Universidade Federal do Rio de Janeiro – UFRJ Centro de Ciências da Saúde
Faculdade de Odontologia
Departamento de Odontopediatria e Ortodontia
Rio de Janeiro 2015
AÇÃO DE COMPOSTOS A BASE DE CÁLCIO E
XILITOL NA PREVENÇÃO DA EROSÃO E DA EROSÀO
ASSOCIADA À ABRASÃO
Adílis Kalina Alexandria de França

Universidade Federal do Rio de Janeiro – UFRJ Centro de Ciências da Saúde
Faculdade de Odontologia
Departamento de Odontopediatria e Ortodontia
Rio de Janeiro 2015
AÇÃO DE COMPOSTOS A BASE DE CÁLCIO E XILITOL NA
PREVENÇÃO DA EROSÃO E DA EROSÀO ASSOCIADA À
ABRASÃO
Adílis Kalina Alexandria de França
Tese de Doutorado apresentada ao Programa de Pós-
Graduação em Odontologia (Área de Concentração
Odontopediatria), Faculdade de Odontologia, Universidade
Federal do Rio de Janeiro, como parte dos requisitos
necessários à obtenção do título de Doutor em Odontologia
(Odontopediatria).
Orientadores:
Prof. Drª. Lucianne Cople Maia de Faria
Prof. Dr. Lúcio Mendes Cabral
Prof. Drª. Ana Maria Gondim Valença

F IC H A C AT ALO G R Á F IC A

F O LH A D E AP R O V AÇ Ã O
ADÍL IS KAL INA AL EXANDRIA DE F RANÇA
“AÇÃO DE COMPOSTOS A BASE DE CÁLCIO E XILITOL NA
PREVENÇÃO DA EROSÃO E DA EROSÀO ASSOCIADA À ABRASÃO”
Tese de Doutorado submetida ao Programa de Pós-Graduação em Odontologia
(Odontopediatria), Faculdade de Odontologia, Universidade Federal do Rio de
Janeiro - UFRJ, como parte dos requisitos necessários à obtenção do título de
Doutor em Odontologia (Odontopediatria).
Rio de Janeiro, 17 de Setembro de 2015.
____________________________________________________________
Prof. Drª. Lucianne Cople Maia de Faria
Profª. Titular do Dept0 de Odontopediatria e Ortodontia FO-UFRJ
____________________________________________________________
Prof. Drª. Aline de Almeida Neves
Profª. Adjunto do Dept0 de Odontopediatria e Ortodontia FO-UFRJ
____________________________________________________________
Prof. Drª. Glória Fernanda Castro
Profa. Adjunto do Dept0 de Odontopediatria e Ortodontia FO-UFRJ
____________________________________________________________
Prof. Drª. Tatiana Kelly da Silva Fidalgo
Prof. do Dept0 de Odontologia da FO-UNIVERSO
_________________________________________________________
Prof. Dr Matheus Melo Pithon
Prof. Adjunto do Dept0 de Odontopediatria da UESB

DEDICATÓRIA
Dedico este trabalho a minha tia/mãe Leticia Ramos de Alexandria, que
sempre deu o seu melhor por todos e que me mostrou em vida o significado de
altruísmo. Ela sempre foi minha maior incentivadora. Sempre me senti amada,
sempre senti abrigo em seus braços, sempre presente em minha vida, indo muitas
vezes além das suas próprias forças, pensando no melhor para mim. Infelizmente
coube a Deus acolhê-la em Seus braços e a saudade é tão grande que muitas
vezes não cabe no peito. Hoje não tenho como demonstrar toda minha gratidão,
desejaria que pudesse estar comigo agora, para juntas comemorarmos essa vitória
que foi tão almejada por nós no passado. Amo você demais “tia Leta”.

AGRADECIMENTOS
Agradeço a Deus pelo dom da vida, graças às Suas bênçãos diárias e Sua
infinita misericórdia que posso hoje comemorar a finalização de mais uma etapa
em minha vida.
Ao meu esposo Tiago Cruz de França, eu agradeço pelo companheirismo,
atenção, e incentivo durante esses seis anos de nossas vidas no Rio de Janeiro.
Você foi à pessoa que o nosso SENHOR usou para me orientar quando, muitas
vezes cansada, eu não sabia que decisões tomar.
Agradeço aos meus familiares, meu pai Carlos Alberto Henrique, minha mãe
Rejane de Alexandria Henrique e as minhas irmãs Isla Kaliane Henrique e Maria
Julia Henrique por compreenderem e apoiarem minha decisão de me ausentar de
casa para estudar longe, a saudade foi um fardo diário, mas o amor e incentivo da
família era um consolo para os dias de tristeza. Agradeço a minha sogra Claudete
Cruz Felício e meu sogro Manoel Felício por suas orações e cuidados.
À professora Lucianne Cople Maia, agradeço por acreditar em mim e sempre
me estimular a ser uma boa profissional. Te admiro pela sua incansável dedicação.
És exemplo de profissional séria e competente.
Ao professor Lúcio Mendes Cabral, agradeço pelo norteamento durante as
etapas de elaboração dos produtos da pesquisa. Obrigada pela atenção em cada
etapa do nosso trabalho.
À professora Ana Maria Gondim Valença, agradeço pelos ensinamentos,
paciência e disponibilidade desde a época da graduação. Você sempre uma grande
incentivadora. E hoje posso dividir com você os frutos dessa caminhada.
Agradeço à professora Andréa Gonçalves Antonio, exemplo de seriedade,
dedicação e competência. Agradeço pela crescente amizade, pelos ensinamentos
no laboratório e também na vida, pela paciência e incentivo. Foi um privilégio
trabalhar com você, que existam mais pessoa como você em minha vida.
Agradeço aos professores Ivete Pomarico, Laura Salignac, Aline Neves,
Glória Fernanda Castro, Marcelo Costa, Rogério Gleizer e Luciana Pomarico
pelo conhecimento adquirido e por compartilharem comigo suas experiências.
Aos amigos, Thiago Isidro Vieira, Adrielle Santos, Tatiana Fidalgo e
Matheus Pithon, amigos queridos, foi um privilégio conviver com vocês, obrigada
pelo companheirismo e auxílio no laboratório.
Aos amigos Jaqueline Villaça, Erika Suzuki, Lilian Amaral e a professora
Flávia Almada da Faculdade de Farmácia da UFRJ que me auxiliaram durante o
período em que utilizei o laboratório. Agradeço a disposição em me ajudar.
Aos professores Aline Soares Freire e Ricardo Erthal Santelli do laboratório
de desenvolvimento analítico, do departamento de Química analítica do Instituto de
Química da UFRJ que me auxiliaram nas análises de cálcio dos nanocompostos.
Agradeço ainda, a professora Maria Teresa Villela Romanos do Laboratório de
Virologia do Instituto de Microbiologia Paulo de Góes da UFRJ. Obrigada pela
receptividade e disposição para realização dos testes.
Agradeço a amiga Claudia Tavares, pelas palavras carinhosas,
companheirismo. Você sempre esteve disposta a me ajudar com um sorriso no
rosto, e muitas ideias. Deixo registrado a minha admiração.
Agradeço aos alunos Nicolli Meckelburg, Ursula Puetter, Jordan Salles,
Amanda Mayworm, Rafael Marambaia, João Victor Frazão e Patrícia
Nadelman, foi uma experiência engrandecedora trabalhar com vocês.
A todos os amigos da minha turma de doutorado Andrea Pintor, Michelle
Ammari, Michele Lenzi e Marcello Roter, que tornaram os momentos em grupos
tão animados.
Aos amigos Lucia, Sophia e Isabelle Medeiros, Rose, Eduardo, Gabriella
e Arthur Taborda, minha família carioca. Agradeço por terem me acolhido tão bem,
vocês realmente moram em meu coração.
À CAPES, pela bolsa de doutorado concedida, e que possibilitou o
desenvolvimento dessa pesquisa e a Faperj e CNPq pelo apoio financeiro.

Por isso não desfalecemos; mas, ainda que o
nosso homem exterior se corrompa, o interior,
contudo, se renova de dia em dia. Porque a nossa
leve e momentânea tribulação produz para nós um
peso eterno de glória mui excelente. Não atentando
nós nas coisas que se vêem, mas nas que se não
vêem; porque as que se vêem são temporais, e as
que se não vêem são eternas.
2 Coríntios 4:16-18
RESUMO
ALEXANDRIA, Adílis Kalina. Ação de compostos a base de cálcio e xilitol na prevenção da erosão e da erosào associada à abrasão. Rio de Janeiro, 2015. Tese (Doutorado em Odontologia, área de concentração em Odontopediatria) – Faculdade de Odontologia, Universidade Federal do Rio de Janeiro, Rio de Janeiro, 2015.
Os compostos fluoretados têm grande importância como agentes preventivos e terapêuticos diante de desafios erosivos e abrasivos. Vários produtos fluoretados de tem sido extensivamente estudados devido a sua ação em prevenir, tratar ou diminuir a progressão da desmineralização dentária. Novos compostos têm sido propostos, em associação ou não ao fluoreto, como uma tentativa em se obter melhores efeitos contra a perda mineral. Na presente tese foi avaliado o efeito de compostos a base de cálcio e xilitol na prevenção da erosão e da erosão associada à abrasão. Vernizes de fluoreto de sódio (NaF) associados ou não ao fosfocaseínato de cálcio (CPP-ACP) e xilitol foram testados. A erosão foi executada por meio da imersão da amostra em refrigerantes ou medicamentos líquidos pediátricos. Para a erosão associada à abrasão, ciclos de escovações também foram aplicados aos blocos erodidos. Em todos os experimentos, a superfície do esmalte foi avaliada por meio do perfilometro 3D de não contato (3D-NCP) nos parâmetros de perda de estrutura dentária e de rugosidade superficial. Imagens foram obtidas no 3D-NCP e em microscópio eletrônico de varredura (MEV). Diferenças entre os tratamentos foram testadas usando estatística inferencial, adotando-se o nível de significância de 5%. As imagens de 3D-NCP e MEV foram avaliadas descritivamente. Os vernizes fluoretados com CPP-ACP e xilitol exibiram efeito preventivo em relação à erosão e à progressão da erosão dentária; além de inibir à erosão associada à abrasão. O verniz de CPP-ACP demonstrou efeito preventivo frente à erosão promovida pelo refrigerante associado a um medicamento líquido pediátrico.

ABSTRACT
ALEXANDRIA, Adílis Kalina. Action of calcium and xylitol composites on preventing of erosion and erosion with abrasion. Rio de Janeiro, 2015. Tese (Doutorado em Odontologia, área de concentração em Odontopediatria) – Faculdade de Odontologia, Universidade Federal do Rio de Janeiro, Rio de Janeiro, 2015. Fluoride compounds are very important as preventive and therapeutic agents in erosive and abrasive challenges. Various fluoride products has been extensively studied because of their action to prevent, treat or slow down the progression of tooth demineralization. Novel compounds have been proposed, in combination or not with fluoride products to obtain better effects against mineral loss. In this thesis was evaluated the effect of NaF varnishes with calcium and xylitol in the prevention of erosion and erosion associated with abrasion. Sodium fluoride varnishes (NaF) associated or not with casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) and xylitol were tested. For erosion experiments, cycles of erosion (immersion in soft drink or in pediatric liquid medications) were made. To erosion associated with abrasion, brushing cycles were also applied to the eroded blocks. In all experiments, the enamel surface was evaluated by profilometry by non-contact 3D (3D-PNC) in following parameters: tooth structure loss and surface roughness. Images were obtained on 3D-PNC and scanning electron microscope (SEM). Differences between treatments were tested using inferencial statistical analysis with 5% os signifficance. 3D-PNC and SEM images were descriptively evaluated. CPP-ACP/NaF and xylitol/NaF varnishes exhibited a preventive effect against erosion and erosion associated with abrasion. The CPP-ACP/NaF varnish showed preventive effect against soft drink plus pediatric liquid medicine erosion.

RESUMEN
ALEXANDRIA, Adílis Kalina. Acción de compuestos de calcio e xilitol en prevención de la erosión e de la erosión asociada a la abrasión. Rio de Janeiro, 2015. Tese (Doutorado em Odontologia, área de concentração em Odontopediatria) – Faculdade de Odontologia, Universidade Federal do Rio de Janeiro, Rio de Janeiro, 2015. Compuestos de flúor son de gran importancia como agentes preventivos y
terapéuticos en desafíos erosivos y abrasivos. Varios productos de fluoruro ha sido
ampliamente estudiado debido a su acción para prevenir, tratar o retrasar la
progresión de la desmineralización de los dientes. Se han propuesto nuevos
compuestos, en combinación o no con fluoruro, en un intento de obtener mejores
efectos contra la pérdida de mineral. Objetivo de la tesis era evaluar el efecto de
los compuestos sobre la base de calcio y xilitol en la prevención de la erosión y la
erosión asociada a la abrasión. Barnices de fluoruro de sodio (NaF) asociados o no
con fosfocaseínato calcio (CPP-ACP) y xilitol se pusieron a prueba. La erosión se
llevó a cabo mediante la inmersión de la muestra en refrigerantes y medicamentos
líquidos de los niños. Para la erosión asociada a la abrasión, los ciclos de cepillado
se aplicaron a los bloques erosionados. En todos los experimentos, la superficie del
esmalte se evaluó mediante perfilometría por 3D sin contacto en los parámetros de
la pérdida de estructura dental y rugosidad de la superficie. Las imágenes se
obtuvieron en perfilometría 3D sin contacto y microscopio electrónico de barrido
(MEB). Las diferencias entre tratamientos se ensayaron usando análisis
estadísticos inferenciales com nível de significacion de 5%, la perfilometría 3D sin
contacto MEB imágenes se evaluaron descriptivamente. Barnices a fluoruro de
CPP-ACP y xilitol exhibieron un efecto preventivo contra la erosión y la progresión
de la erosión dental; además de inhibir la erosión asociada a la abrasión. El barniz
de CPP-ACP mostró efecto preventivo en contra de la erosión de refrigerante
asociado con medicamento líquido pediátrico.
LISTA DE TABELAS
Artigo 1
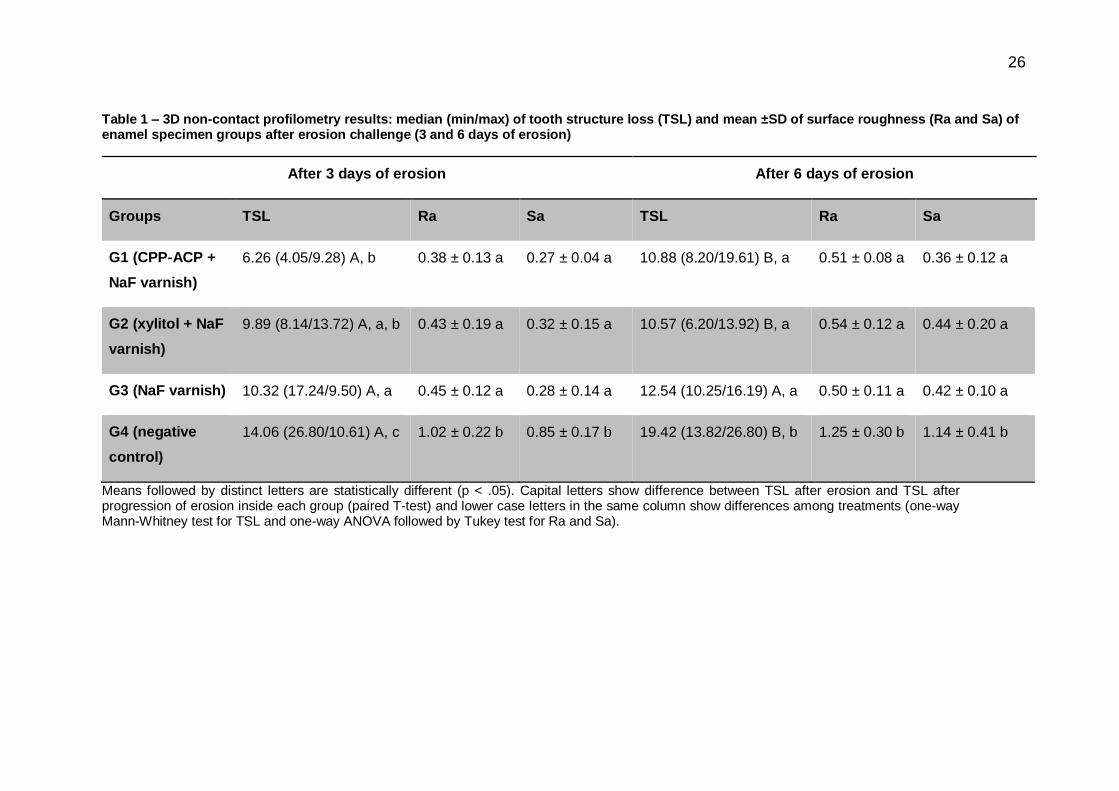
Table 1 – 3D non-contact profilometry results: median (min/max) of tooth structure
loss (TSL) and mean ±SD of surface roughness (Ra and Sa) of enamel specimen
groups after erosion challenge (3 and 6 days of erosion) ..................................... 26
Artigo 2
Table 1 - Mean of surface roughness (Ra and Sa) and tooth structure loss (TSL)
(±SD) of enamel specimen groups ....................................................................... 46
Artigo 3
Table 1 - Parameters of the pediatric medicines and control................................ 65
Table 2 – Median (minimum/maximum value - μm) surface roughness (Ra and Sa)
and Gap mean (μm) ± standard deviation between unexposed and exposed enamel
surfaces ................................................................................................................ 66
Artigo 4
Table 1 - Mean of tooth structure loss (TSL) and surface roughness (Sa) (±SD) of
enamel specimen groups after erosion challenges .............................................. 81

LISTA DE FIGURAS
Artigo 1
Figure 1. Schematic design of the experimental protocol. .................................... 27
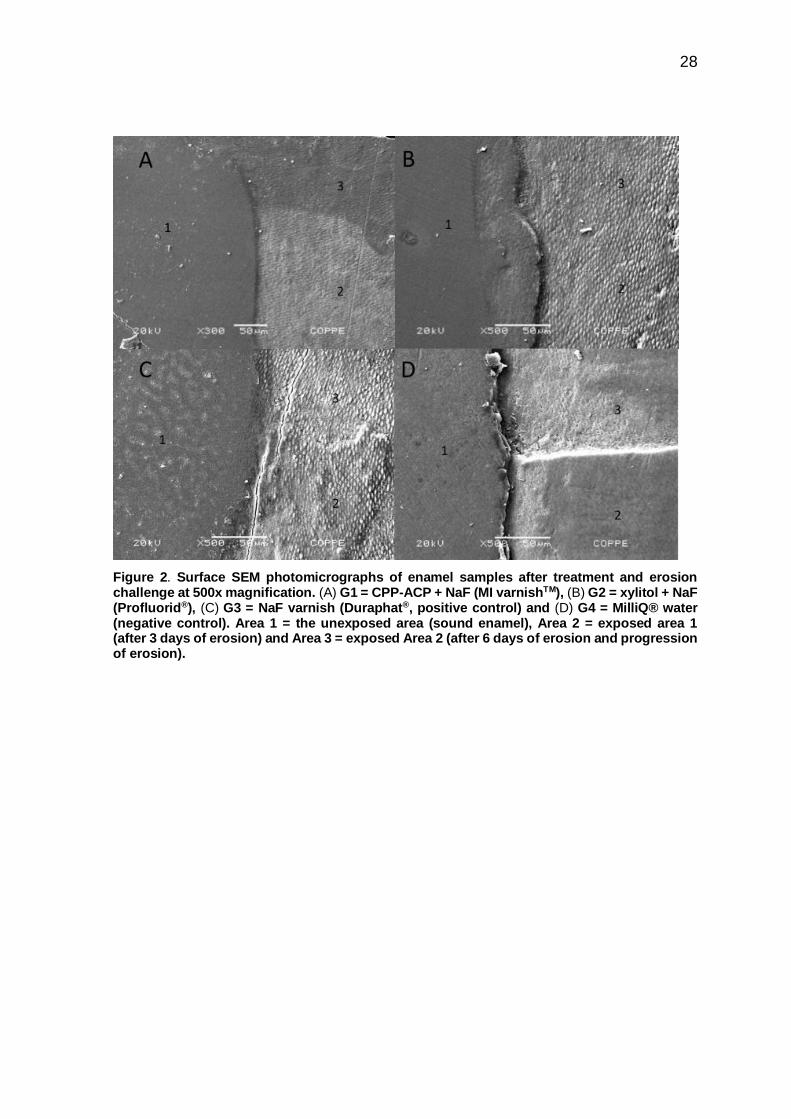
Figure 2. Surface SEM photomicrographs of enamel samples after treatment and
erosion challenge at 500x magnification. (A) G1 = CPP-ACP + NaF (MI varnishTM),
(B) G2 = xylitol + NaF (Profluorid®), (C) G3 = NaF varnish (Duraphat®, positive
control) and (D) G4 = MilliQ® water (negative control). Area 1 = the unexposed area
(sound enamel), Area 2 = exposed area 1 (after 3 days of erosion) and Area 3 =
exposed Area 2 (after 6 days of erosion and progression of erosion). ................. 28
Figure 3. Surface SEM photomicrographs of enamel samples after treatment and
erosion challenge at 1000x magnification. (A) G1 = CPP-ACP + NaF (MI varnishTM),
(B) G2 = xylitol + NaF (Profluorid®), (C) G3 = NaF varnish (Duraphat®, positive
control) and (D) G4 = MilliQ® water (negative control). Photomicrographs I =
exposed Area 1 (after 3 days of erosion) and Photomicrographs II = exposed Area
2 (after 6 days of erosion and progression of erosion). ........................................ 29
Figure 4. 3D profilometry scheme and graphic representation of enamel surface
samples after treatment and erosion challenge (after 3 and 6 days of erosion) for
each group. (A) G1 = CPP-ACP + NaF (MI varnishTM), (B) G2 = xylitol + NaF
(Profluorid®), (C) G3 = NaF varnish (Duraphat®, positive control) and (D) G4 =
MilliQ® water (negative control). Arrow 1 = the unexposed area (sound enamel),
Arrow 2 = exposed Area 1 (after 3 days of erosion) and Arrow 3 = exposed Area 2
(after 6 days of erosion and progression of erosion). Graphic I = profile of unexposed
area to exposed Area 1, Graphic II = profile of unexposed area to exposed Area 2.
............................................................................................................................. 30

Artigo 2
Figure 1 - 3D profilometry scheme representation of surface of enamel samples after
treatment and erosion/abrasion challenge. Left – sound window (unexposed area)
and right – experimental window (exposed area). (A) G1= NaF varnish (Duraphat®)
(B) G2= CPP-ACP + NaF (MI varnishTM), C) G3= Xylitol + NaF (Profluorid®) and D)
G4= MilliQ® water (negative control).................................................................... 47
Figure 2 - Surface SEM images of enamel samples after treatment and
erosion/abrasion challenge at 500X (Photomicrographs of the interface: left – sound
window: unexposed area and right – experimental window: exposed area) and
1000X (Photomicrographs of exposed area in the upper right corner of each photo).
(A) G1= NaF varnish (Duraphat®) (B) G2= CPP-ACP + NaF (MI varnishTM), C) G3=
Xylitol + NaF (Profluorid®) and D) G4= MilliQ® water (negative control). ............. 48
Artigo 3
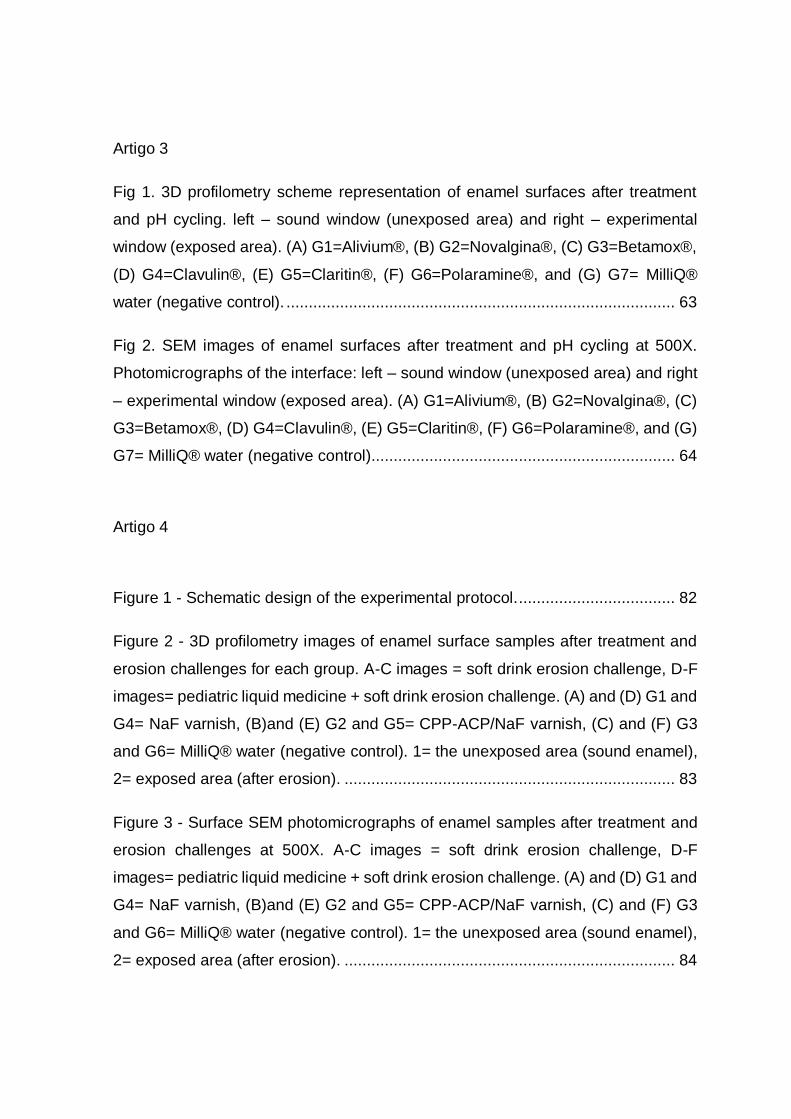
Fig 1. 3D profilometry scheme representation of enamel surfaces after treatment
and pH cycling. left – sound window (unexposed area) and right – experimental
window (exposed area). (A) G1=Alivium®, (B) G2=Novalgina®, (C) G3=Betamox®,
(D) G4=Clavulin®, (E) G5=Claritin®, (F) G6=Polaramine®, and (G) G7= MilliQ®
water (negative control). ....................................................................................... 63
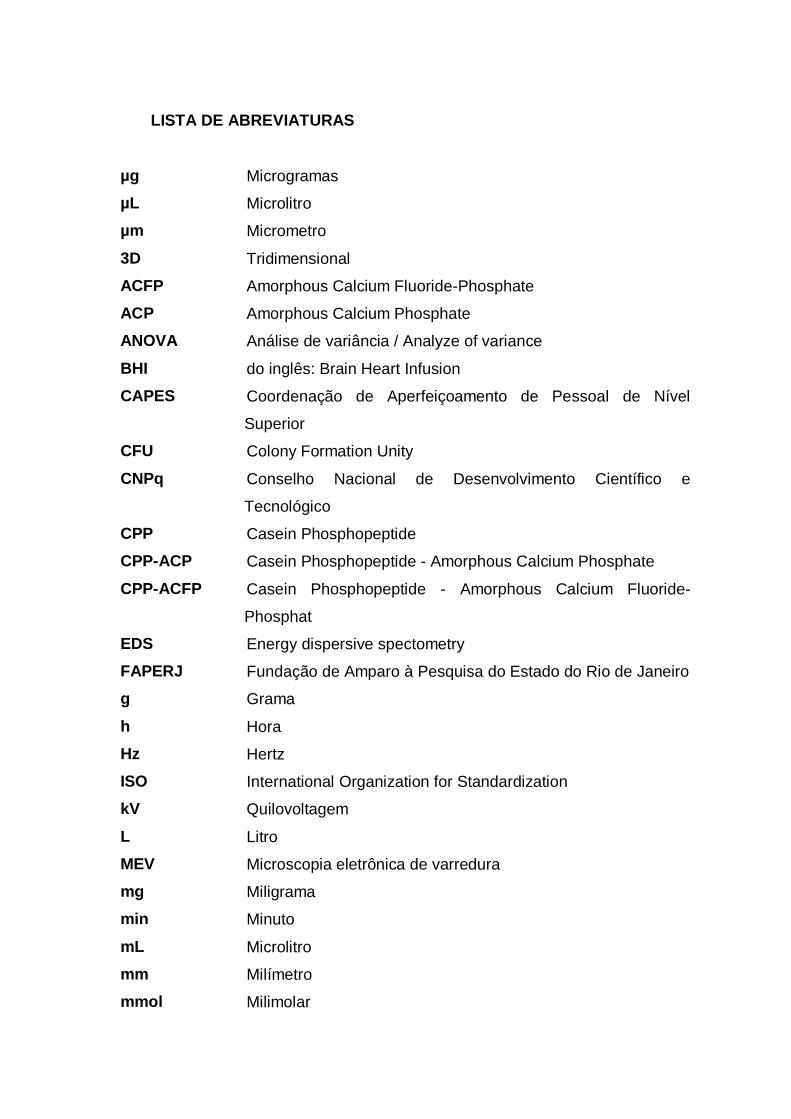
Fig 2. SEM images of enamel surfaces after treatment and pH cycling at 500X.
Photomicrographs of the interface: left – sound window (unexposed area) and right
– experimental window (exposed area). (A) G1=Alivium®, (B) G2=Novalgina®, (C)
G3=Betamox®, (D) G4=Clavulin®, (E) G5=Claritin®, (F) G6=Polaramine®, and (G)
G7= MilliQ® water (negative control).................................................................... 64
Artigo 4
Figure 1 - Schematic design of the experimental protocol. ................................... 82
Figure 2 - 3D profilometry images of enamel surface samples after treatment and
erosion challenges for each group. A-C images = soft drink erosion challenge, D-F
images= pediatric liquid medicine + soft drink erosion challenge. (A) and (D) G1 and
G4= NaF varnish, (B)and (E) G2 and G5= CPP-ACP/NaF varnish, (C) and (F) G3
and G6= MilliQ® water (negative control). 1= the unexposed area (sound enamel),
2= exposed area (after erosion). .......................................................................... 83
Figure 3 - Surface SEM photomicrographs of enamel samples after treatment and
erosion challenges at 500X. A-C images = soft drink erosion challenge, D-F
images= pediatric liquid medicine + soft drink erosion challenge. (A) and (D) G1 and
G4= NaF varnish, (B)and (E) G2 and G5= CPP-ACP/NaF varnish, (C) and (F) G3
and G6= MilliQ® water (negative control). 1= the unexposed area (sound enamel),
2= exposed area (after erosion). .......................................................................... 84

Figure 4 - Surface SEM photomicrographs of enamel samples after treatment and
erosion challenges at 2000X. A-C images = soft drink erosion challenge, D-F
images= pediatric liquid medicine + soft drink erosion challenge. (A) and (D) G1 and
G4= NaF varnish, (B)and (E) G2 and G5= CPP-ACP/NaF varnish, (C) and (F) G3
and G6= MilliQ® water (negative control). Arrow 1= exposure of enamel`s prisms,
arrow 2= little depressions in enamel`s surface, arrow 3= great depressions/craters.
............................................................................................................................. 85
LISTA DE ABREVIATURAS
µg Microgramas
µL Microlitro
µm Micrometro
3D Tridimensional
ACFP Amorphous Calcium Fluoride-Phosphate
ACP Amorphous Calcium Phosphate
ANOVA Análise de variância / Analyze of variance
BHI do inglês: Brain Heart Infusion
CAPES Coordenação de Aperfeiçoamento de Pessoal de Nível
Superior
CFU Colony Formation Unity
CNPq Conselho Nacional de Desenvolvimento Científico e
Tecnológico
CPP Casein Phosphopeptide
CPP-ACP Casein Phosphopeptide - Amorphous Calcium Phosphate
CPP-ACFP Casein Phosphopeptide - Amorphous Calcium Fluoride-
Phosphat
EDS Energy dispersive spectometry
FAPERJ Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro
g Grama
h Hora
Hz Hertz
ISO International Organization for Standardization
kV Quilovoltagem
L Litro
MEV Microscopia eletrônica de varredura
mg Miligrama
min Minuto
mL Microlitro
mm Milímetro
mmol Milimolar

mm2 Milímetro quadrado
mol Molar
P.A. Para análise
Pa Pascal
pH Potencial hidrogeniônico
PLM Pediatric liquid medicine
ppm Parte por milhão
Ra Rugosidade superficial linear
MSI Microdureza Superficial Inicial
rpm Rotações por minuto
s Segundo
Sa Rugosidade superficial volumetrica
SD Soft drink
SDE Soft drink erosion
SEM Scanning electron microscopy
SMH Surface microhardness
SPSS Statistical analysis for social sciences
SR Surface Roughness
UFC Unidade Formadora de Colônia
Tris Tris-hidroximetilaminometano
TSL Tooth Structure Loss
UESB Universidade Estadual do Sudoeste da Bahia
UFPB Universidade Federal da Paraíba
UFRJ Universidade Federal do Rio de Janeiro

LISTA DE SÍMBOLOS
% Porcentagem
± Mais ou menos
® Marca Registrada
< / > Menor que / maior que
°C Graus celsius
Ca Cálcio (elemento químico)
Ca2+ Íon cálcio
CaF 2 Fluoreto de cálcio
F Flúor (elemento químico)
F- Íon flúor
KCl Cloreto de Potássio
NaF Fluoreto de sódio
P Fósforo
PO4 Fosfato
x Vezes
SUMÁRIO
1. INTRODUÇÃO ................................................................................................. 1
2. OBJETIVOS ..................................................................................................... 5
2.1. Objetivo geral .........................................................................................................5
2.2. Objetivos específicos ............................................................................................5
3. MATERIAIS E MÉTODO ................................................................................. 6
3.1. Delineamento da pesquisa ..................................................................................6
3.2. Obtenção e preparo dos espécimes dentários ...............................................6
3.2.1. Corte, planificação e polimento dos espécimes .............................................6
3.2.2. Avaliação da microdureza superficial inicial para seleção dos blocos de
esmalte ...................................................................................................................................7
3.2.3. Tratamento dos espécimes dentários ..............................................................8
3.2.3.1. Experimentos com vernizes ................................................................................8
3.3. Avaliação das características topográficas dos espécimes ........................8
3.5. Protocolo de abrasão dentária artificial .......................................................... 11
3.6. Análise estatística ............................................................................................... 11
4. ARTIGOS CIENTÍFICOS ............................................................................... 13
4.1. Artigo 1 – Inhibition of tooth erosion and its progression by NaF varnishes
containing calcium or xylitol: An in vitro study.............................................................. 14
4.2. Artigo 2 - Enamel erosion and abrasion-inhibiting effect of NaF fluoride
varnishes with or without CPP-ACP or xylitol .............................................................. 34
4.3. Artigo 3 – Do pediatric medicines induce topographic changes in dental
enamel under cariogenic challenge? ............................................................................. 52
4.4. Artigo 4 – Protective effect of NaF varnish with CPP-ACP against dental
erosion caused by soft drink associated to pediatric liquid medicine. .................... 70
5. DISCUSSÃO .................................................................................................. 90
6. CONCLUSÕES .............................................................................................. 92
REFERÊNCIAS .................................................................................................... 93
1
1. INTRODUÇÃO
Apesar da redução dos níveis globais de cárie em países desenvolvidos e em
desenvolvimento (Scavuzzi, De Franca Caldas Junior et al. 2007, Antunes and
Narvai 2010, Nunes, da Silva et al. 2014). A redução dos níveis de cárie foi
acompanhada por um aumento na prevalência de outras desordens dentárias, tais
como o desgaste dentário (lesão do tipo não cariosa) que pode ser observado em
crianças e adolescentes (Mahoney and Kilpatrick 2003, Huysmans, Chew et al.
2011). Essas lesões não cariosas englobam principalmente a erosão e a abrasão
(Shellis and Addy 2014, Shellis, Featherstone et al. 2014).
A cárie e erosão dentária apresentam distintos fatores etiológicos entre si e o
tipo de ácido que determina as características clínicas de ambas são diferentes
(West and Joiner 2014). A respeito da desmineralização associada à cárie, essa é
resultante do desequilíbrio entre os fatores de desmineralização e remineralização,
sendo função direta da fermentação de carboidratos da dieta por bactérias
acidogênicas do biofilme dental que torna o pH bucal crítico, ou seja, menor que
5,5 (Hicks, Garcia-Godoy et al. 2004, Featherstone 2008, Kudiyirickal and
Ivancakova 2008, Marsh 2009).
O principal carboidrato envolvido na produção de ácidos orgânicos pelas
bactérias orais é a sacarose, pois, além de ser fermentada, ela também serve de
substrato para a síntese de polissacarídeos extracelulares, que alteram as
propriedades da matriz do biofilme tornando-o mais poroso e permitindo um melhor
aproveitamento bacteriano dos açúcares e maior penetração de ácidos orgânicos,
culminando em maior perda mineral (Zero, van Houte et al. 1986).
Quanto à desmineralização associada à erosão também é causada pela
frequente exposição do elemento dentário a ácidos que promovem um baixo pH,
porém de origem não bacteriana (Huysmans, Chew et al. 2011, Shellis, Barbour et
al. 2013, Lussi and Carvalho 2014, Lussi and Carvalho 2015). Além disso, a
desmineralização acontece inicialmente como um perda mineral da superfície
dentária, seguido por dissolução contínua do esmalte prismático e interprismático,
gerando uma desmineralização superficial, que evolui a cada desafio erosivo,
levando a perda gradual deste tecido (Lussi and Jaeggi 2006, Shellis, Featherstone

2
et al. 2014). Ressalta-se que esse processo químico erosivo é desencadeado por
ácidos de origem intrínseca ou extrínseca sem envolvimento de microrganismos
(Mahoney and Kilpatrick 2003, Huysmans, Chew et al. 2011).
Atualmente, os ácidos extrínsecos têm sido considerados os principais fatores
relacionados com a ocorrência de erosão dentária. Como exemplo, têm-se as
bebidas ácidas como refrigerantes e sucos de fruta e alguns medicamentos. Em
função de uma mudança dos hábitos dietéticos da população, observa-se o maior
consumo de bebidas ácidas (Barbour and Lussi 2014, West and Joiner 2014). Além
disso, o baixo pH associado aos componentes ácidos que são usados como
conservantes em alguns medicamentos líquidos pediátricos também podem
promover o processo de perda mineral (Hellwig and Lussi 2006).
Uma condição que pode interferir na perda de estrutura dental e
consequentemente no processo de desmineralização do esmalte é a abrasão. Esta
corresponde a um desgaste ocasionado por um fator mecânico, como a escovação
dentária (Shellis and Addy 2014). Os desafios mecânicos são de grande impacto
especialmente sobre superfícies erodidas. A superfície erodida é mais susceptível
ao desgaste devido à diminuição da sua dureza sendo mais facilmente removida
devido as forças mecânicas (Rios, Honorio et al. 2006).
Os compostos fluoretados têm grande importância como agentes preventivos
e terapêuticos, tanto no processo de cárie, quanto diante de desafios erosivos e
abrasivos. Essa condição é atribuída à formação da hidroxiapatita fluoretada, que
apresenta menor grau de dissolução quando comparado à hidroxiapatita, como
também a formação de cristais de fluoreto de cálcio (CaF2), que funcionam como
um reservatório de fluoreto na cavidade oral (Marinho 2006, Newbrun 2010).
Vários produtos fluoretados de uso caseiro ou profissional tem sido
extensivamente estudados devido sua ação em prevenir, tratar ou diminuir a
progressão da desmineralização dentária (Marinho, Higgins et al. 2002, Marinho
2009, Newbrun 2010). Além disso, na literatura, novos compostos têm sido
propostos, em associação ou não ao fluoreto, como uma tentativa em se obter
melhores efeitos contra a desmineralização dentária (Reynolds 2009, Cochrane
and Reynolds 2012). Dentre esses, encontram-se o xilitol e o fosfocaseinato de
3
cálcio, do inglês "Casein Phosphopeptide - Amorphous Calcium Phosphate” (CPP-
ACP).
O xilitol é um açúcar de característica não acidogênico, muito uitlizado na
indústria alimentícia (Makinen 2010), que possui a abilidade de formar complexos
com íons cálcio (Ca2+), e por isso, tem sido adicionado em produtos odontológicos
com intuito de aumentar a deposição de cálcio (Ca) no esmalte dentário (Miake,
Saeki et al. 2003, Makinen 2010), além de inibir a dissolução de cálcio e fostato
(PO4) da estrutura dental (Chunmuang, Jitpukdeebodintra et al. 2007, Vongsavan,
Surarit et al. 2014).
O CPP-ACP é um nanocomposto, que promove a estabilização e a
manutenção de cálcio e fosfato por peptídeos derivados da caseína do leite (CPP,
do inglês: casein phosphopeptide) sem a ocorrência de precipitação. O CPP pode
ligar-se a superfícies, tais como biofilme, esmalte dentário ou dentina, fornecendo
uma reserva de Ca e PO4 disponíveis para a saliva e para a superfície dentária, de
forma a atuar no processo de des-remineralizacao (Cross, Huq et al. 2007,
Reynolds 2008). Além disso, pode existir uma interação com íons flúor formando o
composto ACFP (do inglês: Amorphous Calcium Fluoride-Phosphate). Este
proporcionaria um benefício adicional devido à presença do flúor incorporado ao
nanocomposto (Reynolds, Cai et al. 2008, Reynolds 2009, Cochrane, Shen et al.
2014).
Os compostos de escala nanométrica (nanocomposto) podem trazer
melhorias químicas e físicas em relação às estruturas micrométricas, tais como:
maior estabilidade térmica e mecânica, maior resistência ao calor e menor
dissolução (Gonzalez-Vidal, Muñoz-Guerra et al. 2010, Narayanan, Koodathil et al.
2010, Reyna-valencia, Deyrail et al. 2010).
Devido à tais benefícios do xilitol e do CPP-ACP, pode-se supor que a adição
desses produtos a vernizes odontológicos pode ter um efeito benéfico no que diz
respeito àprevenção e à inibição da perda mineral dentária. Um dos grandes
desafios e motivações da odontologia atual está no desenvolvimento de produtos
odontológicos bioativos, tornando-os capazes de inibir a perda dos tecidos
dentários, sob diferentes condições clínicas (Feitosa, Munchow et al. 2015).

4
Desta forma, o presente estudo tevepor objetivo verificar o efeito preventivo
de erosão e à erosão associada à abrasão de compostos contendo cálcio e xilitol
em sua formulação.
5
2. OBJETIVOS
2.1. Objetivo geral
Avaliar, in vitro, o efeito de compostos a base de cálcio e xilitol na prevenção
da erosão e da erosão associada à abrasão sobre o esmalte bovino.
2.2. Objetivos específicos
2.2.1. Avaliar o efeito preventivo de vernizes a base de CPP-ACP e xilitol
em relação à erosão e a progressão da erosão dentária;
2.2.2. Avaliar o efeito preventivo de vernizes a base de CPP-ACP e xilitol
em relação à erosão associada à abrasão dentária;
2.2.3. Verificar o potencial erosivo de medicamentos líquidos pediátricos e
avaliar o efeito preventivo de um verniz a base de CPP-ACP frente à erosão
promovida por refrigerante ou refrigerante associado a um medicamento
liquido pediátrico.

6
3. MATERIAIS E MÉTODO
3.1. Delineamento da pesquisa
A proposta deste trabalho foi avaliar, in vitro, o efeito da aplicação tópica de
nanocompostos a base de cálcio frente à erosão e à erosão associada à abrasão.
A fim de cumprir o objetivo geral e os objetivos específicos, a presente tese foi
composta por 4 artigos científicos que correspondem ao percurso metodológico
adotado.
A seguir serão apresentadas as etapas realizadas nos diferentes estudos
fazendo a correspondência entre elas e os respectivos artigos que compõem esta
tese.
3.2. Obtenção e preparo dos espécimes dentários
3.2.1. Corte, planificação e polimento dos espécimes
Para obtenção da amostra de cada estudo relatado na forma de artigo,
dentes bovinos hígidos foram selecionados e somente foram escolhidos aqueles
livres de ranhuras, hipoplasias, trincas, manchas, abrasões ou quaisquer
alterações visíveis macroscopicamente sob exame em lupa estereoscópica (40x).
Os dentes foram armazenados à temperatura ambiente em solução aquosa de
formol a 2% com pH 7,0 até o momento da utilização.
Após a seleção, as raízes foram removidas com o auxílio de um disco
diamantado montado em peça-reta e posteriormente as coroas foram fixadas,
separadamente, com cera pegajosa em placas de acrílico. Cada placa de acrílico,
com seu respectivo dente, foi acoplada na cortadeira (Buehler Ltd., Lake Bluff,
Illinois, USA), e com auxílio de um disco diamantado dupla-face (Extec Corp.,
Enfield, Connecticut, USA) foram realizados 4 cortes verticais e horizontais na
região central da face vestibular das coroas para obtenção de blocos dentários com

7
16mm2.
Com o intuito de realizar a planificação da dentina, os fragmentos foram
fixados com cera pegajosa no centro de um dispositivo de polipropileno (tarugo)
com a maior área plana de esmalte voltada para o dispositivo. O conjunto foi
adaptado em uma politriz metalográfica (Fortel Indústria e Comércio, São Paulo,
São Paulo, Brasil) e a planificação foi realizada sob refrigeração utilizando-se lixa
de granulação 600 (Extec Corp., Enfield, Conecticut, EUA) até que os fragmentos
ficassem planos e com espessura de aproximadamente 2mm.
Posteriormente, os blocos foram novamente fixados em dispositivos de
polipropileno, desta vez com o esmalte voltado para cima. O conjunto foi
novamente adaptado na politriz, o desgaste e polimento do esmalte foram
realizados utilizando-se lixas de granulação 600 e 1200 (Extec Corp., Enfield,
Conecticut, EUA) respectivamente. Entre cada etapa de polimento, o conjunto
dente/tarugo foi imerso em água destilada e deionizada e levado a um aparelho de
ultra-som (Cristófoli, São Paulo, São Paulo, Brasil) por 3min.
3.2.2. Avaliação da microdureza superficial inicial para seleção dos
blocos de esmalte
Para a seleção dos blocos utilizados nos artigos da tese foi realizada uma
avaliação da microdureza superficial inicial (MSI) do esmalte. Para tanto, utilizou-
se um microdurômetro (Buehler, MICROMET 5104, 679-MIT4-00335, Yokohama,
Kanagawa, Japão) com um penetrador diamantado piramidal tipo Knoop com carga
de 50g aplicada por 5s. Em cada corpo de prova foram realizadas 5 endentações
dispostas em uma coluna na região central de cada espécime, com espaçamento
de 100µm entre elas (Nassur, Alexandria et al. 2013). Os blocos que apresentaram
o valor de microdureza 10% acima ou abaixo da média dos corpos de prova foram
descartados.
8
Todos os blocos tiveram a metade de sua superfície recoberta com um verniz
ácido resistente (Colorama, L’Óreal, Clichy, França) a fim de favorecer as análises
subsequentes, resultando em uma área não-exposta (área controle de esmalte
hígido) e outra área exposta (área experimental que recebeu o tratamento de
acordo com o grupo ao qual foi alocado).
3.2.3. Tratamento dos espécimes dentários
3.2.3.1. Experimentos com vernizes
Nos experimentos que utilizaram os vernizes de uso tópico como tratamento,
a aplicação do produto foi realizada com auxílio de um micro pincel no início do
experimento, sendo toda a superfície do bloco destinada ao tratamento (área
exposta) recoberta com o produto. Em seguida, os espécimes foram imersos em
saliva artificial por 6h a 37ºC. Após esse tempo, a camada de verniz foi removida
com auxilio de lâmina de bisturi (Advantive, Weert, Limburgo, Holanda) e acetona
P.A. (Sigma-Aldrich, St. Louis, Missouri, USA) diluída em água Mili-Q (na proporcão
de 1:1). A saliva artificial era composta por: 0,1mol/L de tampão Tris; 1,5mmol/L de
Ca; 0,9mmol/L de P; 150mmol/L de KCl e 0,05µgF/mL (Nassur, Alexandria et al.
2013). Os estudos foram desenvolvidos com os seguintes vernizes: 1) verniz a base
de fluoreto de sódio (NaF, 5% de NaF, Duraphat®, Colgate Oral Pharmaceuticals,
New York, New York, EUA); 2) verniz a base de NaF e CPP-ACP (NaF/CPP-ACP,
2% de CPP-ACP e 5% de NaF, MI varnishTM, GC America, Alsip, Illinois, EUA); e
3) verniz a base de NaF e xilitol (NaF/xilitol, 1% de xilitol e 5% de NaF, Profluorid®,
Voco, Cuxhaven, Niedersachsen, Alemanha).
3.3. Avaliação das características topográficas dos espécimes
Nesta etapa, procedeu-se a remoção, com acetona P.A., do verniz ácido-
resistente que recobria a metade da superfície dos blocos para permitir a execução
das análises descritas a seguir.
3.3.1. Perfilômetro 3D de não-contato

9
Para a análise da topografia do esmalte dentário, os espécimes foram
avaliados por meio de perfilômetro 3D de não contato (Nanovea PS50 Optical,
NANOVEA Inc., USA). A captura foi realizada através de um sensor cromático
confocal com uma fonte de luz branca axial a uma velocidade de varredura de
2μm/s e índice de refração de 10000Hz. Os seguintes parâmetros foram avaliados:
Rugosidade linear (Ra) (ISO 4287): Três leituras lineares (horizontais)
foram realizadas na superfície antes e após a exposição. A média dessas 3 leituras
corresponderam ao valor médio de Ra1 (rugosidade linear na área hígida) e Ra2
(rugosidade linear na área experimental). O valor de Ra que correspondeu à
alteração de rugosidade superficial linear foi calculado pela seguinte fórmula:
Ra= Ra2 - Ra1, onde Ra=diferença de rugosidade superficial linear,
Ra1=rugosidade linear na área hígida e Ra2=rugosidade linear na área
experimental.
Rugosidade superficial volumétrica (Sa) (ISO 25 178): Três leituras de
área de 200μm2 foram realizadas na superfície antes e após exposição. A média
dos valores mensurados correspondeu ao valor médio de Sa1 (rugosidade
volumétrica na área hígida) Sa2 (rugosidade volumétrica na área experimental). O
valor de Sa que correspondeu a alteração de rugosidade superficial volumétrica foi
calculado pela seguinte fórmula:
Sa= Sa2 - Sa1, onde Sa=diferença de rugosidade superficial volumétrica,
Sa1=rugosidade volumétrica na área hígida e Sa2=rugosidade volumétrica na área
experimental.
Perda de estrutura dentária (μm): Três leituras com comprimento de 1 mm
foram realizadas englobando a área hígida (não exposta) e a área experimental
(exposta). Dessa forma, foi possível quantificar a diferença em altura (degrau) entre
essas duas áreas, mensurando assim, quanto de estrutura dentária foi perdida após
o experimento.
Avaliação qualitativa da topografia do esmalte dentário: A imagem
gerada após captura foi analisada com os recursos do programa Nanovea

10
Professional 3D, no qual houve nivelamento do corpo de prova, tratamento das
imagens, ajuste das escalas, da cor e da nitidez.
Todas as análises foram realizadas por um examinador cego, o qual
identificou os espécimes apenas pela numeração aleatória previamente
demarcada.
3.3.2. Análise em Microscopia Eletrônica de Varredura (MEV)
Três blocos de esmalte selecionados aleatoriamente de cada grupo foram
analisados em microscopia eletrônica de varredura tendo em vista a análise
qualitativa das alterações superficiais da camada externa do esmalte. Sendo assim,
após o período experimental, os blocos de esmalte foram fixados em stubs com fita
de carbono dupla-face e cobertos com uma fina camada de ouro de
aproximadamente 30µm. As amostras foram analisadas em microscópio (6460LV,
JEOL, Tokyo, Japan) operando com 20kV e vácuo de 45Pa no qual pôde-se
observar a estrutura superficial após cada tratamento.
3.4. Protocolo de erosão dentária artificial
As amostras destinadas aos estudos de erosão (artigos descritos nos tópicos
4.1, 4.2, 4.3 e 4.4) foram imersas em produtos de baixo pH (Sprite®, Coca-Cola® ou
Claritin®) para simular a erosão ácida no esmalte dentário. A imersão foi realizada
por um tempo determinado previamente (5 ou 10min), variando de 3 a 6 vezes ao
dia, durante 3 ou 4 dias, dependendo da metodologia do estudo. A aplicação dos
produtos teste (vernizes) era realizada antes do período de erosão conforme
protocolo descrito no item 3.2.3.1. No intervalo entre os períodos de erosão e ao
final do dia, as amostras foram imersas em saliva artificial (1,5mmol/L de Ca,
0,9mmol/L de P, 150mmol/L de KCl, 0,05μgF/mL e 0,1 mol/L de tampão Tris, pH
7,0, 30mL/espécime).
11
3.5. Protocolo de abrasão dentária artificial
As amostras destinadas ao estudo de erosão associada à abrasão além de
serem imersas em um produto de baixo pH para simular a erosão ácida no esmalte
dentário, também foram expostas à escovação mecânica para simular o processo
de abrasão promovido durante a escovação dentária.
A abrasão foi executada 2 vezes ao dia, por 15s, sendo 50 escovações por
segundo em máquina de escovação com escovas de cerdas macias e um slurry de
dentifrício placebo (sem fluoreto), sendo a carga utilizada de 200g. No intervalo
entre os períodos de erosão/abrasão e ao final do dia as amostras eram imersas
em saliva artificial como descrito anteriormente.
3.6. Análise estatística
O software SPSS versão 22.0 foi utilizado para tabular os dados e executar
os testes estatísticos. O nível de significância adotado foi fixado em 5%.
A distribuição normal dos dados foi verificada para todas as variáveis
testadas, utilizando o teste Shapiro Wilks (p<0.05).
Para testar se os tratamentos causaram efeito em relação aos parâmetros
utilizados comparando o momento inicial versus final, utilizou-se o teste t de Student
pareado.
Vários parâmetros foram utilizados para avaliar a diferença entre os
resultados dos distintos tratamentos. Testes estatísticos foram aplicados de acordo
com a distribuição normal (paramétricos) ou não normal (não paramétricos) dos
dados, estando descritos nos artigos que compõe a presente tese.
Para as alterações na rugosidade superficial (Ra e Sa) utilizaram-se os
testes: análise de variância (ANOVA) seguido pelo teste Tukey, teste Kruskal-Wallis
ou o teste Mann-Whitney de acordo com distribuição normal ou não normal dos
dados nos diferentes estudos.
12
As análises das imagens obtidas no MEV e no perfilômetro 3D de não
contato foram avaliadas descritivamente.

13
4. ARTIGOS CIENTÍFICOS
Artigo 1 – Inhibition of tooth erosion and its progression by NaF varnishes
containing calcium or xylitol: An in vitro study - Artigo a ser enviado para revista
Journal of Dentistry
Artigo 2 – Enamel erosion and abrasion-inhibiting effect of NaF fluoride
varnishes with or without CPP-ACP or xylitol - Artigo a ser enviado para revista
Journal of Dentistry
Artigo 3 – Do pediatric medicines induce topographic changes in dental
enamel? - Artigo aceito na revista Brazillian of Oral Research
Artigo 4 – Protective effect of NaF varnish with CPP-ACP against dental
erosion caused by soft drink associated to pediatric liquid medicine - Artigo a ser
enviado para revista Brazilian Oral Research
14
4.1. Artigo 1 – Inhibition of tooth erosion and its progression by NaF
varnishes containing calcium or xylitol: An in vitro study
Short title: Inhibition of tooth erosion by NaF varnishes
Adílis Kalina Alexandria1
Amanda Garcia Mayworm1
Rafael Lopes Marambaia1
Ana Maria Gondim Valença2
Lúcio Mendes Cabral3
Lucianne Cople Maia1
1 Department of Pediatric Dentistry and Orthodontics, School of Dentistry,
Federal University of Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil
2 Department of Clinical and Social Dentistry, Dental School, Federal
University of Paraiba (UFPB), João Pessoa, PB, Brazil
3 School of Pharmacy, Federal University of Rio de Janeiro (UFRJ), Rio de
Janeiro, RJ, Brazil
Corresponding author:
Lucianne Cople Maia
Disciplina de Odontopediatria da FO-UFRJ, Caixa Postal: 68066 – Cidade
Universitária – CCS, CEP: 21941-971 - Rio de Janeiro – RJ –Brazil
Fax/phone: +5521 39382101
E-mail: [email protected]

15
Abstract
Objectives: To evaluate the preventive effect of NaF varnishes containing
calcium or xylitol against erosion and its progression. Methods: Forty enamel blocks
were divided into four groups (n = 10): G1 = CPP-ACP + NaF varnish (MI varnishTM);
G2 = xylitol + NaF varnish (Profluorid®); G3 = NaF varnish (Duraphat®, positive
control) and G4 = MilliQ® water (negative control). The samples were immersed in
soft drink (4x per day for 3 days), in between immersions, the specimens stayed in
artificial saliva. After 3 days of erosion, the eroded area was divided in two. (Half of
one of these areas received a new treatment while the other half repeated the same
3-day erosion cycle; the other half of the original area was protected.) The 3D, non-
contact profilometry technique was used to determinate tooth structure loss (TSL)
and surface roughness (SR). Scanning electron microscopy (SEM) and 3D images
were utilized to evaluate the topography of the samples. Mann-Whitney, one-way
ANOVA and Tukey tests were used. SEM and 3D images were descriptively
evaluated. Results: After 3 or 6 days of erosion, all tested varnishes were better
than G4 (p < .05) for TSL and SR. In addition, G1 had lower values (6.23 μm) for
TSL than G3 (10.32 μm) (p < .05) after 3 days of erosion. Under SEM and 3D
images observation, all groups presented porosity, irregularities and depressions on
the surface enamel after 3 and 6 days of erosion, which were more pronounced in
G4. Conclusion: An application of topical NaF varnishes was effective in reducing
TSL and enamel roughness after erosion challenges. Furthermore, the presence of
CPP-ACP improved the performance of NaF varnish in protecting against TSL after
3 days of erosion.
16
Introduction
The prevalence of tooth erosion is steadly increasing, specially in children
and adolescents (Kreulen, Van 't Spijker et al. 2010). This disease is defined as
chemical wear of dental hard tissue by intrinsic or extrinsic acids without bacterial
involvement (Shellis, Barbour et al. 2013, Lussi and Carvalho 2014).
In dental erosion, the dissolution of mineral from the enamel surface results
in a roughened structure. If the erosion process persist, the effect of acids on a
roughened surface is inhanced, promoting a fast progression of tissue loss and
fomrtion of a visible defect (Lussi and Carvalho 2014).
Several methods, such as the use of professional topical fluorides, have been
proposed to prevent or slow down the progression of dental erosion and its
consequences (Magalhaes, Wiegand et al. 2011, Mohammed and Dusara 2013,
Lussi and Carvalho 2015, Sar Sancakli, Austin et al. 2015). In this context, the
addition of other remineralizing compounds to fluoride varnishes can be an
alternative to increase protection against erosive wear.
Casein phosphopeptide-amorphous calcium phosphate nanocomplex (CPP-
ACP) is a technology based on amorphous calcium phosphate (ACP) and stabilized
by casein phosphopeptides (CPP) under the name RecaldentTM. It has been
reported that the CPP-ACP nanocomplexes maintain a sufficiently high
concentration of calcium and phosphate ions to promote enamel remineralization
and interact with fluoride ions to produce an ACFP phase, which gives better
benefits because of the fluoride ion (Reynolds, Cai et al. 2008, Reynolds 2009,
Cochrane, Shen et al. 2014).
Xylitol is a non-acidogenic sweetener, very often used in the food industry
(Makinen 2010). Due its ability to form complexes with calcium ions (Miake, Saeki
et al. 2003, Makinen 2010), the addiction of xylitol in dental products can enhance
calcium deposition in dental enamel (Miake, Saeki et al. 2003) and inhibit the
dissolution of calcium and phosphate ions from enamel structure (Chunmuang,
Jitpukdeebodintra et al. 2007, Vongsavan, Surarit et al. 2014). Because of these

17
benefits, the addition of CPP-ACP or xylitol in fluoride dental varnishes could have
an important influence on prevention of tooth erosion.
Thus, this in vitro study assessed the protective effect of NaF varnishes
containing calcium or xylitol in the prevention of enamel erosion and the progression
of dental erosion. Two null hypotheses were formulated: (1) the presence of calcium
or xylitol does not improve the effect of NaF varnish on preventing tooth structure
loss after 3 or 6 days of dental erosion and (2) the presence of calcium or xylitol
does not improve the effect of NaF varnish in preventing alterations in roughness
after 3 or 6 days of dental erosion.
Methods
Specimen preparation
Bovine incisors teeth were cut using an ISOMET low-speed saw (Buehler
Ltd, Lake Bluff, Illinois, USA) with 2 diamond discs (Extec Corp, Enfield,
Connecticut, USA) separated by a 4-mm spacer to obtain 4 x 4mm specimens. The
enamel blocks surface was polished using water-cooled, silicon carbide paper 600
and 1200 (Extec Corp., Enfield, Connecticut, USA), followed by a 1-µm diamond
abrasive slurry (Extec Corp., Enfield, Connecticut, USA). After each polishing
phase, the specimens were cleaned in an ultrasonically device with MilliQ® water for
5min.
Baseline surface microhardness (SMH) was obtained using a microhardness
tester (Buehler, MICROMET 5104, 679-MIT4-00335, Yokohama, Kanagawa,
Japan) with a Knoop diamond under a 50-g load for 5s, while five indentations
spaced 100µm from each other were made at the centre of the enamel surface. A
nail varnish was applied to the left half of the specimen’s surface to maintain the
sound reference (unexposed area, self-control); the other half of the surface (left
side was not covered, exposed area 1) received the treatment and it was exposed
to erosion challenges.
Forty enamel specimens (SMH = 369.7 ± 36.8kg/mm2) were randomly
allocated to each group: G1 = CPP-ACP + NaF varnish (2% CPP-ACP and 5% NaF,
18
MI varnishTM, GC America, Alsip, Illinois, USA); G2 = xylitol + NaF varnish (1% xylitol
and 5% NaF, Profluorid®, Voco, Cuxhaven, Niedersachsen, Germany); G3 = NaF
varnish (5% NaF, Duraphat®, Colgate Oral Pharmaceuticals, New York, New York,
USA, positive control) and G4 = Negative control (MilliQ® water). The specimens
were maintained in 100% humidity until the beginning of the experiment. A sample
size of 10 specimens for each group was calculated by using BioEstat software
version 5.3 (Mamirauá Maintainable Development Institute, Belém, Pará, Brazil)
considering an error level of 5% and b-error level of 20%, based on a previous study
(Alexandria, Meckelburg et al. 2015).
Treatment and erosive challenge
The first treatment was performed at the beginning of the experiment; the
varnishes were applied once as a thin layer on the specimen`s surface using a
microbrush. The specimens were immersed in artificial saliva for 6h, after that, the
layer was removed using a scalpel blade and acetone with water (1:1), and then the
total removal was checked microscopically (40x magnification).
All samples were first subjected to erosion cycles for 3 days; 4 erosion
immersions were performed per day for 5 minutes each, using freshly opened
bottles of Sprite Zero (Coca-Cola Company, Porto Real, Rio de Janeiro, Brazil), pH
2.58, 30ml/specimen. After each erosion period, samples were rinsed in MilliQ®
water. Among the cycles, the samples were immersed in artificial saliva (1.5mmol/L
Ca, 0.9mmol/L P, 150mmol/L KCl, 0.05mg F/mL in 0.1mol/L Tris buffer, pH 7.0,
30ml/sample) (Nassur, Alexandria et al. 2013).
After 3 days of erosion cycles, the specimens were prepared for a new
erosive cycle in which the exposed area (right side of the specimens’ surface) was
divided into two areas: the ‘down’ side was protected with a layer of acid-resistant
nail varnish (exposed area 1), and the ‘up’ side of this area received a new treatment
(exposed area 2), according to allocation groups, and was submitted to a new, 3-
day erosion cycle.
19
Enamel loss measurement and roughness analysis
A chromatic confocal sensor with a white light axial of 3D, non-contact optical
profilometer scanned an area of 1 x 1mm on each specimen (velocity of 2μ/s), which
was then analysed by Nanovea Professional 3D software (Nanovea PS50 Optical,
NANOVEA Inc., Irvine, California, USA) to determine tooth structure loss (TSL) and
two parameters of surface roughness: linear roughness (Ra) and area roughness
(Sa) as described previously (Alexandria, Meckelburg et al. 2015).
The 3D non-contact profilometry technique was used to determine as primary
outcome: tooth structure loss, i.e., the gap between the experimental and control
areas in each group; and as secondary outcomes: surface roughness - linear
surface roughness and volumetric surface roughness. All comparisons between the
unexposed and exposed areas (exposed Area 1 or exposed Area 2) of enamel were
performed after the removal of the acid-resistant nail varnish.
The TSL was calculated from the step-height difference between the
unexposed and exposed enamel surfaces (exposed Area 1 or exposed Area 2) in
each block; three linear measurements were made involving the unexposed and
exposed areas. All measurements were done in triplicate, and the mean values were
used to represent the final result of the surface profile.
To determine Ra, three linear measurements in each area (unexposed or
exposed areas) on the enamel specimen were performed. The average of these
three line measurements was used to determine Ra1 (surface linear roughness in
unexposed area), Ra2 (surface linear roughness in exposed Area 1) and Ra3
(surface linear roughness in exposed Area 2); the Ra value after 3 days of erosion
for all groups was calculated: Ra = Ra2 – Ra1. The Ra value after 6 days of erosion
for all groups was calculated: Ra = Ra3 – Ra1.
Further on, three scanned areas (200µm × 200µm) were acquired for each
block in the unexposed and exposed areas. The average of these three areas was
used to determine Sa1 (surface roughness in unexposed area), Sa2 (surface
roughness in exposed Area 1) and Sa3 (surface roughness in exposed Area 2); the
20
Sa value after 3 days of erosion for all groups was calculated as: Sa = Sa2 – Sa1.
The Sa value after 6 days of erosion for all groups was calculated: Sa = Sa3 – Sa1.
Scanning electron microscopy (SEM) analysis and 3D profilometry images
Three enamel blocks of each group were randomly selected and prepared
for SEM analysis with a scanning electron microscope (6460LV, JEOL, Akishima,
Tokyo, Japan). The blocks were covered with a 30-µm gold layer and fixed on stubs
with double-faced carbon tape. The topography of enamel specimens was analysed
in backscattered electrons at 20kV in low vacuum mode (45Pa). The
photomicrographs were acquired under 500x magnification to observe
morphological changes at the interface among the three areas (unexposed,
exposed Area 1 and exposed Area 2); and 1000x magnification.
The 3D topographical images (schemes and graphics) were generated from
specimens using Nanovea Professional 3D software (Nanovea PS50 Optical,
NANOVEA Inc., Irvine, California, USA); one scheme and two graphics were chosen
to better represent the results. The schematic design of the experimental protocol is
shown in Figure 1.
Statistical analysis
The normal distribution of data was checked for all of the tested variables,
using Shapiro-Wilk's test. Differences in the Ra and Sa among treatments were
tested using one-way ANOVA following by a Tukey test. Differences in TSL among
treatments were tested using a one-way Mann-Whitney test. Comparison between
TSL after erosion and TSL after progression inside of treatment groups were made
by a paired T-test. SPSS software version 22.0 (IBM, New York, New York, USA)
was used for statistical analysis. The significance level was set at 5%. The SEM
photomicrographs and the 3D schemes and graphics generated by the profilometer
were evaluated descriptively.

21
Results
Table 1 summarizes the profilometry results for TSL, Ra, Sa and after the
first erosion (3rd day of erosion) and Table 2 shows the results for the same
parameters after progressive erosion (6 days of erosion).
After 3 days of erosion, all varnishes had a protective effect against erosion
because all of them statistically differed from the negative control (p < .05) for TSL.
The specimens of G1 (6.26μm) had statistically lower values for TSL than G4
(14.08μm, p = .0001) and G3 (10.32μm, p = .025). TSL for G2 (9.89μm) did not
show diffrences from other varnishes groups (p > .05 and p = .149, for G1 and G2,
respectively). However, after varnish re-application and 3 days of erosion (6 days in
total) all treatment groups resulted in protection against TSL in comparison with the
negative control (p = .001 for G1 and G2; p = .004 for G3).
Although not statiscally significant among them (p > .05), G1, G2 and G3 had
less alterations in topographic roughness (Ra and Sa results) compared to the
negative control (G4; p < .05) after 3 or 6 days of erosion.
All groups had a significant increase in surface roughness after 3 days and 6
days of experiment; these results were evident when examining the SEM
photomicrographs (Figures 2 and 3) and 3D topographical images (Figure 4). The
higher differences between unexposed and exposed areas were observed for G4,
in fact, this result was more expressive than in other groups, while small differences
were seen for G1 (Figures 2 and 4). In G2 and G3, there was a similarity of erosion
patterns with irregularities, exposure of enamel prisms, and depressions on surface
enamel after 3 and 6 days of erosion. In G1, exposure of enamel prisms was more
pronounced after 6 days of erosion. In exposed areas of G4, we observed the
greatest alterations in enamel topography, with extensive depressions, craters and
exposure of enamel prisms (Figure 3).
Discussion

22
To the best of the authors knowledge, this is the first study to assess the
protective effect of varnishes containing fluoride with or without calcium or xylitol in
preventing the enamel erosion and progression of the lesion. We observed that the
addition of CPP-ACP in fluoride varnish had a positive effect and protected against
TSL after 3 days of erosion.
Dental erosion causes a chemical wear of dental hard tissue by acids without
bacterial involvement (Shellis, Barbour et al. 2013, Lussi and Carvalho 2014), and
it is an increasing problem in the world (Kreulen, Van 't Spijker et al. 2010, Salas,
Nascimento et al. 2015). Thus, investigations of preventive methods that reduce
erosion and progression of dental erosion is very important to minimize the
consequences to the oral cavity (Mohammed and Dusara 2013, Lussi and Carvalho
2015). Because of its common clinical use, adherence to teeth and high
concentration of fluoride with slow release, varnishes could be an ideal product to
protect against dental erosion (Lippert 2014, Sar Sancakli, Austin et al. 2015).
After 6 days of erosion, TSL pregressed, irrespective of treatment groups. In
fact, all had same capacity to protect against progressive erosion. The enamel
surface of CPP-ACP + NaF varnish group showed slight superficial erosion, when
comparing the SEM photomicrographs and 3D images of other groups; the greater
differences between unexposed and exposed areas were observed for negative
control. So, considering all results together, the first null hypothesis was partially
rejected: the presence of CPP-ACP improved the effect of NaF varnish and
prevented TSL after 3 days of dental erosion.
Additionally, the specimens treated with CPP-ACP + NaF, xylitol + NaF and
NaF varnishes had fewer changes in surface roughness values than the negative
control after 3 and 6 days of erosion, exhibiting equivalent competence to reduce
enamel roughness alterations after erosion challenges; thus, the second null
hypothesis was accepted. By examining the SEM photomicrographs and 3D
topographical images it was possible to observe that the group treated with CPP-
ACP + NaF presented the least alterations on the eroded surface. Furthermore, for
this group the exposure of enamel prisms was more pronounced after 6 days of
erosion. In images of xylitol + NaF varnish group and NaF group, the irregularities,
exposure of enamel prisms, and depressions in exposed areas were more
23
pronounced than in CPP-ACP + NaF varnish group; but in negative control group,
the greatest alterations appeared on the eroded enamel topography, which showed
a destructive aspect, including evident irregularities and porosities.
Although the CPP-ACP and xylitol products have being related to de-
remineralization process, little is known about the anti-erosive effect of CPP-ACP or
xylitol varnishes. In our study, the products presented the same fluoride
concentration. From this observation, we aimed to evaluate if the addition of CPP-
ACP or xylitol in NaF varnishes could offer a better effect than NaF varnish to
prevent against erosion process in sound enamel or in previously eroded enamel
(progression of erosion).
Souza et al. (Souza, Rochel et al. 2010) analysed the effects of applying 10%
or 20% xylitol varnishes or solutions and 5% NaF varnish or solution under soft drink
erosion after 5 and 10 days (a total of 60 min of erosion in 10 days). They concluded
that after 5 days, NaF, xylitol varnishes and the 20% xylitol solution reduced the
enamel loss and, after reapplication and 5 more days of erosive challenge, only
xylitol varnishes significantly reduced the enamel erosion. We also observed good
results for the groups treated with NaF varnish and xylitol + NaF varnish; it had a
preventive effect after 3 or 6 days of erosion, even in the face of severe erosion.
Amaechi et al. (Amaechi, Higham et al. 1998) and Chunmuang et al.
(Chunmuang, Jitpukdeebodintra et al. 2007) evaluated the effect of
supplementation of orange juice with xylitol, fluoride, and xylitol with fluoride,
combined. They immersed enamel samples in these orange juice samples modified
with xylitol and evaluated if any alteration happened to the enamel surface. Both
studies concluded that the combination of xylitol and fluoride in an orange juice
supplement has an additive effect in the reduction of dental erosion. It might be
speculated that the xylitol can act as a calcium ion transporter, lowering the loss of
calcium and phosphate from the teeth (Miake, Saeki et al. 2003, Makinen 2010). In
our study, the addition of xylitol to NaF varnish did not significantly benefit the NaF
varnish and help to protect from dental erosion. In researched literature, we did not
find studies that evaluated the action of xylitol varnish in dental erosion.
24
However, the addition of CPP-ACP to fluoride varnish contributed
significantly to better results, preventing enamel loss after 3 days of erosion. This
was probably because of the high concentration of bioavailable calcium and
inorganic phosphate ions present in the CPP-ACP + NaF varnish product (Reynolds
2009, Cochrane, Shen et al. 2014).
In the examined literature, only studies with CPP-ACP mousse or chewing
gum products were found. The majority of these research studies show good results
in favour of RecaldentTM (Poggio, Lombardini et al. 2009, Turssi, Maeda et al. 2011,
Prestes, Souza et al. 2013, Rallan, Chaudhary et al. 2013, de Alencar, Magalhaes
et al. 2014, Wang, Huang et al. 2014). Considering the use of RecaldentTM
technology, independent of the vehicle utilized, the present results are in agreement
with Poggio et al. (Poggio, Lombardini et al. 2009) and Wang et al. (Wang, Huang
et al. 2014); both studies evaluated a CPP-ACP mousse to prevent dental erosion.
The authors observed that the group treated with CPP-ACP had lower roughness
values than the control group.
Rallan et al. (Rallan, Chaudhary et al. 2013) assessed the effects of CPP-
ACP, CPP-ACFP and fluoridated toothpaste in enamel treatment samples after a
soft drink erosion―using cola―for 3 days. They observed that all treatments had
good microhardness results when compared with the control (without treatment),
but the samples treated with CPP-ACFP showed the best results. Turssi et al.
(Turssi, Maeda et al. 2011) also investigated the effect of CPP-ACP, CPP-ACFP
and fluoridated toothpaste after citric acid erosion, and they concluded that CPP-
ACFP showed results equal to the fluoride dentifrice. Despite this, we evaluated the
preventive effect and our results showed that CPP-ACP + NaF varnish was better
than NaF varnish alone after 3 days of erosion, corroborating Rallan et al. (Rallan,
Chaudhary et al. 2013) results.
Probably the presence of CPP-ACP in NaF varnish promoted mineral
precipitation in enamel, preventing against 3 days of erosion in soft drink, and,
although we had used the CPP-ACP product in varnish form, our results are in
accordance with Prestes et al. (Prestes, Souza et al. 2013) and de Alencar et al. (de
Alencar, Magalhaes et al. 2014) that evaluated in situ the good effect of a

25
commercial CPP-ACP chewing gum on initial erosion lesions. Both observed that
CPP-ACP chewing gum improved the mineral precipitation of eroded enamel.
The combination of CPP-ACP with fluoride gave the solution capability to
prevent enamel erosion: the delivers of calcium and phosphate ions with fluoride
ions at the enamel surface build fluor(hydroxy)apatite crystals, which are more
resistant to dissolution by acids (Wang, Megert et al. 2011). The present study
confirms these findings since the presence of CPP-ACP increased fluoride’s
capacity to prevent the loss of dental hard tissue after 3 days of acidic erosion.
Nevertheless, in view of the conflicting results in literature concerning
prevention of dental erosion and the absence of studies in researched literature
testing the action of CPP-ACP + NaF and xylitol + NaF varnishes on enamel after
such an erosion challenge, we emphasize the need for further in situ and in vivo
research to establish full conclusions about the role of CPP-ACP and xylitol
varnishes in preventing erosive tooth wear.
The application of topical NaF varnishes was effective in reducing enamel
roughness after erosion or progression of erosion, independent of the added
compound (CPP-ACP or xylitol). Additionally, the presence of CPP-ACP improved
the performance of NaF varnish in protecting against tooth structure loss after 3
days of erosion. These findings provided a basis for future in situ studies and clinical
trials that will determine the effect of CPP-ACP + NaF varnish in preventing clinical
erosive tooth wear.
26
Table 1 – 3D non-contact profilometry results: median (min/max) of tooth structure loss (TSL) and mean ±SD of surface roughness (Ra and Sa) of enamel specimen groups after erosion challenge (3 and 6 days of erosion)
After 3 days of erosion After 6 days of erosion
Groups TSL Ra Sa TSL Ra Sa
G1 (CPP-ACP +
NaF varnish)
6.26 (4.05/9.28) A, b 0.38 ± 0.13 a 0.27 ± 0.04 a 10.88 (8.20/19.61) B, a 0.51 ± 0.08 a 0.36 ± 0.12 a
G2 (xylitol + NaF
varnish)
9.89 (8.14/13.72) A, a, b 0.43 ± 0.19 a 0.32 ± 0.15 a 10.57 (6.20/13.92) B, a 0.54 ± 0.12 a 0.44 ± 0.20 a
G3 (NaF varnish) 10.32 (17.24/9.50) A, a 0.45 ± 0.12 a 0.28 ± 0.14 a 12.54 (10.25/16.19) A, a 0.50 ± 0.11 a 0.42 ± 0.10 a
G4 (negative
control)
14.06 (26.80/10.61) A, c 1.02 ± 0.22 b 0.85 ± 0.17 b 19.42 (13.82/26.80) B, b 1.25 ± 0.30 b 1.14 ± 0.41 b
Means followed by distinct letters are statistically different (p < .05). Capital letters show difference between TSL after erosion and TSL after progression of erosion inside each group (paired T-test) and lower case letters in the same column show differences among treatments (one-way Mann-Whitney test for TSL and one-way ANOVA followed by Tukey test for Ra and Sa).

27
Figure 1. Schematic design of the experimental protocol.
28
Figure 2. Surface SEM photomicrographs of enamel samples after treatment and erosion challenge at 500x magnification. (A) G1 = CPP-ACP + NaF (MI varnishTM), (B) G2 = xylitol + NaF (Profluorid®), (C) G3 = NaF varnish (Duraphat®, positive control) and (D) G4 = MilliQ® water (negative control). Area 1 = the unexposed area (sound enamel), Area 2 = exposed area 1 (after 3 days of erosion) and Area 3 = exposed Area 2 (after 6 days of erosion and progression of erosion).

29
Figure 3. Surface SEM photomicrographs of enamel samples after treatment and erosion challenge at 1000x magnification. (A) G1 = CPP-ACP + NaF (MI varnishTM), (B) G2 = xylitol + NaF (Profluorid®), (C) G3 = NaF varnish (Duraphat®, positive control) and (D) G4 = MilliQ® water (negative control). Photomicrographs I = exposed Area 1 (after 3 days of erosion) and Photomicrographs II = exposed Area 2 (after 6 days of erosion and progression of erosion).

30
Figure 4. 3D profilometry scheme and graphic representation of enamel surface samples after treatment and erosion challenge (after 3 and 6 days of erosion) for each group. (A) G1 = CPP-ACP + NaF (MI varnishTM), (B) G2 = xylitol + NaF (Profluorid®), (C) G3 = NaF varnish (Duraphat®, positive control) and (D) G4 = MilliQ® water (negative control). Arrow 1 = the unexposed area (sound enamel), Arrow 2 = exposed Area 1 (after 3 days of erosion) and Arrow 3 = exposed Area 2 (after 6 days of erosion and progression of erosion). Graphic I = profile of unexposed area to exposed Area 1, Graphic II = profile of unexposed area to exposed Area 2.
31
References
Alexandria AK, Meckelburg NA, Puetter UT, Salles JT, Souza IPR, Maia LC: Do
pediatric medicines induce topographic changes in dental enamel? Braz Oral Res
2015;in press.
Amaechi BT, Higham SM, Edgar WM: The influence of xylitol and fluoride on dental
erosion in vitro. Arch Oral Biol 1998;43:157-161.
Chunmuang S, Jitpukdeebodintra S, Chuenarrom C, Benjakul P: Effect of xylitol and
fluoride on enamel erosion in vitro. J Oral Sci 2007;49:293-297.
Cochrane NJ, Shen P, Yuan Y, Reynolds EC: Ion release from calcium and fluoride
containing dental varnishes. Aust Dent J 2014;59:100-105.
de Alencar CR, Magalhaes AC, de Andrade Moreira Machado MA, de Oliveira TM,
Honorio HM, Rios D: In situ effect of a commercial cpp-acp chewing gum on the
human enamel initial erosion. J Dent 2014;42:1502-1507.
Kreulen CM, Van 't Spijker A, Rodriguez JM, Bronkhorst EM, Creugers NH, Bartlett
DW: Systematic review of the prevalence of tooth wear in children and adolescents.
Caries Res 2010;44:151-159.
Lippert F: Fluoride release from fluoride varnishes under acidic conditions. JCPD
2014;39:35-39.
Lussi A, Carvalho TS: Erosive tooth wear: A multifactorial condition of growing
concern and increasing knowledge. Monogr Oral Sci 2014;25:1-15.
Lussi A, Carvalho TS: The future of fluorides and other protective agents in erosion
prevention. Caries Res 2015;49 Suppl 1:18-29.
Magalhaes AC, Wiegand A, Rios D, Buzalaf MA, Lussi A: Fluoride in dental erosion.
Monogr Oral Sci 2011;22:158-170.

32
Makinen KK: Sugar alcohols, caries incidence, and remineralization of caries
lesions: A literature review. Int J Dent 2010;2010:981072.
Miake Y, Saeki Y, Takahashi M, Yanagisawa T: Remineralization effects of xylitol
on demineralized enamel. J Elect Micro 2003;52:471-476.
Mohammed A, Dusara K: What is the role of topical fluoride application in preventing
dental erosion? EBD 2013;14:59-62.
Nassur C, Alexandria AK, Pomarico L, de Sousa VP, Cabral LM, Maia LC:
Characterization of a new tif(4) and beta-cyclodextrin inclusion complex and its in
vitro evaluation on inhibiting enamel demineralization. Arch Oral Biol 2013;58:239-
247.
Poggio C, Lombardini M, Dagna A, Chiesa M, Bianchi S: Protective effect on enamel
demineralization of a cpp-acp paste: An afm in vitro study. J Dent 2009;37:949-954.
Prestes L, Souza BM, Comar LP, Salomao PA, Rios D, Magalhaes AC: In situ effect
of chewing gum containing cpp-acp on the mineral precipitation of eroded bovine
enamel-a surface hardness analysis. J Dent 2013;41:747-751.
Rallan M, Chaudhary S, Goswami M, Sinha A, Arora R, Kishor A: Effect of various
remineralising agents on human eroded enamel of primary teeth. European archives
of paediatric dentistry : official journal of the European Acad Paed Dent
2013;14:313-318.
Reynolds EC: Casein phosphopeptide-amorphous calcium phosphate: The
scientific evidence. Adv Dent Res 2009;21:25-29.
Reynolds EC, Cai F, Cochrane NJ, Shen P, Walker GD, Morgan MV, Reynolds C:
Fluoride and casein phosphopeptide-amorphous calcium phosphate. J Dent Res
2008;87:344-348.

33
Salas MM, Nascimento GG, Huysmans MC, Demarco FF: Estimated prevalence of
erosive tooth wear in permanent teeth of children and adolescents: An
epidemiological systematic review and meta-regression analysis. J Dent
2015;43:42-50.
Sar Sancakli H, Austin RS, Al-Saqabi F, Moazzez R, Bartlett D: The influence of
varnish and high fluoride on erosion and abrasion in a laboratory investigation. Aust
Dent J 2015;60:38-42.
Shellis RP, Barbour ME, Jesani A, Lussi A: Effects of buffering properties and
undissociated acid concentration on dissolution of dental enamel in relation to ph
and acid type. Caries Res 2013;47:601-611.
Souza JG, Rochel ID, Pereira AF, Silva TC, Rios D, Machado MA, Buzalaf MA,
Magalhaes AC: Effects of experimental xylitol varnishes and solutions on bovine
enamel erosion in vitro. J Oral Sci 2010;52:553-559.
Turssi CP, Maeda FA, Messias DC, Neto FC, Serra MC, Galafassi D: Effect of
potential remineralizing agents on acid softened enamel. Am J Dent 2011;24:165-
168.
Vongsavan K, Surarit R, Rirattanapong P: The combined effect of xylitol and fluoride
in varnish on bovine teeth surface microhardness. Southeast Asian J Trop Med
Public Health 2014;45:505-510.
Wang CP, Huang SB, Liu Y, Li JY, Yu HY: The cpp-acp relieved enamel erosion
from a carbonated soft beverage: An in vitro afm and xrd study. Arch Oral Biol
2014;59:277-282.
Wang X, Megert B, Hellwig E, Neuhaus KW, Lussi A: Preventing erosion with novel
agents. J Dent 2011;39:163-170.
34
4.2. Artigo 2 - Enamel erosion and abrasion-inhibiting effect of NaF fluoride
varnishes with or without CPP-ACP or xylitol
Adílis Kalina Alexandria1
Thiago Isidro Vieira1
Matheus Melo Pithon2
Tatiana Kelly da Silva Fidalgo1
Ana Maria Gondim Valença3
Lúcio Mendes Cabral4
Lucianne Cople Maia1
1 Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Federal
University of Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil
2 Department of Healthy, State University of Southwest Bahia (UESB), Jequié, BA,
Brazil
3 Department of Clinical and Social Dentistry, School of Dentistry, Federal
University of Paraiba (UFPB), João Pessoa, PB, Brazil
4 School of Pharmacy, Federal University of Rio de Janeiro (UFRJ), Rio de Janeiro,
RJ, Brazil
Short title: Inhibition of tooth erosion and abrasion by varnishes
Corresponding author:
Lucianne Cople Maia
Disciplina de Odontopediatria da FO-UFRJ, Caixa Postal: 68066 – Cidade
Universitária – CCS, CEP: 21941-971 - Rio de Janeiro – RJ –Brazil, Fax/phone:
+5521 39382101, e-mail: [email protected]

35
Abstract
The aim of this study was investigate the erosion and abrasion inhibiting
effect of NaF fluoride varnishes with or without CPP-ACP or Xylitol. Methods: Bovine
enamel samples were exposed to the following treatments: NaF varnish
(Duraphat®); NaF + CPP-ACP varnish (MI varnishTM); NaF + Xylitol (Profluorid®) or
MilliQ® water (negative control). The samples were divided (n=10) according to the
following treatments. Four cycles/day of erosion= 5 minutes in Sprite Zero and two
cycles of abrasion/day= 750 strokes (soft brushes, 200 g loading in placebo
dentifrice) after the first and the last erosive cycle. This challenge lasted for 3 days.
Among the cycles and after the last daily cycle, the specimens remained in artificial
saliva. The change in the enamel surface was evaluated by using 3D non-contact
optical profilometry with surface roughness and tooth structure loss (TSL)
measurements. Scanning electron microscopy (SEM) was used to assess enamel
topographic characteristics. Differences in the Ra, Sa and TSL among treatments
were tested using one-way Analysis of Variance (ANOVA) followed by the post-hoc
test (Tukey’s test); the significance level was set at 5%. All varnishes showed better
results for surface roughness measurements than the negative control (p=0.0001)
but there was no difference among the varnishes. NaF + CPP-ACP varnish group
had statistically fewer TSL than NaF varnish group (p=0.002), NaF + Xylitol varnish
group (p=0.007) and the negative control group (p=0.0001). A single-application of
topical varnishes was effective in reducing enamel wear and the presence of CPP-
ACP positively influenced the performance of NaF varnish against enamel loss from
erosion-abrasion.
Keywords: Tooth erosion, tooth abrasion, fluoride, CPP-ACP, xylitol

36
Introduction
Dental erosion is defined as a loss of tooth tissue by exogenous or
endogenous acids without bacterial involvement (Mahoney and Kilpatrick 2003,
Huysmans, Chew et al. 2011). The erosive challenge induces mineral dissolution of
prism and interprismatic enamel. Acid attack leads to the irreversible loss of dental
hard tissue accompanied by a progressive softening of the superficial and near-
surface layer of enamel (Huysmans, Chew et al. 2011, Shellis, Barbour et al. 2013,
Lussi and Carvalho 2014, Lussi and Carvalho 2015). The softening surface turns
less resistant, increasing the susceptibility to physical wear such as toothbrush
abrasion (Rios, Honorio et al. 2006, Ganss, Lussi et al. 2014). The application of
high concentrations of fluoride, especially varnish formulations, has been described
to decrease the development of tooth enamel erosion and increase abrasion
resistance (Lippert 2014, Sar Sancakli, Austin et al. 2015).
Xylitol has been used as a non-acidogenic sweetener in food (Makinen 2010)
and the addition of xylitol in dental products might be considered due its ability to
form complexes with calcium ions (Miake, Saeki et al. 2003, Makinen 2010), to
enhance remineralisation (Miake, Saeki et al. 2003) and to inhibit the dissolution of
calcium and/or phosphate ions from enamel structure (Chunmuang,
Jitpukdeebodintra et al. 2007, Vongsavan, Surarit et al. 2014).
Casein Phosphopeptide-Amorphous Calcium Phosphate Nanocomplexes
(CPP-ACP) is the RecaldentTM technology based on amorphous calcium phosphate
(ACP) stabilized by casein phosphopeptides (CPP). The benefits of CPP-ACP
nanocomplexes are the high concentration of calcium and phosphate ions that
promote enamel remineralisation. In the presence of fluoride ions, there is the
production of an ACFP phase, (CPP-ACP addicted with fluoride ion) and the
availability of fluoride ions contributes to remineralisation (Cross, Huq et al. 2005,
Reynolds, Cai et al. 2008).
However, to date, in researched literature there are no studies evaluating the
potential of CPP-ACP + NaF or xylitol + NaF varnishes with regard to preventing
erosion and abrasion. The null hypothesis of this study was the presence of CPP-

37
ACP or xylitol does not improve the effect of NaF varnish in preventing alterations
in roughness and tooth structure loss after an erosion and abrasion challenge.
Materials and Methods
Specimen preparation
Bovine teeth were prepared to obtain 40 enamel samples (4x4x2 mm). The
specimens were cut using an Isomet low-speed saw cutting machine (Buehler Ltd.,
Lake Bluff, Illinois, United States) with two diamond discs (Extec Corp., Enfield,
Connecticut, United States), which were separated by a 4 mm-thick pacer. The
block surfaces were polished using water-cooled silicon carbide paper 600 and 1200
(Extec Corp., Enfield, Connecticut, United States), followed by a 1-µm diamond
abrasive slurry (Extec Corp., Enfield, Connecticut, United States). After each stage
of polishing, the samples were cleaned in an ultrasonic device with MilliQ® water
for 5 min.
Baseline profile and groups allocation
Baseline surface microhardness (SMH) was obtained using a microhardness
tester (Buehler, MICROMET 5104, 679-MIT4-00335, Yokohama, Kanagawa,
Japan) with a Knoop diamond (50 g, 5 s, 5 indentations spaced 100 µm). The
baseline average values were: SMH= 389.71 ± 38.97 kg/mm2; Ra= 0.17 ± 0.017 μm
and Sa= 0.40± 0.04 μm. The enamel blocks were randomly allocated to the following
groups (n=10): G1= NaF varnish (5% NaF, Duraphat®, Colgate Oral
Pharmaceuticals, New York, New York, United States); G2= CPP-ACP + NaF
varnish (2% CPP-ACP and 5% NaF, MI varnishTM, GC America, Alsip, Illinois,
United States); G3= Xylitol + NaF varnish (1% xylitol and 5% NaF, Profluorid®,
Voco, Cuxhaven, Niedersachsen, Germany); and G4= MilliQ® water (negative
control). A sample size of 10 specimens was calculated considering an error level
of 5% and study power level of 80% based on a pilot study.
38
Experimental protocols
Half of the surface of the specimens was covered with acid-resistant nail
varnish in order to create an unexposed area (right side of enamel surface, sound
area) and the other exposed area (left side) was used for the treatment according
to the group.
The varnishes were applied once in a thin layer using a microbrush; after
treatment, the specimens were immersed in artificial saliva for 6 h (Fernandez,
Tenuta et al. 2014). The artificial saliva consisted of 1.5 mmol/L Ca, 0.9 mmol/L P,
150 mmol/L KCl, and 0.05 mg F/mL in 0.1 mol/L Tris buffer, pH 7.0 (Nassur,
Alexandria et al. 2013). Then, the varnish was removed using a scalpel blade and
acetone with water (1:1); total removal was confirmed using a microscope (40X
magnification).
All specimens were submitted to 3-day of erosion/abrasion cycles: the
erosion was performed with freshly opened bottles of Sprite Zero (Coca-Cola
Company, Porto Real, RJ, Brazil, pH 2.58, 30 ml/specimen), 4 times daily, for 5
minutes each. After the erosion protocol, the specimens were rinsed in MilliQ® water
for 5 s, before being immersed in artificial saliva (pH 7.0, 30 ml/specimen) for 2 h.
The artificial saliva solution was replaced daily by fresh solution in order to avoid
oversaturation. The experiment was carried out at 37ºC.
The specimens were also abraded using a mechanical toothbrush machine
(Buehler Ltd., Lake Bluff, Illinois, United States) and fresh slurries (0.5
mL/specimen) of a non-fluoridated toothpaste (Bitufo®, Itupeva, São Paulo, Brazil,
toothpaste/water ratio 1:3) for 15 s (50 strokes/s), with a weight of 200 g. The
abrasion was performed twice daily, after the first and last erosive challenge. After
abrasion, the specimens were rinsed with MilliQ® water for 5 s and transferred into
artificial saliva. After the last daily erosive immersion, the specimens were stored in
artificial saliva overnight.

39
3D non-contact profilometry analysis
The surface topography of the specimens was analysed by the 3D non-
contact chromatic confocal optical profilometry (Nanovea PS50 Optical, NANOVEA
Inc., Irvine, California, United States). The measurements of capture were
performed with a chromatic confocal sensor with a white light axial source, a scan
velocity of 2 μ/s and a refraction index of 10,000. After each experiment, an area of
1mm x 1mm was obtained in the centre of the samples in the same way as at the
baseline measurement. The 3D non-contact profilometry technique was used to
determine: i) surface roughness (linear - Ra; and volumetric - Sa) at baseline (1)
and after treatment (2); and ii) tooth structure loss (TSL) after treatment (Alexandria,
Meckelburg et al. 2015).
For Ra (ISO 4287) estimation, three linear horizontal measurements (500
μm) were taken in experimental area; the average of these three measurements
was used to determine Ra in moments 1 and 2 (surface linear roughness in the
baseline and experimental window, respectively); the Ra value for all groups was
calculated as: Ra = Ra2 – Ra1 (final wear – baseline wear). For Sa (ISO 25178),
three scan areas (250 µm × 250 µm) were acquired and the average was used to
determine Sa. As for Ra, the Sa value for all groups was calculated as Sa = Sa2 –
Sa1 (final wear – baseline wear).
The differences in height between the unexposed (baseline) and exposed
enamel surface (treated) in each group, following removal of the acid-resistant tape,
were defined as tooth structure loss. Three profile measurements (1 mm) were
taken involving the unexposed and exposed areas; the depth of the height between
both areas was measured in µm, with the average expressed as the TSL value for
each group.
The values for Ra, Sa and TSL in μm were calculated using the Nanovea
Professional 3D software, and the final average for each variable per specimen was
used for statistical analysis.

40
Scanning Electron Microscopy (SEM) analysis
Three enamel blocks of each group were randomly selected and prepared
for SEM analysis in a Scanning Electron Microscope (6460LV, JEOL, Tokyo,
Japan). The blocks were fixed on stubs with double-faced carbon tape and covered
with a 30-µm gold layer; the SEM analysis was performed to assess the topography
of the enamel surface. The specimens were examined with the same scanning
electron microscope operating at 20 kV in low vacuum mode (45 Pa) and analysing
the backscattered electrons (BSE). Initially, the specimens were analysed with
panoramic vision (500X) to observe the interface between the windows (sound and
experimental); photomicrographs of the most representative areas of each group
were obtained with magnification of 1000X to observe any changes in detail.
Statistical analysis
The normal distribution of data was assessed for all of the tested variables,
using the Shapiro Wilk’s tests. Differences in the Ra, Sa and TSL among treatments
were tested using one-way Analysis of Variance (ANOVA) followed by a post-hoc
test (Tukey’s test). SPSS software version 22.0 (IBM, New York, New York, United
States) was used for statistical analysis. The significance level was set at 5%.
Results
After erosion/abrasion challenge, all groups had a significantly higher surface
roughness after 3 days of the experiment (Figure 1 and 2). The results of 3D non-
contact profilometry are summarised in Table 1, with mean ± SD values for Ra, Sa
and TSL for all groups.
Regarding the surface roughness alterations, all varnish groups were
statistically superior to the negative control (p=0.0001). Furthermore, they did not
statistically differ between them for Ra and Sa values (p>0.05).

41
The greatest inhibition of TSL occurred when specimens were treated with
CPP/ACP + NaF (7.09 ± 0.70 μm), which had statistically lower values for mineral
loss than NaF varnish (10.33 ± 1.36 μm, p=0.002), Xylitol + NaF (9.96 ± 0.41 μm,
p=0.007), and negative control (18.38 ± 3.32 μm, p=0.0001). NaF and Xylitol + NaF
varnishes were also statistically different from the negative control (p=0.0001), but
they did not differ between them (p=0.970). The differences in the extent of
treatment effect on the surface can be seen on the 3D topographical (Figure 1) and
SEM images (Figure 2).
In Figure 1, it is possible to observe that all groups had a change in surface
roughness after the experiment, but in G4, the loss of tooth structure was more
evident than in other groups. The same can be seen in the images obtained by SEM
analysis (Figure 2), in which the negative control showed the worst alterations in
enamel topography, with the worst loss of enamel structure also. The
photomicrographs of G1 and G3 revealed more porous enamel surfaces than in G2
images.
Discussion
The null hypothesis of this study was the presence of CPP-ACP or xylitol
does not improve the effect of NaF varnish in preventing alterations in roughness
and tooth structure loss after an erosion and abrasion challenge.
Regarding to surface roughness alterations (Ra and Sa values), all of the
tested varnishes were statistically significant better than the negative control,
showing an equal capacity for protection against surface roughness alterations.
However, numerically, a better effect in reducing the TSL depth was observed
for CPP-ACP + NaF compared to other varnishes and to the negative control. Xylitol
+ NaF and NaF varnishes showed the same capacity to reduce the TSL; both were
statistically different from the negative control.

42
So, the null hypothesis was partially rejected; the presence of CPP-ACP
improved the effect of NaF varnish in preventing TSL after erosion/abrasion
challenge, but, did not improve protection against surface roughness alterations.
The lower values of Ra, Sa and TSL were observed when compared to the
negative control group, confirming that the erosion-abrasion model utilised in this
study was able to promote in vitro effective erosion/abrasion on the enamel surface.
According to the searched literature, this study is the first showing an
evaluation of the effect of NaF varnish containing CPP-ACP or xylitol in enamel
topography with regard to roughness profile alterations and tooth enamel loss after
erosion/abrasion.
The eroded teeth are less resistant to physical wear such as toothbrush
abrasion (Ganss, Lussi et al. 2014) and after an erosion and abrasion challenge, an
irreversible loss of dental hard tissue occurs (Rios, Honorio et al. 2006). So, it is
important to study preventive methods to avoid the consequences of the erosion
and abrasion process, like alterations in tooth surface roughness and a loss of
dental tissue. The application of high concentrations of fluoride, especially varnish
formulations, has been related in the scientific literature (Lippert 2014, Sar Sancakli,
Austin et al. 2015).
Casein phosphopeptides can be extracted enzymatically from milk and
complexed with calcium and phosphate (Cross, Huq et al. 2005). The benefits of
CPP-ACP nanocomplexes are the stability and high concentration of bioavailable
calcium and phosphate ions that can be used for enamel remineralisation (Cross,
Huq et al. 2007). While the preventive and remineralising effects of CPP-ACP on
carious lesions having been extensively studied in the last few years, little is known
about the anti-erosive effect of CPP-ACP.
There is a consensus that fluoride products are capable of protecting enamel
against erosive/abrasive tooth wear (Wegehaupt and Attin 2010, Levy, Magalhaes
et al. 2012, Sar Sancakli, Austin et al. 2015). The positive results found in our study
can be explained by the formation of a protective CaF2-like layer on dental tissue by
topical fluoride application (Dijkman and Arends 1988, Fernandez, Tenuta et al.
2014). The CaF2-globules act as a physical barrier inhibiting the contact of acid with
43
the enamel and also act in the de-remineralisation process, since the formation of
fluoride reservoirs occurs that participate in inhibition of the demineralisation
process and the precipitation of fluor(hydroxy)apatite (Levy, Rios et al. 2014, Lippert
2014, Lussi and Carvalho 2015).
In contrast to the remineralisation process of dental caries, which occur
slowly and gradually on the subsurface of the lesion, the fluoride protection
mechanism against erosives/abrasives occurs by the inhibition of near-surface
demineralisation and by not remineralising the eroded enamel (Lussi and Carvalho
2014, Lussi and Carvalho 2015, Sar Sancakli, Austin et al. 2015).
The ability of fluoride products to prevent mineral loss depends of a number
of factors such as fluoride concentration, pH, and the frequency of application
(Cochrane, Shen et al. 2014). In our study, the formulations presented the same
fluoride concentration, type of fluoride salt, frequency of application (only once
before experiment) and similar pH values. It seems that CPP-ACP or xylitol
incorporation in NaF varnishes did not affect the performance in relation to enamel
roughness alterations. The abrasive cycles acted by flattening the softening eroded
surface; this flattening reduced the distance between peaks and valleys (Rios,
Honorio et al. 2006, Ganss, Lussi et al. 2014).
Chunmuang et al. (2007) evaluated the preventive erosion effect of xylitol
varnish with and without fluoride combination. They observed that xylitol/fluoride
(227 ppm F-) varnish reduced the enamel erosion, but did not differ from fluoride
varnish alone. Vongsavan et al. (2014) also showed that the combined effect of
xylitol and fluoride varnish was beneficial for preventing enamel demineralisation,
but was no better than fluoride varnish alone in vitro. It is important to emphasise
that these results are concerned only with erosion and nothing was found in the
dental literature about the associated effect of erosion + abrasion on dental enamel
tooth wear.
The mechanism of action of xylitol in the erosion process is probably the
ability to form complexes with calcium ions on the dental surface (Miake, Saeki et
al. 2003, Makinen 2010). The xylitol acts as a Ca++ carrier, delaying demineralisation
44
by lowering the dissolution of calcium and phosphate from the teeth (Makinen 2010,
Vongsavan, Surarit et al. 2014).
The potential of conventional fluorides, such as NaF varnish, to prevent the
erosive/abrasive process has been reported in the literature (Levy, Magalhaes et al.
2012, Levy, Rios et al. 2014, Lippert 2014). Nevertheless, there are controversial
findings about the preventive potential of CPP-ACP products against erosion and
abrasion.
Ranjitkar et al. (2009) evaluated the preventive effect of CPP-ACP mousse
without fluoride on enamel and dentine after erosion and toothbrush abrasion. They
observed that the CPP-ACP mousse significantly reduced enamel and dentine
wear. The authors confirmed that the wear reduction was because the presence of
calcium and phosphate ions and the lubrication potential of mousse ingredients.
Wegehaupt and Attin (2010) also investigated the effect of CPP-ACP mousse
without fluoride on the reduction of erosive/abrasive tooth wear, but in contrast to
the findings of Ranjitkar et al. (2009), no protective effect of CPP-ACP mousse was
observed. One reason for these contradictory findings might be the higher frequency
of treatment in the study by Ranjitkar et al. (2009); moreover, the erosive cycling in
the study by Wegehaupt and Attin (2010) was longer (20 days) than that of Ranjitkar
et al. (2009). According to the literature, there were no studies testing the effect of
CPP-ACP varnish against erosion/abrasion wear; therefore, the results of the
present study show the potential of CPP-ACP + NaF varnish to prevent TSL due to
acidic erosion and toothbrush abrasion. The high concentration of bioavailable
calcium and inorganic phosphate ions (Cross, Huq et al. 2005, Cross, Huq et al.
2007, Reynolds 2009, Cochrane, Shen et al. 2014) can increase its preventive
potential, allowing the reduction of structural loss.
It was possible to observe in 3D images and SEM images that all groups had
some alterations of surface topography after erosion/abrasion challenge. The
negative control specimens presented the most severely eroded areas; with
irregular patterns of enamel prisms and high wear depth. In experimental varnishes
groups, the images revealed a porous enamel surface with irregularities,
depressions and exposure of enamel prisms.

45
The use of a 3D no-contact profilometer was very advantageous because it
does not promote grooves on the surface of the samples, and is very sensitive and
specific (Attin 2006). Non-contact surface profilometry allowed the quantification of
tooth depth; these measures can be compared to the transverse microradiography
(gold standard) for the quantification of enamel changes in vitro (Elton, Cooper et
al. 2009). No previous investigations in the literature have evaluated the action of
CPP-ACP + NaF or Xylitol + NaF varnishes on enamel wear after erosion/abrasion
challenge using 3D non-contacting profilometry.
Under the conditions of this study, it was concluded that a single-application
of topical NaF varnishes was effective in reducing enamel wear and tooth structure
loss due to erosion-abrasion. Furthermore, the presence of CPP-ACP improved the
performance of NaF varnish, better protecting against tooth structure loss. These
findings provide a basis for future in situ studies and clinical trials that will determine
the effect of CPP-ACP + NaF varnish in preventing clinical erosive tooth wear.
Acknowledgements: The authors acknowledge the financial support from
CAPES, FAPERJ (E-26/201.316/2014) and CNPQ (302800/2012-3). This study is
part of the PhD thesis of the first author.
Disclosure Statement
The authors declare that there is no conflict of interest.
Role of authors
Conceived and designed the experiments: AKA, LCM, AMGV and LMC.
Performed the experiment: AKA, TIV, MMP and TKSF. Performed the analysis:
AKA. Analysed the data: AKA, AMGV and LCM. Wrote and revised the paper: AKA,
LCM, AMGV, LCM, TIV, MMP and TKSF.

46
Table 1 - Mean of surface roughness (Ra and Sa) and tooth structure loss (TSL) (±SD) of
enamel specimen groups.
3D non-contact profilometry results
Groups Ra Sa TSL
G1 (NaF varnish) 0.61 ± 0.09 a 0.56 ± 0.17 a 10.33 ± 1.36 b
G2 (CPP-ACP + NaF
varnish)
0.47 ± 0.05 a 0.44 ± 0.06 a 7.09 ± 0.70 a
G3 (xylitol + NaF
varnish)
0.55 ± 0.17 a 0.53 ± 0.10 a 9.96 ± 0.41 b
G4 (negative control) 0.92 ± 0.13 b 1.32 ± 0.52 b 18.38 ± 3.32 c
Means followed by distinct letters are statistically different (p<0.05).
47
Figure 1 - 3D profilometry scheme representation of surface of enamel samples after treatment and erosion/abrasion challenge. Left – sound window (unexposed area) and right – experimental window (exposed area). (A) G1= NaF varnish (Duraphat®) (B) G2= CPP-ACP + NaF (MI varnishTM), C) G3= Xylitol + NaF (Profluorid®) and D) G4= MilliQ® water (negative control).
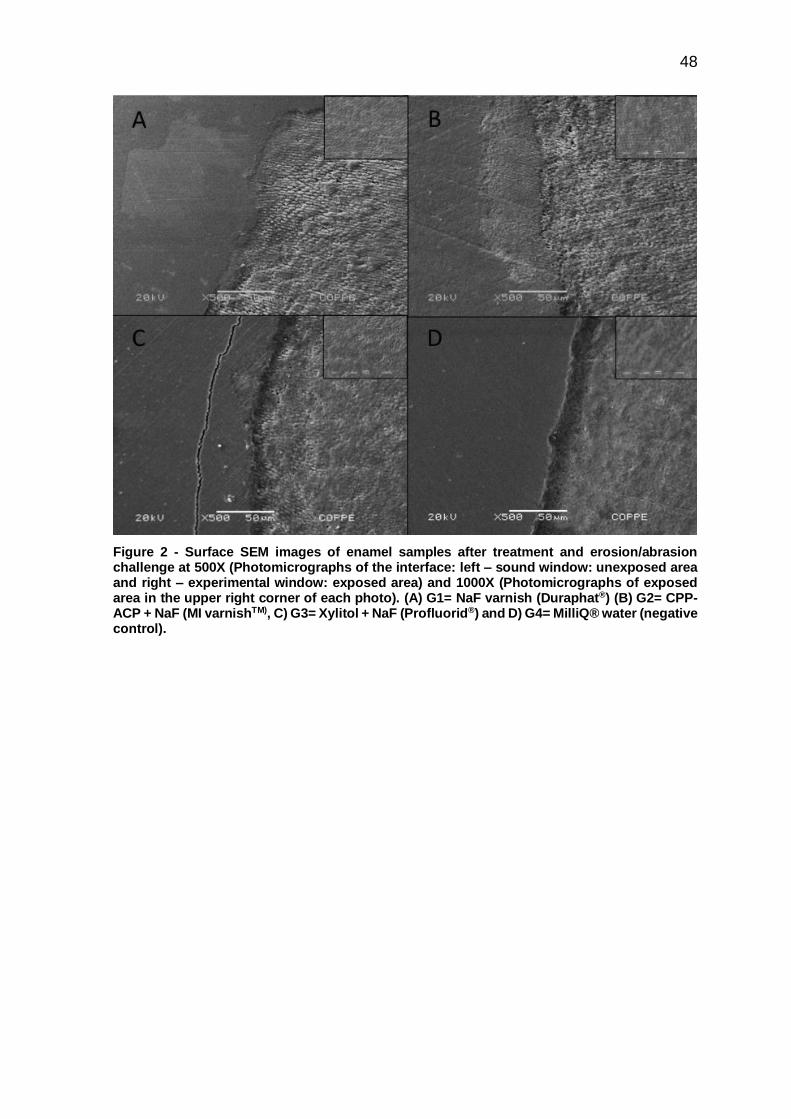
48
Figure 2 - Surface SEM images of enamel samples after treatment and erosion/abrasion challenge at 500X (Photomicrographs of the interface: left – sound window: unexposed area and right – experimental window: exposed area) and 1000X (Photomicrographs of exposed area in the upper right corner of each photo). (A) G1= NaF varnish (Duraphat®) (B) G2= CPP-ACP + NaF (MI varnishTM), C) G3= Xylitol + NaF (Profluorid®) and D) G4= MilliQ® water (negative control).

49
References
Alexandria AK, Meckelburg NA, Puetter UT, Salles JT, Souza IPR, Maia LC: Do
pediatric medicines induce topographic changes in dental enamel? Braz Oral Res
2015;in press.
Attin T: Methods for assessment of dental erosion. Monogr Oral Sci 2006;20:152-
172.
Chunmuang S, Jitpukdeebodintra S, Chuenarrom C, Benjakul P: Effect of xylitol and
fluoride on enamel erosion in vitro. J Oral sci 2007;49:293-297.
Cochrane NJ, Shen P, Yuan Y, Reynolds EC: Ion release from calcium and fluoride
containing dental varnishes. Aust Dent J 2014;59:100-105.
Cross KJ, Huq NL, Palamara JE, Perich JW, Reynolds EC: Physicochemical
characterization of casein phosphopeptide-amorphous calcium phosphate
nanocomplexes. J Biol Chem 2005;280:15362-15369.
Cross KJ, Huq NL, Reynolds EC: Casein phosphopeptides in oral health--chemistry
and clinical applications. Curr Pharm Des 2007;13:793-800.
Dijkman TG, Arends J: The role of 'caf2-like' material in topical fluoridation of enamel
in situ. Acta Odontol Scand 1988;46:391-397.
Elton V, Cooper L, Higham SM, Pender N: Validation of enamel erosion in vitro. J
Dent 2009;37:336-341.
Fernandez CE, Tenuta LM, Zarate P, Cury JA: Insoluble naf in duraphat(r) may
prolong fluoride reactivity of varnish retained on dental surfaces. Braz Dent J
2014;25:160-164.
Ganss C, Lussi A, Schlueter N: The histological features and physical properties of
eroded dental hard tissues. Monogr Oral Sci 2014;25:99-107.
Huysmans MC, Chew HP, Ellwood RP: Clinical studies of dental erosion and erosive
wear. Caries Res 2011;45 Suppl 1:60-68.

50
Levy FM, Magalhaes AC, Gomes MF, Comar LP, Rios D, Buzalaf MA: The erosion
and abrasion-inhibiting effect of tif(4) and naf varnishes and solutions on enamel in
vitro. J Clin Pediatr Dent 2012;22:11-16.
Levy FM, Rios D, Buzalaf MA, Magalhaes AC: Efficacy of tif4 and naf varnish and
solution: A randomized in situ study on enamel erosive-abrasive wear. Clin Oral
Investig 2014;18:1097-1102.
Lippert F: Fluoride release from fluoride varnishes under acidic conditions. JCPD
2014;39:35-39.
Lussi A, Carvalho TS: Erosive tooth wear: A multifactorial condition of growing
concern and increasing knowledge. Monogr Oral Sci 2014;25:1-15.
Lussi A, Carvalho TS: The future of fluorides and other protective agents in erosion
prevention. Caries Res 2015;49 Suppl 1:18-29.
Mahoney EK, Kilpatrick NM: Dental erosion: Part 1. Aetiology and prevalence of
dental erosion. N Z Dent J 2003;99:33-41.
Makinen KK: Sugar alcohols, caries incidence, and remineralization of caries
lesions: A literature review. Int J Dent 2010;2010:981072.
Miake Y, Saeki Y, Takahashi M, Yanagisawa T: Remineralization effects of xylitol
on demineralized enamel. J Electron Microsc 2003;52:471-476.
Nassur C, Alexandria AK, Pomarico L, de Sousa VP, Cabral LM, Maia LC:
Characterization of a new tif(4) and beta-cyclodextrin inclusion complex and its in
vitro evaluation on inhibiting enamel demineralization. Arch Oral Biol 2013;58:239-
247.
Ranjitkar S, Rodriguez JM, Kaidonis JA, Richards LC, Townsend GC, Bartlett DW:
The effect of casein phosphopeptide-amorphous calcium phosphate on erosive
enamel and dentine wear by toothbrush abrasion. J Dent 2009;37:250-254.
Reynolds EC: Casein phosphopeptide-amorphous calcium phosphate: The
scientific evidence. Adv Dent Res 2009;21:25-29.
51
Reynolds EC, Cai F, Cochrane NJ, Shen P, Walker GD, Morgan MV, Reynolds C:
Fluoride and casein phosphopeptide-amorphous calcium phosphate. J Dent Res
2008;87:344-348.
Rios D, Honorio HM, Magalhaes AC, Buzalaf MA, Palma-Dibb RG, Machado MA,
da Silva SM: Influence of toothbrushing on enamel softening and abrasive wear of
eroded bovine enamel: An in situ study. Braz Oral Res 2006;20:148-154.
Sar Sancakli H, Austin RS, Al-Saqabi F, Moazzez R, Bartlett D: The influence of
varnish and high fluoride on erosion and abrasion in a laboratory investigation. Aust
Dent J 2015;60:38-42.
Shellis RP, Barbour ME, Jesani A, Lussi A: Effects of buffering properties and
undissociated acid concentration on dissolution of dental enamel in relation to ph
and acid type. Caries Res 2013;47:601-611.
Vongsavan K, Surarit R, Rirattanapong P: The combined effect of xylitol and fluoride
in varnish on bovine teeth surface microhardness. Southeast Asian J Trop Med
Public Health 2014;45:505-510.
Wegehaupt FJ, Attin T: The role of fluoride and casein phosphopeptide/amorphous
calcium phosphate in the prevention of erosive/abrasive wear in an in vitro model
using hydrochloric acid. Caries Res 2010;44:358-363.

52
4.3. Artigo 3 – Do pediatric medicines induce topographic changes in dental
enamel under cariogenic challenge?
Adílis Kalina Alexandriaa
Nicolli de Araujo Meckelburgb
Ursula Tavares Puetterb
Jordan Trugilho Sallesb
Ivete Pomarico Ribeiro de Souzac
Lucianne Cople Maiac
a Doctoral student, Department of Pediatric Dentistry and Orthodontics, School of
Dentistry, Federal University of Rio de Janeiro, Rio de Janeiro, Rio de Janeiro,
Brazil
b Graduate student, Department of Pediatric Dentistry and Orthodontics, School of
Dentistry, Federal University of Rio de Janeiro, Rio de Janeiro, Rio de Janeiro,
Brazil
c Full Professor, Department of Pediatric Dentistry and Orthodontics, School of
Dentistry, Federal University of Rio de Janeiro, Rio de Janeiro, Rio de Janeiro,
Brazil
Corresponding author:
Lucianne Cople Maia
Disciplina de Odontopediatria da FO-UFRJ, Caixa Postal: 68066 – Cidade
Universitária – CCS, CEP: 21941-971 - Rio de Janeiro – RJ –Brazil
Fax/phone: +5521 25622098
E-mail: [email protected]

53
Abstract
The purpose of the present study was to evaluate the effect of common pediatric
liquid medicines on surface roughness and tooth structure loss and to evaluate the
pH values of these medicines at room and cold temperatures in vitro. Eighty-four
bovine enamel blocks were divided into seven groups (n=12): G1-Alivium®, G2-
Novalgina®, G3-Betamox®, G4-Clavulin®, G5-Claritin®, G6-Polaramine® and G7-
MilliQ® water (negative control). The pH was determined and the samples were
immersed in each treatment 3x/day for 5 min. 3D non-contact profilometry was used
to determine surface roughness (linear Ra, volumetric Sa) and the Gap formed
between treated and control areas in each block. Scanning electron microscopy
(SEM) and energy dispersive spectrometry (EDS) were also performed. The
majority of liquid medicines had pH ≤ 5.50. G1, G4, and G5 showed alterations in
Ra when compared with G7 (p<0.05). According to Sa and Gap results, only G5
was different from G7 (p<0.05). Alteration in surface was more evident in G5 SEM
images. EDS revealed high concentrations of carbon, oxygen, phosphorus, and
calcium in all tested groups. Despite the low pH values of all evaluated medicines,
only Alivium®, Clavulin®, and Claritin® increased linear surface roughness, and
only Claritin® demonstrated the in vitro capacity to produce significant tooth
structure loss.
Keywords: dental enamel, oral administration, pharmaceutical preparations,
acidity, topography.

54
Introduction
Medicines in liquid form are widely used for children because they facilitate
intake.1,2,3 However, some of the inactive agents used in pediatric liquid medications
can cause damage to dental tissues because of their low pH.3 Some medicines have
acid in their compositions in order to preserve their chemical stability and control
their tonicity.4
Certain properties of acidic products in general may be related to the loss of
surface structure of dental enamel: low endogenous pH, high titratable acidity, and
minimal quantities of minerals such as calcium or phosphate, in their
compositions.3,5,6,7,8 Acidic medications may cause dental erosion with loss of dental
tissue.1,4 Besides the presence of acids in some children’s medications, other factors
may also be related to changes in the surface morphology of dental enamel: high
frequency of medication intake, bedtime consumption, high viscosity, and reduction
in salivary flow.3,5
Many oral liquid medicines are usually recommended for sick children for long
periods, and in cases of chronic diseases, they are administered daily. In vitro
studies have shown that an acidic medication may reduce enamel hardness,9,10,11
but, to the best of our knowledge, the influence of pediatric oral liquid medicines on
enamel topography has not been studied yet. For this reason, the purpose of this in
vitro study was to evaluate the effect of common pediatric liquid medicines on
surface roughness and tooth structure loss and to evaluate the pH values of these
medicines at room and cold temperatures.
Methods
Pediatric medicines and pH analysis
The pediatric medicines used in this study were two analgesics – Alivium®
(Mantecorp, São Paulo, Brazil) and Novalgina® (Sanofi-Aventis, Paris, France); two
antibiotics – Betamox® (Atral, Castanheira do Ribatejo, Portugal) and Clavulin®
(GlaxoSmithKline, Brentford, United Kingdom); and two antihistamines – Claritin®
55
(Schering-Plough, New Jersey, United States) and Polaramine® (Mantecorp, São
Paulo, Brazil) (Table 1).
The pH values of the selected medicines at cold and room temperatures were
determined using a pH meter (Orion 261S, Thermo Fisher Scientific Inc.,
Massachusetts, United States). After equipment calibration, three samples of each
pediatric medicine were analyzed with pH electrodes. The average of the three
measurements was used as the pH value (Table 1).
Specimen preparation
Sound bovine incisor crowns were cut using a water-cooled diamond saw
(Bühler, Uzwil, Switzerland) to obtain enamel blocks (4 x 4 x 2 mm). These blocks
were fixed with wax in an acrylic device to polish the enamel surface: 600- and 1200-
grit silicon carbide papers (Extec Corp., Connecticut, United States), followed by a
1-µm diamond abrasive slurry (Extec Corp., Connecticut, United States) and
washed ultrasonically in MilliQ® water. Baseline surface microhardness (SMH) was
measured using a microhardness tester (HVS-1000, Time Group Inc., Beijing,
China) with a Knoop diamond under a 50-g load for 5 s, and five indentations spaced
100 µm from each other were made at the center of the enamel surface to select
the sample. A total of 84 blocks (mean 341.59±34.15 kg/mm2) were selected for the
present study and randomly divided into seven groups (n=12): G1=Alivium®,
G2=Novalgina®, G3=Betamox®, G4=Clavulin®, G5=Claritin®, G6=Polaramine®,
and G7= MilliQ® water (experimental control).
An acid-resistant nail varnish was used to divide the enamel surface into two
distinct areas: 1) a sound window (unexposed area) – the right side of the enamel
surface was covered with acid-resistant nail varnish (self-positive control); and 2) an
experimental window (exposed area) – the left side was not covered.
Experimental protocols

56
Twelve blocks from each group were immersed in pediatric liquid medicines
three times a day for 5 min (15 mL per block) for 7 days. After treatment, the
specimens were rinsed with deionized water (5 s) and transferred into artificial
saliva. All pediatric medicines were stored at 7°C, but removed 5 min before the
treatment period. After block immersion, they were returned to the refrigerator until
new treatment.
Two artificial saliva solutions were prepared to simulate the oral environment
and the pH changes that occur during the day, according to Queiroz et al.,12 with
some modifications. The first solution consisted of 0.05 mol/L acetate buffer, 1.28
mmol/L Ca, 0.74 mmol/L P, and 0.03 µg F/mL with pH 5.0 for 2 h (50 mL per block);
and the second one contained 0.1 mol/L Tris buffer, 1.5 mmol/L Ca, 0.9 mmol/L P,
150 mmol/L KCl, and 0.05 µg F/mL with pH 7.0 for 22 h (25 mL per block).
The experimental protocol consisted of three periods of immersion in
pediatric medicines and four periods in artificial saliva per day: 1st period – 5 min in
pediatric medicines; 2nd period – 6 h in artificial saliva (pH 7.0); 3rd period – 2 h in
artificial saliva (pH 5.0); 4th period – 5 min in pediatric medicines; 5th period – 8 h in
artificial saliva (pH 7.0); 6th period – 5 min in pediatric medicines; and 7th period – 8
h in artificial saliva (pH 7.0).
The experiment was carried out at 37 ºC. On the 4th day, the artificial saliva
solutions were replaced with fresh ones in order to avoid oversaturation.
3D non-contact profilometry
The surface topography of the specimens was analyzed by a 3D profilometer
(Nanovea PS50 Optical, NANOVEA Inc., California, United States). The
measurements of capture were performed with a chromatic confocal sensor with a
white light axial source at a scan velocity of 2 mm/s and with a refractive index of
10,000.
3D non-contact profilometry was used to determine the primary outcome:
tooth structure loss, i.e., the gap between the experimental and control areas (Gap)

57
in each group; and the secondary outcome: surface roughness - linear surface
roughness (Ra) and volumetric surface roughness (Sa). All comparisons between
the exposed and unexposed areas of enamel were performed after the removal of
the acid-resistant nail varnish.
The Gap was calculated from the step height difference between the
unexposed and exposed enamel surfaces in each block; three linear measurements
were made involving the unexposed and exposed areas. All measurements were
done in triplicate, and the mean values were used to represent the final result of the
surface profile.
To determine Ra, three linear measurements (one vertical, one horizontal
and one transversal) were performed in each area (experimental window or sound
window) of the enamel specimen. The average of these three linear measurements
was used to determine Ra1 (surface linear roughness in the sound window) and
Ra2 (surface linear roughness in the experimental window), and the Ra value for all
groups was calculated as Ra =Ra1 – Ra2.
Also, three scan areas (200 µm × 200 µm) were obtained for each block in
the sound and experimental window. The average of these three areas was used to
determine Sa1 (surface roughness in the sound window) and Sa2 (surface
roughness in the experimental window); and the Sa value for all groups was
calculated as Sa = Sa1 – Sa2.
Scanning Electron Microscopy (SEM) and Energy Dispersive Spectrometry
(EDS)
Three enamel blocks from each group were randomly selected and prepared
for EDS and SEM under a scanning electron microscope (6460LV, JEOL, Tokyo,
Japan). The blocks were mounted onto stubs with double-faced carbon tape and
analyzed by EDS. EDS was performed to assess the mineral content of the enamel,
identifying the chemical elements on its surface before and after the experimental
protocol. Therefore, it was possible to compare the chemical elements found in
treated (exposed) and untreated (unexposed) areas. This analysis was performed

58
with a Kontron automatic image analyzer system, and the total area of the block was
evaluated. The results were represented by the mean of the measured values.
After EDS, the samples were covered with a 30-µm gold layer and SEM was
performed to assess the topography of the enamel surface. The specimens were
examined under the same scanning electron microscope at 20 kV in low vacuum
mode (45 Pa) and the backscattered electrons (BSE) were analyzed. Initially, the
specimens were analyzed under a panoramic view (500X) to observe the interface
between the windows (sound and experimental); photomicrographs of the most
representative areas of each group were obtained at 1000X and 5000X
magnification to observe any changes in more detail.
Statistical analysis
The normal distribution of the data was checked for all tested variables, using
the Shapiro Wilk test. A Student’s paired t-test was used to compare Ra1 and Ra2
and Sa1 and Sa2. Differences in Ra and Sa among all treatment groups were tested
with the Kruskal-Wallis test, followed by the Mann-Whitney test. One-way analysis
of variance (one-way ANOVA), followed by a post-hoc test (Tukey’s test), was used
for Gap analysis. The SPSS software version 22.0 (IBM, Armonk, NY, United
States) was used for the statistical analysis. The significance level was set at 5%.
Results
Table 1 shows the pH values of pediatric liquid medicines at room and cold
temperatures. The pH values of pediatric medicines at room temperature were lower
than at cold temperature. G1 and G5 presented the lowest pH values.
The results of 3D non-contact profilometry are summarized in Table 2 with mean
Ra, Sa, and Gap for all groups. All pediatric medicines produced a significant
alteration in surface roughness (Ra and Sa) values after 7 days (p<0.05). These
alterations were evidenced when the images of the sound and experimental areas
were compared (Figure 1).
59
The group treated with Claritin® presented the worst Ra and Sa values, being
statistically different from the negative control (p<0.05). Clavulin®, Betamox®, and
Alivium® also showed statistical differences in Ra value when compared with the
negative control (p<0.05) (Table 2). Claritin® and Clavulin® showed the worst
alteration in surface roughness (Sa value) when compared with the negative control
(p<0.05) (Table 2).
When differences in Gap values were evaluated between the groups, only
Claritin® presented a statistically significant tooth structure loss when compared
with the negative control (p<0.05), but there was a similar trend among Claritin®,
Clavulin®, Polaramine®, and Alivium® since there was no statistical difference
between them (p>0.05). (Table 2).
Figure 1 shows only a change in surface roughness in some groups
(Novalgina®, Polaramine® and MilliQ® water), while in others, such as Claritin®,
the loss of tooth structure was evident in the exposed area. The same can be
observed in the images obtained by SEM (Figure 2). The images of the negative
control showed few signs of alteration; on the other hand, Claritin® produced the
worst alterations in enamel topography, causing loss of enamel structure (e.g.,
erosion).
The images of G1, G3, G4 and G5 showed that the enamel surfaces
appeared to be more porous than the images of groups G2, G6 and G7.
The chemical analysis, made with EDS, revealed the presence of carbon,
oxygen, sodium, phosphorus, calcium, chlorine, and aluminum. Exposed and
unexposed areas retained high rates of carbon, oxygen, phosphorus, and calcium.
In addition, it was possible to observe that calcium and phosphorus concentrations
increased in exposed areas in all groups except for the group treated with
Polaramine®. The other elements had almost the same rates when compared to the
unexposed and exposed areas (Table 3).
Discussion
60
It is widely known that acidic medicines have certain characteristics, such as
low pH, with the potential to produce alterations in the topography of enamel
surface.3,4,8,13 Many of these medicines, such as antibiotics and antihistamines, are
usually used to treat children for long periods.9 So, acidic medicines likely promote
surface degradation of the tooth and increase dental roughness. Other pediatric
medicines (e.g., analgesics) are largely used for children, and even though they are
used for short periods, it is also important to evaluate them once they could
potentially cause surface alterations. Then, it is important to evaluate the effects of
all these medicines chronically or usually used by children, on the topography of
dental enamel surface.
For this reason, our selection of medicines was based on previous results8-
11,14 as well as on prescriptions for children.
Our study is the first in the searched literature that evaluated changes in
surface enamel topography with regard to linear (Ra) and volumetric roughness (Sa)
and between unexposed and exposed enamel surfaces (Gap). The primary
outcome of the present study was the Gap formed between unexposed and exposed
enamel surface areas. This parameter was very important to measure the
magnitude of tooth structure loss in a direct comparison between unexposed and
exposed areas. However, the Ra and Sa parameters were of great importance to
determine the topographic alterations in each area. On the other hand, these
parameters (Ra and Sa) cannot be used to compare the Gap.
We observed that the enamel blocks treated with Claritin® presented the
worst Ra and Sa values, demonstrating a greater increase in roughness. Only
Claritin® presented significant Gap values. Similar results were observed in
previous studies that evaluated the effects of Claritin® on dental enamel. Valinoti et
al.10 evaluated the effect of three acidic medicines (Klaricid®, Claritin®, and
Dimetapp®) and showed Dimetapp® presented high changes in linear roughness
under normal pH-cycling conditions, but Claritin® had the worst linear roughness
under erosive pH-cycling conditions. By analyzing SEM images, the authors
observed that the specimens exposed to Dimetapp® presented the most severely
eroded areas, followed by Claritin®. Babu et al.11 observed an irregular pattern in
61
SEM, such as the erosion area caused by Claritin®. Costa et al.9 demonstrated that
the group treated with Claritin D® had significantly lower enamel hardness.
The use of a 3D non-contact profilometer was very advantageous because it
does not produce grooves on the surface of the samples and is more sensitive and
specific than a roughness tester.15,16,17 Non-contact surface profilometry allowed for
quantification of tooth depth and its measurements can be compared to those of
transverse microradiography (gold standard) for the quantification of enamel
changes in vitro.18 No previous investigations had evaluated the action of pediatric
medicines on roughness and tooth structure loss using 3D non-contact profilometry.
Salivary buffering and changes in oral pH are complex,19,20,21 and many
concomitant factors can influence the potential of substances to promote changes
in tooth topography, such as endogenous pH lower than 5.5, flow and salivary
buffering, and higher titratable acidity.3,6,8,11,19,21 Nevertheless, the evaluation of
these factors alone cannot determine whether a drug does have such potential.6,20
Previous studies1,4,8,11,14,22 evaluated various types of medications, taking
into consideration their chemical components, pH, or titratable acidity. Some authors
observed that Claritin® had low endogenous pH, between 2.1 and 2.8,8,22 and that
Polaramine® presented the highest pH value (6.0).1 Tests using models that may
mimic oral conditions are required to evaluate the real action of drugs on tooth
structure.23 In the literature, there are few studies that test the action of pediatric
medicines on teeth under conditions that mimic the oral cavity.9,10,19
In our study, we observed that the pH values of pediatric medicines at room
temperature were lower than at cold temperature, and that Claritin® and Alivium®
presented the lowest pH values. We found a difference between pH values at room
and cold temperatures. Since antibiotics could only be used at cold temperatures,
the same conditions were utilized for all products. All the pediatric medicines were
stored at 7°C between treatments and were only removed 5 min before block
immersion.
The EDS revealed high rates of carbon, oxygen, phosphorus, and calcium
elements in both (exposed and unexposed) areas. However, calcium and
phosphorus levels were higher in unexposed than in exposed areas only for the

62
blocks treated with Polaramine®. The drug composition itself can interfere with
these results; however, this was not evaluated in the present study. The authors
suggest that other studies be conducted in order to investigate the composition of
these products for a better understanding of the interaction between the ion
concentration of the medicines and tooth structure.
In our study, we used two different types of artificial saliva to mimic the
change in pH in the oral cavity. Nonetheless, the results of this in vitro study
concerning the effects of liquid pediatric medicines cannot be used for clinical
recommendations. Despite the use of pH cycling with dental elements, in vitro
models do not allow properly mimicking all of the events that occur in the oral
cavity.21,22,23
Notwithstanding, our findings are very important for future research, and
these preliminary results can contribute to planning new in situ and in vivo studies
in order to better understand the effect of the chemical and physical properties of
pediatric medicines on enamel topography.
Conclusions
Most of the pediatric medicines analyzed in this study had a low pH, mainly
at room temperature. Claritin®, Clavulin®, Betamox®, and Alivium® increased
linear surface roughness, but only Claritin® demonstrated the in vitro capacity to
create significant Gaps between unexposed and exposed enamel surfaces.
Acknowledgments: The authors acknowledge the financial support from the
CAPES, FAPERJ, and CNPq.

63
Fig 1. 3D profilometry scheme representation of enamel surfaces after treatment and pH cycling. left – sound window (unexposed area) and right – experimental window (exposed area). (A) G1=Alivium®, (B) G2=Novalgina®, (C) G3=Betamox®, (D) G4=Clavulin®, (E) G5=Claritin®, (F) G6=Polaramine®, and (G) G7= MilliQ® water (negative control).
A B
C D
E F
G

64
Fig 2. SEM images of enamel surfaces after treatment and pH cycling at 500X. Photomicrographs of the interface: left – sound window (unexposed area) and right – experimental window (exposed area). (A) G1=Alivium®, (B) G2=Novalgina®, (C) G3=Betamox®, (D) G4=Clavulin®, (E) G5=Claritin®, (F) G6=Polaramine®, and (G) G7= MilliQ® water (negative control).
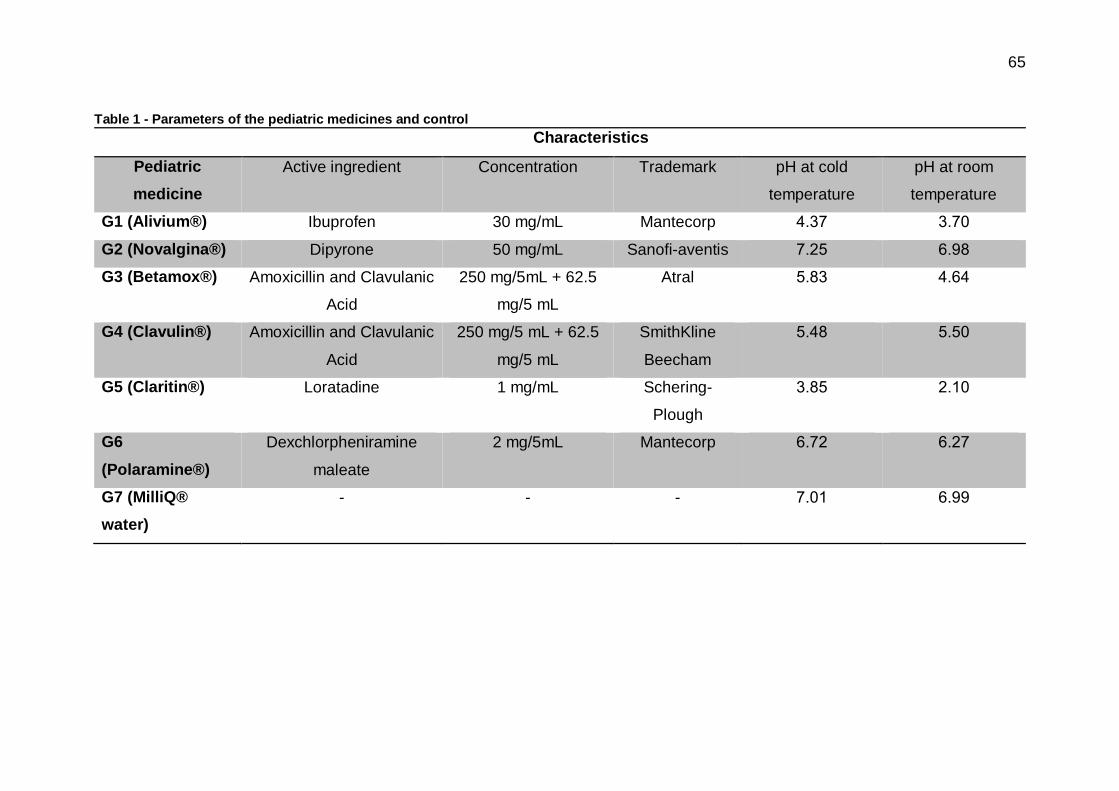
65
Table 1 - Parameters of the pediatric medicines and control
Characteristics
Pediatric
medicine
Active ingredient Concentration Trademark pH at cold
temperature
pH at room
temperature
G1 (Alivium®) Ibuprofen 30 mg/mL Mantecorp 4.37 3.70
G2 (Novalgina®) Dipyrone 50 mg/mL Sanofi-aventis 7.25 6.98
G3 (Betamox®) Amoxicillin and Clavulanic
Acid
250 mg/5mL + 62.5
mg/5 mL
Atral 5.83 4.64
G4 (Clavulin®) Amoxicillin and Clavulanic
Acid
250 mg/5 mL + 62.5
mg/5 mL
SmithKline
Beecham
5.48 5.50
G5 (Claritin®) Loratadine 1 mg/mL Schering-
Plough
3.85 2.10
G6
(Polaramine®)
Dexchlorpheniramine
maleate
2 mg/5mL Mantecorp 6.72 6.27
G7 (MilliQ®
water)
- - - 7.01 6.99
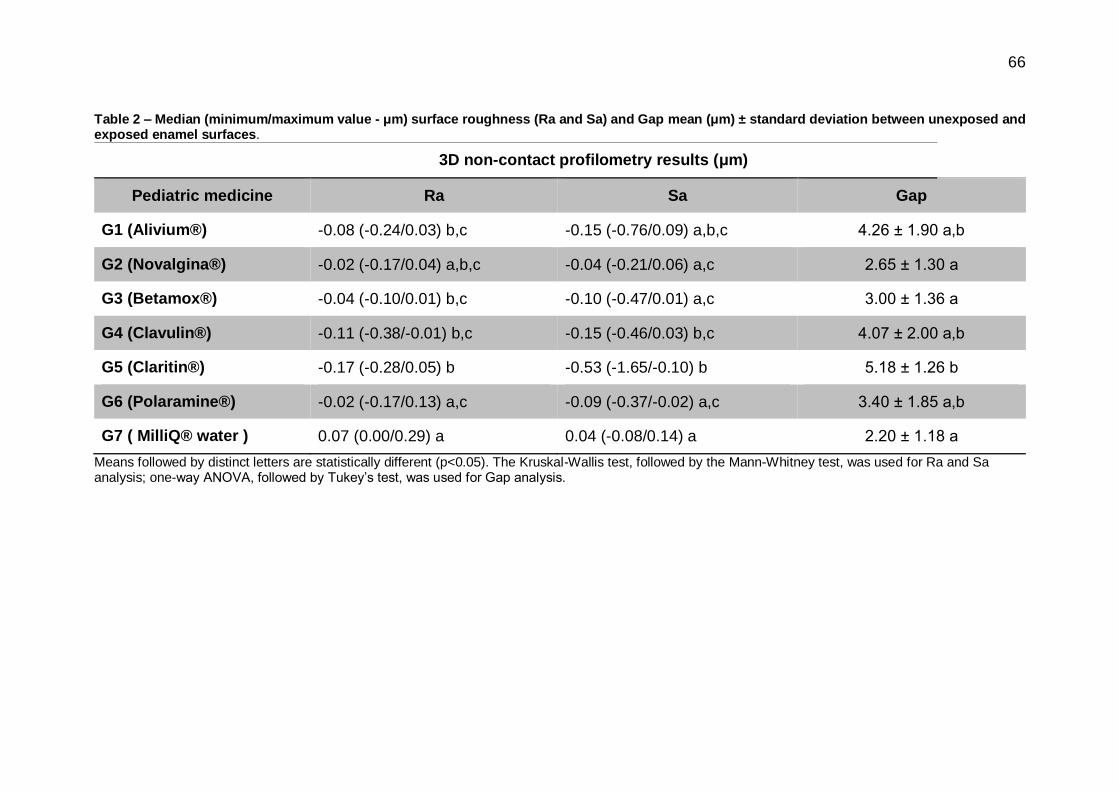
66
Table 2 – Median (minimum/maximum value - μm) surface roughness (Ra and Sa) and Gap mean (μm) ± standard deviation between unexposed and exposed enamel surfaces.
3D non-contact profilometry results (μm)
Pediatric medicine Ra Sa Gap
G1 (Alivium®) -0.08 (-0.24/0.03) b,c -0.15 (-0.76/0.09) a,b,c 4.26 ± 1.90 a,b
G2 (Novalgina®) -0.02 (-0.17/0.04) a,b,c -0.04 (-0.21/0.06) a,c 2.65 ± 1.30 a
G3 (Betamox®) -0.04 (-0.10/0.01) b,c -0.10 (-0.47/0.01) a,c 3.00 ± 1.36 a
G4 (Clavulin®) -0.11 (-0.38/-0.01) b,c -0.15 (-0.46/0.03) b,c 4.07 ± 2.00 a,b
G5 (Claritin®) -0.17 (-0.28/0.05) b -0.53 (-1.65/-0.10) b 5.18 ± 1.26 b
G6 (Polaramine®) -0.02 (-0.17/0.13) a,c -0.09 (-0.37/-0.02) a,c 3.40 ± 1.85 a,b
G7 ( MilliQ® water ) 0.07 (0.00/0.29) a 0.04 (-0.08/0.14) a 2.20 ± 1.18 a
Means followed by distinct letters are statistically different (p<0.05). The Kruskal-Wallis test, followed by the Mann-Whitney test, was used for Ra and Sa analysis; one-way ANOVA, followed by Tukey’s test, was used for Gap analysis.
67
References
1. Neves BG, Farah A, Lucas E, de Sousa VP, Maia LC. Are paediatric
medicines risk factors for dental caries and dental erosion? Community Dent
Health. 2010 Mar;27(1):46-51.
2. Moazzez R, Bartlett D. Intrinsic causes of erosion. Monogr Oral Sci. 2014
Jun;25:180-96
3. Hellwig E, Lussi A. Oral hygiene products, medications and drugs - hidden
aetiological factors for dental erosion. Monogr Oral Sci. 2014 Jun;25:155-62
4. Maguire A, Baqir W, Nunn JH. Are sugars-free medicines more erosive than
sugars-containing medicines? An in vitro study of paediatric medicines with
prolonged oral clearance used regularly and long-term by children. Int J Paediatr
Dent. 2007 Jul;17(4):231-8.
5. Linnett V, Seow WK. Dental erosion in children: a literature review. Pediatr
Dent. 2001 Jan-Feb;23(1):37-43.
6. Serra MC, Messias DCF, Turssi CP. Control of erosive tooth wear:
possibilities and rationale. Braz Oral Res. 2009;23 Suppl 1:49-55.
7. Bartlett DW. The role of erosion in tooth wear: aetiology, prevention and
management. Int Dent J. 2005 Aug;55 Suppl 4:277-84.
8. Arora R, Mukherjee U, Arora V. Erosive potential of sugar free and sugar
containing pediatric medicines given regularly and long term to children. Indian J
Pediatr. 2012 Jun;79(6):759-63.
9. Costa CC, Almeida IC, Costa Filho LC. Erosive effect of an antihistamine-
containing syrup on primary enamel and its reduction by fluoride dentifrice. Int J
Paediatr Dent 2006 May;16(3):174-80.
10. Valinoti AC, Pierro VS, Da Silva EM, Maia LC. In vitro alterations in dental
enamel exposed to acidic medicines. Int J Paediatr Dent 2011 Mar;21(2):141-50.

68
11. Babu KL, Rai K, Hedge AM. Pediatric liquid medicaments--do they erode
the teeth surface? An in vitro study: part I. J Clin Pediatr Dent. 2008
Spring;32(3):189-94.
12. Queiroz CS, Hara AT, Paes Leme AF, Cury JA. pH-cycling models to
evaluate the effect of low fluoride dentifrice on enamel de- and remineralization.
Braz. Dent. J. 2008;19(1):21-27.
13. Lodi CS, Sassaki KT, Fraiz FC, Delbem ACB, Martinhon CCR. Evaluation
of some properties of fermented milk beverages that affect the demineralization
of dental enamel. Braz Oral Res. 2010 Jan-Mar;24(1):95-101.
14. Pierro VS, Abdelnur JP, Maia LC, Trugo LC. Free sugar concentration and
pH of paediatric medicines in Brazil. J Clin Pediatr Dent. 2005 Sep;22(3):180-3.
15. Attin T, Wegehaupt FJ. Methods for assessment of dental erosion. Monogr
Oral Sci. 2014 Jun;25:123-142.
16. Attin T, Becker K, Roos M, Attin R, Paque F. Impact of storage conditions
on profilometry of eroded dental hard tissue. Clin Oral Investig. 2009
Dec;13(4):473-8.
17. Joniot SB, Gregoire GL, Auther AM, Roques YM. Three-dimensional
optical profilometry analysis of surface states obtained after finishing sequences
for three composite resins. Oper Dent. 2000 Jul-Aug;25(4):311-5.
18. Elton V, Cooper L, Higham SM, Pender N. Validation of enamel erosion in
vitro. J Dent. 2009 May;37(5):336-41.
19. Correa MC, Lerco MM, Cunha Mde L, Henry MA. Salivary parameters and
teeth erosions in patients with gastroesophageal reflux disease. Arq
Gastroenterol. 2012 Jul-Sep;49(3):214-8.
20. Hellwig E, Lussi A, Goetz F. Influence of Human Saliva on the
Development of Artificial Erosion. Caries Res. 2013 Jul;47(6):553-8.
21. Hall AF, Buchanan CA, Millett DT, Creanor SL, Strang R, Foye RH. The
effect of saliva on enamel and dentine erosion. J Dent. 1999 Jul;27(5):333-9.
69
22. Xavier AFC, Moura EFF, Azevedo WF, Vieira FF, Abreu MHNG, Cavalcanti
AL. Erosive and cariogenicity potential of pediatric drugs: study of physicochemical
parameters. BMC Oral Health. 2013 Dec;13:71
23. Hara AT, Gonzalez-Cabezas C, Creeth J, Zero DT. The effect of human
saliva substitutes in an erosion-abrasion cycling model. Eur J Oral Sci. 2008
Dec;116(6):552-6.
70
4.4. Artigo 4 – Protective effect of NaF varnish with CPP-ACP against dental
erosion caused by soft drink associated to pediatric liquid medicine.
Short title: Inhibition of tooth erosion by CPP-ACP varnish.
Adílis Kalina Alexandria1
Ana Maria Gondim Valença2
Lúcio Mendes Cabral3
Lucianne Cople Maia1
1 Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Federal
University of Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil
2 Department of Clinical and Social Dentistry, Dental School, Federal University of
Paraiba (UFPB), João Pessoa, PB, Brazil
3 School of Pharmacy, Federal University of Rio de Janeiro (UFRJ), Rio de Janeiro,
RJ, Brazil
Corresponding author:
Lucianne Cople Maia
Disciplina de Odontopediatria da FO-UFRJ, Caixa Postal: 68066 –
CidadeUniversitária – CCS, CEP: 21941-971 - Rio de Janeiro – RJ –Brazil
Fax/phone: +5521 39382101 r. 7
E-mail: [email protected]

71
Abstract
The purpose of this present study was to evaluate the preventive effect of
NaF varnish with and without CPP-ACP against acidic erosion promoted by soft
drink (SD) associated to pediatric liquid medicine (PLM). Sixty bovine enamel
specimens were ramdomly assigned in six groups (n=10) as follows: G1= CPP-
ACP/NaF varnish (MI varnishTM) + SDE; G2= NaF varnish (Duraphat®) + SD
erosion (SDE) (positive control for SDE); G3= MilliQ® water + SDE (negative
control for SDE); G4= CPP-ACP/NaF varnish + PLM/SDE; G5= NaF varnish +
PLM/SDE (positive control for PLM+SDE) and G6= MilliQ® water + PLM/SDE
(negative control for PLM+SDE). Before treatments, the samples`s surface was
divided into two areas (unexposed -UA and exposed area- EA). Between erosive
cycles and after the last daily SDE, the specimens stayed in artificial saliva. The
specimens were evaluated by 3D non-contact profilometry technique to
determinate tooth structure loss (TSL) and surface roughness (Sa). Scanning
electron microscopy (SEM) evaluated the topography of samples. After SDE, only
G1 differed from G3, the CPP-ACP/NaF varnish group presented the lowest TSL
values comparing with negative control (p=0.008). G1 and G2 didn’t differ between
them (p=0.203). However, after PLM+SDE, G4 and G5 differ from G6 (p=0.001
and p=0.0001, respectively). G1, G2, G3, G4 and G5 had lower alterations in Sa
than G6 (p<0.005). Examining 3D and SEM images, the higher differences
between UA and EA were observed to G3 and G6, and the lowest to G1 and G4.
The EA from G3 and G6 presented the worst alterations. The CPP-ACP/NaF
varnish was effective in improving protection against TSL after SDE. Both
varnishes also showed the capacity in reducing TSL and Sa after PLM+SDE.
72
Introduction
Dental erosion is the dissolution of tooth mineral by acids without bacterial
involvement. The chemical wear result in a roughened structure and the loss of
tissue can appear like a visible defect in dental surface [1, 2]. Dental erosion has a
high prevalence, mainly in children and adolescents [3, 4].
Liquid medicines are widely used for children because facility of ingestion
[5, 6]. However, some of inactive acidic components have low pH [5, 7], and
because high frequency of medication intake, bedtime consumption, high viscosity,
and reduction in salivary flow, its may also be related to alterations of surface
morphology of dental enamel [5, 8].
Some preventive actions have been suggested to avoid the beginning of the
erosion process, such as the use of professional topical fluorides [9, 10].
Furthermore, the addition of new remineralizing compounds to fluoride varnishes
can be an alternative to achive better effects against erosive wear.
Casein Phosphopeptide-Amorphous Calcium Phosphate Nanocomplexes
(CPP-ACP), also know as the RecaldentTM technology, is based on stabilization of
amorphous calcium phosphate (ACP) by casein phosphopeptides (CPP). It has
been reported that the CPP-ACP nanocomplexes provides high concentration of
calcium and phosphate ions. CPP-ACP compound can interact with fluoride ions
to produce an ACFP phase and achive better benefits to teeth [11, 12]. It is
important to know the effects of acidic drinks and acidic drugs association as well
as its mechanisms to avoid possible damage to tooth structure. To the best of our
knowledge, the influence of CPP-ACFP varnish on the erosion prevention has not
been studied yet. For this reason, the purpose of this in vitro study was to evaluate
the effect of NaF varnishes containing or not CPP-ACP in preventing tooth
structure loss and alterations in enamel roughness after erosion promoted by soft
drink associated or not to pediatric liquid medicines.

73
Methods
Specimen Preparation
Enamel specimens (4x4x2mm) were prepared from the labial surfaces of
bovine incisors crowns. The specimens were cut using an ISOMET low-speed saw
(Buehler Ltd, Lake Bluff, Illinois, USA) with 2 diamond discs (Extec Corp, Enfield,
Connecticut, USA) separated by a 4-mm spacer. The specimen surface was polish
using water-cooled silicon carbide paper 600 and 1200 (Extec Corp., Enfield,
Connecticut, USA). After each polishing phase, the specimens were cleaned in an
ultrasonically device with MilliQ® water for 5min. The specimens were checked
regarding the presence of white spots and cracks using a microscope (40x
magnification). They were selected by using baseline roughness of enamel surface
values (1.82 ± 0.18), measured using a 3D profilometer (Nanovea PS50 Optical,
NANOVEA Inc., Irvine, California, USA) and randomly allocated in groups [13].
Prior to the experiment, a nail varnish was applied in the left half of the
specimen’s surface to maintain the sound reference surface (unexposed area, self-
control per specimen), the other half of the surface (left side - was not covered,
representing the exposed area). The specimens were maintained in 100% humidity
until the beginning of the experiment.
Treatment and erosive cycling
The fluoride varnishes used in this study were: (1) NaF varnish (5% NaF,
Duraphat®, Colgate Oral Pharmaceuticals, New York, New York, United States) -
representing the positive control groups and (2) CPP-ACP/NaF varnish (2% CPP-
ACP and 5% NaF, MI varnishTM, GC America, Alsip, Illinois, United States) -
representing the experimental groups.
A sample size of 10 specimens was calculated considering an error level of
5% and b-error level of 20% based on previous study [13]. Sixty enamel specimens
were randomly allocated to six groups (n=10) according to treatment and type of
erosion challenge: G1= NaF varnish + soft drink erosion; G2= CPP-ACP/NaF
varnish + soft drink erosion; G3= MilliQ® water + soft drink erosion (soft drink
74
erosion negative control); G4= NaF varnish + pediatric liquid medicine/soft drink
erosion; G5= CPP-ACP/NaF varnish + pediatric liquid medicines/soft drink erosion
and G6= MilliQ® water + pediatric liquid medicine/soft drink erosion (pediatric liquid
medicines + soft drink erosion negative control).
In groups G1, G2 and G3, SDE - soft drink erosion only with Coca-Cola®
(Coca-Cola® Company, Porto Real, Rio de Janeiro, Brazil) were performed and in
G4, G5 and G6, PLM+SDE - pediatric liquid medicine plus soft drink erosion were
performed, in which the sample were immersed in Claritin® (Schering-Plough, New
Jersey, United States) and in Coca-Cola® (Figure 1).
The varnishes were applied once at the beginning of the experiment in a thin
layer on specimen`s surface, using a microbrush. After 6h immerse in artificial
saliva (1.5mmol/L Ca, 0.9mmol/L P, 150mmol/L KCl, 0.05mg F/mL in 0.1mol/L Tris
buffer, pH 7.0, 25ml/sample) [13, 14]. The layer of varnish was removed using a
scalpel blade and acetone with water (1:1), the total removal was checked
microscopically (40x magnification).
All samples were subjected to erosion cycles for 4 days; 6 SDE were
performed per day for 10min each, using freshly opened bottles of Coca-Cola® pH
2.58, 15ml/specimen. Furthermore, the samples of G4, G5 and G6 were immersed
2X/day (before the first and last soft drink immersion) for 5min in a pediatric liquid
medicine (Claritin®), pH 2.12, 15ml/specimen [13]. The experiment was carried out
at 37 ºC. After each erosion period, samples were rinsed in MilliQ® water. Between
each SDE, the samples were immersed in artificial saliva.
Profilometric analysis
After 4 days of experiment, the layer of acid-resistant nail varnish was
removed using acetone with water (1:1). Allowing the comparisons between the
unexposed and exposed areas.
A chromatic confocal sensor with a white light axial of 3D non-contact optical
profilometer scanned an area of 1 x 1mm on each specimen (velocity of 2μm/s),
and generated one image for each sample. The images were analyzed by Nanovea

75
Professional 3D software (Nanovea PS50 Optical, NANOVEA Inc., Irvine,
California, USA) to determine tooth structure loss (TSL) and surface roughness
(Sa), according to Alexandria et al. [13].
The evaluation of tooth structure loss (µm) was performed in the center of
each specimen; three linear measurements (1mm length) were made involving the
unexposed and exposed area to calculate the difference in height difference
between the unexposed and exposed enamel surface in each specimen. All
measurements were done in triplicate, and the average was used to represent the
final result of the specimen surface profile.
To determine Sa, three scans (200µm × 200µm) were acquired in each area
(unexposed and exposed area) on the enamel specimen. The average of these
three measurements in each area was used to determine Sa1 (surface roughness
in unexposed area) and Sa2 (surface roughness in the exposed area), the Sa value
for all groups was calculated as the difference between Sa1 and Sa2 by using the
following formula: Sa = Sa1 – Sa2 [13].
3D profilometry images and Scanning Electron Microscopy (SEM)
One 3D topographical image was choice to represent the results of each
group. Furthermore, two SEM photomicrographs (500X and 2.000X magnification)
of each group were also acquired.
3D topographical images was constructed from scanned area (1 x 1mm) by
Nanovea Professional 3D software, all images were standardized in height. SEM
analysis was performed in scanning electron microscope (6460LV, JEOL,
Akishima, Tokyo, Japan). Three enamel specimens of each group were randomly
selected, covered with a 30-µm gold layer and fixed on stubs with double-faced
carbon tape. The topography of enamel specimens was analyzed in backscattered
electrons at 20kV in low vacuum mode (45Pa). The photomicrograph with 500X
was used to observe the interface among areas (unexposed and exposed) and
2.000X to observe the changes in detail. The schematic design of the experimental
protocol is shown in figure 1.
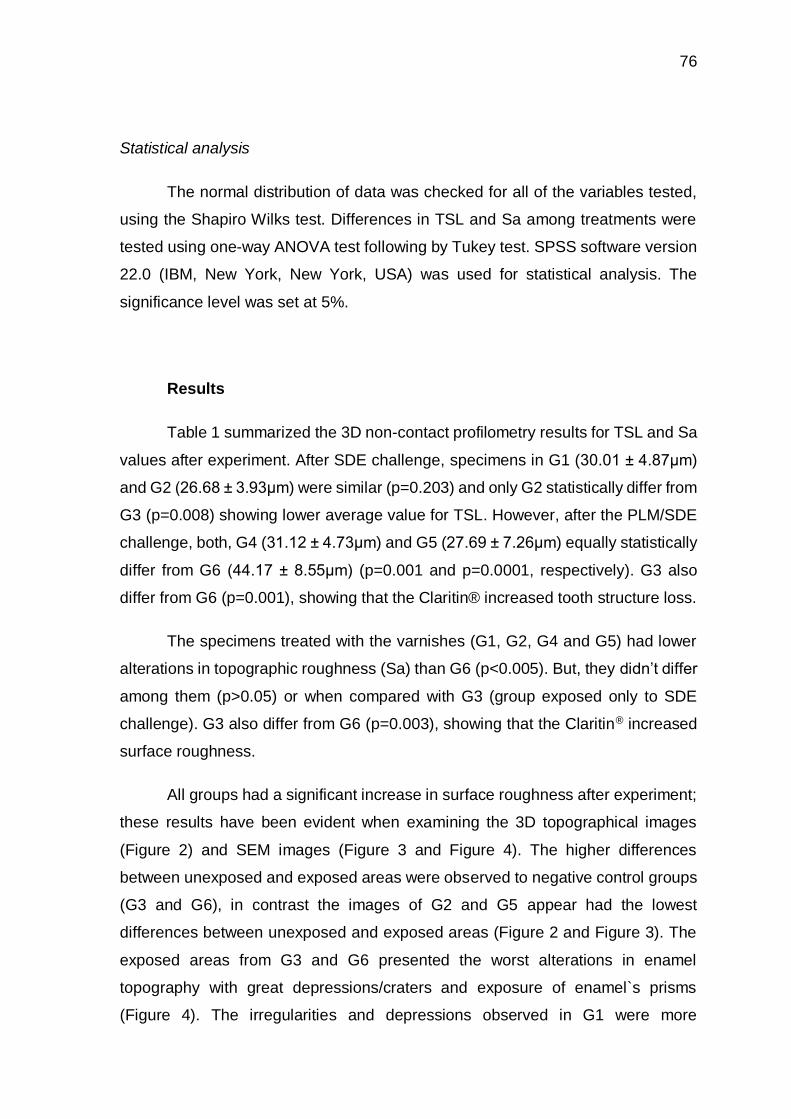
76
Statistical analysis
The normal distribution of data was checked for all of the variables tested,
using the Shapiro Wilks test. Differences in TSL and Sa among treatments were
tested using one-way ANOVA test following by Tukey test. SPSS software version
22.0 (IBM, New York, New York, USA) was used for statistical analysis. The
significance level was set at 5%.
Results
Table 1 summarized the 3D non-contact profilometry results for TSL and Sa
values after experiment. After SDE challenge, specimens in G1 (30.01 ± 4.87μm)
and G2 (26.68 ± 3.93μm) were similar (p=0.203) and only G2 statistically differ from
G3 (p=0.008) showing lower average value for TSL. However, after the PLM/SDE
challenge, both, G4 (31.12 ± 4.73μm) and G5 (27.69 ± 7.26μm) equally statistically
differ from G6 (44.17 ± 8.55μm) (p=0.001 and p=0.0001, respectively). G3 also
differ from G6 (p=0.001), showing that the Claritin® increased tooth structure loss.
The specimens treated with the varnishes (G1, G2, G4 and G5) had lower
alterations in topographic roughness (Sa) than G6 (p<0.005). But, they didn’t differ
among them (p>0.05) or when compared with G3 (group exposed only to SDE
challenge). G3 also differ from G6 (p=0.003), showing that the Claritin® increased
surface roughness.
All groups had a significant increase in surface roughness after experiment;
these results have been evident when examining the 3D topographical images
(Figure 2) and SEM images (Figure 3 and Figure 4). The higher differences
between unexposed and exposed areas were observed to negative control groups
(G3 and G6), in contrast the images of G2 and G5 appear had the lowest
differences between unexposed and exposed areas (Figure 2 and Figure 3). The
exposed areas from G3 and G6 presented the worst alterations in enamel
topography with great depressions/craters and exposure of enamel`s prisms
(Figure 4). The irregularities and depressions observed in G1 were more
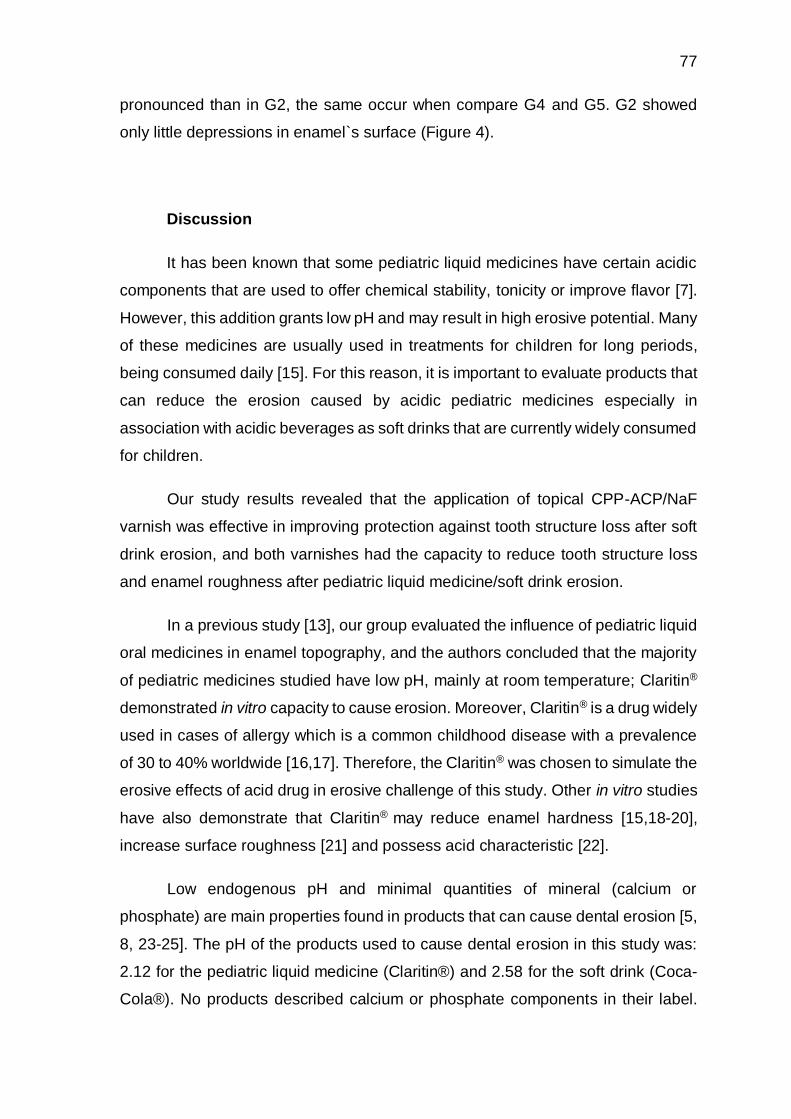
77
pronounced than in G2, the same occur when compare G4 and G5. G2 showed
only little depressions in enamel`s surface (Figure 4).
Discussion
It has been known that some pediatric liquid medicines have certain acidic
components that are used to offer chemical stability, tonicity or improve flavor [7].
However, this addition grants low pH and may result in high erosive potential. Many
of these medicines are usually used in treatments for children for long periods,
being consumed daily [15]. For this reason, it is important to evaluate products that
can reduce the erosion caused by acidic pediatric medicines especially in
association with acidic beverages as soft drinks that are currently widely consumed
for children.
Our study results revealed that the application of topical CPP-ACP/NaF
varnish was effective in improving protection against tooth structure loss after soft
drink erosion, and both varnishes had the capacity to reduce tooth structure loss
and enamel roughness after pediatric liquid medicine/soft drink erosion.
In a previous study [13], our group evaluated the influence of pediatric liquid
oral medicines in enamel topography, and the authors concluded that the majority
of pediatric medicines studied have low pH, mainly at room temperature; Claritin®
demonstrated in vitro capacity to cause erosion. Moreover, Claritin® is a drug widely
used in cases of allergy which is a common childhood disease with a prevalence
of 30 to 40% worldwide [16,17]. Therefore, the Claritin® was chosen to simulate the
erosive effects of acid drug in erosive challenge of this study. Other in vitro studies
have also demonstrate that Claritin® may reduce enamel hardness [15,18-20],
increase surface roughness [21] and possess acid characteristic [22].
Low endogenous pH and minimal quantities of mineral (calcium or
phosphate) are main properties found in products that can cause dental erosion [5,
8, 23-25]. The pH of the products used to cause dental erosion in this study was:
2.12 for the pediatric liquid medicine (Claritin®) and 2.58 for the soft drink (Coca-
Cola®). No products described calcium or phosphate components in their label.
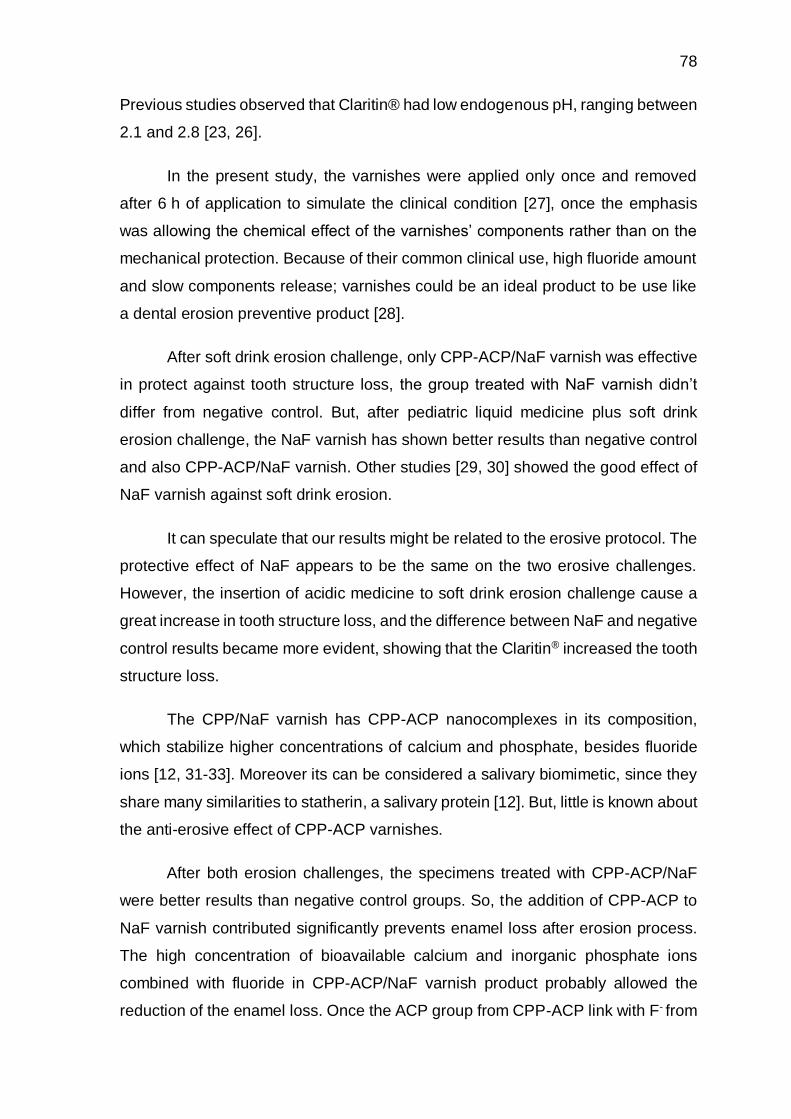
78
Previous studies observed that Claritin® had low endogenous pH, ranging between
2.1 and 2.8 [23, 26].
In the present study, the varnishes were applied only once and removed
after 6 h of application to simulate the clinical condition [27], once the emphasis
was allowing the chemical effect of the varnishes’ components rather than on the
mechanical protection. Because of their common clinical use, high fluoride amount
and slow components release; varnishes could be an ideal product to be use like
a dental erosion preventive product [28].
After soft drink erosion challenge, only CPP-ACP/NaF varnish was effective
in protect against tooth structure loss, the group treated with NaF varnish didn’t
differ from negative control. But, after pediatric liquid medicine plus soft drink
erosion challenge, the NaF varnish has shown better results than negative control
and also CPP-ACP/NaF varnish. Other studies [29, 30] showed the good effect of
NaF varnish against soft drink erosion.
It can speculate that our results might be related to the erosive protocol. The
protective effect of NaF appears to be the same on the two erosive challenges.
However, the insertion of acidic medicine to soft drink erosion challenge cause a
great increase in tooth structure loss, and the difference between NaF and negative
control results became more evident, showing that the Claritin® increased the tooth
structure loss.
The CPP/NaF varnish has CPP-ACP nanocomplexes in its composition,
which stabilize higher concentrations of calcium and phosphate, besides fluoride
ions [12, 31-33]. Moreover its can be considered a salivary biomimetic, since they
share many similarities to statherin, a salivary protein [12]. But, little is known about
the anti-erosive effect of CPP-ACP varnishes.
After both erosion challenges, the specimens treated with CPP-ACP/NaF
were better results than negative control groups. So, the addition of CPP-ACP to
NaF varnish contributed significantly prevents enamel loss after erosion process.
The high concentration of bioavailable calcium and inorganic phosphate ions
combined with fluoride in CPP-ACP/NaF varnish product probably allowed the
reduction of the enamel loss. Once the ACP group from CPP-ACP link with F- from

79
NaF to produce the ACFP phase, this ACFP is unstable and rapidly transform to
fluorhidroxyapatite [34].
Rallan et al. [35] evaluated the effect CPP-ACP and CPP-ACP/NaF
toothpaste against soft drink erosion (Coca-Cola®) and observed that all treatments
had good microhardness results when compared with negative control, but the
samples treated with CPP-ACP/NaF toothpaste showed the best potential to
control dental erosion. Showing the sinergism beteween CPP-ACP and fluoride.
Our previous data demostrated that CPP/NaF and NaF varnishes presented
preventive effect against soft drink erosion and inhibitory effect on erosion
progression [27]. They concluded that the presence of CPP-ACP improved the
performance of NaF varnish to protect against tooth structure loss after 3 days of
erosion. Rallan et al. and Alexandria et al. [27, 35] corroborating, with our results,
in which the presence of CPP-ACP also improved the performance of NaF varnish
in prevent the TSL after 4 days of soft drink erosion.
The negative control groups presented the worst topographical alterations
in enamel with great depressions/craters and exposure of enamel prisms. The
groups treated with CPP/NaF varnish presented only few depressions in enamel
surface. The irregularities and depressions observed in NaF varnish groups were
more pronounced than CPP/NaF varnish groups in both erosion challenges.
Probably the presence of high amount of calcium present in CPP-ACP/NaF varnish
contributes to protect the surface enamel, making this surface less irregular even
in the face of erosion challenges. Our results are in agreement with Poggio et al.
and Alexandria et al. [27, 36]. Both authors observed that the group treated with
CPP-ACP had the lower surface alterations.
Poggio et al. [36] evaluated a CPP-ACP mousse on the prevention of soft
drink dental erosion and they concluded that the group treated with CPP-ACP had
lower roughness values than control group. Alexandria et al. [27] evaluated the
preventive effect of CPP/NaF and NaF varnishes against soft drink erosion and
they concluded that both varnishes protected the enamel against alterations in
surface roughness after 3 days of erosion. Otherwise, in this actual study CPP/NaF
and NaF varnishes didn’t demonstrate protection against Ra alteration after 4 days

80
of soft drink erosion. However, both varnishes were capable to decrease
roughness alterations after medicine erosion challenge. This is an important result
because many children use antihistaminics such Claritin® for long periods of time
[37], the use of these varnishes to prevent roughness alteration in enamel could be
a good alternative.
Despite their advantages, as provides investigations in a controlled
environment with single-variable, this in vitro protocol has limitations, particularly
related to their inability to best simulate the complex biological of dental erosion
processes, due the difficult in matching solid/solution ratios that occur in vivo. But,
our study is the first in the searched literature that evaluated the changes in surface
enamel topography with regard to surface roughness profile and tooth structure
loss after erosion challenge performed by acidic pediatric liquid medicine.
Conclusions
The application of topical CPP-ACP/NaF varnish was effective in improving
protection against tooth structure loss after soft drink erosion challenge, and both
varnishes had the capacity in reducing tooth structure loss and enamel roughness
after pediatric liquid medicine plus soft drink erosion challenge. These findings
provided a basis for future in situ studies and clinical trials that could determine the
effect of CPP-ACP/NaF varnish in preventing clinical erosive tooth wear, especially
in cases of patients who make use of acidic pediatric liquid medicines.
Acknowledgements: The authors acknowledge the financial support from
the CAPES, Faperj (E-26/201.316/2014) and CNPq (302800/2012-3). This study
is part of the PhD thesis of the first author.
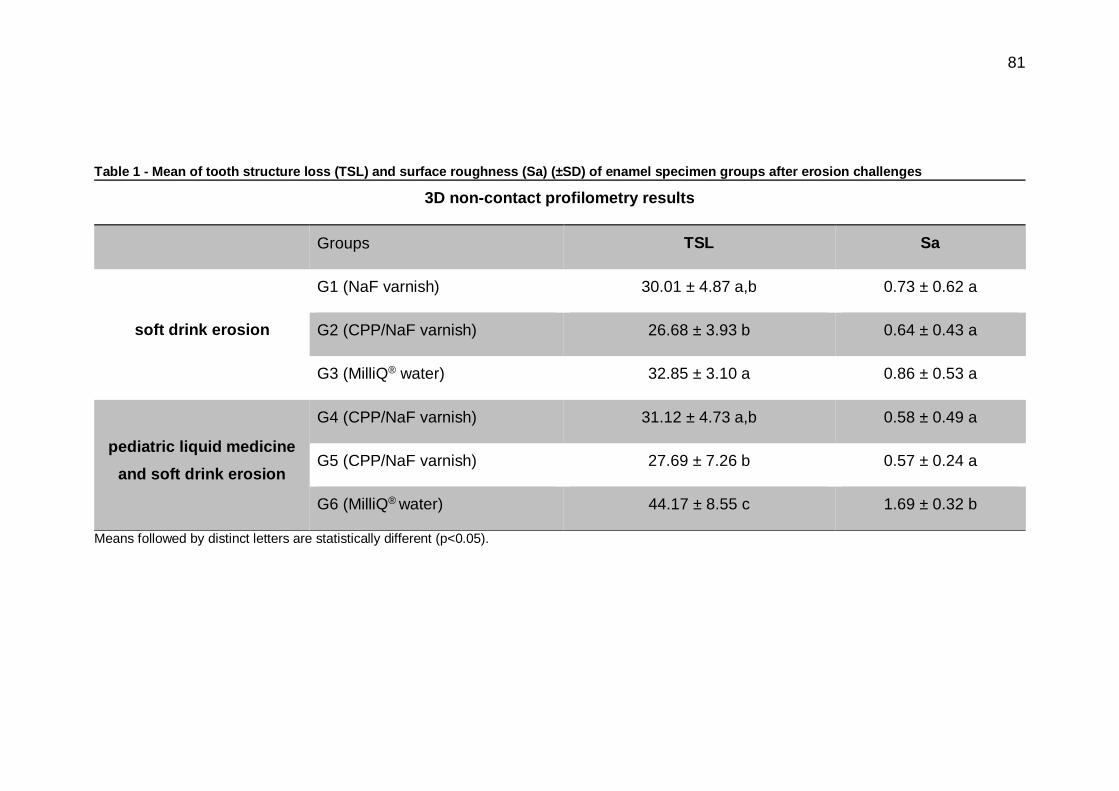
81
Table 1 - Mean of tooth structure loss (TSL) and surface roughness (Sa) (±SD) of enamel specimen groups after erosion challenges
3D non-contact profilometry results
Groups TSL Sa
soft drink erosion
G1 (NaF varnish) 30.01 ± 4.87 a,b 0.73 ± 0.62 a
G2 (CPP/NaF varnish) 26.68 ± 3.93 b 0.64 ± 0.43 a
G3 (MilliQ® water) 32.85 ± 3.10 a 0.86 ± 0.53 a
pediatric liquid medicine
and soft drink erosion
G4 (CPP/NaF varnish) 31.12 ± 4.73 a,b 0.58 ± 0.49 a
G5 (CPP/NaF varnish) 27.69 ± 7.26 b 0.57 ± 0.24 a
G6 (MilliQ® water) 44.17 ± 8.55 c 1.69 ± 0.32 b
Means followed by distinct letters are statistically different (p<0.05).
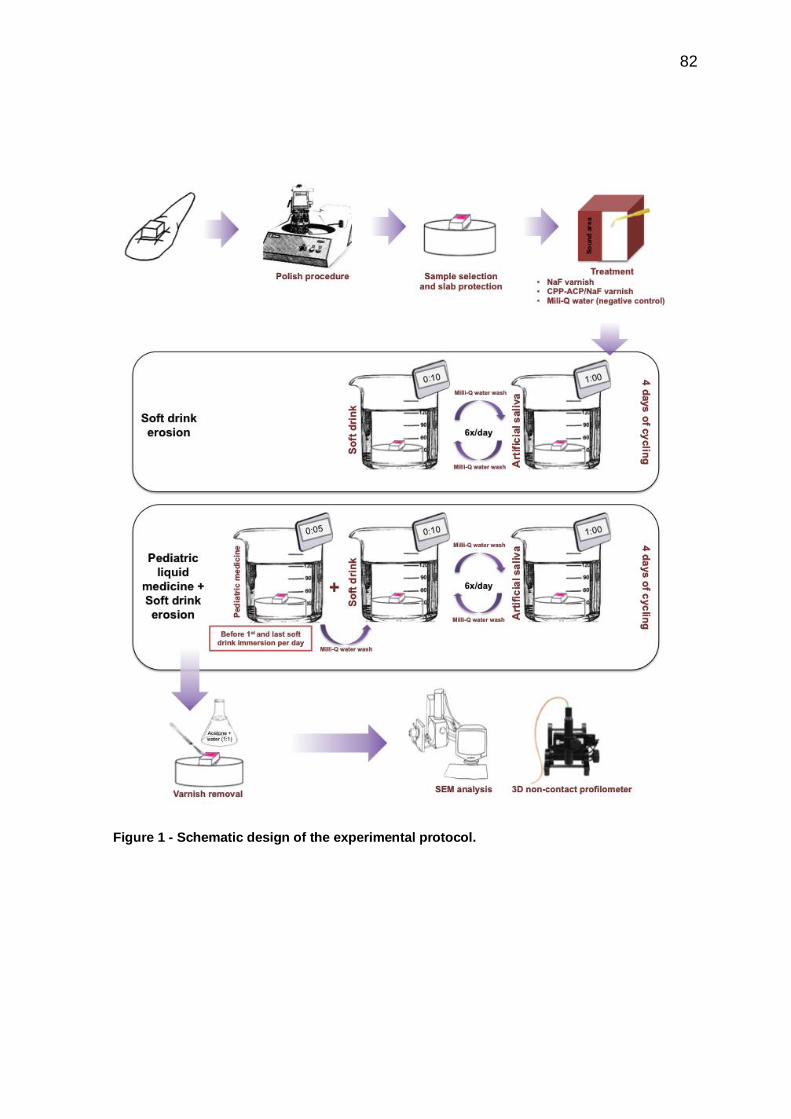
82
Figure 1 - Schematic design of the experimental protocol.

83
Figure 2 - 3D profilometry images of enamel surface samples after treatment and erosion challenges for each group. A-C images = soft drink erosion challenge, D-F images= pediatric liquid medicine + soft drink erosion challenge. (A) and (D) G1 and G4= NaF varnish, (B)and (E) G2 and G5= CPP-ACP/NaF varnish, (C) and (F) G3 and G6= MilliQ® water (negative control). 1= the unexposed area (sound enamel), 2= exposed area (after erosion).

84
Figure 3 - Surface SEM photomicrographs of enamel samples after treatment and erosion challenges at 500X. A-C images = soft drink erosion challenge, D-F images= pediatric liquid medicine + soft drink erosion challenge. (A) and (D) G1 and G4= NaF varnish, (B)and (E) G2 and G5= CPP-ACP/NaF varnish, (C) and (F) G3 and G6= MilliQ® water (negative control). 1= the unexposed area (sound enamel), 2= exposed area (after erosion).

85
Figure 4 - Surface SEM photomicrographs of enamel samples after treatment and erosion challenges at 2000X. A-C images = soft drink erosion challenge, D-F images= pediatric liquid medicine + soft drink erosion challenge. (A) and (D) G1 and G4= NaF varnish, (B)and (E) G2 and G5= CPP-ACP/NaF varnish, (C) and (F) G3 and G6= MilliQ® water (negative control). Arrow 1= exposure of enamel`s prisms, arrow 2= little depressions in enamel`s surface, arrow 3= great depressions/craters.

86
Reference
1. Lussi, A. and T.S. Carvalho, Erosive tooth wear: a multifactorial condition of
growing concern and increasing knowledge. Monogr Oral Sci, 2014. 25: p. 1-15.
2. Shellis, R.P., et al., Effects of buffering properties and undissociated acid
concentration on dissolution of dental enamel in relation to pH and acid type. Caries
Res, 2013. 47(6): p. 601-11.
3. Salas, M.M., et al., Estimated prevalence of erosive tooth wear in permanent
teeth of children and adolescents: an epidemiological systematic review and meta-
regression analysis. J Dent, 2015. 43(1): p. 42-50.
4. Salas, M.M., et al., Diet influenced tooth erosion prevalence in children and
adolescents: Results of a meta-analysis and meta-regression. J Dent, 2015. 43(8):
p. 865-75.
5. Hellwig, E. and A. Lussi, Oral hygiene products and acidic medicines. Monogr
Oral Sci, 2013. 20(2): p. 112-8.
6. Neves, B.G., et al., Are paediatric medicines risk factors for dental caries and
dental erosion? Community Dent Health, 2008. 27(1): p. 46-51.
7. Maguire, A., W. Baqir, and J.H. Nunn, Are sugars-free medicines more
erosive than sugars-containing medicines? An in vitro study of paediatric medicines
with prolonged oral clearance used regularly and long-term by children. International
journal of paediatric dentistry, 2007. 17(4): p. 231-8.
8. Linnett, V., et al., Oral health of children with gastro-esophageal reflux
disease: a controlled study. Aust Dent J, 2002. 47(2): p. 156-62.
9. Lussi, A. and T.S. Carvalho, The future of fluorides and other protective
agents in erosion prevention. Caries Res, 2015. 49 Suppl 1: p. 18-29.

87
10. Sar Sancakli, H., et al., The influence of varnish and high fluoride on erosion
and abrasion in a laboratory investigation. Aust Dent J, 2015. 60(1): p. 38-42.
11. Cochrane, N.J., et al., Ion release from calcium and fluoride containing dental
varnishes. Aust Dent J, 2014. 59(1): p. 100-5.
12. Cochrane, N.J. and E.C. Reynolds, Calcium phosphopeptides -- mechanisms
of action and evidence for clinical efficacy. Adv Dent Res, 2012. 24(2): p. 41-7.
13. Alexandria, A.K., et al., Do pediatric medicines induce topographic changes
in dental enamel? Braz Oral Res, 2015. in press.
14. Nassur, C., et al., Characterization of a new TiF(4) and beta-cyclodextrin
inclusion complex and its in vitro evaluation on inhibiting enamel demineralization.
Arch Oral Biol, 2013. 58(3): p. 239-47.
15. Costa, C.C., I.C. Almeida, and L.C. Costa Filho, Erosive effect of an
antihistamine-containing syrup on primary enamel and its reduction by fluoride
dentifrice. International journal of paediatric dentistry 2006. 16(3): p. 174-80.
16. Masoli, M. et al., The global burden of asthma: executive summary of the
GINA Dissemination Committee report. Allergy. 2004. 59(5): p. 469-78.
17. Warner, J.O. et al., Allergy Practice Worldwide: A Report by the World Allergy
Organization Specialty and Training Council. Int Arch Allergy Immunol. 2006.
139(2): p. 166–174.
18. Babu, K.L., K. Rai, and A.M. Hedge, Pediatric liquid medicaments--do they
erode the teeth surface? An in vitro study: part I. J Clin Pediatr Dent, 2008. 32(3):
p. 189-94.
19. Soares, D.N., et al., Cross-sectional microhardness of bovine enamel
subjected to three paediatric liquid oral medicines: an in vitro study. Eur Arch
Paediatr Dent, 2012. 13(5): p. 261-5.

88
20. Valinoti, A.C., et al., In vitro alterations in dental enamel exposed to acidic
medicines. Int J Paediatr Dent, 2011. 21(2): p. 141-50.
21. Valinoti, A.C., et al., Surface degradation of composite resins by acidic
medicines and pH-cycling. J Appl Oral Sci, 2008. 16(4): p. 257-65.
22. Pierro, V.S.S., et al., Effect of dilution on the pH and titratable acidity of
pediatric syrup medicines. Open Access Scientific Reports, 2013. 2(1): p. 1-4.
23. Arora, R., U. Mukherjee, and V. Arora, Erosive potential of sugar free and
sugar containing pediatric medicines given regularly and long term to children.
Indian J Pediatr, 2012. 79(6): p. 759-63.
24. Bartlett, D., Etiology and prevention of acid erosion. Compend Contin Educ
Dent, 2009. 30(9): p. 616-20.
25. Serra, M.C., D.C.F. Messias, and C.P. Turssi, Control of erosive tooth wear:
possibilities and rationale. Brazilian Oral Reserach, 2009. 23(Spec Iss 1): p. 49-55.
26. Xavier, A.F., et al., Erosive and cariogenicity potential of pediatric drugs:
study of physicochemical parameters. BMC Oral Health, 2013. 13: p. 71.
27. Alexandria, A.K., et al., Inhibition of tooth erosion and its progression by NaF
varnishes containing calcium or xylitol: An in vitro study. X, 2015. in press(X): p. X.
28. Lippert, F., Fluoride release from fluoride varnishes under acidic conditions.
J Clin Pediatr Dent, 2014. 39(1): p. 35-9.
29. Sorvari, R., et al., Effect of fluoride varnish and solution on enamel erosion in
vitro. Caries Res, 1994. 28(4): p. 227-32.
30. Murakami, C., et al., Effect of fluoride varnish and gel on dental erosion in
primary and permanent teeth. Arch Oral Biol, 2009. 54(11): p. 997-1001.
31. Reynolds, E.C., et al., Fluoride and casein phosphopeptide-amorphous
calcium phosphate. J Dent Res, 2008. 87(4): p. 344-8.

89
32. Cross, K.J., et al., Physicochemical characterization of casein
phosphopeptide-amorphous calcium phosphate nanocomplexes. J Biol Chem,
2005. 280(15): p. 15362-9.
33. Cai, F., et al., Remineralization of enamel subsurface lesions by chewing gum
with added calcium. J Dent, 2009. 37(10): p. 763-8.
34. Reynolds, E.C., Calcium phosphate-based remineralization systems:
scientific evidence? Aust Dent J, 2008. 53(3): p. 268-73.
35. Rallan, M., et al., Effect of various remineralising agents on human eroded
enamel of primary teeth. Eur Arch Paediatr Dent, 2013. 14(5): p. 313-8.
36. Poggio, C., et al., Protective effect on enamel demineralization of a CPP-ACP
paste: an AFM in vitro study. J Dent, 2009. 37(12): p. 949-54.
37. Sturkenboom, M.C., et al., Drug use in children: cohort study in three
European countries. BMJ, 2008. 337: p. a2245.

90
5. DISCUSSÃO
Novos compostos têm sido propostos na literatura, em associação ou não ao
fluoreto, como uma tentativa em se bons resultados na prevenção e controle da
desmineralização dentária (Reynolds 2009, Cochrane and Reynolds 2012). Uma
vez que, a ação benéfica dos produtos fluoretados já é conhecida (Marinho, Higgins
et al. 2002, Marinho 2009, Newbrun 2010). Dentre esses, encontram-se o xilitol e o
fosfocaseinato de cálcio, do inglês "Casein Phosphopeptide - Amorphous Calcium
Phosphate” (CPP-ACP).
O xilitol é um açúcar não acidogênico com abilidade de formar complexos com
íons cálcio (Ca2+), aumentando assim a deposição de cálcio (Ca) no esmalte
dentário (Miake, Saeki et al. 2003, Makinen 2010), além disso, pode inibir a
dissolução de cálcio e fostato (PO4) da estrutura dental (Chunmuang,
Jitpukdeebodintra et al. 2007, Vongsavan, Surarit et al. 2014).
A partir de 2008 surgiu no mercado um produto denominado RecaldentTM cujo
composto ativo é o CPP-ACP. Este é um nanocomposto que promove a
estabilização e a manutenção de cálcio e fosfato a partir do fosfato de cálcio amorfo
por parte dos peptídeos derivados da caseína do leite sem a ocorrência de
precipitação (Cross, Huq et al. 2007, Reynolds 2008). Além disso, pode existir uma
interação entre o ACP e íons fluor formando o composto CPP-ACFP, cujos
benefícios já foram relatados em alguns estudos relacionados à erosão e à cárie
dentária (Reynolds, Cai et al. 2008, Poggio, Lombardini et al. 2009, Ranjitkar,
Rodriguez et al. 2009, Turssi, Maeda et al. 2011, Prestes, Souza et al. 2013, Rallan,
Chaudhary et al. 2013, Cochrane, Shen et al. 2014, Wang, Huang et al. 2014)
Embora não tenham sido encontrados, na literatura pesquisada, estudos
avaliando a ação preventiva de vernizes a base de CPP-ACP ou vernizes a base
de xilitol em relação à erosão, erosão associada à abrasão ou erosão provocada
por medicamento líquido pediátrico, na presente tese, os resultados dos artigos 1,
2 corroboram o efeito benéfico adicional do CPP-ACP e do xilitol ao fluoreto de
sódio, uma vez que a presença desses compostos nos vernizes testados
91
protegeram o esmalte dentário contra a perda estrutural superficial. Além disso o
artigo 4 demostra o efeito do verniz a base de CPP-ACP em prevenir à erosão
promovida por refrigerante ou refrigerante associado a um medicamento líquido
pediátrico.
Diante da avaliação da topografia do esmalte por meio das análises das
imagens de MEV e de perfilometria 3D de não-contato, observou-se que a
superfície dos espécimes tratados com os vernizes de CPP-ACP/NaF e xilitol/NaF
mostraram poucos sinais de alteração superficial, quando comparada às imagens
do grupo controle negativo, apesar dos resultados para o verniz de CPP-ACP/NaF
terem sido melhores que aqueles observados para os vernizes a base de xilitol/NaF
e verniz de NaF, independente da metodologia do estudo.
O verniz de xilitol/NaF se mostrou tão eficaz quanto o verniz de NaF no que
diz respeito à prevencão da erosão, da progressão da erosão e da erosão
associada à abrasão. Já o verniz a base de CPP/NaF foi mais eficaz que o verniz
de xilitol/NaF e o verniz de NaF independente do desafio.
Como o CPP-ACP possui altas concentrações de cálcio e fosfato (Cochrane
and Reynolds 2012, Cochrane, Shen et al. 2014), especula-se que a presença de
CPP-ACP no verniz de NaF promoveu a precipitação de cálcio e fosfato no esmalte
dentário além da ação do íon flúor proveniente do NaF que já é conhecida na
literatura (Wang, Megert et al. 2011, Prestes, Souza et al. 2013, de Alencar,
Magalhaes et al. 2014).
Embora o CPP-ACP seja comprovadamente efetivo na remineralização do
esmalte, existe uma carência de estudos que confirmem sua efetividade na
prevenção da erosão ou da erosão associada à abrasão dentária.

92
6. CONCLUSÕES
Com base nos resultados dos artigos que compõem a presente tese é
possível concluir que os produtos a base de CPP-ACP e de xilitol demonstraram
efeito preventivo diante dos desafios de erosão e de erosão associada à
abrasão.
6.1.1. O vernizes a base de CPP-ACP e xilitol exibiram efeito preventivo em
relação à erosão e a progressão da erosão dentária;
6.1.2. O vernizes a base de CPP-ACP e xilitol demonstraram efeito
preventivo frente à erosão associada à abrasão dentária;
6.1.3. Os medicamentos líquidos pediátricos testados apresentaram
potencial erosivo e o verniz a base de CPP-ACP demonstrou efeito
preventivo frente à erosão promovida por refrigerante ou refrigerante
associado a um medicamento líquido pediátrico.

93
REFERÊNCIAS
Alexandria, A. K., N. A. Meckelburg, U. T. Puetter, J. T. Salles, I. P. R. Souza and L. C. Maia (2015). "Do pediatric medicines induce topographic changes in dental enamel?" Braz Oral Res in press.
Amaechi, B. T., S. M. Higham and W. M. Edgar (1998). "The influence of xylitol and fluoride on dental erosion in vitro." Arch Oral Biol 43(2): 157-161.
Antunes, J. L. F. and P. C. Narvai (2010). "Politicas de saude bucal no Brasil e seu impacto sobre as desigualdades em saude." Revista Saude Publica 44(2): 360-365.
Attin, T. (2006). "Methods for assessment of dental erosion." Monogr Oral Sci 20: 152-
172.
Barbour, M. E. and A. Lussi (2014). "Erosion in relation to nutrition and the environment." Monogr Oral Sci 25: 143-154.
Chunmuang, S., S. Jitpukdeebodintra, C. Chuenarrom and P. Benjakul (2007). "Effect of xylitol and fluoride on enamel erosion in vitro." J Oral Sci 49(4): 293-297.
Cochrane, N. J. and E. C. Reynolds (2012). "Calcium phosphopeptides -- mechanisms of action and evidence for clinical efficacy." Adv Dent Res 24(2): 41-47.
Cochrane, N. J., P. Shen, Y. Yuan and E. C. Reynolds (2014). "Ion release from calcium and fluoride containing dental varnishes." Aust Dent J 59(1): 100-105.
Cross, K. J., N. L. Huq, J. E. Palamara, J. W. Perich and E. C. Reynolds (2005). "Physicochemical characterization of casein phosphopeptide-amorphous calcium phosphate nanocomplexes." J Biol Chem 280(15): 15362-15369.
Cross, K. J., N. L. Huq and E. C. Reynolds (2007). "Casein phosphopeptides in oral health chemistry and clinical applications." Curr Pharm Des 13(8): 793-800.
Cross, K. J., N. L. Huq and E. C. Reynolds (2007). "Casein phosphopeptides in oral health--chemistry and clinical applications." Curr Pharm Des 13(8): 793-800.
de Alencar, C. R., A. C. Magalhaes, M. A. de Andrade Moreira Machado, T. M. de Oliveira, H. M. Honorio and D. Rios (2014). "In situ effect of a commercial CPP-ACP chewing gum on the human enamel initial erosion." J Dent 42(11): 1502-1507.
Dijkman, T. G. and J. Arends (1988). "The role of 'CaF2-like' material in topical fluoridation of enamel in situ." Acta Odontol Scand 46(6): 391-397.
Elton, V., L. Cooper, S. M. Higham and N. Pender (2009). "Validation of enamel erosion in vitro." J Dent 37(5): 336-341.
Featherstone, J. D. (2008). "Dental caries: a dynamic disease process." Aust Dent J 53(3): 286-291.

94
Feitosa, S. A., E. A. Munchow, A. O. Al-Zain, K. Kamocki, J. A. Platt and M. C. Bottino (2015). "Synthesis and characterization of novel halloysite-incorporated adhesive resins." J Dent.
Fernandez, C. E., L. M. Tenuta, P. Zarate and J. A. Cury (2014). "Insoluble NaF in Duraphat(R) may prolong fluoride reactivity of varnish retained on dental surfaces." Braz Dent J 25(2): 160-164.
Ganss, C., A. Lussi and N. Schlueter (2014). "The histological features and physical properties of eroded dental hard tissues." Monogr Oral Sci 25: 99-107.
Gonzalez-Vidal, N., S. Muñoz-Guerra, A. M. Ilarduya, S. Benali, S. Peeterbroeck and P. Dubois (2010). "Poly(hexamethylene terephthalate)-layered silicate nanocomposites." European Polymer Journal 46(11): 156-164.
Hellwig, E. and A. Lussi (2006). "Oral hygiene products and acidic medicines." Monogr Oral Sci 20: 112-118.
Hicks, J., F. Garcia-Godoy and C. Flaitz (2004). "Biological factors in dental caries enamel structure and the caries process in the dynamic process of demineralization and remineralization (part 2)." J Clin Pediatr Dent 28(2): 119-124.
Huysmans, M. C., H. P. Chew and R. P. Ellwood (2011). "Clinical studies of dental erosion and erosive wear." Caries Res 45 Suppl 1: 60-68.
Kreulen, C. M., A. Van 't Spijker, J. M. Rodriguez, E. M. Bronkhorst, N. H. Creugers and D. W. Bartlett (2010). "Systematic review of the prevalence of tooth wear in children and adolescents." Caries Res 44(2): 151-159.
Kudiyirickal, M. G. and R. Ivancakova (2008). "Early enamel lesion part I. Classification and detection." Acta Medica 51(3): 145-149.
Levy, F. M., A. C. Magalhaes, M. F. Gomes, L. P. Comar, D. Rios and M. A. Buzalaf (2012). "The erosion and abrasion-inhibiting effect of TiF(4) and NaF varnishes and solutions on enamel in vitro." Int J Paediatr Dent 22(1): 11-16.
Levy, F. M., D. Rios, M. A. Buzalaf and A. C. Magalhaes (2014). "Efficacy of TiF4 and NaF varnish and solution: a randomized in situ study on enamel erosive-abrasive wear." Clin Oral Investig 18(4): 1097-1102.
Lippert, F. (2014). "Fluoride release from fluoride varnishes under acidic conditions." J Clin Pediatr Dent 39(1): 35-39.
Lussi, A. and T. S. Carvalho (2014). "Erosive tooth wear: a multifactorial condition of growing concern and increasing knowledge." Monogr Oral Sci 25: 1-15.
Lussi, A. and T. S. Carvalho (2015). "The future of fluorides and other protective agents in erosion prevention." Caries Res 49 Suppl 1: 18-29.
Lussi, A. and T. Jaeggi (2006). "Chemical factors." Monogr Oral Sci 20: 77-87.

95
Magalhaes, A. C., A. Wiegand, D. Rios, M. A. Buzalaf and A. Lussi (2011). "Fluoride in dental erosion." Monogr Oral Sci 22: 158-170.
Mahoney, E. K. and N. M. Kilpatrick (2003). "Dental erosion: part 1. Aetiology and prevalence of dental erosion." N Z Dent J 99(2): 33-41.
Makinen, K. K. (2010). "Sugar alcohols, caries incidence, and remineralization of caries lesions: a literature review." Int J Dent 2010: 981072.
Marinho, V. (2006). "Substantial caries-inhibiting effect of fluoride varnish suggested." Evid Based Dent 7(1): 9-10.
Marinho, V. C. (2009). "Cochrane reviews of randomized trials of fluoride therapies for preventing dental caries." European Archives of Paediatric Dentistry 10(3): 183-191.
Marinho, V. C., J. P. Higgins, S. Logan and A. Sheiham (2002). "Fluoride varnishes for preventing dental caries in children and adolescents." Cochrane Database of Systematic Reviews (3): CD002279.
Marsh, P. D. (2009). "Dental plaque as a biofilm: the significance of pH in health and caries." Compend Contin Educ Dent 30(2): 76-78, 80, 83-77; quiz 88, 90.
Miake, Y., Y. Saeki, M. Takahashi and T. Yanagisawa (2003). "Remineralization effects of xylitol on demineralized enamel." J Electron Microsc (Tokyo) 52(5): 471-476.
Mohammed, A. and K. Dusara (2013). "What is the role of topical fluoride application in preventing dental erosion?" Evid Based Dent 14(2): 59-62.
Narayanan, B. N., R. Koodathil, T. Gangadharan, Z. Yaakob, F. K. Saidu and S. Chandralayam (2010). "Preparation and characterization of exfoliated polyaniline/montmorillonite nanocomposites." Materials Science and Engineering B 168(10): 242-244.
Nassur, C., A. K. Alexandria, L. Pomarico, V. P. de Sousa, L. M. Cabral and L. C. Maia (2013). "Characterization of a new TiF(4) and beta-cyclodextrin inclusion complex and its in vitro evaluation on inhibiting enamel demineralization." Arch Oral Biol 58(3): 239-247.
Newbrun, E. (2010). "What we know and do not know about fluoride." J Public Health Dent 70(3): 227-233.
Nunes, A. M., A. A. da Silva, C. M. Alves, F. N. Hugo and C. C. Ribeiro (2014). "Factors underlying the polarization of early childhood caries within a high-risk population." BMC Public Health 14: 988.
Poggio, C., M. Lombardini, A. Dagna, M. Chiesa and S. Bianchi (2009). "Protective effect on enamel demineralization of a CPP-ACP paste: an AFM in vitro study." J Dent 37(12): 949-954.
Prestes, L., B. M. Souza, L. P. Comar, P. A. Salomao, D. Rios and A. C. Magalhaes (2013). "In situ effect of chewing gum containing CPP-ACP on the mineral precipitation of eroded bovine enamel-a surface hardness analysis." J Dent 41(8): 747-751.

96
Rallan, M., S. Chaudhary, M. Goswami, A. Sinha, R. Arora and A. Kishor (2013). "Effect of various remineralising agents on human eroded enamel of primary teeth." Eur Arch Paediatr Dent 14(5): 313-318.
Ranjitkar, S., J. M. Rodriguez, J. A. Kaidonis, L. C. Richards, G. C. Townsend and D. W. Bartlett (2009). "The effect of casein phosphopeptide-amorphous calcium phosphate on erosive enamel and dentine wear by toothbrush abrasion." J Dent 37(4): 250-254.
Reyna-valencia, A., Y. Deyrail and M. Bousmina (2010). "In situ follow-up of intercalation process in a clay/polymer nanocomposite model system by Rheo-XDR analyses." Macromolecules 43(34): 354-361.
Reynolds, E. C. (2008). "Calcium phosphate-based remineralization systems: scientific evidence?" Aust Dent J 53(3): 268-273.
Reynolds, E. C. (2009). "Casein phosphopeptide-amorphous calcium phosphate: the scientific evidence." Adv Dent Res 21(1): 25-29.
Reynolds, E. C., F. Cai, N. J. Cochrane, P. Shen, G. D. Walker, M. V. Morgan and C. Reynolds (2008). "Fluoride and casein phosphopeptide-amorphous calcium phosphate." J Dent Res 87(4): 344-348.
Rios, D., H. M. Honorio, A. C. Magalhaes, M. A. Buzalaf, R. G. Palma-Dibb, M. A. Machado and S. M. da Silva (2006). "Influence of toothbrushing on enamel softening and abrasive wear of eroded bovine enamel: an in situ study." Braz Oral Res 20(2): 148-154.
Salas, M. M., G. G. Nascimento, M. C. Huysmans and F. F. Demarco (2015). "Estimated prevalence of erosive tooth wear in permanent teeth of children and adolescents: an epidemiological systematic review and meta-regression analysis." J Dent 43(1): 42-50.
Sar Sancakli, H., R. S. Austin, F. Al-Saqabi, R. Moazzez and D. Bartlett (2015). "The influence of varnish and high fluoride on erosion and abrasion in a laboratory investigation." Aust Dent J 60(1): 38-42.
Scavuzzi, A. I., A. De Franca Caldas Junior, G. B. Couto, M. M. De Vasconcelos, R. P. De Freitas Soares and P. A. Valenca (2007). "Longitudinal study of dental caries in Brazilian children aged from 12 to 30 months." Int J Paediatr Dent 17(2): 123-128.
Shellis, R. P. and M. Addy (2014). "The interactions between attrition, abrasion and erosion in tooth wear." Monogr Oral Sci 25: 32-45.
Shellis, R. P., M. E. Barbour, A. Jesani and A. Lussi (2013). "Effects of buffering properties and undissociated acid concentration on dissolution of dental enamel in relation to pH and acid type." Caries Res 47(6): 601-611.
Shellis, R. P., J. D. Featherstone and A. Lussi (2014). "Understanding the chemistry of dental erosion." Monogr Oral Sci 25: 163-179.
Souza, J. G., I. D. Rochel, A. F. Pereira, T. C. Silva, D. Rios, M. A. Machado, M. A. Buzalaf and A. C. Magalhaes (2010). "Effects of experimental xylitol varnishes and solutions on bovine enamel erosion in vitro." J Oral Sci 52(4): 553-559.

97
Turssi, C. P., F. A. Maeda, D. C. Messias, F. C. Neto, M. C. Serra and D. Galafassi (2011). "Effect of potential remineralizing agents on acid softened enamel." Am J Dent 24(3): 165-168.
Vongsavan, K., R. Surarit and P. Rirattanapong (2014). "The combined effect of xylitol and fluoride in varnish on bovine teeth surface microhardness." Southeast Asian J Trop Med Public Health 45(2): 505-510.
Wang, C. P., S. B. Huang, Y. Liu, J. Y. Li and H. Y. Yu (2014). "The CPP-ACP relieved enamel erosion from a carbonated soft beverage: an in vitro AFM and XRD study." Arch Oral Biol 59(3): 277-282.
Wang, X., B. Megert, E. Hellwig, K. W. Neuhaus and A. Lussi (2011). "Preventing erosion with novel agents." J Dent 39(2): 163-170.
Wegehaupt, F. J. and T. Attin (2010). "The role of fluoride and casein phosphopeptide/amorphous calcium phosphate in the prevention of erosive/abrasive wear in an in vitro model using hydrochloric acid." Caries Res 44(4): 358-363.
West, N. X. and A. Joiner (2014). "Enamel mineral loss." J Dent 42 Suppl 1: S2-11.
Zero, D. T., J. van Houte and J. Russo (1986). "The intra-oral effect on enamel demineralization of extracellular matrix material synthesized from sucrose by Streptococcus mutans." J Dent Res 65(6): 918-923.







