canabinóides sintéticos e as novas drogas...
TRANSCRIPT
Canabinóides Sintéticos e as Novas drogas psicoativas
Leonardo Ludwig Paim
Médico Psiquiatra
Mestre em Psiquiatria – UFRGS

“O termo designer drug refere-se a um grupo de substâncias sintéticas com efeitos similares a
drogas ilícitas”
NIDA

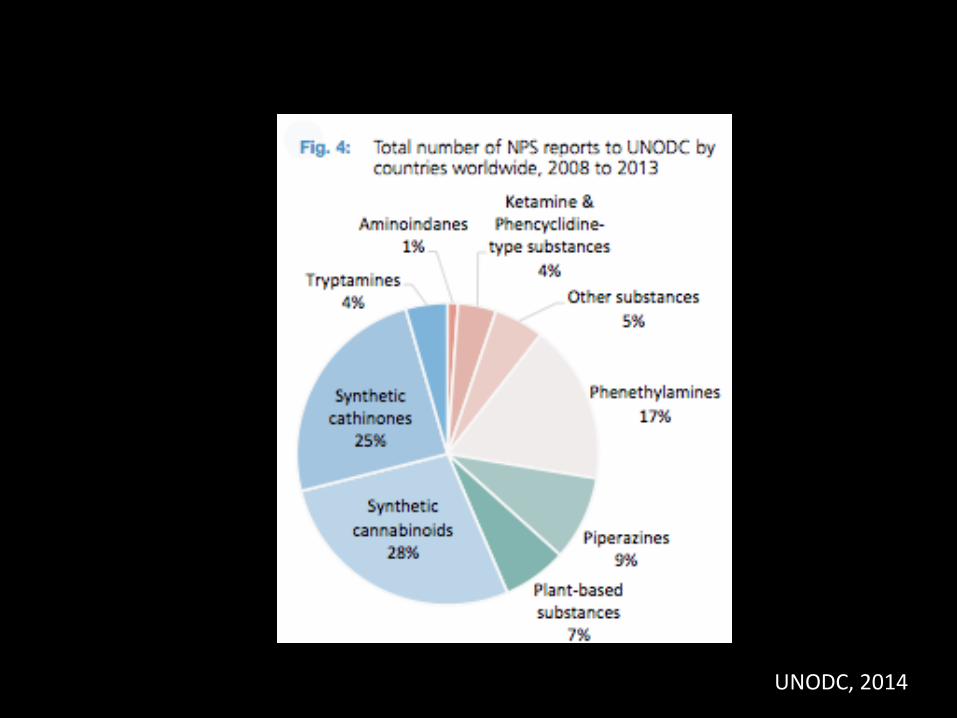
Identificação de Novas Substâncias Psicoativas (NPS)
UNODC, 2014
UNODC, 2014

Novas Substâncias Psicoativas Detectadas
UNODC, 2014



EMMCDDA, 2014

Visitas a emergência por intoxicação
Maxwell JC, Drug Alcohol Dep, 2014

Apreensões Ecstasy America Latina
UNODC, 2014

Ecstasy x Cocaína
LENAD II, resultados parciais

Composição dos Comprimidos de Ecstasy no Brasil
Togni LR et al, J Forensic Sci, 2014

Plano de apresentação
• MDMA
• N-BOME
• Canabinoides sintéticos
• Catinonas sintéticas
“Quantos de vocês viram a Molly hoje?”
Madonna Ultra Music Festival, Miami, 2012


MDMA 3-4 metilenodioximetanfetamina
EMCDA, 2013

MDMA 3-4 metilenodioximetanfetamina
1912 – Síntese pelo laboratório Merck
1950 – Primeiros estudos em animais
1978 – Primeira descrição de seus efeitos
1980 – Inicio do uso recreativo
1985 – Proibida nos Estados Unidos
Meyer JS, Subst Abuse Reab 2013
Nomenclatura
• Ecstasy
• Bala
• XTC
• A
• E
• MD
• ADAM




Mecanismo de Ação
• Ligação ao transportador de monoaminas
– Serotonina
– Dopamina
– Noradrenalina

Principais Vias
• Nucleo da Rafe
• Neocortex
• Amidala
• Hipocampo
NIDA

Ocupação do Transportador
dancesafe.org

Liberação Mediada por Transportador
dancesafe.org

Inundação de 5-HT, DA, NE na Fenda Sináptica
dancesafe.org

Dopamina
• Euforia
• Excitabilidade
• Reforço ao uso


Noradrenalina
• Taquicardia
• Aumento da pressão arterial
• Hipertermia
Hysek CM et al, Br J Pharmacol, 2012

Serotonina
• Alterações de percepção – 5HT2a
• Prazer no movimento e toque
• Efeito pró-social – 5HT1a
– Empatia
– Proximidade com o outro
– Conexão com o mundo ou com sentimentos
Meyer JS, Subst Abuse Reab 2013

Ocitocina e MDMA
• 5-HT1a estimula liberação de ocitocina nos núcleos supraóptico e paraventricular
• Ativação de circuitos de “affiliative behavior”
• Hiponatremia, desidratação e hipertermia aumentam ainda mais a secreção de ocitocina
McGregor IS, Hormon Behav 2012

Efeitos Pós-Uso Agudo
• Midweekend blues
• Alterações cognitivas
Depleção de serotonina
– Bloqueio do transportador de monoaminas
– Bloqueio da triptofano-hidroxilase

Efeitos Crônicos
• Trajetória de uso de cerca de 1 ano
– 1 a 2 comprimidos por semana
• Alteração de Funções cognitivas superiores
• Maior presença de sintomas psiquiátricos
Smirnov et al, Addict Behav, 2013; Parrot ES, Neurosci Biobehav Rev, 2013
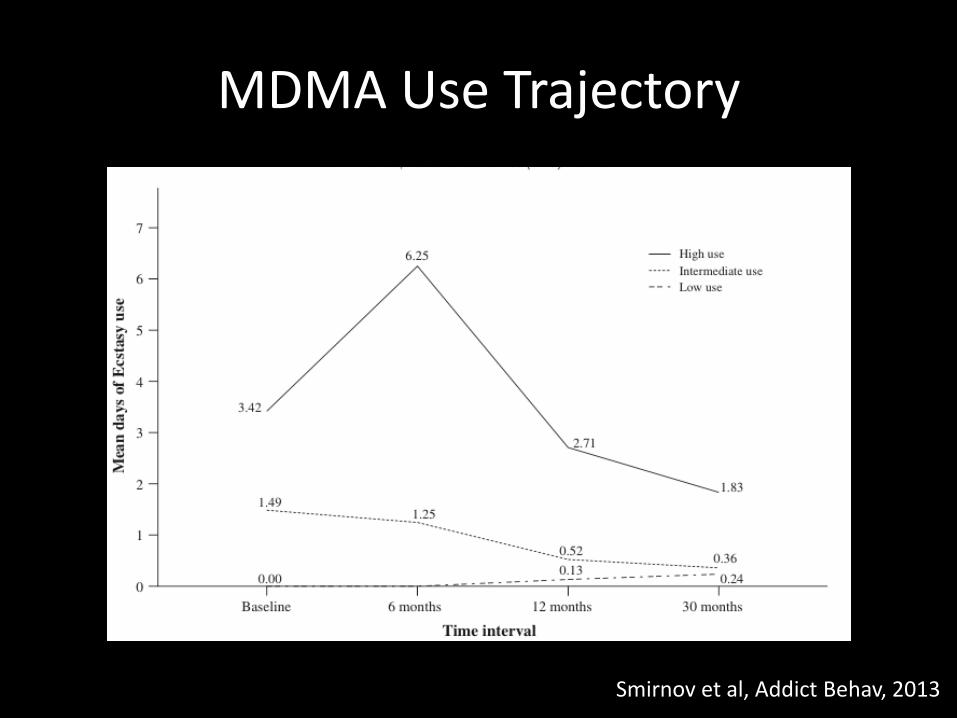
MDMA Use Trajectory
Smirnov et al, Addict Behav, 2013
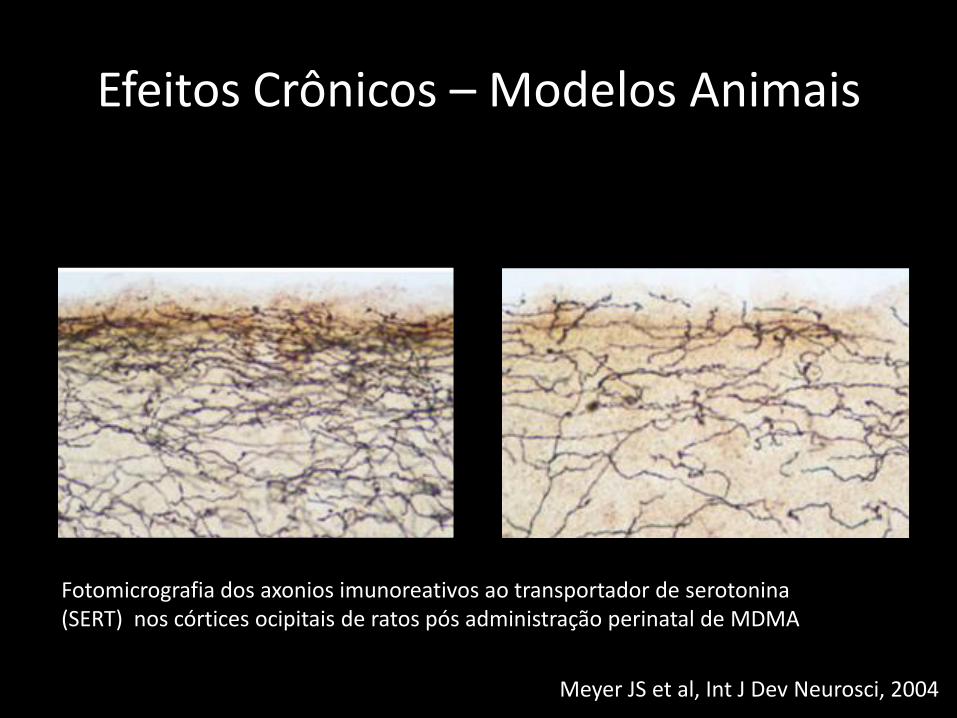
Efeitos Crônicos – Modelos Animais
Substance Abuse and Rehabilitation 2013:4submit your manuscript | www.dovepress.com
Dovepress
Dovepress
90
Meyer
Fisk and Sharp68 proposed that working memory consists
of a central executive function along with four subcompo-
nents which they termed “updating,” “attention shifting,”
“inhibition,” and “access to long-term memory.” A recent
meta-analysis comparing ecstasy users to polydrug-using
controls on these four subcomponents found significant
ecstasy-associated deficits in updating, attention shifting, and
access to long-term memory.69 Effect sizes were generally
moderate for the three significant subcomponents, whereas
the inhibition subcomponent was not significantly affected.
Meta-analyses that examined aspects of cognitive function
other than memory found significant impairment in attention
and concentration, verbal comprehension, processing speed,
and motor/psychomotor speed.70,71 Together with the reviews
of memory performance, these findings suggest that regular
ecstasy users suffer from widespread problems across a wide
range of cognitive domains.
Despite the positive findings from a number of different
analyses, the literature on cognitive deficits in ecstasy users
suffers from some of the same interpretive problems as the lit-
erature on mood changes. For example, Gouzoulis-Mayfrank
and Daumann19 discuss the issue that, even if ecstasy users
are compared to drug users who do not consume ecstasy, the
latter often have a more moderate pattern of drug consumption
than the ecstasy-using group. Cannabis is particularly prob-
lematic in studies of cognitive function, given the evidence
for significant cognitive deficits in heavy cannabis users.72
Comorbidity of psychopathology with ecstasy use may
additionally contribute to the cognitive impairment observed
in some studies.73 Finally, the typical use of cross-sectional
studies again makes it impossible, in such cases, to ascertain
whether cognitive differences between the ecstasy-using and
control group(s) preceded or followed the onset of ecstasy
use. Two prospective studies have addressed this issue by
recruiting new ecstasy users, assessing their cognitive function
at baseline, and then retesting the subjects from 1 to 3 years
later.74,75 Interestingly, in both cases, the users did not differ
from controls at baseline but did exhibit significant deficits in
immediate and delayed verbal recall memory. These findings
point up the limitations inherent in cross-sectional studies in
which baseline mood or cognitive function prior to the onset
of ecstasy use is not known. Importantly, the results suggest
that, at least for some ecstasy users, repeated exposure to the
drug leads to later impairment in certain cognitive domains.
Longitudinal studies of up to 2 years in length have also
asked whether cognitive function keeps declining with con-
tinued ecstasy use, and whether cessation of use leads to a
recovery of cognitive function. In general, such studies have
found neither further deterioration in users nor recovery of
function in subjects who discontinued ecstasy use76–78 (see
Zakzanis and Campbell79 for an exception to these findings).
Because in these studies the ecstasy users already differed from
controls at the time of initial testing, the results are difficult to
interpret. There may have been preexisting cognitive differences
that were unchanged by ecstasy use, or the typical use patterns
of the subjects in the first three studies may have caused an
asymptotic decline in cognitive performance that neither got
worse over time nor recovered upon 2 years of abstinence.
NeurotoxicityThe abovementioned evidence for mood changes and neurop-
sychological deficits in ecstasy users raises the question of
how MDMA might be acting within the brain to cause these
effects. The answer given most often centers around numer-
ous findings obtained from experimental animals, mainly
rats and nonhuman primates (eg, squirrel monkeys), for a
toxic effect of MDMA on the serotonergic system. The first
evidence for MDMA neurotoxicity was published in the mid-
1980s, and these and numerous follow-up studies showed that
high doses of MDMA (or MDA) lead to a long-lasting deple-
tion of 5-HT, reduced 5-HT uptake and SERT binding sites,
and decreased activity of tryptophan hydroxylase in forebrain
areas such as the neocortex, hippocampus, and striatum (see
Green et al33). Time-course studies demonstrated a biphasic
action of MDMA consisting of the initial 5-HT depletion
discussed earlier, a short-term recovery of 5-HT levels seen
at 1–2 days following dosing, and then a secondary, more
long-lasting depletion measured at 1–2 weeks and beyond.33
Histological examination of brain tissues from treated rats
and monkeys consistently showed a persistent reduction in
the density of axons immunoreactive for 5-HT or for SERT
(Figure 1). Moreover, staining of brain tissues obtained at
Figure 1 Photomicrograph of serotonin transporter-immunoreactive axons
in the upper layers of occipital cortex of a control rat (A) compared to a 3,4-
methylenedioxymethamphetamine (MDMA)-treated rat ( B).
Notes: The animals received twice-daily injections of either saline or MDMA
(10 mg/kg per injection) from the firs t to the fourth day of life and then were
killed at 9 months of age (see Meyer et al80 for experimental details). These results
illustrate the long-lasting nature of MDMA-induced serotonergic defici ts when the
drug is administered early in development.
Substance Abuse and Rehabilitation 2013:4submit your manuscript | www.dovepress.com
Dovepress
Dovepress
90
Meyer
Fisk and Sharp68 proposed that working memory consists
of a central executive function along with four subcompo-
nents which they termed “updating,” “attention shifting,”
“inhibition,” and “access to long-term memory.” A recent
meta-analysis comparing ecstasy users to polydrug-using
controls on these four subcomponents found significant
ecstasy-associated deficits in updating, attention shifting, and
access to long-term memory.69 Effect sizes were generally
moderate for the three significant subcomponents, whereas
the inhibition subcomponent was not significantly affected.
Meta-analyses that examined aspects of cognitive function
other than memory found significant impairment in attention
and concentration, verbal comprehension, processing speed,
and motor/psychomotor speed.70,71 Together with the reviews
of memory performance, these findings suggest that regular
ecstasy users suffer from widespread problems across a wide
range of cognitive domains.
Despite the positive findings from a number of different
analyses, the literature on cognitive deficits in ecstasy users
suffers from some of the same interpretive problems as the lit-
erature on mood changes. For example, Gouzoulis-Mayfrank
and Daumann19 discuss the issue that, even if ecstasy users
are compared to drug users who do not consume ecstasy, the
latter often have a more moderate pattern of drug consumption
than the ecstasy-using group. Cannabis is particularly prob-
lematic in studies of cognitive function, given the evidence
for significant cognitive deficits in heavy cannabis users.72
Comorbidity of psychopathology with ecstasy use may
additionally contribute to the cognitive impairment observed
in some studies.73 Finally, the typical use of cross-sectional
studies again makes it impossible, in such cases, to ascertain
whether cognitive differences between the ecstasy-using and
control group(s) preceded or followed the onset of ecstasy
use. Two prospective studies have addressed this issue by
recruiting new ecstasy users, assessing their cognitive function
at baseline, and then retesting the subjects from 1 to 3 years
later.74,75 Interestingly, in both cases, the users did not differ
from controls at baseline but did exhibit significant deficits in
immediate and delayed verbal recall memory. These findings
point up the limitations inherent in cross-sectional studies in
which baseline mood or cognitive function prior to the onset
of ecstasy use is not known. Importantly, the results suggest
that, at least for some ecstasy users, repeated exposure to the
drug leads to later impairment in certain cognitive domains.
Longitudinal studies of up to 2 years in length have also
asked whether cognitive function keeps declining with con-
tinued ecstasy use, and whether cessation of use leads to a
recovery of cognitive function. In general, such studies have
found neither further deterioration in users nor recovery of
function in subjects who discontinued ecstasy use76–78 (see
Zakzanis and Campbell79 for an exception to these findings).
Because in these studies the ecstasy users already differed from
controls at the time of initial testing, the results are difficult to
interpret. There may have been preexisting cognitive differences
that were unchanged by ecstasy use, or the typical use patterns
of the subjects in the first three studies may have caused an
asymptotic decline in cognitive performance that neither got
worse over time nor recovered upon 2 years of abstinence.
NeurotoxicityThe abovementioned evidence for mood changes and neurop-
sychological deficits in ecstasy users raises the question of
how MDMA might be acting within the brain to cause these
effects. The answer given most often centers around numer-
ous findings obtained from experimental animals, mainly
rats and nonhuman primates (eg, squirrel monkeys), for a
toxic effect of MDMA on the serotonergic system. The first
evidence for MDMA neurotoxicity was published in the mid-
1980s, and these and numerous follow-up studies showed that
high doses of MDMA (or MDA) lead to a long-lasting deple-
tion of 5-HT, reduced 5-HT uptake and SERT binding sites,
and decreased activity of tryptophan hydroxylase in forebrain
areas such as the neocortex, hippocampus, and striatum (see
Green et al33). Time-course studies demonstrated a biphasic
action of MDMA consisting of the initial 5-HT depletion
discussed earlier, a short-term recovery of 5-HT levels seen
at 1–2 days following dosing, and then a secondary, more
long-lasting depletion measured at 1–2 weeks and beyond.33
Histological examination of brain tissues from treated rats
and monkeys consistently showed a persistent reduction in
the density of axons immunoreactive for 5-HT or for SERT
(Figure 1). Moreover, staining of brain tissues obtained at
Figure 1 Photomicrograph of serotonin transporter-immunoreactive axons
in the upper layers of occipital cortex of a control rat (A) compared to a 3,4-
methylenedioxymethamphetamine (MDMA)-treated rat ( B).
Notes: The animals received twice-daily injections of either saline or MDMA
(10 mg/kg per injection) from the firs t to the fourth day of life and then were
killed at 9 months of age (see Meyer et al80 for experimental details). These results
illustrate the long-lasting nature of MDMA-induced serotonergic defici ts when the
drug is administered early in development.
Fotomicrografia dos axonios imunoreativos ao transportador de serotonina (SERT) nos córtices ocipitais de ratos pós administração perinatal de MDMA
Meyer JS et al, Int J Dev Neurosci, 2004

Efeitos Crônicos - Humanos
Iorio CR et al, Arch Gen Psych, 2012

Efeitos Crônicos - Humanos
Urban NB et al, neuropsychophamacology, 2012

Mecanismos de Neurotoxidade
• Pouco elucidado
• Envolve Espécies Ativas de Oxigênio (ROS)
• Hipotese do metabólito neurotóxico
• Hipotese do influxo de dopamina nos neurônios serotonérgicos
Meyer JS, Subst Abuse Reab 2013

Morbi-Mortalidade
• Série de casos de uma rave em San Francisco:
– 12 pacientes admitidos em CTI
– 10 deles com temperaturas de 40-43oC
– 8 necessitaram entubação endotraqueal
– 2 óbitos
• Análise de 106 casos de óbitos por MDMA
– 43% envolviam antidepressivos ou fármacos serotonérgicos
Pilgrim JL et al 2011; Armenian P et al, 2013

“Seu Doce era LSD ou N-BOME?”
Anônimo
Web Forum

N-BOME

N-BOME
• Família de compostos derivados da feniletilamina
• Notoriedade recente devido a múltiplos óbitos relacionados com overdose
• Ingerido inadvertidamente com LSD
• Vendido livremente em webpages
Ninneman A et al, 2013; Bersani FS et al, 2013, Zuba D, 2013

N-BOME
• Não existem estudos de prevalência
• 2,6% de 22,289 individuos que responderam ao Global drug Survey usaram
• 11,3% dos frequentadores de casas noturnas conhecem a droga
Wood DM, 2015, Bersani FS, 2013

LSD

Nomenclatura
• N-Bomb
• Pandora
• Boom
• Holland Film
• Dime

Mecanismo de Ação
• Potente agonista parcial 5HT2A
• Efeitos lembram os alucinógenos clássicos como LSD com algumas características de anfetaminas
Bersani FS et al, 2013

Efeitos
• Adormecimento da língua
– Diferencia da intoxicação por LSD
• Body high: formigamento em todo corpo
• Euforia
• Agitação psicomotora intensa
Bersani FS et al, 2013

Efeitos Psicodélicos
• Instrospeção
• Despersonalização
• Desrealização
• Alucinações visuais e auditivas
– Reconhecimento de padrões
– Borramento visual
– Tracing
Bersani FS et al, 2013

Litgens RP et al 2014

Litgens RP et al 2014

Litgens RP et al 2014

Modulação de Impulsos Visuais por Neurônios Serotonérgicos
Litgens RP et al 2014

Toxicidade
• Confusão
• Agitação psicomotora
• Hipertensão
• Taquicardia
• Hipertermia
• Convulsões
• Acidose metabólica
• Falência de múltiplos orgãos
Síndrome Serotonérgica

Toxicidade
• 29 óbitos por toxicidade aguda
• 25 casos adicionais relatados no EMMCDA
• Muito mais tóxico que o ácido lisérgico
• Conhecimento dos efeitos desta nova droga são especialmente importantes no contexto das emergências médicas
Bersani FS et al, 2013

Canabinóides Sintéticos

Introdução
• Canabinóides sintéticos: análogos ao THC (princípio ativo da maconha).
• Fazem parte das designer drugs.
Vendidos misturados a ervas em produtos chamados:
• Spice, K2, Synthetic Marijuana, Dream, Yucatan Fire, Aroma…
• Brasil: Hi-5, Incenso do Mal
• Pouca informação (não ECR).
Amsterdam JV 2015; NIDA 2014
Spaderna M 2014


Introdução
• 2014 (EMCDDA): relato de 207 canabinóides sintéticos.
• Canabinóides mais encontrados: JWH-018, JWH-07, CP-47,497, XLR11, AM2201, JWH-122, JWH-210.
• Efeitos similares a maconha, porém mais intensos.
Brents LK 2014; Seely KA 2013
Hohmann N 2014

Histórico “Maconha Sintética”
Adaptado de Fattore L 2011; cortesia de Dr Petros Levounis
Br: ANVISA proibe
JWH-018

Introdução
• Vendidos: internet , postos de gasolina ou em lojas como incensos ou odorizadores de ambiente.
• “Not for human consumption”.
Cottencin O 2014
Castaneto MS 2014

Introdução
Motives de uso:
•Curiosidade (78-91%),
•Sentir-se Bem/ficar “chapado”(89%)
•Relaxar (71%)
•Ficar “chapado” e escapar do screening de drogas(30%)
Amsterdam JV 2015, Castaneto MS 2014; Bonar 2014

Introdução
• Não são detectados em testes usuais de maconha.
• EUA: Apenas 34% dos médicos que trabalham em emergências sabiam o que era K2 e 49% o que era Spice.
• 91,3% dos usuários de canabonóides sintéticos também usam maconha.
Spaderna M 2014; Lank PM 2013
Lank PM 2013
Castaneto MS 2014

Mecanismo de Ação Canabinóides Sintéticos
Canabinóides Sintéticos (JWH-018) THC
Agonista de CB1 e CB2 Agonista CB1 e CB2
Agonista total de CB1 Agonista parcial CB1
4 X mais afinidade ao CB1 -
10 X mais afinidade ao CB2 -
• Canabinóides sintéticos 2-100 vezes mais potentes que THC.
Castaneto MS 2014; Spaderna M 2014; Fattore L 2011
• Não há dados sobre a ação do Spice em seres humanos. Alves AO 2012

Adaptado de NIDA 2014 por Ribeiro M

Estrutura de um Canabinóide Sintético
JWH-018
Hohmann N 2014

Number of New Psychoactive
Substance reported EU Early Warning System
(2005-14)
EMCDDA 2015

Uso de Drogas em Estudantes da 8th e 12th Séries
Monitoring The Future 2014 (NIDA)

NIDA 2014

Efeitos Canabinóides Sintéticos
Cardiovascular:
•Taquicardia
•Hipertensão
•IAM
Neurológico:
•Tontura
•Convulsão
•AVC
•Déficit cognitivo
•Déficit de memória
Psiquiátrico:
•Euforia/relaxamento
•Agitação
•Alucinação
•Ansiedade
•Pânico
•Psicose (18–41% nas emergências)
Castaneto MS 2014; Hohmann N 2014; EMCDDA 2014
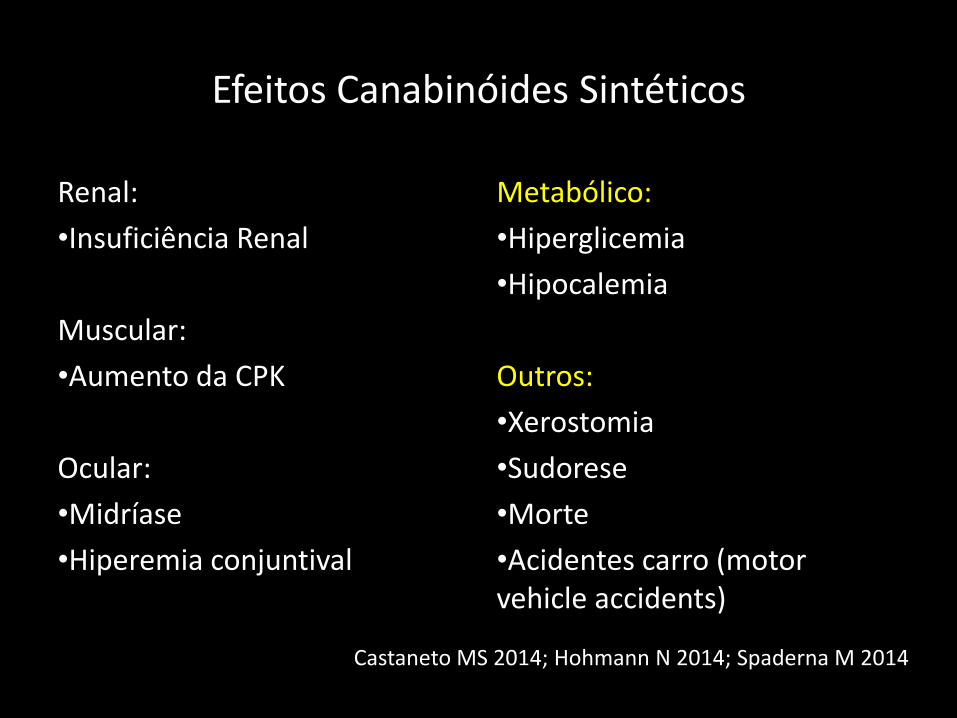
Efeitos Canabinóides Sintéticos
Renal:
•Insuficiência Renal
Muscular:
•Aumento da CPK
Ocular:
•Midríase
•Hiperemia conjuntival
Metabólico:
•Hiperglicemia
•Hipocalemia
Outros:
•Xerostomia
•Sudorese
•Morte
•Acidentes carro (motor vehicle accidents)
Castaneto MS 2014; Hohmann N 2014; Spaderna M 2014

Tratamento de Emergência
• 30 vezes mais chance de necessitar de serviço de emergência após o uso de canabinoides sintéticos do que com canabis
Sintomas mais comuns:
• Pânico
• Ansiedade
• Paranóia
Winstock A 2015
Mais frequente em usuários de canabinóides sintéticos

NIDA 2014
41 casos de overdose em New Hampshire em agosto 2014

Catinonas Sintéticas (Sais de Banho)

Histórico
• Catinona encontrada nas folhas da planta Catha edulis (Kthat).
• Catinonas sintéticas são derivados anfetamínicos similares às metanfetaminas e ao ecstasy.
Katz DP 2014; Capriola M 2013
Hohmann N 2014

Catinonas Sintéticas
• Vendidas como sais de banho, repelentes de insetos, odorizador de ambiente, fertilizantes para plantas.
• Mais comuns: mefedrona, metilona e MDPV (3,4-metilenodioxipirovalerona).
• Nomes coloquiais: Sais de Banho, Vanila Sky, Ivory Wave, Cloud 9, Miau Miau.
Hohmann N 2014
Capriola M 2013

Histórico
• 2000: surgiu como alterantiva legalizada para o “high” das anfetaminas, cocaína, ecstasy.
• 2012 (EUA): mefedrone, MDPV e metilona entram na lista das
substâncias controladas . No Brasil também são proscritas.
• Muitas ainda legalizadas (dificuldade de reconhecer). • Existem > 40 tipos de catinonas sintéticas no mercado
clandestino.
Glennon RA 2014
Valente MJ 2014
ANVISA 2014; Capriola M 2013
Valente MJ 2014


Catinonas Sintéticas
Capriola M 2013

Catinonas Sintéticas
•Origem: China e India.
•Venda: internet, postos de gasolina, “head shops”, lojas de conveniência.
•Uso: oral, intranasal ou injetável.
•Não detectada por screening.
Capriola M 2013
Paillet-Loilier M 2014

Mecanismos de Ação Catinonas Sintéticas
• Inibem a recaptação da dopamina, noradrenalina, serotonina
• Estudos ratos: também demonstrou aumento da liberação desses neurotransmissores
• Algumas (mefedrona): aumentam liberação de dopamina, como as metanfetaminas
• Outras: inibem a recaptação de dopamina, como a cocaína
Paillet-Loilier M 2014; Zawilska JB 2013

Prevalência Anual de uso de substâncias ilicitas por estudantes da 12a série
UNODC 2014

Efeitos Catinonas Sintéticas
Aumento:
•Energia/ Euforia
•Libido
•Percepções (orgãos sentidos)
•Sociabilidade
Redução:
•Apetite
Johnson PS 2014; Hohmann N 2014; Paillet-Loilier M 2014

Efeitos Adversos Catinonas Sintéticas
Cardiovascular:
•Taquicardia
•Hipertensão
•Dor precordial
Neurológico:
•Convulsão
•Cefaléia
•Midríase
Psiquiátricos:
•Agitação
•Agressão
•Paranóia
•Alucinação
•Depressão
•Ansiedade
Hohmann N 2014; Blum K 2013
Efeitos Adversos Catinonas Sintéticas
Gastrointestinal:
•Vômitos
Renal:
•Aumento de CPK
•Insuficiência Renal
Muscular:
•Rabdomiólise
Metabólico:
•Hipocalemia
Outros:
•Febre
•Bruxismo
•Morte
Hohmann N 2014; Blum K 2013

Conclusões
• Novo desafio para profissionais de saúde.
• Consumo de drogas sintéticas vem aumentando em todo o mundo nos últimos anos.
• Parecem ser mais potentes do que as drogas não sintéticas.
• Pouca informação sobre consumo e efeitos à longo prazo em humanos.
• Dificuldades legais de conter novas subsâncias.