carcinoma pancreático aspectos gerais pancreatic ... · carcinoma pancreático – aspectos gerais...
TRANSCRIPT

Sofia Eduarda Tavares Sousa Castro
Carcinoma Pancreático – Aspectos Gerais
Pancreatic Adenocarcinoma – An overview
2009/2010
Abril, 2010

Sofia Eduarda Tavares Sousa Castro
Carcinoma Pancreático – Aspectos Gerais
Pancreatic Adenocarcinoma – An overview
Mestrado Integrado em Medicina
Área: Cirurgia Geral
Trabalho efectuado sob a Orientação de:
Prof. Doutor António Taveira Gomes
Abril, 2010
Revista:
World Journal of Surgical Oncology


Projecto de Opção do 6º ano - DECLARAÇÃO DE INTEGRIDADE
Eu, _ Sofia Eduarda Tavares Sousa Castro ____________, abaixo assinado, nº
mecanográfico_040801148____, aluno do 6º ano do Mestrado Integrado em Medicina, na
Faculdade de Medicina da Universidade do Porto, declaro ter actuado com absoluta integridade
na elaboração deste projecto de opção.
Neste sentido, confirmo que NÃO incorri em plágio (acto pelo qual um indivíduo, mesmo por
omissão, assume a autoria de um determinado trabalho intelectual, ou partes dele). Mais
declaro que todas as frases que retirei de trabalhos anteriores pertencentes a outros autores,
foram referenciadas, ou redigidas com novas palavras, tendo colocado, neste caso, a citação da
fonte bibliográfica.
Faculdade de Medicina da Universidade do Porto, 19 / 04 / 2010__
Assinatura: ________________________________________________

Projecto de Opção do 6º ano - DECLARAÇÃO DE REPRODUÇÃO
Nome: Sofia Eduarda Tavares Sousa Castro
Endereço electrónico: [email protected] Telefone ou Telemóvel: 917032226
Número do Bilhete de Identidade: 12942726
Título da Dissertação/Monografia/Relatório de Estágio:
Carcinoma Pancreático – Aspectos Gerais / Pancreatic Adenocarcinoma – An Overview
Nome completo do Orientador:
Professor Doutor António Taveira Gomes
Nome completo do Co-Orientador:
_____________________________________________________________________________
Ano de conclusão: _2010______
Designação da área do projecto de opção:
Cirurgia Geral
É autorizada a reprodução integral desta Dissertação/Monografia/Relatório de Estágio (cortar o
que não interessar) apenas para efeitos de investigação, mediante declaração escrita do
interessado, que a tal se compromete.
Faculdade de Medicina da Universidade do Porto, 19 / 04 / 2010_
Assinatura: ________________________________________________

1
Carcinoma Pancreático – Aspectos gerais
Pancreatic Adenocarcinoma – An Overview
Sofia Eduarda Tavares Sousa Castro1§
1Student from Faculty of Medicine University of Porto, Porto, Portugal
§Corresponding author:
Email Address: [email protected]; [email protected].

2
INDEX
Abstract 4
Resumo 5
Introduction 6
Epidemiology 7
Risk Factors 9
Environmental Factors 9
Smoking 9
Dietary Factors 10
Pre-Existing Diseases 11
Chronic Pancreatitis and other Digestive Diseases 11
Diabetes 12
Genetic Factors 13
Percursor Lesions 16
Mucinous Cystic Neoplasms (MCNs) 16
Intraductal Papillary Mucinous Neoplasms (IPMNs) 17
Pancreatic Intraepithelial Neoplasias (PanINs) 19
Ductal Adenocarcinoma 20
Diagnosis 21
Clinical Findings 21
Laboratory Studies 22
Imaging Studies 25
Transabdominal Ultrasound 26
Computed Tomography (CT) 26
Magnetic Resonance Imaging (MRI) 27
Endoscopic Ultrasound (EUS) 29
Biopsy 30
Endoscopic Retrograde Cholangiopancreatography 31

3
Laparoscopy 32
Positron Emission Tomography (PET) 32
Staging and Resectability 34
Distinction between Resectable, Locally Advanced and Metastatic disease 35
Borderline Resectable Disease 37
Surgical Treatment 38
Resection for Tumors of the Head of the Pancreas 39
Pancreaticoduodenectomy (Kausch-Whipple procedure) 39
Pylorus-Preserving Pancreaticoduodenectomy (PPPD) 40
Pancreatic Anastomosis and Reconstruction 40
Resection for Tumors of the Body/Tail of the Pancreas 42
Distal Pancreatectomy 42
Central Pancreatectomy 42
Total Pancreatectomy 43
Extended Lymphadenectomy – Extended Lymph Node Dissection 43
Arterial/Venous Resections 44
Short-Term Outcome 44
Long-Term Outcome 45
Chemoradiotherapy 47
Palliation Treatment 52
Biliary Obstruction 52
Gastric Outlet Obstruction 52
Severe Abdominal Pain 53
Pancreatic Insufficiency 53
Conclusions 54
Acknowledgements 55
References 56
Figures 70
Tables 71

4
ABSTRACT
Pancreatic cancer remains a fearsome disease. This article focuses on the epidemiology,
pathogenesis, diagnosis, staging, and treatment of pancreatic adenocarcinoma.
Smoking has been clearly established as a major risk factor affecting the carcinogenesis
of pancreatic cancer. Other risk factors are still to be confirmed.
Different genetic alterations have been observed in pancreatic adenocarcinoma and new
developments have been made in our understanding on progression from benign lesion to
invasive cancer.
Imaging studies play a crucial role in the diagnosis, staging and management of patients
with pancreatic adenocarcinoma and computed tomography is the most widely used and best-
validated imaging method.
Surgery remains the single most important modality for curative treatment of pancreatic
adenocarcinoma, however, it can only be performed in about 10-15% of the patients. Surgery
for this disease is a complex procedure associated with considerable perioperative morbidity and
mortality. Many aspects of surgery for pancreatic adenocarcinoma, such as the extent of
resection and limphadenectomy, the value of vascular resection, and the importance of treatment
by experienced surgeons, are currently under debate.
Adjuvant treatment improves survival after surgical resection and each patient should be
offered this treatment option. However, a standard treatment protocol has not been established
yet.
For the majority of patients, treatment is palliative and may include surgery or endoscopic
or percutaneous stenting to relieve obstructive jaundice or gastric obstruction, other
interventional radiological techniques, chemotherapy or radiotherapy. Adequate pain relief and
treatment of pancreatic insufficiency are also important components of treatment.

5
RESUMO
O cancro do pâncreas continua a ser uma doença temível. Este artigo aborda a
epidemiologia, patogénese, diagnóstico, estadiamento e tratamento do adenocarcinoma
pancreático.
O tabaco é um factor de risco claramente estabelecido na carcinogénese desta neoplasia.
Outros factores de risco estão ainda por confirmar.
Diferentes alterações genéticas foram observadas nas neoplasias pancreáticas e novos
desenvolvimentos têm sido feitos na compreensão da progressão de uma lesão benigna para
carcinoma invasivo.
Os estudos imagiológicos são cruciais no diagnóstico, estadiamento e abordagem de
doentes com adenocarcinoma pancreático e a tomografia computorizada é o método de imagem
mais usado e validado.
A cirurgia mantém-se como a estratégia terapêutica curativa mais importante, contudo,
esta só pode ser realizada em cerca de 10-15% dos doentes. A cirurgia para esta patologia é
complexa e está associada a uma morbilidade e mortalidade perioperatória consideráveis.
Diversos aspectos desta continuam em discussão, como a extensão de ressecção e da
linfadenectomia, o valor da ressecção vascular e a importância da realização do tratamento por
cirurgiões experientes.
O tratamento adjuvante melhora a sobrevida após ressecção e esta opção deve ser
oferecida aos doentes. Contudo, ainda não foi estabelecido um protocolo terapêutico standard.
Para a maioria dos doentes, o tratamento paliativo pode incluir procedimentos cirúrgicos
ou colocação de stents via endoscópica ou percutânea para aliviar icterícia obstrutiva ou
obstrução gástrica; outras técnicas radiológicas de intervenção, quimioterapia ou radioterapia.
Alívio adequado da dor e tratamento da insuficiência pancreática são também componentes
importantes do tratamento.

6
INTRODUCTION
Pancreatic adenocarcinoma remains one of the most feared gastrointestinal tract
malignancies. It has the highest ratio of diagnosis to mortality.[1-2] Most patients die within a
year after establishment of the diagnosis[3], and the overall prognosis is dismal, with a 5-year
survival rate of <5% [2, 4]. The reasons for this low survival are related to late diagnosis and to
the aggressive biology of this disease: early development of retroperitoneal and perineural
infiltration, angioinvasion, peritoneal, lymphogenic, and hematogenic dissemination, and
resistance to most of the available treatment regimens.[5-6] Thus, this makes patient
management a complex and challenging task.
Despite this grim picture, significant advances have been made in recent years, both in
our understanding of the molecular behavior and pathogenesis of this disease and in its clinical
management.[6-7] Better prognosis could be achieved by combining earlier diagnose (with
markers and modern imaging techniques), surgery, and chemotherapy/radiotherapy with
targeted molecular and immune therapies. [6] Therefore, the main focus of academic medicine
in the field of pancreatic adenocarcinoma will be translational research, transferring advances
from basic research to clinical studies for the benefit of patients.[6]
This article has the objective of reviewing the current knowledge on many aspects
concerning pancreatic adenocarcinoma, like epidemiology and risk factors, as well as the recent
developments in molecular genetics and disease progression. Moreover, it has the purpose of
updating the current thinking on management of this malignant disease, including diagnosis,
staging, surgical resection, adjuvant therapy, and palliation.

7
EPIDEMIOLOGY
Over the last few decades, the study of pancreatic cancer has assumed a position of
growing importance because of its increasing incidence and poor prognosis.[8] Ductal
adenocarcinoma is the most common form of pancreatic cancer.[9]
In Europe, pancreatic cancer is the tenth most frequent cancer, accounting for 3% of
cancer in both sexes and in the year 2000 an estimated 74 000 new cases were diagnosed.[10]
In the United States pancreatic cancer develops in approximately 30,000 patients per
year, and about 20,000 annual cases in Japan. Compared with more common tumors such as
lung, breast, colon, or prostate tumors, it is a rare cancer.[11-12] However, because it is so
lethal, it ranks fourth as cause of death from cancer [11], with 80–90% of cases diagnosed in the
non-resectable stage. Consequently, the survival rate is extremely low.[8] For all stages
combined, the 1-year survival rate is 19% and the 5-year survival rate is 4%. Survival is low
because of the late development of clinical symptoms. Surgical resection (when margin negative
and node negative) offers the best possibility for cure in pancreatic cancer, with the 5-year
survival rate improving to 40%, when performed at specialized medical institutions.[9]
With the rapid advancement of effective screening and therapeutic regimes for breast and
colon cancer resulting in decreased deaths from these diseases, pancreatic cancer is likely to
become an increasingly frequent cause of death from cancer.[11]
In North America, the incidence rate of pancreatic cancer has remained constant or has
declined slightly during the last 25 years, while its frequency tend to rise in Japan and in
virtually all European countries.[7-9]
As with nearly all other types of digestive tract cancer, pancreatic cancer exhibits an
uneven world distribution. Incidence rates in high-risk countries are about 5–7 times higher than
incidence rates in low-risk countries, implying that environmental factors play an important
role.[13] There is substantial geographical variation in incidence of pancreatic cancer with the
highest rates being seen in the USA (particularly in black men), Europe and in other western,
industrialized countries.[7-8, 10-11, 14] The lowest rates are generally found in Africa and some
8
Asian countries, although Japan, which has seen a substantial increase in rates in recent decades,
now has rates similar to those seen in the USA.[10]
There may be also racial differences in survival patterns after diagnosis of pancreatic
cancer, perhaps related to racial differences in aggressiveness of tumor type.[11] Asian patients
tended to have less aggressive tumors.[13] In Europe, the highest mortality rates occur in
Austria and Sweden and in southern Europe (Spain, Portugal and Greece) the corresponding
rates are generally lower.[10]
Moreover, in all cancer registries, pancreatic cancer is slightly more common in males
than in females.[8-9, 12]
Pancreatic cancer is predominately a disease of older individuals.[13] Incidence rates
increase steadily with age, with over 80% of cases occurring between the ages of 60 and 80[7-
8], with the average age at diagnosis being 60 to 65 years[9]. The diagnosis of pancreatic
cancer in individuals younger than age 40 is uncommon and is rare in people under 25 years of
age.[7-8]

9
RISK FACTORS
The causes of all types of disease fall along a continuum ranging from diseases where a
genetic mutation causes all cases, to a purely environmental disease. Environmental factors are
believed to be the most important cause of most types of cancer, including pancreatic cancer,
although there are subgroups of patients where genetic factors are important.[12]
Environmental Factors
Smoking
For more than 30 years, we have known that exposure to tobacco smoke is the most
important environmental factor leading to pancreatic cancer.[11-12]
Pancreatic cancer is unquestionably one of the major smoking related tumors. Unlike the
lung, where tobacco smoke and tobacco degradation products are in direct contact with
pulmonary tissue, the pancreas is exposed to tobacco products indirectly. Tobacco-related
carcinogens reach the pancreas either via the blood stream, or perhaps through exposure to
either duodenal contents or to bile. Most pancreatic cancers occur in the head of the gland and
this region is where exposure to tobacco carcinogens contained in the duodenal juice or bile
could occur.[11]
Since exposure to tobacco products is lower in the pancreas than in the lung, it is
understandable that the smoking-related risk of pancreatic cancer is not as high as that of lung
cancer.[11] Most studies have found that smoking results in about a two-fold increased risk of
pancreatic cancer. [9-14] Also, it has been demonstrated a graded dose response, with heavy
smokers having a substantially higher risk.[13]
Based on current smoking prevalence rates it has been estimated that it contributes to the
development of almost 30% of all pancreatic cancers.[9-10, 12-13] Differential smoking rates
10
cause much of the gender-specific and country-specific differences in pancreatic cancer
rates.[12]
As a public health measure avoiding smoking will substantially reduce the risk of
pancreatic cancer.[12] Smoking cessation is also beneficial, but it takes about 15 years after
quitting cigarette smoking, among the heaviest smokers, for the risk to fall to a level comparable
with that in never-smokers.[8]
Dietary Factors
Some of the strongest evidence for the importance of dietary factors comes from the
several-fold differences observed in incidence rates in various countries. Dietary differences
would explain some of the wide variation in incidence rates for pancreatic cancer. However,
attempts to associate specific dietary items with an increased or decreased risk have been
frustrating. Nearly 500 published articles have examined the link between pancreatic cancer and
various dietary items. In most of these reports there is a possibility for recall bias, which would
explain why the results are often contradictory.[12]
Several studies show that caloric consumption and/or obesity can be risk factors for
pancreatic cancer. [12] Diet high in vegetables and fruits are probably protective against
pancreatic cancer, and the diets containing substantial amounts of red meat and cholesterol
possibly increase risk.[10]
Alcohol is a major risk factor for pancreatitis, but does it cause pancreatic cancer? Nearly
all studies fail to support this association. Coffee, another widely consumed beverage is also
unlikely to cause pancreatic cancer.[13]

11
Pre-Existing Diseases
Are there pre-existing diseases that increase the risk of pancreatic cancer? For other
digestive tract organs, there are established links between the occurrence of a nonmalignant
disease and the eventual appearance of cancer in the same organs. Therefore, it is reasonable to
assume that non-malignant pancreatic disorders would increase the risk of pancreatic
cancer.[12]
Chronic Pancreatitis and other Digestive Diseases
Chronic pancreatitis develops in people who have had repeated attacks of acute
pancreatitis.[11] Several studies have now linked chronic pancreatitis with an increased risk of
pancreatic cancer.[12-13, 15-16] Most patients are males who smoke and drink heavily,
although „„idiopathic‟‟ pancreatitis can develop in persons without any history of heavy
drinking.[11]
Hereditary pancreatitis is a rare inherited disease with symptoms that mimic other types
of chronic pancreatitis. It is an autosomal dominant disease with an onset in childhood or early
adulthood [12] and with a penetrance of 80% [8, 11]. Cystic fibrosis affects the digestive tract,
including the pancreas: a few patients with pancreatic cancer have been reported with this
disease.[13] Finally, there is a type of chronic pancreatitis occurring in persons living in the
southern parts of India or Africa. This disease of unknown etiology has been termed tropical
pancreatitis.[11]
In all types of pancreatitis, the risk of pancreatic cancer is elevated. For example, patients
with idiopathic or alcoholic pancreatitis have a 15-fold increased risk of pancreatic cancer. For
those patients with hereditary pancreatitis, the lifetime risk of pancreatic cancer is
approximately 30%–40%; for patients with tropical pancreatitis the risk of pancreatic cancer is
also high.[11]

12
The link between chronic pancreatitis and pancreatic cancer is similar to the well known
increased cancer in other digestive organs where there is a background inflammatory
disease.[11] Thus, increased cell turnover and defected DNA could increase the possibility of
coding errors leading to deleterious mutations.[11-12]
Both gallstone disease and peptic ulcer disease have been suggested as possible
preexisting diseases that might cause pancreatic cancer, but the evidence is weaker than for
chronic pancreatitis.[7, 13]
Diabetes
Diabetes is a common disorder found in 5–10% of the general population [12-13] and it
has been associated with pancreatic cancer for a long time.[15]
The possible role of diabetes in the etiology of pancreatic cancer has been examined with
conflicting results by several investigators. There is an increased frequency of pancreatic cancer
among individuals with a long history of diabetes. Diabetes is an early manifestation of
pancreatic dysfunction, and it may play a causative role in the development of pancreas cancer
in subjects with a long history of diabetes.[8]
As pancreatic cancer is a rapidly progressing disorder with high mortality within 1 year of
diagnosis, it is unlikely to lead to the development of diabetes many years prior to its diagnosis.
Approximately 50% of individuals with diabetes are not aware of their disease, and non-insulin
dependent diabetic patients can live with their undiagnosed condition for extended periods of
time.[8]
A significant proportion of the cases simultaneously diagnosed with diabetes and
pancreatic cancer probably had diabetes for several years before their cancer was detected, but
the diabetes was only discovered during the exploration of pancreas dysfunction and cancer.[8]
As yet, there is no evidence that screening recent onset diabetics would reduce the
mortality from pancreatic cancer.[12]

13
Genetic Factors
The accumulation of multiple nonrandom genetic changes over time is a hallmark of
pancreatic cancer. Genetic abnormalities include alterations in chromosome or gene copy
number, microsatellite instability, epigenetic silencing, intragenic point mutations, and gene
overexpression secondary to increased transcription.[17-18]
Chromosome losses are more common than chromosome gains in pancreatic cancer.
Some of the most common regions of genomic loss in pancreatic cancers contain known tumor
suppressor genes such as CDKN2A/P16/MTS1 (9p21), p53 (17p13), and
MADH4/SMAD4/DPC4 (18q).[17, 19] Frequent gains of DNA have been observed in
pancreatic cancers in several chromosomes (for example in 12p – location of KRAS2
oncogene).[17]
Medullary carcinoma, a rare subtype of pancreatic adenocarcinoma, often contains a
defective DNA mismatch repair mechanism which gives rise to microsatellite instability.[17,
20]
Epigenetic phenomena are DNA modifications that do not involve alterations in DNA
sequence [17, 21] (chromatin structural changes, such as histone modifications and nucleosome
rearrangements, and deregulation of cytosine methylation at the promoter site) [17]. The
expression of many tumor suppressor genes and oncogenes appears to be influenced through
this mechanism.[17]
Many tumor suppressors regulate cell proliferation. Therefore, biallelic inactivation of
these genes can provide a growth advantage for tumors. Conversely, oncogenes promote cell
growth.[17]
CDKN2A/p16/MTS1 is the most frequently inactivated tumor suppressor gene in
pancreatic cancer (95%).[17, 22-23] The gene can be inactivated through homozygous deletion
(40%), single allele loss combined with an intragenic mutation in the second allele (40%), or
promoter hypermethylation (15%). When p16 is inactivated, progression through the G1/S cell
cycle checkpoint is facilitated.[17, 24]
14
p53 is the second most commonly inactivated tumor suppressor gene in pancreatic cancer
(50-75%). Usually, one p53 allele is deleted while the other allele acquires an intragenic
mutation.[17, 24] Activated p53 causes the cell to arrest in G1 or G2 of the cell cycle and
responds to genetic injury by activating apoptotic pathways. Thus, p53 inactivation allows the
tumor to proliferate despite the continued accumulation of genetic defects.[17]
MADH4/SMAD4/DPC4 is the third most frequently inactivated tumor suppressor gene in
pancreatic cancer (55%). SMAD4 is a downstream component of the transforming growth
factor (TGF) and activin signaling pathways. Loss of SMAD4 impairs the cell cycle check
mechanism during the G1/S transition. SMAD4 loss is also believed to affect pro-apoptotic
signaling.[17]
BRCA2 is altered in 7% of pancreatic cancers, but germline mutations can be seen in a
larger proportion of patients (17%) that cluster in pancreatic cancer families.[17]
KRAS2 is the most commonly mutated oncogene in pancreatic cancer (90%). Gain-of-
function mutations that impair KRAS2 GTPase activity augment downstream signaling and
increase cell proliferation.[17]
Individuals with a strong family history of pancreatic cancer have a significantly
increased risk of developing the disease. For example, individuals with a first-degree relative
with pancreatic cancer have a 2,3-fold increased risk.[25]
Five hereditary tumor predisposition syndromes associated with pancreatic cancer have
been identified so far, although these known syndromes account for only a minority (<20%) of
familial cases.
Hereditary nonpolyposis colorectal cancer (HNPCC) is an autosomal dominant disorder
responsible for roughly 3% of colorectal cancers, and has an estimated population prevalence of
1:740. Individuals with HNPCC have a 1-5% lifetime risk of developing pancreatic cancer.[17]
The pancreatic carcinomas that arise in these patients often have a “medullary histology”.[9]
Peutz-Jeghers syndrome (PJS) is an autosomal dominant disorder with an incidence of
1:25 000. The disease is characterized by mucocutaneous pigmentations and hamartomatous

15
intestinal polyps, due to mutations in the STK11/LKB1 gene.[17] Patients with PJS have a 132
fold increased risk of developing pancreatic cancer.[9, 17]
Familial atypical multiple mole-melanoma syndrome (FAMMM) is associated with
multiple nevi, melanomas, and extracutaneous tumors. The disease is caused by a mutation in
CDKN2A/p16 and accounts for approximately 12% of familial pancreatic cancers.[17] Affected
individuals have a 20-fold increased risk for developing pancreatic cancer.[9, 17]
Familial breast and ovarian cancer syndrome is due to mutations in the BRCA1 or
BRCA2 genes. Individuals with germline BRCA1 mutations have a twofold risk increase of
pancreatic cancer; those with BRCA2 mutations have between a 4 and 13-fold risk increase.[17]
Inherited BRCA2 mutations are responsible for roughly 17% of familial pancreatic cancer
cases, which makes BRCA2 the most common inherited defect contributing to pancreatic cancer
identified to date.[9, 17] Of interest, not all patients with pancreatic cancer and a germline
BRCA2 mutation come from classical BRCA2 families. In fact, some have no family history of
breast cancer.[9]
In addition to the above described familial cancer predisposition syndromes, familial
pancreatic cancer can be associated with hereditary pancreatitis. It is an autosomal dominant
disease caused in 70% of the cases by a mutation in PRSS1 gene, leading to pancreatic auto-
digestion. Affected individuals have a 50-fold increased risk of developing pancreatic
cancer.[17] Patients with hereditary pancreatitis have development of severe pancreatitis at a
young age, may have pancreatic pseudocysts and diabetes [9], and have a 50-fold increased risk
for development of pancreatic cancer [9, 17].
In the overwhelming majority (~80%) of familial pancreatic cancer cases, the underlying
genetic predisposition remains unknown.[17]
At present, screening patients with germ line mutations known to be associated with
pancreatic cancer has not been widely used. The patients most likely to benefit from screening
would be patients with a strong family history of pancreatic cancer and patients with hereditary
pancreatitis.[12]

16
PRECURSOR LESIONS
One of the most exciting developments has been a dramatically improved understanding
of the non-invasive precursor lesions that give rise to invasive pancreatic cancer. [26] The early
detection and treatment of noninvasive precursor lesions provide the best hope for reducing
mortality.[27]
Our current understanding of pancreatic neoplasia suggests that invasive pancreatic
carcinoma can arise from noninvasive mucinous cystic neoplasms (MCNs), Intraductal papillary
mucinous neoplasms (IPMNs), and Pancreatic intraepithelial neoplasia (PanINs).[28-29]
Mucinous Cystic Neoplasms (MCNs)
The MCN is a cystic neoplasm composed of mucin-producing epithelial cells.[27, 30-31]
By definition, MCNs are associated with an ovarian type of stroma and the vast majority does
not communicate with the larger pancreatic ducts. [17, 25, 31-32]
The degree of dysplasia can range from minimal dysplasia (MCN with low-grade
dysplasia – adenoma), to moderate cytological and architectural atypia (MCN with moderate
dysplasia – borderline), to significant architectural and cytological atypia (MCN with high-
grade dysplasia – carcinoma in situ).[27] One-third of MCNs have an associated invasive
carcinoma.[27, 30] The invasive carcinoma associated with MCN is usually a ductal type of
adenocarcinoma.[27, 30, 33]
Of note is that a spectrum of dysplasia can be present in a single MCN (mild dysplasia
adjacent to epithelium with marked dysplasia). Similarly, invasive carcinoma can arise focally
in an otherwise benign-appearing MCN.[27, 30] Therefore, because invasive carcinoma can be
focal, MCNs need to be completely resected surgically to rule out a focal malignancy; biopsy of
a MCN is likely to underestimate the degree of dysplasia, or even miss an invasive
carcinoma.[27]
17
Clinical, pathological, and molecular observations have established that a MCN with mild
dysplasia can progress to moderate dysplasia, and from there to carcinoma in situ. It is clear that
if left untreated, noninvasive MCN can progress to invasive carcinoma.[27, 32, 34-35] This
progression is associated with the accumulation of genetic alterations in cancer-associated
genes, including KRAS, TP53, and SMAD4/DPC4. [27, 31-32, 36-39]
The good news is that noninvasive MCNs are curable. MCNs are localized lesions;
multifocality is rare, and therefore the surgical resection of a single neoplasm can be
curative.[27]
Intraductal Papillary Mucinous Neoplasms (IPMNs)
IPMNs are papillary mucin-producing pancreatic neoplasms with prominent intraductal
growth.[27, 31] Noninvasive IPMNs are classified into: IPMN with low-grade dysplasia
(adenoma), IPMN with moderate dysplasia, and IPMN with high-grade dysplasia (carcinoma in
situ).[27] Approximately one-third of IPMNs have an associated invasive carcinoma.[27, 40]
The distinction between a noninvasive IPMN and an IPMN with an associated invasive
carcinoma is clinically critical because the presence or absence of invasion is the most important
clinical prognostic factor. Like for MCN, the invasive carcinoma in IPMNs can be very focal,
and therefore a benign diagnosis cannot be established on biopsy alone.[27]
In half of IPMNs with an associated invasive carcinoma, it has a colloid or
“muconodular” pattern of invasion, and the other half has a “tubular” or conventional ductal
pattern.[39-41] This distinction is important because the prognosis is significantly better for
patients with an IPMN with an associated invasive colloid carcinoma.[31, 41-42]
Noninvasive IPMNs can progress from IPMN with mild dysplasia, to IPMN with
moderate dysplasia, to IPMN carcinoma in situ, and to invasive carcinoma.[43] At the
molecular level, the frequency of KRAS gene mutations in IPMNs increase with increasing
grades of dysplasia.[44-45] It suggests that it takes years for noninvasive IPMNs to progress to

18
an invasive cancer, and that the treatment of a noninvasive IPMN can save lives by interrupting
the progression.[27]
IPMNs that arise in the main pancreatic duct are classified as “main-duct-type” IPMNs,
while those that arise in the secondary branches are referred to as “branch-duct-type”
IPMNs.[25, 43, 46-48] “Combined-type” IPMNs involve both the main- and branch ducts.
Branch-duct IPMNs are less likely to harbor an invasive carcinoma [27, 48] and less likely to
progress to invasive cancer[27].
A number of histologic subtypes of IPMNs have also been identified based on the
direction of differentiation of the neoplastic epithelial cells:
IPMNs “intestinal-type” because they resemble villous adenomas of the large
intestine, they express an intestinal pattern of mucins (MUC2 and MUC5AC-positive,
and MUC1-negative), and they express CDX2, a transcription factor and determinant
of intestinal differentiation.[28, 31-32, 42, 49-53]
“Gastric foveolar” type of IPMN, often seen in branch-duct-type IPMNs, and usually
express MUC5AC, and are MUC1 and MUC2 negative.[28, 31-32, 53]
“Pancreatobiliary type” of IPMNs are usually MUC2 negative, and MUC1 and
MUC5AC positive.[28, 31-32, 50, 53]
Intraductal oncocytic papillary neoplasm (IOPN) usually express MUC1 and
MUC5AC, but are MUC2 negative.[28, 31-32, 53-54]
The morphological classification of IPMNs has clinical significance. Intestinal-type,
when with invasive carcinoma, is often associated with invasive colloid carcinomas (that also
strongly express MUC2 and are MUC1 negative) (Figure 1).[41, 49, 53] Pancreatobiliary-type
IPMNs, when with invasive cancer, are usually associated with a tubular type of ductal
adenocarcinoma (that are also usually MUC1 positive and MUC2 negative) (Figure 1).[49-50,
53] These associations are important because invasive colloid carcinomas appear to have a
significantly better prognosis than invasive tubular-type adenocarcinomas of the pancreas.[41] It
should be noted that there is a significant overlap in the groups, and that a single IPMN can
contain more than one type of epithelium. The prognosis of patients with a noninvasive IPMNs

19
is significantly better than for patients with an IPMN with an associated invasive
carcinoma.[27]
Although MCNs are almost always unifocal, the same is not true for IPMNs. As many as
30% of IPMNs are grossly multifocal.[42, 55-56] It suggests that patients with one IPMN are at
risk of developing additional IPMNs, and therefore they need to be followed carefully.[40, 42,
57-58] Most IPMNs are large enough to be detected clinically. We have the opportunity to save
patients by treating noninvasive IPMNs before they progress to invasive cancer.[27]
Pancreatic Intraepithelial Neoplasia (PanINs)
PanIN is defined as a microscopic noninvasive neoplastic epithelial proliferation in the
pancreatic duct system.[59-60] PanIN lesions have been classified into three grades: PanIN-1
has only mild dysplasia, PanIN-2 has moderate cytological and architectural atypia, and PanIN-
3 has marked dysplasia. As with MCNs and IPMNs, PanINs can progress from PanIN-1 to
PanIN-2 to PanIN-3 and to infiltrating ductal adenocarcinoma (Figure 1).[25, 31-32, 61-63]
PanINs do not express MUC2 regardless of the grade of atypia, but generally express
MUC5AC.[28, 41] MUC1 immunoreactivity is identified in the majority of high-grade PanINs
and invasive adenocarcinoma.[27]
The progression of noninvasive PanIN lesions to invasive ductal adenocarcinomas of the
pancreas suggests a huge opportunity to treat and cure pancreatic neoplasia before it progresses
to an incurable invasive cancer. However, most PanINs are too small to be detected using
available imaging technologies. Remarkably, PanINs, even the low-grade PanIN-1 lesions, were
associated with lobular parenchymal atrophy.[64]
The larger lesions, IPMNs and MCNs, can readily be detected using available imaging
techniques, and new findings suggest that even the smaller PanIN lesions may be detectable
because of the lobular parenchymal atrophy they may produce. Once detected, precursor lesions
in the pancreas can be treated, thereby preventing the development of a lethal cancer.[27]

20
DUCTAL ADENOCARCINOMA
Pancreatic ductal adenocarcinoma remains a formidable challenge because of the lack of
early diagnostic tests and effective therapies.[65]
Ductal adenocarcinoma accounts for >80% of pancreatic cancers. Grossly, they are
white/yellow and firm masses. Sixty percent of the cases arise in the pancreatic head, 15% in the
body or tail, and 20% involve the gland diffusely. They are characterized microscopically by
infiltrating small glands that are lined with low-columnar, mucin-containing cells. Typically, a
strong desmoplastic reaction occurs around the cancer. [17, 66]
Ductal adenocarcinomas are highly aggressive cancers with frequent invasion of vascular,
lymphatic, and perineural tissue. Approximately 80% of surgical specimens show disease in
regional lymph nodes. There is clinically evident disease at distant organ sites in up to 80% of
all patients who are discovered to have pancreatic adenocarcinoma. The most common sites for
distant metastases are the liver (80%), peritoneum (60%), lung and pleura (50-70%), and
adrenal glands (25%).[17, 66]
Complete surgical resection offers the best hope for long-term control of the disease,
although only approximately 30% of patients present with potentially resectable disease by
imaging studies, and less than 20% of all patients ultimately undergo resection. [65] The 5-year
survival rate for all patients with pancreatic ductal adenocarcinoma is <5%. The 5-year survival
rate is 15-25% in patients who undergo surgery, and 30-40% in patients who undergo surgery
with small tumors and node-negative disease.[17]
Other rare primary non-endocrine tumors of the pancreas include adenosquamous
carcinoma, acinar cell carcinoma, giant cell carcinoma, giant cell carcinoma with osteoclast-like
giant cells, pancreatoblastoma, serous cystadenoma/cystadenocarcinoma, and solid
pseudopapillary (Hamoudi) neoplasm.[17, 66]

21
DIAGNOSIS
Clinical Findings
The early symptoms of pancreatic adenocarcinoma include anorexia, weight loss,
abdominal discomfort, and nausea. Unfortunately, the nonspecific nature of these symptoms
often contributes to a delay in diagnosis. Specific symptoms usually only develop after invasion
or obstruction of a nearby structure.[7, 9]
As most pancreatic adenocarcinomas arise in the head of the pancreas, obstruction of the
biliary tree (mainly in the intrapancreatic portion of the common bile duct) resulting in jaundice
is the hallmark presentation. Jaundice is progressive and often associated with dark urine, light
stools and significant pruritus.[7, 9]
Pain is a common symptom of pancreatic adenocarcinoma. The most common pain
pattern is described by patients as a dull epigastric pain often accompanied by back pain, worse
in the supine position, and relieved by sitting forward. Pain can be caused by invasion of the
tumor into the splanchnic plexus and retroperitoneum, as well as by obstruction of the
pancreatic duct. Although intractable pain is frequently associated with pancreatic
adenocarcinoma, it is seldom an early manifestation, with fewer than one-third of patients
presenting with moderate to severe pain.[7]
Other symptoms found in a small percentage of patients include nausea and vomiting
related to gastro-duodenal obstruction. Mechanical obstructions of the proximal duodenum by
right-sided neoplasms, or at the ligament of Treitz by cancers of the midbody of the pancreas
are often later findings of pancreatic adenocarcinoma and suggest relatively advanced
disease.[7, 9]
At times, pancreatic adenocarcinoma may present in an unusual manner. New-onset
diabetes may be the first clinical feature in approximately 10% to 20% of patients.[7, 9-10]
Occasionally pancreatitis may also be the first signal, especially in the elderly when there is no
obvious cause such as gallstones or alcohol abuse.[9-10]
22
The most common physical findings at the time of initial examination are scleral icterus
and jaundice in patients with cancer of the head of the pancreas, while patients with tail and
body tumors may complain only of pain without any other specific sign. [7, 9-10] Often,
patients with deep jaundice will exhibit cutaneous signs of scratching, related to the pruritis.
Hepatomegaly and a palpable gallbladder may also be found.[9-10] In cases of advanced
disease, there may be evidence of cachexia, muscle wasting, or an enlarged, nodular liver
consistent with metastatic disease. In patients with advanced cancer, ascites, left supraclavicular
adenopathy (Virchow‟s node), periumbilical lymphadenopathy (Sister Mary Joseph‟s nodes) or
findings of dropped metastasis in the pelvis encircling the perirectal region (Blumer‟s shelf)
may be present.[7, 9]
Laboratory Studies
Results of laboratory studies in patients with adenocarcinoma of the head of the pancreas
typically are marked by elevated serum total bilirubin, alkaline phosphatase, and -glutamyl
transpeptidase, with mild elevations of the hepatic aminotransferases.[7, 9] Hepatitis serologic
study results are often assessed as part of the workup for jaundice, and they are typically
negative.[9] In patients with localized cancer of the body and tail of the pancreas, standard
laboratory values are usually normal.[7, 9] For these tumors, when liver function test
abnormalities do occur, they typically indicate diffuse metastatic disease with involvement of
the liver or porta hepatis.[9]
Normochromic anemia and hypoalbuminemia may reflect a chronic nature of the
neoplastic process and its nutritional sequelae.
It is uncommon for patients with standard ductal adenocarcinoma of the pancreas to have
either hyperamylasemia or hyperlipasemia.[7, 9]
In patients with deep jaundice, the coagulation parameters should be checked because
prolonged exclusion of bile from the gastrointestinal tract leads to malabsorption of the fat-
23
soluble vitamins and decreased the hepatic production of vitamin K-dependent clotting
factors.[7, 9] This can result in prologation of the prothrombin time.[9]
The development of biomarkers for screening holds enormous promise for increasing
early detection and impacting mortality.[67] A wide variety of serum tumor markers have been
proposed for use in the diagnosis and follow-up of pancreatic adenocarcinoma.
One of the first systematically investigated markers is carcinoembrionary antigen (CEA).
This test identifies nearly half of patients with pancreatic adenocarcinoma, and may tell
pancreatic malignancies from benign conditions in more than 90% of the patients. However,
CEA is not a valid marker for diagnosis or follow-up.
The carbohydrate antigen 125 (CA-125) is a marker of ovarian epithelial malignancies
that has been studied with regard to other gastrointestinal tract tumors. In patients with
pancreatic adenocarcinoma, CA-125 is detected in fewer than 50% of cases. CA-125 is
unsatisfactory as a single test for pancreatic adenocarcinoma.[16]
The most widely used and best validated marker for pancreatic adenocarcinoma is the
carbohydrate antigen 19-9 (CA 19-9).[7, 9, 68] CA 19-9 has been associated with both
pancreatic neoplasms and other abdominal malignancies. Approximately 80% of patients with
pancreatic adenocarcinoma may be correctly diagnosed using marker. Steinberg et al.[69]
reported that CA 19-9 was statistically more specific than CEA (86.5 versus 48.4%) but only
slightly more sensitive than CEA (92.5 versus 87.3%).[69] Therefore, CA 19-9 may be a useful
clinical marker to detect pancreatic adenocarcinoma progression in patients with either recurrent
or advanced disease.[16, 69]
CA19-9 is a Lewis blood group–related mucin that has been extensively studied in the
diagnosis, prognosis, and monitoring of pancreatic cancer. [9]
Although CA 19-9 is not accurate enough to be used in screening asymptomatic subjects
for pancreatic adenocarcinoma, it is currently the single most useful blood test in differentiating
benign from malignant pancreatic disorders. CA 19-9 has limited value in the diagnosis,
especially for early forms of the disease. However, it may complement radiological procedures
(such as computed tomography – CT – or endoscopic ultrasound – EUS), particularly in non-

24
jaundiced patients. Moreover, appropriately interpreted CA 19-9 results can guide further
invasive testing such as endoscopic retrograde cholangiopancreatography (ERCP), laparoscopy
or EUS fine-needle aspiration. [68]
Based on the above, most expert groups cautiously recommend measurement of CA 19-9
in the initial work-up of patients presenting with suspected pancreatic adenocarcinoma.[68]
Moreover, it should be borne in mind that: benign diseases (such as pancreatitis, liver
cirrhosis, cholangitis and obstructive jaundice) may have elevated CA 19-9 levels; it can be also
increased in other types of adenocarcinoma [68, 70]; CA 19-9 lacks sensitivity for small lesions;
and poorly differentiated pancreatic cancers also appear to produce less CA 19-9 than well
differentiated ones[68].
Multiple studies showed that newly presenting patients with elevated levels of CA 19-9
had a worse prognosis than those with low levels.[68, 71-72] Significant prognostic factors for
good outcome are, among others, a postoperative CA 19-9 level <200 kU/L, a decrease in CA
19-9 levels following surgical resection as well as negative lymph nodes and low tumor
stage.[68, 72] Serum CA 19-9 levels should be considered for risk stratification in patients with
pancreatic adenocarcinoma. Although high concentrations are indicative of poor outcome, CA
19-9 is only one of the multiple factors that affect prognosis and treatment planning.[68]
One of the most frequent uses of tumor markers is in postoperative surveillance following
curative surgery for a primary cancer. The aim of this surveillance is to detect
recurrences/metastases as early as possible. This practice is based on the assumption that the
early detection and the initiation of therapy enhance the chance of cure or results in a better
outcome. A number of studies have shown that serial determinations of CA 19-9 can detect
recurrent/metastatic disease several months before finding clinical or radiological evidence of
disease and CA 19-9 should be used in the follow-up of patients after surgery.[68]
In patients with advanced inoperable pancreatic adenocarcinoma, the aim of systemic
therapy is palliative. Evaluating response to systemic therapy in patients with locally advanced
pancreatic cancer may be difficult using imaging procedures due to extensive desmoplasia and
surrounding inflammatory changes. Because of these difficulties, a number of investigators have

25
attempted to use serial CA 19-9 measurements to assess response and/or determine prognosis in
patients with advanced pancreatic adenocarcinoma undergoing systemic treatment. Patients with
declining marker levels, following initiation of chemotherapy, had a better outcome than those
showing no decrease. Serial measurements of CA 19-9 should be used along with imaging to
monitor response to therapy. If CA 19-9 increases, this may indicate disease progression.[68]
Several other serum markers have been proposed for pancreatic adenocarcinoma. None of
these have been shown to be superior to CA 19-9 and none are widely used for clinical
purposes. [68] CA 19-9 remains the most useful molecular marker for the diagnosis and follow-
up of clinically and radiological evident pancreatic adenocarcinoma.[73]
One hope for the future involves new developments in the area of early detection, by use
of molecular strategies. With gene expression data and data from other molecular strategies,
earlier detection of pancreatic cancer may be possible. [9]
Imaging Studies
The early diagnosis of pancreatic adenocarcinoma requires a high index of suspicion and
appropriate aggressiveness in pursuing the diagnosis.[7] Imaging has an important role in the
diagnosis and management of patients with pancreatic adenocarcinoma. Early tumor detection
and accurate radiologic staging are crucial for identifying patients with potentially resectable
disease and avoiding unnecessary surgery in patients with unresectable disease. To ensure that
the correct imaging study is requested, physicians must have an understanding of the strengths
and limitations of the imaging modalities available. [74]
Many diagnostic modalities have been used in patients with suspected pancreatic tumors.
These modalities include transabdominal ultrasound (US), CT, magnetic resonance imaging
(MRI), ERCP, EUS and positron emission tomography (PET).[10]

26
Transabdominal Ultrasound (US)
Transabdominal US is often the initial investigation performed in patients with jaundice
or upper abdominal pain.[74-75] It is extremely sensitive in distinguishing non-obstructive
jaundice and obstructive jaundice – the presenting feature in majority of patients with pancreatic
cancer.[75] The presence of biliary dilatation in pancreatic head cancer facilitates tumor
detection. For assessing the pancreatic body and tail, the oral administration of water or other
contrast agents may help delineate the organ.[4]
Masses as small as 2cm can be detected, as well as secondary features, such as atrophy,
pancreatic duct dilatation, hepatic metastases and ascites. [16, 75] However, transabdominal US
is not a reliable method for confident diagnosis or exclusion of small pancreatic tumors.[4]
Vascular invasion and local extension are poorly depicted which often prompts further
investigations.[75]
Although it has been reported that US performed by experienced operators using proper
equipment is equivalent to or better than CT for detection and staging of pancreatic
adenocarcinoma, US is likely to remain a tool for initial assessment of patients with suspected
pancreatic disease that will be followed up by additional imaging procedures.[74]
Computed Tomography (CT)
CT remains the premier imaging test for diagnosing and staging of suspected pancreatic
adenocarcinoma because it is a robust and reliable technique.[2, 4, 75] Dual phase, contrast
enhanced thin section (spiral or multidetector) CT has greatly increased our ability to diagnose
and stage this neoplasm and to determine patient suitability for resection. Multidetector CT
(MDCT) acquisition technology was introduced in the late 1990s. Before this, high-quality
spiral CT was the preferred noninvasive imaging modality.[9]
MDCT incorporates dual-phase imaging in both the arterial and venous phases of
enhancement. Water is used as the oral contrast agent of choice and slices through the pancreas
are obtained every 1.25 mm.[9] With the development of MDCT, the acquisition of the third
27
dimension has stimulated pancreatic imaging[4] and improved the detection, staging, and
surgical planning.[9]
CT features of pancreatic adenocarcinoma are variable, depending on the size and extent
of the disease.[75] The most common abnormality is a small hypodense/hypovascular mass
within the pancreas.[2, 4, 9, 74-75] Rarely they can be isodense to the normal pancreatic
parenchyma, and difficult to detect. [2, 4] In most cases, the presence and location of a
pancreatic mass can be inferred from secondary signs, including interruption and dilation of the
pancreatic duct and/or the common bile duct, mass effect, convex abnormality of the contour,
and atrophy of the pancreas.[2, 4, 74-75]
Although radiologic signs used to diagnose pancreatic adenocarcinoma are not
pathognomonic of the condition, biopsy is usually not necessary before surgical intervention in
patients with potentially resectable disease. When the diagnosis is in doubt, or if chemotherapy
and/or radiation therapy is planned, confirmation by biopsy is necessary before treatment.[74]
The reported sensitivity of CT for detecting pancreatic adenocarcinoma is high, ranging
from 89% to 97%.[74] Not surprisingly, the sensitivity of CT is higher for larger lesions than
smaller ones.[4, 74]
Ideally, CT should be performed before biliary stenting because the stent may cause
artifact in the pancreatic head that can mask the lesion, and the trauma of stent insertion often
produces inflammatory changes that can be indistinguishable from tumor.[74]
Magnetic Resonance Imaging (MRI)
Recent advances in technology allowed MRI to improve its ability to diagnose and stage
pancreatic adenocarcinoma (high-resolution and fast imaging, volume acquisitions, magnetic
resonance cholangiopancreatography, and functional imaging).[9]
The normal pancreas is high in signal intensity on noncontrast T1-weighted fat-
suppressed images. Regarding gadolinium enhancement, it demonstrates a uniform capillary
blush on immediate postcontrast images and fades to isointense signal to the liver on interstitial

28
phase images.[76] Conversely, pancreatic adenocarcinoma appears as a low-signal intensity
mass on noncontrast T1-weighted fat-suppressed images and enhances to a lesser extent than the
surrounding normal pancreatic tissue on immediate postcontrast images.[2, 76] These MRI
features are related to the tumor sparse vascularity and dense cellularity.[9, 76] T2 weighted
sequences are employed to detect liver metastasis; vascular invasion can be evaluated with T1
weighted images post-contrast.[75]MRI may be helpful for differentiating an inflammatory
pancreatic mass from a pancreatic adenocarcinoma.[74]
There have been several studies in the past comparing MRI with CT in terms of
diagnosing and staging and all of them concluded that there is no significant benefit of MRI
over CT in its ability to predict resectability.[9, 16, 75] Because of the increased cost, room time
and potential inability of MRI in assessment of lung metastases, CT remains the primary
imaging modality of choice.[75] Moreover, some recent studies have shown slight superiority
for MDCT, in part due to the recent technical improvements.[2]
Currently, contrast-enhanced MRI has a role as a problem-solving tool if MDCT reveals
equivocal results or is not possible.[4] MRI is of value in patients with impaired renal function
or patients sensitive to iodinated contrast material.[74, 77] In selected cases, MRI may be useful
as an adjunct to CT, as for example, in characterization of small (<1 cm) hepatic lesions (when
CT findings are indeterminate)[74-75] and when there is clear biliary dilatation with no obvious
mass seen on CT.[74]
Nowadays, the MRI-cholangiopancreatography has shown promise as a noninvasive
technique with the ability to visualize both the bile duct and the pancreatic duct with images
similar to those obtained by ERCP. MRI-cholangiopancreatography may also provide important
information about the level and degree of obstruction. [75]
29
Endoscopic Ultrasound (EUS)
Another tool used for the diagnosis and staging of patients with pancreatic cancer is EUS.
It produces high-frequency images of the pancreatic parenchyma using the wall of the stomach
and duodenum as an acoustic window, thereby improving image resolution. [9-10, 74]
Therefore, EUS can evaluate peripancreatic structures, detect distinct parenchymal changes, and
it also enables the detection and evaluation of focal lesions with a minimum size of 2–3
mm.[78] For small tumors EUS has been reported to be superior to CT.[2, 4, 10, 16, 78]
Another advantage of EUS is that it can observe the whole pancreas, especially the uncinate
process and farthest tail near the splenic hilum, which is difficult to scan using transabdominal
US.[78]
An additional aspect of the EUS is the ability to perform EUS-guided fine-needle
aspiration (EUS–FNA) biopsy.[10, 16, 74, 78] Compared with other imaging modalities, the
results of EUS–FNA biopsy of pancreatic masses are excellent, with sensitivity of around 90%
and specificity of virtually 100% with a low frequency of complication. [78]
Notable disadvantages of EUS include its limited availability, marked operator
dependence, and inability to evaluate for distant metastases.[74-75]
A recent study by DeWitt et al.[79] has shown that EUS had a sensitivity of 98%
compared to 86% for MDCT. [2, 4, 74, 79-80] EUS has also been shown to have a high
negative predictive value for excluding pancreatic cancer (almost 100%), and may therefore
play a role in screening for pancreatic malignancies.[2, 4, 80]
EUS is indicated when there is high suspicion of pancreatic malignancy with no definite
mass seen on CT or MRI and also when there is some doubt regarding the local extent of the
disease (vascular invasion) and to assess involvement of normal size lymph nodes. [74-75]
However, despite these facts, CT remains the imaging modality of choice for patients
with suspected pancreatic adenocarcinoma.[74]

30
Biopsy
Biopsies can be performed under US or CT (percutaneously) or under EUS guidance,
using an aspiration technique.[10] With the advent of EUS-FNA, it became a viable and useful
alternative procedure for acquiring a tissue diagnosis. For diagnostic purposes, the sensitivity of
EUS-FNA varies from 75% to > 90%, the specificity being 82%-100%.[10, 81]
If a pancreatic mass is clearly unresectable based on CT or MRI results or if metastatic
disease is identified, either percutaneous image-guided or EUS-guided FNA can be performed
for a tissue diagnosis to confirm the presence of cancer and to offer chemotherapy or
radiation.[9, 16, 81] EUS-FNA offers some advantages over other techniques in cases where a
tissue diagnosis of pancreatic adenocarcinoma is required before treatment.[9]
Multiple factors favoring EUS-FNA over percutaneous FNA of pancreatic cancer are: (1)
it is the most cost-effective approach as a diagnostic modality; (2) it has a smaller risk when
compared with percutaneous FNA; and (3) EUS-FNA uses a short needle track. Indeed, the
aspiration needle travels from the gut lumen to the lesion, a pathway that usually does not cross
peritoneal or pleural surfaces. The exception to this is in EUS-FNA of liver lesions and of
pancreatic body/tail masses where the lesser sac of the peritoneum is breached.[81]
Moreover, EUS-FNA is more accurate than percutaneous techniques for masses < 3 cm
and is the only preoperative procedure which can demonstrate invasion of lymph nodes located
in the celiac, lumboaortic, retroduodenopancreatic or superior mesenteric regions. Also,
aspiration of ascitic fluid with a cytological study done by EUS can validate a carcinomatosis
that could not be revealed using conventional imaging. Small metastases of the left liver lobe
can be found and are easily accessible. The finding of such lesions modifies considerably the
management of supposed resectable cancer.[81]
In case of a resectable tumor, a histological diagnosis is not necessary and of little use
because it does not change the ultimate need for surgery. However, because some institutions
have a policy of giving preoperative neoadjuvant chemotherapy or radiation in resectable
pancreatic adenocarcinoma, tissue diagnosis would be a pre-requisite for that.[9, 74, 81] Others

31
argue that pre-operative diagnosis can exclude the occasional patients with unusual histology
found in 5% to 10% of pancreatic tumors (lymphoma, endocrine tumors and metastases) who
would not benefit from surgery.[81]
If CT or MRI results show a pancreatic mass with equivocal resectability, EUS is
generally the next staging procedure. If it reveals that the mass is clearly unresectable, one can
proceed with EUS-guided FNA for tissue diagnosis. If the EUS results show that the mass is
potentially resectable, then EUS-FNA should be reconsidered.[81]
Endoscopic Retrograde Cholangiopancreatography (ERCP)
Traditionally, in the evaluation of the jaundiced patient we have the cholangiography,
either by the endoscopic or percutaneous approach. The choice of technique depends primarily
on local expertise. Using the endoscopic approach, ampullary and duodenal carcinomas can be
visualized and biopsied. In addition, a pancreatogram may be obtained, which may be important
in differential diagnosis. In most cases of pancreatic adenocarcinoma, the ductal system is
obstructed, with no distal filling of the duct.[7] ERCP allows direct imaging of the pancreatic
duct, the site of origin of most pancreatic adenocarcinomas. [9-10] The sensitivity of ERCP for
diagnosis is quite high, with the finding of long, irregular stricture in an otherwise normal
pancreatic duct being virtually pathognomonic in the appropriate clinical setting.[9]
The percutaneous cholangiography is usually technically easier with a dilated biliary tree
and is useful in defining the proximal biliary system.[7]
Although there is no question that ERCP is reliable in confirming the clinical suspicion of
pancreatic adenocarcinoma, it is rarely necessary and should not be routinely used.[9-10] With
the current sophistication of CT scanning and MRI, the routine practice of diagnostic ERCP is
unsupported.[7, 9] The ERCP should be reserved for: the evaluation of a patient with presumed
pancreatic cancer and obstructive jaundice in whom no mass is evident on CT; the symptomatic
but nonjaundiced patient without an obvious pancreatic mass; or the patient with chronic
pancreatitis in whom the development of a pancreatic neoplasm is suspected.[7]
32
In addition, a biliary stent can be placed through the obstructing lesion by either the
endoscopic or percutaneous approach to decompress of the biliary tree and to alleviate
jaundice.[7, 10]
Laparoscopy
Laparoscopy has been recently introduced as a diagnostic and staging technique
potentially allowing palliative therapy.[16]
Staging laparoscopy is often performed in patients who appear to have resectable disease
on imaging studies with the purpose of avoiding unnecessary laparotomy. Many surgeons
routinely perform diagnostic laparoscopy in all patients being considered for surgical resection,
but recent studies suggest this may be unnecessary. Among the recommended indications for
diagnostic laparoscopy are small hypodense hepatic lesions that are not amenable to
percutaneous biopsy and findings that are equivocal for peritoneal carcinomatosis.[74]
Positron Emission Tomography (PET)
Recently, PET scanning has been evaluated as a tool for the diagnosis and staging of
pancreatic tumors.[4, 10, 74] At the present time, the role of PET scanning in the management
of patients with pancreatic adenocarcinoma is under development. [10, 74]
PET uses the increased metabolism of glucose by pancreatic cancer cells as the basis of
imaging. Current PET scanning for pancreatic cancer uses fluorine-18 (a positron-emitting
tracer) as a glucose-like substrate. This substance is rapidly taken up by malignant tumor cells.
However, it localizes not only tumor sites, but also sites of inflammation and infection.[9]
Therefore, PET scan has a high sensitivity (89%) but suffers from a moderate specificity
(69%).[4] Moreover, PET may have the biggest impact for detection of distant metastases and
its sensitivity may be superior to that of standard staging procedures.[74] PET has been shown

33
to give information relevant to prognosis, and to add diagnostic accuracy to CT and ERCP in
detecting tumor dissemination.[9]
The diagnosis of pancreatic adenocarcinoma still represents a difficult task and multiple
imaging tests have been proposed over the years, including transabdominal US, CT, PET, MRI,
EUS, and ERCP. Taken individually, these methods have variable sensitivity for the diagnosis
of specific pancreatic disorders. All these imaging methods improve the specificity of the
diagnosis substantially, usually providing complementary information that determines the best
treatment option. [80]
After the diagnosis of pancreatic adenocarcinoma is made, the key to management is
determining whether or not a patient has potentially resectable disease.[74]

34
STAGING AND RESECTABILITY
The tumor-node-metastasis (TNM) staging system facilitates the objective description
and classification of the anatomic extent of malignant disease in a simple, reproducible, site-
specific way. Fundamental to this staging system is the premise that cancers of the same
anatomic site and histology, with a similar extent of disease, share a common natural history.
This system provides physicians a language with which to estimate and communicate prognosis,
allows for the development and selection of stage-specific treatment strategies, and permits the
evaluation of similar groups of patients in clinical trials.[82]
For pancreatic adenocarcinoma, the definition of a resectable tumor has become more
clearly defined anatomically based on the availability of high-quality CT scans.[82] Such
imaging techniques provide more accurate staging, which has an impact on preoperative
decision making regarding tumor resectability.[16]
The current Sixth Edition of the AJCC staging system [82] evaluates pancreatic exocrine
malignancies in terms of the size and anatomic extent of the primary tumor (T), the presence or
absence of regional lymph node metastases (N), and the presence or absence of distant
metastases (M) (Table 1). [82]
The T-stage of pancreatic cancer is defined by the tumor size and the local spread.[2, 4]
T1 and T2 describe tumors confined to the pancreas, with T1 tumors being ≤2 cm in size (rarely
found) and with T2 tumors being >2 cm in size [2, 4, 82]; T3 and T4 indicate extrapancreatic
extension by the primary tumor. T4 tumors are those that are unresectable due to tumor
extension to the celiac axis (CA) or superior mesenteric artery (SMA). In contrast,
extrapancreatic tumor extension that does not involve the CA or SMA does not typically
influence the local resectability status of the tumor and, therefore, carries the T3
designation.[82]
The N-stage is dependent on the presence of nodal metastasis, with N1 representing
peripancreatic nodal metastases. [2, 4]

35
Metastasis to more distant nodes such as para-aortic nodes is defined as M1 disease.
Other common sites of distant metastases are the liver and peritoneum. [2, 4]
The combination of T, N and M is made into Stage groups (Table 1). Stage 1 disease is
tumor limited to pancreas with no nodal involvement and it is potentially resectable. In Stage 2
disease there may be extension into adjacent tissue (duodenum, bile duct, venous structures, and
regional lymph nodes) with no involvement of SMA or CA and it is usually potentially
resectable. Stage 3 is classified as unresectable locally advanced disease with invasion of SMA
and/or CA. Stage 4 disease is unresectable with distant metastasis. [75, 82]
This system now divides patients with pancreatic adenocarcinoma into distinct prognostic
and clinical groups based on contemporary definitions of resectability (Stage I/II) and
unresectability (local-regional, Stage III; metastatic, Stage IV).[82]
Distinction between Resectable, Locally Advanced and
Metastatic Disease
At present, it is accepted that surgical resection offers the only chance of cure for patients
with pancreatic adenocarcinoma.[74, 82] Whether or not the primary tumor can be removed
represents the strongest prognostic factor for patients with this disease and underlies the
distinction between Stages I and II (resectable) and Stages III and IV (unresectable due to
locally advanced or metastatic disease).
Specific oncologic and anatomic findings distinguish resectable (Stages I and II) from
unresectable (Stages III and IV) pancreatic cancer. Surgical resection of the pancreatic tumor is
generally considered to be inappropriate in patients with metastatic disease (Stage IV), as the
metastases are virtually always multifocal and associated with survival duration of
approximately 6 months. Patients with unresectable disease together account for the
overwhelming majority of patients who present with newly diagnosed pancreatic cancer. These

36
patients are generally treated with a nonsurgical strategy (chemoradiotherapy and/or
chemotherapy alone). [82]
One of the most common causes of non-resectability is vascular infiltration.[16, 75]
Pancreatic cancer has a great propensity to involve the adjacent vessels including the main
portal vein, the superior mesenteric vein (SMV), the CA and its branches, and the SMA. [76]
Nowadays, the terms “abutment” (involvement of 180 degrees or less of the
circumference of the vessel) and “encasement” (involvement of greater than 180 degrees of the
vessel) are more precise to describe tumor-vessel relationships. There is general consensus that
a tumor mass encasing the SMA or CA is considered to represent locally advanced, surgically
unresectable, Stage III disease. Arterial resection and reconstruction is technically difficult and
is associated with increased risk of perioperative morbidity and mortality. Moreover, resection
of tumors involving the CA or SMA is unlikely to be complete, and the majority of patients
with such locally advanced disease also have synchronous systemic metastases.[82]
Nowadays, the T3 category includes all forms of nonarterial tumor extension beyond the
pancreas, including extension to the SMV and portal vein. Venous resection and reconstruction
can be performed safely with no additional morbidity or mortality.[74, 82] Therefore, it is no
longer viewed as a contraindication to surgery.[4, 74, 82]
The presence of metastases to regional lymph nodes is difficult to determine
radiographically because small, benign-appearing lymph nodes frequently harbor occult
micrometastatic disease, whereas many enlarged lymph nodes are reactive and benign.[74, 82]
Moreover, metastatic involvement in normal sized lymph nodes is not detected. [75] In a patient
with pancreatic adenocarcinoma, the finding of enlarged peripancreatic lymph nodes on CT
should not preclude attempted resection.[74]
Metastatic disease is most commonly seen in the peritoneum and liver and in these
patients surgical resection is of no benefit.[74-76, 83] When the liver lesions are large, the
diagnosis of metastatic disease is usually straightforward. However, in the presence of small
lesions (<10 mm), the diagnosis of metastatic disease is difficult and biopsy may yield a
definitive role. Findings of peritoneal carcinomatosis on CT include ascites, peritoneal
37
thickening, nodular bowel wall thickening (serosal implants), and soft-tissue infiltration of the
omentum. Peritoneal carcinomatosis is diagnosed readily when advanced, but the sensitivity of
imaging studies for small peritoneal implants is limited.[74-75] Other common sites of
metastases include lung, pleura and adrenal glands. [75]
Current criteria for resectability include: (1) no evidence of tumor involvement of major
arteries (such as SMA or CA); (2) (if there is venous invasion) a suitable segment of SMV
below and portal vein above the site of venous involvement to allow for venous reconstruction;
and (3) absence of distant metastases.[74, 82] It should be also remembered that the definition
of resectability is evolving, and what was once considered unresectable disease may now be
resectable.[74]
Borderline Resectable Disease
Even though CT and MRI can provide very accurate assessments of the relationship
between the pancreatic adenocarcinoma and adjacent structures, the Stage III category includes
a wide range of tumor-vessel involvement. Tumors that demonstrate arterial abutment may be
considered for surgery as part of a multimodality approach to the disease. Patients with
borderline resectable pancreatic cancer include those whose tumors exhibit abutment or
encasement of a short segment of the hepatic artery, without evidence of tumor extension to the
CA; tumor abutment of the SMA involving 180 degrees or less of the circumference of the
artery; or short-segment occlusion of the SMV, portal vein, or their confluence, with a suitable
option available for vascular reconstruction. [82]

38
SURGICAL TREATMENT
Ductal pancreatic adenocarcinoma, the most frequent malignancy of the pancreas, is
characterized by retroperitoneal and perineural infiltration, early formation of multiple
metastases, and resistance to most of the treatment regimens currently available. Handling the
aggressive growth of this disease represents a complex and challenging task.[84]
Surgical resection, the patient‟s only hope for cure, offers a significantly improved
prognosis. Pancreatic surgery is considered one of the most technically demanding and
challenging surgical disciplines. Steady improvement in surgical techniques and advances in
perioperative supportive care have reduced the mortality.[85] However, only a minority of
patients (10–20%) present with resectable disease at the time of diagnosis.[85-86]
The anatomic location of the tumor within the pancreas dictates the type of resection.[87]
A lesion confined to the pancreatic head/uncinate process requires pancreaticoduoedenectomy
(PD).[5, 84-85, 87] Given that 60%–70% of pancreatic cancers arise in the head, PD is by far
the most common operation performed.
Because of the late presentation of symptoms, most patients with adenocarcinoma of the
body and tail present with locally advanced disease or distant metastases, thus precluding
surgical therapy.[87] However, for patients with clinically localized disease, a distal
pancreatectomy is the appropriate surgical resection. [5, 84, 87] Central pancreatic tumors of the
neck and body are rarely resectable, again because of either the presence of metastatic disease or
extension to the SMA. If they are nearer to the head of the gland, an extended PD may be
performed. For lesions nearer the tail, a distal subtotal pancreatectomy is performed.[87] Central
pancreatectomy, which is now often used to resect premalignant and low-grade lesions of the
neck and mid body [5, 87], has not been adopted for the treatment of pancreatic adenocarcinoma
by most surgeons because of concerns regarding adequate lymph node and retroperitoneal soft
tissue clearance.[87]

39
Resection for Tumors of the Head of the Pancreas
Pancreaticoduodenectomy (Kausch-Whipple procedure)
The first successful en bloc resection of part of the pancreatic head, distal common bile
duct, and duodenum was actually performed by Kausch in 1909. Twenty-five years later,
Whipple performed his first PD, also as a two-stage procedure.[4-5] It took another 7 years
before the one-stage resection was perfected, much as we know it today.[4] It consists of the
resection of the pancreatic head and duodenum along with a distal gastrectomy,
cholecystectomy, removal of the common bile duct and proximal jejunum, and enbloc resection
of regional lymph nodes.[4, 85] For a long time, this technically demanding procedure was
associated with high morbidity and mortality and a poor long-term outcome.[5, 84] However,
remarkable advances have been made in (peri)operative management and especially in the
surgical techniques used in the operation and PD has become the standard operative procedure
for tumors of the pancreatic head.[84]
The PD is divided into three parts: exploration, resection, and reconstruction.[5, 84] After
examination of the peritoneal cavity and the liver for metastatic disease, the gastrocolic ligament
is opened, the transverse and right colon are mobilized, and the duodenum is exposed.[87]
Then, a wide Kocher maneuver is performed to examine the retroperitoneum and the SMA, the
CA, the portal vein and the SMV for potential tumor infiltration.[5, 84-85] Furthermore, the size
of the tumor, and its relation to the retroperitoneal margin of the pancreas should be evaluated,
and infiltration of the retroperitoneal space needs to be ruled out.[5]
Following the gastrocolic venous trunk distally, the SMV is localized and a tunnel is
dissected between the neck of the pancreas anteriorly and the SMV-portal vein trunk
posteriorly, while at the same time the portal vein is exposed at the superior part of the pancreas.
The gallbladder and the common bile duct are then removed, and a transaction is performed
1cm from the tumor at the neck of the pancreas. The (distal) stomach and duodenum are
dissected, enabling complete removal of the specimen.[5, 84-85]

40
The reconstruction is then completed, beginning with a pancreaticojejunostomy (PJ) or
pancreaticogastrostomy (PG) and followed by a choledochojejunostomy and gastrojejunostomy
or duodenojejunostomy.[87]
Pylorus-preserving Pancreaticoduodenectomy (PPPD)
Complications seen following the Kausch-Whipple procedure, such as gastric dumping
syndromes, gastritis, and ulcerations due to bile reflux, led to the introduction of a pylorus-
preserving modification of the classical PD.[84] Introduced by Watson in the 1940s, the PPPD
was not frequently used until Traverso and Longmire re-introduced it in the late 1970s.[5, 84-
85, 87] The rationale behind preservation of the stomach is to improve gastrointestinal
function. To retain a functioning pylorus, the entire stomach and 2 cm of the first part of the
duodenum are preserved along with their neurovascular supply.[85]
There has been controversy over whether PPPD is a sufficiently radical treatment for
pancreatic cancer with respect to tumor outgrowth to the pylorus and spread to lymph nodes
along the greater and lesser curvatures of the stomach.[85, 87] Some retrospective studies
showed benefits in digestive function and quality of life for the PPPD.[5, 84] However,
eventually, many studies showed that there are no significant differences in postoperative rates
of delayed gastric emptying (DGE) between PD and PPPD.[5, 84, 87-88] Both classic and
PPPD are thus recommended for patients with resectable pancreatic adenocarcinomas.[84-85]
Therefore, surgeon‟s preference and experience should dictate the type of pancreatic resection
and reconstruction.[87]
Pancreatic Anastomosis and Reconstruction
Several prognostic factors have been identified for pancreatic anastomosis failure,
including the pancreatic tissue texture, the surgical technique, the extent of resection, and the

41
extent of dilatation of the pancreatic duct. The two most common pancreatic anastomosis
techniques are PJ and PG.[85]
The PJ can be performed by invaginating the transected pancreas into the jejunum.
Another possibility is the duct-to-mucosa technique, anastomosing the pancreatic duct directly
to the jejunum. Separate duct-to-mucosa adaptation helps to keep the duct orifice open, allowing
the unobstructed flow of pancreatic juice through the anastomosis. Using the end-to-side
anastomosis, the jejunal opening can be adapted specifically to the requirements of the
pancreatic remnant. [85]
Another technique (PG) often used is to anastomose the pancreatic remnant to the
stomach.[85] PG is technically easier to perform because of the proximity of the stomach and
the pancreatic remnant, which usually assures that the anastomosis is well perfused. Moreover,
pancreatic enzymes are not directly activated in the acidic milieu of the stomach.[5]
Large series were not able to show superiority of any of the techniques, suggesting equal
results for PG and PJ.[5, 84-85, 88]
As a third option, the pancreatic duct can be occluded by sutures, glue, or biologic
material. This practice, however, has been associated with higher fistula rates [84-85] and an
increased risk of pancreatic insufficiency[85]. As a result, ductal occlusion has largely been
abandoned.
Based on current data, there is no evidence in favor of one particular technique.[85] As
long as the three basic requirements of a safe anastomosis are met – a tension-free adaptation,
well-perfused tissues, and no distal obstruction – any anastomotic technique can result in good
outcome.[5, 84-85]
Prophylactic pharmacological approaches using somatostatin analogs (octreotide) have
been used in Europe and the United States with conflicting results.[88]
For re-establishment of gastrointestinal continuity, a variety of techniques may be
performed, such as retrocolic reconstruction with a single limb for all anastomoses, antecolic or
infracolic reconstructions, but there is no definitive evidence in favor of any one of them.[84]

42
However, some recent studies suggest that antecolic reconstruction may have some superiority
over retrocolic duodenojejunostomy in terms of decreased rates of DGE.[5]
Resection for Tumors of the Body/Tail of the Pancreas
Distal pancreatectomy
A distal pancreatectomy is performed for tumors of the pancreatic body and/or tail.[5, 84,
89] In most cases, a splenectomy has to be performed when tumor localization and surgical
technique do not permit preservation of the splenic vessels.[5] Conventionally, this was
believed to be necessary, because it was thought that splenic preservation might compromise the
oncological resection. However, it has been demonstrated that splenic preservation could be
accomplished with no increase in complication rate, operative time, or length of postoperative
stay. It is recommended that a spleen-preserving procedure should be performed for patients
with pancreatic adenocarcinoma at any intrapancreatic location unless the splenic capsule is
directly involved with or adherent to the tumor. Furthermore, the splenic vessels must be
unaffected by the tumor. [85]
Numerous techniques have been described for the subsequent division of the pancreas:
linear stapling, duct ligation and fibrin glue sealing.[5] The conventional method is ligation of
the main pancreatic duct and additional suturing of the stump to approximate the anterior and
posterior capsule. With the advent of surgical stapling devices, a new tool became available for
sealing the pancreatic stump, joining the harmonic scalpel, fibrin glue, and prolamine injection.
However, the use of a stapling device for closure of the pancreatic remnant was associated with
a significantly higher fistula rate.[85]
Central pancreatectomy
Central pancreatectomy (CP) has been proposed as an alternative for patients with small,
benign or low-grade malignant tumors such as endocrine and cystic neoplasms located in the

43
neck of the pancreas. The rationale for CP is to remove the neoplasm with preservation of the
functional parenchyma, and thereby avoiding a major resection. This method reduces the risk of
diabetes and exocrine insufficiency, and maintains the upper digestive and biliary anatomy.
Therefore, CP might be a safe and effective treatment option for small and/or low-grade
malignant neoplasms as well as for pancreatic metastases. However, it is questionable whether
this technique will also be applicable in patients with ductal adenocarcinoma, because this
tumor has a more aggressive biology. [89]
Total pancreatectomy
Total pancreatectomy (TP) is a combination of PD and distal pancreatectomy together
with a local lymphadenectomy. It is reserved for patients with multilocular or large tumors of
the pancreas. However, because the procedure is accompanied by postoperative exocrine and
endocrine insufficiency, and is associated with the highest mortality rates from all pancreatic
surgeries, it is rarely used. [84]
In the last decades, however, TP has become a possible treatment option, since
remarkable improvements in both surgery and postoperative management of the apancreatic
patient, with successful management of endocrine and exocrine insufficiency, were achieved.
However, there has not been shown any long-term survival benefit. [89]
Extended Lymphadenectomy – Extended Lymph Node
Dissection (ELND)
Up to 30% of patients with pancreatic cancer have retroperitoneal lymph node disease
that would not be resected by standard PD. It was hypothesized that survival could be improved
by using an ELND to help achieve node negativity. ELND involves, in addition to removal of
the pancreaticoduodenal nodes, removal of the lymph nodes along the hepatic artery, SMA, CA,

44
and between the aorta and the inferior pancreaticoduodenal artery. Furthermore, the
anterolateral aspect of the aorta and the inferior vena cava are also dissected. The earliest
proponents of ELND were the Japanese, who demonstrated improved survival rates with
extended surgery.[90] However, several studies, including for example Yeo et al.[91] and
Michalsky et al.[92], confirmed that ELND increased morbidity and offered no survival benefit
over standard lymphadenectomy with PD and concluded that ELND should only be performed
within controlled trials, if at all.[89-92]
Arterial/Venous Resections with Reconstruction
Vascular resections can be performed based on two rationales: firstly, to achieve negative
resection margins in case of vessel invasion by the tumor, making separation impossible;
secondly, it can be performed as a part of an extended pancreactectomy. Vein resections include
the portal vein, SMV, or the SMV-portal vein confluence.[90] Venous resections followed by
graft reconstruction can be performed without increased morbidity and mortality and may be
performed to achieve negative resection margins. [84, 90] Therefore, venous infiltration should
not be viewed as a contraindication for resection.[5]
In contrast, arterial resections of the SMA, celiac, and hepatic arteries are rarely
performed and they are considered by most as contraindicated in PD due to the greatly increased
morbidity and mortality.[90]
Short-Term Outcome
The main complications of PD are pancreatic fistulas, DGE, intra-abdominal abscesses,
and hemorrhage.[5]
A review article by Alexakis et al.[93] showed that the incidence of fistula or leakage was
2–24%.[5, 88, 93] Importantly, pancreatic fistula is closely associated with subsequent
mortality, mainly because of retroperitoneal sepsis and bleeding.[93-94] Thus, meticulous

45
surgical technique during construction of the pancreaticoenteric anastomosis is of high
importance. The value of octreotide is still debated in the literature: some studies show a
decrease in the occurrence of pancreatic fistula with octreotide, whereas others show no benefit.
Intra-abdominal abscesses can frequently occur following pancreatic fistula
development.[93, 95-96] These abscesses can usually be drained percutaneously and are most
commonly found sub-hepatically or at the left diaphragm.[5] The usual cause is a leak from the
pancreatic-enteric anastomosis. A CT scan will usually diagnose the abscess, and image-guided
drainage is usually successful.[88]
DGE is usually related to intra-abdominal complications.[93, 95] The incidence of DGE
reported by various studies has varied considerably (14–30%), because there is no standard
definition.[5, 95-96]
Bleeding can be classified roughly into early and late hemorrhage. Bleeding within the
first 24 hours postoperatively is usually a result of inadequate intraoperative hemostasis or
hemorrhage from one of the enteric anastomoses, and it can usually be treated conservatively.
Late hemorrhage is a severe complication, with considerable mortality (up to 60%), and occurs
mainly after leakage of the pancreatic anastomosis.[5] Its management is still controversial:
radiological embolization of the bleeding vessel and surgical hemostasis are both valid
treatment options.[5, 88, 93, 95, 97]
In pancreatic resection, perioperative mortality is closely associated with the level of
experience of the team providing therapy, thus it should be performed by experienced
surgeons.[5, 88]
Long-Term Outcome
Pancreatic cancer is commonly viewed as a disease uniformly leading to death. The long-
term prognosis, however, has improved over the past decade.[5] Recent studies demonstrated 5
year survival rates of approximately 20% after curative resection.[5, 98-99] In a subgroup of
patients with lymph-node and margin-negative tumors, 5-year survival of up to 40% has been
46
achieved.[5, 100] Recently, it has been shown that patients who survive 5 years after resection
have a subsequent 5-year survival rate of approximately 55%.[5, 101]
The most important factors influencing outcome after PD are curative resection, absence
of lymph node metastases, tumor size (<2cm), well or moderately differentiated tumors, absence
of perineural or vascular invasion, and the surgeons‟ experience. [5, 88] Wagner et al.
concluded that “curative resection is the single most important factor determining the outcome
in patients with pancreatic cancer”.[99]
CA19-9 levels also seem to predict long-term outcome. Preoperative CA19-9 levels
correlate with disease stage, and a postoperative decrease are strong independent predictors of
survival.[5]
Recently, quality of life after PD was evaluated, and shown to be impaired only in the
first 3-6 months after surgery, following this period quality of life was comparable to
preoperative levels.[5]
47
CHEMORADIOTHERAPY
Despite attempted curative resection of localized pancreatic adenocarcinoma, most
patients recur and die of their disease.[102] The high risk of local and systemic disease
recurrence, as well as overall poor prognosis, laid down the rationale for adjuvant therapy after
resection of pancreatic adenocarcinoma.[103-105] There is no consensus on what constitutes
“standard” adjuvant therapy. This controversy derives from several studies, each one with its
own limitations.[105]
The Gastro-Intestinal Study Group (GITSG) trial was the first prospective randomized
trial suggesting survival advantage with postoperative chemo-radiotherapy using bolus 5-
Fluorouracil (5-FU).[106] However, this study was criticized for poor patient selection, early
termination, small patient number, and suboptimal radiotherapy dose.[102]
The European Organization of Research and Treatment of Cancer (EORTC) compared 5-
FU plus radiotherapy with observation only in patients with resected pancreatic
adenocarcinoma.[107] The study showed a trend toward benefit in median survival (17.1
months vs. 12.6 months; P=0.099) of the 5-FU plus radiotherapy group.[107] This study was
also criticized for suboptimal dose of radiotherapy and split courses.[102]
ESPAC-1 trial sparked a new debate over the role of radiotherapy in the adjuvant therapy
of pancreatic cancer.[108] ESPAC-1 trial was designed to compare adjuvant concurrent
chemoradiotherapy (5-FU plus radiotherapy), chemotherapy alone (5-FU), chemoradiotherapy
followed by chemotherapy, and observation. Chemotherapy only arm had statistically
significant benefit over observation arm in median survival (20.1 months vs. 15.5 months;
P=0.009). However, chemoradiotherapy arm showed worse median survival compared with
patients who did not receive chemo-radiotherapy (15.9 months vs. 17.9 months; P=0.05).[108]
Major criticism was made on this study for possible selection bias, suboptimal radiotherapy, and
for allowing the final radiotherapy dose to be left to the judgment of the treating
physicians.[102]

48
CONKO-001 study randomized patients with resected pancreatic cancer to gemcitabine
or observation.[109] This trial showed statistically significant disease free survival benefit (13.4
months vs. 6.9 months; P<0.001) of gemcitabine over observation. This benefit of
chemotherapy in CONKO-001 study was consistent with the result from ESPAC-1 trial which
showed benefit of 5-FU over no adjuvant therapy.[108-109]
Radiation Therapy Oncology Group (RTOG) 97-04 was the first American cooperative
group study since the GITSG trial. The study had no observation alone arm. RTOG 97-04 study
randomized resected pancreatic cancer patients to evaluate benefit of adding gemcitabine to 5-
FU combined with radiotherapy.[109] One arm received 5-FU plus radiotherapy and the other
arm was treated with gemcitabine before and after 5-FU plus radiotherapy.[105] The addition of
gemcitabine to adjuvant fluorouracil-based chemoradiation was associated with a survival
benefit for patients, although this improvement was not statistically significant.[110]
Neoptolemos et al. presented the results of ESPAC-3 study.[102] This is a multicenter,
international, open-label, randomized, controlled, phase III trial that aimed at comparing of
adjuvant 5-FU/leucovorin versus gemcitabine in patients with resected pancreatic ductal
adenocarcinoma. The primary outcome measure was overall survival; the secondary measures
were toxicity, progression free survival and quality of life. The study confirmed the role of
adjuvant chemotherapy. However, overall survival was similar on both arms, hence showing
that gemcitabine is not superior to 5-FU in adjuvant setting. Median overall survival was 23.0
months with 5-FU and it was 23.6 months with gemcitabine. However, safety and dose intensity
favors gemcitabine. This study is very important because there has been a tendency to reject 5-
FU in pancreatic cancer and now it is very much back on the stage.[102]
Pancreatic adenocarcinoma remains a dismal disease with poor prognosis, even after
curative resection and most aggressive combine-modality approaches. This serves as a reminder
that we need to push the envelope even further.
The varying results of these randomized trials make it difficult to establish a standard
adjuvant therapy for resected pancreatic adenocarcinoma.[105]
49
The National Comprehensive Cancer Network (NCCN) recommends that investigational
options should be considered in all phases of disease management.[105, 111] Additionally, until
further data are available, the NCCN recommends postoperative radiotherapy plus 5-FU with or
without additional chemotherapy (gemcitabine), or chemotherapy alone (gemcitabine based) for
all patients after curative resection for pancreatic cancer, regardless of nodal status.[105, 111]
One way of eliminating potential treatment delays is to consider neoadjuvant
chemoradiotherapy or chemotherapy. This approach leads to increased survival, down-staging
marginal lesions, and sparing patients with rapidly progressive disease unnecessary
surgery.[105, 112] Single institution studies including neoadjuvant chemoradiotherapy or
chemotherapy have shown promise and provide the framework for larger controlled trials
evaluating the role of neoadjuvant therapy in the management of both resectable and marginally
resectable lesions.[105]
In patients with locally advanced disease local control remains an important issue in
terms of palliation (discussed later). There is promise that the therapeutic ratio using modern
radiotherapy techniques will improve and patients should be offered trials employing these
techniques. Furthermore, it is still to be proven whether chemotherapy alone can provide to
these patients tumor control, symptom palliation and survival with less toxicity.[1]
In patients with metastatic disease improvements in supportive care have dramatically
altered their quality of life: the use of anabolic agents such as Megestrol acetate, dexamethasone
and pancreatic supplements.[1]
Until 1995 there was little evidence that chemotherapy provided any benefit, and it was
recognized that the agents used showed no major apparent gains in survival and were toxic.
However, some small studies, all showing improved survival over best supportive care, have
altered perceptions. The first study using gemcitabine in 5-FU refractory patients showed a
response rate of 9.5%, a median survival of 3.9 months and a 6-month survival rate of 31%.[1,
113] Gemcitabine has subsequently been studied in a large number of studies involving
alternative comparisons including both 5-FU and novel therapies.[1]

50
Nowadays, single agent gemcitabine remains the treatment of choice for metastatic
pancreatic cancer patients of reasonable performance status, with the promise of both improved
symptom control, survival and tolerable toxicity.[1]
In patients with confirmed failure of gemcitabine first-line therapy one should consider a
second-line strategy. Some regimens showed activity in second-line therapy like paclitaxel,
gemcitabine and capecitabine or oxaliplatin combinations, raltitrexed, irinotecan, erlotinib.
However, these results were never confirmed. The available data suggest that some selected
patients can benefit from second-line therapy, but there is no standard option at this time.[114]
Novel targeted agents have received extensive attention because of the relative
insensitivity to conventional therapy. Recent attention has been directed at epidermal growth
factor (EGF) inhibition.[1] Human epidermal growth factor receptor (EGFR) type 1 is
overexpressed in many pancreatic tumors and is associated with poor prognosis and disease
progression. In experimental models, blocking EGFR improves the anticancer effects of
gemcitabine. Ongoing studies are incorporating inhibitors of the EGFR (e.g., erlotinib) as well
as monoclonal antibodies (e.g., cetuximab). A trial compared gemcitabine with and without
erlotinib in patients with locally advanced or metastatic pancreatic cancer and it showed an
overall survival significantly prolonged on the erlotinib plus gemcitabine arm. One-year
survival and progression free survival were also greater with this combination. However, there
was a higher incidence of some adverse events. Although the gain in survival was statistically
significant, the modest 2-week improvement in median survival hardly has a clinical
impact.[114]
Cetuximab presented promising results in early studies in combination with gemcitabine.
Those results led to a trial (gemcitabine alone or plus cetuximab).[112] Unfortunately, in a
preliminary report, the addition of cetuximab did not improve any of the planned
outcomes.[114]
As many other tumors, pancreatic cancers also frequently overexpress vascular
endothelial growth factor (VEGF) and its receptor.[114] Therefore, there has been substantial
interest in the role of bevacizumab (a VEGF ligand inhibitor). Other VEGF receptor inhibitors

51
are also likely to be studied given the high expression of VEGF receptor on pancreatic cancer
cells.[1]
Systemic therapy benefits pancreatic cancer patients who are not suitable for surgical
therapy. The regimens that proved benefit in survival always involved gemcitabine, establishing
such drug as the backbone of the treatment. The association of a second agent like capecitabine
or erlotinib helps some patients, especially those with better performance, but the cost-benefit
analysis has to be considered. For patients with a good performance status after failing initial
gemcitabine-based therapy, second-line therapy can be considered. The optimal regimen is
unknown, but options include fluoropyrimidines alone or oxaliplatin plus either 5-FU,
capecitabine, irinotecan or single-agent paclitaxel.[114]

52
PALLIATION TREATMENT
Treatment depends upon the probable length of survival, presence of metastatic disease or
advanced local disease as well as symptoms. Common symptoms include jaundice, weight loss,
pain, and vomiting from gastric outlet obstruction.[83]
Biliary Obstruction
Patients with metastatic disease and biliary obstruction are candidates for endoscopic or
percutaneous placement of biliary stent.[114] Perforation and pancreatitis are unusual
complications and antibiotic coverage of biliary flora is required to prevent cholangitis.
Pancreatitis, hemorrhage and biliary peritonitis have all been described as complications of
percutaneous stent placement.[83]
Surgical options to relieve obstructive jaundice are preferably performed in patients with
locally advanced disease and when stent placement is impracticable for technical reasons. A
bypass between the gallbladder and jejunum or, preferably, the common bile duct and jejunum
are the main options available. One advantage of surgical bypass is to perform a prophylactic
gastrojejunostomy to prevent a later duodenal obstruction. The high incidence of jaundice
recurrence following endoscopic stenting and the occurrence of tumor-associated duodenal
obstruction are points favoring operative palliative management in selected patients.[114]
Gastric Outlet Obstruction
Duodenal obstruction leading to gastric outlet obstruction occurs in 15–20% of patients
with advanced disease.[114] Although routine prophylactic gastrojejunostomy for operative
palliation of pancreatic cancer has been proposed by many authors [114-116], it has been

53
contested by others due to the high incidence of postoperative DGE [114, 117]. Some reports
show an incidence of DGE after duodenum bypass surgery ranging from 24 to 29%.[114, 117-
118] Endoscopically placed stents are a more favorable option in patients with metastatic
disease, when a shorter survival is expected. They offer palliative benefit with less
morbidity.[83, 114]
Severe Abdominal Pain
Pharmacologic therapy with opioids and neurolytic celiac plexus block are the most
commonly used techniques for palliation of pain associated with unresectable pancreatic
adenocarcinoma. Existing studies suggest that celiac plexus block is a well-tolerated
intervention that may improve analgesia, decrease opioid requirements, and minimize
deterioration of quality of life. Celiac plexus block can be performed percutaneously, surgically,
or under endosonographic guidance.[114] Pain relief lasting for up 24 weeks has been observed
in 70% of patients. The main complications include transient diarrhea and hypotension because
of sympathetic blockade and may be present in about 40% of patients. Severe adverse effects
are uncommon.[114, 119] Radiotherapy can be used to relieve pain due local invasion of
pancreatic cancer and is successful in 35–65% of patients.[114]
Pancreatic insufficiency
Obstruction of the pancreatic duct may lead to symptoms of pancreatic insufficiency such
as steatorrhoea and weight loss. The addition of oral pancreatic exocrine supplements will
usually control these symptoms. Pancreatic endocrine insufficiency (diabetes mellitus) should
be treated as type 2 diabetes.[83]

54
CONCLUSIONS
Pancreatic adenocarcinoma still remains a disease with a dismal prognosis, despite all of
the advances made in its management. The etiology of this neoplasia is still unknown, but
smoking is strongly associated with it. Also, in the last decades we have witnessed an explosion
in our understanding of the genetic modifications underlining the pathogenesis and progression
to invasive carcinoma. Moreover, recent advances in imaging techniques and tumor markers
allowed a better and earlier diagnose and staging as well as more accurate follow-up. Therefore,
aggressive evaluation should be performed.
Surgical resection is still the best hope for cure for pancreatic adenocarcinoma. However,
only a small number of patients have indication for curative resection. Between the different
surgical techniques, it has been proved that there are no significant differences in outcome.
Therefore, surgeon‟s preference and experience should dictate the type and procedure.
Moreover, surgical management (either resection for cure or operative palliation) should be
performed by experienced surgeons to minimize morbidity and mortality.
Following resection, postoperative adjuvant radiation and chemotherapy should be
offered to most patients for improved long-term survival. However, a standard treatment is not
yet available.

55
ACKNOWLEDGEMENTS
The author would like to thank Prof. António Taveira Gomes for his support and
contribution in this article.
56
REFERENCES
1. Goldstein D, Carroll S, Apte M, Keogh G: Modern management of pancreatic
carcinoma. Intern Med J, 2004. 34(8): p. 475-81.
2. Francis IR: Pancreatic adenocarcinoma: diagnosis and staging using multidetector-
row computed tomography (MDCT) and magnetic resonance imaging (MRI). Cancer
Imaging, 2007. 7 Spec No A: p. S160-5.
3. Beger HG, Rau B, Gansauge F, Poch B, Link KH: Treatment of pancreatic cancer:
challenge of the facts. World J Surg, 2003. 27(10): p. 1075-84.
4. Schima W, Ba-Ssalamah A, Kolblinger C, Kulinna-Cosentini C, Puespoek A, Gotzinger P:
Pancreatic adenocarcinoma. Eur Radiol, 2007. 17(3): p. 638-49.
5. Michalski CW, Weitz J, Buchler MW: Surgery insight: surgical management of
pancreatic cancer. Nat Clin Pract Oncol, 2007. 4(9): p. 526-35.
6. Kleeff J, Michalski C, Friess H, Buchler MW: Pancreatic cancer: from bench to 5-year
survival. Pancreas, 2006. 33(2): p. 111-8.
7. Lillemoe KD, Yeo CJ, Cameron JL: Pancreatic cancer: state-of-the-art care. CA Cancer J
Clin, 2000. 50(4): p. 241-68.
8. Ghadirian P, Lynch HT, Krewski D: Epidemiology of pancreatic cancer: an overview.
Cancer Detect Prev, 2003. 27(2): p. 87-93.
9. Yeo TP, Hruban RH, Leach SD, Wilentz RE, Sohn TA, Kern SE, Iacobuzio-Donahue CA,
Maitra A, Goggins M, Canto MI, Abrams RA, Laheru D, Jaffee EM, Hidalgo M, Yeo CJ:
Pancreatic cancer. Curr Probl Cancer, 2002. 26(4): p. 176-275.
10. de Braud F, Cascinu S, Gatta G: Cancer of pancreas. Crit Rev Oncol Hematol, 2004.
50(2): p. 147-55.
11. Lowenfels AB, Maisonneuve P: Risk factors for pancreatic cancer. J Cell Biochem, 2005.
95(4): p. 649-56.

57
12. Lowenfels AB, Maisonneuve P: Epidemiology and risk factors for pancreatic cancer.
Best Pract Res Clin Gastroenterol, 2006. 20(2): p. 197-209.
13. Lowenfels AB, Maisonneuve P: Epidemiology and prevention of pancreatic cancer. Jpn
J Clin Oncol, 2004. 34(5): p. 238-44.
14. Fraumeni JF Jr.: Cancers of the pancreas and biliary tract: epidemiological
considerations. Cancer Res, 1975. 35(11 Pt. 2): p. 3437-46.
15. Flanders TY, Foulkes WD: Pancreatic adenocarcinoma: epidemiology and genetics. J
Med Genet, 1996. 33(11): p. 889-98.
16. Hidalgo Pascual M, Ferrero Herrero E, Castillo Fe MJ, Guadarrama Gonzalez FJ, Pelaez
Torres P, Botella Ballesteros F: Epidemiology and diagnosis of the pancreatic cancer.
Rev Esp Enferm Dig, 2004. 96(10): p. 714-8; 719-22.
17. Winter JM, Maitra A, Yeo CJ: Genetics and pathology of pancreatic cancer. HPB
(Oxford), 2006. 8(5): p. 324-36.
18. Hansel DE, Kern SE, Hruban RH: Molecular pathogenesis of pancreatic cancer. Annu
Rev Genomics Hum Genet, 2003. 4: p. 237-56.
19. Iacobuzio-Donahue CA, van der Heijden MS, Baumgartner MR, Troup WJ, Romm JM,
Doheny K, Pugh E, Yeo CJ, Goggins MG, Hruban RH, Kern SE: Large-scale allelotype of
pancreaticobiliary carcinoma provides quantitative estimates of genome-wide allelic
loss. Cancer Res, 2004. 64(3): p. 871-5.
20. Wilentz RE, Goggins M, Redston M, Marcus VA, Adsay NV, Sohn TA, Kadkol SS, Yeo CJ,
Choti M, Zahurak M, Johnson K, Tascilar M, Offerhaus GJ, Hruban RH, Kern SE: Genetic,
immunohistochemical, and clinical features of medullary carcinoma of the pancreas:
A newly described and characterized entity. Am J Pathol, 2000. 156(5): p. 1641-51.
21. Feinberg AP: The epigenetics of cancer etiology. Semin Cancer Biol, 2004. 14(6): p.
427-32.

58
22. Caldas C, Hahn SA, da Costa LT, Redston MS, Schutte M, Seymour AB, Weinstein CL,
Hruban RH, Yeo CJ, Kern SE: Frequent somatic mutations and homozygous deletions
of the p16 (MTS1) gene in pancreatic adenocarcinoma. Nat Genet, 1994. 8(1): p. 27-
32.
23. Schutte M, Hruban RH, Geradts J, Maynard R, Hilgers W, Rabindran SK, Moskaluk CA,
Hahn SA, Schwarte-Waldhoff I, Schmiegel W, Baylin SB, Kern SE, Herman JG:
Abrogation of the Rb/p16 tumor-suppressive pathway in virtually all pancreatic
carcinomas. Cancer Res, 1997. 57(15): p. 3126-30.
24. Feldmann G, Maitra A: Molecular genetics of pancreatic ductal adenocarcinomas and
recent implications for translational efforts. J Mol Diagn, 2008. 10(2): p. 111-22.
25. Maitra A, Hruban RH: Pancreatic cancer. Annu Rev Pathol, 2008. 3: p. 157-88.
26. Maitra A, Kern SE, HrubanRH: Molecular pathogenesis of pancreatic cancer. Best Pract
Res Clin Gastroenterol, 2006. 20(2): p. 211-26.
27. Hruban RH, Takaori K, Canto M, Fishman EK, Campbell K, Brune K, Kern SE, Goggins M:
Clinical importance of precursor lesions in the pancreas. J Hepatobiliary Pancreat
Surg, 2007. 14(3): p. 255-63.
28. Takaori K: Current understanding of precursors to pancreatic cancer. J Hepatobiliary
Pancreat Surg, 2007. 14(3): p. 217-23.
29. Feldmann G, Beaty R, Hruban RH, Maitra A: Molecular genetics of pancreatic
intraepithelial neoplasia. J Hepatobiliary Pancreat Surg, 2007. 14(3): p. 224-32.
30. Wilentz RE, Albores-Saavedra J, Hruban RH: Mucinous cystic neoplasms of the
pancreas. Semin Diagn Pathol, 2000. 17(1): p. 31-42.
31. Maitra A, Fukushima N, Takaori K, Hruban RH: Precursors to invasive pancreatic
cancer. Adv Anat Pathol, 2005. 12(2): p. 81-91.
32. Singh M, Maitra A: Precursor lesions of pancreatic cancer: molecular pathology and
clinical implications. Pancreatology, 2007. 7(1): p. 9-19.

59
33. van den Berg W, Tascilar M, Offerhaus GJ, Albores-Saavedra J, Wenig BM, Hruban RH,
Gabrielson E: Pancreatic mucinous cystic neoplasms with sarcomatous stroma:
molecular evidence for monoclonal origin with subsequent divergence of the
epithelial and sarcomatous components. Mod Pathol, 2000. 13(1): p. 86-91.
34. Hyde GL, Davis JB Jr, McMillin RD, McMillin M: Mucinous cystic neoplasm of the
pancreas with latent malignancy. Am Surg, 1984. 50(4): p. 225-9.
35. Le Borgne J, de Calan L, Partensky C: Cystadenomas and cystadenocarcinomas of the
pancreas: a multiinstitutional retrospective study of 398 cases. French Surgical
Association. Ann Surg, 1999. 230(2): p. 152-61.
36. Iacobuzio-Donahue CA, Wilentz RE, Argani P, Yeo CJ, Cameron JL, Kern SE, Hruban RH:
Dpc4 protein in mucinous cystic neoplasms of the pancreas: frequent loss of
expression in invasive carcinomas suggests a role in genetic progression. Am J Surg
Pathol, 2000. 24(11): p. 1544-8.
37. Flejou JF, Boulange B, Bernades P, Belghiti J, Henin D: p53 protein expression and DNA
ploidy in cystic tumors of the pancreas. Pancreas, 1996. 13(3): p. 247-52.
38. Jimenez RE, Warshaw AL, Z'Graggen K, Hartwig W, Taylor DZ, Compton CC, Fernandez-
del Castillo C: Sequential accumulation of K-ras mutations and p53 overexpression in
the progression of pancreatic mucinous cystic neoplasms to malignancy. Ann Surg,
1999. 230(4): p. 501-9; discussion 509-11.
39. Luttges J, Feyerabend B, Buchelt T, Pacena M, Kloppel G: The mucin profile of
noninvasive and invasive mucinous cystic neoplasms of the pancreas. Am J Surg
Pathol, 2002. 26(4): p. 466-71.
40. Chari ST, Yadav D, Smyrk TC, DiMagno EP, Miller LJ, Raimondo M, Clain JE, Norton IA,
Pearson RK, Petersen BT, Wiersema MJ, Farnell MB, Sarr MG: Study of recurrence
after surgical resection of intraductal papillary mucinous neoplasm of the pancreas.
Gastroenterology, 2002. 123(5): p. 1500-7.

60
41. Adsay NV, Pierson C, Sarkar F, Abrams J, Weaver D, Conlon KC, Brennan MF, Klimstra
DS: Colloid (mucinous noncystic) carcinoma of the pancreas. Am J Surg Pathol, 2001.
25(1): p. 26-42.
42. D'Angelica M, Brennan MF, Suriawinata AA, Klimstra D, Conlon KC: Intraductal
papillary mucinous neoplasms of the pancreas: an analysis of clinicopathologic
features and outcome. Ann Surg, 2004. 239(3): p. 400-8.
43. Kobayashi G, Fujita N, Noda Y, Ito K, Horaguchi J, Takasawa O, Akaishi S, Tsuchiya T,
Kobari M: Mode of progression of intraductal papillary-mucinous tumor of the
pancreas: analysis of patients with follow-up by EUS. J Gastroenterol, 2005. 40(7): p.
744-51.
44. Yoshizawa K, Nagai H, Sakurai S, Hironaka M, Morinaga S, Saitoh K, Fukayama M:
Clonality and K-ras mutation analyses of epithelia in intraductal papillary mucinous
tumor and mucinous cystic tumor of the pancreas. Virchows Arch, 2002. 441(5): p.
437-43.
45. Z'Graggen K, Rivera JA, Compton CC, Pins M, Werner J, Fernandez-del Castillo C,
Rattner DW, Lewandrowski KB, Rustgi AK, Warshaw AL: Prevalence of activating K-ras
mutations in the evolutionary stages of neoplasia in intraductal papillary mucinous
tumors of the pancreas. Ann Surg, 1997. 226(4): p. 491-8; discussion 498-500.
46. Kobari M, Egawa S, Shibuya K, Shimamura H, Sunamura M, Takeda K, Matsuno S,
Furukawa T: Intraductal papillary mucinous tumors of the pancreas comprise 2
clinical subtypes: differences in clinical characteristics and surgical management.
Arch Surg, 1999. 134(10): p. 1131-6.
47. Nakagohri T, Kenmochi T, Kainuma O, Tokoro Y, Asano T: Intraductal papillary
mucinous tumors of the pancreas. Am J Surg, 1999. 178(4): p. 344-7.
48. Terris B, Ponsot P, Paye F, Hammel P, Sauvanet A, Molas G, Bernades P, Belghiti J,
Ruszniewski P, Flejou JF: Intraductal papillary mucinous tumors of the pancreas

61
confined to secondary ducts show less aggressive pathologic features as compared
with those involving the main pancreatic duct. Am J Surg Pathol, 2000. 24(10): p.
1372-7.
49. Adsay NV, Merati K, Andea A, Sarkar F, Hruban RH, Wilentz RE, Goggins M, Iocobuzio-
Donahue C, Longnecker DS, Klimstra DS: The dichotomy in the preinvasive neoplasia
to invasive carcinoma sequence in the pancreas: differential expression of MUC1 and
MUC2 supports the existence of two separate pathways of carcinogenesis. Mod
Pathol, 2002. 15(10): p. 1087-95.
50. Luttges J, Zamboni G, Longnecker D, Kloppel G: The immunohistochemical mucin
expression pattern distinguishes different types of intraductal papillary mucinous
neoplasms of the pancreas and determines their relationship to mucinous noncystic
carcinoma and ductal adenocarcinoma. Am J Surg Pathol, 2001. 25(7): p. 942-8.
51. Terris B, Dubois S, Buisine MP, Sauvanet A, Ruszniewski P, Aubert JP, Porchet N,
Couvelard A, Degott C, Flejou JF: Mucin gene expression in intraductal papillary-
mucinous pancreatic tumours and related lesions. J Pathol, 2002. 197(5): p. 632-7.
52. Adsay NV, Merati K, Basturk O, Iacobuzio-Donahue C, Levi E, Cheng JD, Sarkar FH,
Hruban RH, Klimstra DS: Pathologically and biologically distinct types of epithelium in
intraductal papillary mucinous neoplasms: delineation of an "intestinal" pathway of
carcinogenesis in the pancreas. Am J Surg Pathol, 2004. 28(7): p. 839-48.
53. Furukawa T, Kloppel G, Volkan Adsay N, Albores-Saavedra J, Fukushima N, Horii A,
Hruban RH, Kato Y, Klimstra DS, Longnecker DS, Luttges J, Offerhaus GJ, Shimizu M,
Sunamura M, Suriawinata A, Takaori K, Yonezawa S: Classification of types of
intraductal papillary-mucinous neoplasm of the pancreas: a consensus study.
Virchows Arch, 2005. 447(5): p. 794-9.
54. Adsay NV, Adair CF, Heffess CS, Klimstra DS: Intraductal oncocytic papillary neoplasms
of the pancreas. Am J Surg Pathol, 1996. 20(8): p. 980-94.

62
55. Cuillerier E, Cellier C, Palazzo L, Deviere J, Wind P, Rickaert F, Cugnenc PH, Cremer M,
Barbier JP: Outcome after surgical resection of intraductal papillary and mucinous
tumors of the pancreas. Am J Gastroenterol, 2000. 95(2): p. 441-5.
56. Inagaki M, Maguchi M, Kino S, Obara M, Ishizaki A, Onodera K, Yokoyama K, Makino I,
Ojima H, Tokusashi Y, Miyokawa N, Kasai S: Mucin-producing tumors of the pancreas:
clinicopathological features, surgical treatment, and outcome. J Hepatobiliary
Pancreat Surg, 1999. 6(3): p. 281-5.
57. Kitagawa Y, Unger TA, Taylor S, Kozarek RA, Traverso LW: Mucus is a predictor of
better prognosis and survival in patients with intraductal papillary mucinous tumor
of the pancreas. J Gastrointest Surg, 2003. 7(1): p. 12-8; discussion 18-9.
58. Sugiura H, Kondo S, Islam HK, Ito K, Ono K, Morikawa T, Okushiba S, Katoh H:
Clinicopathologic features and outcomes of intraductal papillary-mucinous tumors of
the pancreas. Hepatogastroenterology, 2002. 49(43): p. 263-7.
59. Hruban RH, Adsay NV, Albores-Saavedra J, Compton C, Garrett ES, Goodman SN, Kern
SE, Klimstra DS, Kloppel G, Longnecker DS, Luttges J, Offerhaus GJ: Pancreatic
intraepithelial neoplasia: a new nomenclature and classification system for
pancreatic duct lesions. Am J Surg Pathol, 2001. 25(5): p. 579-86.
60. Hruban RH, Takaori K, Klimstra DS, Adsay NV, Albores-Saavedra J, Biankin AV, Biankin
SA, Compton C, Fukushima N, Furukawa T, Goggins M, Kato Y, Kloppel G, Longnecker
DS, Luttges J, Maitra A, Offerhaus GJ, Shimizu M, Yonezawa S: An illustrated consensus
on the classification of pancreatic intraepithelial neoplasia and intraductal papillary
mucinous neoplasms. Am J Surg Pathol, 2004. 28(8): p. 977-87.
61. Hruban RH, Goggins M, Parsons J, Kern SE: Progression model for pancreatic cancer.
Clin Cancer Res, 2000. 6(8): p. 2969-72.

63
62. Brat DJ, Lillemoe KD, Yeo CJ, Warfield PB, Hruban RH: Progression of pancreatic
intraductal neoplasias to infiltrating adenocarcinoma of the pancreas. Am J Surg
Pathol, 1998. 22(2): p. 163-9.
63. Brockie E, Anand A, Albores-Saavedra J: Progression of atypical ductal
hyperplasia/carcinoma in situ of the pancreas to invasive adenocarcinoma. Ann
Diagn Pathol, 1998. 2(5): p. 286-92.
64. Brune K, Abe T, Canto M, O'Malley L, Klein AP, Maitra A, Volkan Adsay N, Fishman EK,
Cameron JL, Yeo CJ, Kern SE, Goggins M, Hruban RH: Multifocal neoplastic precursor
lesions associated with lobular atrophy of the pancreas in patients having a strong
family history of pancreatic cancer. Am J Surg Pathol, 2006. 30(9): p. 1067-76.
65. Brown KM: Multidisciplinary approach to tumors of the pancreas and biliary tree.
Surg Clin North Am, 2009. 89(1): p. 115-31, ix.
66. Wilentz RE, Hruban RH: Pathology of cancer of the pancreas. Surg Oncol Clin N Am,
1998. 7(1): p. 43-65.
67. Hoimes CJ, Moyer MT, Saif MW: Biomarkers for early detection and screening in
pancreatic cancer. Highlights from the 45th ASCO annual meeting. Orlando, FL, USA.
May 29-June 2, 2009. JOP, 2009. 10(4): p. 352-6.
68. Duffy MJ, Sturgeon C, Lamerz R, Haglund C, Holubec VL, Klapdor R, Nicolini A, Topolcan
O, Heinemann V: Tumor markers in pancreatic cancer: a European Group on Tumor
Markers (EGTM) status report. Ann Oncol, 2009.
69. Steinberg WM, Gelfand R, Anderson KK, Glenn J, Kurtzman SH, Sindelar WF, Toskes PP:
Comparison of the sensitivity and specificity of the CA19-9 and carcinoembryonic
antigen assays in detecting cancer of the pancreas. Gastroenterology, 1986. 90(2): p.
343-9.

64
70. Goonetilleke KS, Siriwardena AK: Systematic review of carbohydrate antigen (CA 19-9)
as a biochemical marker in the diagnosis of pancreatic cancer. Eur J Surg Oncol, 2007.
33(3): p. 266-70.
71. Karachristos A, Scarmeas N, Hoffman JP: CA 19-9 levels predict results of staging
laparoscopy in pancreatic cancer. J Gastrointest Surg, 2005. 9(9): p. 1286-92.
72. Ferrone CR, Finkelstein DM, Thayer SP, Muzikansky A, Fernandez-delCastillo C,
Warshaw AL: Perioperative CA19-9 levels can predict stage and survival in patients
with resectable pancreatic adenocarcinoma. J Clin Oncol, 2006. 24(18): p. 2897-902.
73. Fry LC, Monkemuller K, Malfertheiner P: Molecular markers of pancreatic cancer:
development and clinical relevance. Langenbecks Arch Surg, 2008. 393(6): p. 883-90.
74. Wong JC, Lu DS: Staging of pancreatic adenocarcinoma by imaging studies. Clin
Gastroenterol Hepatol, 2008. 6(12): p. 1301-8.
75. Peddu P, Quaglia A, Kane PA, Karani JB: Role of imaging in the management of
pancreatic mass. Crit Rev Oncol Hematol, 2009. 70(1): p. 12-23.
76. Vachiranubhap B, Kim YH, Balci NC, Semelka RC: Magnetic resonance imaging of
adenocarcinoma of the pancreas. Top Magn Reson Imaging, 2009. 20(1): p. 3-9.
77. Miller FH, Rini NJ, Keppke AL: MRI of adenocarcinoma of the pancreas. AJR Am J
Roentgenol, 2006. 187(4): p. W365-74.
78. Irisawa A, Sato A, Sato M, Ikeda T, Suzuki R, Ohira H: Early diagnosis of small
pancreatic cancer: role of endoscopic ultrasonography. Dig Endosc, 2009. 21 Suppl 1:
p. S92-6.
79. DeWitt J, Devereaux B, Chriswell M, McGreevy K, Howard T, Imperiale TF, Ciaccia D,
Lane KA, Maglinte D, Kopecky K, LeBlanc J, McHenry L, Madura J, Aisen A, Cramer H,
Cummings O, Sherman S: Comparison of endoscopic ultrasonography and
multidetector computed tomography for detecting and staging pancreatic cancer.
Ann Intern Med, 2004. 141(10): p. 753-63.

65
80. Saftoiu A, Vilmann P: Role of endoscopic ultrasound in the diagnosis and staging of
pancreatic cancer. J Clin Ultrasound, 2009. 37(1): p. 1-17.
81. Boujaoude J: Role of endoscopic ultrasound in diagnosis and therapy of pancreatic
adenocarcinoma. World J Gastroenterol, 2007. 13(27): p. 3662-6.
82. Katz MH, Hwang R, Fleming JB, Evans DB: Tumor-node-metastasis staging of
pancreatic adenocarcinoma. CA Cancer J Clin, 2008. 58(2): p. 111-25.
83. Thomson BN, Banting SW, Gibbs P: Pancreatic cancer - current management. Aust
Fam Physician, 2006. 35(4): p. 212-7.
84. Bachmann J, Michalski CW, Martignoni ME, Buchler MW, Friess H: Pancreatic
resection for pancreatic cancer. HPB (Oxford), 2006. 8(5): p. 346-51.
85. Loos M, Kleeff J, Friess H, Buchler MW: Surgical treatment of pancreatic cancer. Ann N
Y Acad Sci, 2008. 1138: p. 169-80.
86. Hines OJ, Reber HA: Pancreatic surgery. Curr Opin Gastroenterol, 2006. 22(5): p. 520-6.
87. Wray CJ, Ahmad SA, Matthews JB, Lowy AM: Surgery for pancreatic cancer: recent
controversies and current practice. Gastroenterology, 2005. 128(6): p. 1626-41.
88. Ujiki MB, Talamonti MS: Surgical management of pancreatic cancer. Semin Radiat
Oncol, 2005. 15(4): p. 218-25.
89. Glanemann M, Shi B, Liang F, Sun XG, Bahra M, Jacob D, Neumann U, Neuhaus P:
Surgical strategies for treatment of malignant pancreatic tumors: extended, standard
or local surgery? World J Surg Oncol, 2008. 6: p. 123.
90. D'Souza MA, Shrikhande SV: Pancreatic resectional surgery: an evidence-based
perspective. J Cancer Res Ther, 2008. 4(2): p. 77-83.
91. Yeo CJ, Cameron JL, Lillemoe KD, Sohn TA, Campbell KA, Sauter PK, Coleman J, Abrams
RA, Hruban RH: Pancreaticoduodenectomy with or without distal gastrectomy and
extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma,

66
part 2: randomized controlled trial evaluating survival, morbidity, and mortality. Ann
Surg, 2002. 236(3): p. 355-66; discussion 366-8.
92. Michalski CW, Kleeff J, Wente MN, Diener MK, Buchler MW, Friess H: Systematic
review and meta-analysis of standard and extended lymphadenectomy in
pancreaticoduodenectomy for pancreatic cancer. Br J Surg, 2007. 94(3): p. 265-73.
93. Alexakis N, Halloran C, Raraty M, Ghaneh P, Sutton R, Neoptolemos JP: Current
standards of surgery for pancreatic cancer. Br J Surg, 2004. 91(11): p. 1410-27.
94. Aranha GV, Aaron JM, Shoup M, Pickleman J:et al., Current management of pancreatic
fistula after pancreaticoduodenectomy. Surgery, 2006. 140(4): p. 561-8; discussion
568-9.
95. Halloran CM, Ghaneh P, Bosonnet L, Hartley MN, Sutton R, Neoptolemos JP:
Complications of pancreatic cancer resection. Dig Surg, 2002. 19(2): p. 138-46.
96. Yeo CJ, Cameron JL, Sohn TA, Lillemoe KD, Pitt HA, Talamini MA, Hruban RH, Ord SE,
Sauter PK, Coleman J, Zahurak ML, Grochow LB, Abrams RA: Six hundred fifty
consecutive pancreaticoduodenectomies in the 1990s: pathology, complications, and
outcomes. Ann Surg, 1997. 226(3): p. 248-57; discussion 257-60.
97. Berberat PO, Friess H, Kleeff J, Uhl W, Buchler MW: Prevention and treatment of
complications in pancreatic cancer surgery. Dig Surg, 1999. 16(4): p. 327-36.
98. Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, Coleman J, Hodgin MB,
Sauter PK, Hruban RH, Riall TS, Schulick RD, Choti MA, Lillemoe KD, Yeo CJ: 1423
pancreaticoduodenectomies for pancreatic cancer: A single-institution experience. J
Gastrointest Surg, 2006. 10(9): p. 1199-210; discussion 1210-1.
99. Wagner M, Redaelli C, Lietz M, Seiler CA, Friess H, Buchler MW: Curative resection is
the single most important factor determining outcome in patients with pancreatic
adenocarcinoma. Br J Surg, 2004. 91(5): p. 586-94.

67
100. Cameron JL, Riall TS, Coleman J, Belcher KA: One thousand consecutive
pancreaticoduodenectomies. Ann Surg, 2006. 244(1): p. 10-5.
101. Riall TS, Cameron JL, Lillemoe KD, Winter JM, Campbell KA, Hruban RH, Chang D, Yeo
CJ: Resected periampullary adenocarcinoma: 5-year survivors and their 6- to 10-year
follow-up. Surgery, 2006. 140(5): p. 764-72.
102. Saif MW: Adjuvant treatment of pancreatic cancer in 2009: where are we? Highlights
from the 45th ASCO annual meeting. Orlando, FL, USA. May 29-June 2, 2009. JOP,
2009. 10(4): p. 373-7.
103. Mu DQ, Peng SY, Wang GF: Risk factors influencing recurrence following resection of
pancreatic head cancer. World J Gastroenterol, 2004. 10(6): p. 906-9.
104. Shibata K, Matsumoto T, Yada K, Sasaki A, Ohta M, Kitano S: Factors predicting
recurrence after resection of pancreatic ductal carcinoma. Pancreas, 2005. 31(1): p.
69-73.
105. Saif MW: Controversies in the adjuvant treatment of pancreatic adenocarcinoma.
JOP, 2007. 8(5): p. 545-52.
106. Kalser MH, Ellenberg SS: Pancreatic cancer. Adjuvant combined radiation and
chemotherapy following curative resection. Arch Surg, 1985. 120(8): p. 899-903.
107. Klinkenbijl JH, Jeekel J, Sahmoud T, van Pel R, Couvreur ML, Veenhof CH, Arnaud JP,
Gonzalez DG, de Wit LT, Hennipman A, Wils J: Adjuvant radiotherapy and 5-
fluorouracil after curative resection of cancer of the pancreas and periampullary
region: phase III trial of the EORTC gastrointestinal tract cancer cooperative group.
Ann Surg, 1999. 230(6): p. 776-82; discussion 782-4.
108. Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, Beger H, Fernandez-
Cruz L, Dervenis C, Lacaine F, Falconi M, Pederzoli P, Pap A, Spooner D, Kerr DJ, Buchler
MW: A randomized trial of chemoradiotherapy and chemotherapy after resection of
pancreatic cancer. N Engl J Med, 2004. 350(12): p. 1200-10.

68
109. Oettle H, Post S, Neuhaus P, Gellert K, Langrehr J, Ridwelski K, Schramm H, Fahlke J,
Zuelke C, Burkart C, Gutberlet K, Kettner E, Schmalenberg H, Weigang-Koehler K,
Bechstein WO, Niedergethmann M, Schmidt-Wolf I, Roll L, Doerken B, Riess H:
Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing
curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA,
2007. 297(3): p. 267-77.
110. Regine WF, Winter KA, Abrams RA, Safran H, Hoffman JP, Konski A, Benson AB,
Macdonald JS, Kudrimoti MR, Fromm ML, Haddock MG, Schaefer P, Willett CG, Rich
TA: Fluorouracil vs gemcitabine chemotherapy before and after fluorouracil-based
chemoradiation following resection of pancreatic adenocarcinoma: a randomized
controlled trial. JAMA, 2008. 299(9): p. 1019-26.
111. Tempero MA, Behrman S, Ben-Josef E, Benson AB 3rd, Cameron JL, Casper ES,
Hoffman JP, Karl RC, Kim P, Koh WJ, Kuvshinoff BW 2nd, Melvin WS, Muscarella P 2nd,
Sasson AR, Shibata S, Shrieve DC, Talamonti MS, Tyler DS, Vickers SM, Warren RS,
Willett C, Wolff RA: Pancreatic adenocarcinoma: Clinical Practice Guidelines in
Oncology. J Natl Compr Canc Netw, 2005. 3(5): p. 598-626.
112. Kim R, Saif MW: Is there an optimal neoadjuvant therapy for locally advanced
pancreatic cancer? JOP, 2007. 8(3): p. 279-88.
113. Rothenberg ML, Moore MJ, Cripps MC, Andersen JS, Portenoy RK, Burris HA 3rd, Green
MR, Tarassoff PG, Brown TD, Casper ES, Storniolo AM, Von Hoff DD: A phase II trial of
gemcitabine in patients with 5-FU-refractory pancreas cancer. Ann Oncol, 1996. 7(4):
p. 347-53.
114. Freitas D, Fernandes Gdos S, Hoff PM, Cunha JE: Medical management of pancreatic
adenocarcinoma. Pancreatology, 2009. 9(3): p. 223-32.

69
115. van Wagensveld BA, Coene PP, van Gulik TM, Rauws EA, Obertop H, Gouma DJ:
Outcome of palliative biliary and gastric bypass surgery for pancreatic head
carcinoma in 126 patients. Br J Surg, 1997. 84(10): p. 1402-6.
116. Lillemoe KD, Cameron JL, Yeo CJ, Sohn TA, Nakeeb A, Sauter PK, Hruban RH, Abrams
RA, Pitt HA: Pancreaticoduodenectomy. Does it have a role in the palliation of
pancreatic cancer? Ann Surg, 1996. 223(6): p. 718-25; discussion 725-8.
117. van der Schelling GP, van den Bosch RP, Klinkenbij JH, Mulder PG, Jeekel J: Is there a
place for gastroenterostomy in patients with advanced cancer of the head of the
pancreas? World J Surg, 1993. 17(1): p. 128-32; discussion 132-3.
118. Konishi M, Ryu M, Kinoshita T, Kawano N, Tanizaki H, Cho A: Stomach-preserving
gastric bypass for unresectable pancreatic cancer. Surg Today, 1997. 27(5): p. 429-33.
119. Wong GY, Schroeder DR, Carns PE, Wilson JL, Martin DP, Kinney MO, Mantilla CB,
Warner DO: Effect of neurolytic celiac plexus block on pain relief, quality of life, and
survival in patients with unresectable pancreatic cancer: a randomized controlled
trial. JAMA, 2004. 291(9): p. 1092-9.

70
FIGURES
Figure 1. Hypothesis of progression from precursor lesions to invasive carcinoma.
Schematic presentation of a hypothesis for the progression pathways from pancreatic
intraepithelial neoplasias (PanINs) and various subtypes of intraductal papillary mucinous
neoplasms (IPMNs) towards invasive carcinoma. Also, the mucin expression pattern of the
different types of PanINs and IPMNs, as well as the invasive carcinomas. PB type,
pancreatobiliary type; MNCC, mucinous noncystic carcinoma. Adapted from Takaori et al. [28]

71
TABLES
Table1. Staging of Pancreatic Adenocarcinoma (6th edition of the American Joint
Association on Cancer).
Note that, in general, Stages I and II are reserved for potentially resectable disease, Stage III for
locally unresectable disease, and Stage IV for metastatic disease. LN, lymph node; CA, celiac
axis; SMA, superior mesenteric artery; CHA, hepatic artery. Adapted from Katz et al [82].
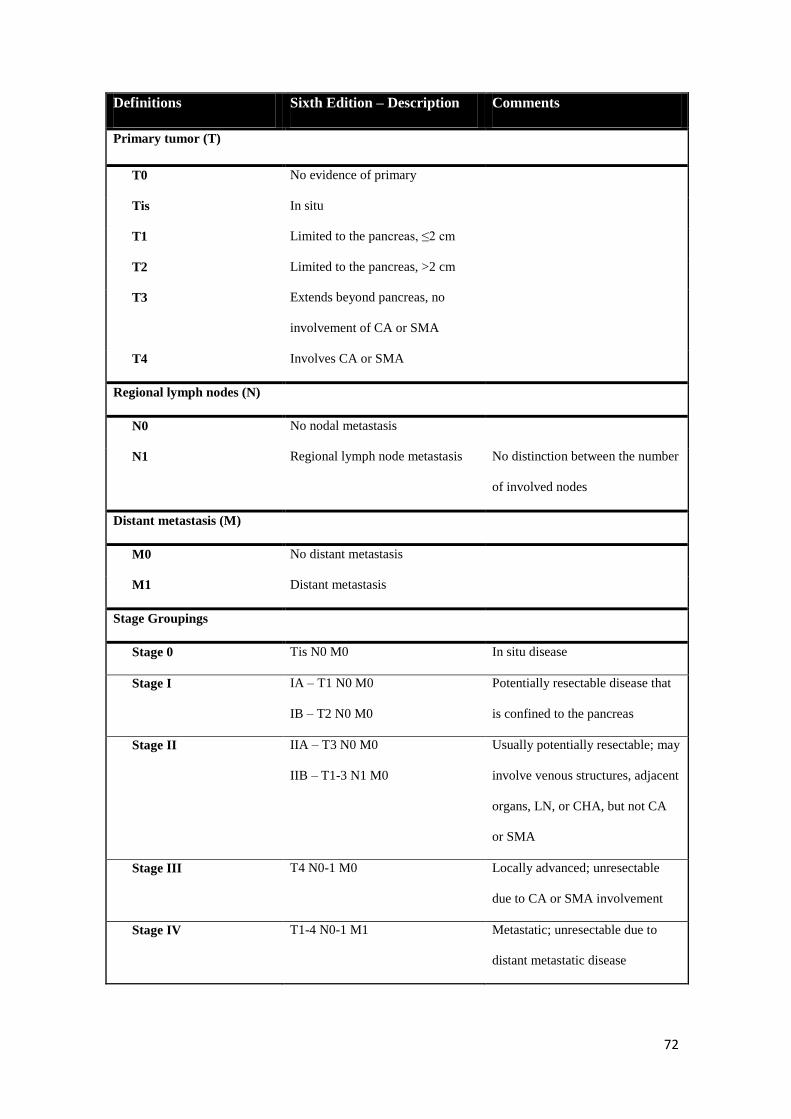
72
Definitions Sixth Edition – Description Comments
Primary tumor (T)
T0 No evidence of primary
Tis In situ
T1 Limited to the pancreas, ≤2 cm
T2 Limited to the pancreas, >2 cm
T3 Extends beyond pancreas, no
involvement of CA or SMA
T4 Involves CA or SMA
Regional lymph nodes (N)
N0 No nodal metastasis
N1 Regional lymph node metastasis No distinction between the number
of involved nodes
Distant metastasis (M)
M0 No distant metastasis
M1 Distant metastasis
Stage Groupings
Stage 0 Tis N0 M0 In situ disease
Stage I IA – T1 N0 M0
IB – T2 N0 M0
Potentially resectable disease that
is confined to the pancreas
Stage II IIA – T3 N0 M0
IIB – T1-3 N1 M0
Usually potentially resectable; may
involve venous structures, adjacent
organs, LN, or CHA, but not CA
or SMA
Stage III T4 N0-1 M0 Locally advanced; unresectable
due to CA or SMA involvement
Stage IV T1-4 N0-1 M1 Metastatic; unresectable due to
distant metastatic disease