simpÓsio internacional de cÂncer de pulmÃo · 2018-03-22 · carlos henrique teixeira...
TRANSCRIPT

CÂNCER DE PULMÃO DE PEQUENAS CÉLULAS: UPDATES 2018Carlos Henrique Teixeira
Coordenador do grupo de tórax do centro de oncologia do HAOC

CONFLITOS DE INTERESSE
• AULAS MÉDICAS – ROCHE, BMS, MSD, BI, AZ
• PESQUISA CLÍNICA – PI estudos AZ, MSD
• APOIO CONGRESSOS – MSD, BMS, AZ, ROCHE, BI
• MEMBRO DO GBOT, SBOC, ASCO

SCLC (CPPC)
Tabagismo, dça bulky
Rápida progressão
Disseminação precoce
15% CP
adeno cec cppc outros
Oronsky B, et al. Neoplasia. 2017;19:842-847. Alvarado-Luna G, et al. Transl Lung
Cancer Res. 2016;5:26-38. Howlander N, et al. SEER Cancer Statistics Review,
1975-2014.

CPPC (SCLC)• DOENÇA LIMITADA ~30% • DOENÇA EXTENSA ~70%
• 74 – 84% recorrência
• 71 - 76 % em 2y
PADRÃO:
• RT + (Cis + Etop) PCI*
• ORR: 70 – 90%;
• OS: 14 – 23 m; 5y 16 – 26%
Definição: EC I-III
INCLUIDO NUM
CAMPO RT.
novas terapias
2L:
•2L Plat-r: No SOC (ORR <5%)
•2L Plat-s (>3 < 6m): topotecan
•ORR: 24%, PFS: 3mo, OS: 6m
•2L Plat-S (> 6 m): Cis + Etop
•ORR: 50-60%, PFS: 4-6m
PADRÃO 1L:
•Cis + Etop PCI*
•ORR: 50-70%
•PFS: 4-6m / OS: 8-10m
Definição: EC IV ou muito
extensa para um campo de
RT
• Lopez-Chavez et al. Curr Probl Cancer. 2012;Turrisi et al. NEJM 1999• SCLC NCCN guidelines 2015, www.nccn.org; Kantar Health CancerMPact SCLC 2014; www.cancer.gov

Timeline SCLC
Sabari JK, et al. Nat Rev Clin Oncol. 2017;14:549-561.
1985 1990 1995 2000 2005 2010 2015
First-linesetting
Refractory/recurrentsetting
Radiationtherapy
Cisplatin +etoposide*
1985
Carboplatin +etoposide*
1999
Carboplatin + irinotecan2006
Cisplatin + irinotecan2006
Irinotecan1992
Topotecan*1996
Docetaxel1994
Paclitaxel1998
Gemcitabine2001
Temozolomide2012
Thoracicradiotherapy(LS-SCLC)*
1992
45 Gy BID (LS-SCLC)*
1999PCI (LS-SCLC)*1999
PCI (ES-
SCLC)2007
Thoracicradiotherapy(ES-SCLC)
2015*FDA approved.

INTERGROUP 0096
Nejm 1999

CONVERT TRIAL
• Fase 3 R
• EP: OS
• ESTUDO COM PODER PARA MOSTRAR SUP RT QD SE 2-yr OS 12% MAIOR QUE RT BID
• 2-yr OS rate: 51% for QD vs 56% for BID; absolute difference: 5.3%
• SEM DIF SIGNIFICATIVA RT QD vs BID
• 25 mos for QD vs 30 mosfor BID; HR: 1.18 (95% CI: 0.95-1.45; P = .14)
TOXICIDADE SIMILAR
ADULTOS COM
DOENÇA LOCALIZADA
PS – 0-1
(N = 547)
Fup
5y
BID 1.5 Gy thoracic RT
45 Gy/30F/19D* +
Chemotherapy†
(n = 274)
Once-daily 2 Gy thoracic RT
66 Gy/33F/45D* +
Chemotherapy†
(n = 273)
Faivre-Finn C, et al. Lancet Oncol 2017;18:1116-1125.
*RT started on Day 22 after starting chemotherapy. †Cisplatin 25 mg/m2 on Days 1-3 or cisplatin 75 mg/m2 on Day 1 and etoposide 100 mg/m2 on Days 1-3 for 4 or 6 cycles Q3W.


JAMA OncologyPublished online January 4, 2018

ALL POP:
23% No QT
41% - No RT
Treatment Patterns in Extensive Disease Small Cell Lung Cancer Across the United States, Europe, and Japan
Karen Higginbottom,1 Marco DiBonaventura,1 John R. Penrod,2 Yong Yuan2
1Ipsos Healthcare, Mahwah, NJ, USA; 2Bristol-Myers Squibb, Princeton, NJ, USA
8479: Treatment Patterns in Extensive Disease Small Cell Lung Cancer Across the United States, Europe, and Japan – Yong Yuan
13
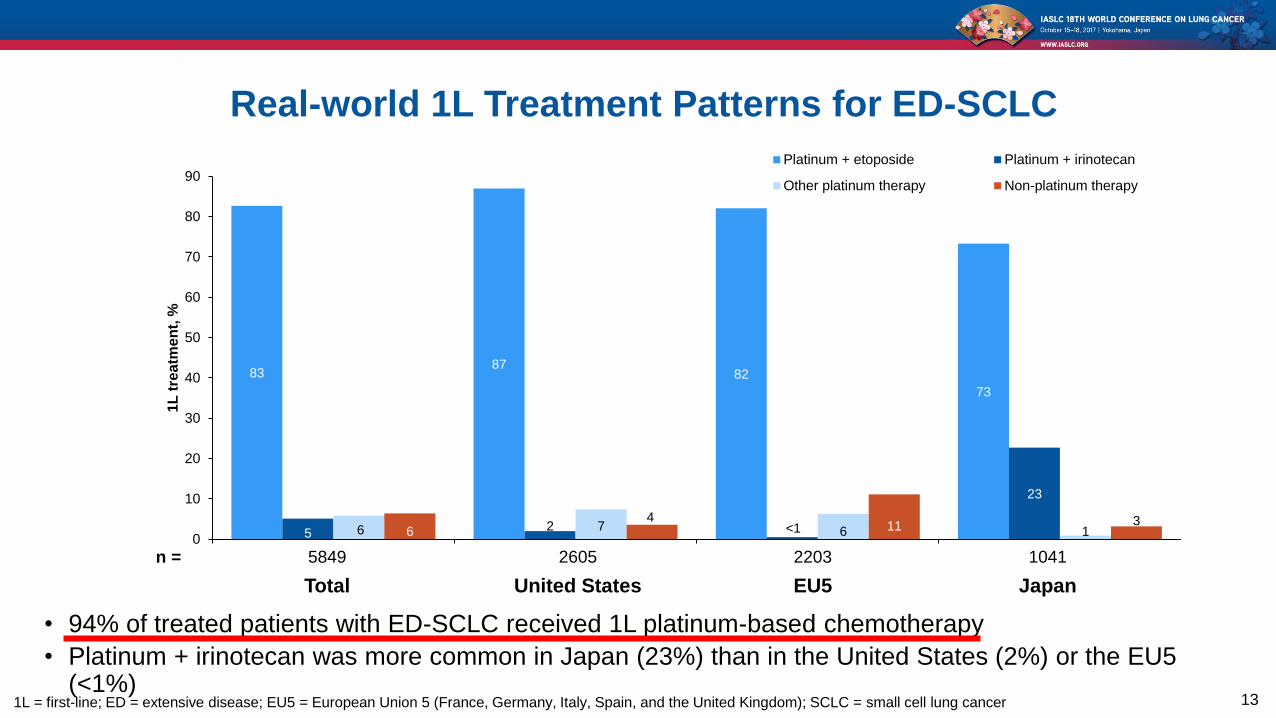
n = 5849 2605 2203 1041
Total United States EU5 Japan
Real-world 1L Treatment Patterns for ED-SCLC
1L = first-line; ED = extensive disease; EU5 = European Union 5 (France, Germany, Italy, Spain, and the United Kingdom); SCLC = small cell lung cancer
8387
82
73
52 <1
23
6 7 6 164
11 3
0
10
20
30
40
50
60
70
80
901
L t
rea
tme
nt,
%Platinum + etoposide Platinum + irinotecan
Other platinum therapy Non-platinum therapy
• 94% of treated patients with ED-SCLC received 1L platinum-based chemotherapy
• Platinum + irinotecan was more common in Japan (23%) than in the United States (2%) or the EU5 (<1%)

14
Real-world 2L Treatment Patterns for ED-SCLC
aTotals may not equal 100% due to rounding
2L = second-line; ED = extensive disease; EU5 = European Union 5 (France, Germany, Italy, Spain, and the United Kingdom); SCLC = small cell lung cancer
30
1930
20
59 60
42
48
60
56
5
2
8
6
6
4
5 1
11
10
1
2 15
8
817
4
18 16
30
0
10
20
30
40
50
60
70
80
90
100
2L
tre
atm
en
t, %
aPlatinum + etoposide
Platinum + irinotecan
Other platinum therapy
Topotecan
Other non-platinum therapy
n = 227 273 148 214 143 112
Platinum group Resistant Sensitive Resistant Sensitive Resistant Sensitive
United States EU5 Japan
• 19% of patients received 2L treatment (19% in the United States, 16% in the EU5, and 24% in Japan)
• Among platinum-resistant patients receiving a 2L treatment, 27% in the United States, 11% in the EU5, and
36% in Japan were administered platinum-based therapy
• Despite platinum sensitivity, the most common 2L treatment in the United States and EU5 was topotecan

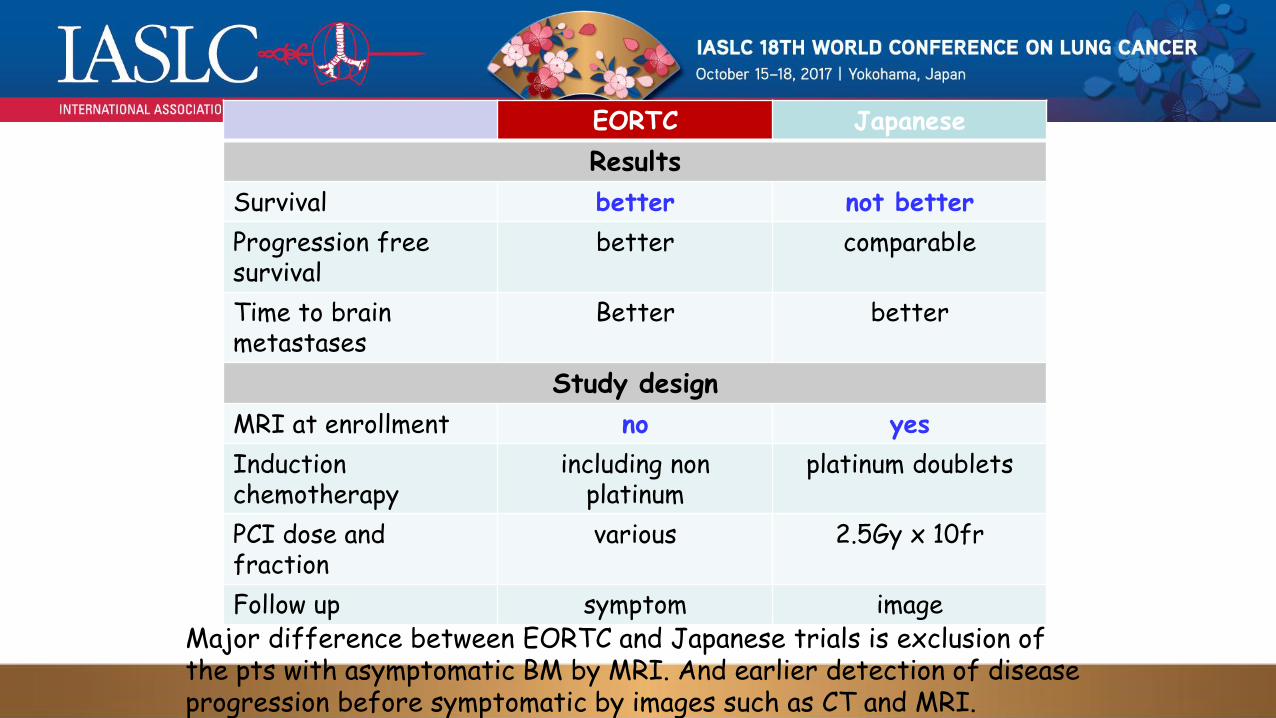
EORTC Japanese
Results
Survival better not better
Progression free survival
better comparable
Time to brain metastases
Better better
Study design
MRI at enrollment no yes
Induction chemotherapy
including non platinum
platinum doublets
PCI dose and fraction
various 2.5Gy x 10fr
Follow up symptom imageMajor difference between EORTC and Japanese trials is exclusion of the pts with asymptomatic BM by MRI. And earlier detection of disease progression before symptomatic by images such as CT and MRI.
TRT PRO
Alta incidência ED dx
Controle local melhora meta
dist
Aumento SV 2y 5.4%
local controle with 25.3%
TRT CON
CREST negativo para EP
p=0.066
Sec end positivo aos 2y
Highlights of the Day: Paul Baas, MD, PhD
Warde & Payne, J Clin Oncol 1992;10:890-895

Highlights of the Day: Paul Baas, MD, PhD
13 X
3%

Highlights of the Day: Paul Baas, MD, PhD
• TRT mais indicada em pacientes com massa
residual
• Pacientes > 2 sítios metástases – pior
Take home messages


Karve et al. BMC Health Services Research 2014, 14:555

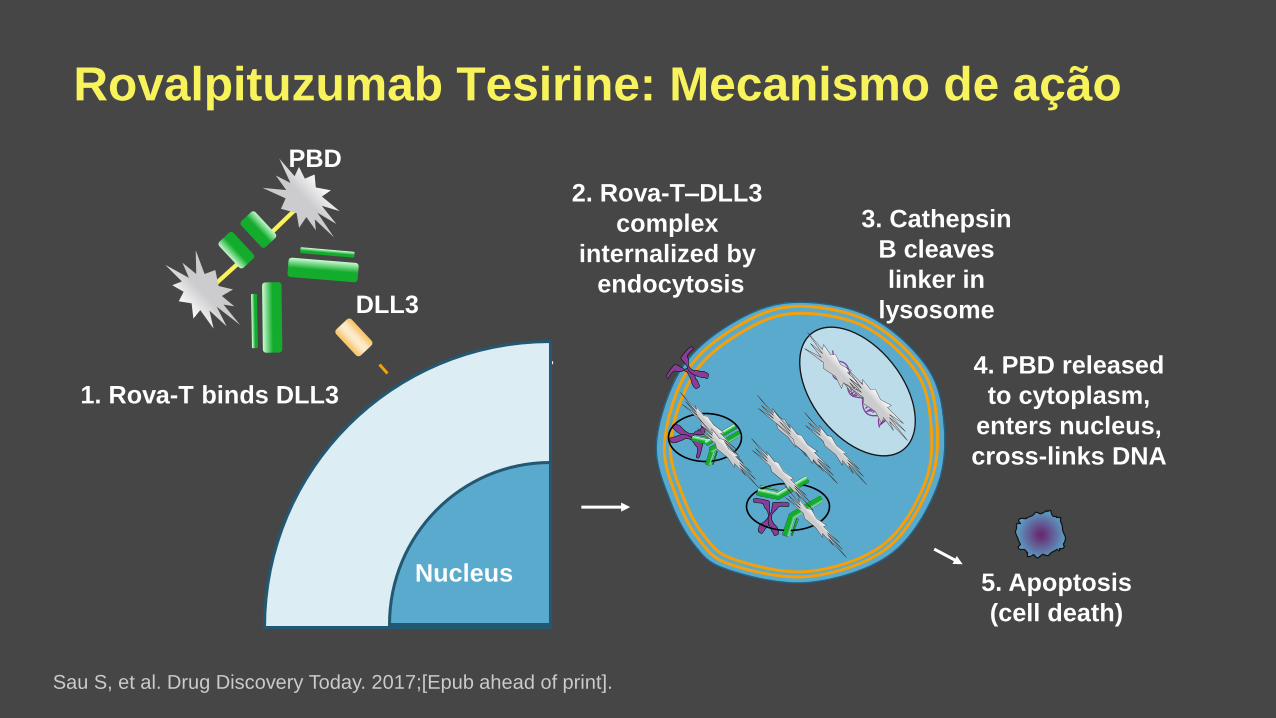
Rovalpituzumab Tesirine: Mecanismo de ação
Tumor
Cell
DLL3
PBD
Nucleu
s
1. Rova-T binds DLL3
2. Rova-T–DLL3
complex
internalized by
endocytosis
4. PBD released
to cytoplasm,
enters nucleus,
cross-links DNA
5. Apoptosis
(cell death)
Sau S, et al. Drug Discovery Today. 2017;[Epub ahead of print].
3. Cathepsin
B cleaves
linker in
lysosome
Nucleus


Lancet Oncol 2017; 18: 42–51c

Lancet Oncol 2017; 18: 42–51c

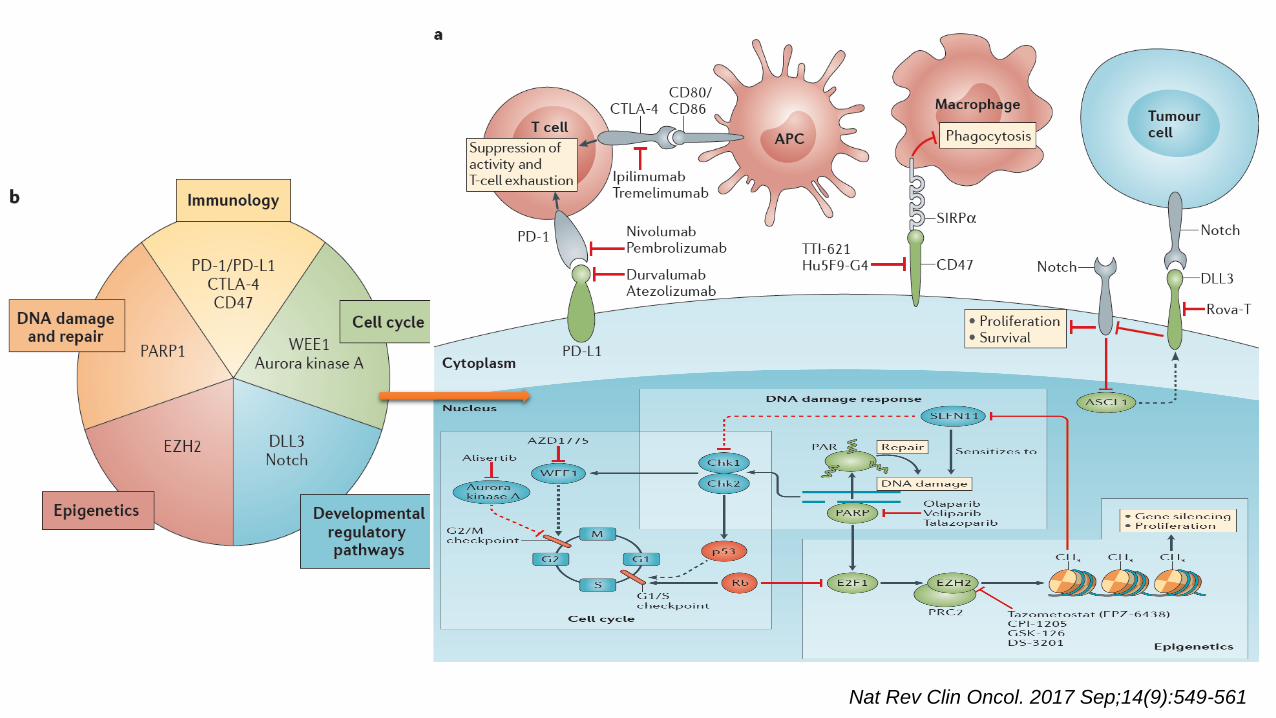
Nat Rev Clin Oncol. 2017 Sep;14(9):549-561

Owonikoko TK, et al. WCLC 2016. Abstract OA05.05

Owonikoko TK, et al. WCLC 2016. Abstract OA05.05

Owonikoko TK, et al. WCLC 2016. Abstract OA05.05

Slide 1
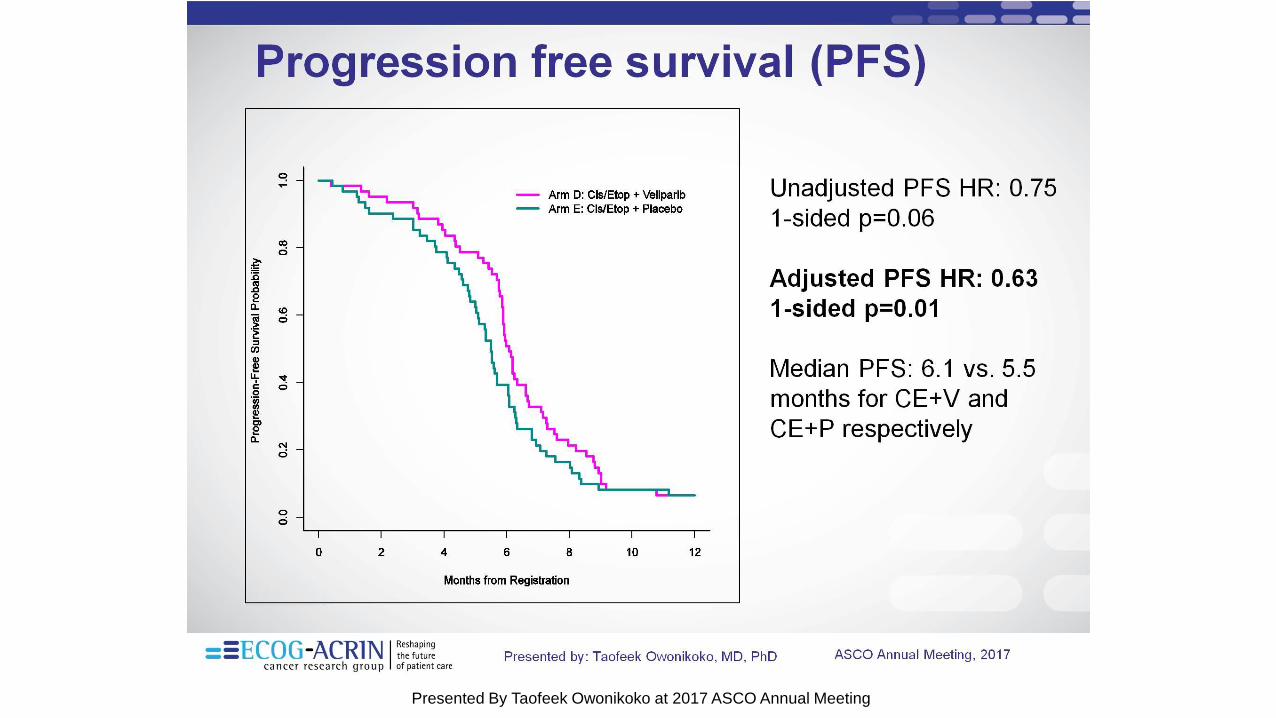
Presented By Taofeek Owonikoko at 2017 ASCO Annual Meeting

Slide 5
Presented By Taofeek Owonikoko at 2017 ASCO Annual Meeting
Slide 9
Presented By Taofeek Owonikoko at 2017 ASCO Annual Meeting

Slide 11
Presented By Taofeek Owonikoko at 2017 ASCO Annual Meeting
MA 01 - SCLC: Research Perspectives. Abstract #8480
Lanreotide Maintenance in SCLC Expressing Somatostatine Receptors: Efficacy Results of Multicenter Randomized G04.2011 Trial – Sara Pilotto
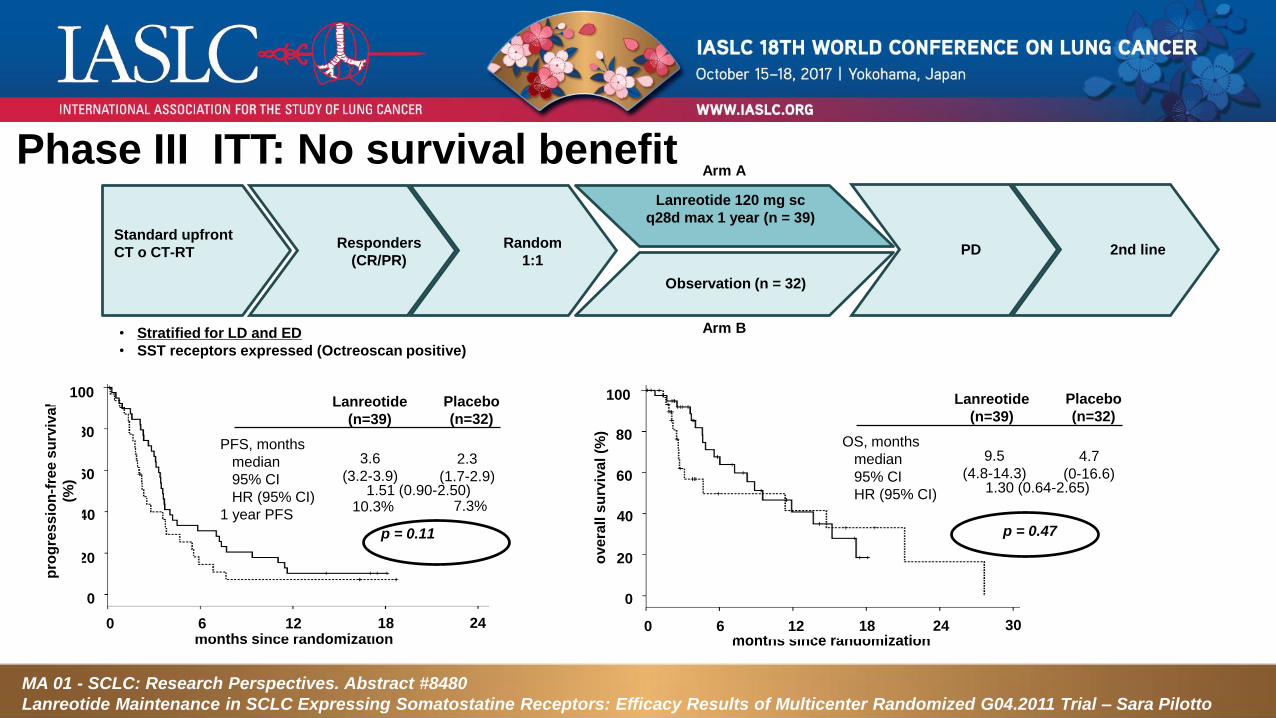
Phase III ITT: No survival benefit
Standard upfront
CT o CT-RT
• Stratified for LD and ED
• SST receptors expressed (Octreoscan positive)
Responders
(CR/PR)
Lanreotide 120 mg sc
q28d max 1 year (n = 39)
Observation (n = 32)
Arm A
Arm B
Random
1:1PD 2nd line
80
60
40
20
pro
gre
ss
ion
-fre
e s
urv
iva
l
(%)
0
0 24months since randomization
PFS, months
median
95% CI
HR (95% CI)
1 year PFS
Lanreotide
(n=39)
Placebo
(n=32)
3.6
(3.2-3.9)
2.3
(1.7-2.9)1.51 (0.90-2.50)
10.3% 7.3%
p = 0.11
80
60
40
20
0
0
ove
rall
su
rviv
al (%
)
30months since randomization
OS, months
median
95% CI
HR (95% CI)
Lanreotide
(n=39)
Placebo
(n=32)
9.5
(4.8-14.3)
4.7
(0-16.6)1.30 (0.64-2.65)
p = 0.47
66 12 18 12 18 24
100 100
months since randomization
pro
gre
ss
ion
-fre
e s
urv
iva
l (%
)
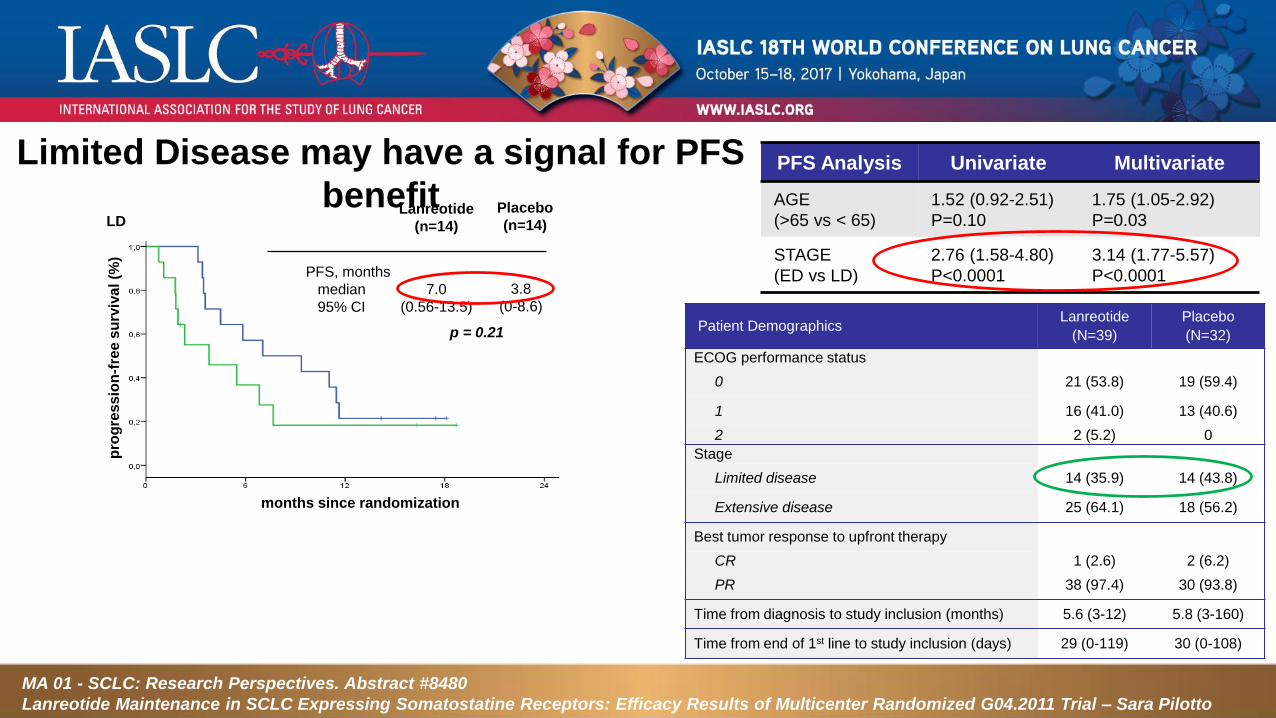
PFS, months
median
95% CI
Lanreotide
(n=14)
Placebo
(n=14)
7.0
(0.56-13.5)
3.8
(0-8.6)
p = 0.21
LD
PFS Analysis Univariate Multivariate
AGE
(>65 vs < 65)
1.52 (0.92-2.51)
P=0.10
1.75 (1.05-2.92)
P=0.03
STAGE
(ED vs LD)
2.76 (1.58-4.80)
P<0.0001
3.14 (1.77-5.57)
P<0.0001
Limited Disease may have a signal for PFS
benefit
Patient DemographicsLanreotide
(N=39)
Placebo
(N=32)
ECOG performance status
0 21 (53.8) 19 (59.4)
1 16 (41.0) 13 (40.6)
2 2 (5.2) 0
Stage
Limited disease 14 (35.9) 14 (43.8)
Extensive disease 25 (64.1) 18 (56.2)
Best tumor response to upfront therapy
CR 1 (2.6) 2 (6.2)
PR 38 (97.4) 30 (93.8)
Time from diagnosis to study inclusion (months) 5.6 (3-12) 5.8 (3-160)
Time from end of 1st line to study inclusion (days) 29 (0-119) 30 (0-108)
MA 01 - SCLC: Research Perspectives. Abstract #8480
Lanreotide Maintenance in SCLC Expressing Somatostatine Receptors: Efficacy Results of Multicenter Randomized G04.2011 Trial – Sara Pilotto


Tratada com Cisp e Etop x 4 + RT bid C#2 com excelente
RP
Recidiva em LN para esofágico e frênico em menos de 3
meses.....

22/11/17
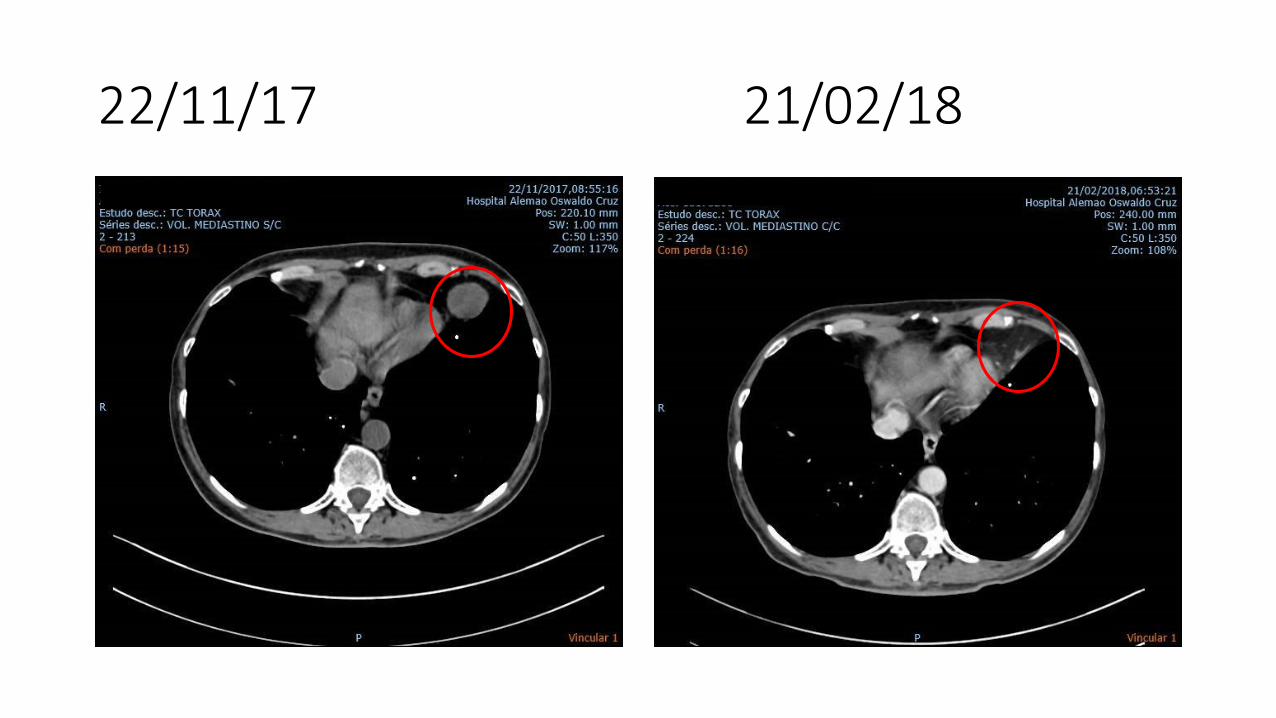
22/11/17 21/02/18
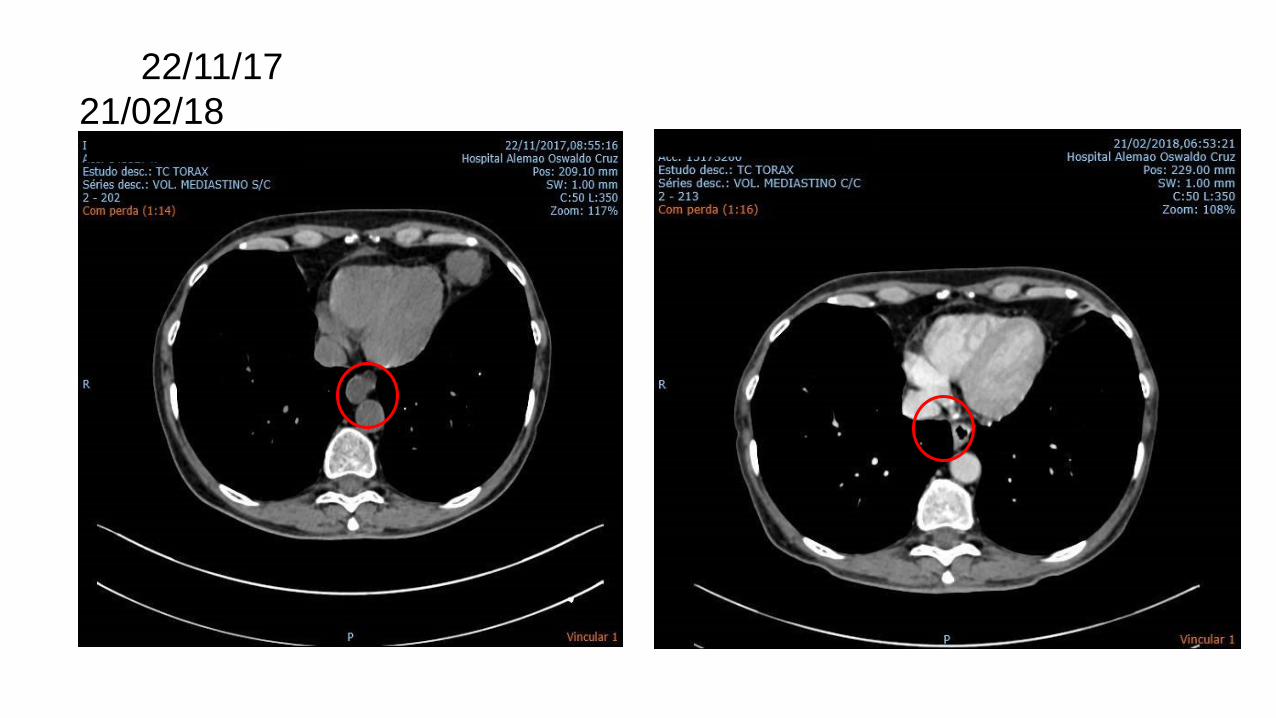
22/11/17
21/02/18


1000
100
10
1.0
0.1
0.001So
mati
c m
uta
tio
n p
revale
nce
(# m
uta
tio
ns/m
eg
ab
ase
)
0.01
1. Adapted by permission from Macmillan Publishers Ltd: Alexandrov LB, et al. Nature 2013;500:415-421, copyright 2013. 2. Morabito A, et al. Crit Rev Oncol Hematol 2014;91:257–
270. 3. Carbone DP et al. N Engl J Med. 2017;376:2415–2426. 4. Snyder A, et al. N Engl J Med 2014;371:2189–2199. 5 Galsky MD, et al. Poster Discussion at ESMO 2017. 848PD.
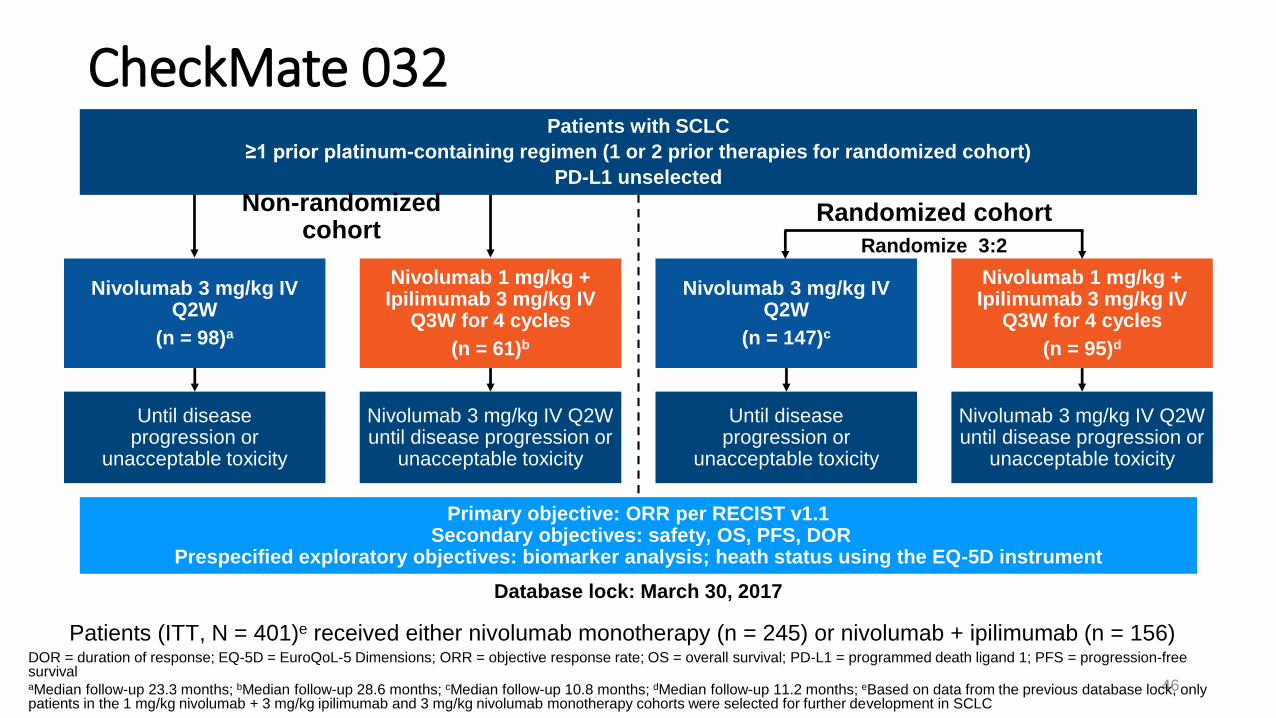
CheckMate 032
46
DOR = duration of response; EQ-5D = EuroQoL-5 Dimensions; ORR = objective response rate; OS = overall survival; PD-L1 = programmed death ligand 1; PFS = progression-free survivalaMedian follow-up 23.3 months; bMedian follow-up 28.6 months; cMedian follow-up 10.8 months; dMedian follow-up 11.2 months; eBased on data from the previous database lock, only patients in the 1 mg/kg nivolumab + 3 mg/kg ipilimumab and 3 mg/kg nivolumab monotherapy cohorts were selected for further development in SCLC
Randomized cohort
Primary objective: ORR per RECIST v1.1Secondary objectives: safety, OS, PFS, DOR
Prespecified exploratory objectives: biomarker analysis; heath status using the EQ-5D instrument
Randomize 3:2
Database lock: March 30, 2017
Nivolumab 3 mg/kg IV Q2W
(n = 98)a
Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg IV
Q3W for 4 cycles
(n = 61)b
Nivolumab 3 mg/kg IV Q2W
(n = 147)c
Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg IV
Q3W for 4 cycles
(n = 95)d
Until disease progression or
unacceptable toxicity
Nivolumab 3 mg/kg IV Q2W until disease progression or
unacceptable toxicity
Until disease progression or
unacceptable toxicity
Nivolumab 3 mg/kg IV Q2W until disease progression or
unacceptable toxicity
Patients with SCLC
≥1 prior platinum-containing regimen (1 or 2 prior therapies for randomized cohort)
PD-L1 unselected
Non-randomized cohort
Patients (ITT, N = 401)e received either nivolumab monotherapy (n = 245) or nivolumab + ipilimumab (n = 156)


Matthew D , et al. ASCO 2017 Abstract 8503

Matthew D , et al. ASCO 2017 Abstract 8503

aFor germline sequencing; bDNA was sequenced on the Illumina HiSeq 2500 using 2 × 100-bp paired-end reads
ITT population
(N = 401)
Patients with paired tumor and whole blood samplesa
(n = 246; 61%)
TMB-evaluable patients
(n = 211; 53%) [86% of patients with paired samples]
Nivolumab
(n = 133; 54.3%)
Nivolumab + ipilimumab
(n = 78; 50.0%)
Nivolumab
(n = 245)
Nivolumab + ipilimumab
(n = 156)
• TMB was determined by whole exome sequencingb and calculated as the total number of
missense mutations in the tumor
• For exploratory analyses, patients were divided into 3 subgroups based on TMB tertile
TMB

ORR by TMBCheckMate 032 Exploratory TMB Analysis
11,3
4,86,8
21,3
28,2
22,2
16,0
46,2
0
10
20
30
40
50
TMB-evaluable Low TMB Medium TMB High TMB
OR
R, %
Nivolumab Nivolumab + ipilimumab
42 27 44 25 47 26n 133 78

PFS - TMB
52
44 5 1 1 1 0 0 0 5 2 2 2 2 1 1 0 0 0
47 15 12 8 5 5 5 2 15 10 5 4 4 3 2 1 0 0
42 3 2 1 0 0 0 0 6 2 1 0 0 0 0 0 0 0No. at risk
1-y PFS = 21.2%1-y PFS =
30.0%
1-y PFS = NC
1-y PFS =
3.1%
1-y PFS = 8.0%1-y PFS = 6.2%
Median (95% CI) PFS, overall TMB-evaluable population: 1.4 (1.3, 1.4) months for nivolumab and 1.7 (1.4, 2.7) months for nivolumab + ipilimumab
NC = not calculable
Medium
High
Low
Months
100
75
50
25
0
0 3 6 9 12 15 18 21 24 27 30 33 36
PF
S, %
100
75
50
25
0
0 3 6 9 12 15 18 21 24 27 30 33 36
Months
Low TMB Med TMB High TMB
Median PFS
(95% CI), mo
1.3
(1.2, 1.4)
1.3
(1.2, 1.4)
1.4
(1.3, 2.7)
Low TMB Med TMB High TMB
Median PFS
(95% CI), mo
1.5
(1.3, 2.7)
1.3
(1.2, 2.1)
7.8
(1.8, 10.7)
Nivolumab Nivolumab + ipilimumab
25 0
26 0
27 0
0 0 0 0 0
2 2 2 2 1
0 0 0 0 0
3
12
5
100
75
50
25
0
0 3 6 9 12 15 18 21 24 27 30 33 36
1-y OS = 62.4%
1-y OS = 19.6%1-y OS = 23.4%
Months
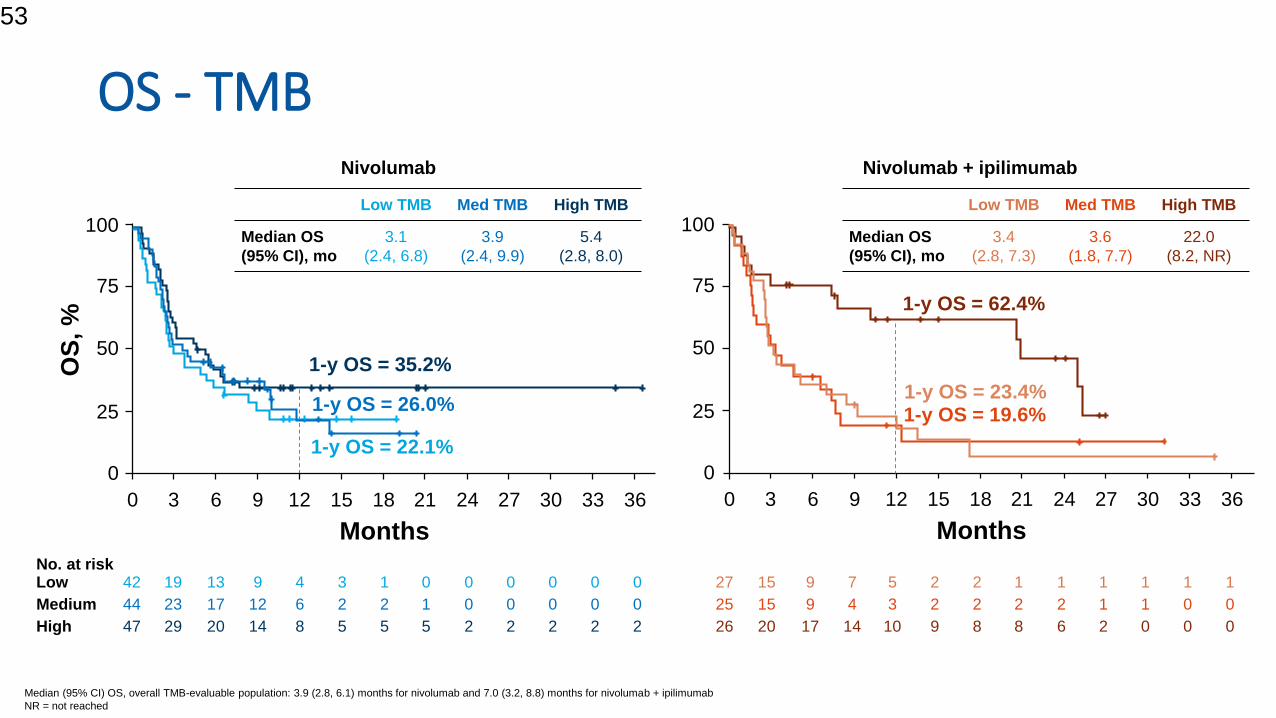
OS - TMB
53
44 23 17 12 6 2 2 1 0 0 0 0 0 25 15 9 4 3 2 2 2 2 1 1 0 0
47 29 20 14 8 5 5 5 2 2 2 2 2 26 20 17 14 10 9 8 8 6 2 0 0 0
42 19 13 9 4 3 1 0 0 0 0 0 0 27 15 9 7 5 2 2 1 1 1 1 1 1
Months
100
75
50
25
0
0 3 6 9 12 15 18 21 24 27 30 33 36
OS
, %
1-y OS = 35.2%
1-y OS = 22.1%
1-y OS = 26.0%
Low TMB Med TMB High TMB
Median OS
(95% CI), mo
3.1
(2.4, 6.8)
3.9
(2.4, 9.9)
5.4
(2.8, 8.0)
Low TMB Med TMB High TMB
Median OS
(95% CI), mo
3.4
(2.8, 7.3)
3.6
(1.8, 7.7)
22.0
(8.2, NR)
Nivolumab Nivolumab + ipilimumab
Median (95% CI) OS, overall TMB-evaluable population: 3.9 (2.8, 6.1) months for nivolumab and 7.0 (3.2, 8.8) months for nivolumab + ipilimumab
NR = not reached
No. at risk
Medium
High
Low

KEYNOTE-028: SCLC Cohort
ASCO 2015 Abstract 7502; ESMO 2017, Abstract 427O; 2016WCLC, OA05.01
-1 0 0
-8 0
-6 0
-4 0
-2 0
0
2 0
4 0
6 0
8 0
1 0 0
Ch
an
ge
Fro
m B
as
eli
ne
in
Su
m o
f
Lo
ng
es
t D
iam
ete
r o
f T
arg
et
Le
sio
n,
%
S D
P R
P D
C R
Change From Baseline in Tumor Size (RECIST v1.1,
investigator review)
Primary endpoint
Updated ORR: 33.3%
(95% CI, 15.6%-55.3%)
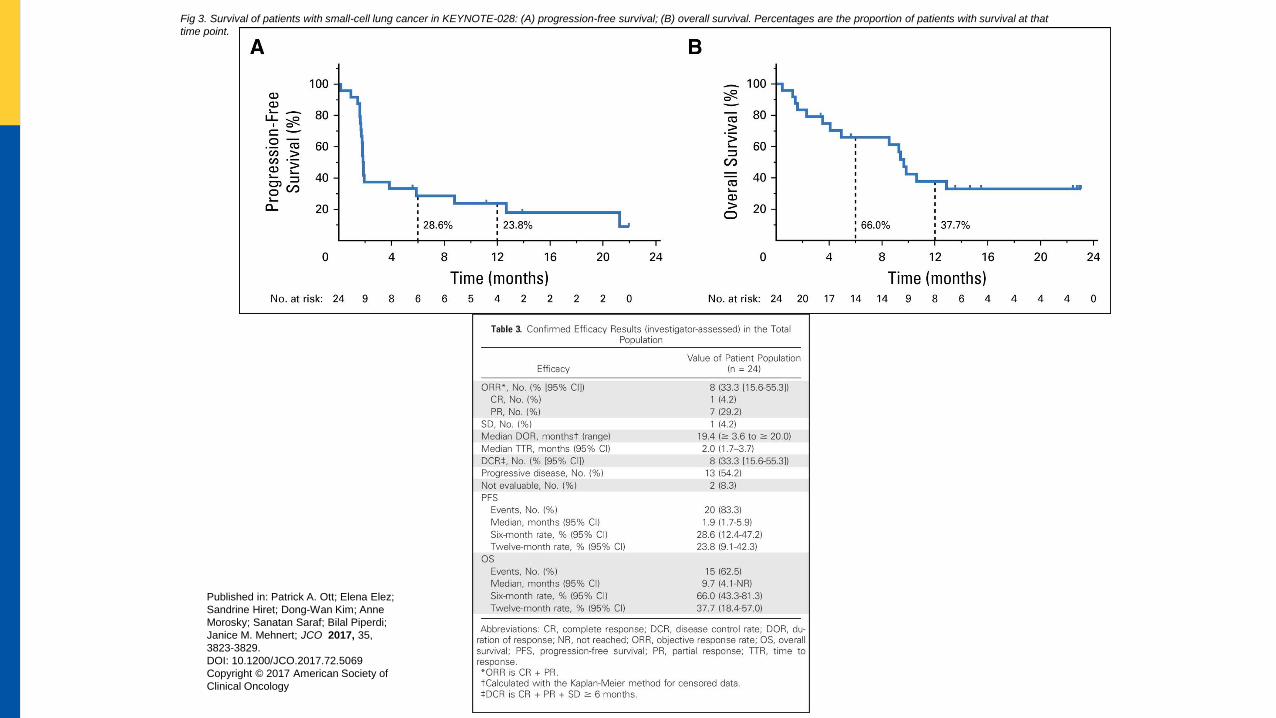
Fig 3. Survival of patients with small-cell lung cancer in KEYNOTE-028: (A) progression-free survival; (B) overall survival. Percentages are the proportion of patients with survival at that
time point.
Published in: Patrick A. Ott; Elena Elez;
Sandrine Hiret; Dong-Wan Kim; Anne
Morosky; Sanatan Saraf; Bilal Piperdi;
Janice M. Mehnert; JCO 2017, 35,
3823-3829.
DOI: 10.1200/JCO.2017.72.5069
Copyright © 2017 American Society of
Clinical Oncology


Agents Phase NCT Target Population Planned NPrimary
endpoint
REACTION: Cis-etop +/- pembrolizumab
EORTCII 02580994 PD-1 + chemo
Frontline ES-
SCLC118 PFS
KEYNOTE 011 SCLC cohort
Pembrolizumab +/- platinum-etoposideI 01840579 PD-1 +/- chemo
Frontline ES-
SCLC75 Safety (DLT)
Pembrolizumab after chemo II 02359019Chemo then maintenance
PD-1 inhibitor
Maintenance ES-
SCLC54 PFS
Pembrolizumab+chemo +/- XRT II 02934503 PD-1 + chemo +/- XRT ES-SCLC 60Change n PD-L1
IHC status
KEYNOTE 158 SCLC cohort
pembrolizumabII 02628067 PD-1 ES-SCLC 1100 ORR
Pembrolizumab vs topotecan
AllianceII 02963090 PD-L1 vs chemo Salvage ES-SCC 98 PFS
Pembrolizumab + chemoXRT I 02402920 PD-1+ chemoXRTES-SCLC and
LS-SCLC80 Safety (MTD)
Carbo-etoposide +/- atezolizumab I/II 02748889 Chemo +/- PD-L1Frontline ES-
SCLC178 Toxicity
Carbo-etoposide +/- atezolizumab
IMpower133I/III 02763579 Chemo +/- PD-L1
Frontline ES-
SCLC400
Duration OS,
PFS
Atezolizumab vs topotecan II 03059667 PD-L1 vs chemoSalvage ES-
SCLC 70 ORR
Selected SCLC Immunotherapy trials
Clinical trials.gov

Agents Phase NCT Target Population Planned NPrimary
endpoint
CASPIAN: chemo vs chemo+durvalumab
vs chemo + Durvalumab + tremelimumabIII 03043872
Chemo vs Chemo +PD-L1
vs Chemo + PD-L1 +
CTLA4
Frontline ES-
SCLC795 OS, PFS
Durv + treme +/- XRT II 02701400 PD-L1 vs chemo Salvage ES-SCC 20 PFS, ORR
Durvalumab + tremelimumab vs AZD1775 +
carboII 02937818 PD-L1 + CTLA4 vs
Refractory ES-
SCLC80 ORR
Olaparib + durva I/II 02734004 PD-L1 SCLC cohort 133 Safety
CHECKMATE 451 chemo followed by nivo,
ipi-nivo, or placebo maintenanceIII 02538666
PD-1 vs PD-1+CTLA4 vs
placebo maintenance
Maintenance
ES-SCLC 810 OS, PFS
CHECKMATE 331
Nivo vs topotecan vs amrubicinIII 02481830 PD-1 vs chemo
Salvage ES-
SCLC558 OS
Chemo followed by ipi-nivo + XRT I/II 03043599 PD-1 + CTLA4 ES-SCLC 52 OS
STIMULI: Ipi-nivo after chemoXRT
ETOPII 02046733
PD-1+CTLA4 after
chemoXRT
Consolidation
LS-SCLC260 OS, PFS
Selected SCLC Immunotherapy trials (con’t)
Clinical trials.gov

Selected Other AgentsAntibody-Drug Conjugates
Rovalpituzumab Tesirine (Rova-T)
Sacituzumab Govitecan (IMMU-132)
PARP inhibitors
Veliparib
Talazoparib
Wee-1 inhibitors
AZD1775
Apoptotic Agents
ABT-263 +/- mTOR AZD8055
Epi-immune agents
RRx-001
Aurora kinase inhibitors
Alisertib
AZD1152
Notch inhibitors
MEDI0639 (DLL4)
OMP-59R5
Demcizumab
FGFR inhibitors
Ponatinib
Lucitanib
PIK3CA inhibitors
VS5584
Transcription Targeting
Ruzolitinib
Tofactinib
AZD1480
Cytotoxic Agents
amrubicin
palifosfamide
aldoxorubicin

CARLOS HENRIQUE TEIXEIRA
HAOC – CPO/ONCOCLÍNICAS
OBRIGADO!!