universidade do estado do amazonas … apparently occurredindependently of sex, age, ... 3.3 desenho...
TRANSCRIPT

UNIVERSIDADE DO ESTADO DO AMAZONAS FUNDAÇÃO DE MEDICINA TROPICAL DO AMAZONAS
PROGRAMA DE PÓS-GRADUAÇÃO EM MEDICINA TROPICAL MESTRADO EM DOENÇAS TROPICAIS E INFECCIOSAS
PROTEÇÃO CONTRA A DIMINUIÇÃO DA HEMOGLOBINA EM ESCOLARES COM MALÁRIA POR Plasmodium vivax COINFECTADOS POR HELMINTOS
INTESTINAIS
GISELY CARDOSO DE MELO
MANAUS
2009
i
GISELY CARDOSO DE MELO
PROTEÇÃO CONTRA A DIMINUIÇÃOk DA HEMOGLOBINA EM ESCOLARES COM MALÁRIA POR Plasmodium vivax COINFECTADOS POR HELMINTOS
INTESTINAIS
Orientador: Prof. Dr. Marcus Vinícius Guimarães de Lacerda
MANAUS 2009
Dissertação apresentada ao Programa de Pós-Graduação em Medicina Tropical da Universidade do Estado do Amazonas em Convênio com a Fundação de Medicina Tropical do Amazonas, para obtenção do título de Mestre em Doenças Tropicais e Infecciosas.
FICHA CATALOGRAFICA
Melo, Gisely Cardoso de
Proteção contra a diminuição da hemoglobina em escolares contra a diminuição da hemoglobina em escolares com malária por Plasmodium vivax coinfectados por helmintos intestinais. Gisely Cardoso de Melo. - Manaus, 2009.
vii, 54p
Dissertação (Mestrado) – Universidade do Estado do Amazonas. Programa de Pós-graduação em Doenças Tropicais e Infecciosas.
Título em inglês: Protection against hemoglobin decrease in schoolchildren with Plasmodium vivax malaria and concurrent intestinal helminthic infection.
1. Plasmodium vivax. 2. Ascaris lumbricoides. 3. Hookworm. 4. Trichuris trichiura, 5.Crianças. 6.Hemoglobin.
iii
AGRADECIMENTOS
A Deus agradeço pelo dom da vida e por todas as oportunidades a mim oferecidas.
Aos meus pais Gileno e Maria Augusta (in memoriam), porque acreditaram em mim
e investiram com amor na minha formação, sempre me incentivando.
Ao meu marido Wuelton, pelo amor, compreensão e presença, mesmo nos
momentos mais difíceis.
Ao meu orientador Dr. Marcus Vinícius Guimarães de Lacerda, antes de tudo um
amigo, pela dedicação, incentivo, sabedoria, paciência e atenção durante todo esse
tempo.
À Dra Maria das Graças Vale Barbosa, pela forma com que conduz a coordenação
da pós- graduação e pelas contribuições neste trabalho.
À Dra Maria Paula Gomes Mourão e ao Dr. Emerson Silva Lima, pelas contribuições
realizadas no exame de qualificação.
Aos meus amigos Sheila Vitor da Silva, Roberto Carlos Reyes Lecca e Juscelino
Torres dos Santos pela grande ajuda durante a realização do projeto.
Aos meus amigos de mestrado em Doenças Tropicais e Infecciosas, pela
convivência e amizade conquistadas.
À Universidade do Estado do Amazonas, Fundação Muraki, Superintendência da
Zona Franca de Manaus (SUFRAMA) e Fundação de Amparo à Pesquisa do Estado
do Amazonas (FAPEAM) pelos recursos para realização deste trabalho.
A todos os funcionários da FMTAM que direta e indiretamente contribuíram para a
execução deste.
iv
RESUMO Como em diversas outras partes do mundo, na Amazônia Brasileira, as áreas de distribuição da malária coincidem com locais de alta prevalência de helmintoses intestinais. O objetivo deste trabalho foi avaliar a influência das helmintoses intestinais sobre a concentração de hemoglobina em crianças com malária por Plasmodium vivax, em áreas rurais, no Município do Careiro, na Amazônia Ocidental Brasileira. Estudo de coorte, realizado de abril a novembro de 2008, envolvendo crianças de 5 a 14 anos nas duas áreas rurais endêmicas de malária. Em abril, realizou-se uma avaliação transversal para a busca ativa de casos de malária, pelo exame da gota espessa, determinação da concentração inicial de hemoglobina e avaliação nutricional. As crianças foram seguidas durante seis meses para a detecção passiva de malária. Neste período, dos que apresentaram malária por P. vivax, foi realizada a dosagem de hemoglobina e o exame parasitológico de fezes. Dos 54 alunos com infecção única por P. vivax, a hemoglobina durante o episódio de malária foi similar à hemoglobina inicial em crianças coinfectadas com Ascaris lumbricoides (18), ancilostomídeos (11) e Trichuris trichiura (9). Para os alunos sem helmintos intestinais, uma diminuição significativa na hemoglobina no episódio de malária foi observado quando comparada com hemoglobina inicial. Isto aparentemente ocorreu independente do sexo, idade, estado nutricional, hemoglobina inicial e parasitemia da malária. Pela primeira vez, um estudo de coorte mostrou que helmintos intestinais protegem contra diminuição da hemoglobina durante episódio de malária por P. vivax. Palavras-chave: Plasmodium vivax, Ascaris lumbricoides, Ancilostomídeos, Trichuris trichiura, Crianças, Hemoglobina

v
ABSTRACT
As in many other parts of the world, in the Brazilian Amazon areas the distribution of malaria coincides with locations of high prevalence of intestinal helminthiasis. The objective of this study was to evaluate the influence of intestinal helminthiasis on the concentration of hemoglobin in children with Plasmodium vivax malaria in rural areas in the Municipality of Careiro, in the Western Brazilian Amazon. A cohort study was conducted from April to November 2008, enrolling children from 5 to 14 years old in two rural areas endemic for malaria. A cross-sectional evaluation was performed in April in order to actively detect cases of malaria, baseline hemoglobin and to assess the nutritional status. Children were followed-up for six months with passive case detection of malaria. Throughout the follow-up, from children who developed P. vivax malaria, hemoglobin dosage and stool examination (three samples in alternate days) was performed. For 54 schoolchildren with single infection by P. vivax, hemoglobin during the malaria episode was similar to the baseline hemoglobin for children co-infected with Ascaris lumbricoides (n=18), hookworm (n=11) and Trichuris trichiura (n=9). In children without intestinal helminthes, a significant decrease in the hemoglobin during the malarial attack was seen as compared to the baseline concentration. That apparently occurred independently of sex, age, nutritional status, baseline hemoglobin and peripheral Plasmodium parasitemia. For the first time, a cohort study showed that intestinal helminthes protect against hemoglobin decrease during an acute malarial attack by P. vivax. Keywords: Plasmodium vivax, Ascaris lumbricoides, Hookworm, Trichuris trichiura, Children, Hemoglobin.
vi
LISTA DE FIGURAS
Figura 1 Município de Careiro, Estado do Amazonas....................................... 06
Figura 2 Imagem Land Sat, destacando-se a localização do Projeto de Assentamento Agrícola Panelão e a Comunidade Céu Azul.............. 08
Figura 3
Representação esquemática do desenho do estudo..........................
09
Figura 1 (artigo)
Algoritmo do estudo, descrevendo os detalhes das crianças elegíveis, recrutadas e analisadas ………………………………………. 32
Figura 2 (artigo)
Média (± erro padrão da média) da concentração da hemoglobina inicial (Hb inicial) e durante (Hb na malária) o primeiro ataque agudo causado por P. vivax em 54 escolares acompanhados de abril a Novembro de 2008, em área endêmica para malária (Município do Careiro, Amazonas, Brasil), pela detecção de helmintos pelo exame parasitológico de fezes…….................................................................. 34
vii
SUMÁRIO
1 INTRODUÇÃO..................................................................................................... 01 2 OBJETIVOS........................................................................................................ 05 2.1 Geral................................................................................................................. 05 2.2 Específicos........................................................................................................ 05 3 MATERIAL E MÉTODOS.................................................................................... 06 3.1 Área de estudo.................................................................................................. 06 3.1.1 Projeto de Assentamento Panelão................................................................ 07 3.1.2 Comunidade Céu Azul................................................................................... 07 3.2 Tipo de estudo e população.............................................................................. 08 3.3 Desenho do estudo e procedimentos............................................................... 09 3.3.1 Realização da gota espessa.......................................................................... 10 3.3.2 Determinação de hemoglobina...................................................................... 10 3.3.3 Avaliação nutricional ..................................................................................... 10 3.3.4 Coproscopia................................................................................................... 11 3.3.5 Processamento e análise dos dados............................................................. 11 3.4 Considerações éticas........................................................................................ 11
4 RESULTADOS/DISCUSSÃO.............................................................................. 12 5 CONCLUSÃO...................................................................................................... 37 6 REFERÊNCIAS BIBLIOGRÁFICAS................................................................... 38 7 ANEXOS............................................................................................................. 42
7.1 Ficha clínica...................................................................................................... 42 7.2 Termo de Consentimento informado livre e esclarecido................................... 44

1
1 INTRODUÇÃO
A malária é uma doença parasitária, febril e aguda de elevada prevalência e
morbidade em diversas áreas tropicais e subtropicais do mundo (1). É talvez a mais
antiga, a mais distribuída e a mais conhecida das doenças parasitárias que
acometem o homem. Nos últimos anos, adquiriu particular importância devido à
extensa distribuição geográfica e à sua atuação como fator limitante do crescimento
demográfico, cultural e econômico em vastas áreas do mundo, particularmente nos
países em desenvolvimento (2).
Os agentes etiológicos da malária humana são protozoários pertencentes à
classe Sporozoa, família Plasmodiidae e ao gênero Plasmodium. São conhecidas
quatro espécies: Plasmodium malariae Laveran, 1881, Plasmodium falciparum
Welch, 1897, Plasmodium vivax Grassi e Feletti, 1890 e Plasmodium ovale
Stephens,1922 (3, 4). No Brasil, não há registro de autoctonia de apenas uma
espécie, o P. ovale. O P. falciparum é o responsável pelas formas mais graves e
complicadas da doença e é encontrado mais comumente nas regiões tropicais (5).
Mais de 75 % dos episódios clínicos causado pelo P. falciparum por ano concentra-
se na África (6). O P. vivax é o mais amplamente distribuído pelas zonas tropicais e
subtropicais do globo (2).
A malária continua sendo um grande problema de saúde pública em muitos
países do mundo. Há de 300 a 500 milhões de novos casos de malária, no mundo, a
cada ano, e estes resultam em 0,7 a 2,7 milhões de mortes (7). Os países mais
afetados são os africanos, situados ao sul do deserto do Saara, os do Sudeste
Asiático e os da América Latina, particularmente os situados na região da Bacia
Amazônica (8). No Brasil, no ano de 2004, quase todos os 459.013 casos eram
provenientes da região amazônica (9).
Atualmente, o P. vivax é a espécie de plasmódio mais amplamente distribuída no
mundo, causando 80-90 milhões de casos anuais. Nas Américas e na Ásia, é a
espécie mais prevalente. No Brasil, P. vivax representa mais de 80% dos casos
clínicos notificados anualmente na região amazônica (10). Em 2006, foram
registrados cerca de 396.000 casos de malária causada por essa espécie (11).

2
As infecções helmínticas constituem um importante problema de saúde pública,
especialmente nos países em desenvolvimento. As crianças são as mais atingidas e
apresentam as repercussões clínicas mais significativas da infecção. No Brasil,
diversos estudos realizados em pré-escolares e escolares mostraram elevada
prevalência de parasitoses intestinais (12, 13). Existem poucos trabalhos que se
dedicam ao estudo das infecções helmínticas na Região Amazônica. Em estudo
realizado no Estado do Acre, verificou-se que 32,5% das crianças possuíam
parasitoses intestinais (14). Em outro estudo, realizado em Santa Isabel do Rio Negro,
no Estado do Amazonas, 44% das crianças infectadas tinham carga parasitária entre
5-50.000 ovos/g de fezes (15).
É estimado que um terço da população mundial que vive em regiões tropicais e
subtropicais está infectada por helmintos e por uma ou mais espécies de plasmódio (6). Os helmintos mais freqüentes nestas associações são os geo-helmintos como
Ascaris lumbricoides, Trichuris trichiura e ancilostomídeos(16). Estudos preliminares
sugerem que um quarto de crianças em idade escolar na África estão em risco de
infecção por ancilostomídeo e P. falciparum (17). Porém, pouco se conhece sobre o
mecanismo pelo qual um parasita afeta a imunidade ou a patogênese um do outro. A
ubiqüidade destes parasitos resulta em altas freqüências de co-infecção (18).
Infecções por helmintos podem alterar a susceptibilidade para malária (19), o que tem
suscitado numerosos estudos sobre esta co-infecção, apesar de, em sua maioria,
estudarem apenas a infecção por P. falciparum (20-23).
Em experimentos laboratoriais realizados em animais de experimentação, os
resultados são conflitantes. Em estudo realizado em ratos co-infectados com
Schistosoma mansoni e Plasmodium chabaudi, verificou-se que a parasitemia
malárica era maior em ratos co-infectados do que em ratos apenas com P. chabaudi (24). Porém, em outro estudo, constatou-se que S. mansoni protege os ratos da forma
letal da infecção por P. chabaudi pelo aumento da produção de intérferon γ (INF γ ) (25).
Existem vários estudos realizados em seres humanos, na África, que chamam a
atenção para a forte associação entre infecção helmíntica e malária (26-30). Infecção
helmíntica pode amenizar(28, 29) ou exacerbar a severidade da malária (22, 31). Em
3
estudo realizado no Senegal, verificou-se que a taxa de ataque malárico foi maior
entre crianças infectadas concomitantemente com malária e S. mansoni (21). Porém,
em outro estudo, também realizado em crianças no Senegal, verificou-se que
crianças co-infectadas com S. haematobium e P. falciparum tinham menor
densidade parasitária de P. falciparum que crianças não-infectadas (32). Dois estudos
realizados em Madagascar demonstraram que o A. lumbricoides promove efeito
protetor na malária causada por P. falciparum (26, 27). Em outra pesquisa realizada em
Uganda, verificou-se que não houve aumento da susceptibilidade para malária
clínica em pacientes com infecção por helmintos (33).
Uma conseqüência importante da co-infecção malárica e helmíntica é a anemia.
É comprovado que a malária é um significante contribuinte para a ocorrência de
anemia entre crianças, por mecanismos como fagocitose e hemólise, enquanto a
infecção por ancilostomídeo é causa de anemia em função de perda sangüínea (34).
Recentemente, demonstrou-se que infecções helmínticas e malárica apresentam
impacto aditivo na redução da concentração de hemoglobina. Em um estudo
realizado na Tailândia, foi constatada uma diminuição do nível de hemoglobina em
pacientes co-infectados com malária e helmintos, associada ao agravamento da
anemia malarial (35). Em outro estudo realizado na África, foi verificado que alta carga
parasitária por helmintos em co-infecções envolvendo P. falciparum pode exacerbar
a anemia causada pela malária(36).
A anemia é uma manifestação freqüente e precoce da malária, mas, apesar de
intensamente estudada, sua patogenia continua não totalmente esclarecida. Sabe-
se que a destruição de eritrócitos, durante a infecção pelo plasmódio, envolve
mecanismos que variam em importância com a espécie do hospedeiro e do
plasmódio, e com a fase evolutiva da doença. A anemia pode decorrer da destruição
dos eritrócitos (por ação da esquizogonia intra-eritrocitária, por alterações de
membrana ou por fagocitose), de alterações da eritropoiese, do seqüestro dos
eritrócitos, ou de perda sangüínea decorrente de coagulopatia, que ocasionalmente
se associa à infecção (37). A anemia é um estado hematológico determinado por
combinações de deficiência nutricional, perda de ferro por helmintos, destruição e
diminuição da produção de eritrócitos (38, 39) e fatores genéticos como anemia
falciforme e talassemia (40).
4
São poucos os estudos com pacientes infectados por P. vivax, em parte porque
esta espécie não está relacionada freqüentemente com casos fatais. Entretanto, a
gravidade clínica por esta espécie tem aumentado nos últimos anos em várias
partes do planeta e a necessidade de conhecer a interação desta infecção tão
incidente entre nós com outras infecções sabidamente espoliantes é de extrema
necessidade, especialmente na população em idade pediátrica.
Existem poucos estudos, que avaliaram a associação entre malária e infecções
helmínticas como causa de anemia em população infantil. A literatura,
especialmente no Brasil, não apresenta dados sobre a associação de malária e
infecção por helmintos em crianças, justificando trabalhos que possam contribuir
para aumentar o conhecimento acerca da realidade local, com novos subsídios para
o estabelecimento de estratégias de prevenção e controle deste agravo.
Os trabalhos existentes apontam para a importância da associação existente
entre infecções helmínticas e malária nas crianças, especialmente aquelas com
malária vivax. Além das orientações já estabelecidas em relação à importância do
acesso rápido ao tratamento adequado na prevenção das formas graves da doença,
sugere-se que a monitorização do nível de hemoglobina pode ser importante na
avaliação do impacto das infecções helmínticas sobre a anemia causada pelo P.
vivax, justificando, mais uma vez, a realização deste trabalho.
5
2 OBJETIVOS 2.1 Geral
Avaliar a influência das helmintoses intestinais sobre a concentração de
hemoglobina em crianças com malária por Plasmodium vivax, em área rural, no
município do Careiro, Estado do Amazonas.
2.2 Específicos
- Verificar se existe diferença na concentração de hemoglobina nos casos de malária
vivax aguda com e sem helmintose intestinal.
- Verificar o estado nutricional.
- Verificar a freqüência de helmintose intestinal em crianças com malária por
Plasmodium vivax.
6
3 MATERIAL E MÉTODOS
3.1 Área de estudo
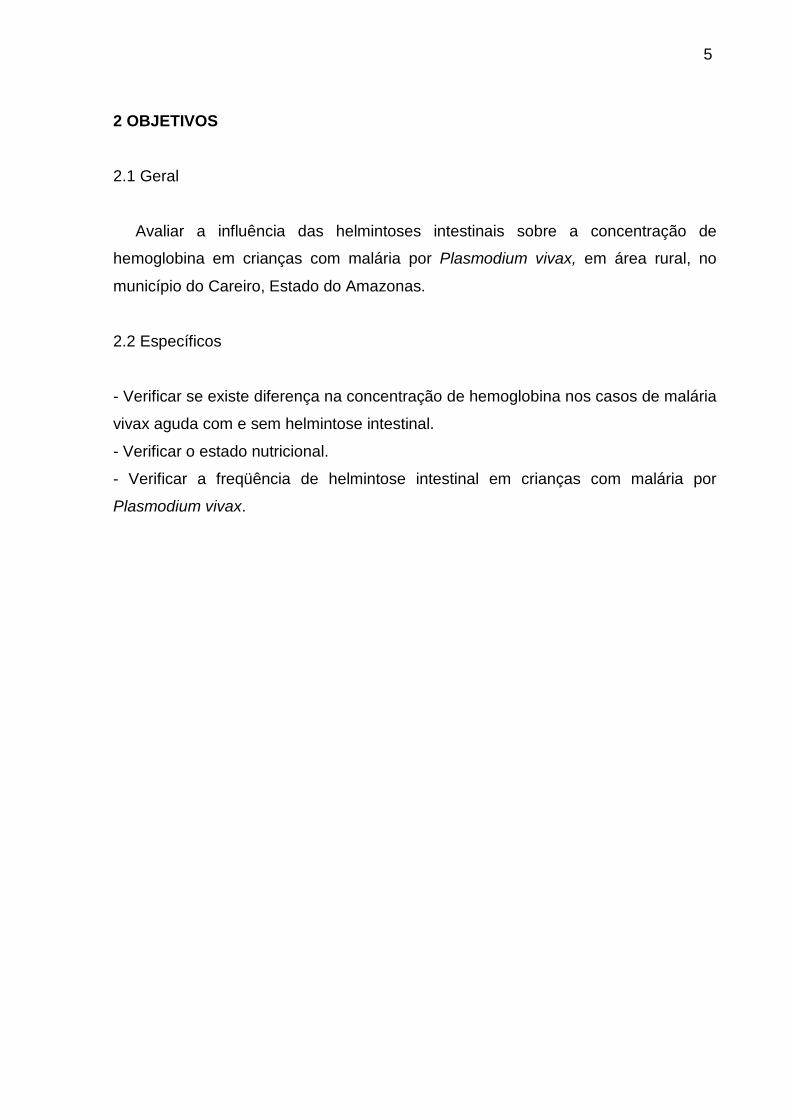
Figura 1- Município de Careiro, Estado do Amazonas.
O estudo foi desenvolvido em duas comunidades: Projeto de Assentamento
Panelão (P. A. Panelão) e na Comunidade Céu Azul, ambos localizados no
Município do Careiro, Estado do Amazonas.
O Município do Careiro está localizado na 7ª Sub-Região – Região do Rio Negro
– Solimões. Possui uma área territorial de 6.097 km². Limita-se com os municípios
de Autazes, Borba, Careiro da Várzea, Manaquiri, Iranduba, Manaus e Itacoatiara. A
sede do município possui uma distância de 112 Km, em linha reta, de Manaus
(Figura 2).
No período de 2005 a 2007, foram registrados 32.848 casos de malária no
município de Careiro. Destes, 24.517 casos foram causados pelo P. vivax, 8.041
casos por P. falciparum e 290 casos mistos. Neste período, foram notificados 9.140
casos de malária em crianças de 5 a 14 anos.
3.1.1 Projeto de Assentamento Panelão

7
O P. A. Panelão, criado pelo INCRA em 1998, localiza-se na BR 319 (Manaus-
Porto Velho), km 117, no município do Careiro. É um ramal de 9 km divididos em 6
vicinais, com aproximadamente 462 indivíduos residindo na área atualmente. Possui
como atividade econômica a agricultura. Como fonte de alimento os moradores
utilizam a caça e a pesca, além da agricultura familiar. O assentamento não
apresenta água encanada, energia elétrica, coleta de lixo e saneamento básico. A
água utilizada pelos moradores provém de cacimba ou igarapé. As vicinais que dão
acesso às moradias não são pavimentadas. As moradias são construídas de
madeira e não apresentam forro. O assentamento é cercado por mata nativa ou
modificada.
3.1.2 Comunidade Céu Azul
A comunidade Céu Azul localiza-se na BR 319 (Manaus-Porto Velho), km 140, no
Município do Careiro. Apresenta aproximadamente 328 indivíduos residindo na área
atualmente. Possui como atividade econômica a agricultura. Como fonte de alimento
os moradores utilizam a caça e a pesca, além da agricultura familiar. A comunidade
não apresenta esgoto, coleta de lixo e saneamento básico; possui energia elétrica e
asfalto. A água utilizada pelos moradores provém de cacimba ou igarapé. As
moradias são construídas de madeira sem forro ou de palha.
8
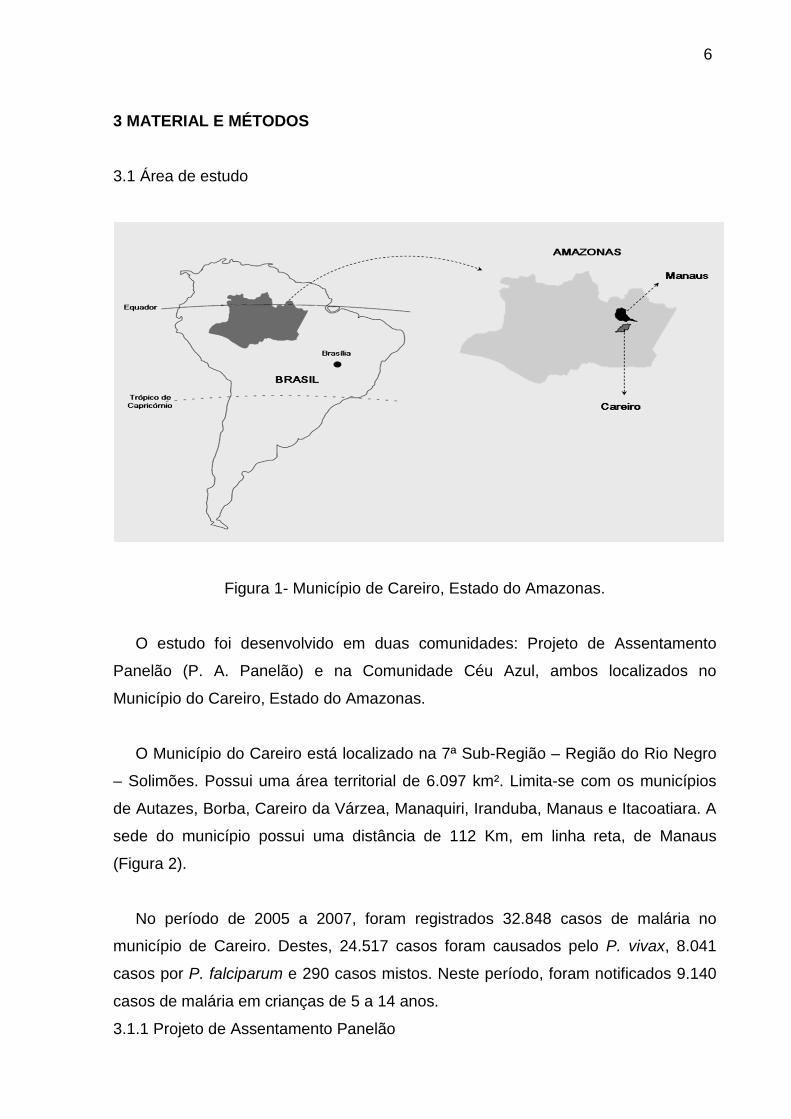
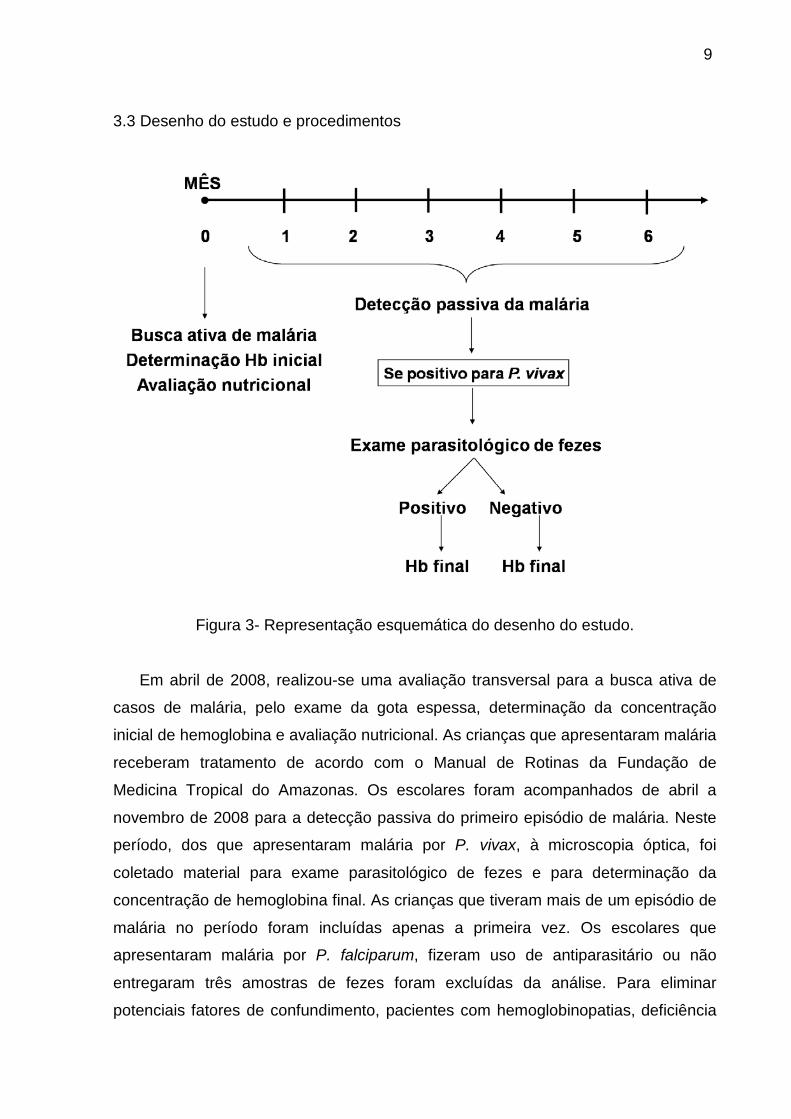
Figura 2 - Imagem Land Sat, destacando-se a localização do Projeto de Assentamento Agrícola Panelão e a Comunidade Céu Azul. Fonte: Google Earth
3.2 Tipo de estudo e população
Estudo de coorte com amostra constituída por todos os alunos de 5-14 anos,
matriculados na Escola Municipal Fred Fernandes da Silva e na Escola Municipal
Antônia Oliveira da Silva no ano letivo de 2008. No ano letivo 2008, estima-se que
na primeira escola 160 alunos encontrem-se na faixa etária do estudo, e na segunda
180 alunos, totalizando 340 crianças. Estas escolas desenvolvem atividades do
ensino fundamental, desde alfabetização até a 8ª série, com alunos de 5 a 20 anos
de idade, todos residentes nos assentamento.
Os pais ou responsáveis foram previamente informados da pesquisa e, estando
de acordo, assinaram o termo de consentimento livre e esclarecido (Anexo 7.2),
onde declararam conhecer o conteúdo do documento e entender os objetivos da
pesquisa realizada.
9
3.3 Desenho do estudo e procedimentos
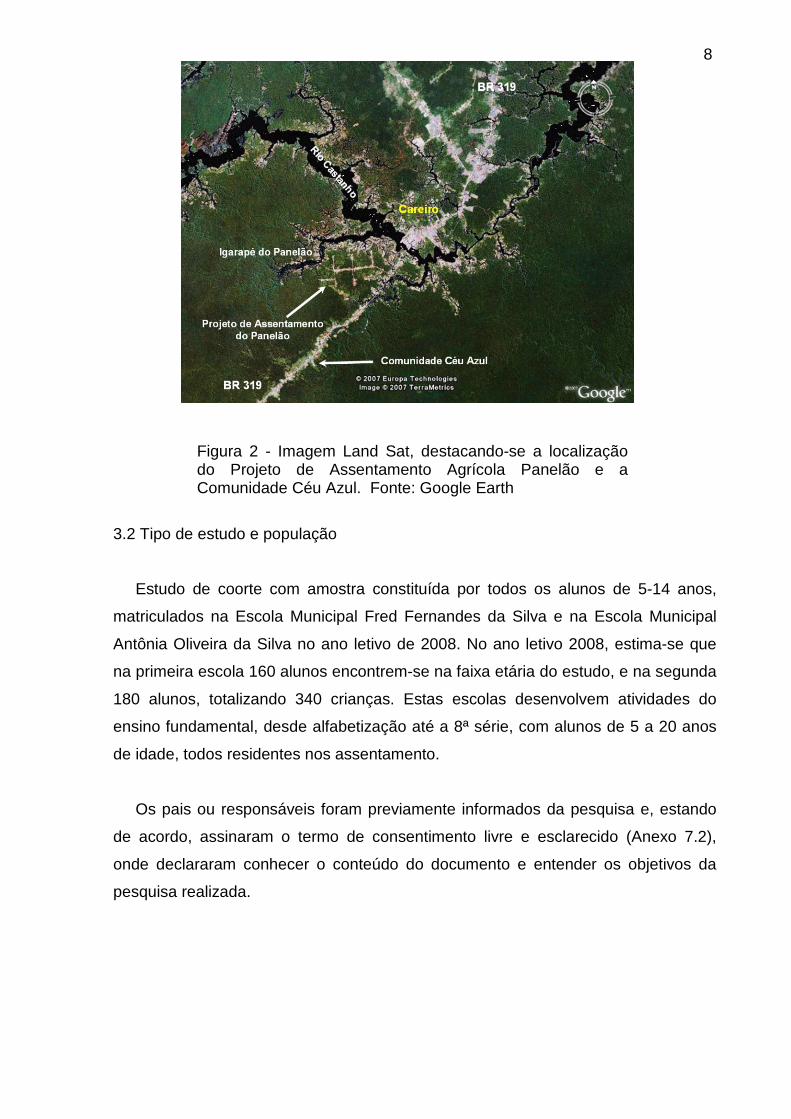
Figura 3- Representação esquemática do desenho do estudo.
Em abril de 2008, realizou-se uma avaliação transversal para a busca ativa de
casos de malária, pelo exame da gota espessa, determinação da concentração
inicial de hemoglobina e avaliação nutricional. As crianças que apresentaram malária
receberam tratamento de acordo com o Manual de Rotinas da Fundação de
Medicina Tropical do Amazonas. Os escolares foram acompanhados de abril a
novembro de 2008 para a detecção passiva do primeiro episódio de malária. Neste
período, dos que apresentaram malária por P. vivax, à microscopia óptica, foi
coletado material para exame parasitológico de fezes e para determinação da
concentração de hemoglobina final. As crianças que tiveram mais de um episódio de
malária no período foram incluídas apenas a primeira vez. Os escolares que
apresentaram malária por P. falciparum, fizeram uso de antiparasitário ou não
entregaram três amostras de fezes foram excluídas da análise. Para eliminar
potenciais fatores de confundimento, pacientes com hemoglobinopatias, deficiência
10
da glicose 6-fosfato desidrogenase e infecções mistas por P. vivax e P. falciparum
foram excluídos.
3.3.1 Realização da gota espessa
Foi realizado exame microscópico de gota espessa para pesquisa de plasmódio
corada pela técnica de Walker (9). A determinação da parasitemia foi realizada
usando uma estimativa de 5.000 leucócitos/mm3 para cada criança, quantificando as
formas parasitárias na gota espessa até o número de 100 leucócitos.
.
3.3.2 Determinação de hemoglobina
A coleta do sangue venoso das crianças foi realizada por punção digital. A
determinação da concentração de hemoglobina foi feita utilizando o sistema
HemoCue® (Anglholm, Suécia).
A técnica é baseada em uma cuveta de medição ótica de pequeno volume e
curta trajetória de luz. A cavidade da cuveta contém reagentes depositados em suas
paredes internas e a amostra de sangue é puxada para a cavidade pela força
capilar, sendo espontaneamente misturada com os reagentes. A cuveta é colocada
então em um fotômetro HemoCue no qual é medida a absorção e é calculado a
concentração de hemoglobina. A reação na cuveta é uma reação
azidametahemoglobina modificada.
3.3.3 Avaliação nutricional
O peso e a estatura foram obtidos por métodos internacionalmente
recomendados. O peso foi medido pelo uso de balança digital. A estatura foi
verificada pelo uso de uma fita métrica inelástica. Para o cálculo das relações
estatura para o Índice de Massa Corporal (IMC) utilizou-se o programa EPI-INFO
3.4.3. Para o IMC considerou-se escore Z < - 2 como desnutrição, escore Z entre –2
e < - 1 como zona de risco; escore Z entre – 1 e 2 peso normais e escore Z > 2
como obesidade.
11
3.3.4 Coproscopia
Para a realização do exame parasitológico de fezes, foram coletadas três
amostras de fezes de cada criança, em dias alternados. As amostras foram
armazenadas em frascos de boca larga com tampa, contendo formol a 10% como
conservante. Os frascos foram devidamente etiquetados com nome do paciente,
data da coleta e deixados sob temperatura ambiente até o momento da realização
do exame. Os métodos coproparasitológicos utilizados foram o método de
sedimentação espontânea e o método centrífugo-flutuação em sulfato de zinco (42).
3.3.5 Processamento e análise dos dados
Os dados epidemiológicos e os resultados dos exames foram compilados em
fichas individuais (Anexo 7.1). Os dados epidemiológicos foram obtidos por
questionário aplicado por um único pesquisador na primeira visita. A análise foi feita
no programa estatístico SPSS para Windows® PC versão 16.0. Para verificar a
normalidade dos dados foi utilizado o teste Kolmorov-Smirnov. O teste Qui-quadrado
ou teste de Fisher foi utilizado para comparação de proporções e o teste t Student
para comparação de médias. A significância foi admitida para p< 0,05.
3.4 Considerações éticas
Todos os procedimentos para a realização do estudo foram realizados após
parecer favorável do Comitê de Ética em Pesquisa com Seres Humanos da
Fundação de Medicina Tropical do Amazonas (Processo n° 0683/2008-FMT_AM).
Os pacientes diagnosticados com parasitoses intestinais e malária foram tratados de
acordo com as rotinas desta instituição.

12
4 RESULTADOS O resultado e discussão deste trabalho estão apresentados na forma de artigo
científico, apresentado a seguir, segundo as normas de publicação da Plos One,
uma vez que o artigo foi publicado nesta revista.

13
Concurrent Helminthic Infection Protects Schoolchildren with Plasmodium vivax from
Anemia
(Running title: Helminths and Vivax Malaria)
Gisely C. Melo3, Roberto C. Reyes-Lecca2, Sheila Vitor-Silva3,
Wuelton M. Monteiro3, Marilaine Martins 1,3, Silvana G. Benzecry3,
Maria G. C. Alecrim3,4, Marcus V.G. Lacerda1,3,4*
1 Tropical Medicine Foundation of Amazonas, Manaus, Brazil, 2 University of
Brasilia, Brazil, 3 University of the State of Amazonas, Manaus, Brazil, 4 Nilton Lins
Universitary Center, Manaus, Brazil
*E-mail: [email protected], Phone: + 55 92 2127 3537
Funding: This study was funded by Fundação de Amparo à Pesquisa do Estado do
Amazonas (FAPEAM) (grant number 1514-08) and by Superintendência da Zona
Franca de Manaus (SUFRAMA) (Grant number 016/2004).The funders had no role in
study design, data collection and analysis, decision to publish, or
preparation of the manuscript.
14
Abstract
Background: Plasmodium vivax is responsible for a significant portion of malaria
cases worldwide, especially in Asia and Latin America, where geo-helminthiasis have
a high prevalence. Impact of the interaction between vivax malaria and intestinal
helminthes has been poorly explored. The objective of this study was to evaluate the
influence of intestinal helminthiasis on the concentration of hemoglobin in children
with Plasmodium vivax malaria in rural areas in the municipality of Careiro, in the
Western Brazilian Amazon.
Methodology/Principal Findings: A cohort study was conducted from April to
November 2008, enrolling children from 5 to 14 years old in two rural areas endemic
for malaria. A cross-sectional evaluation was performed in April to actively detect
cases of malaria and document baseline hemoglobin and nutritional status. Children
were followed-up for six months through passive case detection of malaria based on
light microscopy. Throughout the follow-up interval, hemoglobin value and stool
examination (three samples on alternate days) were performed on children who
developed P. vivax malaria. For 54 schoolchildren with a single infection by P. vivax,
hemoglobin during the malaria episode was similar to the baseline hemoglobin for
children co-infected with Ascaris lumbricoides (n=18), hookworm (n=11) and Trichuris
trichiura (n=9). In children without intestinal helminthes, a significant decrease in the
hemoglobin during the malarial attack was seen as compared to the baseline
concentration. In the survival analysis, no difference was seen in the time (in days)
from the baseline cross-sectional to the first malarial infection, between parasitized
and non-parasitized children.
15
Conclusion/Significance: For the first time, a cohort study showed that intestinal
helminthes protect against hemoglobin decrease during an acute malarial attack by
P. vivax.
Introduction
Malaria is one of the most important public health problems in the world, with 3.3
billion people at risk of contracting the disease and almost one million deaths
annually, mainly in children under five years [1]. In Latin America, from 2000 to 2007,
7,554,993 cases of malaria were recorded, of which 5,507,167 (72.9%) were caused
by Plasmodium vivax. In this same period, 3,833,477 cases were reported in Brazil,
mainly in the Amazon Region, with the same predominance of P. vivax (76.7%) [2].
Malaria contributes to hemoglobin concentration decrease through a number of
mechanisms, primarily through destruction and removal of parasitized erythrocytes,
and a decrease in the average life span and rate of production of red blood cells [3].
In acute cases hemolysis is frequently seen, while in chronic or repeated infections
dyserythropoiesis plays an important role in the pathogenesis of anemia [4]. Few
studies are available focusing in anemia and vivax malaria in Latin America [5,6].
In Brazil, especially in the Amazon region, geo-helminthiasis have a high
prevalence [7,8]. The most common intestinal helminthes infecting people are
Ascaris lumbricoides, hookworm and Trichuris trichiura. These are widely distributed
in tropical countries, infecting 1.3, 1.4 and 1 billion people, respectively [9].
Hookworm are causative agents of anemia in humans [10,11], and infections of
moderate or high intensity by Trichuris trichiura [11,12,13] are also associated with
16
anemia. Infection by Ascaris lumbricoides influences the nutritional status [14], but its
impact on anemia is unclear.
In the Amazon region, as in many other parts of the world, endemic areas for
malaria coincide with locations of high prevalence of intestinal helminthiasis [15,16].
Recently studies have focused on the interactions between malaria and helminthiasis
co-infection. Preliminary data suggest a decrease in the severity of malaria due to P.
falciparum among those co-infected with intestinal helminthes [17].
Research on the interaction between these parasites is predominantly focused on
P. falciparum [18,19,20,21], the predominant species in Africa. However, P. vivax is
responsible for a significant portion of malaria cases worldwide, especially in Asia
and Latin America [22], and the interaction between this species and intestinal
helminthes has been poorly explored.
The objective of this study was to evaluate the influence of intestinal
helminthiasis on the hemoglobin concentration in children with P. vivax malaria in
rural areas highly endemic for malaria, in the Western Brazilian Amazon.
Methods
Area of Study
A cohort study was carried out in two schools located in two recently colonized
areas devoted to agriculture (Panelão and Céu Azul Communities), from April to
November 2008. These settlements are located in the Municipality of Careiro,
Amazonas State. The municipality has an area of 6,124.30 km2 and 31,063
inhabitants. The climate is tropical and humid, with rainfall ranging from 2,100 to
2,400mm per annum. The municipality is connected with the capital of the state,
Manaus, through a federal road (112 km of distance).
17
The total population of both communities is 790 persons, according to the census
performed before the beginning of the study. The major economical activities are family
farming, hunting and fishing. Water for drinking comes from rain water reservoirs or creeks.
Garbage collection and sanitation are absent. Two health agents in each community are
responsible for health care.
The studied population was composed of 236 schoolchildren 5 to 14 years old.
Study Design
In April 2008, a cross-sectional study was conducted to actively detect malaria
cases or asymptomatic Plasmodium carriers, establish baseline hemoglobin, assess
nutritional status. Children who had a positive thick blood smear were treated
according to the Brazilian Anti-Malarial Treatment Guidelines and not included in the
analysis afterwards. Children were followed from April to November 2008, and when
presented with measured or reported history of fever, a thick blood smear was
performed (passive case detection). In this period, children who developed the first
episode of P. vivax infection had a stool examination and hemoglobin concentration
performed on the day of the diagnosis. After the first malarial episode, the child was
not subsequently followed. Children diagnosed with P. falciparum or mixed infection
(P. vivax/P. falciparum), or those who had received anti-helminthic drugs during the
study interval, those who could not collect three samples of feces on alternate days,
or those who declined to participate in the study were excluded from the analysis. To
eliminate potential confounding factors, patients with known hemoglobinopathies,
glucose 6-phosphate dehydrogenase deficiency, and/or other chronic diseases were
excluded.
18
Diagnosis of Malaria and Parasitemia Quantitation
Thick blood smear was prepared as recommended by the Walker technique
[23] and evaluated by a local microscopist. The slides were sent to Manaus and
reviewed by an experienced microscopist, who confirmed the species and
determined the peripheral parasitemia, quantifying the asexual forms per 100
leukocytes counted in high-magnification fields, using an estimate of 5,000
leukocytes/mm3 for each child. Parasitemia was quantified as asexual parasites/mm3.
Nutritional Status Assessment
Weight and height were obtained by internationally recommended methods, as
follows. Weight was measured by use of a digital scale and height was assessed with
the help of a tape. Body Mass Index (BMI) was calculated using the program EPI-
INFO 3.4.3. BMI Z-score < -2 was defined as malnutrition, scores between -2 and Z
<- 1 as the risk zone; Z score between - 1 and 2 normal weight and Z score> 2 as
obesity [24].
Stool Examination
The search for hookworm, Ascaris lumbricoides and Trichuris trichiura was
performed by examination of three samples of stool from each child, collected on
alternate days. A single researcher performed all the exams, in order to avoid
examiner’s bias. The stool samples were stored in flasks containing 10% formalin as
preservative. Flasks were labeled with the patient's name, date of collection and kept
at room temperature until the end of the month, when all the stool samples were
examined. Spontaneous sedimentation [25] and centrifugal-flotation in zinc sulphate

19
solution [26] methods were applied before the samples were analyzed by direct
observation with a microscope.
Hemoglobin Concentration
Hemoglobin concentration was measured in venous blood obtained from
digital puncture, using a portable HemoCue® photometer (Anglholm, Sweden).
Statistical Analyses
Data were analyzed using SPSS® version 16.0 for Windows (SPSS Inc.®
Chicago, IL, USA). Normal distribution of data was evaluated with the Kolmogorov-
Smirnov test. Chi-square or Fisher's test was used to test differences in proportions,
and Student t test was used to test differences in means. Non-parametric
Spearman’s test was used for the correlation analyses. A Kaplan-Meier survival
analysis was performed in order to detect differences in the time elapsed from the
baseline cross-sectional to the first malarial episode between children with and
without intestinal helminthes. Log-rank test was used to test differences. Statistical
significance was considered if p<0.05.
Ethical Considerations
The study was approved by the Ethical Review Board of the Tropical Medicine
Foundation of Amazonas (approval number 1899). Parents´ participants were
instructed about the objectives of the study and signed an informed consent. Patients
diagnosed with intestinal parasites and malaria were treated according to the
guidelines of this institution.
20
Results
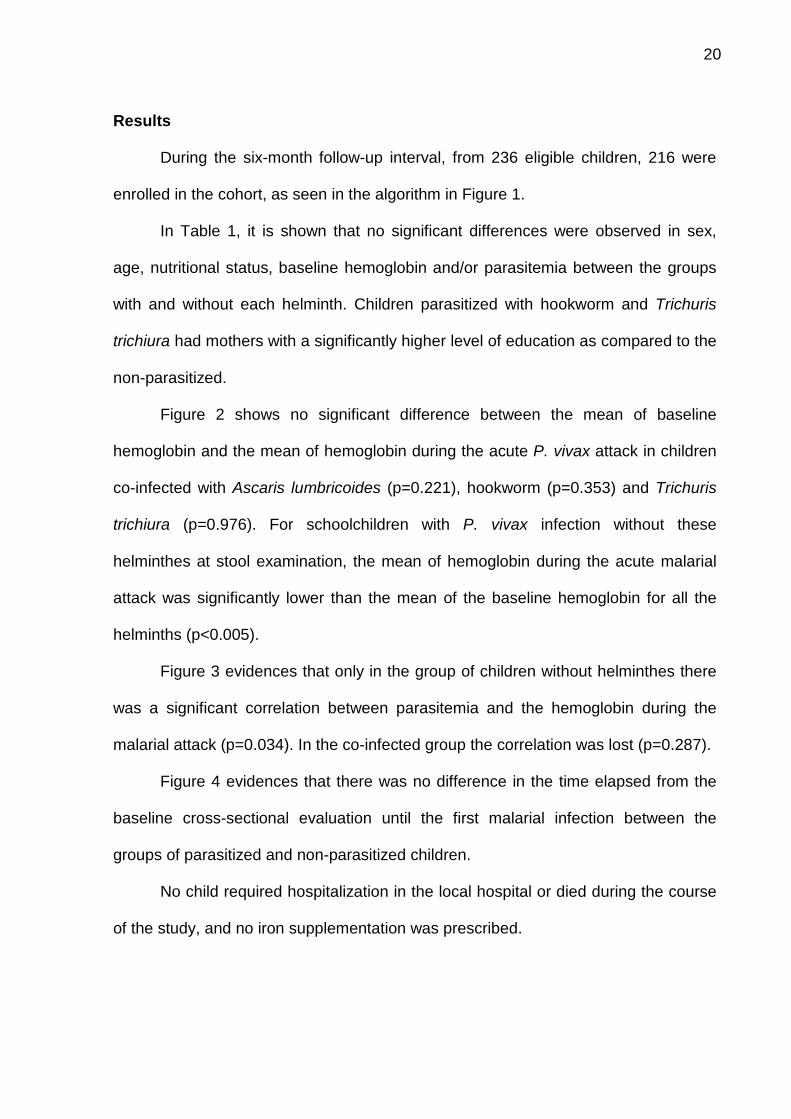
During the six-month follow-up interval, from 236 eligible children, 216 were
enrolled in the cohort, as seen in the algorithm in Figure 1.
In Table 1, it is shown that no significant differences were observed in sex,
age, nutritional status, baseline hemoglobin and/or parasitemia between the groups
with and without each helminth. Children parasitized with hookworm and Trichuris
trichiura had mothers with a significantly higher level of education as compared to the
non-parasitized.
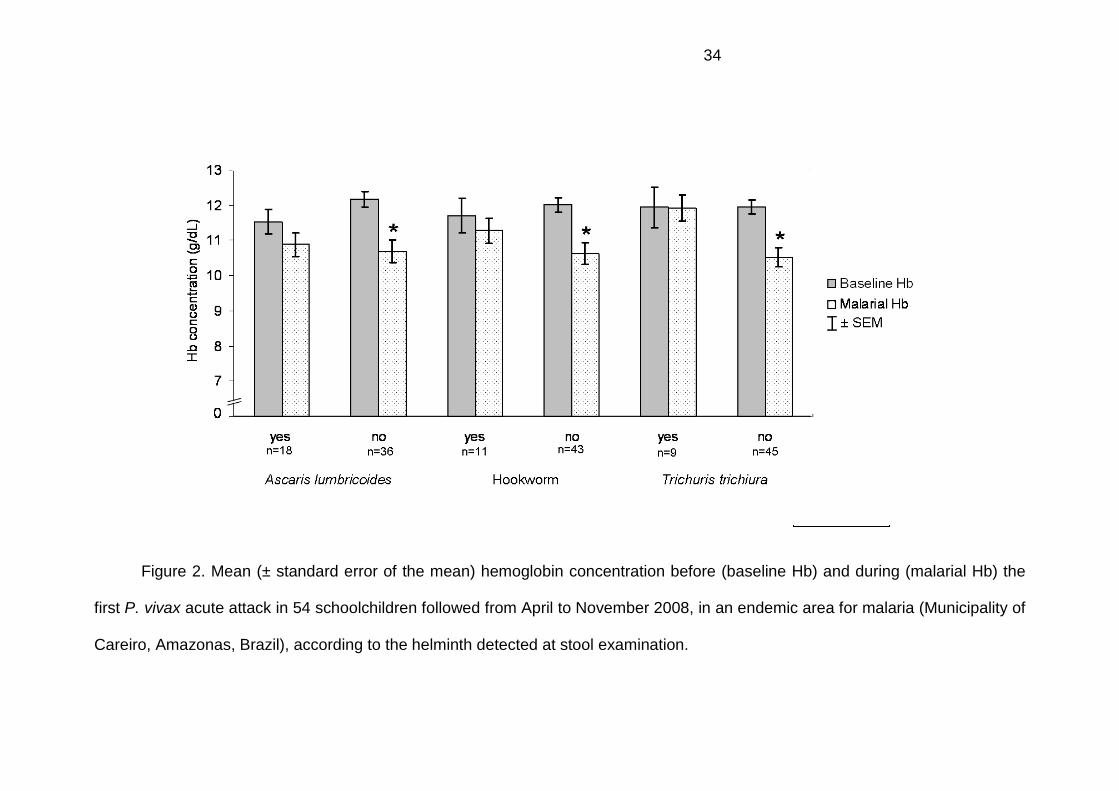
Figure 2 shows no significant difference between the mean of baseline
hemoglobin and the mean of hemoglobin during the acute P. vivax attack in children
co-infected with Ascaris lumbricoides (p=0.221), hookworm (p=0.353) and Trichuris
trichiura (p=0.976). For schoolchildren with P. vivax infection without these
helminthes at stool examination, the mean of hemoglobin during the acute malarial
attack was significantly lower than the mean of the baseline hemoglobin for all the
helminths (p<0.005).
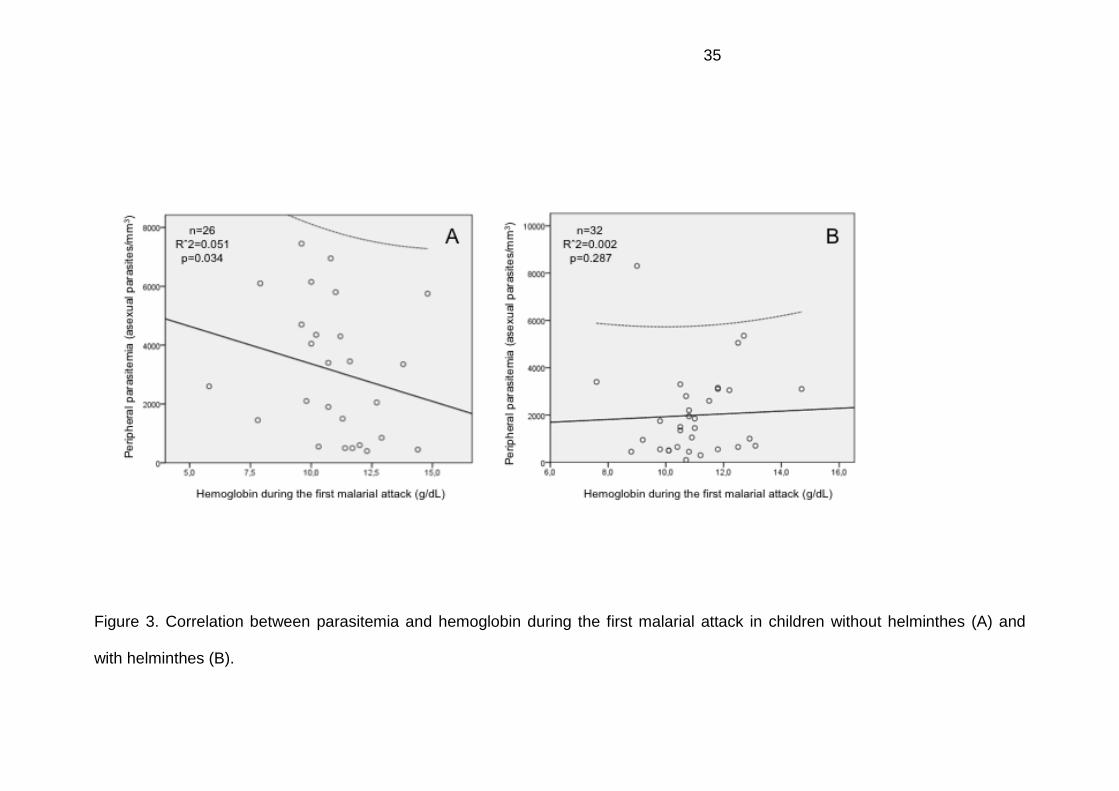
Figure 3 evidences that only in the group of children without helminthes there
was a significant correlation between parasitemia and the hemoglobin during the
malarial attack (p=0.034). In the co-infected group the correlation was lost (p=0.287).
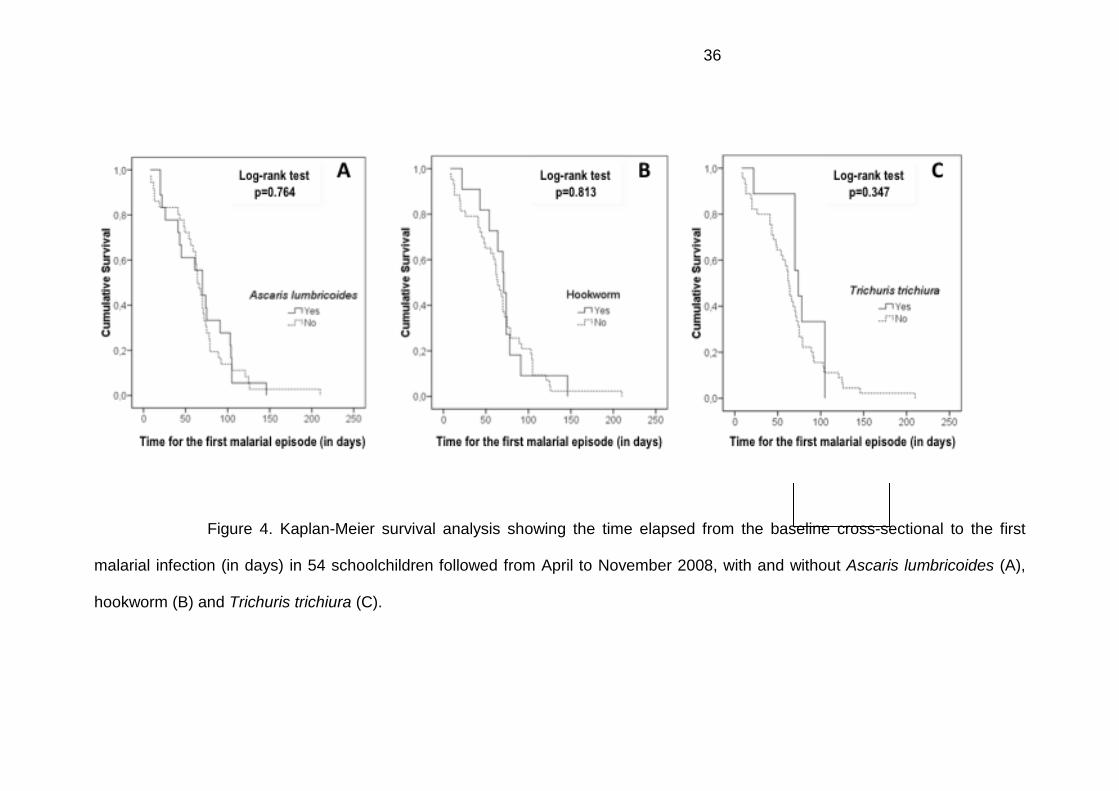
Figure 4 evidences that there was no difference in the time elapsed from the
baseline cross-sectional evaluation until the first malarial infection between the
groups of parasitized and non-parasitized children.
No child required hospitalization in the local hospital or died during the course
of the study, and no iron supplementation was prescribed.
21
Discussion
Anemia is widely distributed and often found in developing countries [27]. The
consequences of anemia are particularly severe for children and pregnant women
[28,29]. Chronic anemia during childhood is associated with retardation in physical
development, cognition and school performance [30], while severe anemia
(hemoglobin < 5g/dL) is responsible for more than half of the deaths attributed to
malaria in children under five years of age [31].
Although the etiology of anemia is complex and multifactorial, parasitic
diseases, including malaria and intestinal parasites are recognized as the major
cause of anemia in endemic countries [32,33]. There are few studies evaluating the
association between malaria and helminth infections as a cause of anemia in children
[32,34]. Although the association between helminthiasis and malaria is well
documented in endemic regions such as Africa and Asia [17,18,19,35,36,37], this
information is not available for Latin America, where P. vivax predominates and
malnutrition is not as frequent and severe as on the African Continent.
This study demonstrated that intestinal helminthiasis is associated with
protection against a decline in hemoglobin concentration during episodes of P. vivax
malaria. Previous studies have shown that helminth infections provide protection
against infection by P. falciparum [17,20,21,38,39]. The first studies on this co-
infection in the 1970s suggested that infection by A. lumbricoides was associated
with biological suppression of malaria [40,41]. More recent studies have shown that
A. lumbricoides promotes a protective effect against cerebral malaria [17] and renal
failure [42]. In Thailand, it was observed that hookworm-infected patients with mild P.
falciparum malaria had lower mean of admission temperatures than patients without
hookworm [38]. In our children, temperature was not measured because most of the
22
population was already using antipyretics when they presented to the local health
post. Using clinical severity in general as an endpoint of protection conferred by
helminths in the case of P. vivax infection would not be appropriate in our field study,
in an unstable transmission area, where no child needed hospitalization or died
during the course of the study. Further studies are needed focusing in patients from
tertiary care centers, where clinical severity is more common [43,44].
The influence of helminthic infections on malaria is not entirely straightforward.
In Madagascar, it was observed that infection by A. lumbricoides is associated with
lower parasitemia in P. falciparum malaria [20,21]. However, in Senegal, the rate of
malarial attack was higher among children co-infected with S. mansoni [45] and an
association between A. lumbricoides infection and severe malaria was found
elsewhere, despite of the loose definition of severity in this particular case [46]. In
Thailand, it was observed that helminth infections are associated with increased
incidence of P. falciparum [18]. In our study, the degree of asexual parasitemia by P.
vivax was not different between children with and without helminthiasis. This is
probably because they were diagnosed very early (diagnostic tests are available for
everyone at no cost in the community) and also because P. vivax lacks the
development of high parasitemia due to its selective reticulocyte invasion. In children
with severe falciparum malaria, co-infection with helminthes leaded to the decrease
in circulating reticulocyte counts [47]. Therefore, helminthes may also influence P.
vivax-triggered anemia through the reduction of reticulocytes, although this issue was
not addressed in our study. The presence of helminthes contributed to a lack of
association between parasitemia and hemoglobin in this group, suggesting that
helminthes may modulate the impact of parasitemia upon anemia. Recently, it was
shown that the frequency of CD4+CD25+FoxP3+ regulatory T cells correlates with P.
23
vivax parasitemia [48]. However, another study has shown that the presence of
helminthes associates with a suppressive Treg activity in vitro for P. falciparum [49].
Further studies are needed to confirm this speculation. Children with P. falciparum
infection or mixed infection (P. vivax/P. falciparum) were not analyzed as a
comparator group due to the small number of cases. An active case detection design
(using thick blood smear and PCR, and children without malaria as a control group)
could additionally identify if intestinal helminths are able to confer protection against
the clinical manifestations of the disease and/or the state of asymptomatic carrier of
the parasite.
Despite evidence that malaria/intestinal helminthiasis co-infection increases
the risk of anemia, little is known about the impact of co-infection on anemia amongst
different age groups [32]. In preschool, co-infection was associated with a lower
hemoglobin concentration as compared to children without malaria [50]. This control
group (children without malaria) was not evaluated in our study. Among
schoolchildren, hemoglobin was lower in the co-infected as opposed to children with
only one infection [51]. However, no significant difference was observed among
pregnant women, although single infections by malaria or hookworm had an impact
on the concentration of hemoglobin [52]. It is important to emphasize that all these
studies were performed using a cross-sectional study design. This poses some
difficulty in the comparison with our data. The likelihood that these differences may
be distinct in each age group is also very high, because anemia due to P. vivax
infection is mostly seen in children under 5 years of age [44]. Children this young
were not enrolled in our study.
Surprisingly, not even hookworm infection was associated with a decrease in
the hemoglobin concentration in children with malaria. Due to the anemic effect of
24
this helminth per se, we expected that in this group anemia would be more severe.
However, it is important to note that in all the groups children sometimes had more
than one helminth at stool examination, precluding an isolated analysis. Due to the
lack of a professional who could perform the Kato-Katz technique in the field to
quantify the intestinal helminth load in fresh stool, we could not evaluate for the
potential effects of intensity of helminth infection. Further studies should explore this
aspect.
A clear bias of this study could have been the longer time elapsed from the
baseline cross-sectional until the first malarial episode in children without intestinal
helminthes, subjected therefore to other determinants of anemia. However, for every
studied helminth, this time was very similar, what additionally suggests that intestinal
helminthes do not contribute to P. vivax clinical protection.
It was noted that helminthes protect against the reduction of hemoglobin
during acute malarial attacks by P. vivax. To our knowledge, this is the first report to
demonstrate the impact of helminthic co-infection on a complication triggered by P.
vivax, based on a cohort study. The mechanism by which helminthes apparently
protect against a decrease in hemoglobin in vivax malaria is unknown. One
speculates that high levels of the Th2 cytokines (IL-10) during helminth infection
counteract the Th1 cytokines (TNF) induced by malaria to prevent the development
of severe anemia [4]. The overall Th2/Th1 balance, the homeostatic role of
interleukin 10 and TGF-β as modulators of the immune response [53], and the role of
the CD23/NO pathway in reducing sequestration [17] are additional possible
mechanisms of protection against severe malaria. Other epidemiological studies are
needed to confirm our findings with a higher number of patients, and especially in
preschool children where the effect could be more evident. Studies are also
25
necessary to evaluate the effect of the intensity of helminth load on the course of P.
vivax infection.
Competing interests
The authors have declared that no competing interests exist.
Acknowledgments
We thank all the microscopists from the rural areas in the municipality of
Careiro, namely Mr. Juscelino Torres dos Santos, for his help during the collection of
stool samples.
Author contributions
Conceived and designed the experiments: GCM MGCA MVGL. Performed the
experiments: GCM SVS WMM RCRL SGB MM. Analyzed the data: GCM WMM
MVGL. Wrote the paper: GCM WMM MVGL.
References
1. WHO (2008) World malaria report 2008. Geneva.
2. PAHO (2008) Malaria in the Americas: Time Series Epidemiological Data from 2000 to
2007.
3. McDevitt MA, Xie J, Gordeuk V, Bucala R (2004) The anemia of malaria infection: role of
inflammatory cytokines. Curr Hematol Rep 3: 97-106.
4. Menendez C, Fleming AF, Alonso PL (2000) Malaria-related anaemia. Parasitol Today 16:
469-476.
26
5. Oliveira M (2004) Hematological characterization of children with vivax malaria in the
Tropical Medicine Foundation of Amazonas. Manaus: University of State of Amazonas.
6. Caicedo O, Ramirez O, Mourao MP, Ziadec J, Perez P, et al. (2009) Comparative
hematologic analysis of uncomplicated malaria in uniquely different regions of unstable
transmission in Brazil and Colombia. Am J Trop Med Hyg 80: 146-151.
7. Boia MN, da Motta LP, Salazar MD, Mutis MP, Coutinho RB, et al. (1999) Cross-
sectional study of intestinal parasites and Chagas' disease in the Municipality of Novo
Airao, State of Amazonas, Brazil. Cad Saude Publica 15: 497-504.
8. Araujo CF, Fernandez CL (2005) Prevalence of intestinal parasitosis in the city of
Eirunepe, Amazon. Rev Soc Bras Med Trop 38: 69.
9. WHO (2002) Malaria, Filariasis other parasitic diseases. Geneva.
10. Tatala S, Svanberg U, Mduma B (1998) Low dietary iron availability is a major cause of
anemia: a nutrition survey in the Lindi District of Tanzania. Am J Clin Nutr 68: 171-178.
11. Stephenson LS, Holland CV, Cooper ES (2000) The public health significance of
Trichuris trichiura. Parasitology 121 Suppl: S73-95.
12. Stephenson LS, Latham MC, Ottesen EA (2000) Malnutrition and parasitic helminth
infections. Parasitology 121 Suppl: S23-38.
13. Pearson RD (2002) An Update on the Geohelminths: Ascaris lumbricoides, Hookworms,
Trichuris trichiura, and Strongyloides stercoralis. Curr Infect Dis Rep 4: 59-64.
14. O'Lorcain P, Holland CV (2000) The public health importance of Ascaris lumbricoides.
Parasitology 121 Suppl: S51-71.
15. Buck AA, Anderson RI, MacRae AA (1978) Epidemiology of poly-parasitism. I.
Occurrence, frequency and distribution of multiple infections in rural communities in
Chad, Peru, Afghanistan, and Zaire. Tropenmed Parasitol 29: 61-70.
27
16. Petney TN, Andrews RH (1998) Multiparasite communities in animals and humans:
frequency, structure and pathogenic significance. Int J Parasitol 28: 377-393.
17. Nacher M, Gay F, Singhasivanon P, Krudsood S, Treeprasertsuk S, et al. (2000) Ascaris
lumbricoides infection is associated with protection from cerebral malaria. Parasite
Immunol 22: 107-113.
18. Nacher M, Singhasivanon P, Yimsamran S, Manibunyong W, Thanyavanich N, et al.
(2002) Intestinal helminth infections are associated with increased incidence of
Plasmodium falciparum malaria in Thailand. J Parasitol 88: 55-58.
19. Brooker S, Clements AC, Hotez PJ, Hay SI, Tatem AJ, et al. (2006) The co-distribution of
Plasmodium falciparum and hookworm among African schoolchildren. Malar J 5: 99.
20. Brutus L, Watier L, Briand V, Hanitrasoamampionona V, Razanatsoarilala H, et al. (2006)
Parasitic co-infections: does Ascaris lumbricoides protect against Plasmodium
falciparum infection? Am J Trop Med Hyg 75: 194-198.
21. Brutus L, Watier L, Hanitrasoamampionona V, Razanatsoarilala H, Cot M (2007)
Confirmation of the protective effect of Ascaris lumbricoides on Plasmodium falciparum
infection: results of a randomized trial in Madagascar. Am J Trop Med Hyg 77: 1091-
1095.
22. Mendis K, Sina BJ, Marchesini P, Carter R (2001) The neglected burden of Plasmodium
vivax malaria. Am J Trop Med Hyg 64: 97-106.
23. WHO (2006) Microscopic diagnosis of Malaria. 4th edition ed. Geneva.
24. Yang H, de Onis M (2008) Algorithms for converting estimates of child malnutrition based
on the NCHS reference into estimates based on the WHO Child Growth Standards. BMC
Pediatr 8: 19.
25. Lutz A (1919) Schistosoma mansoni e a schistosomose, segundo observações feitas no
Brasil. Mem Inst Oswaldo Cruz 11: 121-155.
28
26. Faust EC, Sawitz W, Tobie J (1939) Comparative efficiency of various techniques for the
diagnosis of protozoa and helminths in feces. J Parasitol 25: 241-262.
27. WHO (2002) Reducing risks, promoting healthy life. The World Health Report 2002.
Annex Table 3. Burden of Disease in DALYs by Cause, Sex and Mortality Stratums in
WHO Regions, Estimates for 2001. Geneva.
28. Brabin BJ, Hakimi M, Pelletier D (2001) An analysis of anemia and pregnancy-related
maternal mortality. J Nutr 131: 604S-614S; 614S-615S.
29. Crawley J (2004) Reducing the burden of anemia in infants and young children in
malaria-endemic countries of Africa: from evidence to action. Am J Trop Med Hyg 71:
25-34.
30. Grantham-McGregor S, Ani C (2001) A review of studies on the effect of iron deficiency
on cognitive development in children. J Nutr 131: 649S-666S; discussion 666S-668S.
31. Korenromp EL, Armstrong-Schellenberg JR, Williams BG, Nahlen BL, Snow RW (2004)
Impact of malaria control on childhood anaemia in Africa - a quantitative review. Trop
Med Int Health 9: 1050-1065.
32. Brooker S, Akhwale W, Pullan R, Estambale B, Clarke SE, et al. (2007) Epidemiology of
plasmodium-helminth co-infection in Africa: populations at risk, potential impact on
anemia, and prospects for combining control. Am J Trop Med Hyg 77: 88-98.
33. Ndyomugyenyi R, Kabatereine N, Olsen A, Magnussen P (2008) Malaria and hookworm
infections in relation to haemoglobin and serum ferritin levels in pregnancy in Masindi
district, western Uganda. Trans R Soc Trop Med Hyg 102: 130-136.
34. Stoltzfus RJ, Chwaya HM, Montresor A, Albonico M, Savioli L, et al. (2000) Malaria,
hookworms and recent fever are related to anemia and iron status indicators in 0- to 5-y
old Zanzibari children and these relationships change with age. J Nutr 130: 1724-1733.
29
35. Nacher M, Singhasivanon P, Gay F, Silachomroon U, Phumratanaprapin W, et al. (2001)
Contemporaneous and successive mixed Plasmodium falciparum and Plasmodium vivax
infections are associated with Ascaris lumbricoides: an immunomodulating effect? J
Parasitol 87: 912-915.
36. Nacher M, Singhasivanon P, Silachamroon U, Treeprasertsu S, Krudsood S, et al. (2001)
Association of helminth infections with increased gametocyte carriage during mild
falciparum malaria in Thailand. Am J Trop Med Hyg 65: 644-647.
37. Nacher M, Singhasivanon P, Krudsood S, Phumratanaprapin W, Vanaphan S, et al.
(2005) Inverse relationship between the number of fertilized Ascaris eggs excreted and
fever, in patients co-infected with Plasmodium vivax and Ascaris lumbricoides. Ann Trop
Med Parasitol 99: 623-625.
38. Nacher M, Singhasivanon P, Traore B, Dejvorakul S, Phumratanaprapin W, et al. (2001)
Short report: Hookworm infection is associated with decreased body temperature during
mild Plasmodium falciparum malaria. Am J Trop Med Hyg 65: 136-137.
39. Briand V, Watier L, JY LEH, Garcia A, Cot M (2005) Coinfection with Plasmodium
falciparum and Schistosoma haematobium: protective effect of schistosomiasis on
malaria in senegalese children? Am J Trop Med Hyg 72: 702-707.
40. Murray MJ, Murray AB, Murray MB, Murray CJ (1977) Parotid enlargement, forehead
edema, and suppression of malaria as nutritional consequences of ascariasis. Am J Clin
Nutr 30: 2117-2121.
41. Murray J, Murray A, Murray M, Murray C (1978) The biological suppression of malaria:
an ecological and nutritional interrelationship of a host and two parasites. Am J Clin Nutr
31: 1363-1366.
42. Nacher M, Singhasivanon P, Silachamroon U, Treeprasertsuk S, Vannaphan S, et al.
(2001) Helminth infections are associated with protection from malaria-related acute
renal failure and jaundice in Thailand. Am J Trop Med Hyg 65: 834-836.
30
43. Kochar DK, Saxena V, Singh N, Kochar SK, Kumar SV, et al. (2005) Plasmodium vivax
malaria. Emerg Infect Dis 11: 132-134.
44. Tjitra E, Anstey NM, Sugiarto P, Warikar N, Kenangalem E, et al. (2008) Multidrug-
resistant Plasmodium vivax associated with severe and fatal malaria: a prospective
study in Papua, Indonesia. PLoS Med 5: e128.
45. Sokhna C, Le Hesran JY, Mbaye PA, Akiana J, Camara P, et al. (2004) Increase of
malaria attacks among children presenting concomitant infection by Schistosoma
mansoni in Senegal. Malar J 3: 43.
46. Le Hesran JY, Akiana J, Ndiaye el HM, Dia M, Senghor P, et al. (2004) Severe malaria
attack is associated with high prevalence of Ascaris lumbricoides infection among
children in rural Senegal. Trans R Soc Trop Med Hyg 98: 397-399.
47. Nacher M, Singhasivanon P, Gay F, Phumratanaprapin W, Silachamroon U, et al. (2001)
Association of helminth infection with decreased reticulocyte counts and hemoglobin
concentration in Thai falciparum malaria. Am J Trop Med Hyg 65: 335-337.
48. Bueno LL, Morais CG, Araujo FF, Gomes JA, Correa-Oliveira R, et al. (2010)
Plasmodium vivax: induction of CD4+CD25+FoxP3+ regulatory T cells during infection
are directly associated with level of circulating parasites. PLoS ONE 5: e9623.
49. Wammes LJ, Hamid F, Wiria AE, de Gier B, Sartono E, et al. Regulatory T cells in human
geohelminth infection suppress immune responses to BCG and Plasmodium falciparum.
Eur J Immunol 40: 437-442.
50. Brooker S, Peshu N, Warn PA, Mosobo M, Guyatt HL, et al. (1999) The epidemiology of
hookworm infection and its contribution to anaemia among pre-school children on the
Kenyan coast. Trans R Soc Trop Med Hyg 93: 240-246.
51. Stephenson LS, Latham MC, Kurz KM, Kinoti SN, Oduori ML, et al. (1985) Relationships
of Schistosoma hematobium, hookworm and malarial infections and metrifonate
31
treatment to hemoglobin level in Kenyan school children. Am J Trop
Med Hyg 34: 519-528.
52. Shulman CE, Graham WJ, Jilo H, Lowe BS, New L, et al. (1996) Malaria is an important
cause of anaemia in primigravidae: evidence from a district hospital in coastal Kenya.
Trans R Soc Trop Med Hyg 90: 535-539.
53. Nacher M (2004) Interactions between worm infections and malaria. Clin Rev Allergy
Immunol 26: 85-92.

32
Figure 1. Algorithm of the study, describing the details of eligible, enrolled and analyzed
children.

33
Table 1. Baseline characteristics of 54 schoolchildren followed from April to November 2008, in an endemic area for malaria
(Municipality of Careiro, Amazonas, Brazil), according to the helminth detected at stool examination during P. vivax infection.
Ascaris lumbricoides p
Hookworm p
Trichuris trichiura p yes
n (%) no
n (%) yes
n (%) no
n (%) yes
n (%) no
n (%) Sex (n=54)
Male 12 (66.7) 14 (38.9) 0.05 5 (45.5) 21 (48.8) 0.84 4 (44.4) 22 (48.9) 1.00* Female 6 (33.3) 22 (61.1) 6 (54.5) 22 (51.2) 5 (55.6) 23 (51.1) Age (years) (n=54)
5-11 16 (88.9) 26 (72.2) 0.30* 8 (72.7) 34 (79.1) 0.70* 8 (88.9) 34 (75.6) 0.67* 12-14 2 (11.1) 10 (27.8) 3 (27.3) 9 (20.9) 1 (11.1) 11 (24.4) Mother’s education (years) (n=53)
0-4 11 (61.1) 25 (71.4) 0.45 4 (36.4) 32 (76.2) 0.03* 3 (33.3) 33 (75.0) 0.02* >5 7 (38.9) 10 (28.6) 7 (63.3) 10 (23.8) 6 (66.7) 11 (25.0) Nutritional evaluation (n=54)
Nutritional risk or malnutrition 3 (16.7) 5 (14.7) 1.00* 1 (10.0) 7 (16.7) 1.00* 0 (0.0) 8 (17.8) 0.38* Eutrophic 15 (83.3) 31 (85.3) 10 (90.0) 36 (83.3) 9 (100.0) 37 (82.2) Mean of baseline Hb (n=54) 11.5 12,1 0.12 11.7 12.0 0.52 11.9 11.9 0.97* Mean of asexual malarial parasites/mm3 (n=43) 2450.0 2740.4 0.76 1805.0 2874.2 0.33 2137.5 2737.1 0.61* Total 18 (100.0) 36 (100.0) 11 (100.0) 43 (100.0) 9 (100.0) 45 (100.0)
* Fisher test.
34
Figure 2. Mean (± standard error of the mean) hemoglobin concentration before (baseline Hb) and during (malarial Hb) the
first P. vivax acute attack in 54 schoolchildren followed from April to November 2008, in an endemic area for malaria (Municipality of
Careiro, Amazonas, Brazil), according to the helminth detected at stool examination.
35
Figure 3. Correlation between parasitemia and hemoglobin during the first malarial attack in children without helminthes (A) and
with helminthes (B).
36
Figure 4. Kaplan-Meier survival analysis showing the time elapsed from the baseline cross-sectional to the first
malarial infection (in days) in 54 schoolchildren followed from April to November 2008, with and without Ascaris lumbricoides (A),
hookworm (B) and Trichuris trichiura (C).
37
5 CONCLUSÃO
Observou-se que os helmintos protegem da diminuição da hemoglobina nos
episódios de malária por P. vivax. Trata-se da primeira observação na literatura
demonstrando o impacto de coinfecção helmíntica sobre uma complicação
desencadeada por P. vivax. São necessários outros estudos epidemiológicos para
confirmarem tal achado, com maior número de pacientes, bem como em outras
áreas.
O mecanismo pelo qual ocorreu a proteção contra a diminuição da hemoglobina
nos indivíduos coinfectados deve ser objeto de investigações futuras. Estas deverão
incluir o estudo do perfil imunológico humoral e/ou celular destas duas populações
de crianças.
É importante discutir as implicações potenciais desses achados na saúde pública
dada a escassez de estudos. Futuros estudos com outras abordagens
metodológicas podem melhorar o conhecimento sobre esta associação. Além disso,
não se conhece como a coinfecção pode influenciar no controle integrado das
helmintoses intestinais e da malária.
38
6 REFERÊNCIAS BIBLIOGRÁFICAS 1. Mutis MCS, Martinez-Espinosa FE, Albuquerque BC, Coura JR. Malária. In: Coura JR, editor. Dinâmica das Doenças infecciosas e parasitárias. Rio de Janeiro: Guanabara Koogan; 2005. p. 833-904. 2. Ferreira MS. Malária. In: Focaccia R, editor. Veronezi: tratado de infectologia. Sâo Paulo: Editora Atheneu; 2005. p. 1589-632. 3. Bruce-Chwatt LJ. Essential malariology. London: William Heinemann Medical Books; 1980. 4. Oliveira MS. Caracterização hematológica em crianças, com malária vivax, diagnosticadas e tratadas na Fundação de Medicina Tropical do Amazonas Manaus: Universidade do Estado do Amazonas; 2004. 5. Gilles HM. Morbidity and mortality from parasitic disease in the year 2000. Ann Parasitol Hum Comp. 1990;65 Suppl 1:43-4. 6. Snow RW, Guerra CA, Noor AM, Myint HY, Hay SI. The global distribution of clinical episodes of Plasmodium falciparum malaria. Nature. 2005 Mar 10;434(7030):214-7. 7. US. Centers for Disease Control and Prevention, 2004. A-Z Index: Malaria. About Malaria, Malaria Facts: Global Distribution. 2004 [cited 20/08/07]; Available from: www.cdc.gov/malaria/facts.htm#WorldMalaria 8. OPAS. Informe de la situación de los programas de malaria en las Américas. 2001 [cited 10/08/07]; Available from: www.opas.org.br 9. MS. Diretoria Técnica da Gestão, Secretaria de Vigilância em Saúde, Ministério da Saúde: Situação Epidemiológica da Malária no Brasil. 2005 [cited 10/08/07; Available from: www.saude.gov.br 10. MS. Investigação epidemiológica da malária no Brasil. 2002 [cited 2007 07/07/07]; Available from: www.saude.gov.br 11. MS. Situação epidemiológica da malária no Brasil. 2007 [cited 2008 20/02/08]; Available from: http://portal.saude.gov.br/portal/arquivos/pdf/folder_malaria_2007_web.pdf 12. Campos MR, Valencia LI, Fortes Bde P, Braga RC, Medronho Rde A. [Spatial distribution of Ascaris lumbricoides infection]. Rev Saude Publica. 2002 Feb;36(1):69-74. 13. Costa-Macedo LM, Machado-Silva JR, Rodrigues-Silva R, Oliveira LM, Vianna MSR. Enteroparasitoses em pré-escolares de comunidades favelizadas da cidade do Rio de Janeiro, Brasil. Cad Saúde Pública. 1998;14:851-55.
39
14. Muniz PT, Castro TG, Araujo TS, Nunes NB, Silva-Nunes M, Hoffmann EH, et al. Child health and nutrition in the Western Brazilian Amazon: population-based surveys in two counties in Acre State. Cad Saude Publica. 2007 Jun;23(6):1283-93. 15. Carvalho-Costa FA, Goncalves AQ, Lassance SL, Silva Neto LM, Salmazo CA, Boia MN. Giardia lamblia and other intestinal parasitic infections and their relationships with nutritional status in children in Brazilian Amazon. Rev Inst Med Trop Sao Paulo. 2007 May-Jun;49(3):147-53. 16. Brooker S, Clements AC, Bundy DA. Global epidemiology, ecology and control of soil-transmitted helminth infections. Adv Parasitol. 2006;62:221-61. 17. Brooker S, Clements AC, Hotez PJ, Hay SI, Tatem AJ, Bundy DA, et al. The co-distribution of Plasmodium falciparum and hookworm among African schoolchildren. Malar J. 2006;5:99. 18. Petney TN, Andrews RH. Multiparasite communities in animals and humans: frequency, structure and pathogenic significance. Int J Parasitol. 1998 Mar;28(3):377-93. 19. Nacher M. Malaria vaccine trials in a wormy world. Trends Parasitol. 2001 Dec;17(12):563-5. 20. Nacher M, Gay F, Singhasivanon P, Krudsood S, Treeprasertsuk S, Mazier D, et al. Ascaris lumbricoides infection is associated with protection from cerebral malaria. Parasite Immunol. 2000 Mar;22(3):107-13. 21. Sokhna C, Le Hesran JY, Mbaye PA, Akiana J, Camara P, Diop M, et al. Increase of malaria attacks among children presenting concomitant infection by Schistosoma mansoni in Senegal. Malar J. 2004 Nov 15;3:43. 22. Spiegel A, Tall A, Raphenon G, Trape JF, Druilhe P. Increased frequency of malaria attacks in subjects co-infected by intestinal worms and Plasmodium falciparum malaria. Trans R Soc Trop Med Hyg. 2003 Mar-Apr;97(2):198-9. 23. Brooker S, Akhwale W, Pullan R, Estambale B, Clarke SE, Snow RW, et al. Epidemiology of plasmodium-helminth co-infection in Africa: populations at risk, potential impact on anemia, and prospects for combining control. Am J Trop Med Hyg. 2007 Dec;77(6 Suppl):88-98. 24. Helmby H, Kullberg M, Troye-Blomberg M. Altered immune responses in mice with concomitant Schistosoma mansoni and Plasmodium chabaudi infections. Infect Immun. 1998 Nov;66(11):5167-74. 25. Yoshida A, Maruyama H, Kumagai T, Amano T, Kobayashi F, Zhang M, et al. Schistosoma mansoni infection cancels the susceptibility to Plasmodium chabaudi through induction of type 1 immune responses in A/J mice. Int Immunol. 2000 Aug;12(8):1117-25.
40
26. Brutus L, Watier L, Briand V, Hanitrasoamampionona V, Razanatsoarilala H, Cot M. Parasitic co-infections: does Ascaris lumbricoides protect against Plasmodium falciparum infection? Am J Trop Med Hyg. 2006 Aug;75(2):194-8. 27. Brutus L, Watier L, Hanitrasoamampionona V, Razanatsoarilala H, Cot M. Confirmation of the Protective Effect of Ascaris lumbricoides on Plasmodium falciparum Infection: Results of a Randomized Trial in Madagascar. Am J Trop Med Hyg. 2007 Dec;77(6):1091-5. 28. Nacher M, Singhasivanon P, Silachamroon U, Treeprasertsuk S, Vannaphan S, Traore B, et al. Helminth infections are associated with protection from malaria-related acute renal failure and jaundice in Thailand. Am J Trop Med Hyg. 2001 Dec;65(6):834-6. 29. Nacher M, Singhasivanon P, Traore B, Dejvorakul S, Phumratanaprapin W, Looareesuwan S, et al. Short report: Hookworm infection is associated with decreased body temperature during mild Plasmodium falciparum malaria. Am J Trop Med Hyg. 2001 Aug;65(2):136-7. 30. Nacher M. Comment on: Severe malaria attack is associated with high prevalence of Ascaris lumbricoides infection among children in rural Senegal. Trans R Soc Trop Med Hyg. 2005 Feb;99(2):161-3; discussion 4-5. 31. Le Hesran JY, Akiana J, Ndiaye el HM, Dia M, Senghor P, Konate L. Severe malaria attack is associated with high prevalence of Ascaris lumbricoides infection among children in rural Senegal. Trans R Soc Trop Med Hyg. 2004 Jul;98(7):397-9. 32. Briand V, Watier L, JY LEH, Garcia A, Cot M. Coinfection with Plasmodium falciparum and Schistosoma haematobium: protective effect of schistosomiasis on malaria in senegalese children? Am J Trop Med Hyg. 2005 Jun;72(6):702-7. 33. Shapiro AE, Tukahebwa EM, Kasten J, Clarke SE, Magnussen P, Olsen A, et al. Epidemiology of helminth infections and their relationship to clinical malaria in southwest Uganda. Trans R Soc Trop Med Hyg. 2005 Jan;99(1):18-24. 34. Hotez PJ, Brooker S, Bethony JM, Bottazzi ME, Loukas A, Xiao S. Hookworm infection. N Engl J Med. 2004 Aug 19;351(8):799-807. 35. Nacher M, Singhasivanon P, Gay F, Phumratanaprapin W, Silachamroon U, Looareesuwan S. Association of helminth infection with decreased reticulocyte counts and hemoglobin concentration in Thai falciparum malaria. Am J Trop Med Hyg. 2001 Oct;65(4):335-7. 36. Nkuo-Akenji TK, Chi PC, Cho JF, Ndamukong KK, Sumbele I. Malaria and helminth co-infection in children living in a malaria endemic setting of mount Cameroon and predictors of anemia. J Parasitol. 2006 Dec;92(6):1191-5. 37. Lhanos C, Flórez MH, Arévalo-Herrera M, Herrera S. Mecanismos de generación de anemia em malaria. Colomb Med. 2004;35:205-14.
41
38. Korenromp EL, Armstrong-Schellenberg JR, Williams BG, Nahlen BL, Snow RW. Impact of malaria control on childhood anaemia in Africa -- a quantitative review. Trop Med Int Health. 2004 Oct;9(10):1050-65. 39. Menendez C, Fleming AF, Alonso PL. Malaria-related anaemia. Parasitol Today. 2000 Nov;16(11):469-76. 40. Kahigwa E, Schellenberg D, Sanz S, Aponte JJ, Wigayi J, Mshinda H, et al. Risk factors for presentation to hospital with severe anaemia in Tanzanian children: a case-control study. Trop Med Int Health. 2002 Oct;7(10):823-30. 41. Carneiro IA, Drakeley CJ, Owusu-Agyei S, Mmbando B, Chandramohan D. Haemoglobin and haematocrit: is the threefold conversion valid for assessing anaemia in malaria-endemic settings? Malar J. 2007;6:67. 42. Neves DP. Parasitologia Humana. 10ª ed. São Paulo: Editora Atheneu; 2001.

42
7 ANEXOS
INFLUÊNCIA DAS HELMINTOSES INTESTINAIS SOBRE A CONCENTRAÇÃO DE HEMOGLOBINA EM CRIANÇAS COM MALÁRIA POR Plasmodium vivax
EM ASSENTAMENTO RURAL, NA AMAZÔNIA BRASILEIRA
Dissertação de Mestrado Aluna responsável: Gisely Cardoso de Melo
FICHA CLÍNICA
Data de inclusão: ........ / ........ / ........ IDENTIFICAÇÃO Nome: ..........................................................................................................................................
Registro: ....................................
Cor/Raça: 1-branca 2-parda 3-preta 4-indígena 5-amarela ........
Data de nascimento: .......... / .......... / .......... Idade: ............ anos Gênero: 1-M 2-F ........
Pai: ........................................................................................................................................................................................................................
Mãe: .....................................................................................................................................................................................................................
Residência: ....................................................................................................................................................................................................
Escola:
................................................................................................................................................................................................................ CARACTERÍSTICAS INDIVIDUAIS Local provável de infecção: ............................................................................................................................................................
1-Careiro 2- Manaus 3-Outro estado ........ Qual? .....................................................................
Há quanto tempo vive em área endêmica? 1-< 6m 2-6m-1a 3-1a-2a 4-2a-3a 5->3a .......
Já teve malária? 1-sim 2-não ....... Última vez há ..................... meses Tipo: 1-V 2-F 3-F+V 4-não sabe ........
Número de episódios prévios de malária: 1- 1-3 2- 4-6 3- 7-10 4- >10 .......
Já ficou internado com malária? 1-sim 2-não .......
Uso de alguma medicação antimalárica nos últimos 60 dias? 1-sim 2-não .......
Qual? ..................................................................................................................................................................................................................
Está apresentando diarréia? 1-sim 2-não .......
Número

43
Já fez exame de fezes? 1-sim 2-não .......
Já teve verminose? 1-sim 2-não .......
Uso de alguma medicação antiparasitária ultimamente? 1-sim 2-não .......
Qual? ..................................................................................................................................................................................................................
EXAME DA GOTA ESPESSA Exame 1- Data: ........../............./...........
Tipo de malária: 1- V 2- F 3- negativo ............
Parasitemia: 1- <½+ 2-½ + 3- + 4- ++ 5- +++ 6- ++++ ............
Esquizontes? 1-sim 2-não 3-não se aplica ...... Gametócitos? 1-sim 2-não 3-não se aplica ......
Parasitas/200 leucócitos: .................................
Exame 2- Data: ........../............./...........
Tipo de malária: 1- V 2- F 3- negativo ............
Parasitemia: 1- <½+ 2-½ + 3- + 4- ++ 5- +++ 6- ++++ ............
Esquizontes? 1-sim 2-não 3-não se aplica ...... Gametócitos? 1-sim 2-não 3-não se aplica ......
Parasitas/200 leucócitos: .................................
DOSAGEM DE HEMOGLOBINA Exame 1- Data: ......./........../........ Hemoglobina: ......................g/dL. Anemia: 1- sim 2- não ......
Exame 2 - Data: ......./........../........ Hemoglobina: ......................g/dL. Anemia: 1- sim 2- não ......
Δ Hb
EXAME PARASITOLÓGICO DE FEZES
Exame 1- Data: ......./........../........ 1-Positivo 2- Negativo ......... Parasitologia: 1-Protozoários 2- Helmintos ...........
Resultado:........................................................
CONCLUSÕES Malária? 1-sim 2-não .......
Hemoglobina? 1-sim 2-não .......
Parasitose intestinal? 1-sim 2-não .......
44
Termo de consentimento informado livre e esclarecido
NOME DA PESQUISA
INFLUÊNCIA DAS HELMINTOSES INTESTINAIS SOBRE A CONCENTRAÇÃO DE HEMOGLOBINA EM CRIANÇAS COM MALÁRIA POR Plasmodium vivax
EM ÁREA RURAL, NA AMAZÔNIA BRASILEIRA
Patrocinadores: Universidade do Estado do Amazonas (UEA)
Fundação de Medicina Tropical do Amazonas (FMT-AM)
Equipe responsável: Gisely Cardoso de Melo (Bioquímica)
Dr. Marcus Vinícius Guimarães de Lacerda (Médico)
Dra Maria das Graças Costa Alecrim (Médica)
OBJETIVO E DESCRIÇÃO DO ESTUDO
Este é um estudo que estamos fazendo na Escola Municipal Fred Fernandes da Silva e na Escola
Municipal Antônia Oliveira da Silva, com o objetivo de avaliar a influência dos vermes sobre a anemia em crianças com malária por Plasmodium vivax.
A malária é uma doença transmitida pela picada do carapanã, desde as 6 horas da tarde até as 6
horas da manhã. No Brasil existem dois tipos de malária: a malária vivax e a malária falciparum.
Nos dois tipos, o paciente pode ter só febre, mas também pode morrer se não for tratado.
Às vezes a malária pode causar anemia nas crianças o que pode favorecer o desenvolvimento da
malária grave.
Etiqueta com o código de pesquisa do paciente
A picada do carapanã (Anopheles darlingi) pode transmitir a malária vivax ou falciparum durante a
noite.
45
Para podermos estudar a associação entre verminoses e malária vivax nas crianças,
precisamos acompanhar durante 6 meses a criança na escola. Realizaremos os exames de
dosagem de hemoglobina, fezes e malária.
Para isso, é preciso que sejam colhidos, além da gota de sangue do dedo para o exame da malária,
mais uma gota de sangue do dedo para determinação da anemia e amostra de fezes para realização
do exame parasitológico de fezes.
Depois que os resultados dos exames estiverem prontos, o responsável pela criança que participar
da pesquisa poderá ver estes resultados, que ficarão sob a responsabilidade dos pesquisadores.
Os remédios para malária, que são de distribuição gratuita, vão depender do tipo da malária e da
gravidade do caso. Se a malária for grave, a criança poderá ser encaminhada ao Hospital Tropical.
As crianças que apresentarem alguma verminose receberão também tratamento gratuito.
QUAIS SÃO OS BENEFÍCIOS EM PARTICIPAR DA PESQUISA?
Além de ter uma equipe especializada em malária que vai acompanhar o aluno (a) durante todo o
ano letivo, ao participar deste estudo, ela não receberá qualquer benefício adicional, nem ganhará dinheiro, mas estará contribuindo para o estudo desta doença, que ainda mata muitas
pessoas.
Se a criança tiver algum prejuízo participando da pesquisa, os pesquisadores poderão lhe ajudar de alguma maneira, basta conversar com eles !!!!!
A malária pode dar febre, mal-estar,
calafrios, vômitos, diarréia e até
sangramento na pele, nariz ou na
boca.

46
QUEM VAI FICAR SABENDO DO RESULTADO DOS EXAMES?
A participação nesse estudo será confidencial e os resultados dos exames serão mostrados às
pessoas do Hospital Tropical que trabalham com malária, mas o nome da criança que participar
nunca será revelado.
O QUE ACONTECE SE O RESPONSÁVEL OU A CRIANÇA QUISER DESISTIR DE PARTICIPAR DA PESQUISA?
A criança que participar da pesquisa tem todo o direito de dizer que não quer mais participar. E
mesmo que isso aconteça, a criança será tratada e terá direito ao atendimento no Hospital Tropical
caso precisar.
ATENÇÃO: NENHUM PESQUISADOR PODE DEIXAR DE TRATAR BEM A CRIANÇA CASO RESPONSÁVEL OU ELA MESMA DIGA QUE NÃO QUER ENTRAR NA PESQUISA OU QUERER
SAIR DELA, DEPOIS DE ALGUNS DIAS!!!!
EU GUARDAREI COMIGO ALGUM PAPEL DIZENDO QUE A CRIANÇA PARTICIPOU DA PESQUISA?
O responsável que permitir que a criança participe da pesquisa assinará duas cópias deste documento, uma cópia ficará com o pesquisador, na Gerência de Malária, e a outra ficará com o
responsável.
E O QUE FAZER SE ACONTECER ALGUMA COISA COM A CRIANÇA DEPOIS DA PESQUISA?
Para qualquer esclarecimento ou ajuda, o paciente poderá falar com o Presidente do Comitê de Ética em Pesquisa do Hospital Tropical (grupo de pessoas que avalia os projetos de pesquisa que
são realizados em um hospital): Dr. Luiz Carlos de Lima Ferreira (Telefone: 238-1711, ramal 319) ou com a farmacêutica-bioquímica abaixo:
A farmacêutica-bioquímica Gisely Cardoso de Melo, cujo
número de telefone é 9159-8604, terá disponibilidade para
atender e esclarecer quaisquer dúvidas.
47
CONSENTIMENTO PÓS-INFORMAÇÃO
Eu, ............................................................................................................................................., pai ou
responsável pelo aluno...........................................................................................................................,
recebi a explicação de que meu filho (a) será um dos participantes dessa pesquisa e entendo todas
as suas etapas e objetivos. Se eu não souber ler ou escrever, uma pessoa de minha confiança lerá
este documento para mim e depois escreverá nesta página o meu nome e a data do preenchimento.
E por estar devidamente informado e esclarecido sobre o conteúdo deste termo, livremente, sem
qualquer pressão por parte dos pesquisadores, expresso meu consentimento para inclusão do meu
filho (a) nesta pesquisa.
........................................................................................... ........../........../.........
Assinatura do paciente Data
Impressão do polegar direito do paciente,
caso este não saiba escrever seu nome.
............................................................................................
Nome do pesquisador que conversou com o pai ou responsável
............................................................................................ ......../........../.........
Assinatura do pesquisador que conversou com o pai ou responsável Data