atÉ onde É possÍvel predizer invasÃo vascular e … · ao revestimento pleural tumores t3 e t4...
TRANSCRIPT

ATÉ ONDE É POSSÍVEL
PREDIZER INVASÃO
VASCULAR E DE VIAS
AÉREAS POR IMAGEM EM
NEOPLASIA BRÔNQUICA
RODRIGO MOREIRA BELLO
RADIOLOGIA TORÁCICA
COMPLEXO HOSPITALAR SANTA CASA
HOSPITAL MOINHOS DE VENTO
SERPAL CLINICA DE DIAGNÓSTICO
PORTO ALEGRE - RS

Estadiamento Loco-regional
Avaliação T:
- Localização anatômica
- Contato / Sintopia- Invasão de estruturas adjacentes
- Invasão vascular
- Invasão Brônquica
- Invasão Mediastinal
- Invasão de Parede torácica

AVALIAÇÃO DE INVASÃO DE ESTRUTURAS
ADJACENTES:
- Estadiamento
- Ressecabilidade
- Planejamento terapêutico (cir+quimio+rxt)
Tu centrais:
- Cruzamento de fissuras interlobares
- Invasão de vasos centrais
- Invasão traqueal
IRRESSECÁVEIS

Tumores T1 e T2Em geral restritos ao pulmão e
Ao revestimento pleural
Tumores T3 e T4Invasão de estruturas mediastinais,
vasculares, de parede e da via aérea
AVALIAÇÃO DE INVASÃO DE ESTRUTURAS
ADJACENTES:
- Literatura fraca (poucos estudos bem estruturados)
- Maioria era Pré – Multidetectores (“multisclice”)
- Dados sem pixel isotrópico
- Imensa maioria décadas de 80-90 (1982-1999)
- Alguns estudos 2000...com multidetectores
- Alguns estudos com ressonância magnética
- Alguns estudos com PET-CT

Artigo 1991 – cortes TC 8 mm

Glazer HS, Kaiser LR, Anderson DJ, Molina PL, Emami B, Roper CL, et al.
Indeterminate mediastinal invasion in bronchogenic carcinoma:
CT evaluation. Radiology 1989;173:37-42.
Yokoi K, Mori K, Miyazawa N, Saito Y, Okuyama A, Sasagawa M.
Tumor invasion of the chest wall and mediastinum in lung cancer:
evaluation with pneumothorax CT. Radiology 1991;181:147-52
Shirakawa T, Fukuda K, Miyamoto Y, Tanabe H, Shimpei T.
Parietal pleural invasion of the lung masses: evaluation with CT performed
during deep inspiration and expiration. Radiology 1994;192:809-11.
. Murata K, Takahashi M, Mori M, Shimoyama K, Mishina A, Fujino I, et al.
Chest wall and mediastinal invasion by lung cancer: evaluation with multisection
expiratory dynamic CT. Radiology 1994;191:251-5.
Gefter WB. Magnetic resonance in the evaluation of lung cancer.
Semin Roentgenol 1990;25:73-84
Glazer GM, Orringer MB, Gross BH, Quint LE.
The mediastinum in non-small-cell lung cancer CT-surgical correlation. AJR 1994;142: 1101-5
Lewis JW Jr, Pearlberg JL, Beute GH, Alpern M, Kvale PA, Gross BH, et al.
Can computed tomography of the chest stage lung cancer? Yes and no. Ann Thorac Surg 1990;49:591
Harman SJ, Winton TL, Weisbrod GL, Towers MJ, Mentzer SJ.
Mediastinal invasion by bronchogenic carcinoma: CT signs. Radiology 1994; 190:841-6.

Hermam SJ, Winton TL, Weisbrod GL, Towers MJ, Mentzer SJ.
Mediastinal invasion by bronchogenic carcinoma: CT signs. Radiology 1994; 190:841-6.
Quint LE, Francis IR, Whal RL, Gross BH, Glazer GM.
Preoperative staging of non-small-cell carcinoma of the lung: imaging methods.
AJR 1995;164:1349-59
Shaffer K. Radiologic evaluation in lung cancer. Chest 1997;112:235- 8.
Webb WR, Gatsonis C, Zerhouni EA, Heelan R, Glazer GM, Francis IR, et al.
CT and MR imaging in staging non-small bronchogenic carcinoma: report of the radiologic
diagnostic oncology group. Radiology 1991;178:705-13.
Chin Jr R, Ward R, Keys J Jr, Choplin RH, Reed JC, Wallenhaupt S, et al.
Mediastinal staging of non- small-cell lung cancer with positron emission tomography.
Am J Respir Crit Care Med 1995;152:2090-6.
Yee ES, Raper SE, Thomas AN, Ebert PA.
Technical accuracy and clinical efficacy of thoracic computed tomography.
Am J Surg 1982;144:35-43.
Goldstraw P, Kurzer M, Edwards D.
Preoperative staging of lung cancer: accuracy of computed tomography x mediastinoscopy.
Thorax 1983;38:10-5.

Goldstraw P, Kurzer M, Edwards D.
Preoperative staging of lung cancer: accuracy of computed tomography x mediastinoscopy.
Thorax 1983;38:10-5.
Glazer GM, Orringer MB, Gross BH, Quint LE. The mediastinum in non-small cell lung câncer
: CT-surgical correlation. AJR 1984; 142:1101-5
Inouye SK, Sox HC. Standard and computed tomography in the evaluation of neoplasms
of the chest: a comparative efficacy assessment. Ann Intern Med 1986;105:906-24.
Patterson GA, Ginsberg RJ, Poon PY, et al.
A prospective evaluation of magnetic resonance imaging, computed tomography, and
mediastinoscopy in the preoperative assessment of mediastinal node status in bronchogenic
carcinoma. J Thorac Cardiovasc Surg 1987;94:679-84.
Kernstine KH, Stanford W, Mullan BF et al.
PET, CT, and MRI with Combidex for mediastinal staging in non-small cell lung carcinoma.
Ann Thorac Surg 1999; 68: 1022–8
Yokoi K, Mori K, Miyazawa N, Saito Y, Okuyama A, Sasagawa M.
Tumor invasion of the chest wall and mediastinum in lung cancer:
evaluation with pneumothorax CT. Radiology 1991; 181: 147–52
Gonzalez-Stawinski GV. A comparative analysis of positron emission tomography
and mediastinoscopy in staging non–small cell lung cancer.
J Thorac Cardiovasc Surg 2003;126(6):1900–5.

Há invasão vascular?
(A)Veia Cava Superior
(B) Artéria Pulmonar direita
(C)Veia ázigos
(D) invasão mediastinal
“Staging classification does not correlate
perfectly with surgical resectability”Cancer Imaging (2003) : 4 ; 15 - 18

CRESCIMENTO TUMORAL
- Hílico- Crescimento sólido, comprimindo estruturas
adjacentes
- Infiltrativo
Infiltra e invade membranas
basais e tecidos
- Lepídico
Cresce por proliferação celular e se
deposita no órgão/estrutura

The major thoracic vascular invasion of lung câncer
Soichi Oka a, * , Shuichi Shinohara a , Taiji Kuwata a , Masaru Takenaka a , Yasuhiro Chikaishi
Annals of Medicine and Surgery 20 (2017) 13e18

Klein JS, Webb WR, The radiology Staging of Lung Cancer
Journal of Thoracic Imaging 7:29-47, 1991

AVALIAR LESÃO:
- Janela Adequada
- Filtro Adequado
- Espessura Adequada
- Pixel isotrópico
- Olhar todos os Planos
- Ressonância

Se parece invasão em um corte...
Olhar o volume, sagital, coronal

Se parece invasão em um corte...
Olhar o volume, sagital, coronal

Se parece invasão em um corte...
Olhar o volume, sagital, coronal

OBJETIVAMENTE:
TC:
- Limitado contato com a estrutura
- Gordura mediastinal preservada
- < 3 cm de contato
- < 90 graus de contato circunferencial
- São razoavelmente acurados para excluir
Invasão vascular e de vias aéreas
- São critérios de ressecabilidade
Imaging of Diseases of the Chest 5th Edition Elsevier
David Hansell David LynchH. Page McAdams Alexander Bankier
Pagina 801 – Staging the primar tumor
Klein JS, Webb WR, The radiology Staging of Lung Cancer
Journal of Thoracic Imaging 7:29-47, 1991
Glazer HS, Kaiser LR, Anderson DJ, Molina PL, Emami B, Roper CL, et al.
Indeterminate mediastinal invasion in bronchogenic carcinoma:
CT evaluation. Radiology 1989;173:37-42.

RM:
- Acurácea melhor que TC multisclice*
- Vantagem em regiões específicas
- Tumor de ápice
- Invasão parede
- Invasão mediastino (“gated – cine”)
- Padrão ouro (áureo) – cirurgia
(transoperatório)
Imaging of Diseases of the Chest 5th Edition Elsevier
David Hansell David LynchH. Page McAdams Alexander Bankier
Pagina 801 – Staging the primar tumor

OBJETIVAMENTE:
CRITÉRIOS DE INVASÃO:
- borramento da gordura mediastinal
- > 3 cm de contato
- > 90 graus de contato circunferencial
- Indefinição da parede da estrutura
TC e RM:
- Boas para invasão grosseira (sens 63-90%/esp 84-86%)
- Ruins para invasão sutil (“subtle”) – sens 56-89%/esp 50-93%
Imaging of Diseases of the Chest 5th Edition Elsevier
David Hansell David LynchH. Page McAdams Alexander Bankier
Pagina 801 – Staging the primar tumor
Klein JS, Webb WR, The radiology Staging of Lung Cancer
Journal of Thoracic Imaging 7:29-47, 1991
Glazer HS, Kaiser LR, Anderson DJ, Molina PL, Emami B, Roper CL, et al.
Indeterminate mediastinal invasion in bronchogenic carcinoma:
CT evaluation. Radiology 1989;173:37-42.

CRITÉRIOS DE INVASÃO, segundo Herman:
- borramento da camada de gordura ao redor
- Ângulo de contato tumoral > 90 graus
- Estenose e deformação do lúmen vascular
Herman SJ, Winton TL, Weisbrod GL, Towers MJ, Mentzer SJ.
Mediastinal invasion by bronchogenic carcinoma: CT signs. Radiology 1994; 190:841-6.

CRITÉRIOS DE INVASÃO:
- borramento da gordura adjacente
- > 3 cm de contato
- > 90 graus de contato circunferencial
- Indefinição da parede da estrutura/Infiltração da parede
- Defeito de enchimento/endoluminal
- Irregularidade dos contornos
- “mordida” na estrutura vascular
- Estreitamento Infundibuliforme
- Importante compressão* - sinal muito fraco
Herman SJ, Winton TL, Weisbrod GL, Towers MJ, Mentzer SJ.
Mediastinal invasion by bronchogenic carcinoma: CT signs. Radiology 1994; 190:841-6.

- VPP 20% invasão em artérias
- VPP 36 % invasão em veias e átrio
387 casos cirúrgicos

Invasão de parede Invasão traqueal
Sinais inequívocos
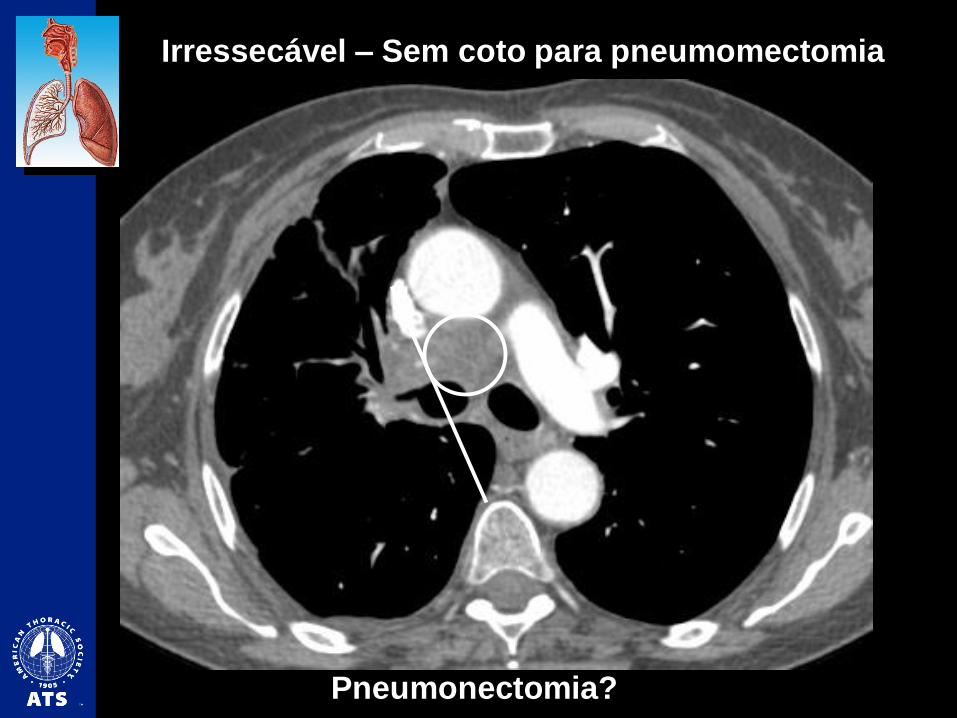
Irressecável – Sem coto para pneumomectomia
Pneumonectomia?

Invasão da VCS com trombo tumoral
Invasão mediastinal

Pitmann AG, Solomon B, Padmanabhan R, McKenzie AF, Hicks RJ.
Intra ven ous extension of lun g carcinoma to the left atrium: demonstration by positron emission
tomography with CT correlation. Br J Radiol 73:206-208, 200
Espessura parede muscular – Veias risco maior invasão
Invasão de átrio esquerdoInvasão de veias pulmonares
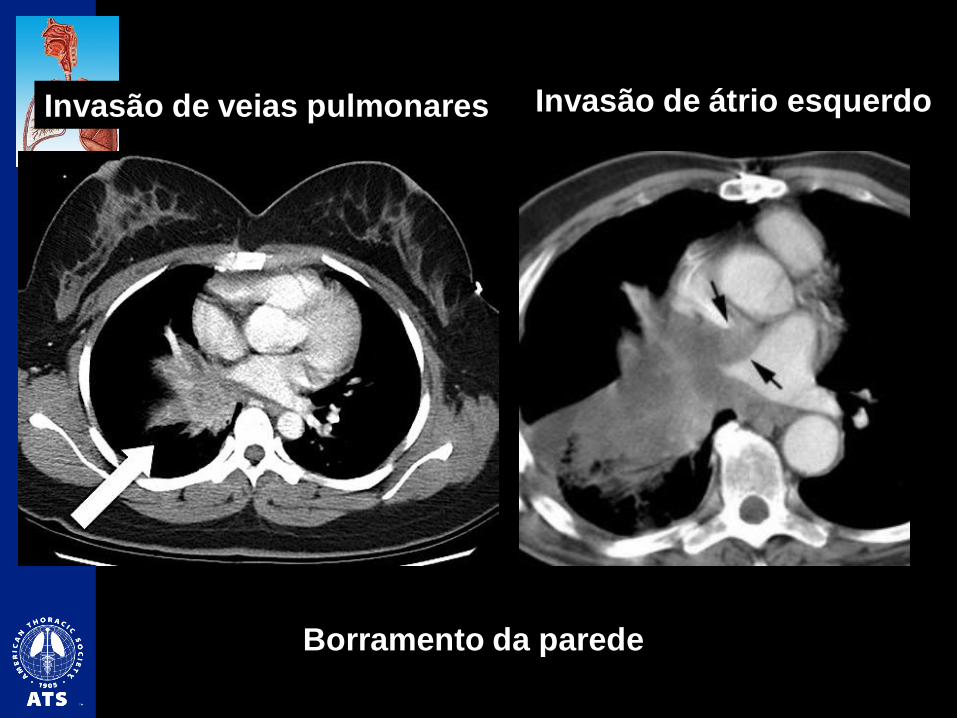
Borramento da parede
Invasão de átrio esquerdoInvasão de veias pulmonares

Contorno bem definido
Gordura preservada
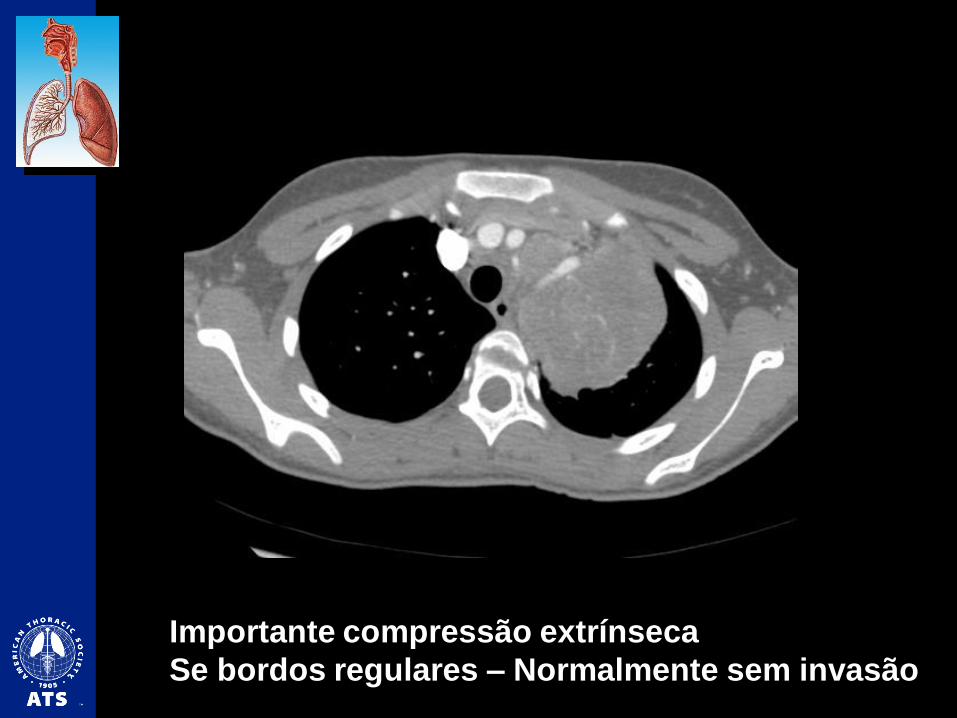
Importante compressão extrínseca
Se bordos regulares – Normalmente sem invasão

Contorno bem definido
Gordura preservada

Grande lesão justa-mediastinal à direita
Borramento gordura??
Lesão benigna - Teratoma

Defeito de enchimento – invasão / trombo tumoral
Invasão brônquica à direita
Invasão mediastinal

Invasão VCS Invasão artéria pulmonar
direita

Invasão Brônquio
Principal esquerdo
Invasão artéria pulmonar
esquerda

Obstrução VSC Invasão artéria pulmonar direita

Muito provável invasão arteria pulmonar esquerda

Lesão central
Compressão da artéria pulmonar esquerda
Não há segurança para inferir invasão

Estenose infundibuliforme

Lesão infiltrativa central - invasão artéria pulmonar esq

Borramento da parede

Defeito endoluminal sólido/vascularizado
Invasão brônquica

Infiltração da artéria do lobo superior (Boyden)

Epidermóide Sinal do brônquio “mordido”

- Invasão artéria pulmonar direita
- Invasão VCS
- Invasão brônquio principal direito

Contraste:
- Pouca diferença no estadiamento
- Melhora para avaliação de invasão grosseira
Glazer GM, Orringer MB, Gross BH, Quint LE.
The mediastinum in non-small-cell lung cancer CT-surgical correlation. AJR 1994;142: 1101-5
Lewis JW Jr, Pearlberg JL, Beute GH, Alpern M, Kvale PA, Gross BH, et al.
Can computed tomography of the chest stage lung cancer? Yes and no. Ann Thorac Surg 1990;49:591-6




RESSONÂNCIA MAGNÉTICA
Melhor resolução de contraste - tecidos

RESSONÂNCIA MAGNÉTICA
Melhor resolução de contraste - tecidos

RESSONÂNCIA MAGNÉTICA
Melhor resolução de contraste - tecidos

Marten K, Molinari F. Interstitial lung disease. In: Kauczor HU, editor. MRI of the lung.
Heidelberg: Springer Berlin Heidelberg; 2009. p. 277-91.
Ohno Y, Koyama H, Dinkel J, Hintze C. Lung Cancer. In: Kauczor HU, editor. MRI of the lung.
Heidelberg: Springer Berlin Heidelberg; 2009. p. 179-216.
RM – parece mostrar benefício
para avaliar invasão vascular

RESSONÂNCIA MAGNÉTICA
Melhor resolução de contraste - tecidos

Invasão vasos supra-aórticos







Grande lesão LSE

Invasão do mediastino?
Ausência de invasão vascular...
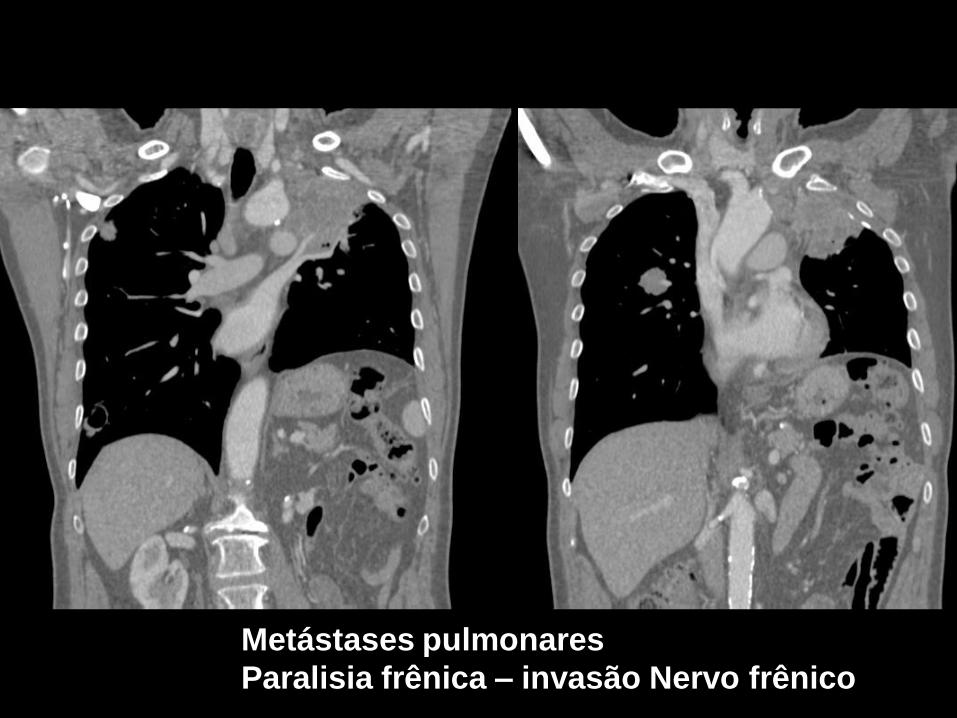
Metástases pulmonares
Paralisia frênica – invasão Nervo frênico






Lesão esofágica
Compressão e deslocamento traqueal
Porção membranosa – Invasão??

Invasão traqueal

Compressão... Invasão indeterminada

CRITÉRIOS DE INVASÃO:
- borramento da gordura adjacente
- > 3 cm de contato
- > 90 graus de contato circunferencial
- Indefinição da parede da estrutura/Infiltração da parede
- Defeito de enchimento/endoluminal
- Irregularidade dos contornos
- “mordida” na estrutura vascular
- Estreitamento Infundibuliforme
- Importante compressão* - sinal muito fraco

MUITO OBRIGADO!