidade de desempenho de
determinadas tarefas, verifica-se uma séria ameaça à qualidade de vida destes
indivíduos (Bodur et al., 2011; Reveille et al., 2012).
Tendo em consideração as diferentes intervenções na EA, a escassez
de estudos científicos nesta área relativamente aos programas de exercício
físico regular, sua duração, tipologia e efeitos nos parâmetros funcionais e
bioquímicos, reforça a necessidade de se investigar mais esta temática. Neste
seguimento, o objetivo principal desta tese foi avaliar os efeitos de um
programa de exercícios específicos com um follow up de 6 meses em
indivíduos com EA. Enquadrados neste objetivo principal foram definidos
objetivos específicos tais como: (1) Analisar o efeito de programas de exercício
em indivíduos com EA, através da realização de uma revisão sistemática; (2)
Avaliar o conhecimento que estes indivíduos com EA possuem sobre a sua
doença, através da adaptação cultural e validação de um instrumento para
esse fim; (3) Caracterizar uma população de indivíduos com EA, pretendendo
verificar a associação entre parâmetros funcionais e bioquímicos sanguíneos;
(4) Analisar o efeito de um programa de exercícios, em grupo ou no domicilio,
com a duração de 6 meses, na evolução de parâmetros funcionais e
bioquímicos da doença.
Assim, esta tese está organizada e dividida em seis capítulos. O
primeiro capítulo é constituído pela introdução, que aborda a definição da
doença, sua prevalência e incidência, sintomatologia, diagnóstico e
intervenção. O segundo capítulo apresenta-se o enquadramento teórico,
resultado do primeiro estudo realizado (estudo I), onde são analisados e
Capítulo I. Introdução
12
revistos vários estudos sobre programas de exercício físico em EA realizados
em grupo vs domicílio. O terceiro capítulo, constituído por três estudos originais
(estudo II, III e IV), pretende responder às questões que foram levantadas no
decorrer da introdução, em que cada estudo tem o seu objetivo, metodologia,
resultados, discussão e conclusão. O quarto capítulo integra a discussão geral
dos resultados dos diferentes estudos originais efetuados. O quinto e penúltimo
capítulo, contempla as conclusões dos resultados obtidos e, por último, o sexto
capítulo compreende aspetos julgados pertinentes para futuros estudos a
serem realizados. No fim, encontram-se as referências bibliográficas que
sustentam os capítulos de introdução e discussão geral.
Capítulo II
Revisão da Literatura
_____________________________________________________

Estudo I. Artigo de Revisão
_______________________________________________________________
Programas de exercício no domicílio e em grupo em doentes com
espondilite anquilosante: revisão sistemática
Sofia Lopes1,2; Sara Costa2; Cristina Mesquita1; José Alberto Duarte3
1 Escola Superior de Tecnologia da Saúde do Porto, Instituto Politécnico do
Porto
2 Escola Superior de Saúde de Vale do Sousa, CESPU
3 Faculdade de Desporto, Universidade do Porto
Publicado na Acta Reumatológica Portuguesa, nº2, Abr/Jun 2016
_______________________________________________

Capítulo II. Revisão da Literatura
17
Resumo
Introdução: A Espondilite Anquilosante (EA) é uma patologia reumática
inflamatória crónica caraterizada pela inflamação das articulações da coluna
vertebral e das articulações sacroilíacas e em menor percentagem das
articulações periféricas. É uma patologia incapacitante, o que diminui a
qualidade de vida nos doentes com EA. A prática de exercício físico é
recomendada como tratamento não farmacológico, assim como no controlo e
prevenção das deformidades associadas.
Objetivo: recolher e sumariar a evidência científica disponível em bases de
dados científicas para perceber a eficácia de programas no domicílio e em
grupo em doentes com EA.
Métodos: Estudo de revisão sistemática, onde os artigos pesquizados para o
estudo foram recolhidos da base de dados científica PubMed. Encontraram-se
65 artigos com, data de publicação entre 1 de janeiro de 2004 e 31 de janeiro
de 2014. Foram estabelecidos critérios de inclusão e exclusão para proceder à
seleção dos artigos a incluir no estudo. Houve reunião de consenso com os
investigadores para uma seleção final dos artigos, sendo numa fase posterior,
os artigos lidos na íntegra pelos três investigadores.
Resultados: A revisão sistemática presente compreende 8 estudos clínicos
randomizados controlados. Todos os artigos evidenciaram benefícios
funcionais nos doentes com EA sujeitos a programas de exercícios em grupo
Capítulo II. Revisão da Literatura
18
e/ou domicílio. Destes 8 artigos, 4 abordavam programas realizados em
contexto domiciliário e 4 abordavam programas em grupo.
Conclusão: Parece haver evidência de que os programas realizados em grupo
são mais eficazes do que os realizados no domicílio em doentes com EA.
Concluiu-se também ser vantajosa a realização de programas de exercício no
domicílio do que a ausência de qualquer programa de exercício.
PALAVRAS-CHAVE: Programas de exercício, revisão sistemática, RCT
Capítulo II. Revisão da Literatura
19
Abstract
Introduction: Ankylosing Spondylitis (AS) is a chronic inflammatory rheumatic
disease characterized by inflammation of the joints of the spine and sacroiliac
and to a lesser percentage of the peripheral joints. It is a debilitating condition
which reduces quality of life in patients with AS. The practice of physical therapy
is recommended as non-pharmacological treatment as well as the treatment
and prevention of associated deformities.
Objective: To collect and summarize the available evidence in scientific
databases to realize the effectiveness of home based and group based
programs in patients with AS.
Methods: Systematic review, where articles for the study were collected from
scientific database PubMed. We have found 65 articles with publication date
between January 1, 2004 and January 31, 2014. Inclusion and exclusion criteria
were established to make the selection of articles to include in the study. All
investigators provided their agreement in presencial meeting for a final
selection, and at a later stage, the articles were read in full by the three
investigators.
Results: The present systematic review includes eight randomized controlled
trials. All articles show functional benefits in patients with AS subject to exercise
programs in group based and / or home based. From the eight articles, 4
addressed programs conducted in home based context and 4 addressed in
group based context programs.
Conclusion: There appears to be evidence that the programs carried out based
on group are more effective than those home based conducted in patients with
AS. It was concluded also be advantageous to carry out home based exercise
programs than the absence of any exercise program.
KEYWORDS: exercise programs, systematic review, RCT
Capítulo II. Revisão da Literatura
20
Introdução
A Espondilite Anquilosante (EA) é uma patologia reumática inflamatória
crónica, que afeta o esqueleto axial, o tecido sinovial, os ligamentos espinais,
os discos intervertebrais e facetas articulares. Tem repercussões funcionais,
nomeadamente a perda de mobilidade da coluna vertebral, e diminuição de
força dos músculos respiratórios e o comprometimento da expansibilidade
torácica resultando numa perda de qualidade de vida para o doente
(Férnandez-de-las-Peñas et al., 2006; Machado et al., 2011; Masiero et al.,
2011; Rodríguez-Lozano et al., 2013; Strumse et al., 2011). Trata-se de uma
doença que normalmente começa na terceira década de vida, sendo que, em
80% dos indivíduos os sintomas já se revelaram antes dos 30 anos e cerca de
5% manifestam sintomatologia depois dos 45 anos (Sieper et al., 2009).
Como principais sintomas da EA destaca-se a dor e a rigidez na coluna
vertebral, predominantemente no segmento lombar e pélvico. A rigidez matinal,
referida pela maioria dos doentes, tende a melhorar ao longo do dia com a
realização contínua das atividades diárias ou exercício físico (Altan et al., 2012;
Sieper et al., 2009).
Nos últimos anos, têm-se verificado uma intervenção cada vez mais
precoce na EA de forma a prevenir posturas inadequadas, tais como, protusão
da mandíbula, anteriorização da cabeça, hipercifose torácica, retificação da
lordose lombar, retroversão pélvica e flexão com rotação medial da
coxofemural assim como a flexão dos joelhos. O impacto destas alterações
influenciam a capacidade física, social ou psicológica o que afeta em grande
escala a qualidade de vida do doente com EA (Silva et al., 2012).
As terapias mais utilizadas na EA, são a combinação de tratamentos
farmacológicos e não farmacológicos. O exercício físico surge como parte
integrante do tratamento não farmacológico para os doentes com EA, tendo
apresentado bons resultados no controlo da sintomatologia, na diminuição da
rigidez, no aumento da mobilidade articular, capacidade funcional e qualidade
de vida destes indivíduos. Atualmente, vários estudos enfatizam que a eficácia
da prática de programas de exercício físico adequado como adjuvante à terapia
farmacológica (Férnandez-de-las-Peñas et al., 2006; Widberg et al., 2009).
Capítulo II. Revisão da Literatura
21
Relativamente à prática de exercícios, esta pode ser realizada de forma
supervisionada em grupo ou realizada no domicílio, apresentando ambos os
programas resultados benéficos (Braun et al., 2011).
A realização de programas no domicilio ou em grupo, são cada vez mais
uma prática comum no tratamento da EA, comummente com a terapia
farmacológica, pois ambos apresentam benefícios, no entanto, os programas
supervisionados têm mostrado maior eficácia na redução da incapacidade
funcional (Braun et al., 2011). Porque ambos apresentam vantagens e
desvantagens realizou-se esta revisão sistemática da literatura para analisar a
evidência da eficácia de programas no domicílio e em grupo, relativamente ao
aumento da funcionalidade em indivíduos com EA.
Metodologia
A amostra foi constituída por artigos retirados da base de dados
científica PubMed/MEDLINE. A expressão utilizada para a procura dos estudos
foi: ("physical therapy" OR physical activity OR home based program exercices
OR group based) AND (Ankylosing Spondylitis).
Foram apenas considerados os estudos randomizados controlados,
realizados em humanos, publicados na língua inglesa entre janeiro 2004 e
janeiro de 2014, e com qualidade metodológica de pontuação >5 na escala de
PEDro (Maher, 2003). Excluíram-se artigos que não descreviam programas de
exercícios em grupo ou no domicílio e programas de exercício realizados em
meio aquático.
Procedimentos
Toda a bibliografia relevante para o estudo foi lida e analisada por três
investigadores. Através da expressão de pesquisa utilizada na base de dados
PEDro foram obtidos artigos que pudessem ser importantes para o estudo. A
primeira seleção foi realizada pelos limites de pesquisa presentes na base de
dados o que excluiu alguns artigos. Após esta seleção, foram lidos os títulos de
todos os artigos, onde também se excluíram estudos que não direcionassem a
informação para a questão de pesquisa. Após a leitura dos títulos e a seleção
Capítulo II. Revisão da Literatura
22
dos artigos mais relevantes para o estudo, foram lidos os resumos onde se
excluíram artigos que também não se emolduravam com a questão de
pesquisa. As seleções supracitadas foram baseadas nos critérios de
inclusão e exclusão. Após a pesquisa na base de dados, a seleção através da
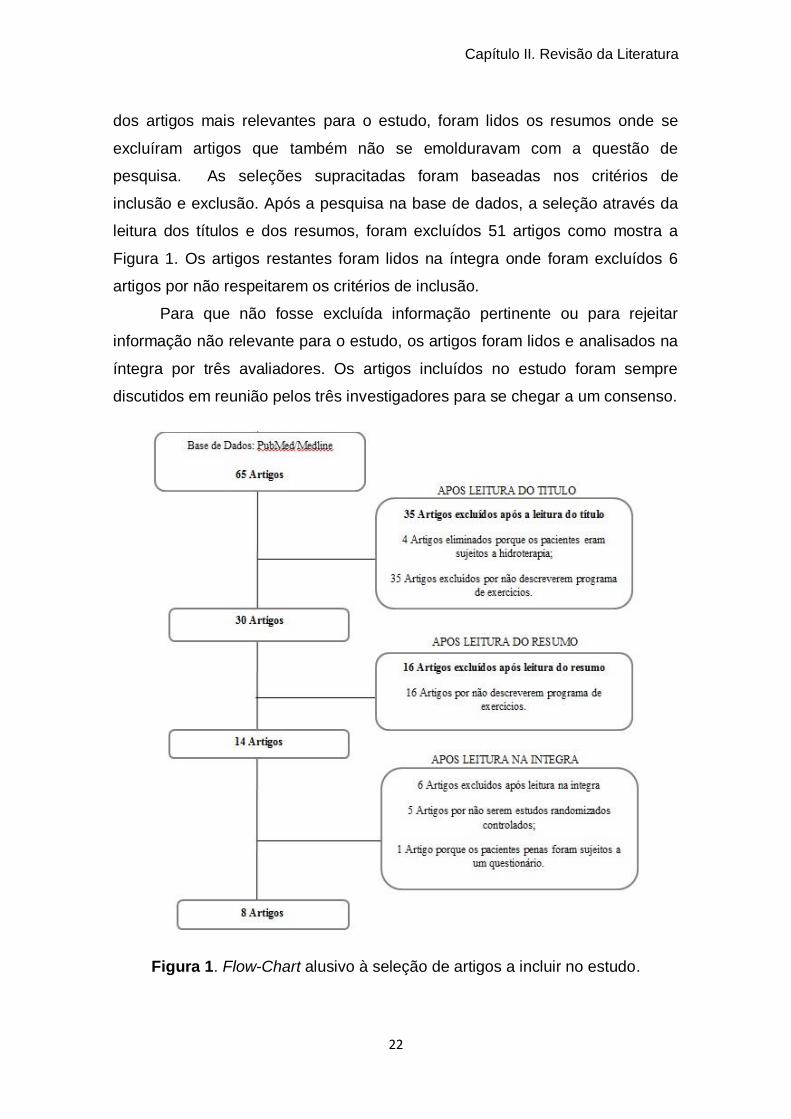
leitura dos títulos e dos resumos, foram excluídos 51 artigos como mostra a
Figura 1. Os artigos restantes foram lidos na íntegra onde foram excluídos 6
artigos por não respeitarem os critérios de inclusão.
Para que não fosse excluída informação pertinente ou para rejeitar
informação não relevante para o estudo, os artigos foram lidos e analisados na
íntegra por três avaliadores. Os artigos incluídos no estudo foram sempre
discutidos em reunião pelos três investigadores para se chegar a um consenso.
Figura 1. Flow-Chart alusivo à seleção de artigos a incluir no estudo.
Capítulo II. Revisão da Literatura
23
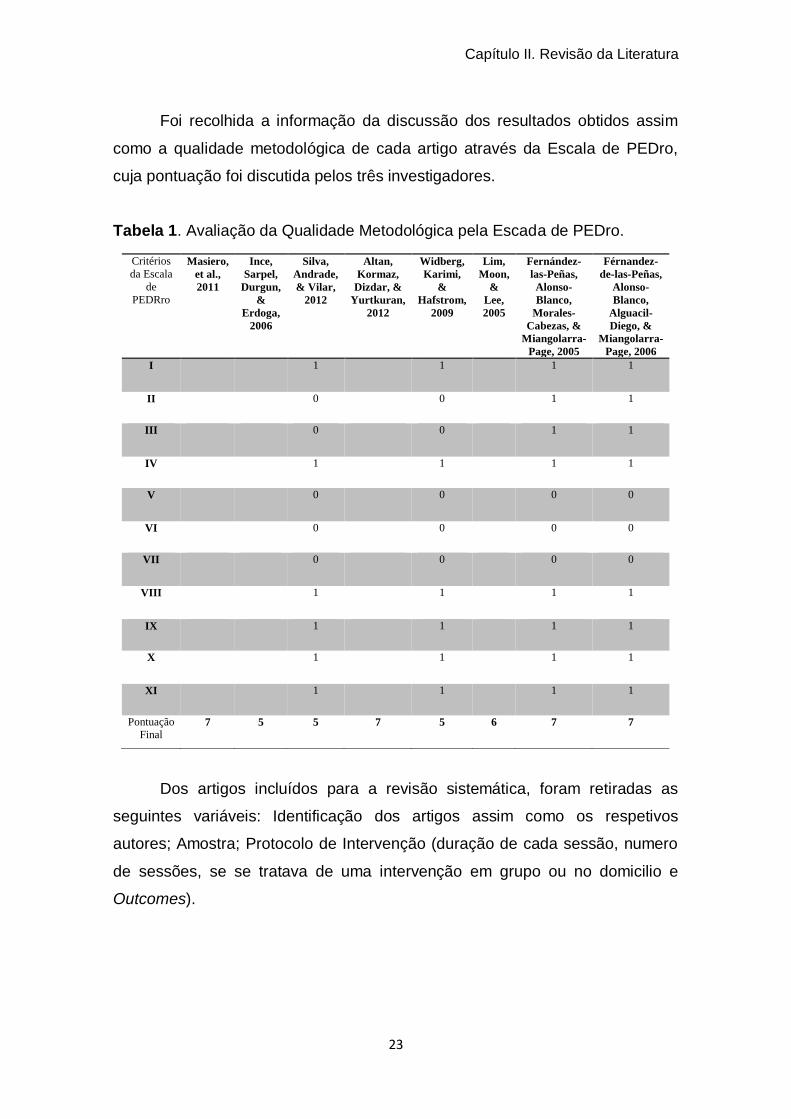
Foi recolhida a informação da discussão dos resultados obtidos assim
como a qualidade metodológica de cada artigo através da Escala de PEDro,
cuja pontuação foi discutida pelos três investigadores.
Tabela 1. Avaliação da Qualidade Metodológica pela Escada de PEDro.
Dos artigos incluídos para a revisão sistemática, foram retiradas as
seguintes variáveis: Identificação dos artigos assim como os respetivos
autores; Amostra; Protocolo de Intervenção (duração de cada sessão, numero
de sessões, se se tratava de uma intervenção em grupo ou no domicilio e
Outcomes).
Tabela I -Avaliação da Qualidade Metodológica pela Escala de PEDro
Critérios
da Escala
de
PEDRro
Masiero,
et al.,
2011
Ince,
Sarpel,
Durgun,
&
Erdoga,
2006
Silva,
Andrade,
& Vilar,
2012
Altan,
Kormaz,
Dizdar, &
Yurtkuran,
2012
Widberg,
Karimi,
&
Hafstrom,
2009
Lim,
Moon,
&
Lee,
2005
Fernández-
las-Peñas,
Alonso-
Blanco,
Morales-
Cabezas, &
Miangolarra-
Page, 2005
Férnandez-
de-las-Peñas,
Alonso-
Blanco,
Alguacil-
Diego, &
Miangolarra-
Page, 2006
I 1 1 1 1
II 0 0 1 1
III 0 0 1 1
IV 1 1 1 1
V 0 0 0 0
VI 0 0 0 0
VII 0 0 0 0
VIII 1 1 1 1
IX 1 1 1 1
X 1 1 1 1
XI 1 1 1 1
Pontuação
Final 7 5 5 7 5 6 7 7
Capítulo II. Revisão da Literatura
24
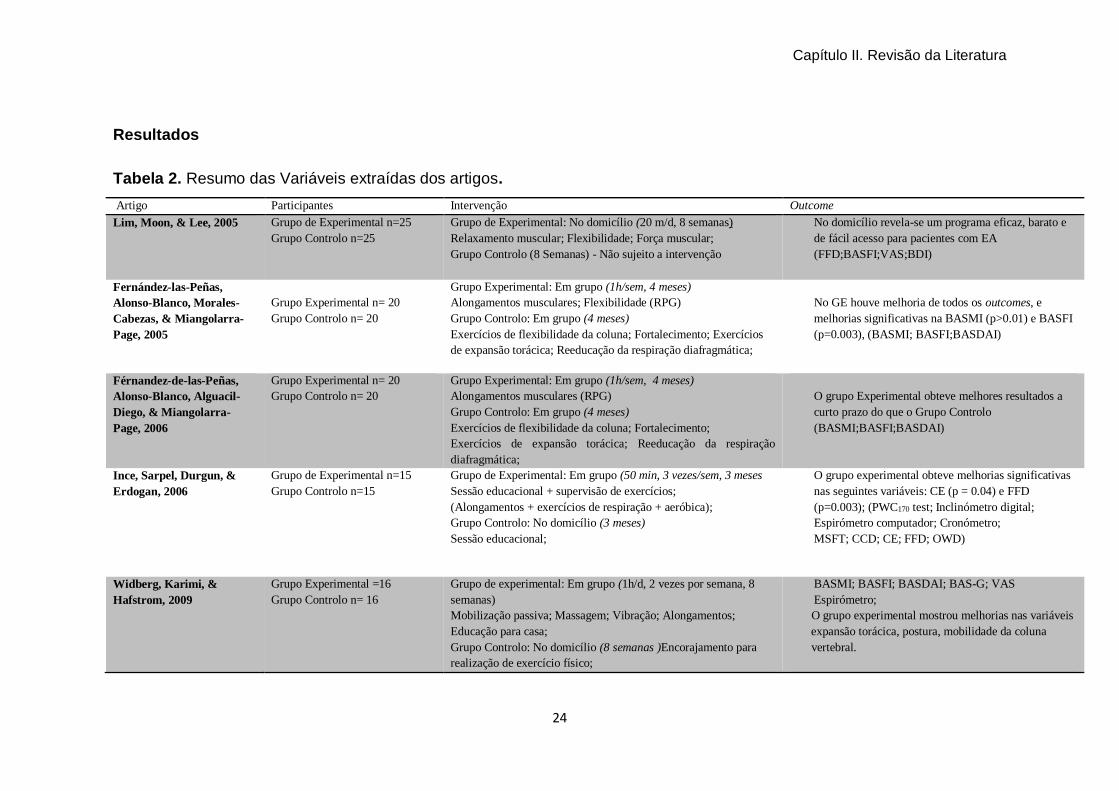
Resultados
Tabela 2. Resumo das Variáveis extraídas dos artigos.
Artigo Participantes Intervenção Outcome
Lim, Moon, & Lee, 2005 Grupo de Experimental n=25
Grupo Controlo n=25
Grupo de Experimental: No domicílio (20 m/d, 8 semanas)
Relaxamento muscular; Flexibilidade; Força muscular;
Grupo Controlo (8 Semanas) - Não sujeito a intervenção
No domicílio revela-se um programa eficaz, barato e
de fácil acesso para pacientes com EA
(FFD;BASFI;VAS;BDI)
Fernández-las-Peñas,
Alonso-Blanco, Morales-
Cabezas, & Miangolarra-
Page, 2005
Grupo Experimental n= 20
Grupo Controlo n= 20
Grupo Experimental: Em grupo (1h/sem, 4 meses)
Alongamentos musculares; Flexibilidade (RPG)
Grupo Controlo: Em grupo (4 meses)
Exercícios de flexibilidade da coluna; Fortalecimento; Exercícios
de expansão torácica; Reeducação da respiração diafragmática;
No GE houve melhoria de todos os outcomes, e
melhorias significativas na BASMI (p>0.01) e BASFI
(p=0.003), (BASMI; BASFI;BASDAI)
Férnandez-de-las-Peñas,
Alonso-Blanco, Alguacil-
Diego, & Miangolarra-
Page, 2006
Grupo Experimental n= 20
Grupo Controlo n= 20
Grupo Experimental: Em grupo (1h/sem, 4 meses)
Alongamentos musculares (RPG)
Grupo Controlo: Em grupo (4 meses)
Exercícios de flexibilidade da coluna; Fortalecimento;
Exercícios de expansão torácica; Reeducação da respiração
diafragmática;
O grupo Experimental obteve melhores resultados a
curto prazo do que o Grupo Controlo
(BASMI;BASFI;BASDAI)
Ince, Sarpel, Durgun, &
Erdogan, 2006
Grupo de Experimental n=15
Grupo Controlo n=15
Grupo de Experimental: Em grupo (50 min, 3 vezes/sem, 3 meses
Sessão educacional + supervisão de exercícios;
(Alongamentos + exercícios de respiração + aeróbica);
Grupo Controlo: No domicílio (3 meses)
Sessão educacional;
O grupo experimental obteve melhorias significativas
nas seguintes variáveis: CE (p = 0.04) e FFD
(p=0.003); (PWC170 test; Inclinómetro digital;
Espirómetro computador; Cronómetro;
MSFT; CCD; CE; FFD; OWD)
Widberg, Karimi, &
Hafstrom, 2009
Grupo Experimental =16
Grupo Controlo n= 16
Grupo de experimental: Em grupo (1h/d, 2 vezes por semana, 8
semanas)
Mobilização passiva; Massagem; Vibração; Alongamentos;
Educação para casa;
Grupo Controlo: No domicílio (8 semanas )Encorajamento para
realização de exercício físico;
BASMI; BASFI; BASDAI; BAS-G; VAS
Espirómetro;
O grupo experimental mostrou melhorias nas variáveis
expansão torácica, postura, mobilidade da coluna
vertebral.
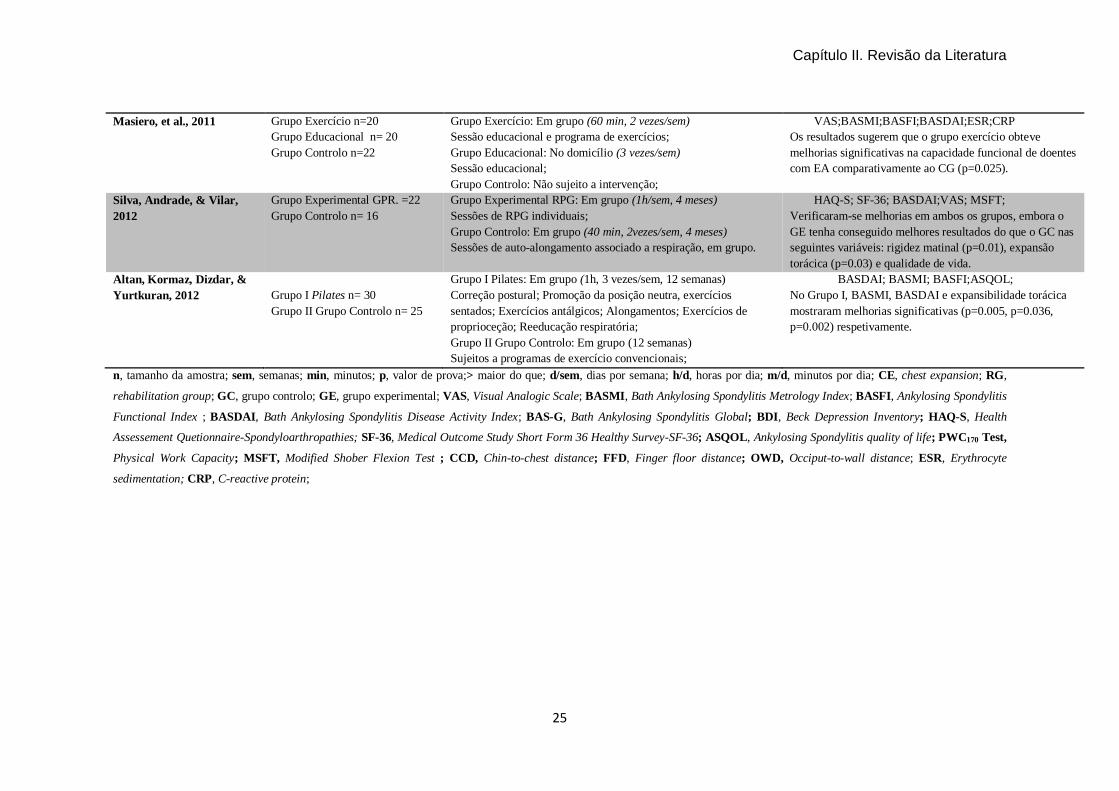
Capítulo II. Revisão da Literatura
25
Masiero, et al., 2011 Grupo Exercício n=20
Grupo Educacional n= 20
Grupo Controlo n=22
Grupo Exercício: Em grupo (60 min, 2 vezes/sem)
Sessão educacional e programa de exercícios;
Grupo Educacional: No domicílio (3 vezes/sem)
Sessão educacional;
Grupo Controlo: Não sujeito a intervenção;
VAS;BASMI;BASFI;BASDAI;ESR;CRP
Os resultados sugerem que o grupo exercício obteve
melhorias significativas na capacidade funcional de doentes
com EA comparativamente ao CG (p=0.025).
Silva, Andrade, & Vilar,
2012
Grupo Experimental GPR. =22
Grupo Controlo n= 16
Grupo Experimental RPG: Em grupo (1h/sem, 4 meses)
Sessões de RPG individuais;
Grupo Controlo: Em grupo (40 min, 2vezes/sem, 4 meses)
Sessões de auto-alongamento associado a respiração, em grupo.
HAQ-S; SF-36; BASDAI;VAS; MSFT;
Verificaram-se melhorias em ambos os grupos, embora o
GE tenha conseguido melhores resultados do que o GC nas
seguintes variáveis: rigidez matinal (p=0.01), expansão
torácica (p=0.03) e qualidade de vida.
Altan, Kormaz, Dizdar, &
Yurtkuran, 2012
Grupo I Pilates n= 30
Grupo II Grupo Controlo n= 25
Grupo I Pilates: Em grupo (1h, 3 vezes/sem, 12 semanas)
Correção postural; Promoção da posição neutra, exercícios
sentados; Exercícios antálgicos; Alongamentos; Exercícios de
proprioceção; Reeducação respiratória;
Grupo II Grupo Controlo: Em grupo (12 semanas)
Sujeitos a programas de exercício convencionais;
BASDAI; BASMI; BASFI;ASQOL;
No Grupo I, BASMI, BASDAI e expansibilidade torácica
mostraram melhorias significativas (p=0.005, p=0.036,
p=0.002) respetivamente.
n, tamanho da amostra; sem, semanas; min, minutos; p, valor de prova;> maior do que; d/sem, dias por semana; h/d, horas por dia; m/d, minutos por dia; CE, chest expansion; RG,
rehabilitation group; GC, grupo controlo; GE, grupo experimental; VAS, Visual Analogic Scale; BASMI, Bath Ankylosing Spondylitis Metrology Index; BASFI, Ankylosing Spondylitis
Functional Index ; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; BAS-G, Bath Ankylosing Spondylitis Global; BDI, Beck Depression Inventory; HAQ-S, Health
Assessement Quetionnaire-Spondyloarthropathies; SF-36, Medical Outcome Study Short Form 36 Healthy Survey-SF-36; ASQOL, Ankylosing Spondylitis quality of life; PWC170 Test,
Physical Work Capacity; MSFT, Modified Shober Flexion Test ; CCD, Chin-to-chest distance; FFD, Finger floor distance; OWD, Occiput-to-wall distance; ESR, Erythrocyte
sedimentation; CRP, C-reactive protein;
Capítulo II. Revisão da Literatura
26
Os oito estudos analisados são Estudos Randomizados Controlados
(RCT). Os critérios de exclusão dos doentes são comuns à maioria dos artigos,
sendo os seguintes: participação em programas de exercícios nos 6 meses
anteriores ao estudo; fraturas por osteoporose; alteração na medicação;
anquilose completa da coluna vertebral (Altan et al., 2012; Férnandez-de-las-
Peñas et al., 2006; Fernández-las-Peñas et al., 2005; Ince et al., 2006; Lim et
al., 2005; Masiero et al., 2011; Silva et al., 2012; Widberg et al., 2009)
Após uma análise relativamente ao número de participantes, não se
verificam diferenças significativas na aleatorização dos grupos. O tamanho
amostral variou entre 30 (Ince et al., 2006) e 62 participantes (Masiero et al.,
2011).
Os estudos de Masiero (Masiero et al., 2011) de Ince(Ince et al., 2006),
de Widberg(Braun et al., 2011) e de Férnandez-de-las-Peñas(Fernández-las-
Peñas et al., 2005), incidiram em programas compostos por exercícios
respiratórios, mobilização da coluna vertebral e membros, exercícios
proprioceptivos para promover postura correta e equilíbrio, alongamento e
fortalecimento dos músculos da coluna vertebral e treino de força.
Num programa de exercícios, no estudo de Silva e colegas (Silva et al., 2012),
basearam-se em oito posições de Reeducação Postural Global (RPG)
associando a respiração com contração e relaxamento dos músculos. Foi
também descrito um programa de exercícios de Pilates, em que os pacientes
foram sujeitos a 9 módulos: correção postural, promoção da posição neutra,
exercícios sentados, exercícios antálgicos, alongamentos, exercícios de
proprioceção e reeducação respiratória (Altan et al., 2012). O único programa
alusivo a exercício no domicílio incluiu exercícios para relaxamento muscular,
flexibilidade, força muscular, reeducação para postura correta, flexão/extensão
do pescoço, inclinação do pesoço e rotação do tronco, alongamentos dos
musculos isquiotibiais, fortalecimento abdominal e glúteos(Lim et al., 2005).
As medidas de outcome mais utilizadas foram: Bath Ankylosing
Spondylitis scales (BAS scales) Bath Ankylosing Spondylitis Metrology Index
(BASMI), Bath Ankylosing Spondylitis Functional Index (BASFI); Bath
Ankylosing Spondylitis Disease Activity Index (BASDAI); Health Assessement
Capítulo II. Revisão da Literatura
27
Questionnaire-Spondyloarthropathies (HAQ); Medical Outcome Study Short
Form 36 Healthy Survey-SF-36; Beck Depression Inventory (BDI).
A maior parte dos instrumentos de avaliação foi aplicada antes e após o
programa de exercício (Lim et al., 2005). Quanto à duração dos programas,
constatou-se alguma heterogeneidade, tendo os follow up variado entre 12
semanas (Férnandez-de-las-Peñas et al., 2006) a 12 meses (Altan et al., 2012).
Discussão
Após a análise da literatura, pode afirmar-se que há suficiente evidência
de que programas de exercício no domicilio e em grupo são eficazes no
tratamento da EA. Alguns resultados descrevem que programas de exercício
supervisionados (em grupo) têm melhores resultados comparativamente a
programas de exercícios realizados em casa sem supervisão (no domicílio),
embora ambos relatem melhorias (Altan et al., 2012; Férnandez-de-las-Peñas
et al., 2006; Fernández-las-Peñas et al., 2005; Ince et al., 2006; Lim et al.,
2005; Masiero et al., 2011; Silva et al., 2012; Widberg et al., 2009).
Relativamente aos programas de exercícios em grupo, estes são
supervisionados, o que se revela uma vantagem no sentido de promover uma
correta realização dos exercícios, associada também a uma constante
estimulação verbal e à realização dos exercícios em grupo promovendo uma
maior motivação por parte dos doentes. Parece que pela associação destes
factores os programas em grupo se têm verificado mais eficazes (Souza et al.,
2012). Os custos inerentes surgem neste tipo de programas como a sua maior
desvantagem, visto ser necessário o deslocamento para o local da sessão. Nos
programas no domicílio, os doentes apenas têm sessões educacionais, onde
são ensinados exercícios para realizar em casa, sem supervisão, ou seja, não
se efetua a correcção de possíveis erros de execução de exercícios e
tendencialmente a motivação tende a ser menor. Apesar deste tipo de
programa se ter também revelado eficaz, não se mostra tão eficiciente como os
programas supervisionados (em grupo). Sendo assim, é percetível que haja
maior adesão a programas em grupo, apesar de os programas em domicílio
serem mais económicos, no entanto, também são efetivos pela capacitação do
Capítulo II. Revisão da Literatura
28
doente no cumprimento das recomendações realizadas pelo profissional de
saúde nomeadamente no tipo de exercícios, duração e frequência (Lim et al.,
2005; Souza et al., 2012)
A prática contínua de exercício proporciona uma estimulação
propriocetiva, fator de estabilidade dinâmica, promovendo uma modulação e
coordenação da atividade muscular, benéfico para estes doentes com
espondilite anquilosante. Os exercícios em grupo e no domicílio não variam
muito na sua tipologia, estando na maioria dos programas de exercícios
presentes os alongamentos, a correção postural, o fortalecimento muscular e a
reeducação respiratória, atenuando desta forma as complicações inerentes à
EA, nomeadamente a dor, a performance funcional, e respiratória (Passalent,
2011).
Têm sido igualmente estudados programas de treino baseados no RPG
e Pilates que se têm revelado também válidos e eficazes (Altan et al., 2012;
Férnandez-de-las-Peñas et al., 2006; Fernández-las-Peñas et al., 2005).
No estudo de Masiero (Masiero et al., 2011), os resultados sugerem que
a combinação de exercício físico supervisionado com sessões de educação e
esclarecimento podem promover resultados promissores em doentes com EA
em situação clinicamente estável.
A combinação de exercícios aeróbicos, fortalecimento e exercícios
respiratórios durante um período de 3 meses também se revela eficaz, levando
a melhorias na mobilidade da coluna vertebral, volume corrente e capacidade
física de trabalho (Ince et al., 2006).
No estudo de Silva (Silva et al., 2012) foram demonstradas melhorias em
ambos os grupos de tratamento, no entanto, elas foram mais evidentes no
Grupo RPG em algumas variáveis, nomeadamente rigidez matinal, mobilidade
da coluna vertebral, expansão torácica e qualidade de vida.
Outros autores planearam os seus programas de exercícios com base
no método de RPG, mostrando também melhorias a curto e a longo prazo
comparativamente a programas convencionais em doentes com EA. Este
método baseia-se em alongamentos posturais globais, de forma mais estática,
prolongados no tempo, trabalhando cadeias musculares anti gravitacionais,
Capítulo II. Revisão da Literatura
29
utilizando oito posições em pé ou deitado (Férnandez-de-las-Peñas et al.,
2006; Fernández-las-Peñas et al., 2005). Isto significa que o método de RPG é
uma hipótese válida e eficaz no tratamento destes doentes em programas em
grupo.
Também o método de Pilates mostrou ser uma possibilidade válida no
tratamento de doentes com EA, visto que foi eficaz no estudo realizado por
Altan (Altan et al., 2012). Neste estudo foi comprovado que o método de Pilates
é eficaz, seguro e que melhora a capacidade física neste tipo de doentes. Este
método baseia-se em alongamentos dinâmicos dirigidos essencialmente à
coluna vertebral com o objetivo de corrigir a postura e fortalecer a musculatura.
Segundo Altan (Altan et al., 2012), após um programa de 8 semanas,
verificaram-se melhorias a nível da expansibilidade torácica, postura e
mobilidade da coluna vertebral em programas em grupo.
No estudo de Lim (Lim et al., 2005), foi relatado um programa no
domicílio que se verificou seguro, dado que melhorou a mobilidade articular e
influenciou positivamente os níveis de capacidade funcional, dor e depressão
em doentes com EA.
Relativamente às avaliações, os instrumentos de avaliação mais
utilizados foram: BAS-G, BASMI, BASFI, BASDAI. Estes instrumentos têm por
base população com EA e são específicos para avaliar esta condição de saúde
e a funcionalidade destes indivíduos.
É de salientar a escassez de estudos randomizados controlados nesta
área o que sugere a necessidade de se realizar mais estudos que comparem
estas duas modalidades de programas em simultâneo.
Conclusão
Tendo por base a revisão efetuada, parece que os programas em grupo
são mais eficazes do que no domicílio, no entanto, apesar de os programas no
domicílio não se revelarem tão eficazes, são recomendados a doentes que não
praticam qualquer tipo de programa de exercício físico. São necessários mais
Capítulo II. Revisão da Literatura
30
estudos randomizados controlados para que este tipo de programas se torne
numa rotina diária para estes doentes.
Bibliografia
Altan, L., Korkmaz, N., Dizdar, M., & Yurtkuran, M. (2012). Effect of Pilates
training on people with ankylosing spondylitis. Rheumatol Int, 32(7),
2093-2099.
Braun, J., van den Berg, R., Baraliakos, X., Boehm, H., Burgos-Vargas, R.,
Collantes-Estevez, E., Dagfinrud, H., Dijkmans, B., Dougados, M.,
Emery, P., Geher, P., Hammoudeh, M., Inman, R. D., Jongkees, M.,
Khan, M. A., Kiltz, U., Kvien, T., Leirisalo-Repo, M., Maksymowych, W.
P., Olivieri, I., Pavelka, K., Sieper, J., Stanislawska-Biernat, E.,
Wendling, D., Ozgocmen, S., van Drogen, C., van Royen, B., & van der
Heijde, D. (2011). 2010 update of the ASAS/EULAR recommendations
for the management of ankylosing spondylitis. Ann Rheum Dis, 70(6),
896-904.
Férnandez-de-las-Peñas, C., Alonso-Blanco, C., Alguacil-Diego, I. M., &
Miangolarra-Page, J. C. (2006). One-Year Follow-up of Two Exercice
Interventions for the Management of Patients with Ankylosing
Spondylitis. Am. J. Phys. Med. Rehabil, 559-567.
Fernández-las-Peñas, C., Alonso-Blanco, C., Morales-Cabezas, M., &
Miangolarra-Page, J. C. (2005). Two Exercise Interventions for the
Management of Patients with Ankylosing Spondilitis. American Journal of
Physical Medicine e Rehabilitation, 407-419.
Ince, G., Sarpel, T., Durgun, B., & Erdogan, S. (2006). Effects of a Multimodal
Exercise Program for People With Ankylosing Spondylitis. Physical
Therapy, 924-935.
Lim, H. J., Moon, Y. I., & Lee, M. S. (2005). Effects of home-based daily
exercise therapy on joint mobility, daily activity, pain, and depression in
patients with ankylosing spondylitis. Rheumatol Int, 25(3), 225-229.
Machado, P., Landewé, R., Lie, E., Kvien, T. K., Braun, J., Baker, D., & Heijde,
D. v. d. (2011). Ankylosing Spondylitis Disease Activity Score (ASDAS):
Capítulo II. Revisão da Literatura
31
defi ning cut-off values for disease activity states and improvement
scores. Ann Rheum Dis, 47-53.
Maher, C., Sherrington, C., Herbert, R.D., Moseley, A. and Elkins, M. (2003).
Reliability of the PEDro Scale for Rating Quality of Randomized
Controlled Trials. PHYS THER., 83, 713-721.
Masiero, S., Bonaldo, L., Pigatto, M., Lo Nigro, A., Ramonda , R., & Punzi , L.
(2011). Rehabilitation Treatment in Patients with Ankylosing Spondylitis
Stabilized with Tumor Necrosis Factor Inhibitor Therapy. A Randomized
Controlled Trial. The Journal of Rheumatology 1-8.
Passalent, L. A. (2011). Physiotherapy for ankylosing spondylitis: evidence and
application. Curr Opin Rheumatol, 23(2), 142-147.
Rodríguez-Lozano, C., Juanola, X., Cruz-Martínez, J., Peña-Arrébola, A.,
Mulero, J., Gratacós, J., & Collantes, E. (2013). Outcome of an education
and home-based exercice programme for patients with ankylosing
spondylitis: a nationwide randomized study. Education and home based
exercicie programme for AS patients, 1-10.
Sieper, J., Rudwaleit, M., Baraliakos, X., Brandt, J., Braun, J., Burgos-Vargas,
R., Dougados, M., Hermann, K. G., Landewe, R., Maksymowych, W., &
van der Heijde, D. (2009). The Assessment of SpondyloArthritis
international Society (ASAS) handbook: a guide to assess
spondyloarthritis. Ann Rheum Dis, 68 Suppl 2, ii1-44.
Silva, E. M., Andrade, S. C., & Vilar, M. J. (2012). Evaluation of the effects of
Global Postural Reeducation in patients with ankylosing spondylitis.
Rheumatol Int, 32(7), 2155-2163.
Souza, M. C., Orlandi, A., Jones, A., Jennings, F., & Biruel, E. (2012). Grupos
educacionais para pacientes com Espondilite Anquilosante: revisão
sistemática. Rev Dor, 256-260.
Strumse, Y. A. S., Nordvag, B.-Y., Stanghelle, J. K., Roisland, M., Winther , A.,
Pajunen, P.-A., Garen, T., & Flato, B. (2011). Efficacy of rehabilitation for
patients with ankylosing spondilytis: comparison of four-week
rehabilitation programme in a mediterranean and a norwegian setting. J
Rehabil Med 534-542.

Capítulo II. Revisão da Literatura
32
Widberg, K., Karimi, H., & Hafstrom, I. (2009). Self-and manual mobilization
improves spine mobility in men with ankylosing spondylitis - a
randomized study. Clinical Rehabilitation, 599-608.
Capítulo III
Estudos Originais
_____________________________________________________


Estudo II _____________________________________________________
Cross-cultural adaptation and validation of the Portuguese version of
“The assessment of knowledge in ankylosing spondylitis patients by a
self-administered questionnaire”
Sofia Lopes1; José Alberto Duarte 2; Cristina Mesquita1
1 Escola Superior de tecnologia da Saúde do Porto, Instituto Politécnico do
Porto
2 Faculdade de Desporto, Universidade do Porto
Publicado na Rheumatology International (2016)
DOI 10.1007/s00296-016-3434-2
_____________________________________________________


Capítulo III. Estudos Originais
37
Sofia Manuela da Rocha Lopes, Escola Superior de Tecnologia de Saúde (School of
Health Technology), Polytechnic Institute of Porto, Rua Valente Perfeito, 322, 4400-
330 Vila Nova de Gaia, Portugal, Tel.:+351 222061000, e-mail: [email protected]
José Alberto Duarte, Faculty of Sport, University of Porto, Rua Dr. Plácido Costa, 91 -
4200,450 Porto, Portugal, Tel.:+351 220 425 200, e-mail: [email protected]
Cristina Teresa Torrão Carvalho Mesquita, Escola Superior de Tecnologia de Saúde
(School of Health Technology), Polytechnic Institute of Porto, Rua Valente Perfeito,
322, 4400-330 Vila Nova de Gaia, Portugal, Tel.:+351 222061000, e-mail:

Capítulo III. Estudos Originais
38
Abstract
Background: Knowledge is an important factor in patients with ankylosing
spondylitis regarding the adoption of appropriate behaviours and education.
Aim: To culturally adapt and validate "The assessment of knowledge in
ankylosing spondylitis patients by the self-administered questionnaire" for the
Portuguese population with ankylosing spondylitis. Methods: The Portuguese
version of “The assessment of knowledge in ankylosing spondylitis patients by a
self-administered questionnaire” was administered to a sample of 180 subjects,
from which 63 individuals responded. The adaptation process involved
translation, back translation and submission to a committee of experts in the
area, culminating with a Portuguese version of the instrument. Next, the scale
reliability and validity were assessed. Results: There was a statistical
significant decrease from test to re-test, although the intra-class correlation
coefficient (ICC) between test and re-test was 0.76 (95%: 0.61; 0.86), which
was considered good. From 180 individuals, 63 (35.0%) subjects were available
for the present study. The proportion of individuals that correctly answered each
item ranged from 19% to 92%, corresponding to items 8 and 13, respectively.
The mean number of correct answers was 8.5 (SD=2.4) in 12 questions.
Conclusions: The proposed Portuguese version of the ankylosing spondylitis
knowledge scale showed good psychometric proprieties, with good internal
consistency and good reproducibility.
Key words: cross-cultural validation; ankylosing spondylitis knowledge;
ankylosing spondylitis education.
Capítulo III. Estudos Originais
39
Introduction
Ankylosing spondylitis (AS) is a systemic disease characterised by
chronic inflammation and leading to a loss of mobility and functionality of the
entire axial skeleton (Arturi et al., 2013; Bodur et al., 2011; Gyurcsik et al.,
2012). Intervention for AS has generally a pharmacological and
nonpharmacological nature, with nonpharmacological measures including
physical exercise and patient education (Marcelo Cardozo de Souza, 2012;
Passalent, 2011; Yigit et al., 2013).
Education is of the utmost importance when it comes to patients with
chronic condition, in particular with rheumatic diseases, as in the case of
patients with AS. According to the recommendations of the European League
against Rheumatism (EULAR) (2010), education is considered the cornerstone
of nonpharmacological treatment (Braun et al., 2011).Education programmes
shall be used as a complement to treatment, to teach patients how to deal with
pain, to control symptoms and to deal with the worsening and chronic nature of
their condition. These programmes must be patient-oriented, focused on
improving their skills and self-efficiency as to the disease, thereby promoting the
psychological and behavioural well-being and inducing in the long run a better
understanding of their disease (Marcelo Cardozo de Souza, 2012; Rat, 2013).
A better knowledge of the disease provides a greater involvement in
decision-making, with patients taking an active role in managing their situation
(Roxanne Cooksey, 2012). In addition, it affects the reduction of the associated
costs, both direct, such as medication, outpatient visits, hospitalisations,
surgery, and indirect, such as absence from work, anxiety and decreased
quality of life (Frauendorf et al., 2013; Marcelo Cardozo de Souza, 2012;
Reveille et al., 2012). Developing the skills of patients with AS and their
relatives is fundamental for a good understanding inside the family, so that the
appropriate behaviours can be adopted by the family as a whole (Younes et al.,
2010).
Currently, in Portugal, few data are available on the knowledge of
patients with AS regarding their disease, as there is no instrument in the
Capítulo III. Estudos Originais
40
Portuguese language which allows doing that assessment. In the United
Kingdom, Lubrano et al.(E. Lubrano, 1998) developed a questionnaire to
evaluate the knowledge of patients with AS, with this questionnaire being
afterwards translated and validated by Claudepierre et al.(Claudepierre et al.,
2004) for the French population with this disease.
The relevance of creating a Portuguese version of this questionnaire is
based on the need to assess the type of knowledge each patient has about
themselves and about their condition, so as to minimise the negative impact AS
has on their quality of life and also on the country’s socioeconomical context.
The aim of the present study was to culturally adapt and validate “The
assessment of knowledge in ankylosing spondylitis patients by a self-
administered questionnaire” for the Portuguese population with AS.
Methods
Sample and recruitment
The present study was observational, cross-sectional and included a
population of 180 individuals, members of the National Association of
Ankylosing Spondylitis (ANEA), from the Northern Portugal branch, diagnosed
with AS. As inclusion criteria, we have defined the diagnosis of AS, according to
the Modified New York criteria (Claudepierre et al., 2004). The study excluded
individuals with other clinical conditions common to AS, such as rheumatoid
arthritis and systemic lupus.
Original instrument
The questionnaire “The assessment of knowledge in ankylosing
spondylitis patients by a self-administered questionnaire” is used to assess AS
patients’ level of knowledge, using 14 multiple-choice questions. It has 72
possible responses, but only 25 of them are correct. This questionnaire
examines different areas:(1) general knowledge, aetiology, symptoms, blood
tests; (2) immunogenetic tests (B27 antigen) and inheritance; (3) general
management, including pharmacological and nonpharmacological (posture,
exercise regimen) intervention; (4) joint protection, pacing and priorities
Capítulo III. Estudos Originais
41
(Claudepierre et al., 2004; E. Lubrano, 1998). The score is obtained by
assigning one point for each correct answer, with a possible maximum score of
25 points, and by assigning one point to each question (14 questions) with all
correct answers (maximum of 14 points), being then these two scores summed
to give a final score (Claudepierre et al., 2004).
Cross-cultural adaptation
This process included two stages. In the first stage, two bilingual
translators working independently translated and adapted the questionnaire to
the Portuguese culture, to detect possible understanding and translation
problems resulting from the use of technical and uncommon vocabulary
(Ferreira, 2000a, 2000b). The two resulting translations were compared and
merged into one single version. Then, two different bilingual translators working
independently from one another performed the translation into English (back
translation) of the document. Following this step, two rheumatology specialists
proofread the translated questionnaire, comparing the original and final versions
to merge them into a single document, analyzing and discussing the differences
found between the two versions until reaching an agreement. The final version
of the questionnaire was first piloted in a group of 10 individuals with AS, to
understand if the vocabulary used was appropriate and if the questionnaire was
easily understood. On the second stage, the questionnaire was assessed as to
its psychometric properties, reliability and validity (Ramada-Rodilla et al., 2013).
The present study was approved by the Ethical Committee of Escola Superior
de Tecnologia da Saúde do Porto (ESTSP). The access to data of ANEA’s
members, in particular their addresses, was granted by the president of ANEA’s
North branch.
One-hundred eighty envelopes were sent by post, each one containing a
characterisation questionnaire, the knowledge questionnaire which constitutes
the object of the present study and an informed consent statement. Individuals
who returned the questionnaire were sent the same questionnaire 4 weeks after
the first, to assess its reproducibility (E. Lubrano, 1998).
Capítulo III. Estudos Originais
42
Statistical analysis
In the present study, and given the binary structure of the data, the latent
trait model (LTM) was used to identify dimensions in knowledge about AS in the
patient population. LTM is simply a binary data factor analysis that considers
one or more factors (Milton Severo, 2010).
Interpretation of the model is usually done considering the standardised
factor loadings. A standardised factor loading is classified as weak if the
corresponding absolute value is less than 0.30, moderate if it is between 0.30
and 0.70, and strong if it is higher than 0.70.
The standardised Cronbach’s alpha was estimated to evaluate the
internal consistency of the group of items.
The final score was the sum of all items in the questionnaire with
absolute standardised factor loadings higher than 0.3. A question was
considered correctly answered when the 2 correct options were selected (1
point).
The test–retest reliability was assessed using a two-way mixed intra-
class correlation coefficient (ICC) for single-measures.
Two independent sample t-student test and one factor analysis of
variance (ANOVA) were used to compare the score between two or three
independent groups, respectively.
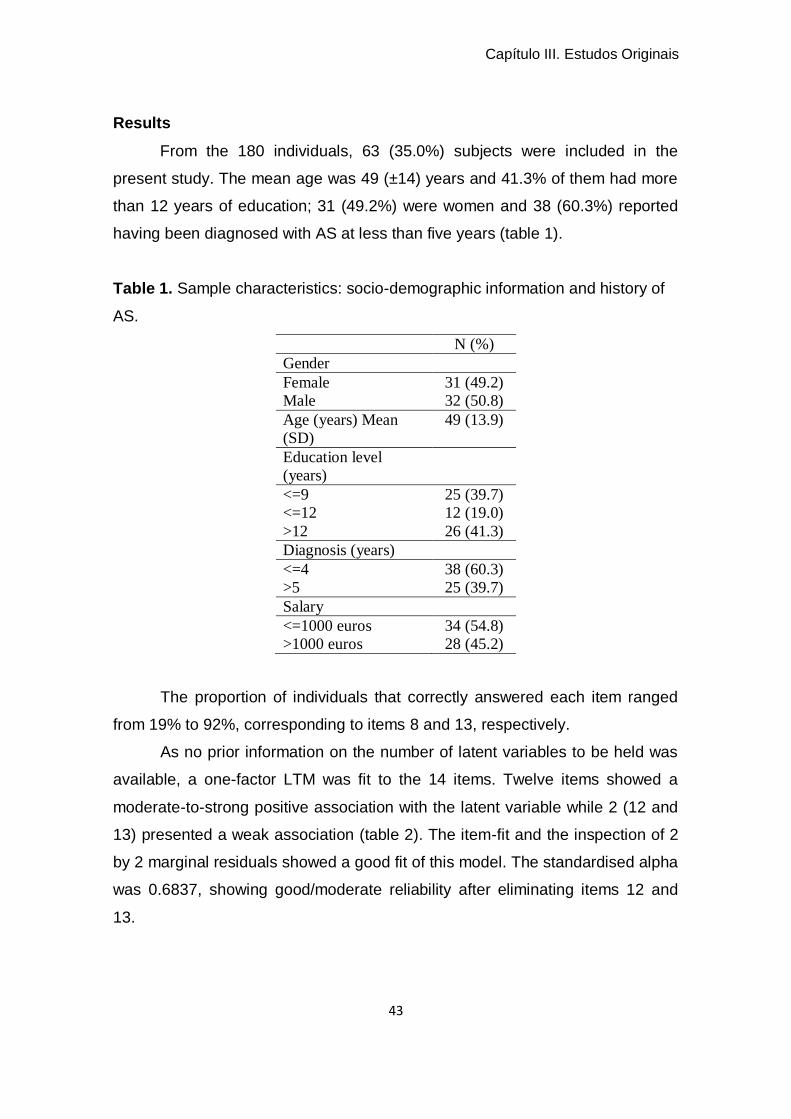
Capítulo III. Estudos Originais
43
Results
From the 180 individuals, 63 (35.0%) subjects were included in the
present study. The mean age was 49 (±14) years and 41.3% of them had more
than 12 years of education; 31 (49.2%) were women and 38 (60.3%) reported
having been diagnosed with AS at less than five years (table 1).
Table 1. Sample characteristics: socio-demographic information and history of
AS.
N (%)
Gender
Female 31 (49.2)
Male 32 (50.8)
Age (years) Mean
(SD)
49 (13.9)
Education level
(years)
<=9 25 (39.7)
<=12 12 (19.0)
>12 26 (41.3)
Diagnosis (years)
<=4 38 (60.3)
>5 25 (39.7)
Salary
<=1000 euros 34 (54.8)
>1000 euros 28 (45.2)
The proportion of individuals that correctly answered each item ranged
from 19% to 92%, corresponding to items 8 and 13, respectively.
As no prior information on the number of latent variables to be held was
available, a one-factor LTM was fit to the 14 items. Twelve items showed a
moderate-to-strong positive association with the latent variable while 2 (12 and
13) presented a weak association (table 2). The item-fit and the inspection of 2
by 2 marginal residuals showed a good fit of this model. The standardised alpha
was 0.6837, showing good/moderate reliability after eliminating items 12 and
13.
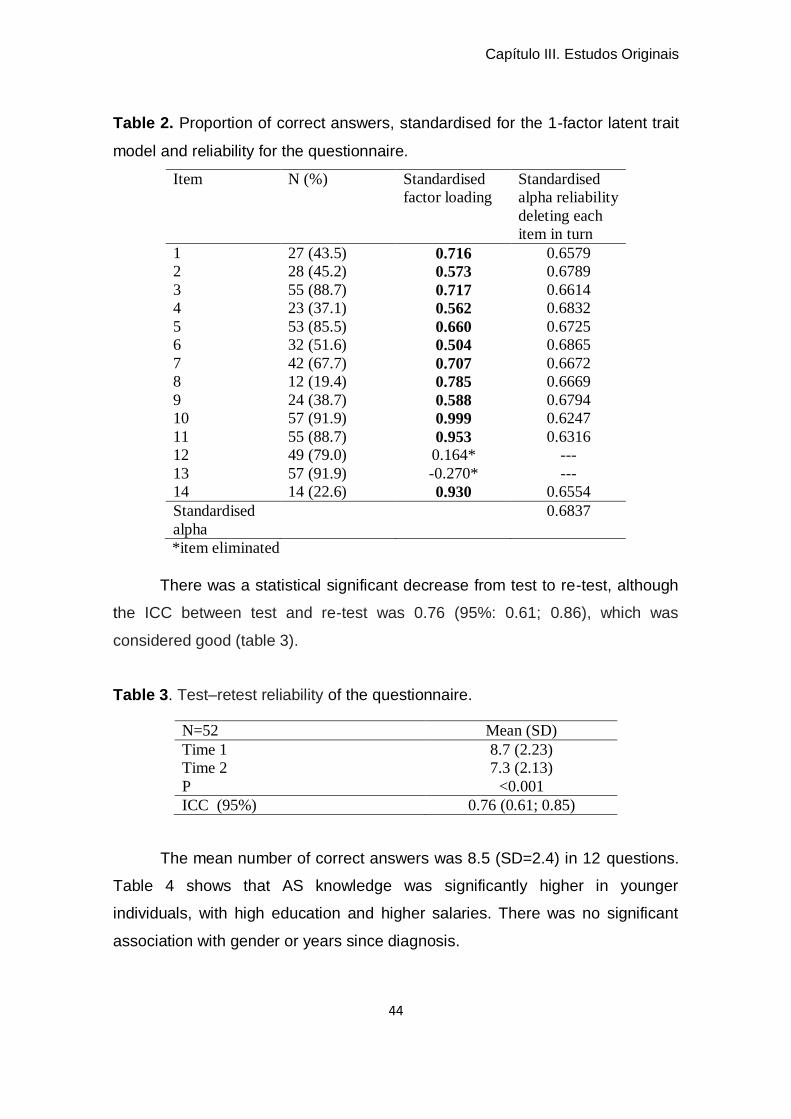
Capítulo III. Estudos Originais
44
Table 2. Proportion of correct answers, standardised for the 1-factor latent trait
model and reliability for the questionnaire.
Item N (%) Standardised
factor loading
Standardised
alpha reliability
deleting each
item in turn
1 27 (43.5) 0.716 0.6579
2 28 (45.2) 0.573 0.6789
3 55 (88.7) 0.717 0.6614
4 23 (37.1) 0.562 0.6832
5 53 (85.5) 0.660 0.6725
6 32 (51.6) 0.504 0.6865
7 42 (67.7) 0.707 0.6672
8 12 (19.4) 0.785 0.6669
9 24 (38.7) 0.588 0.6794
10 57 (91.9) 0.999 0.6247
11 55 (88.7) 0.953 0.6316
12 49 (79.0) 0.164* ---
13 57 (91.9) -0.270* ---
14 14 (22.6) 0.930 0.6554
Standardised
alpha
0.6837
*item eliminated
There was a statistical significant decrease from test to re-test, although
the ICC between test and re-test was 0.76 (95%: 0.61; 0.86), which was
considered good (table 3).
Table 3. Test–retest reliability of the questionnaire.
N=52 Mean (SD)
Time 1 8.7 (2.23)
Time 2 7.3 (2.13)
P <0.001
ICC (95%) 0.76 (0.61; 0.85)
The mean number of correct answers was 8.5 (SD=2.4) in 12 questions.
Table 4 shows that AS knowledge was significantly higher in younger
individuals, with high education and higher salaries. There was no significant
association with gender or years since diagnosis.
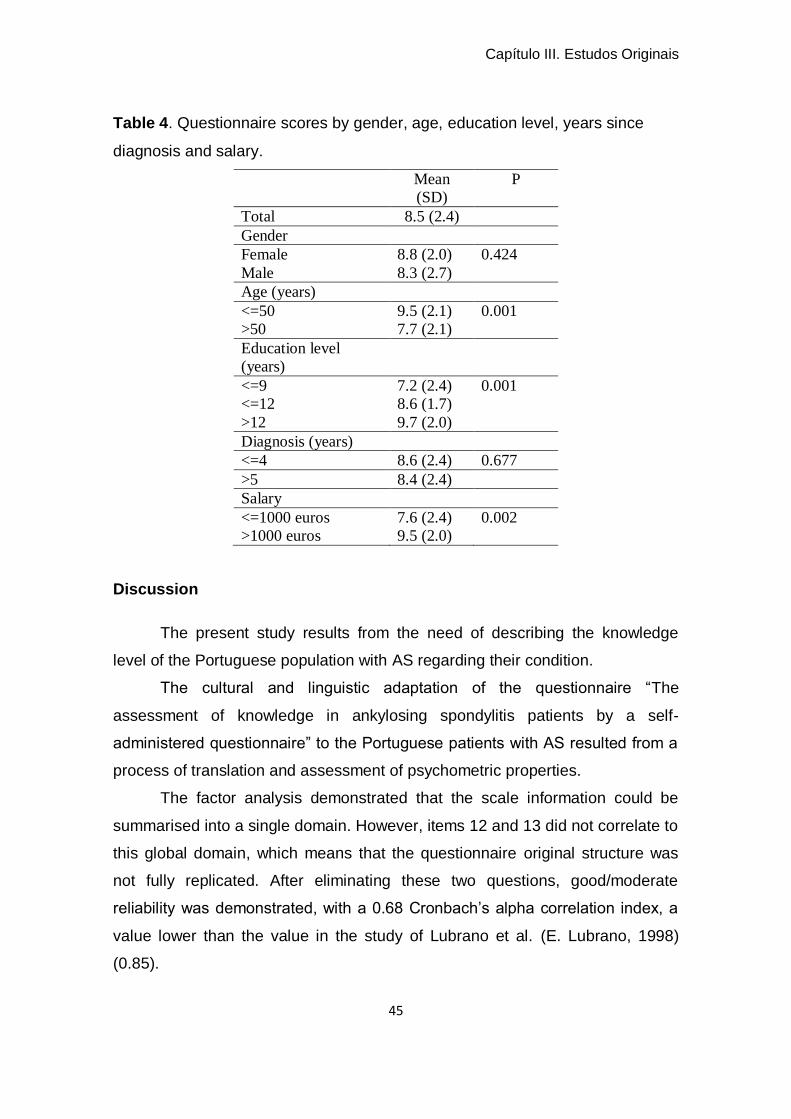
Capítulo III. Estudos Originais
45
Table 4. Questionnaire scores by gender, age, education level, years since
diagnosis and salary.
Mean
(SD)
P
Total 8.5 (2.4)
Gender
Female 8.8 (2.0) 0.424
Male 8.3 (2.7)
Age (years)
<=50 9.5 (2.1) 0.001
>50 7.7 (2.1)
Education level
(years)
<=9 7.2 (2.4) 0.001
<=12 8.6 (1.7)
>12 9.7 (2.0)
Diagnosis (years)
<=4 8.6 (2.4) 0.677
>5 8.4 (2.4)
Salary
<=1000 euros 7.6 (2.4) 0.002
>1000 euros 9.5 (2.0)
Discussion
The present study results from the need of describing the knowledge
level of the Portuguese population with AS regarding their condition.
The cultural and linguistic adaptation of the questionnaire “The
assessment of knowledge in ankylosing spondylitis patients by a self-
administered questionnaire” to the Portuguese patients with AS resulted from a
process of translation and assessment of psychometric properties.
The factor analysis demonstrated that the scale information could be
summarised into a single domain. However, items 12 and 13 did not correlate to
this global domain, which means that the questionnaire original structure was
not fully replicated. After eliminating these two questions, good/moderate
reliability was demonstrated, with a 0.68 Cronbach’s alpha correlation index, a
value lower than the value in the study of Lubrano et al. (E. Lubrano, 1998)
(0.85).
Capítulo III. Estudos Originais
46
The test-retest value obtained was good (0.6), as in the study of Lubrano
et al. (E. Lubrano, 1998) (0.77), demonstrating good reliability.
The patients with AS included in the present study demonstrated a high
level of knowledge regarding their condition. Knowledge levels were higher in
younger individuals, having higher levels of general education and higher
salaries, as in the study of Lubrano et al. and Claudepierre et al.(Claudepierre
et al., 2004; E. Lubrano, 1998), which confirms the scale validity. These
associations can be explained by the fact that individuals with higher education
levels are more demanding in their search for information regarding their
disease, as a way to control it more effectively. The same happens with
younger individuals or with higher economic power,who have access to a
different type of information (Marcelo Cardozo de Souza, 2012). In most
individuals with chronic diseases, the education level is a good predictor of a
favourable outcome, considering that low education levels, associated with
lower socio-economical condition, are normally associated with poor health
(Ramos-Remus C, 2000).
As in the study of Hennell et al. (Hennell et al., 2004), in the present
study no correlation was found between the level of disease knowledge and
gender. This can result from the lack of interest demonstrated by male patients
in getting more information regarding their condition, as in the study of Cooksey
et al. (Roxanne Cooksey, 2012), which proves that, between gender, women
are more interested than men in gathering information on AS. No correlation
was verified between knowledge and the number of years since diagnosis,
which corroborates the results in the study of Jenningset al. (F. Jennings, 2006)
as to knowledge regarding rheumatoid arthritis. These authors have justified
this by the fact that old individuals’ time since diagnosis is longer and, as they
get older, they show no interest in increasing their knowledge as to their
disease.
The results obtained demonstrate that in the present study symptoms,
immunological testing and treatment are the areas where knowledge is higher,
which can be explained by the fact that the clinical onset of the disease occurs
early, motivating a quick search of diagnosis and treatment. The characteristics
Capítulo III. Estudos Originais
47
of these patients and their surrounding environment, in particular their attitude
and knowledge as regards the disease, and the type of treatment they are
submitted to, can be responsible for increasing/reducing symptoms (Roxanne
Cooksey, 2012).
Most individuals affected by AS discover the characteristics of their
disease as symptoms appear and limitations become more visible. Even the
management of pain, fatigue and negative emotions commonly associated with
changes in some family and professional roles make that basic information is
not enough for these patients,with the search of more complete knowledge and
education as regards the disease becoming crucial (Rat, 2013).
The present study has some limitations, such as the fact that participants
are members of an association of AS, which in some way results from their
interest in being more informed. Another limitation is related with the sample
size, which is very reduced when compared to the study of Lubrano et al. (E.
Lubrano, 1998).
In the future, it would be appropriate to study the correlation between
knowledge and other variables, such as the Bath indexes and the perception on
the quality of life, to facilitate the understanding and knowledge influence on this
disease. According to the results of the present study, we suggest a reflection to
be made on the application of strategies such as education, as this must be
regarded as the cornerstone in adopting behaviours and making decisions with
a positive impact on the quality of life of individuals with AS.
Main findings
The proposed Portuguese version of the ankylosing spondylitis
knowledge scale showed good psychometric proprieties. The ankylosing
spondylitis knowledge scale showed one dimension with good internal
consistency. The test-retest showed that the ankylosing spondylitis knowledge
scale had good reproducibility.
Capítulo III. Estudos Originais
48
Bibliography
Arturi, P., Schneeberger, E. E., Sommerfleck, F., Buschiazzo, E., Ledesma, C.,
Maldonado Cocco, J. A., & Citera, G. (2013). Adherence to treatment in
patients with ankylosing spondylitis. Clin Rheumatol, 32(7), 1007-1015.
Bodur, H., Ataman, S., Rezvani, A., Bugdayci, D. S., Cevik, R., Birtane, M.,
Akinci, A., Altay, Z., Gunaydin, R., Yener, M., Kocyigit, H., Duruoz, T.,
Yazgan, P., Cakar, E., Aydin, G., Hepguler, S., Altan, L., Kirnap, M.,
Olmez, N., Soydemir, R., Kozanoglu, E., Bal, A., Sivrioglu, K., Karkucak,
M., & Gunendi, Z. (2011). Quality of life and related variables in patients
with ankylosing spondylitis. Qual Life Res, 20(4), 543-549.
Braun, J., van den Berg, R., Baraliakos, X., Boehm, H., Burgos-Vargas, R.,
Collantes-Estevez, E., Dagfinrud, H., Dijkmans, B., Dougados, M.,
Emery, P., Geher, P., Hammoudeh, M., Inman, R. D., Jongkees, M.,
Khan, M. A., Kiltz, U., Kvien, T., Leirisalo-Repo, M., Maksymowych, W.
P., Olivieri, I., Pavelka, K., Sieper, J., Stanislawska-Biernat, E.,
Wendling, D., Ozgocmen, S., van Drogen, C., van Royen, B., & van der
Heijde, D. (2011). 2010 update of the ASAS/EULAR recommendations
for the management of ankylosing spondylitis. Ann Rheum Dis, 70(6),
896-904.
Claudepierre, P., Flipo, R. M., Sibilia, J., Berthelot, J. M., Goupille, P.,
Cortinovis, S., Cunin, P., Chevalier, X., & Wendling, D. (2004). Patient
knowledge of their disease: a French multicenter study in ankylosing
spondylitis. Joint Bone Spine, 71(6), 550-556.
E. Lubrano, P. H., P. Moreno, B. Griffiths, P. Emery and D. Veale. (1998). The
Assessment of Knowledge in Ankylosing Spondylitis Patients by a Self-
Administered Questionnaire. British Journal of Rheumatology(37), 437–
441.
F. Jennings, S. T., M.R. de Assis, J. Natour. (2006). Brazil Patient Knowledge
Questionnaire (PKQ) and evaluation of disease-specific knowledge in
patients with rheumatoid arthritis. Clin Exp Rheumatol., 24(5) 521-528.
Capítulo III. Estudos Originais
49
Ferreira, P. L. (2000a). Criação da versão portugues do MOS SF-36 Parte I -
Adaptação cultural e linguística. Acta Médica Portuguesa, 13, 55-66.
Ferreira, P. L. (2000b). Criação da versão portuguesa do MOS Parte II - Testes
de Validação. Acta médica Portuguesa, 13, 119-127.
Frauendorf, R., Medeiros Pinheiro, M. d., & Mesquita Ciconelli, R. (2013).
Variables related to work productivity loss in patients with ankylosing
spondylitis. Revista Brasileira de Reumatologia (English Edition), 53(3),
303-309.
Gyurcsik, Z. N., Andras, A., Bodnar, N., Szekanecz, Z., & Szanto, S. (2012).
Improvement in pain intensity, spine stiffness, and mobility during a
controlled individualized physiotherapy program in ankylosing spondylitis.
Rheumatol Int, 32(12), 3931-3936.
Hennell, S. L., Brownsell, C., & Dawson, J. K. (2004). Development, validation
and use of a patient knowledge questionnaire (PKQ) for patients with
early rheumatoid arthritis. Rheumatology, 43(4), 467-471.
Marcelo Cardozo de Souza, A. O., AnaMaria Jones, Fábio Jennings, Elisabeth
Biruel. (2012). Grupos educacionais para pacientes com espondilite
anquilosante: revisão sistemática. Revista Dor, 13 (3), 256-260.
Milton Severo, R. G., Raquel lucas, Henrique Barros (2010). Assessment of the
general public´s Knowledge about rheumatic diseases: evidence from a
Protuguese population-based survey. BMC Musculosketal Disorders,
11:211.
Passalent, L. A. (2011). Physiotherapy for ankylosing spondylitis: evidence and
application. Curr Opin Rheumatol, 23(2), 142-147.
Ramada-Rodilla, J. M., Serra-Pujadas, C., & Delclós-Clanchet, G. L. (2013).
Adaptación cultural y validación de cuestionarios de salud: revisión y
recomendaciones metodológicas. Salud Pública de México, 55, 57-66.
Ramos-Remus C, S.-R. A., Prieto-Parra RE, Galvan-Villegas F: . (2000). <How
important is patient education?.pdf>. Baillieres Best Pract Res Clin
Rheumatol, 14(4), 689-703

Capítulo III. Estudos Originais
50
Rat, A.-C. (2013). Efficacité de l’éducation thérapeutique du patient dans les
rhumatismes inflammatoires : quelles preuves ? Revue du Rhumatisme
Monographies, 80(3), 170-173.
Reveille, J. D., Ximenes, A., & Ward, M. M. (2012). Economic considerations of
the treatment of ankylosing spondylitis. Am J Med Sci, 343(5), 371-374.
Roxanne Cooksey, S. B., Muhammad Jmai Husain, Elizabeth Irvine, Helen
Davies, Stefan Siebert. (2012). The information needs of people living
with ankylosing spondylitis: a questionnaire survey. BMC Musculosketal
Disorders, 13, 243.
Yigit, S., Sahin, Z., Demir, S. E., & Aytac, D. H. (2013). Home-based exercise
therapy in ankylosing spondylitis: short-term prospective study in patients
receiving tumor necrosis factor alpha inhibitors. Rheumatol Int, 33(1), 71-
77.
Younes, M., Jalled, A., Aydi, Z., Zrour, S., Korbaa, W., Ben Salah, Z., Letaief,
M., Bejia, I., Touzi, M., & Bergaoui, N. (2010). Socioeconomic impact of
ankylosing spondylitis in Tunisia. Joint Bone Spine, 77(1), 41-46.

Estudo III
The relation between functional parameters and C-Reactive Protein,
Erythrocyte Sedimentation Race in Ankylosing Spondylitis: a cross
sectional study
Sofia Lopes1,2; Anabela Moreira 1; Ana Daniela Simões 2; José Alberto Duarte3;
Cristina Mesquita1
1 Escola Superior de Saúde, Politécnico do Porto
2 Escola Superior de Saúde de Vale do Sousa, CESPU
3 Faculdade de Desporto, Universidade do Porto
Submetido para publicação em Rheumatology International
_____________________________________________________

Capítulo III. Estudos Originais
53
Sofia Manuela da Rocha Lopes, Escola Superior de Saúde (School of Health Allied
Sciences), Polytechnic Institute of Porto, Rua Dr. António Bernardino de Almeida nº
400, 4200-072 Porto, Portugal, Tel.: +351 222 061 000, e-mail: [email protected] and
Escola Superior de Saúde de Vale do Sousa, Instituto Politécnico de Saúde do Norte,
Rua Central de Gandra nº 1317, 4585-116 Gandra – Paredes, Portugal, Tel.:
+351 224 157100, e-mail: [email protected], [email protected]
Anabela Moreira, Escola Superior de Saúde (School of Health Allied Sciences),
Polytechnic Institute of Porto, Rua Dr. António Bernardino de Almeida nº 400, 4200-
072 Porto, Portugal, Tel.: +351 222 061 000, e-mail: [email protected]
Ana Daniela Gomes Araújo Simões, Escola Superior de Saúde de Vale do Sousa,
Instituto Politécnico de Saúde do Norte, Rua Central de Gandra nº 1317, 4585-116
Gandra – Paredes, Portugal, Tel.: +351 224 157 100, e-mail:
José Alberto Duarte, Faculty of Sport, University of Porto, Rua Dr. Plácido Costa, 91 -
4200,450 Porto, Portugal, Tel.: +351 220 425 200, e-mail: [email protected]
Cristina Teresa Torrão Carvalho Mesquita, Escola Superior de Saúde (School of
Health Allied Sciences), Polytechnic Institute of Porto, Rua Valente Perfeito, 322, 4400-
330 Vila Nova de Gaia, Portugal, Tel.: +351 222061000, e-mail: [email protected]
Capítulo III. Estudos Originais
54
Abstract
Introduction: Ankylosing spondylitis (AS) is a chronic inflammatory rheumatic
disease characterised by inflammation of the spine and the sacroiliac joints and
stiffness, which leads to a progressive decline in the quality of life of individuals.
Bath indices are considered the principal functional outcome measure and
Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP) are the
most widely used biomarkers in AS to assess disease activity.
Objective: To characterise individuals with AS and to examine the association
between functional parameters and biomarkers.
Methods: Thirty-one patients were recruited from the National Association of
Ankylosing Spondylitis (ANEA) – Centre of northern region of Portugal, between
February 2014 and June 2015, to be included in the present study. The Bath
indices [Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath
Ankylosing Spondylitis Functional Index (BASFI) and Bath Ankylosing
Spondylitis Metrology Index (BASMI)], the Neck Disability Index (NDI), the
Oswestry Disability Index (ODI) and laboratory parameters such as ESR and
CRP were analysed.
Results: The participants’ mean age was 42.77 (±14.37) years, with 18 (58.1%)
women and 13 (41.9%) men. The mean scores were 3.55 (BASDAI), 2.78
(BASFI) and 2.58 (BASMI). The final mean scores were 25.81± 18.36 (NDI) and
23.29±15.32 (ODI). We found a negative association between ESR and
BASDAI (β=-0.038, p=0.025), and between ESR and BASFI (β=-0.044,
p=0.013). As to CRP, there was no statistically significant association between
Bath indices.
Conclusion: This cross-sectional study in AS patients demonstrated that, on
the one hand, this sample had a high education level, having been diagnosed
with AS for more than 15 years, with a moderate disability and, on the other
hand, with the adjustment of education level and years since diagnosis, there
was an association between ESR and BASDAI and BASFI scores.
Keywords: Ankylosing spondylitis, functionality, biomarkers, inflammation,
pain.
Capítulo III. Estudos Originais
55
Introduction
Ankylosing spondylitis (AS) is a chronic rheumatic disease, characterised
by inflammation of the spine, the sacroiliac joints and stiffness, which can lead
to a progressive decrease in the quality of life (Braun & Sieper, 2007; O'Dwyer
et al., 2015).
Disease activity, functionality and symptoms are great impact areas in
AS (Jane Zochling et al., 2006). Pain, stiffness, fatigue and spinal mobility are
symptoms which reflect the disease’s inflammatory effect (Jane Zochling et al.,
2006). As a consequence, the irreversible changes that accompany AS, the
decreased functionality in activities of daily living, the direct and indirect costs
associated with the disease and its effect on patients’ quality of life are
important parameters to take into account in the clinical practice to achieve a
good diagnosis and an adequate intervention (Braun & Sieper, 2007). The
socioeconomic impact of AS is substantial, considering the reduced working
hours, occasional work changes/adaptations, missed professional opportunities
and early retirement. On the other hand, it has been reported that a higher
educational level is associated with maintenance in the labour force, decreased
years since AS diagnosis, a higher socioeconomic level and a better
understanding of the disease (Frauendorf et al., 2013; Younes et al., 2010).
The most commonly used biomarkers to monitor AS activity are
Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP) (de Vlam,
2010). These parameters are usually high in AS, in association with lumbar and
cervical pain, as inflammation and entheses in these regions are the first
symptoms of the disease (Kaya et al., 2007). However, there is some issue as
to the sensitivity of these inflammatory biomarkers in AS activity and their
correlation with functional parameters (de Vlam, 2010; de Vries et al., 2009).
The basis for this controversy is the assessment of their specificity regarding
AS, as these biomarkers are specific to assess the inflammation in structures
affected by the disease, such as tendons, bone, ligaments, cartilage, among
others, but are also influenced by non-inflammatory aspects, such as age,
gender, anaemia and renal failure, which can influence these laboratory
parameters (de Vlam, 2010; Kisacik et al., 2008). Their correlation with
Capítulo III. Estudos Originais
56
functional parameters has been more evident in the assessment of disease
activity (BASDAI) (de Vries et al., 2009). However, to achieve a deeper and
more specific understanding of the disease it is necessary to include functional
(BASFI), metric (BASMI) and disease activity (BASDAI) parameters in the
assessment of an individual with AS, as these are the preferred methods to
evaluate individuals with AS (Braun & Sieper, 2007; de Vlam, 2010; Pimentel-
Santos, Mourao, et al., 2012; Sieper et al., 2009).
Equally important, given the complexity of this chronic disease, in
particular the ankylosis of some segments of the spine, is to explore the
assessment of more specific parameters associated with the impact of spinal
mobility (cervical and lumbar regions) on activities of daily living. (Robinson et
al., 2013). The characterisation of AS individuals in the literature is still scarce.
For this reason, it is important to enhance knowledge regarding functional and
biomarker parameters, improving the orientation of health professionals in the
management of this disease and in providing patient advice. The aims of this
study were: (1) to characterise individuals with AS and (2) to verify the
association between functional joint and biomarker parameters.
Methods
Study design and participants
A cross-sectional study with a convenience sample of patients with AS
was conducted in the northern region of Portugal. The study received approval
from the Ethics Committee of the School of Health Allied Sciences of the
Polytechnic Institute of Porto. Potential candidates were identified by
physiotherapists from the institution and from the National Association of
Ankylosing Spondylitis (ANEA) – Centre of northern region of Portugal, and the
recruitment occurred between February 2014 and June 2015.
Subjects were eligible to participate in the study if they: (1) were
diagnosed with AS according to the modified New York criteria (Pimentel-
Santos, Mourao, et al., 2012); (2) were aged 18 years or older and (Pimentel-
Santos, Mourao, et al., 2012); (3) voluntarily consented to participate. The study
excluded all patients presenting any other clinically diagnosed
Capítulo III. Estudos Originais
57
spondyloarthropathy, neurological or cardiorespiratory pathologies (Pimentel-
Santos, Mourao, et al., 2012).
Instruments
All patients completed the Portuguese version of the Bath Spondylitis
Functional Index (BASFI) (Pimentel-Santos, Pinto, et al., 2012), a
characterisation questionnaire which measures the functional status of patients
with AS through ten questions regarding daily activities, with the mean score
(range, 0–10) being obtained from the sum of all values.
The Portuguese version of the Bath Spondylitis Metrics Index (BASMI)
(Pimentel-Santos, Pinto, et al., 2012) was used to determine the participants’
physical mobility, with the Shober’s test, lateral spine flexion, tragus to wall
distance, cervical rotation and intermalleolar distance, with a final score ranging
from 0 to 2 in each one of the five parameters (0 – mild disease involvement, 1
– moderate disease involvement, 2 – severe disease involvement).
The Portuguese version of the Bath Spondylitis Disease Activity Index
(BASDAI) (Pimentel-Santos, Pinto, et al., 2012) was used to measure the
disease activity status through six questions with a score ranging from 0 to 10,
regarding fatigue, spinal pain, peripheral joint, entheses and morning stiffness,
to determine a final mean score. A mean of the two scores relating to morning
stiffness was calculated before averaging all the answers (A. Calin, 1999;
Pimentel-Santos, Pinto, et al., 2012).
The Portuguese version of the Oswestry Disability Index (ODI) was used
in each of its ten items, each of them including 6 statements, and patients were
requested to select only one, obtaining a score from 0 to 5. The Portuguese
version of the Neck Disability Index (NDI) also includes 6 statements and the
score 0-5. ODI and NDI total scores were converted into a percentage score
with 0-20% indicating minimal disability, 21-40% moderate disability, 41-60%
severe disability, 61-80% crippled and 81-100% total incapacitation (Beattie &
Maher, 1997; Fairbank, 1980; Vernon, 2008). Disease activity variables used
included both C-Reactive Protein (CRP) and Erythrocyte Sedimentation Rate
(ESR).
Capítulo III. Estudos Originais
58
Data collection procedures
Aspects such as age, gender, level of education and employment
situation were identified as sociodemographic and anthropometric. Physical
examination of patients by a blind trained observer included the assessment of
BASMI. Patients have completed two self-administered questionnaires – the
NDI and the ODI.
As laboratory assessments of patients’ ESR and CRP were determined,
overnight fasting blood samples from all subjects were collected through
standard antecubital forearm venepuncture to 8 ml serum-separator and 3.5 ml
K2-EDTA tubes (BD Vacutainer® System, BD Diagnostics, Franklin Lakes, NJ).
After room temperature clotting, serum was separated by low speed
centrifugation (4500 rpm, 10 min, 22°C) (Sigma ® 3k15, SIGMA
Laborzentrifugen GmbH, Osterode am Harz, Germany), transferred into
aliquots, and stored at -80°C until analysis ("Third Report of the National
Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation,
and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III)
Final Report", 2002) and latex immunoturbidimetry (CRP) (Roberts et al., 2001)
techniques.
For ESR estimation, K2-EDTA anticoagulated blood samples were mixed
for 10 minutes before the test. Samples were aspirated into a Westergren
pipette and the distance that the column of blood fell in 1h was recorded
according to the International Council for Standardisation in Haematology
(ICSH) standardised method (Jou et al., 2011).
Data analysis
Sample characteristics are presented as counts and proportions for
categorical variables and as mean ± standard deviation (SD) for biomarkers and
functional parameters. The association between biomarkers and functional
parameters was estimated through crude regression coefficients and years
since diagnosis and education level-adjusted regression coefficients (β and
adjβ). Since the regression prerequisites were not achieved when analysing the
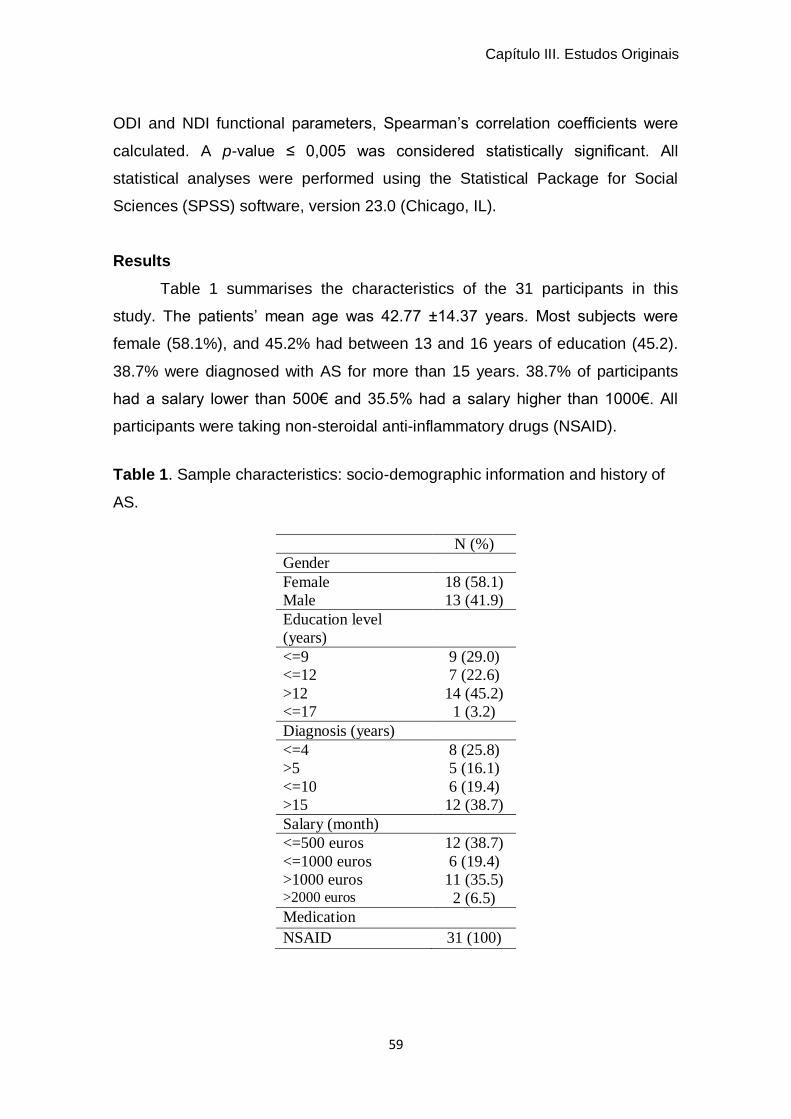
Capítulo III. Estudos Originais
59
ODI and NDI functional parameters, Spearman’s correlation coefficients were
calculated. A p-value ≤ 0,005 was considered statistically significant. All
statistical analyses were performed using the Statistical Package for Social
Sciences (SPSS) software, version 23.0 (Chicago, IL).
Results
Table 1 summarises the characteristics of the 31 participants in this
study. The patients’ mean age was 42.77 ±14.37 years. Most subjects were
female (58.1%), and 45.2% had between 13 and 16 years of education (45.2).
38.7% were diagnosed with AS for more than 15 years. 38.7% of participants
had a salary lower than 500€ and 35.5% had a salary higher than 1000€. All
participants were taking non-steroidal anti-inflammatory drugs (NSAID).
Table 1. Sample characteristics: socio-demographic information and history of
AS.
N (%)
Gender
Female 18 (58.1)
Male 13 (41.9)
Education level
(years)
<=9 9 (29.0)
<=12 7 (22.6)
>12
<=17
14 (45.2)
1 (3.2)
Diagnosis (years)
<=4 8 (25.8)
>5
<=10
>15
5 (16.1)
6 (19.4)
12 (38.7)
Salary (month)
<=500 euros 12 (38.7)
<=1000 euros
>1000 euros >2000 euros
6 (19.4)
11 (35.5)
2 (6.5)
Medication
NSAID 31 (100)
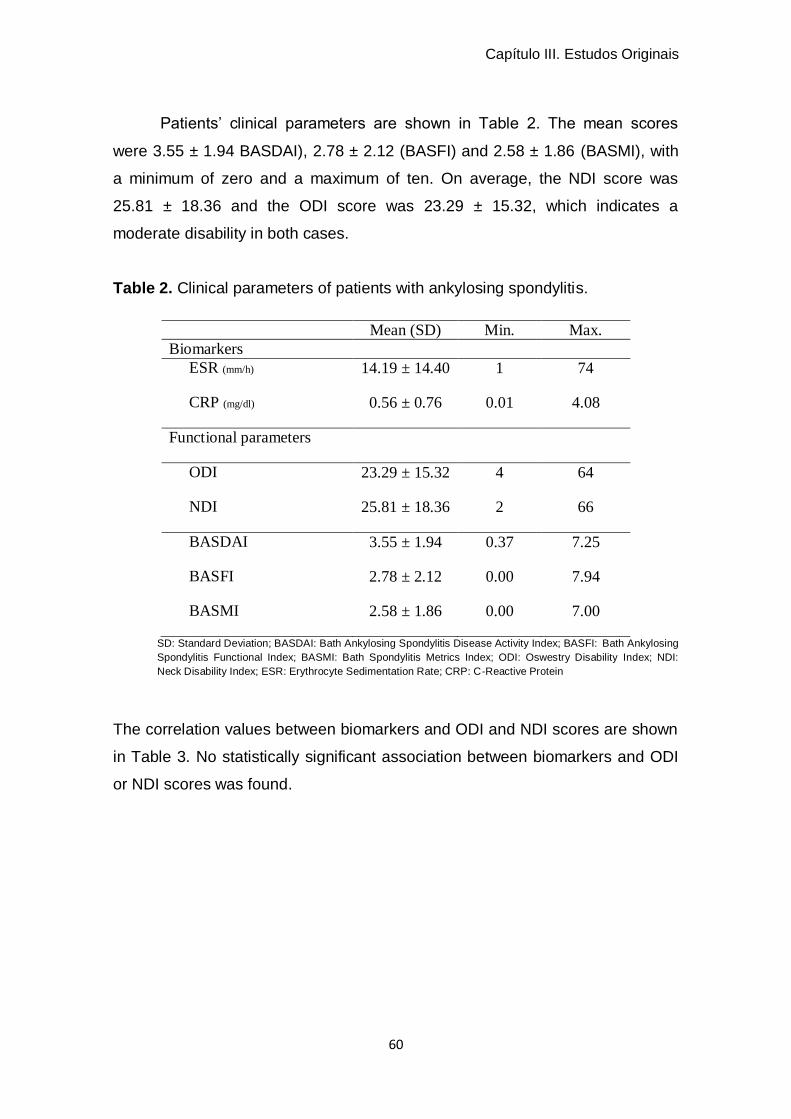
Capítulo III. Estudos Originais
60
Patients’ clinical parameters are shown in Table 2. The mean scores
were 3.55 ± 1.94 BASDAI), 2.78 ± 2.12 (BASFI) and 2.58 ± 1.86 (BASMI), with
a minimum of zero and a maximum of ten. On average, the NDI score was
25.81 ± 18.36 and the ODI score was 23.29 ± 15.32, which indicates a
moderate disability in both cases.
Table 2. Clinical parameters of patients with ankylosing spondylitis.
Mean (SD) Min. Max.
Biomarkers
ESR (mm/h) 14.19 ± 14.40 1 74
CRP (mg/dl) 0.56 ± 0.76 0.01 4.08
Functional parameters
ODI 23.29 ± 15.32 4 64
NDI 25.81 ± 18.36 2 66
BASDAI 3.55 ± 1.94 0.37 7.25
BASFI 2.78 ± 2.12 0.00 7.94
BASMI 2.58 ± 1.86 0.00 7.00
SD: Standard Deviation; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; BASFI: Bath Ankylosing
Spondylitis Functional Index; BASMI: Bath Spondylitis Metrics Index; ODI: Oswestry Disability Index; NDI:
Neck Disability Index; ESR: Erythrocyte Sedimentation Rate; CRP: C-Reactive Protein
The correlation values between biomarkers and ODI and NDI scores are shown
in Table 3. No statistically significant association between biomarkers and ODI
or NDI scores was found.
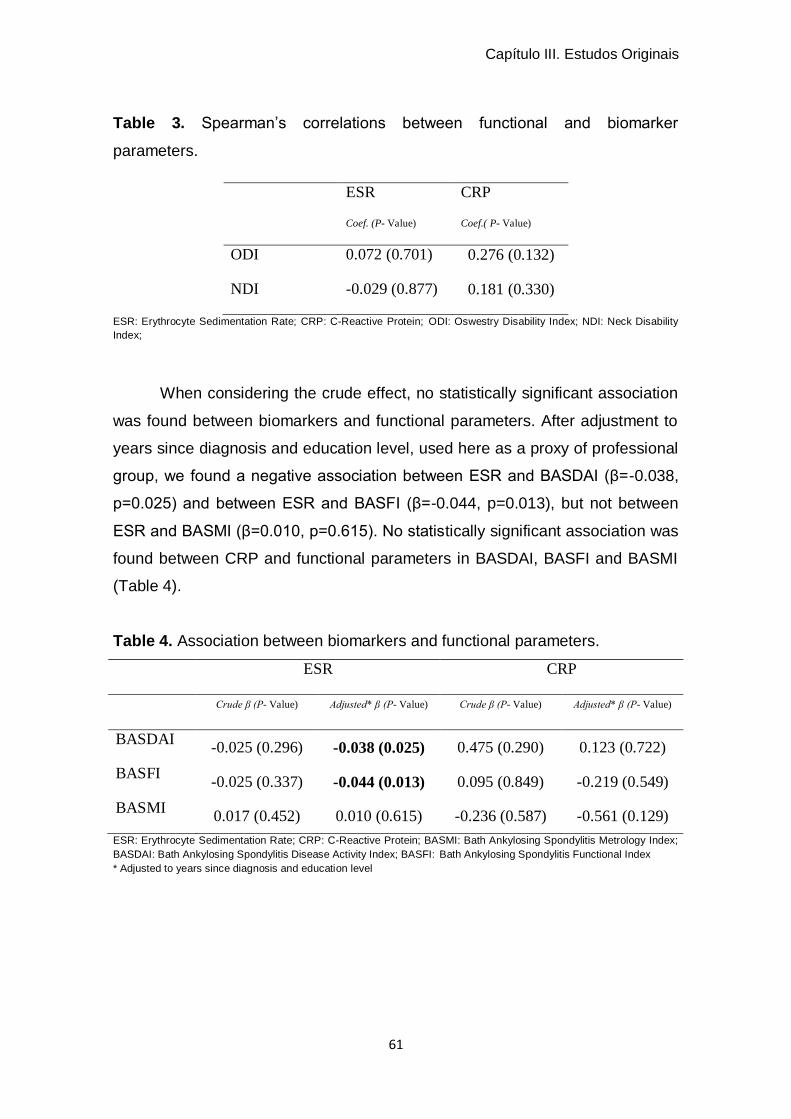
Capítulo III. Estudos Originais
61
Table 3. Spearman’s correlations between functional and biomarker
parameters.
ESR
Coef. (P- Value)
CRP
Coef.( P- Value)
ODI 0.072 (0.701) 0.276 (0.132)
NDI -0.029 (0.877) 0.181 (0.330)
ESR: Erythrocyte Sedimentation Rate; CRP: C-Reactive Protein; ODI: Oswestry Disability Index; NDI: Neck Disability
Index;
When considering the crude effect, no statistically significant association
was found between biomarkers and functional parameters. After adjustment to
years since diagnosis and education level, used here as a proxy of professional
group, we found a negative association between ESR and BASDAI (β=-0.038,
p=0.025) and between ESR and BASFI (β=-0.044, p=0.013), but not between
ESR and BASMI (β=0.010, p=0.615). No statistically significant association was
found between CRP and functional parameters in BASDAI, BASFI and BASMI
(Table 4).
Table 4. Association between biomarkers and functional parameters.
ESR CRP
Crude β (P- Value) Adjusted* β (P- Value) Crude β (P- Value) Adjusted* β (P- Value)
BASDAI -0.025 (0.296) -0.038 (0.025) 0.475 (0.290) 0.123 (0.722)
BASFI -0.025 (0.337) -0.044 (0.013) 0.095 (0.849) -0.219 (0.549)
BASMI 0.017 (0.452) 0.010 (0.615) -0.236 (0.587) -0.561 (0.129)
ESR: Erythrocyte Sedimentation Rate; CRP: C-Reactive Protein; BASMI: Bath Ankylosing Spondylitis Metrology Index; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; BASFI: Bath Ankylosing Spondylitis Functional Index
* Adjusted to years since diagnosis and education level
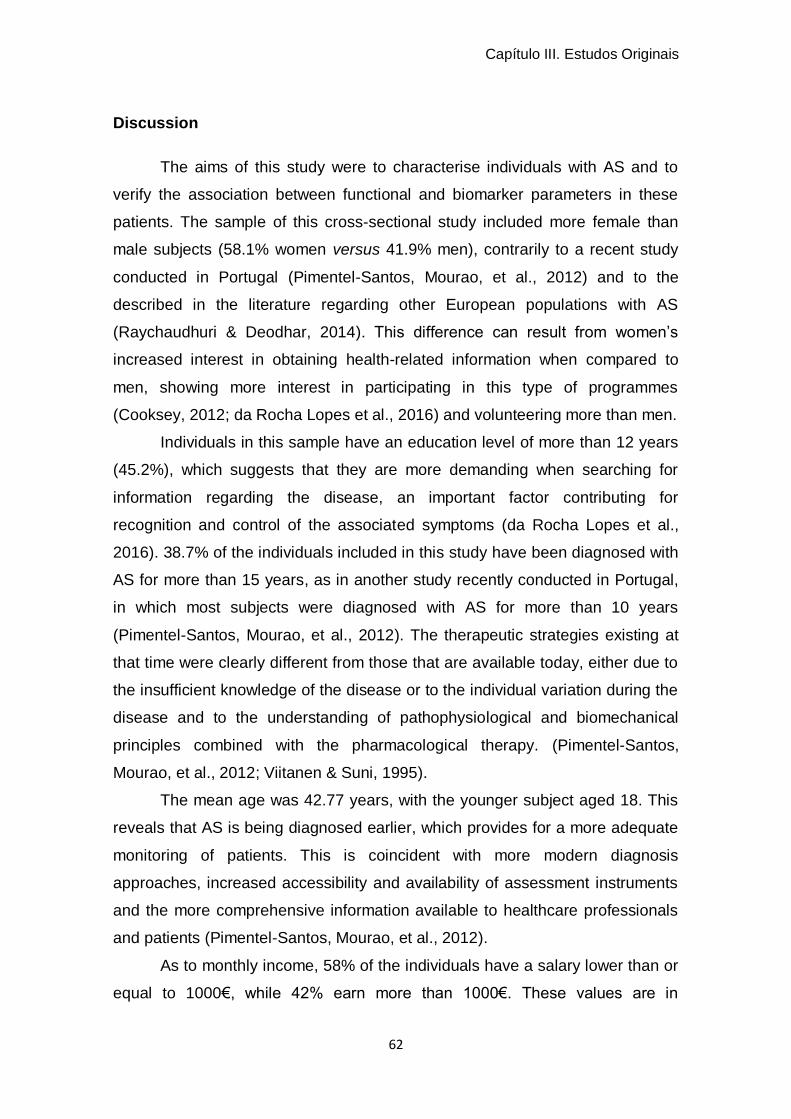
Capítulo III. Estudos Originais
62
Discussion
The aims of this study were to characterise individuals with AS and to
verify the association between functional and biomarker parameters in these
patients. The sample of this cross-sectional study included more female than
male subjects (58.1% women versus 41.9% men), contrarily to a recent study
conducted in Portugal (Pimentel-Santos, Mourao, et al., 2012) and to the
described in the literature regarding other European populations with AS
(Raychaudhuri & Deodhar, 2014). This difference can result from women’s
increased interest in obtaining health-related information when compared to
men, showing more interest in participating in this type of programmes
(Cooksey, 2012; da Rocha Lopes et al., 2016) and volunteering more than men.
Individuals in this sample have an education level of more than 12 years
(45.2%), which suggests that they are more demanding when searching for
information regarding the disease, an important factor contributing for
recognition and control of the associated symptoms (da Rocha Lopes et al.,
2016). 38.7% of the individuals included in this study have been diagnosed with
AS for more than 15 years, as in another study recently conducted in Portugal,
in which most subjects were diagnosed with AS for more than 10 years
(Pimentel-Santos, Mourao, et al., 2012). The therapeutic strategies existing at
that time were clearly different from those that are available today, either due to
the insufficient knowledge of the disease or to the individual variation during the
disease and to the understanding of pathophysiological and biomechanical
principles combined with the pharmacological therapy. (Pimentel-Santos,
Mourao, et al., 2012; Viitanen & Suni, 1995).
The mean age was 42.77 years, with the younger subject aged 18. This
reveals that AS is being diagnosed earlier, which provides for a more adequate
monitoring of patients. This is coincident with more modern diagnosis
approaches, increased accessibility and availability of assessment instruments
and the more comprehensive information available to healthcare professionals
and patients (Pimentel-Santos, Mourao, et al., 2012).
As to monthly income, 58% of the individuals have a salary lower than or
equal to 1000€, while 42% earn more than 1000€. These values are in
Capítulo III. Estudos Originais
63
accordance with the sample’s education level and another recent Portuguese
study (da Rocha Lopes et al., 2016).
The sample’s mean BASDAI (3.55±1.94), BASFI (2.78±2.12) and BASMI
(2.58±1.86) scores show that these individuals are between percentiles 25 and
50 for the Portuguese population, taking the disease’s evolution in years into
account (Pimentel-Santos, Mourao, et al., 2012). These values are similar to
those obtained in previous cross-sectional studies, with similar values as to the
education level, years since diagnosis and medication intake, although with a
higher sample (Berg et al., 2014; Bodur et al., 2011; Konca et al., 2012). It
should be noted that NDI mean scores in this sample were higher (25.8 ±18.36)
than ODI scores (23.29±15.32), although all of them are in the same interval,
revealing an increased mean score of cervical disability compared to lumbar
disability, as opposed to the described in the literature, which reports that the
latter is the most affected segment (El Tecle et al., 2015). This evidence can be
due to the female predominance of the sample, as women are more commonly
affected at the cervical segment than at the lumbar segment, as opposed to
men. (El Maghraoui et al., 2003; Ortega Castro et al., 2013). On the other hand,
our results show that both segments have mean scores situated in the interval
21-40, which means a moderate disability, in accordance with the Bath indices’
scores (BASDAI, BASMI and BASFI), taking into account the percentiles for the
Portuguese population with AS (Pimentel-Santos, Mourao, et al., 2012).
As to ESR and CRP parameters, several studies have been reporting
that these biomarkers have no predictive value to determine disease activity in
individuals with AS (Braun & Sieper, 2007; de Vlam, 2010; Kaya et al., 2007;
Kisacik et al., 2008). Our results show low ESR and CRP values, suggesting
that individuals in our sample have low disease activity. This can be due to the
fact that all individuals take anti-inflammatory medication, which can influence
these biomarkers (Plasqui et al., 2012), or to the fact that most subjects were
diagnosed with AS for more than 12 years, having an increased knowledge and
control of the disease. Patients who have been diagnosed for more years have
an increased need of information than recently diagnosed individuals, which
provides a safer management of the disease (Cooksey, 2012).
Capítulo III. Estudos Originais
64
It has been verified that when values were adjusted for years since
diagnosis and education levels, there was an association between ESR and
BASDAI and BASFI scores. As ESR levels increase, BASDAI scores also
increase, deteriorating these individuals’ functionality; in the same way, when
ESR values increase, BASFI scores also increase, which translates into higher
disease activity. This can be explained by disease duration/evolution because
of the progressive activation of bone reparative/remodelling pathways that are
likely to affect these biomarkers (Braem & Lories, 2012; Maksymowych, 2012).
As concerns the education level, it influences functionality and disease activity
by the knowledge these individuals have regarding the disease (Song et al.,
2015), although there is no association between this parameter and BASMI
scores. As to CRP, there was no association between Bath indices, possibly
because this biomarker is more sensitive in inflammation detection and is not
increased by the influence of age, sex or anaemia. As this biomarker values
were low in individuals of this sample, no association was found with the Bath
indices (Krzysztof Bochen & Dzida, 2011).
Both cervical and lumbar vertebral mobility and the inflammation of these
segments are dynamic processes which vary in time and with time. This
inflammation is a non-linear process, which improves, deteriorates and even
disappears throughout time, which makes that its assessment using biomarker
parameters is a point estimation, as they are sensitive to changes (de Vlam,
2010).
Our results also show that the NDI and ODI present a low association
with the biomarker parameters. These findings may be explained by the number
of years of disease evolution of patients participating in this study, which has
somehow provided for adaptations to perform activities of daily living,
decreasing the impact of chronic pain in the cervical and lumbar segments.
These results have implications for healthcare professionals dealing directly
with patients with AS, as they would allow to better understand and monitor
these individuals.
Our study has some limitations, such as the reduced number of
individuals who constitute our sample and the fact that it is a convenience
Capítulo III. Estudos Originais
65
sample. A second limitation in result analysis was that it was not possible to
adjust the years since diagnosis and the education level for NDI and ODI
scores, as these parameters do not meet the requirements for that analysis. For
these reasons, additional studies with a bigger sample using these two
instruments (NDI and ODI), together with additional objective parameters such
as imaging examinations, for their sensitivity to detect active inflammation, are
required for correlation with biomarkers.
Conclusion
Individuals with AS included in this study have a high education level, an
aspect which is in accordance with their monthly income, a disease evolution of
at least 15 years and a moderate functional disability.
Our results show a negative association between ESR and BASDAI and
BASFI scores.
Bibliography
A. Calin, J.-P. N., A. Gueguen, H. Zeidler, H. Mielants and M. Dougados.
(1999). A new approach to defining functional ability in ankylosing
spondylitis: the development of the Bath Ankylosing Spondylitis
Functional Index. Rheumatology, 38(9), 878-882.
Beattie, P., & Maher, C. (1997). The role of functional status questionnaires for
low back pain. Australian Journal of Physiotherapy, 43(1), 29-38.
Berg, I. J., Semb, A. G., van der Heijde, D., Kvien, T. K., Hisdal, J., Olsen, I. C.,
Dagfinrud, H., & Provan, S. A. (2014). Uveitis is associated with
hypertension and atherosclerosis in patients with ankylosing spondylitis:
a cross-sectional study. Semin Arthritis Rheum, 44(3), 309-313.
Bodur, H., Ataman, S., Rezvani, A., Bugdayci, D. S., Cevik, R., Birtane, M.,
Akinci, A., Altay, Z., Gunaydin, R., Yener, M., Kocyigit, H., Duruoz, T.,
Yazgan, P., Cakar, E., Aydin, G., Hepguler, S., Altan, L., Kirnap, M.,
Olmez, N., Soydemir, R., Kozanoglu, E., Bal, A., Sivrioglu, K., Karkucak,
Capítulo III. Estudos Originais
66
M., & Gunendi, Z. (2011). Quality of life and related variables in patients
with ankylosing spondylitis. Qual Life Res, 20(4), 543-549.
Braem, K., & Lories, R. J. (2012). Insights into the pathophysiology of
ankylosing spondylitis: contributions from animal models. Joint Bone
Spine, 79(3), 243-248.
Braun, J., & Sieper, J. (2007). Ankylosing spondylitis. The Lancet, 369(9570),
1379-1390.
Cooksey, R. B., S.; Husain, M.; I. Elizabeth, Davies,H. and Siebert, S. (2012).
The information needs of people living with ankylosing spondylitis: a
questionnaire survey. BMC Musculosketal Disorders, 13, 243.
da Rocha Lopes, S. M., Duarte, J. A., & Mesquita, C. T. (2016). Cross-cultural
adaptation and validation of the Portuguese version of "The assessment
of knowledge in ankylosing spondylitis patients by a self-administered
questionnaire". Rheumatol Int.
de Vlam, K. (2010). Soluble and tissue biomarkers in ankylosing spondylitis.
Best Pract Res Clin Rheumatol, 24(5), 671-682.
de Vries, M. K., van Eijk, I. C., van der Horst-Bruinsma, I. E., Peters, M. J.,
Nurmohamed, M. T., Dijkmans, B. A., Hazenberg, B. P., & Wolbink, G. J.
(2009). Erythrocyte sedimentation rate, C-reactive protein level, and
serum amyloid a protein for patient selection and monitoring of anti-tumor
necrosis factor treatment in ankylosing spondylitis. Arthritis Rheum,
61(11), 1484-1490.
El Maghraoui, A., Bensabbah, R., Bahiri, R., Bezza, A., Guedira, N., & Hajjaj-
Hassouni, N. (2003). Cervical spine involvement in ankylosing
spondylitis. Clin Rheumatol, 22(2), 94-98.
El Tecle, N. E., Abode-Iyamah, K. O., Hitchon, P. W., & Dahdaleh, N. S. (2015).
Management of spinal fractures in patients with ankylosing spondylitis.
Clin Neurol Neurosurg, 139, 177-182.
Fairbank, J. C., Couper, J., Davies, J.B., & O'Brien, J.P. (1980). The Oswestry
low back pain disability questionnaire. Physiotherapy, 66, 271-273.
Frauendorf, R., Medeiros Pinheiro, M. d., & Mesquita Ciconelli, R. (2013).
Variables related to work productivity loss in patients with ankylosing
Capítulo III. Estudos Originais
67
spondylitis. Revista Brasileira de Reumatologia (English Edition), 53(3),
303-309.
Jane Zochling, Jürgen Braun, & Désirée van der Heijde, D. (2006).
Assessments in ankylosing spondylitis. Best Pract Res Clin Rheumatol,
20(3), 521-537.
Jou, J. M., Lewis, S. M., Briggs, C., Lee, S. H., De La Salle, B., McFadden, S.,
& For The International Council For Standardization In, H. (2011). ICSH
review of the measurement of the erythocyte sedimentation rate.
International Journal of Laboratory Hematology, 33(2), 125-132.
Kaya, T., Bal, S., & Gunaydin, R. (2007). Relationship between the severity of
enthesitis and clinical and laboratory parameters in patients with
ankylosing spondylitis. Rheumatol Int, 27(4), 323-327.
Kisacik, B., Tufan, A., Kalyoncu, U., Karadag, O., Akdogan, A., Ozturk, M. A.,
Kiraz, S., Ertenli, I., & Calguneri, M. (2008). Mean platelet volume (MPV)
as an inflammatory marker in ankylosing spondylitis and rheumatoid
arthritis. Joint Bone Spine, 75(3), 291-294.
Konca, S., Keskin, D., Ciliz, D., Bodur, H., & Sakman, B. (2012). Spinal
inflammation by magnetic resonance imaging in patients with ankylosing
spondylitis: association with disease activity and outcome parameters.
Rheumatol Int, 32(12), 3765-3770.
Krzysztof Bochen, A. K., Sylwia Milaniuk, Monika Kulczyńska, Andrzej
Prystupa,, & Dzida, G. (2011). Erythrocyte sedimentation rate - an old
marker with new applications. Journal of Pre-Clinical and Clinical
Research, Vol 5(2), 50-55.
Maksymowych, W. P. (2012). Biomarkers in spondyloarthritis: from
pathophysiology to disease assessment. Joint Bone Spine, 79(1), 4-6.
O'Dwyer, T., O'Shea, F., & Wilson, F. (2015). Decreased health-related physical
fitness in adults with ankylosing spondylitis: a cross-sectional controlled
study. Physiotherapy.
Ortega Castro, R., Font Ugalde, P., Castro Villegas, M. C., Calvo Gutiérrez, J.,
Muñoz Gomariz, E., Zarco Montejo, P., Almodóvar, R., Mulero Mendoza,
J., Torre-Alonso, J. C., Gratacós Masmitjá, J., Juanola Roura, X., Ariza
Capítulo III. Estudos Originais
68
Ariza, R., Fernández Dapica, P., Linares Ferrando, L. F., Brito Brito, M.
E., Cuende Quintana, E., Vázquez Galeano, C., Moreno Ramos, M. J.,
Giménez Úbeda, E., Rodríguez Lozano, J. C., Fernández Prada, M.,
Queiro Silva, R., Moreno Ruzafa, E., Júdez Navarro, E., Más, A. J.,
Medrano Le Quement, C., Ornilla, E., Montilla Morales, C., Pujol
Busquets, M., Clavaguera Poch, T., Fernández-Espartero, M. C.,
Carmona Ortell, L., & Collantes Estévez, E. (2013). Different Clinical
Expression of Patients With Ankylosing Spondylitis According to Gender
in Relation to Time Since Onset of Disease. Data From REGISPONSER.
Reumatología Clínica (English Edition), 9(4), 221-225.
Pimentel-Santos, F. M., Mourao, A. F., Ribeiro, C., Costa, J., Santos, H.,
Barcelos, A., Pinto, P., Godinho, F., Cruz, M., Vieira-Sousa, E., Santos,
R. A., Rabiais, S., Felix, J., Fonseca, J. E., Guedes-Pinto, H., Brown, M.
A., Branco, J. C., & Group, C. S. (2012). Spectrum of ankylosing
spondylitis in Portugal. Development of BASDAI, BASFI, BASMI and
mSASSS reference centile charts. Clin Rheumatol, 31(3), 447-454.
Pimentel-Santos, F. M., Pinto, T., Santos, H., Barcelos, A., Cunha, I., Branco, J.
C., & Ferreira, P. L. (2012). Portuguese version of the bath indexes for
ankylosing spondylitis patients: a cross-cultural adaptation and
validation. Clin Rheumatol, 31(2), 341-346.
Plasqui, G., Boonen, A., Geusens, P., Kroot, E. J., Starmans, M., & van der
Linden, S. (2012). Physical activity and body composition in patients with
ankylosing spondylitis. Arthritis Care Res (Hoboken), 64(1), 101-107.
Raychaudhuri, S. P., & Deodhar, A. (2014). The classification and diagnostic
criteria of ankylosing spondylitis. J Autoimmun, 48-49, 128-133.
Roberts, W. L., Moulton, L., Law, T. C., Farrow, G., Cooper-Anderson, M.,
Savory, J., & Rifai, N. (2001). Evaluation of Nine Automated High-
Sensitivity C-Reactive Protein Methods: Implications for Clinical and
Epidemiological Applications. Part 2. Clinical Chemistry, 47(3), 418-425.
Robinson, Y., Sanden, B., & Olerud, C. (2013). Increased occurrence of spinal
fractures related to ankylosing spondylitis: a prospective 22-year cohort
Capítulo III. Estudos Originais
69
study in 17,764 patients from a national registry in Sweden. Patient Saf
Surg, 7(1), 2.
Sieper, J., Rudwaleit, M., Baraliakos, X., Brandt, J., Braun, J., Burgos-Vargas,
R., Dougados, M., Hermann, K. G., Landewe, R., Maksymowych, W., &
van der Heijde, D. (2009). The Assessment of SpondyloArthritis
international Society (ASAS) handbook: a guide to assess
spondyloarthritis. Ann Rheum Dis, 68 Suppl 2, ii1-44.
Song, I. H., Brenneis, C., Hammel, L., Feldtkeller, E., Listing, J., Sieper, J., &
Rudwaleit, M. (2015). Ankylosing spondylitis self-help organisations - do
members differ from non-members? Joint Bone Spine.
Third Report of the National Cholesterol Education Program (NCEP) Expert
Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol
in Adults (Adult Treatment Panel III) Final Report. (2002). Circulation,
106(25), 3143.
Vernon, H. (2008). The Neck Disability Index: state-of-the-art, 1991-2008. J
Manipulative Physiol Ther, 31(7), 491-502.
Viitanen, J. V., & Suni, J. (1995). Management Principles of Physiotherapy in
Ankylosing Spondylitis — Which Treatments are Effective?
Physiotherapy, 81(6), 322-329.
Younes, M., Jalled, A., Aydi, Z., Zrour, S., Korbaa, W., Ben Salah, Z., Letaief,
M., Bejia, I., Touzi, M., & Bergaoui, N. (2010). Socioeconomic impact of
ankylosing spondylitis in Tunisia. Joint Bone Spine, 77(1), 41-46.


Estudo IV
Effects of group-based vs home-based exercise programs in
patients with ankylosing spondylitis
Sofia Lopes1,2; Anabela Moreira 1; Ana Daniela Simões 2; José Alberto Duarte 3;
Cristina Mesquita1
1 Escola Superior de Saúde, Politécnico do Porto
2 Escola Superior de Saúde de Vale do Sousa, CESPU
3 Faculdade de Desporto, Universidade do Porto
Submetido para publicação em International Journal of Rheumatic Diseases
_____________________________________________________

Capítulo III. Estudos Originais
73
Abstract
Introduction: Exercise programmes are an important component of standard
therapy for patients with ankylosing spondylitis. Exercise therapy is important to
reduce pain and stiffness, to prevent postural deformities, and to improve
mobility for maintaining function and global health.
Objective: To assess the effects of 6-month group-based vs home-based
exercise programmes in patients with ankylosing spondylitis on functional and
biomarker parameters.
Methods: Thirty one patients were recruited from the National Association of
Ankylosing Spondylitis (ANEA) – Centre of northern region of Portugal –
between February 2014 and June 2015, and were divided into three groups.
The group-based and home-based exercise groups included 12 individuals
each, while the control group was composed of 7 subjects. The BATH indices
[Bath Ankylosing Spondylitis Functional Index (BASFI), Bath Ankylosing
Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis
Capítulo III. Estudos Originais
74
Metrology Index (BASMI)] were used to assess functional capacity, disease
activity and physical mobility; the cervical and lumbar pain in daily life activities
was assessed using the Neck Disability Index (NDI) and the Oswestry Disability
Index (ODI), respectively; the biomarkers used were the Erythrocyte
Sedimentation Rate (ESR) and the C-Reactive Protein (CRP). All participants
were assessed at baseline and at the end of 6 months.
Results: There were no statistically significant differences in patients' baseline
characteristics between the three groups. At the end of 6 months, participants in
the group-based exercise group showed significant improvements in BASFI
(p=0.048) and BASMI (p=0.001) scores. In the home-based exercise group
there was a decrease in CRP scores (p=0.037). Individuals in the control group
decreased all Bath indexes and NDI scores.
Conclusion: The results of the present study show that a supervised exercise
programme improves physical mobility and functional status. However, no
changes as to the biomarker parameters were observed at the end of 6 months.
Keywords: Disease activity, functionality, biomarkers, physiotherapy.
Capítulo III. Estudos Originais
75
Introduction
Ankylosing spondylitis (AS) is a disease that affects young adults, being
more frequent in men than in women. It is characterised by pain, stiffness and
impairment of the spinal mobility, associated with other axial skeleton
inflammations such as peripheral arthritis, entheses, uveitis and affecting other
organs (Braun & Sieper, 2007). All these signs and symptoms affect negatively
patients’ functionality and quality of life (Yigit et al., 2013).
AS standard management consists of a combination of pharmacological
therapy such as the administration of non-steroidal anti-inflammatory drugs, and
non-pharmacological treatment such as physical therapy, with the adoption of
specific and structured exercise programmes (Aytekin et al., 2012; Braun &
Sieper, 2007; Karapolat et al., 2008; Lim et al., 2005; Passalent, 2011).
Physical therapy has a crucial role in the management and increase of joint
mobility, in the prevention of joint deformities, in strength and in the physical
condition and coordination of individuals with AS (Aytekin et al., 2012), as
endorsed by The Assessment in Ankylosing Spondylitis International
Society/European League Against Rheumatism (ASAS/EULAR) (Braun et al.,
2011).
Exercise programmes can be group- or home-based (Ching-Yi WANG,
2009; Karapolat et al., 2008; Yigit et al., 2013). Home-based programmes are
not supervised in person but can receive remote orientation, they are cheaper
and more convenient, as individuals may execute exercises in the comfort of
their homes [4, 8], while group-based exercise programmes are supervised by a
physiotherapist, with increased effects as to functionality improvement and
reduction in disease activity, encouraging AS patients’ adherence (Gunendi et
al., 2010; Karapolat et al., 2008).
Although several scientific studies have reported the beneficial effects of
exercise, either performed in group or individually, the literature comparing
these two modalities in terms of functional and biomarker parameters is still
scarce, which makes it pertinent to further study this question. Therefore, the
aim of this study was to assess the effects of a specific exercise programme in
patients with AS regarding functional and biomarker parameters.
Capítulo III. Estudos Originais
76
Methods
Study design and participants
This quasi-experimental study involved a convenience sample of 31
patients with AS, and was conducted in the northern region of Portugal. The
study received approval from the Ethics Committee of the School of Health
Allied Sciences of the Polytechnic Institute of Porto, under number 3116/2013.
Potential candidates were identified by physiotherapists from the institution and
from the National Association of Ankylosing Spondylitis (ANEA) – Centre of
northern region of Portugal, and the recruitment occurred between February
2014 and June 2015.
Subjects were eligible to participate in the study if they: (1) were
diagnosed with AS according to the modified New York criteria (Yigit et al.,
2013); (2) were aged 18 years or older (Yigit et al., 2013) and (3) voluntarily
consented to participate. The study excluded all patients presenting any other
clinically diagnosed spondyloarthropathy, neurological and/or cardiorespiratory
pathologies, and who had performed regular exercise during the previous 3
months (Gunendi et al., 2010).
The patients were divided into three groups: the group-based exercise
programme group (n=12) included patients who were willing to participate in the
group-based exercise programme (Karapolat et al., 2008), the home-based
exercise group (n=12) included patients who had problems with transport or
getting permission from work (Karapolat et al., 2008), and the control group
(n=7) included patients who did not want to participate in the exercise
programme. All participants were assessed at baseline and 6 months after the
onset of the exercise programme. Of the initial 31 participants, 3 patients failed
to complete the programme because of unwillingness to participate (1 from the
control and 2 from the home-based exercise group).
Exercise programme
The exercise programme consisted of 12 exercises (Aytekin et al., 2012;
Dagfinrud et al., 2011; Durmus et al., 2009; Gunendi et al., 2010; Karapolat et
al., 2008; Lim et al., 2005; Yigit et al., 2013) designed to improve flexibility,
Capítulo III. Estudos Originais
77
mobility of the spine and chest expansion and to increase muscle
strengthening. The program included exercises for postural muscles, including
the transversus abdominis and deep flexors of the neck, strengthening
exercises of the spine extensors, adductors of the scapulae, lateral rotators and
flexors of the cervical spine and stretching of the posterior chain, lumbar and
cervical spine, as well as chest expansion exercises. The complete session
lasted 45 minutes.
The group-based exercise patients were treated with a group-based
exercise programme once a week for 6 months, under the supervision of the
same experienced physiotherapist, while home-based exercise group patients
practised the same programme individually at home, once a week for 6 months.
Participants in this group were provided with a CD with all the exercises, so that
they could follow the programme. They were also asked to register their
sessions in a book which has also been provided. All individuals in the home-
based exercise group were contacted every week for 6 months as a method of
ensuring adherence and clarifying any questions. Patients in the control group
were instructed to continue their usual daily activities. For ethical reasons, after
the 6-month period, the control group had the opportunity to participate in the
exercise programme.
Instruments
All patients completed the Portuguese version of the Bath Spondylitis
Functional Index (BASFI) (Pimentel-Santos et al., 2012), a characterisation
questionnaire which measures the functional status of patients with AS through
ten questions regarding daily activities, with the mean score (range, 0–10) being
obtained from the sum of all values.
The Portuguese version of the Bath Spondylitis Metrics Index (BASMI)
(Pimentel-Santos et al., 2012) was used to determine the participants’ physical
mobility, with the Shober’s test, lateral spine flexion, tragus-to-wall distance,
cervical rotation and intermalleolar distance, with a final score ranging from 0 to
2 in each one of the five parameters (0 – mild disease involvement, 1 –
Capítulo III. Estudos Originais
78
moderate disease involvement, 2 – severe disease involvement), resulting in a
total BASMI score of 0-10.
The Portuguese version of the Bath Spondylitis Disease Activity Index
(BASDAI) (Pimentel-Santos et al., 2012) was used to measure the disease
activity status through 6 questions with a score ranging from 0 to 10, regarding
fatigue, spinal pain, peripheral joint, entheses and morning stiffness, to
determine a final mean score. A mean of the two scores relating to morning
stiffness was calculated before averaging all the answers (A. Calin, 1999;
Pimentel-Santos et al., 2012).
The Portuguese version of the Oswestry Disability Index (ODI) was used
in each of its ten items, each of them including 6 statements, and patients were
requested to select only one, obtaining a score from 0-5. The Portuguese
version of the Neck Disability Index (NDI) also includes 6 statements and the
score 0-5. ODI and NDI total scores are converted into a percentage score with
0-20% indicating minimal disability, 21-40% moderate disability, 41-60% severe
disability, 61-80% crippled and 81-100% total incapacitation (Beattie & Maher,
1997; Fairbank, 1980; Vernon, 2008). Disease activity variables used include
both the C-Reactive Protein (CRP) and the Erythrocyte Sedimentation Rate
(ESR).
Data collection procedures
Aspects such as age, gender, level of education and employment
situation were identified as sociodemographic. Patients have completed four
self-administered questionnaires – NDI, ODI, BASFI and BASDAI.
As laboratory assessments of patients’ ESR and CRP were determined,
overnight fasting blood samples from all subjects were collected through
standard antecubital forearm venepuncture to 8 ml serum-separator and 3.5 ml
K2-EDTA tubes (BD Vacutainer® System, BD Diagnostics, Franklin Lakes, NJ).
After room temperature clotting, serum was separated by low speed
centrifugation (4500rpm, 10 min, 22°C) (Sigma ® 3k15, SIGMA
Laborzentrifugen GmbH, Osterode am Harz, Germany), transferred into
aliquots, and stored at -80°C until analysis ("Third Report of the National
Capítulo III. Estudos Originais
79
Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation,
and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III)
Final Report", 2002) and latex immunoturbidimetry (CRP) (Roberts et al., 2001)
techniques.
For ESR estimation, K2-EDTA anticoagulated blood samples were mixed
for 10 minutes before the test. Samples were aspirated into a Westergren
pipette and the distance that the column of blood fell in 1h was recorded
according to the International Council for Standardisation in Haematology
(ICSH) standardised method (Jou et al., 2011).
Data collection was performed at baseline and after the 6-month
programme to all participants, taking into account the location and time of
completion of the questionnaires, as well as collections of blood.
Data analysis
Data were analysed using the Statistical Package for Social Sciences
(SPSS) software, version 23.0 for Windows (Chicago, IL), using a significance
level of α=0.05. Normality tests were computed. Sample characteristics are
presented as counts and proportions for categorical variables and as mean and
standard deviation or median and interquartile range (IQR) for continuous
variables. Chi-Square tests were used to compare categorical variables
between groups. To compare continuous variables between groups, we have
used one-way ANOVA tests and, when the assumptions for its use were not
achieved, the Kruskal-Wallis test. Additionally, to compare baseline and 6-
month assessments the Paired samples T-test or the Wilcoxon test were used,
as appropriate.
Results
The socio-demographic information and history of the 31 individuals
included in the three groups were very similar at baseline (Table 1). Groups
were homogeneous as to age, diagnosis, gender, salary, education and
achievement programme at baseline, before the onset of the exercise
programme (p > 0.05).
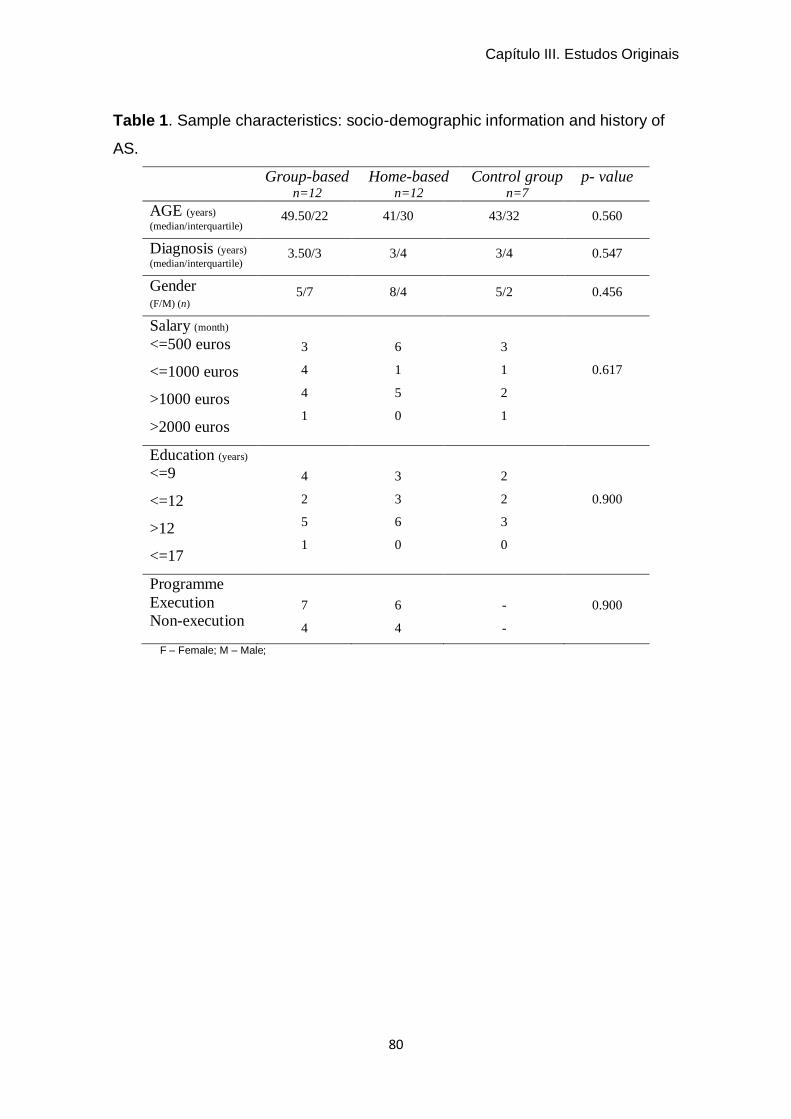
Capítulo III. Estudos Originais
80
Table 1. Sample characteristics: socio-demographic information and history of
AS.
Group-based n=12
Home-based n=12
Control group n=7
p- value
AGE (years) (median/interquartile)
49.50/22 41/30 43/32 0.560
Diagnosis (years)
(median/interquartile) 3.50/3 3/4 3/4 0.547
Gender (F/M) (n)
5/7 8/4 5/2 0.456
Salary (month)
<=500 euros
<=1000 euros
>1000 euros
>2000 euros
3
4
4
1
6
1
5
0
3
1
2
1
0.617
Education (years)
<=9
<=12
>12
<=17
4
2
5
1
3
3
6
0
2
2
3
0
0.900
Programme
Execution
Non-execution
7
4
6
4
-
-
0.900
F – Female; M – Male;
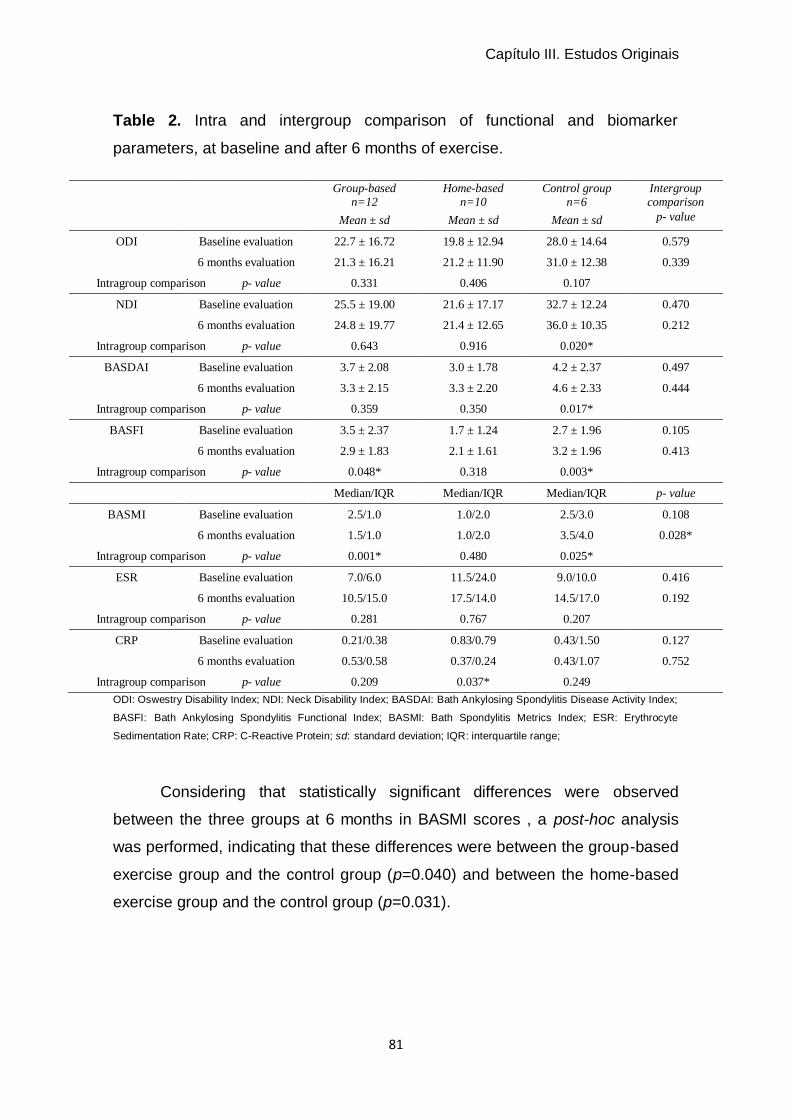
Capítulo III. Estudos Originais
81
Table 2. Intra and intergroup comparison of functional and biomarker
parameters, at baseline and after 6 months of exercise.
Group-based n=12
Home-based n=10
Control group n=6
Intergroup comparison
Mean ± sd Mean ± sd Mean ± sd p- value
ODI Baseline evaluation 22.7 ± 16.72 19.8 ± 12.94 28.0 ± 14.64 0.579
6 months evaluation 21.3 ± 16.21 21.2 ± 11.90 31.0 ± 12.38 0.339
Intragroup comparison p- value 0.331 0.406 0.107
NDI Baseline evaluation 25.5 ± 19.00 21.6 ± 17.17 32.7 ± 12.24 0.470
6 months evaluation 24.8 ± 19.77 21.4 ± 12.65 36.0 ± 10.35 0.212
Intragroup comparison p- value 0.643 0.916 0.020*
BASDAI Baseline evaluation 3.7 ± 2.08 3.0 ± 1.78 4.2 ± 2.37 0.497
6 months evaluation 3.3 ± 2.15 3.3 ± 2.20 4.6 ± 2.33 0.444
Intragroup comparison p- value 0.359 0.350 0.017*
BASFI Baseline evaluation 3.5 ± 2.37 1.7 ± 1.24 2.7 ± 1.96 0.105
6 months evaluation 2.9 ± 1.83 2.1 ± 1.61 3.2 ± 1.96 0.413
Intragroup comparison p- value 0.048* 0.318 0.003*
Median/IQR Median/IQR Median/IQR p- value
BASMI Baseline evaluation 2.5/1.0 1.0/2.0 2.5/3.0 0.108
6 months evaluation 1.5/1.0 1.0/2.0 3.5/4.0 0.028*
Intragroup comparison p- value 0.001* 0.480 0.025*
ESR Baseline evaluation 7.0/6.0 11.5/24.0 9.0/10.0 0.416
6 months evaluation 10.5/15.0 17.5/14.0 14.5/17.0 0.192
Intragroup comparison p- value 0.281 0.767 0.207
CRP Baseline evaluation 0.21/0.38 0.83/0.79 0.43/1.50 0.127
6 months evaluation 0.53/0.58 0.37/0.24 0.43/1.07 0.752
Intragroup comparison p- value 0.209 0.037* 0.249
ODI: Oswestry Disability Index; NDI: Neck Disability Index; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index;
BASFI: Bath Ankylosing Spondylitis Functional Index; BASMI: Bath Spondylitis Metrics Index; ESR: Erythrocyte
Sedimentation Rate; CRP: C-Reactive Protein; sd: standard deviation; IQR: interquartile range;
Considering that statistically significant differences were observed
between the three groups at 6 months in BASMI scores , a post-hoc analysis
was performed, indicating that these differences were between the group-based
exercise group and the control group (p=0.040) and between the home-based
exercise group and the control group (p=0.031).
Capítulo III. Estudos Originais
82
Discussion
Groups involved in this study were homogeneous at baseline as to
sociodemographic characteristics and as to the variables under analysis –
functional and biomarker parameters.
As to Bath indices analysis, more specifically in BASDAI, there was an
increase of disease activity in the control group (p=0.017) and a small decrease
with no statistical significance in the group-based exercise group. These results
seem to suggest that the practice of specific exercise contributes to the
functional management of individuals with AS (Dernis et al., 2007), and
corroborate the study of Yigit et al., (Yigit et al., 2013), who have reported that
the non-participation in exercise programmes increases disease activity,
although these authors only compare home-based programmes with a control
group, with a 10-week follow-up.
The group-based exercise group has shown statistically significant
differences in BASFI and BASMI scores (p=0.048 and p=0.001 respectively),
showing that the participation in a group exercise programme increased
functionality at the end of 6 months, which did not happen in the home-based
exercise group. The control group has shown statistically significant differences
in the same variables (p=0.003 and p=0.025 respectively), showing that the
non-participation in the exercise programme decreased the functional capacity
of these individuals. These results are similar to the findings of Günendi et al.,
(Gunendi et al., 2010), who reported an improvement in the BASFI score in the
group-based exercise group, in contrast to what happened in the control group,
although this study’s reassessment was performed after 3 weeks only. The
same occurred in the study of Cagliyan et al., (Cagliyan, 2007), with the group-
based exercise group improving in the same index after 3 months. With respect
to BASMI scores, our results show no statistically significant difference between
groups, in opposition with the observed by Karapolat et al. (Karapolat et al.,
2008) that found improvements in both the group-based exercise group and the
home-based exercise group.
ODI and NDI scores obtained at baseline and after 6 months were
different for the two groups. These differences corroborate the idea that
Capítulo III. Estudos Originais
83
exercise decreases cervical and lumbar functional disability, although the
values obtained are not statistically significant. Only the control group has
shown statistically significant differences in the NDI score, with increased
functional incapacity of the cervical region. This may be due to the fact that
most patients are female, the most affected gender, and also to the usual AS
consequences, such as pain, joint restriction and loss of functionality, which
originate cervical disability (Aytekin et al., 2012; El Tecle et al., 2015). ESR
scores have increased after 6 months of exercise for the three groups, although
this increase is not statistically significant in any of the groups.
Although regular physical activity is regarded as an effective therapy in
chronic diseases, particularly its anti-inflammatory effect, by the action of
cytokines to reduce inflammatory levels in AS (Papini et al., 2014), several
studies have obtained different results (Chen et al., 2015; Hulejova et al., 2012;
Kisacik et al., 2016; Londono et al., 2012; Ugur, 2015; Xu et al., 2011). It is
acknowledged that its predictive value for reflecting disease activity as to
sensitivity and specificity is low, and that the influence of factors such as age,
gender and anaemia throughout the disease inflammation process vary with
time, affecting its analytical values (Bochen, 2011; Kisacik et al., 2008; Ugur,
2015). CRP scores increased in the group-based exercise group and in the
control group, while decreasing in the home-based exercise group after 6
months. However, only the home-based exercise group has shown statistically
significant differences between assessments (p=0.037). Some studies have
been carried out regarding this biomarker in AS. Although CRP is the most
consistent parameter regarding the relationship between physical exercise and
inflammation markers, the underlying physiological mechanism is unclear, and
the great variation of studies regarding intergroup differences as to the intensity,
volume, duration and type of training must be taken into account, as the
decrease of this biomarker is not analysed consistently in experimental studies
(Campbell et al., 2008; Papini et al., 2014). This finding in the home-based
exercise group can result from different reasons, such as disease activity and
the small sample size (Plasqui et al., 2012).
Capítulo III. Estudos Originais
84
Intergroup comparison has shown statistically significant differences in
BASMI scores. After analysing comparatively each two groups, it was observed
that the most significant results occurred in the group-based and home-based
exercise groups, which suggests that the practice of exercise is essential to
improve joint mobility.
Individuals were recruited from the National Association of Ankylosing
Spondylitis (ANEA), which suggests greater availability, awareness, information
and up-to-date knowledge regarding the benefits of practising and participating
in exercise programmes (Song et al., 2015).
During this study, two subjects were excluded from the home-based
exercise group. Although this group, which executed the prescribed exercises
individually and without supervision, was contacted every week by the
investigation team and was provided with specific orientations regarding the
programme, it is known that supervised programmes increase patient
adherence, due to the monitoring of exercise duration, intensity and feedback
(Dagfinrud et al., 2011). One subject was also excluded from the control group
because of changes in the pharmacological therapy.
One of the distinguishing aspects of this study is follow-up duration (6
months), as most studies on this theme have reassessments 12, 10 and 3
weeks after the onset of the exercise programme (Cagliyan, 2007; Gunendi et
al., 2010; Yigit et al., 2013). Another important element is the existence of three
groups, while most previous literature only used two groups. A third strength is
the reduced number of patient loss during the 6 months. It should also be noted
that this study contributes to increase the insufficient number of studies
analysing the effect of supervised versus unsupervised exercise programmes
on functional and biomarker parameters.
On the other hand, our study also has some limitations. The sample size
did not allow carrying out more complex statistical analyses. Despite the small
size of the control group, the assessment of effect size revealed that it can be
considered of reasonable dimension, which suggests that our results have
implications on the clinical practice regarding these individuals. Biomarker
scores require further research regarding the relationship between specific
Capítulo III. Estudos Originais
85
exercise programmes and CRP and ESR levels in individuals with rheumatic
inflammatory diseases such as AS. Further studies that include other variables
are needed to evaluate the disease psychological impact and to monitor
individuals after the conclusion of the exercise programme.
Conclusions
The results of our study show that the execution of a supervised exercise
programme improves BASFI and BASMI scores. ESR and CRP tests are not
sufficient to reflect disease activity, as no changes in these biomarkers were
found after 6 months of following an exercise programme.
Bibliography
A. Calin, J.-P. N., A. Gueguen, H. Zeidler, H. Mielants and M. Dougados.
(1999). A new approach to defining functional ability in ankylosing
spondylitis: the development of the Bath Ankylosing Spondylitis
Functional Index. Rheumatology, 38(9), 878-882.
Aytekin, E., Caglar, N. S., Ozgonenel, L., Tutun, S., Demiryontar, D. Y., &
Demir, S. E. (2012). Home-based exercise therapy in patients with
ankylosing spondylitis: effects on pain, mobility, disease activity, quality
of life, and respiratory functions. Clin Rheumatol, 31(1), 91-97.
Beattie, P., & Maher, C. (1997). The role of functional status questionnaires for
low back pain. Australian Journal of Physiotherapy, 43(1), 29-38.
Bochen, K., Krasowska, A., Milaniuk, S., Kulczyńska, M., Prystupa, A., Dzida,
G. (2011). Erythrocyte sedimentation rate - an old marker with new
applications. Journal of Pre-Clinical and Clinical Research, Vol 5(2), 50-
55.
Braun, J., & Sieper, J. (2007). Ankylosing spondylitis. The Lancet, 369(9570),
1379-1390.
Braun, J., van den Berg, R., Baraliakos, X., Boehm, H., Burgos-Vargas, R.,
Collantes-Estevez, E., Dagfinrud, H., Dijkmans, B., Dougados, M.,
Emery, P., Geher, P., Hammoudeh, M., Inman, R. D., Jongkees, M.,
Capítulo III. Estudos Originais
86
Khan, M. A., Kiltz, U., Kvien, T., Leirisalo-Repo, M., Maksymowych, W.
P., Olivieri, I., Pavelka, K., Sieper, J., Stanislawska-Biernat, E.,
Wendling, D., Ozgocmen, S., van Drogen, C., van Royen, B., & van der
Heijde, D. (2011). 2010 update of the ASAS/EULAR recommendations
for the management of ankylosing spondylitis. Ann Rheum Dis, 70(6),
896-904.
Cagliyan, A., Kotevoglu, N., Onal, T., Tekkus, B., & Kuran, B. . (2007). Does
group exercise program add anything. Journal of Back & Musculoskeletal
Rehabilitation, 20(2/3), 79-85.
Campbell, K. C., P.; Ulrich,C.; Wener, M.; , Alfano, C. F.-S., K.; Rudolph, R.;
Potter,J.; and , & McTiernan, A. (2008). No reduction in C-reactive
protein following a 12-month randomized controlled trial of exercise in
men and women. Cancer Epidemiol Biomarkers Prev, 17(7), 1714–1718.
Chen, C. H., Chen, H. A., Liao, H. T., Liu, C. H., Tsai, C. Y., & Chou, C. T.
(2015). The clinical usefulness of ESR, CRP, and disease duration in
ankylosing spondylitis: the product of these acute-phase reactants and
disease duration is associated with patient's poor physical mobility.
Rheumatol Int, 35(7), 1263-1267.
Ching-Yi WANG, P.-Y. C., Hong-Shen LEE and James Cheng-Chung WEI.
(2009). The effectiveness of exercise therapy for ankylosing.
International Journal of Rheumatic Diseases, 12, 207–210.
Dagfinrud, H., Halvorsen, S., Vollestad, N. K., Niedermann, K., Kvien, T. K., &
Hagen, K. B. (2011). Exercise programs in trials for patients with
ankylosing spondylitis: do they really have the potential for
effectiveness? Arthritis Care Res (Hoboken), 63(4), 597-603.
Dernis, E., Lavie, F., Pavy, S., Wendling, D., Flipo, R. M., Saraux, A., Cantagrel,
A., Claudepierrre, P., Goupille, P., Le Loet, X., Maillefert, J. F., Mariette,
X., Schaeverbeke, T., Tebib, J., & Combe, B. (2007). Clinical and
laboratory follow-up for treating and monitoring patients with ankylosing
spondylitis: development of recommendations for clinical practice based
on published evidence and expert opinion. Joint Bone Spine, 74(4), 330-
337.

Capítulo III. Estudos Originais
87
Durmus, D., Alayli, G., Cil, E., & Canturk, F. (2009). Effects of a home-based
exercise program on quality of life, fatigue, and depression in patients
with ankylosing spondylitis. Rheumatol Int, 29(6), 673-677.
El Tecle, N. E., Abode-Iyamah, K. O., Hitchon, P. W., & Dahdaleh, N. S. (2015).
Management of spinal fractures in patients with ankylosing spondylitis.
Clin Neurol Neurosurg, 139, 177-182.
Fairbank, J. C., Couper, J., Davies, J.B., & O'Brien, J.P. (1980). The Oswestry
low back pain disability questionnaire. Physiotherapy, 66, 271-273.
Gunendi, Z., Sepici Dincel, A., Erdogan, Z., Aknar, O., Yanpal, S., Gogus, F., &
Atalay, F. (2010). Does exercise affect the antioxidant system in patients
with ankylosing spondylitis? Clin Rheumatol, 29(10), 1143-1147.
Hulejova, H., Levitova, A., Kuklova, M., Stochl, J., Haluzik, M., Pavelka, K.,
Vencovsky, J., & Senolt, L. (2012). No effect of physiotherapy on the
serum levels of adipocytokines in patients with ankylosing spondylitis.
Clin Rheumatol, 31(1), 67-71.
Jou, J. M., Lewis, S. M., Briggs, C., Lee, S. H., De La Salle, B., McFadden, S.,
& For The International Council For Standardization In, H. (2011). ICSH
review of the measurement of the erythocyte sedimentation rate.
International Journal of Laboratory Hematology, 33(2), 125-132.
Karapolat, H., Akkoc, Y., Sari, I., Eyigor, S., Akar, S., Kirazli, Y., & Akkoc, N.
(2008). Comparison of group-based exercise versus home-based
exercise in patients with ankylosing spondylitis: effects on Bath
Ankylosing Spondylitis Indices, quality of life and depression. Clin
Rheumatol, 27(6), 695-700.
Kisacik, B., Tufan, A., Kalyoncu, U., Karadag, O., Akdogan, A., Ozturk, M. A.,
Kiraz, S., Ertenli, I., & Calguneri, M. (2008). Mean platelet volume (MPV)
as an inflammatory marker in ankylosing spondylitis and rheumatoid
arthritis. Joint Bone Spine, 75(3), 291-294.
Kisacik, P., Unal, E., Akman, U., Yapali, G., Karabulut, E., & Akdogan, A.
(2016). Investigating the effects of a multidimensional exercise program
on symptoms and antiinflammatory status in female patients with
Capítulo III. Estudos Originais
88
ankylosing spondylitis. Complementary Therapies in Clinical Practice, 22,
38-43.
Lim, H. J., Moon, Y. I., & Lee, M. S. (2005). Effects of home-based daily
exercise therapy on joint mobility, daily activity, pain, and depression in
patients with ankylosing spondylitis. Rheumatol Int, 25(3), 225-229.
Londono, J., Romero-Sanchez, M., Torres, V., Bautista, W., Fernandez, D.,
Quiroga, J., Valle-Oñate, R., Santos, A., & Medina, J. (2012). The
association between serum levels of potential biomarkers with the
presence of factors related to the clinical activity and poor prognosis in
Spondyloarthritis. Rev Bras Reumatol, 52(4), 529-544.
Papini, C. B., Nakamura, P. M., Zorzetto, L. P., Thompson, J. L., Phillips, A. C.,
& Kokubun, E. (2014). The effect of a community-based, primary health
care exercise program on inflammatory biomarkers and hormone levels.
Mediators Inflamm, 2014, 185707.
Passalent, L. A. (2011). Physiotherapy for ankylosing spondylitis: evidence and
application. Curr Opin Rheumatol, 23(2), 142-147.
Pimentel-Santos, F. M., Pinto, T., Santos, H., Barcelos, A., Cunha, I., Branco, J.
C., & Ferreira, P. L. (2012). Portuguese version of the bath indexes for
ankylosing spondylitis patients: a cross-cultural adaptation and
validation. Clin Rheumatol, 31(2), 341-346.
Plasqui, G., Boonen, A., Geusens, P., Kroot, E. J., Starmans, M., & van der
Linden, S. (2012). Physical activity and body composition in patients with
ankylosing spondylitis. Arthritis Care Res (Hoboken), 64(1), 101-107.
Roberts, W. L., Moulton, L., Law, T. C., Farrow, G., Cooper-Anderson, M.,
Savory, J., & Rifai, N. (2001). Evaluation of Nine Automated High-
Sensitivity C-Reactive Protein Methods: Implications for Clinical and
Epidemiological Applications. Part 2. Clinical Chemistry, 47(3), 418-425.
Song, I. H., Brenneis, C., Hammel, L., Feldtkeller, E., Listing, J., Sieper, J., &
Rudwaleit, M. (2015). Ankylosing spondylitis self-help organisations - do
members differ from non-members? Joint Bone Spine.
Third Report of the National Cholesterol Education Program (NCEP) Expert
Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol
Capítulo III. Estudos Originais
89
in Adults (Adult Treatment Panel III) Final Report. (2002). Circulation,
106(25), 3143.
Ugur, M. B., N.; Melikoglu, M.; Baygutalp, F.; Altas, E; and Seferoglu, B.
(2015). Elevated serum interleukin-23 levels in ankylosing spondylitis
patients and the relationship with disease activity. Nagoya J. Med. Sci.,
77, 621-627.
Vernon, H. (2008). The Neck Disability Index: state-of-the-art, 1991-2008. J
Manipulative Physiol Ther, 31(7), 491-502.
Xu, M., Lin, Z., Deng, X., Li, L., Wei, Y., Liao, Z., Li, Q., Wei, Q., Hu, Z., Zhang,
Y., Lin, Q., Huang, J., Li, T., Pan, Y., Wu, Y., Jin, O., Yu, B., & Gu, J.
(2011). The Ankylosing Spondylitis Disease Activity Score is a highly
discriminatory measure of disease activity and efficacy following tumour
necrosis factor-alpha inhibitor therapies in ankylosing spondylitis and
undifferentiated spondyloarthropathies in China. Rheumatology (Oxford),
50(8), 1466-1472.
Yigit, S., Sahin, Z., Demir, S. E., & Aytac, D. H. (2013). Home-based exercise
therapy in ankylosing spondylitis: short-term prospective study in patients
receiving tumor necrosis factor alpha inhibitors. Rheumatol Int, 33(1), 71-
77.


Capítulo IV
Discussão _______________________________________________________________
Capítulo IV. Discussão
93
Os principais resultados da revisão sistemática apresentada neste
trabalho sugerem que os programas realizados em grupo parecem ser mais
eficazes do que os realizados individualmente no domicílio. Os resultados dos
estudos originais revelaram que os doentes com EA apresentavam um elevado
conhecimento sobre a patologia, e verificou-se também uma fraca associação
entre parâmetros funcionais e bioquímicos nestes doentes. A realização de um
programa de exercícios específico para a EA supervisionado em grupo, foi
eficaz na melhoria da mobilidade e funcionalidade articular nestes indivíduos.
O primeiro estudo realizado, sob a forma de revisão sistemática, teve
por base fazer um levantamento e posterior análise de todos os estudos
publicados sobre o efeito de programas de exercício na EA, quer realizados em
grupo, quer realizados de forma individualizada. Os resultados desta revisão
sistemática sugerem que os programas de exercício em grupo são mais
eficazes do que os programas realizados no domicílio. Apesar de os programas
no domicílio não se revelarem tão eficazes, não deixam de ser recomendados,
pois também se verificam melhorias nos indivíduos após a sua execução, no
entanto, são necessários mais estudos randomizados controlados nesta área,
para promover maior evidência científica para este tipo de intervenção.
Os estudos incluídos na revisão sistemática mostram-nos que os
programas de exercícios utilizados não são muito variáveis na sua tipologia, ou
seja, a grande parte dos estudos incluí no programa de exercícios,
alongamentos, fortalecimento muscular, reeducação respiratória e correção
postural, com o objetivo de diminuir a dor, aumentar a funcionalidade e a
capacidade respiratória (Altan et al., 2012; Fernandez-de-Las-Penas et al.,
2006; Fernandez-de-las-Penas et al., 2005; Ince, 2006; Lim et al., 2005;
Masiero et al., 2011; Passalent, 2011; Silva et al., 2012; Widberg et al., 2009).
Embora não variem na tipologia, uns autores incidem mais em exercícios
respiratórios, na mobilização vertebral, exercícios propriocetivos e em
educação para a saúde (Fernandez-de-las-Penas et al., 2005; Ince, 2006;
Masiero et al., 2011; Widberg et al., 2009), outros na reeducação global
postural (RPG) (Fernandez-de-Las-Penas et al., 2006; Silva et al., 2012), um
autor na correção postural aliada à respiração (Altan et al., 2012) e um outro
Capítulo IV. Discussão
94
autor focando-se em exercícios de relaxamento, flexibilidade, força e correção
postural (Lim et al., 2005). Esta variabilidade de exercícios apresentada nestes
estudos, mas com o mesmo fim, torna difícil, de certa forma a comparação
entre estudos e dificulta a obtenção de um padrão típico de programa de
exercícios, dirigido a estes indivíduos para realização em grupo ou de forma
individualizada. Programas de exercício facilmente reproduzíveis em grupo ou
no domicílio com e sem supervisão devem ser programas, com um
planeamento de exercícios multivariados capazes de serem efetuados pelos
doentes de forma fácil e eficaz.
A educação para a saúde, também eleita por alguns autores, é uma
forma de intervenção eficaz na promoção de conhecimento sobre a patologia e
com vantagens na funcionalidade, quando associada a outro tipo de
intervenção, nomeadamente programas de exercício em grupo (Masiero et al.,
2011). Relativamente à eficácia de realizar o mesmo programa em grupo vs
domicílio, nenhum estudo incluído na revisão sistemática optou por esta
metodologia. Todos os estudos apresentados na revisão sistemática que
comparam programas em grupo vs domicílio, realizam programas diferentes,
nos diferentes contextos de intervenção (Ince, 2006; Masiero et al., 2011;
Widberg et al., 2009).
Nesta revisão sistemática é de realçar que um dos outcomes
transversal a todos os estudos é a utilização de parâmetros funcionais,
nomeadamente, os índices de Bath, à exceção do estudo realizado por Ince
(2006), que utilizou como outcome, medidas funcionais cardiorespiratórias
(Ince, 2006). De salientar também que apenas um estudo utilizou em
simultâneo parâmetros funcionais e bioquímicos (VS e PCR) como outcome
(Masiero et al., 2011). Após a realização desta revisão sistemática, é de certa
forma percetível a escassez de estudos que compararam o mesmo programa
em grupo vs domicílio, em parâmetros funcionais e bioquímicos com um follow-
up superior a 16 semanas. É notório, igualmente, a escassez de estudos, que
também abordem a educação como potencial fator de desenvolvimento de
conhecimento, aliada a programas de intervenção. Sendo esta uma doença
crónica, é importante desenvolver competências nestes indivíduos, de forma a
Capítulo IV. Discussão
95
potenciar o empowerment, para promover uma maior autonomia e gestão
proporcionando assim ganhos em saúde nestes utentes. Uma limitação sentida
na elaboração desta revisão sistemática foi o número reduzido de estudos para
análise o que não permitiu a realização de uma meta-análise.
Após a realização desta revisão sistemática, surgiu a necessidade de
fazer um levantamento relativamente ao conhecimento que estes indivíduos
apresentam relativamente à sua doença. Esta necessidade foi reforçada após
os contactos iniciais com a população em causa, tendo sido verificado que
muitos indivíduos com a doença, desconheciam sinais e sintomas e diferentes
opções de tratamento.
Assim, no estudo II, realizado e incluído neste trabalho, é evidenciada a
importância da utilização de instrumentos válidos e comparáveis a nível
internacional com propriedades psicométricas adaptadas, para que os seus
resultados permitam alcançar conclusões credíveis e aceites por toda a
comunidade científica. Este estudo em particular refere-se ao conhecimento da
EA, desenvolvido e induzido pela educação que estes indivíduos possuem. A
educação é também recomendada pela ASAS/EULAR (2010), como forma
integrante da intervenção não farmacológica em indivíduos com EA (Braun et
al., 2011). No contexto da EA, a educação tem por objetivo capacitar o
individuo de reconhecer e controlar a sua dor, a fadiga a funcionalidade de
forma a fazer uma melhor autogestão da sua doença, promovendo o bem-estar
psicológico e aumentando a sua qualidade de vida (Masiero et al., 2011). Sem
dúvida que a aposta na educação pode aumentar o conhecimento destes
indivíduos, no entanto, na EA, são ainda escassos os estudos nesta temática.
O estudo II contribuiu para esta área através da validação e adaptação cultural
de um instrumento de avaliação sobre o conhecimento da doença na
população portuguesa com EA. Os estudos publicados na área do
conhecimento, e com o mesmo instrumento de avaliação, reportam-se apenas
a dois países, ao Reino Unido (E. Lubrano, 1998; Lubrano, 1998) e a França
(Claudepierre et al., 2004). Com o estudo II, verificou-se que a população
portuguesa com EA, evidencia um elevado conhecimento da doença, em
especial em indivíduos mais novos e com um nível educacional e salarial mais
Capítulo IV. Discussão
96
elevado, indo ao encontro dos estudos desenvolvidos por Lubrano (1998) e
Claudepierre et al., (2004). Neste estudo II, não se verificou qualquer
associação do conhecimento da doença com o género, indo ao encontro dos
resultados de outro estudo, efetuado em doentes com artrite reumatóide, onde
também não se verificou associação do conhecimento da doença com o género
(Hennell et al., 2004). Segundo um estudo desenvolvido por Cooksey (2012)
em EA, verificou que os homens demonstram menos interesse em aumentar o
conhecimento relativo à doença de que padecem, comparativamente com as
mulheres, que por norma se mostram mais proactivas na busca de informação
e conhecimento sobre a doença (Cooksey, 2012). Outros estudos também
demonstram que o conhecimento tem impacto a nível da redução dos custos
associados, nomeadamente sobre os custos diretos, tais como medicação, idas
às urgências, internamentos e cirurgia, mas também sobre os custos indiretos,
como o absentismo laboral, os níveis de ansiedade e diminuição da qualidade
de vida (Frauendorf et al., 2013; Marcelo Cardozo de Souza, 2012; Reveille et
al., 2012). Pertencer a organizações relacionadas com a doença é uma outra
variável potencialmente relevante pela sua influência no nível de conhecimento
da doença (Song et al., 2015).
Após a realização do estudo II surgiu a necessidade de caracterizar a
população em estudo, e verificar a existência de associação entre parâmetros
funcionais e bioquímicos. Assim, neste seguimento, o estudo III, caracteriza
indivíduos com EA, sócios da ANEA - Núcleo Região do Porto. Esta amostra foi
constituída por maior número de mulheres do que homens, situação que não
está de acordo com outros estudos desenvolvidos em EA recentemente em
Portugal e na Europa (Pimentel-Santos et al., 2012; Raychaudhuri & Deodhar,
2014). Esta divergência poderá dever-se ao facto de as mulheres estarem mais
disponíveis para a participação deste tipo de programas do que os homens, e
mostrarem-se mais interessadas na busca de conhecimento, voluntariando-se
assim, mais facilmente que os homens (da Rocha Lopes et al., 2016; Roxanne
Cooksey, 2012). Verificou-se também que o nível de escolaridade desta
amostra foi superior a 12 anos de estudos, sugerindo indivíduos mais exigentes
na procura de informação (da Rocha Lopes et al., 2016). Outro fator importante
Capítulo IV. Discussão
97
foi o número de anos de diagnóstico que caracterizou a amostra deste estudo
III, tendo a maioria destes indivíduos um diagnóstico com mais de 15 anos,
indo ao encontro de outro estudo desenvolvido em Portugal em que os
indivíduos possuíam um diagnóstico com mais de 10 anos (Pimentel-Santos et
al., 2012). A média de idades desta amostra foi de 42.77 anos, apresentando o
individuo mais jovem 18 anos de idade, facto importante, pois demonstra que
atualmente o diagnóstico é realizado mais precocemente, permitindo desta
forma, um acompanhamento mais diferenciado destes indivíduos, um maior
controlo e gestão da doença, com maior acessibilidade aos serviços de saúde
para avaliação e monotorização da doença (Pimentel-Santos et al., 2012).
Foram também analisados parâmetros funcionais como o Oswestry Disability
Index (ODI) e Neck Disability Index (NDI). Estes parâmetros, embora se
encontrem dentro do mesmo intervalo em termos de “média de score”
(incapacidade moderada), verifica-se que os valores de NDI se apresentam
superiores aos de ODI. Isto significa que os indivíduos da amostra
apresentavam uma maior limitação funcional na coluna cervical
comparativamente à coluna lombar. Este achado não vai ao encontro do que
está descrito pela literatura pois, na EA, a coluna lombar é normalmente mais
afetada comparativamente à coluna cervical (El Tecle et al., 2015). Uma
justificação para este achado pode residir no facto de nesta amostra a maioria
dos indivíduos serem mulheres e estas, de um modo geral, apresentarem uma
maior limitação na coluna cervical comparativamente à coluna lombar,
contrariamente aos homens (El Maghraoui et al., 2003; Ortega Castro et al.,
2013). Relativamente aos parâmetros bioquímicos, os valores de VS e PCR
apresentavam-se baixos, revelando uma baixa atividade da doença. Vários
estudos demonstram que estes marcadores não têm valor preditivo suficiente
para avaliar a atividade da doença (Braun & Sieper, 2007; de Vlam, 2010; Kaya
et al., 2007; Kisacik et al., 2008), possuindo baixa sensibilidade, especificidade
e reprodutibilidade como se verificou noutros estudos (Hulejova et al., 2012;
Londono et al., 2012). Uma possível justificação para estes valores reduzidos
no nosso estudo pode ser devida, ao tratamento farmacológico que tende a
atenuar estes parâmetros bioquímicos. Neste estudo III, aquando do
Capítulo IV. Discussão
98
ajustamento da variável anos de diagnóstico e nível educacional, verificou-se
que à medida que os valores de VS aumentavam o índice BASDAI e BASFI
também, mostrando assim uma associação direta entre eles. Esta associação
mostrou que com o aumento da VS a atividade e funcionalidade da doença
também aumentavam, indicando um agravamento do quadro clínico nestes
indivíduos. Quanto ao biomarcador PCR, não se verificou associação com
nenhum dos índices de Bath, indo ao encontro dos resultados de outro estudo
que demonstra uma pobre associação com fatores relacionados com a
atividade da doença, apesar de este biomarcador ser mais sensível do que a
VS (Londono et al., 2012). Quanto à associação do ODI e NDI com os
parâmetros bioquímicos, verificou-se uma fraca associação, situação que pode
ser justificada pelos anos de evolução da doença que estes indivíduos
apresentavam, o que lhes permitiu ao longo do tempo delinear estratégias para
fazer face a estas incapacidades da vida diária, de forma a diminuir o impacto
da dor crónica em termos de incapacidade cervical e lombar. O facto de
pertencerem a uma associação também pode contribuir para desenvolver e
explicar estas estratégias, uma vez que, como associados, recebem
aconselhamento e informação mais diferenciado do que aqueles que não
pertencem a associações ligadas à doença (Song et al., 2015). Os resultados
neste estudo III têm implicações para a prática clínica, especialmente na forma
como se podem delinear estratégias específicas nas diferentes fases de
evolução da doença, tendo em conta que se trata de uma doença crónica e
incapacitante. Permitem também uma monitorização e acompanhamento mais
diferenciado em todo o processo evolutivo da doença. A importância destes
resultados surge também como um contributo para a prescrição de uma
intervenção adequada. De notar que o número reduzido da amostra pode ser
apontado como uma limitação do estudo.
Neste seguimento, e após a realização do estudo III, levantou-se uma
nova questão relacionada com a necessidade de avaliar o efeito desta amostra
quando submetida a uma intervenção particular, nomeadamente a realização
de um programa de exercícios específico. Surgiu assim a necessidade de se
avançar para o estudo seguinte.
Capítulo IV. Discussão
99
Assim, de forma sequencial, surge o estudo IV, que pretendeu verificar
o efeito de um programa regular e prolongado de exercícios específicos em
indivíduos com EA. O programa de exercício físico regular foi criado e
desenvolvido tendo por base estudos científicos publicados sobre a temática
(Aytekin et al., 2012; Cagliyan, 2007; Gunendi et al., 2010; Karapolat et al.,
2008; Yigit et al., 2013). Ao fim de seis meses de execução deste programa, e
relativamente aos índices BASFI e BASMI, apenas se verificaram melhorias
nos indivíduos que praticavam exercício em grupo, ostentando que a prática de
exercício em grupo promove a mobilidade e funcionalidade nestes indivíduos,
não se verificando o mesmo no programa efetuado no domicílio. Estes
resultados vão ao encontro aos de outros estudos, nomeadamente no estudo
desenvolvido por Gunendi e colaboradores onde os indivíduos que praticam
exercício em grupo também obtiveram melhorias relativamente ao índice de
BASFI (Gunendi et al., 2010). Outro estudo, que também sustenta estes
resultados, foi desenvolvido por Cagliyan e colaboradores onde, os indivíduos
que praticavam exercício em grupo apresentam melhores resultados (Cagliyan,
2007). Relativamente ao índice de BASMI, estes resultados não vão ao
encontro de um estudo desenvolvido por Karapolat e colaboradores, mostrando
que os indivíduos que executavam o programa em grupo ou no domicílio
obtinham iguais melhorias (Karapolat et al., 2008). No nosso estudo, na análise
das variáveis ODI e NDI, verificou-se na comparação intragrupos, diferenças
estatisticamente significativas, no que diz respeito ao grupo controlo, e apenas
quanto ao NDI, sugerindo maior incapacidade funcional na coluna cervical. O
facto de se verificarem estas diferenças estatisticamente significativas, apenas
na coluna cervical, pode ser explicado pelo facto da maioria dos indivíduos
deste grupo controlo serem mulheres, cuja região vertebral é mais atingida
sintomaticamente pelo curso normal da doença, relativamente à rigidez
articular, dor e diminuição da funcionalidade (Aytekin et al., 2012; El Tecle et
al., 2015). Na análise dos parâmetros bioquímicos, verificou-se, relativamente à
VS, um aumento deste parâmetro nos três grupos em estudo após os seis
meses de intervenção, indo de encontro a estudos publicados sobre esta
temática (Chen et al., 2015; Hulejova et al., 2012; Kisacik et al., 2016; Londono
Capítulo IV. Discussão
100
et al., 2012; Ugur, 2015; Xu et al., 2011). Uma justificação para este facto pode
ser devido ao baixo valor preditivo deste marcador inflamatório para refletir a
verdadeira atividade da doença, relativamente à sensibilidade e especificidade,
sendo também influenciado por vários fatores, tais como a idade e o sexo, e
todo o processo de inflamação no decorrer da evolução da doença (Bochen,
2011; Kisacik et al., 2008; Plasqui et al., 2012; Ugur, 2015). Assim, os
resultados relativamente aos biomarcadores justificam a necessidade de mais
pesquisas sobre a relação entre a prática de programas de exercício específico
e os níveis de PCR e VS em indivíduos com EA, para permitirem conclusões
mais seguras.
Os resultados obtidos neste estudo IV, demonstram que no grupo
controlo, o índice BASDAI, evidencia um aumento da atividade da doença
nestes indivíduos ao fim de seis meses, sugerindo que a prática de exercício
físico é fundamental para a manutenção funcional destes indivíduos (Dernis et
al., 2007). Outro estudo desenvolvido por Yigit e colaboradores, mostra um
aumento da atividade da doença em indivíduos que não praticam qualquer tipo
de exercício, no entanto, estes autores, compararam indivíduos que realizaram
o programa no domicílio com indivíduos que não realizavam qualquer tipo de
programa, com um follow up de apenas 10 semana (Yigit et al., 2013). Ainda
relativo ao grupo controlo do nosso estudo, verificou-se nos índices BASFI e
BASMI que a não execução deste programa promoveu um agravamento na
mobilidade e funcionalidade ao fim de seis meses.
Há algumas limitações a apontar a este estudo, tais como o reduzido
número de indivíduos que constituíram o grupo controlo e a não inclusão de
parâmetros imagiológicos de forma a os poder relacionar com os parâmetros
funcionais e bioquímicos, com objetivo de predizer com maior sustentabilidade
a eficácia do programa de exercícios.
Implicações na prática clínica
Estes resultados, mostram-nos que em termos de intervenção não
farmacológica, a prática de programas de exercício é uma opção disponível e
eficaz para estes indivíduos com EA. Apesar da grande heterogeneidade de

Capítulo IV. Discussão
101
programas de exercício, a sua prática em grupo evidencia melhores resultados
do que quando efectuada no domicilio. Recomenda-se a prática de programas
de exercício na EA, no entanto, também a promoção de conhecimento sobre a
sua patologia é fundamental para estes indivíduos, pois permite uma
autogestão mais adequada e segura tendo em conta as manifestações clínicas.

Capitulo V
Conclusões
_______________________________________________________________

Capítulo V. Conclusões
105
A revisão sistemática, demonstrou que os programas realizados em
grupo parecem ser mais eficazes do que os realizados individualmente no
domicílio, revelando a importância da supervisão dos programas em grupo,
assim como, o facto de estar inserido num grupo de indivíduos com a mesma
doença. Apesar deste achado, estes programas no domicílio também são
recomendados, em detrimento de não realizar qualquer tipo de programa, uma
vez que a execução de exercícios em indivíduos com esta doença parece
atenuar a progressiva deterioração estrutural e funcional articular consequentes
da evolução da doença. Os estudos originais permitiram concluir, que os
indivíduos com EA, apresentam um elevado conhecimento sobre a patologia,
especialmente em áreas como a sintomatologia, testes imunológicos e
intervenção, talvez por serem as áreas crucias na procura de conhecimento
após a confirmação do diagnóstico. Demonstraram também, que os indivíduos
que são membros de associações, como o caso da Associação Nacional de
Espondilite Anquilosante, apresentam um elevado nível educacional e
rendimento mensal, uma evolução da doença com pelo menos 15 anos e com
moderada incapacidade funcional. São indivíduos mais interessados pelo
conhecimento acerca da doença e, sendo esta uma doença crónica, torna-se
importante potenciar o empowerment nestes doentes. Tendo em conta que a
doença é prolongada, que apresenta variações ao longo do tempo, com
períodos de exacerbação e ou diminuição de sintomas, ou até com períodos
assintomáticos, verifica-se uma fraca associação entre parâmetros funcionais e
bioquímicos nestes indivíduos. Verificou-se também que a realização de um
programa de exercícios específico para a EA supervisionado em grupo, é
determinante na melhoria da mobilidade e funcionalidade destes indivíduos,
verificando-se uma elevada adesão por partes dos doentes ao longo de seis
meses. A não realização de qualquer tipo de programa induz um agravamento
na mobilidade e funcionalidade articular em vários segmentos.


Capítulo VI
Perspetivas Futuras _______________________________________________________________

Capítulo VI. Perspetivas Futuras
109
Após a redação deste trabalho e tendo em conta os resultados obtidos,
urge a necessidade de futuras investigações dirigidas essencialmente para a
fisiopatologia da espondilite anquilosante, permitindo assim de certa forma
estabelecer maior rigor no tipo de intervenção. A necessidade de um maior
entendimento de toda a fisiopatologia surge também pela carência de estudos
que mostrem a relação entre parâmetros bioquímicos inflamatórios e a prática
de programas de exercício de forma sólida e sustentada. Novos estudos
deviam ser desenvolvidos tendo em conta a influência de programas
educacionais no conhecimento e autogestão da doença, considerando os
indivíduos com EA como os primeiros e principais gestores da sua doença. Por
último, é importante desenvolver estudos em áreas como a nutrição, de forma a
compreender a importância e relação da ingestão de determinados alimentos
com a inflamação subjacente a todo o processo fisiopatológico da doença
como uma mais-valia para estes indivíduos. Atualmente têm surgido estudos
novos relacionados com a ingestão de alimentos ricos em amido, como sendo
potenciadores do processo inflamatório, assim como, certos alimentos
antioxidantes promoverem uma diminuição deste processo nestes doentes.

Capítulo VII
Referências _______________________________________________________________

Capítulo VII. Referências
113
Aissaoui, N., Rostom, S., Hakkou, J., Berrada Ghziouel, K., Bahiri, R., Abouqal,
R., & Hajjaj-Hassouni, N. (2012). Fatigue in patients with ankylosing
spondylitis: prevalence and relationships with disease-specific variables,
psychological status, and sleep disturbance. Rheumatol Int, 32(7), 2117-
2124.
Altan, L., Korkmaz, N., Dizdar, M., & Yurtkuran, M. (2012). Effect of Pilates
training on people with ankylosing spondylitis. Rheumatol Int, 32(7),
2093-2099.
Aytekin, E., Caglar, N. S., Ozgonenel, L., Tutun, S., Demiryontar, D. Y., &
Demir, S. E. (2012). Home-based exercise therapy in patients with
ankylosing spondylitis: effects on pain, mobility, disease activity, quality
of life, and respiratory functions. Clin Rheumatol, 31(1), 91-97.
Bardos, T., Szabo, Z., Czipri, M., Vermes, C., Tunyogi-Csapo, M., Urban, R. M.,
Mikecz, K., & Glant, T. T. (2005). A longitudinal study on an autoimmune
murine model of ankylosing spondylitis. Ann Rheum Dis, 64(7), 981-987.
Bochen, K., Krasowska, A., Milaniuk, S., Kulczyńska, M., Prystupa, A., Dzida,
G. (2011). Erythrocyte sedimentation rate - an old marker with new
applications. Journal of Pre-Clinical and Clinical Research, Vol 5(2), 50-
55.
Bodur, H., Ataman, S., Rezvani, A., Bugdayci, D. S., Cevik, R., Birtane, M.,
Akinci, A., Altay, Z., Gunaydin, R., Yener, M., Kocyigit, H., Duruoz, T.,
Yazgan, P., Cakar, E., Aydin, G., Hepguler, S., Altan, L., Kirnap, M.,
Olmez, N., Soydemir, R., Kozanoglu, E., Bal, A., Sivrioglu, K., Karkucak,
M., & Gunendi, Z. (2011). Quality of life and related variables in patients
with ankylosing spondylitis. Qual Life Res, 20(4), 543-549.
Braem, K., & Lories, R. J. (2012). Insights into the pathophysiology of
ankylosing spondylitis: contributions from animal models. Joint Bone
Spine, 79(3), 243-248.
Braun, J., & Sieper, J. (2007). Ankylosing spondylitis. The Lancet, 369(9570),
1379-1390.
Braun, J., van den Berg, R., Baraliakos, X., Boehm, H., Burgos-Vargas, R.,
Collantes-Estevez, E., Dagfinrud, H., Dijkmans, B., Dougados, M.,
Capítulo VII. Referências
114
Emery, P., Geher, P., Hammoudeh, M., Inman, R. D., Jongkees, M.,
Khan, M. A., Kiltz, U., Kvien, T., Leirisalo-Repo, M., Maksymowych, W.
P., Olivieri, I., Pavelka, K., Sieper, J., Stanislawska-Biernat, E.,
Wendling, D., Ozgocmen, S., van Drogen, C., van Royen, B., & van der
Heijde, D. (2011). 2010 update of the ASAS/EULAR recommendations
for the management of ankylosing spondylitis. Ann Rheum Dis, 70(6),
896-904.
Cagliyan, A., Kotevoglu, N., Onal, T., Tekkus, B., & Kuran, B. . (2007). Does
group exercise program add anything. Journal of Back & Musculoskeletal
Rehabilitation, 20(2/3), 79-85.
Chen, C. H., Chen, H. A., Liao, H. T., Liu, C. H., Tsai, C. Y., & Chou, C. T.
(2015). The clinical usefulness of ESR, CRP, and disease duration in
ankylosing spondylitis: the product of these acute-phase reactants and
disease duration is associated with patient's poor physical mobility.
Rheumatol Int, 35(7), 1263-1267.
Ching-Yi WANG, P.-Y. C., Hong-Shen LEE and James Cheng-Chung WEI.
(2009). The effectiveness of exercise therapy for ankylosing.
International Journal of Rheumatic Diseases, 12, 207–210.
Claudepierre, P., Flipo, R. M., Sibilia, J., Berthelot, J. M., Goupille, P.,
Cortinovis, S., Cunin, P., Chevalier, X., & Wendling, D. (2004). Patient
knowledge of their disease: a French multicenter study in ankylosing
spondylitis. Joint Bone Spine, 71(6), 550-556.
Cooksey, R. B., S.; Husain, M.; I. Elizabeth, Davies,H. and Siebert, S. (2012).
The information needs of people living with ankylosing spondylitis: a
questionnaire survey. BMC Musculosketal Disorders, 13, 243.
da Rocha Lopes, S. M., Duarte, J. A., & Mesquita, C. T. (2016). Cross-cultural
adaptation and validation of the Portuguese version of "The assessment
of knowledge in ankylosing spondylitis patients by a self-administered
questionnaire". Rheumatol Int.
Dagfinrud, H., Halvorsen, S., Vollestad, N. K., Niedermann, K., Kvien, T. K., &
Hagen, K. B. (2011). Exercise programs in trials for patients with
Capítulo VII. Referências
115
ankylosing spondylitis: do they really have the potential for
effectiveness? Arthritis Care Res (Hoboken), 63(4), 597-603.
de Vlam, K. (2010). Soluble and tissue biomarkers in ankylosing spondylitis.
Best Pract Res Clin Rheumatol, 24(5), 671-682.
de Vries, M. K., van Eijk, I. C., van der Horst-Bruinsma, I. E., Peters, M. J.,
Nurmohamed, M. T., Dijkmans, B. A., Hazenberg, B. P., & Wolbink, G. J.
(2009). Erythrocyte sedimentation rate, C-reactive protein level, and
serum amyloid a protein for patient selection and monitoring of anti-tumor
necrosis factor treatment in ankylosing spondylitis. Arthritis Rheum,
61(11), 1484-1490.
Dernis, E., Lavie, F., Pavy, S., Wendling, D., Flipo, R. M., Saraux, A., Cantagrel,
A., Claudepierrre, P., Goupille, P., Le Loet, X., Maillefert, J. F., Mariette,
X., Schaeverbeke, T., Tebib, J., & Combe, B. (2007). Clinical and
laboratory follow-up for treating and monitoring patients with ankylosing
spondylitis: development of recommendations for clinical practice based
on published evidence and expert opinion. Joint Bone Spine, 74(4), 330-
337.
E. Lubrano, P. H., P. Moreno, B. Griffiths, P. Emery and D. Veale. (1998). The
Assessment of Knowledge in Ankylosing Spondylitis Patients by a Self-
Administered Questionnaire. British Journal of Rheumatology(37), 437–
441.
El Maghraoui, A., Bensabbah, R., Bahiri, R., Bezza, A., Guedira, N., & Hajjaj-
Hassouni, N. (2003). Cervical spine involvement in ankylosing
spondylitis. Clin Rheumatol, 22(2), 94-98.
El Tecle, N. E., Abode-Iyamah, K. O., Hitchon, P. W., & Dahdaleh, N. S. (2015).
Management of spinal fractures in patients with ankylosing spondylitis.
Clin Neurol Neurosurg, 139, 177-182.
Fernandez-de-Las-Penas, C., Alonso-Blanco, C., Alguacil-Diego, I. M., &
Miangolarra-Page, J. C. (2006). One-year follow-up of two exercise
interventions for the management of patients with ankylosing spondylitis:
a randomized controlled trial. Am J Phys Med Rehabil, 85(7), 559-567.
Capítulo VII. Referências
116
Fernandez-de-las-Penas, C. s., Alonso-Blanco, C., Morales-Cabezas, M., &
Miangolarra-Page, J. C. (2005). Two Exercise Interventions for the
Management of Patients with Ankylosing Spondylitis. American Journal
of Physical Medicine & Rehabilitation, 84(6), 407-419.
Frauendorf, R., Medeiros Pinheiro, M. d., & Mesquita Ciconelli, R. (2013).
Variables related to work productivity loss in patients with ankylosing
spondylitis. Revista Brasileira de Reumatologia (English Edition), 53(3),
303-309.
Gunendi, Z., Sepici Dincel, A., Erdogan, Z., Aknar, O., Yanpal, S., Gogus, F., &
Atalay, F. (2010). Does exercise affect the antioxidant system in patients
with ankylosing spondylitis? Clin Rheumatol, 29(10), 1143-1147.
Hennell, S. L., Brownsell, C., & Dawson, J. K. (2004). Development, validation
and use of a patient knowledge questionnaire (PKQ) for patients with
early rheumatoid arthritis. Rheumatology, 43(4), 467-471.
Hulejova, H., Levitova, A., Kuklova, M., Stochl, J., Haluzik, M., Pavelka, K.,
Vencovsky, J., & Senolt, L. (2012). No effect of physiotherapy on the
serum levels of adipocytokines in patients with ankylosing spondylitis.
Clin Rheumatol, 31(1), 67-71.
Ince, G. S., T.; Durgun, B.; and Erdogan, S. (2006). Effects of a Multimodal
Exercise Program for People With Ankylosing Spondylitis. PHYS THER.,
86(7), 924-935.
Karapolat, H., Akkoc, Y., Sari, I., Eyigor, S., Akar, S., Kirazli, Y., & Akkoc, N.
(2008). Comparison of group-based exercise versus home-based
exercise in patients with ankylosing spondylitis: effects on Bath
Ankylosing Spondylitis Indices, quality of life and depression. Clin
Rheumatol, 27(6), 695-700.
Kaya, T., Bal, S., & Gunaydin, R. (2007). Relationship between the severity of
enthesitis and clinical and laboratory parameters in patients with
ankylosing spondylitis. Rheumatol Int, 27(4), 323-327.
Kisacik, B., Tufan, A., Kalyoncu, U., Karadag, O., Akdogan, A., Ozturk, M. A.,
Kiraz, S., Ertenli, I., & Calguneri, M. (2008). Mean platelet volume (MPV)

Capítulo VII. Referências
117
as an inflammatory marker in ankylosing spondylitis and rheumatoid
arthritis. Joint Bone Spine, 75(3), 291-294.
Kisacik, P., Unal, E., Akman, U., Yapali, G., Karabulut, E., & Akdogan, A.
(2016). Investigating the effects of a multidimensional exercise program
on symptoms and antiinflammatory status in female patients with
ankylosing spondylitis. Complementary Therapies in Clinical Practice, 22,
38-43.
Lazennec, J. Y., d'Astorg, H., & Rousseau, M. A. (2015). Cervical spine surgery
in ankylosing spondylitis: Review and current concept. Orthop Traumatol
Surg Res, 101(4), 507-513.
Lim, H. J., Moon, Y. I., & Lee, M. S. (2005). Effects of home-based daily
exercise therapy on joint mobility, daily activity, pain, and depression in
patients with ankylosing spondylitis. Rheumatol Int, 25(3), 225-229.
Londono, J., Romero-Sanchez, M., Torres, V., Bautista, W., Fernandez, D.,
Quiroga, J., Valle-Oñate, R., Santos, A., & Medina, J. (2012). The
association between serum levels of potential biomarkers with the
presence of factors related to the clinical activity and poor prognosis in
Spondyloarthritis. Rev Bras Reumatol, 52(4), 529-544.
Lubrano, E. H., P.; Moreno,P.; Griffiths, B.; Emery, P. and Veale, D. (1998).
The assessment of knowledge in ankylosing spondylitis patients by a
self-administered questionnaire. British Journal of Rheumatology, 37,
437–441.
Lucas, R., Monjardino MT. ( 2010). O Estado da Reumatologia em Portugal.
Observatório Nacional das Doenças Reumáticas (ONDOR).
Marcelo Cardozo de Souza, A. O., AnaMaria Jones, Fábio Jennings, Elisabeth
Biruel. (2012). Grupos educacionais para pacientes com espondilite
anquilosante: revisão sistemática. Revista Dor, 13 (3), 256-260.
Masiero, S., Bonaldo, L., Pigatto, M., Lo Nigro, A., Ramonda, R., & Punzi, L.
(2011). Rehabilitation treatment in patients with ankylosing spondylitis
stabilized with tumor necrosis factor inhibitor therapy: a randomized
controlled trial. J Rheumatol, 38(7), 1335-1342.
Capítulo VII. Referências
118
Millner, J. R., Barron, J. S., Beinke, K. M., Butterworth, R. H., Chasle, B. E.,
Dutton, L. J., Lewington, M. A., Lim, E. G., Morley, T. B., O'Reilly, J. E.,
Pickering, K. A., Winzenberg, T., & Zochling, J. (2015). Exercise for
ankylosing spondylitis: An evidence-based consensus statement. Semin
Arthritis Rheum.
Momeni, M., Taylor, N., & Tehrani, M. (2011). Cardiopulmonary manifestations
of ankylosing spondylitis. Int J Rheumatol, 2011, 728471.
Ortega Castro, R., Font Ugalde, P., Castro Villegas, M. C., Calvo Gutiérrez, J.,
Muñoz Gomariz, E., Zarco Montejo, P., Almodóvar, R., Mulero Mendoza,
J., Torre-Alonso, J. C., Gratacós Masmitjá, J., Juanola Roura, X., Ariza
Ariza, R., Fernández Dapica, P., Linares Ferrando, L. F., Brito Brito, M.
E., Cuende Quintana, E., Vázquez Galeano, C., Moreno Ramos, M. J.,
Giménez Úbeda, E., Rodríguez Lozano, J. C., Fernández Prada, M.,
Queiro Silva, R., Moreno Ruzafa, E., Júdez Navarro, E., Más, A. J.,
Medrano Le Quement, C., Ornilla, E., Montilla Morales, C., Pujol
Busquets, M., Clavaguera Poch, T., Fernández-Espartero, M. C.,
Carmona Ortell, L., & Collantes Estévez, E. (2013). Different Clinical
Expression of Patients With Ankylosing Spondylitis According to Gender
in Relation to Time Since Onset of Disease. Data From REGISPONSER.
Reumatología Clínica (English Edition), 9(4), 221-225.
Papini, C. B., Nakamura, P. M., Zorzetto, L. P., Thompson, J. L., Phillips, A. C.,
& Kokubun, E. (2014). The effect of a community-based, primary health
care exercise program on inflammatory biomarkers and hormone levels.
Mediators Inflamm, 2014, 185707.
Passalent, L. A. (2011). Physiotherapy for ankylosing spondylitis: evidence and
application. Curr Opin Rheumatol, 23(2), 142-147.
Pham, T. (2008). Pathophysiology of ankylosing spondylitis: what's new? Joint
Bone Spine, 75(6), 656-660.
Pimentel-Santos, F. M., Mourao, A. F., Ribeiro, C., Costa, J., Santos, H.,
Barcelos, A., Pinto, P., Godinho, F., Cruz, M., Vieira-Sousa, E., Santos,
R. A., Rabiais, S., Felix, J., Fonseca, J. E., Guedes-Pinto, H., Brown, M.
A., Branco, J. C., & Group, C. S. (2012). Spectrum of ankylosing
Capítulo VII. Referências
119
spondylitis in Portugal. Development of BASDAI, BASFI, BASMI and
mSASSS reference centile charts. Clin Rheumatol, 31(3), 447-454.
Plasqui, G., Boonen, A., Geusens, P., Kroot, E. J., Starmans, M., & van der
Linden, S. (2012). Physical activity and body composition in patients with
ankylosing spondylitis. Arthritis Care Res (Hoboken), 64(1), 101-107.
Ramiro, S. C., Helena; Branco JC. (2010). EpiReumaPt Protocol - Portuguese
epidemiologic study of the rheumatic diseases. Acta Reumatol Port, 35,
384-390.
Raychaudhuri, S. P., & Deodhar, A. (2014). The classification and diagnostic
criteria of ankylosing spondylitis. J Autoimmun, 48-49, 128-133.
Reveille, J. D., Ximenes, A., & Ward, M. M. (2012). Economic considerations of
the treatment of ankylosing spondylitis. Am J Med Sci, 343(5), 371-374.
Roxanne Cooksey, S. B., Muhammad Jmai Husain, Elizabeth Irvine, Helen
Davies, Stefan Siebert. (2012). The information needs of people living
with ankylosing spondylitis: a questionnaire survey. BMC Musculosketal
Disorders, 13, 243.
Schett, G., & Rudwaleit, M. (2010). Can we stop progression of ankylosing
spondylitis? Best Pract Res Clin Rheumatol, 24(3), 363-371.
Sieper, J., Braun, J., Rudwaleit, M., Boonen, A., & Zink, A. (2002). Ankylosing
spondylitis: an overview. Annals of the Rheumatic Diseases, 61(suppl 3),
iii8-iii18.
Silva, E. M., Andrade, S. C., & Vilar, M. J. (2012). Evaluation of the effects of
Global Postural Reeducation in patients with ankylosing spondylitis.
Rheumatol Int, 32(7), 2155-2163.
Song, I. H., Brenneis, C., Hammel, L., Feldtkeller, E., Listing, J., Sieper, J., &
Rudwaleit, M. (2015). Ankylosing spondylitis self-help organisations - do
members differ from non-members? Joint Bone Spine.
Ugur, M. B., N.; Melikoglu, M.; Baygutalp, F.; Altas, E; and Seferoglu, B.
(2015). Elevated serum interleukin-23 levels in ankylosing spondylitis
patients and the relationship with disease activity. Nagoya J. Med. Sci.,
77, 621-627.
Capítulo VII. Referências
120
Vastesaeger, N., van der Heijde, D., Inman, R. D., Wang, Y., Deodhar, A., Hsu,
B., Rahman, M. U., Dijkmans, B., Geusens, P., Vander Cruyssen, B.,
Collantes, E., Sieper, J., & Braun, J. (2011). Predicting the outcome of
ankylosing spondylitis therapy. Ann Rheum Dis, 70(6), 973-981.
Widberg, K., Karimi, H., & Hafstrom, I. (2009). Self- and manual mobilization
improves spine mobility in men with ankylosing spondylitis-a randomized
study. Clin Rehabil, 23(7), 599-608.
Xu, M., Lin, Z., Deng, X., Li, L., Wei, Y., Liao, Z., Li, Q., Wei, Q., Hu, Z., Zhang,
Y., Lin, Q., Huang, J., Li, T., Pan, Y., Wu, Y., Jin, O., Yu, B., & Gu, J.
(2011). The Ankylosing Spondylitis Disease Activity Score is a highly
discriminatory measure of disease activity and efficacy following tumour
necrosis factor-alpha inhibitor therapies in ankylosing spondylitis and
undifferentiated spondyloarthropathies in China. Rheumatology (Oxford),
50(8), 1466-1472.
Yigit, S., Sahin, Z., Demir, S. E., & Aytac, D. H. (2013). Home-based exercise
therapy in ankylosing spondylitis: short-term prospective study in patients
receiving tumor necrosis factor alpha inhibitors. Rheumatol Int, 33(1), 71-
77.
Younes, M., Jalled, A., Aydi, Z., Zrour, S., Korbaa, W., Ben Salah, Z., Letaief,
M., Bejia, I., Touzi, M., & Bergaoui, N. (2010). Socioeconomic impact of
ankylosing spondylitis in Tunisia. Joint Bone Spine, 77(1), 41-46.
Zarco, P., Florez, M., & Almodóvar, R. (2016). Expert Opinion of Spanish
Rheumatologists About the Role of Physical Exercise in Ankging
Spondylitis and Other Rheumatic Diseases. Reumatología Clínica
(English Edition), 12(1), 15-21.
Zochling, J., Braun, J., & Désirée van der Heijde, D. (2006). Assessments in
ankylosing spondylitis. Best Pract Res Clin Rheumatol, 20(3), 521-537.
Anexos _______________________________________________________________

Anexos
XXV
Anexo I. Aprovação pela Comissão de Ética.

Anexos
XXVII
Anexo II. Consentimento informado.