tumores snc: aspectos novedosos · astrocitoma pilocítico astrocitoma pilomixoide astrocitoma...
TRANSCRIPT

1.- TUMORES NEUROEPITELIALES
T. ASTROCÍTICOS
Astrocitoma pilocítico
Astrocitoma pilomixoide
Astrocitoma subepend. de cél. gigantes
Xantoastrocitoma pleomórfico
Astrocitoma difuso (Fibrilar, Protoplásmico, Gemistocítico)
Astrocitoma anaplásico
Glioblastoma - gliosarcoma
- glioblastoma de células gigantes
Gliomatosis cerebri
T. OLIGODENDROGLIALES - Oligodendroglioma
- Oligodendroglioma anaplásico
T. OLIGOASTROCITICOS - Oligoastrocitoma
- Oligoastrocitoma anaplásico
T. EPENDIMARIOS - Subependimoma
- Ependimoma Mixopapilar, Celular, Papilar,
Células claras, Tanicitico, Anaplásico
T. PLEXOS COROIDES Papiloma y Carcinoma
Papiloma Atípico de plexos coroides
OTROS TUMORES NEUROEPITELIALES - Astroblastoma
- Glioma cordoide del 3º ventrículo
- Glioma Angiocéntrico
T. NEURONALES Y MIXTOS GLIONEURONALES - Neurocitoma extraventricular
- T. glioneuronal papilar
- T. glioneuronal con rosetas del 4º ventrículo
- Gangliocitoma displásico del cerebelo, Astrocitoma
desmoplásico, infantil/ganglioglioma, T. neuroepitelial
disembrioplásico, Gangliocitoma, Ganglioglioma,
Ganglioglioma anaplásico, Neurocitoma central,
Liponeurocitoma cerebeloso, Paraganglioma
T. REGIÓN PINEAL - T. papilar de la región pineal
- Pineocitoma
- Pineoblastoma
- T. parenquima pineal con diferenciación intermedia
T. EMBRIONARIOS - Meduloblastoma (desmoplásico nodular, intensa
nodularidad, anaplásico, células grandes)
- PNET
- T. teratoide/rabdoide Atípico
Louis DN et al. 2007. IARC, Lyon, France
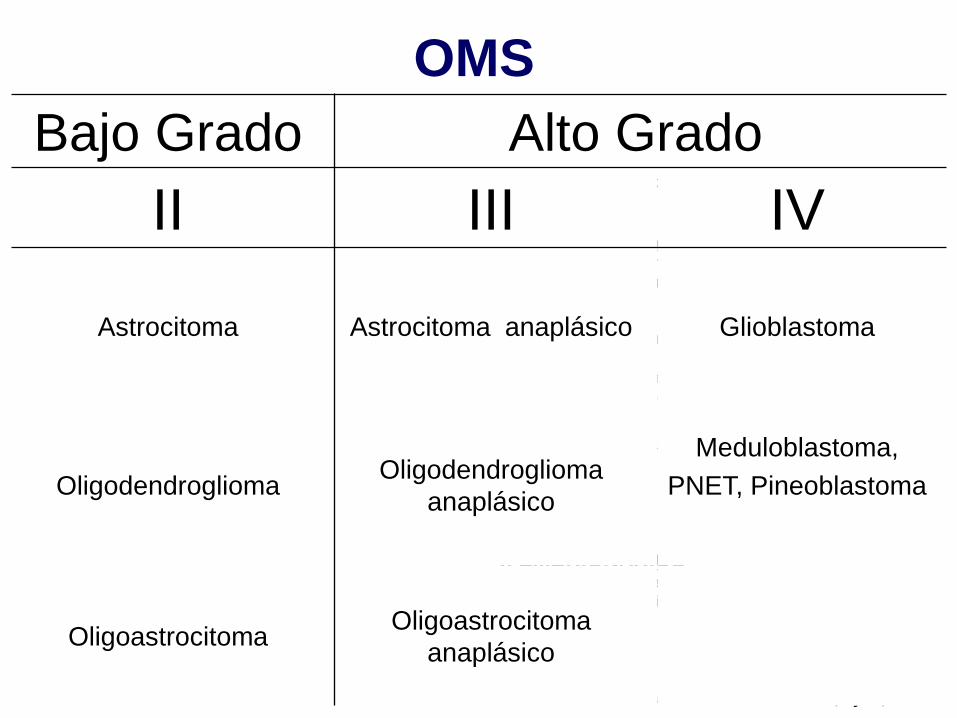
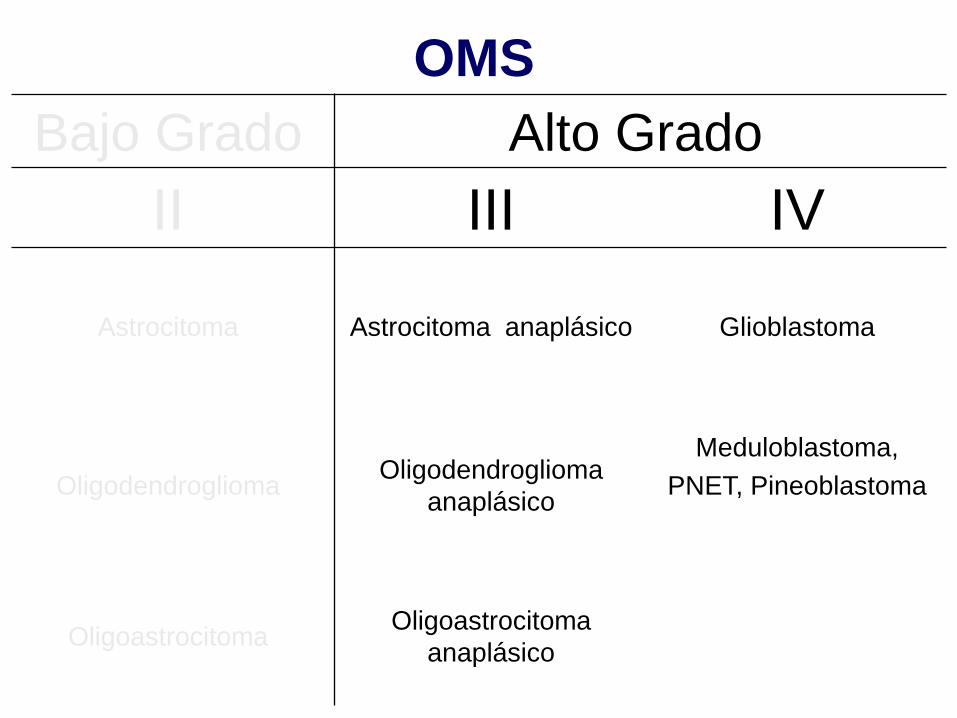
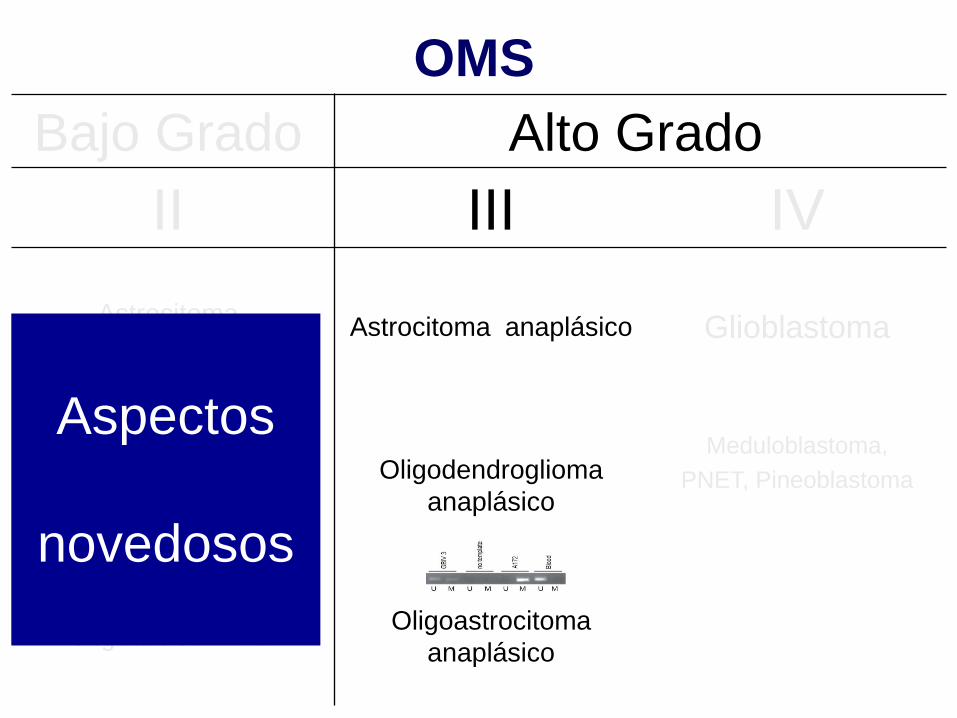
OMS
Bajo Grado Alto Grado
II III IV
Astrocitoma Astrocitoma anaplásico Glioblastoma
Oligodendroglioma Oligodendroglioma
anaplásico
Meduloblastoma,
PNET, Pineoblastoma
Oligoastrocitoma Oligoastrocitoma
anaplásico
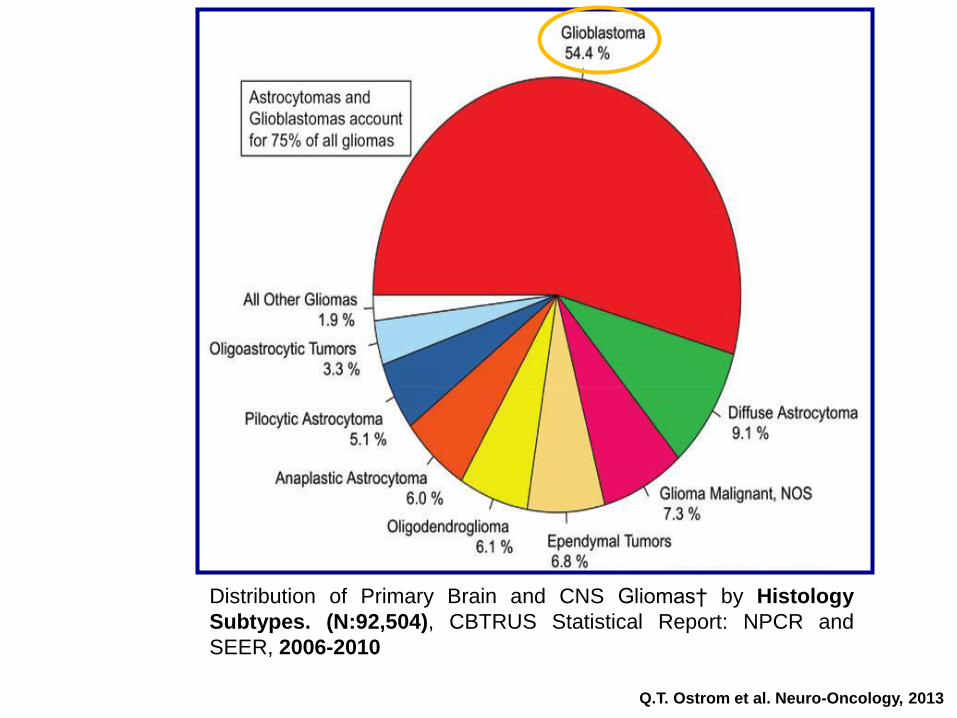
Q.T. Ostrom et al. Neuro-Oncology, 2013
Distribution of Primary Brain and CNS Gliomas† by Histology
Subtypes. (N:92,504), CBTRUS Statistical Report: NPCR and
SEER, 2006-2010
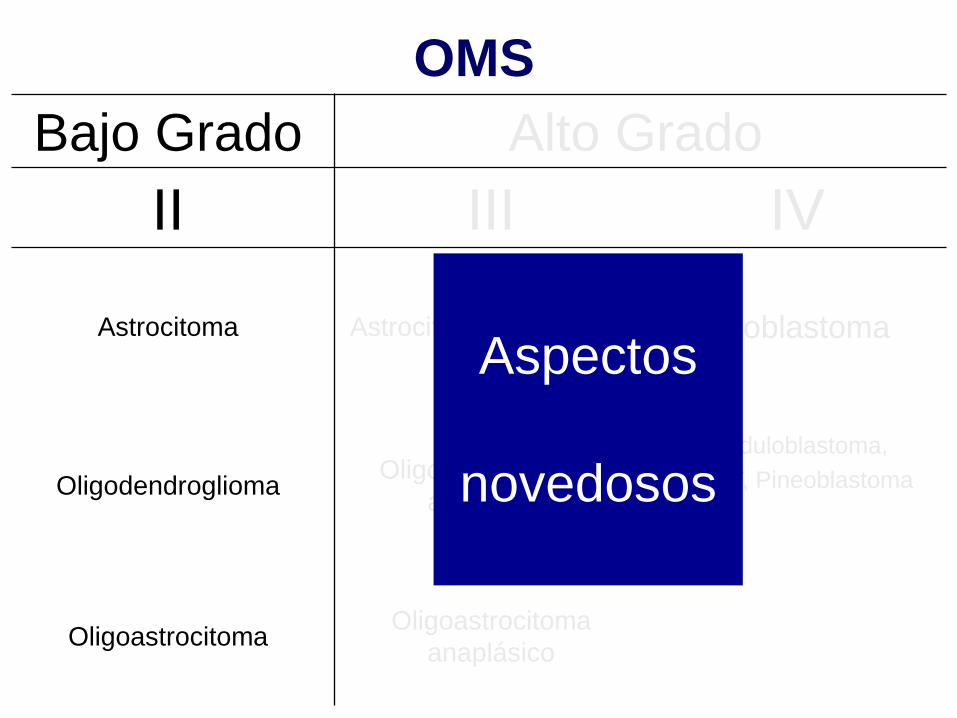
OMS
Bajo Grado Alto Grado
II III IV
Astrocitoma Astrocitoma anaplásico Glioblastoma
Oligodendroglioma Oligodendroglioma
anaplásico
Meduloblastoma,
PNET, Pineoblastoma
Oligoastrocitoma Oligoastrocitoma
anaplásico
Aspectos
novedosos

Conclusions
Grade 2 glioma with less than gross total
tumor resection or >40 years of age, PCV +
RT prolongs both OS and PFS compared
with RT alone.
A or A-dominant OA have worse outcomes,
as do males. IDH and 1p19q pending
J.C.Buckner et al. ASCO 2014; #2000, Shaw et al: J Clin Oncol. 2012
Subtotal resection, biopsy or >40 yrs
Grade II astrocytoma, oligo-
astrocytoma, or oligodendroglioma.
N:251 from 1998 to 2002
RT + PCV RT HR ; p
mOS (yrs) 13.3 7.8 0.59
p 0.03
mPFS (yrs): 10.4 4.0 0.50
p 0.002
5 yrs survival 73 62
10 yrs survival 64 41
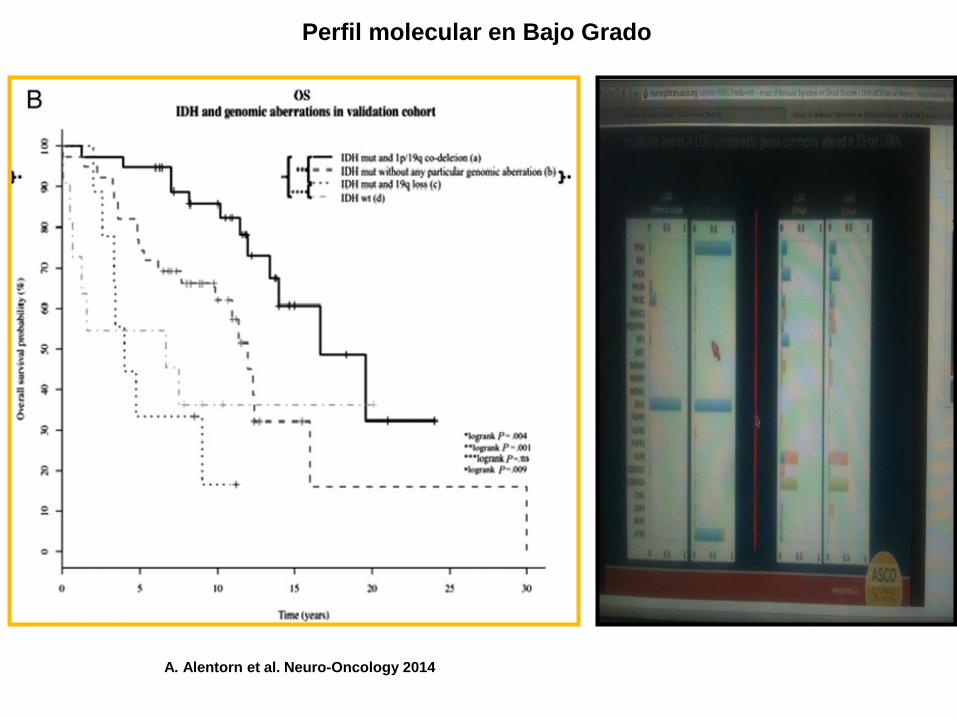
Perfil molecular en Bajo Grado
A. Alentorn et al. Neuro-Oncology 2014
OMS
Bajo Grado Alto Grado
II III IV
Astrocitoma Astrocitoma anaplásico Glioblastoma
Oligodendroglioma Oligodendroglioma
anaplásico
Meduloblastoma,
PNET, Pineoblastoma
Oligoastrocitoma Oligoastrocitoma
anaplásico
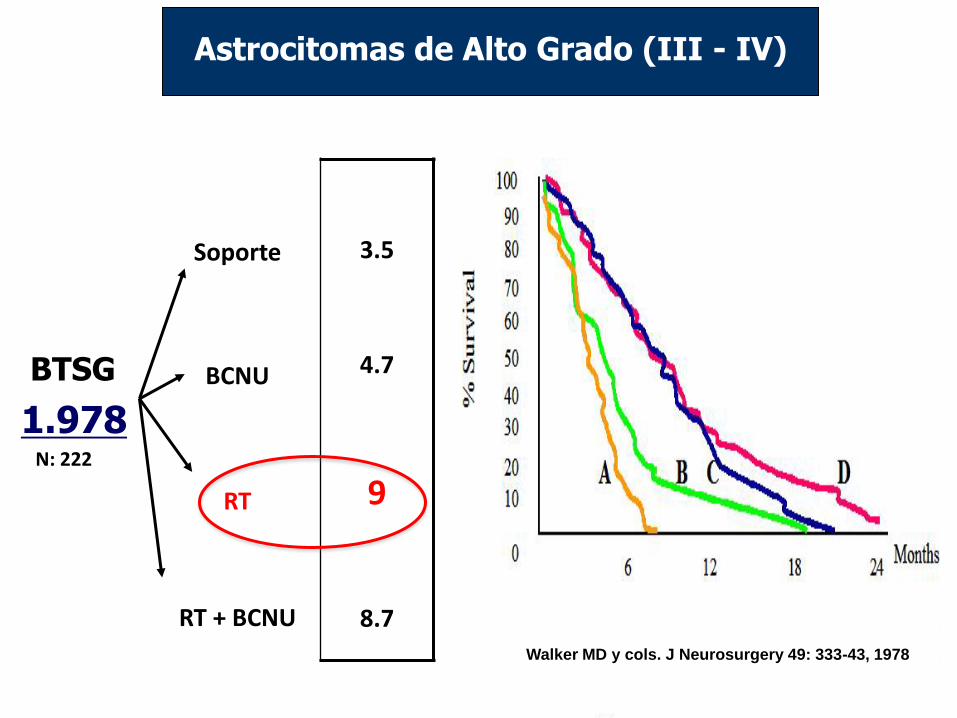
BTSG
1.978 N: 222
Soporte
BCNU
RT
RT + BCNU
3.5
4.7
9
8.7
Astrocitomas de Alto Grado (III - IV)
Mediana de Supervivencia (meses)
Walker MD y cols. J Neurosurgery 49: 333-43, 1978
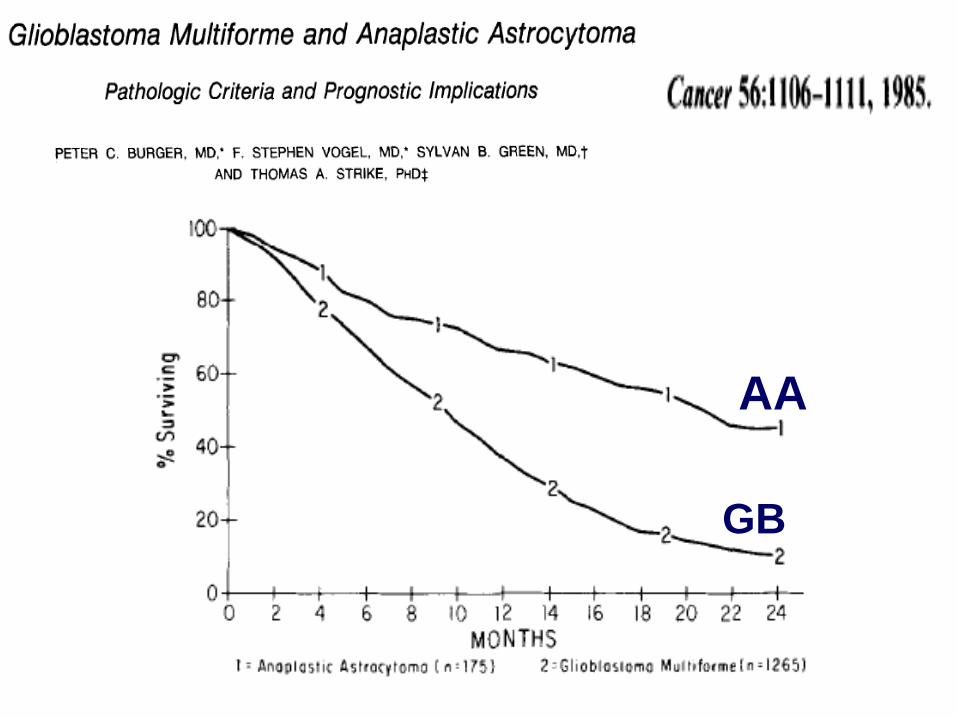
AA
GB
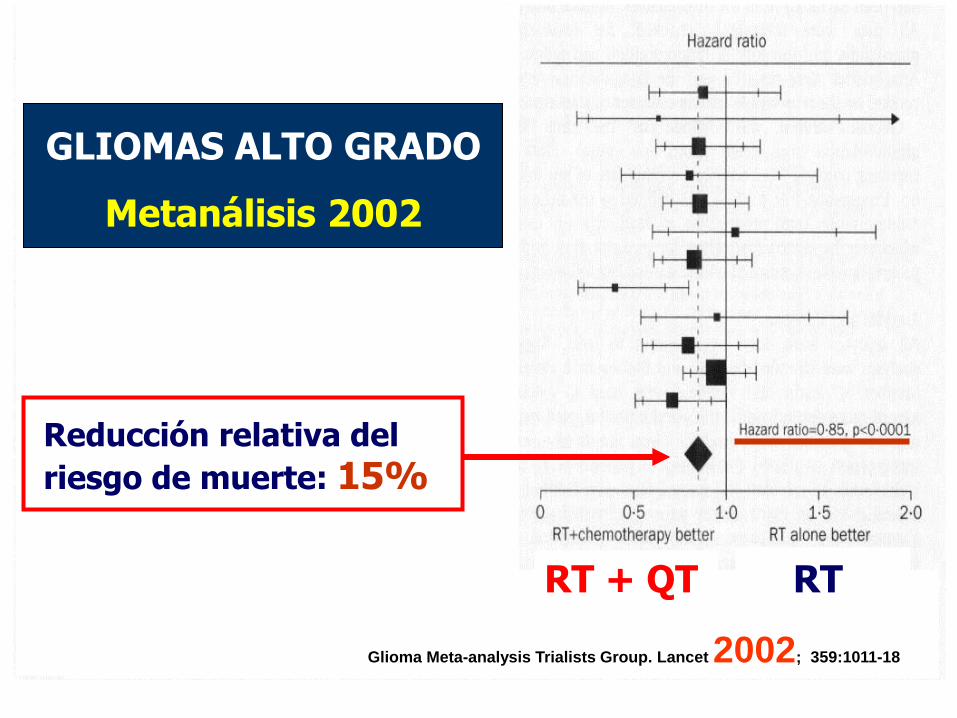
Reducción relativa del
riesgo de muerte: 15%
GLIOMAS ALTO GRADO
Metanálisis 2002
RT + QT RT
Glioma Meta-analysis Trialists Group. Lancet 2002; 359:1011-18
OMS
Bajo Grado Alto Grado
II III IV
Astrocitoma med SG: ≈ 5 año
Astrocitoma anaplásico Glioblastoma
Oligodendroglioma Oligodendroglioma
anaplásico
Meduloblastoma,
PNET, Pineoblastoma
Oligoastrocitoma Oligoastrocitoma
anaplásico
Aspectos
novedosos
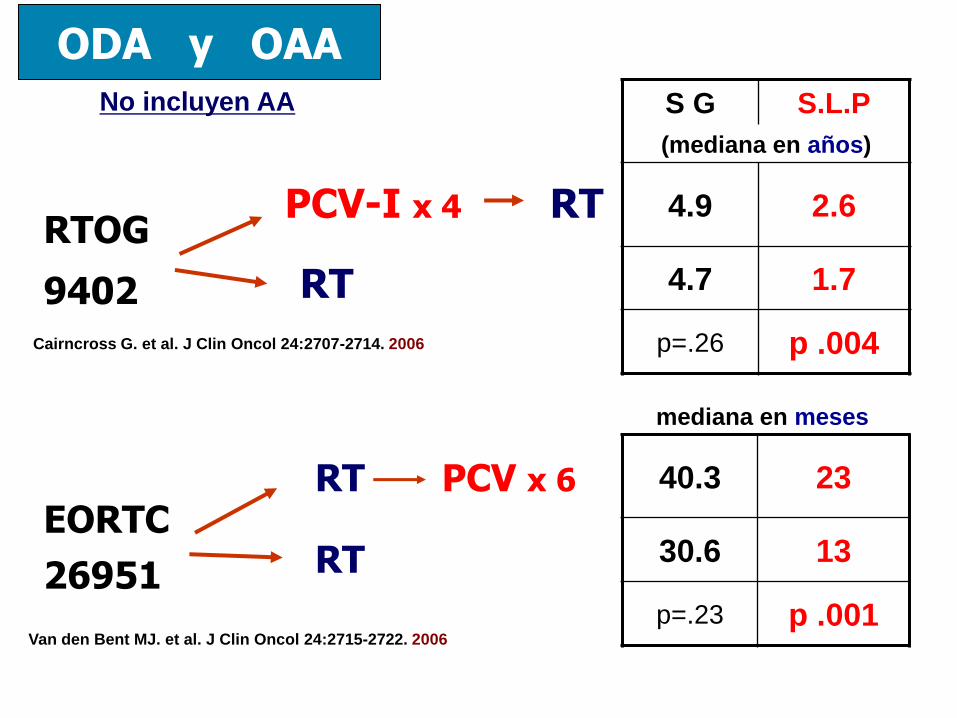
ODA y OAA
PCV-I x 4 RT
RT
RTOG
9402
RT PCV x 6
RT
S G S.L.P
(mediana en años)
4.9 2.6
4.7 1.7
p=.26 p .004
EORTC
26951
40.3 23
30.6 13
p=.23 p .001
mediana en meses
Van den Bent MJ. et al. J Clin Oncol 24:2715-2722. 2006
Cairncross G. et al. J Clin Oncol 24:2707-2714. 2006
No incluyen AA
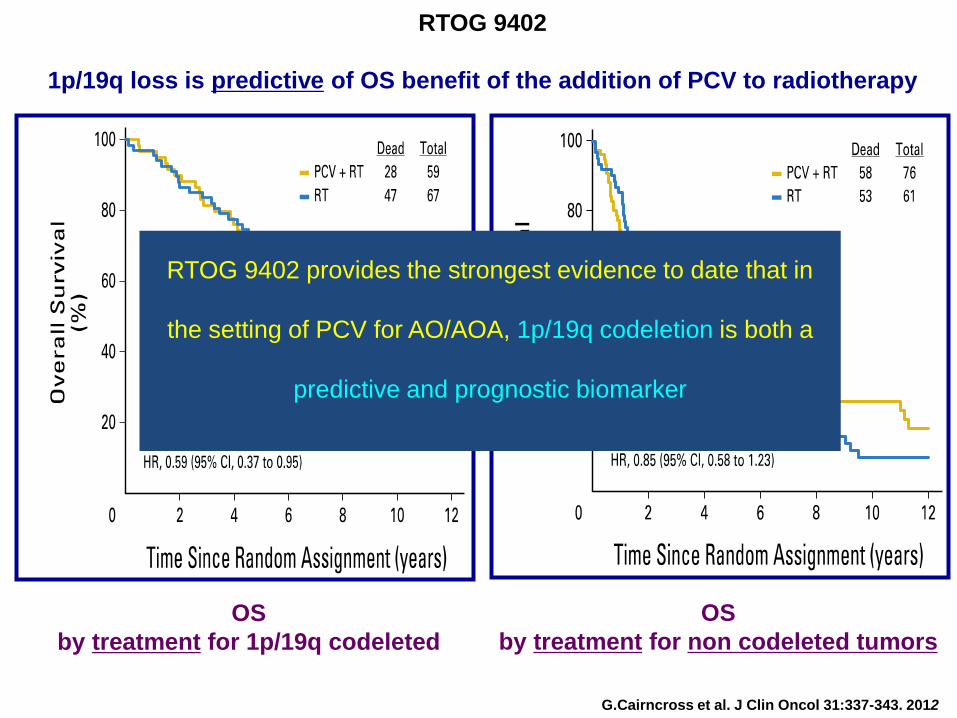
OS
by treatment for 1p/19q codeleted
G.Cairncross et al. J Clin Oncol 31:337-343. 2012
RTOG 9402
1p/19q loss is predictive of OS benefit of the addition of PCV to radiotherapy
OS
by treatment for non codeleted tumors
RTOG 9402 provides the strongest evidence to date that in
the setting of PCV for AO/AOA, 1p/19q codeletion is both a
predictive and prognostic biomarker
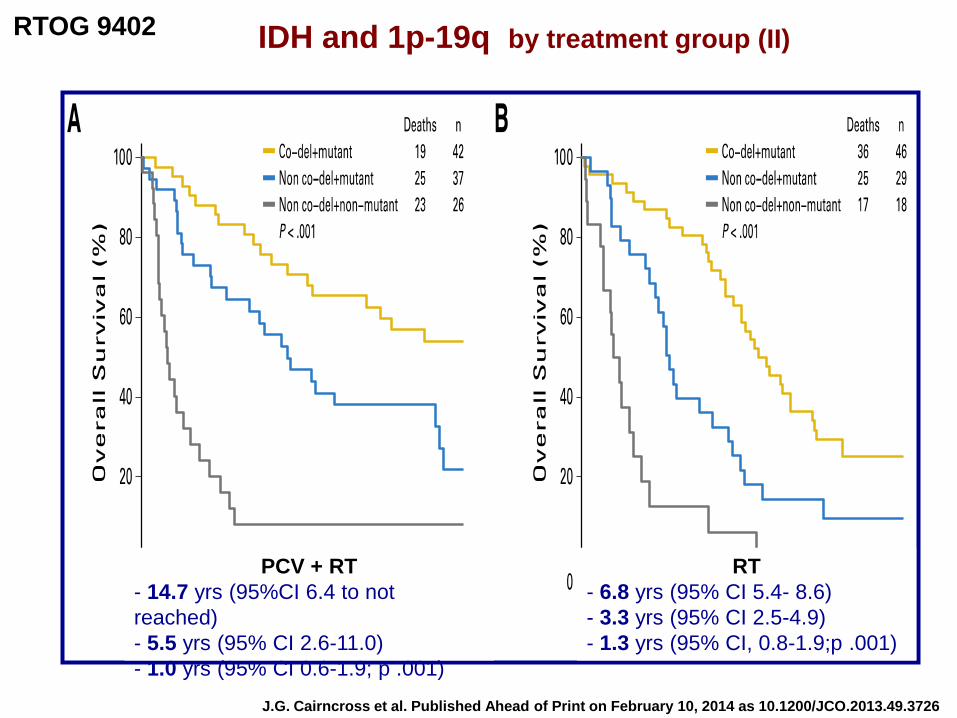
J.G. Cairncross et al. Published Ahead of Print on February 10, 2014 as 10.1200/JCO.2013.49.3726
PCV + RT
- 14.7 yrs (95%CI 6.4 to not
reached)
- 5.5 yrs (95% CI 2.6-11.0)
- 1.0 yrs (95% CI 0.6-1.9; p .001)
RT
- 6.8 yrs (95% CI 5.4- 8.6)
- 3.3 yrs (95% CI 2.5-4.9)
- 1.3 yrs (95% CI, 0.8-1.9;p .001)
RTOG 9402 IDH and 1p-19q by treatment group (II)
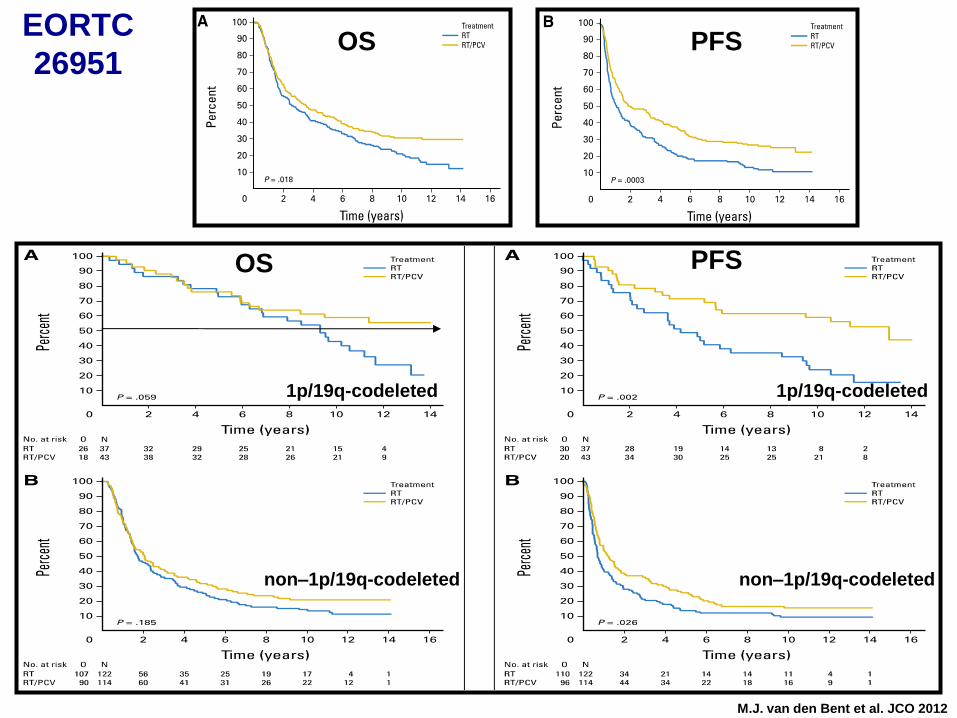
OS
M.J. van den Bent et al. JCO 2012
PFS
non–1p/19q-codeleted
1p/19q-codeleted
OS PFS
1p/19q-codeleted
non–1p/19q-codeleted
EORTC
26951
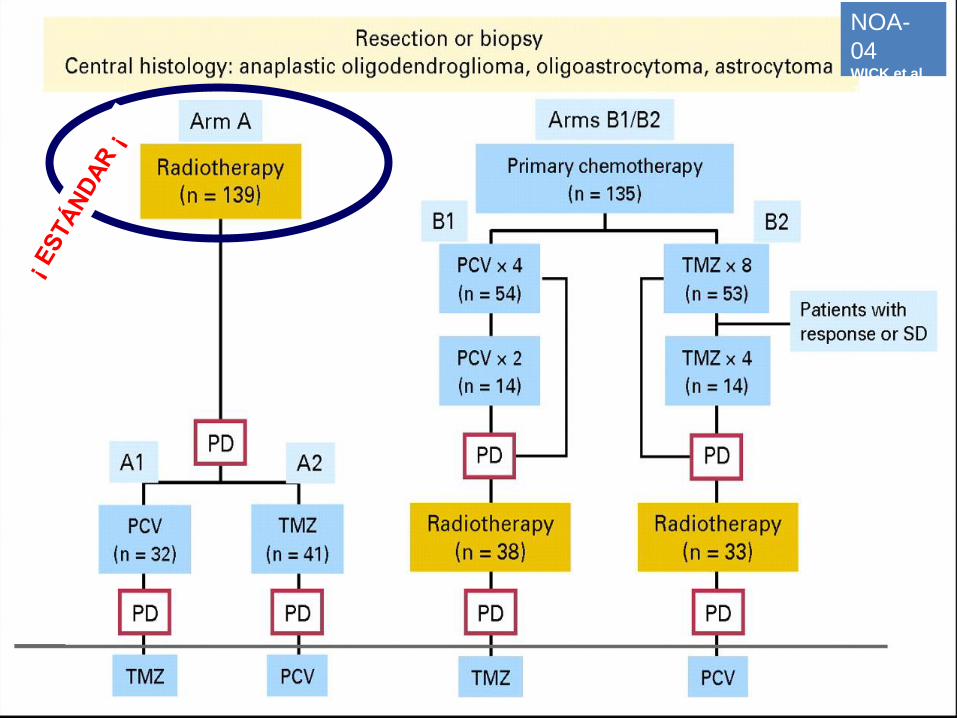
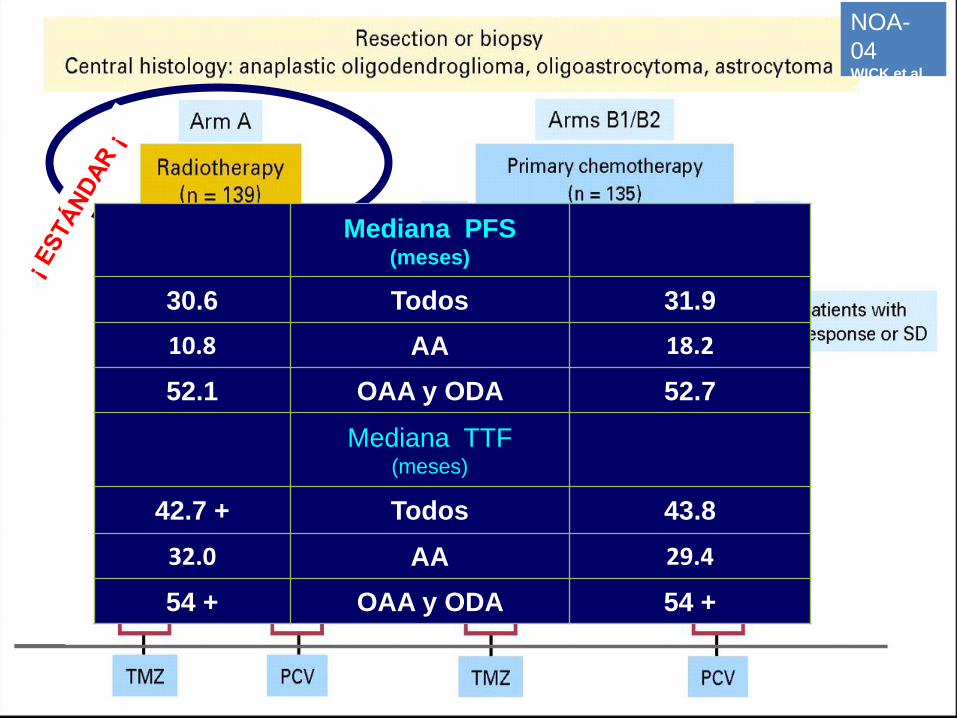
NOA-
04 WICK et al.
JCO 2009
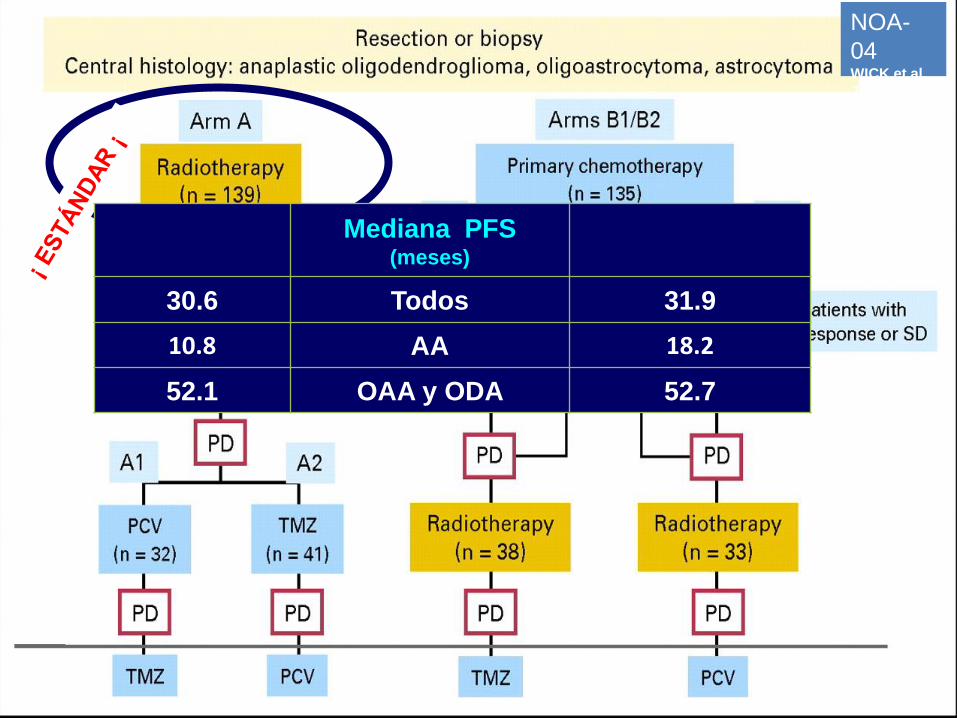
Mediana PFS (meses)
30.6 Todos 31.9
10.8 AA 18.2
52.1 OAA y ODA 52.7
NOA-
04 WICK et al.
JCO 2009
Mediana PFS (meses)
30.6 Todos 31.9
10.8 AA 18.2
52.1 OAA y ODA 52.7
Mediana TTF (meses)
42.7 + Todos 43.8
32.0 AA 29.4
54 + OAA y ODA 54 +
NOA-
04 WICK et al.
JCO 2009
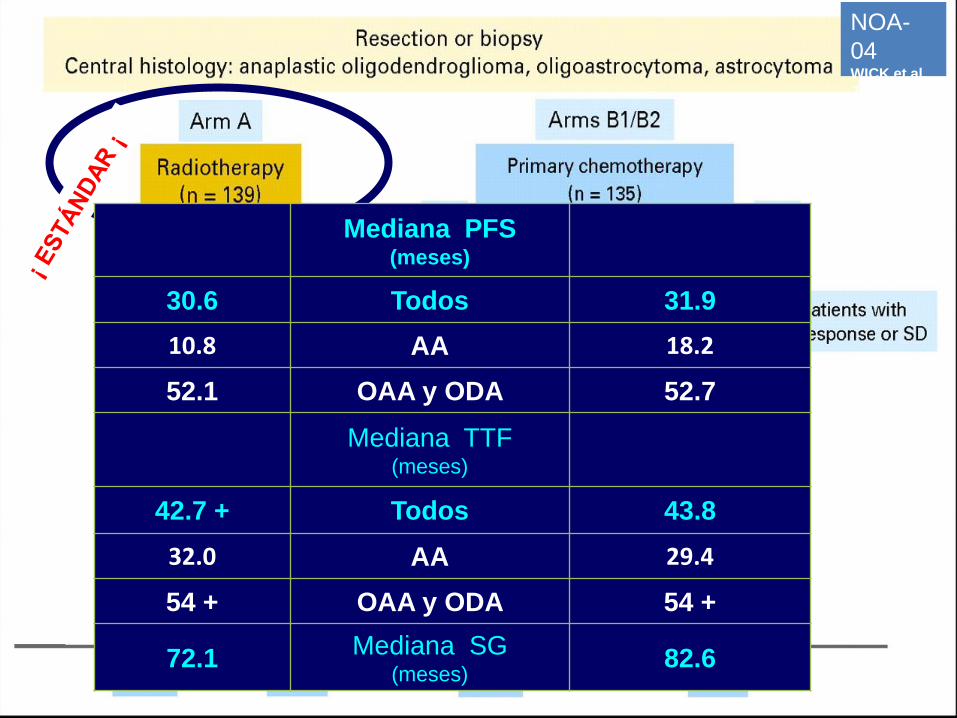
Mediana PFS (meses)
30.6 Todos 31.9
10.8 AA 18.2
52.1 OAA y ODA 52.7
Mediana TTF (meses)
42.7 + Todos 43.8
32.0 AA 29.4
54 + OAA y ODA 54 +
72.1 Mediana SG
(meses) 82.6
NOA-
04 WICK et al.
JCO 2009
ASTROCITOMAS ANAPLÁSICOS
IDH / MGMT ?
RT o TMZ o PCV (… pero no Stupp ????)
La “mejor” evidencia
(NOA 04)
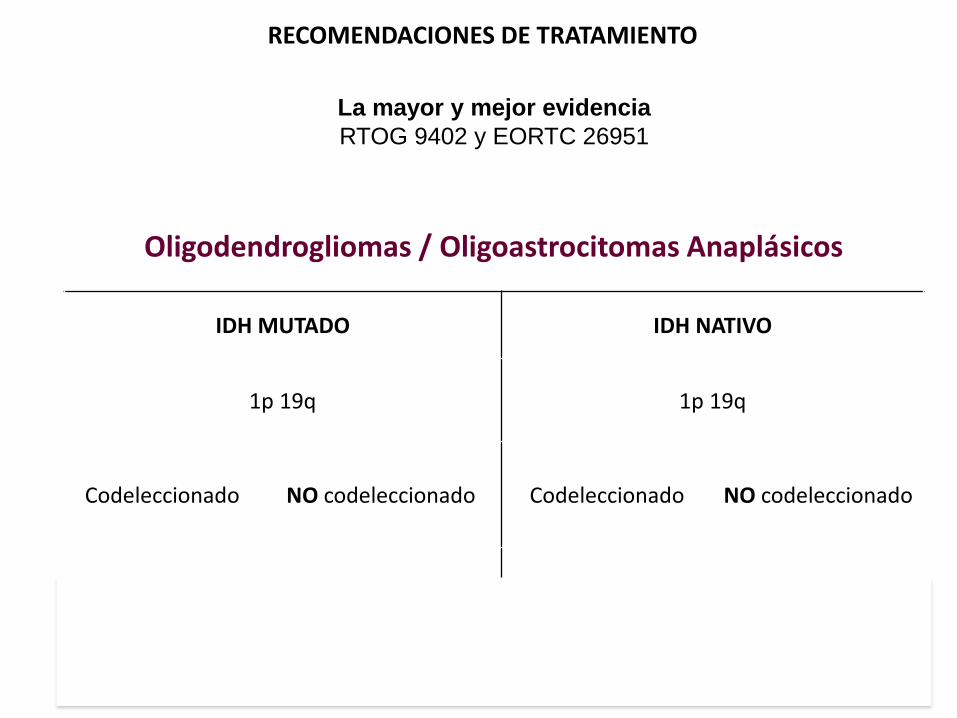
RECOMENDACIONES DE TRATAMIENTO
Oligodendrogliomas / Oligoastrocitomas Anaplásicos
IDH MUTADO IDH NATIVO
1p 19q 1p 19q
Codeleccionado NO codeleccionado Codeleccionado NO codeleccionado
PCV + RT PCV+RT ?
MGMT ? RT
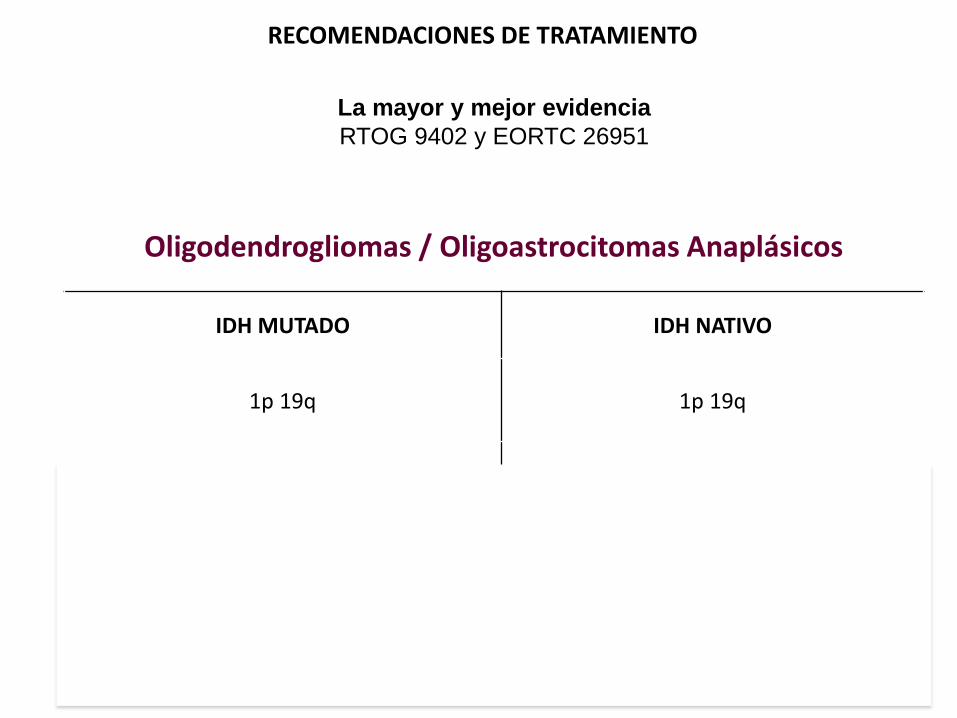
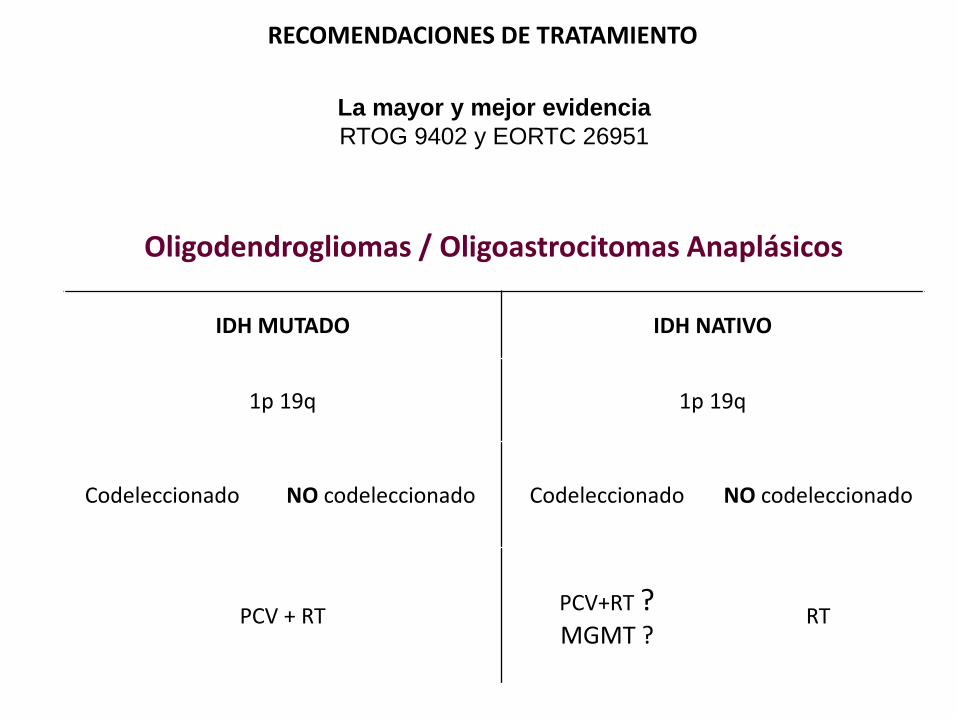
RECOMENDACIONES DE TRATAMIENTO
La mayor y mejor evidencia
RTOG 9402 y EORTC 26951
Oligodendrogliomas / Oligoastrocitomas Anaplásicos
IDH MUTADO IDH NATIVO
1p 19q 1p 19q
Codeleccionado NO codeleccionado Codeleccionado NO codeleccionado
PCV + RT PCV+RT ?
MGMT ? RT
RECOMENDACIONES DE TRATAMIENTO
La mayor y mejor evidencia
RTOG 9402 y EORTC 26951
Oligodendrogliomas / Oligoastrocitomas Anaplásicos
IDH MUTADO IDH NATIVO
1p 19q 1p 19q
Codeleccionado NO codeleccionado Codeleccionado NO codeleccionado
PCV + RT PCV+RT ? MGMT ?
RT
RECOMENDACIONES DE TRATAMIENTO
La mayor y mejor evidencia
RTOG 9402 y EORTC 26951
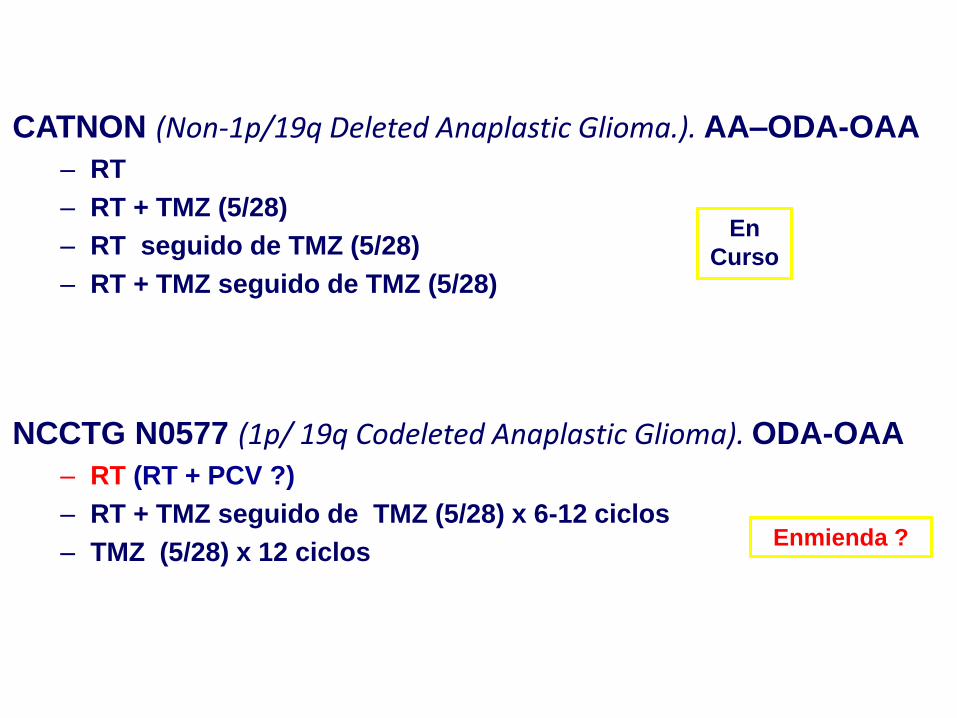
Estudios pendientes
CATNON (Non-1p/19q Deleted Anaplastic Glioma.). AA–ODA-OAA
– RT
– RT + TMZ (5/28)
– RT seguido de TMZ (5/28)
– RT + TMZ seguido de TMZ (5/28)
NCCTG N0577 (1p/ 19q Codeleted Anaplastic Glioma). ODA-OAA
– RT (RT + PCV ?)
– RT + TMZ seguido de TMZ (5/28) x 6-12 ciclos
– TMZ (5/28) x 12 ciclos Enmienda ?
En
Curso
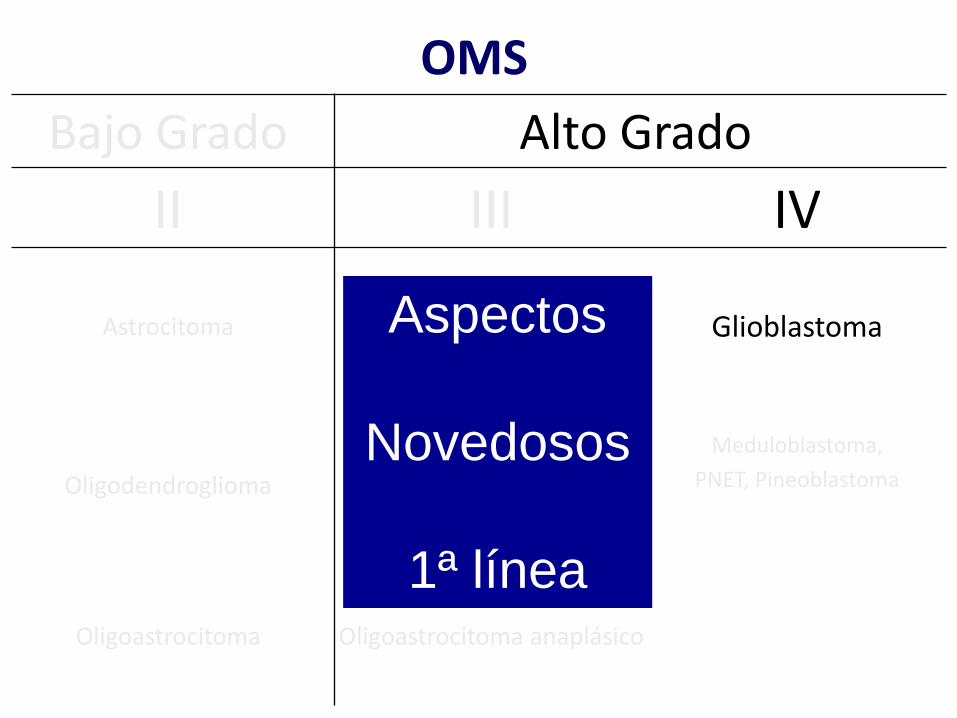
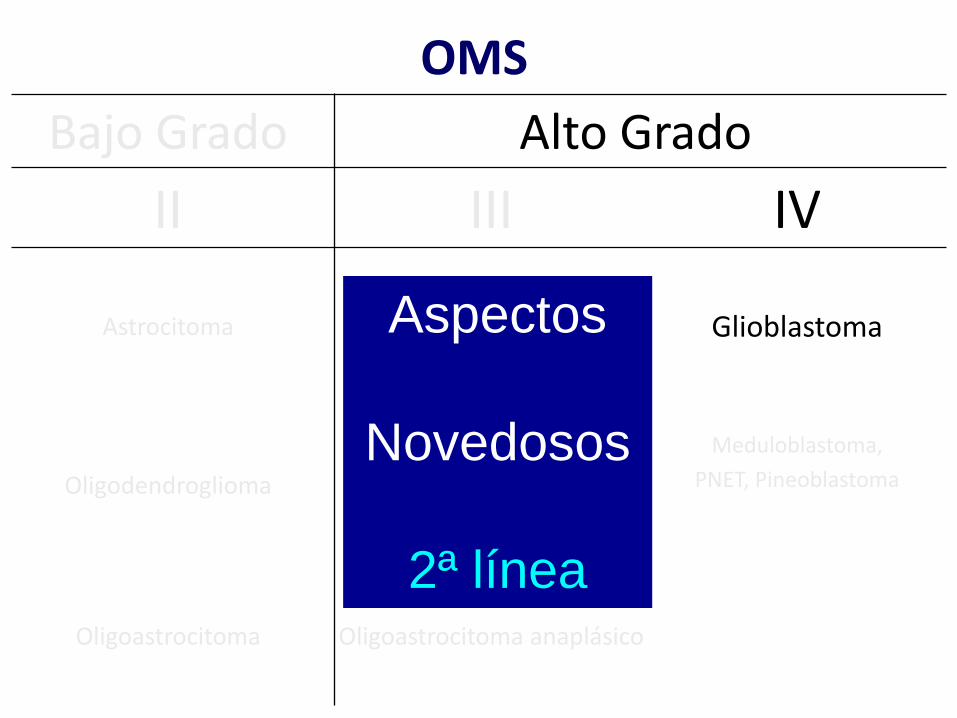
OMS
Bajo Grado Alto Grado
II III IV
Astrocitoma Astrocitoma anaplásico
med SG: ≈ 2-3 años Glioblastoma
Oligodendroglioma Oligodendroglioma
anaplásico
Meduloblastoma,
PNET, Pineoblastoma
Oligoastrocitoma Oligoastrocitoma anaplásico
Aspectos
Novedosos
1ª línea
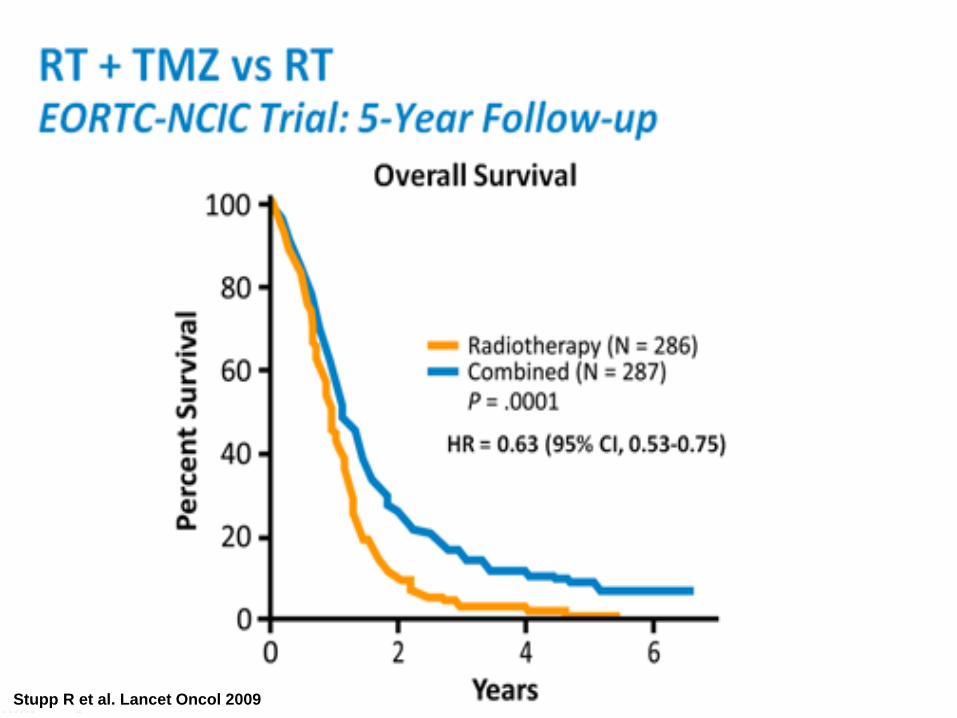
Stupp R et al. Lancet Oncol 2009
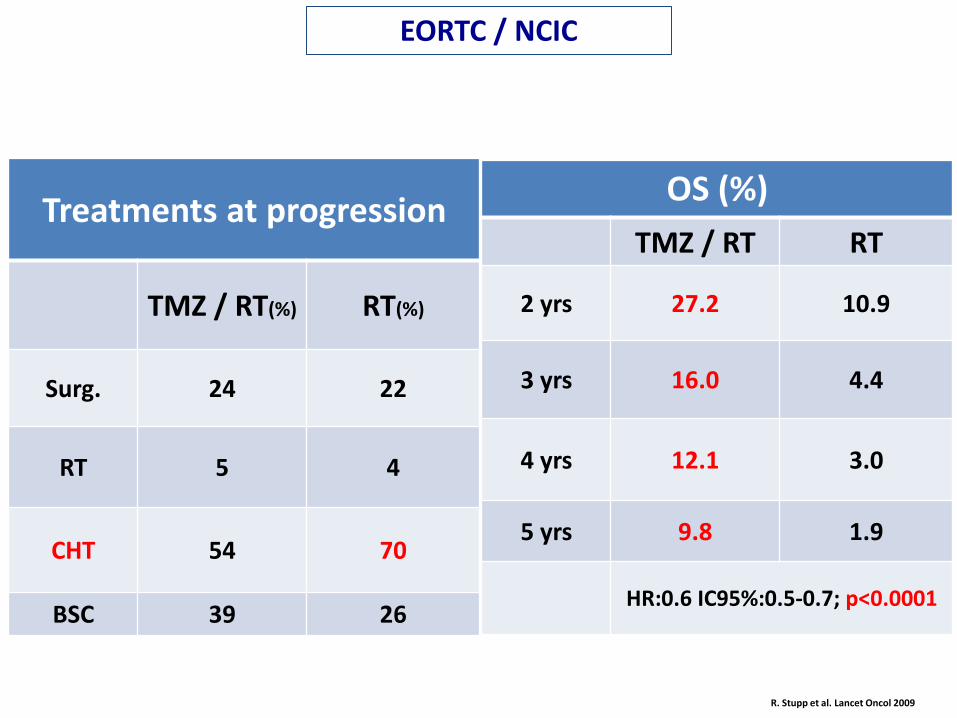
R. Stupp et al. Lancet Oncol 2009
EORTC / NCIC
OS (%)
TMZ / RT RT
2 yrs 27.2 10.9
3 yrs 16.0 4.4
4 yrs 12.1 3.0
5 yrs 9.8 1.9
HR:0.6 IC95%:0.5-0.7; p<0.0001
Treatments at progression
TMZ / RT(%) RT(%)
Surg. 24 22
RT 5 4
CHT 54 70
BSC 39 26
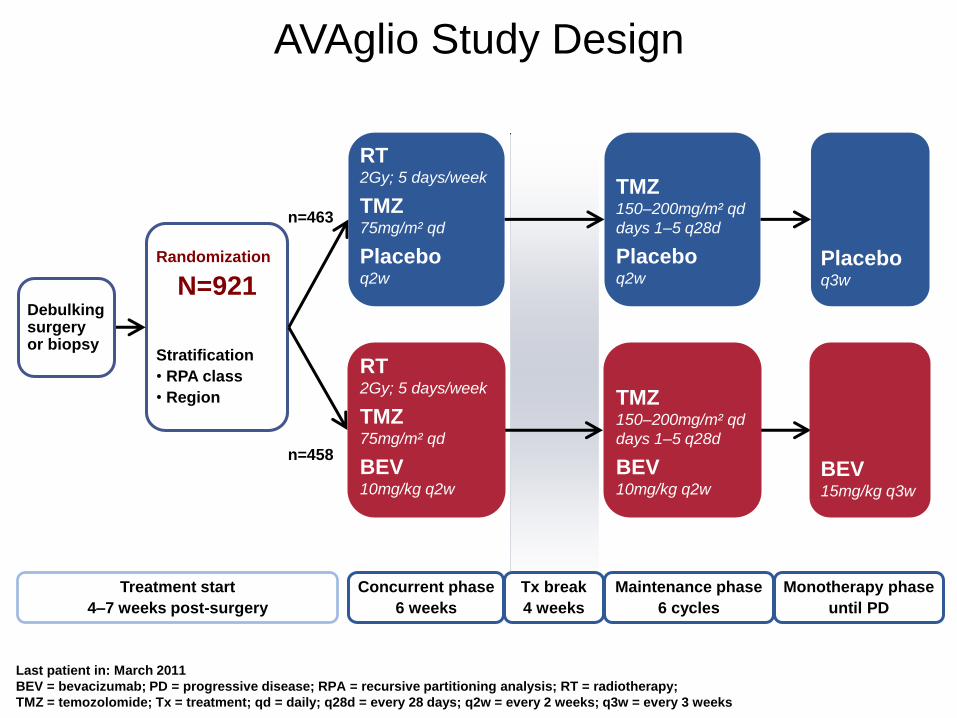
AVAglio Study Design
n=463
n=458
Randomization
N=921
Stratification
• RPA class
• Region
Last patient in: March 2011
BEV = bevacizumab; PD = progressive disease; RPA = recursive partitioning analysis; RT = radiotherapy;
TMZ = temozolomide; Tx = treatment; qd = daily; q28d = every 28 days; q2w = every 2 weeks; q3w = every 3 weeks
Treatment start
4–7 weeks post-surgery
RT 2Gy; 5 days/week
TMZ 75mg/m² qd
Placebo q2w
TMZ 150–200mg/m² qd
days 1–5 q28d
Placebo q2w
RT 2Gy; 5 days/week
TMZ 75mg/m² qd
BEV
10mg/kg q2w
TMZ 150–200mg/m² qd
days 1–5 q28d
BEV
10mg/kg q2w BEV 15mg/kg q3w
Placebo q3w
Debulking surgery or biopsy
Concurrent phase
6 weeks
Tx break
4 weeks
Maintenance phase
6 cycles
Monotherapy phase
until PD
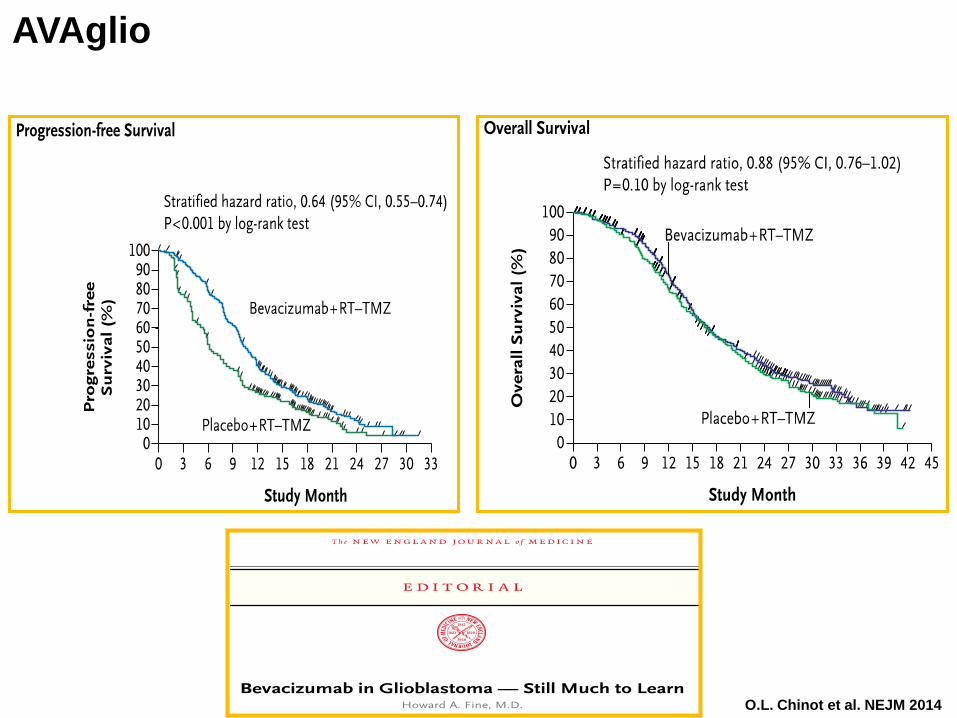
O.L. Chinot et al. NEJM 2014
AVAglio
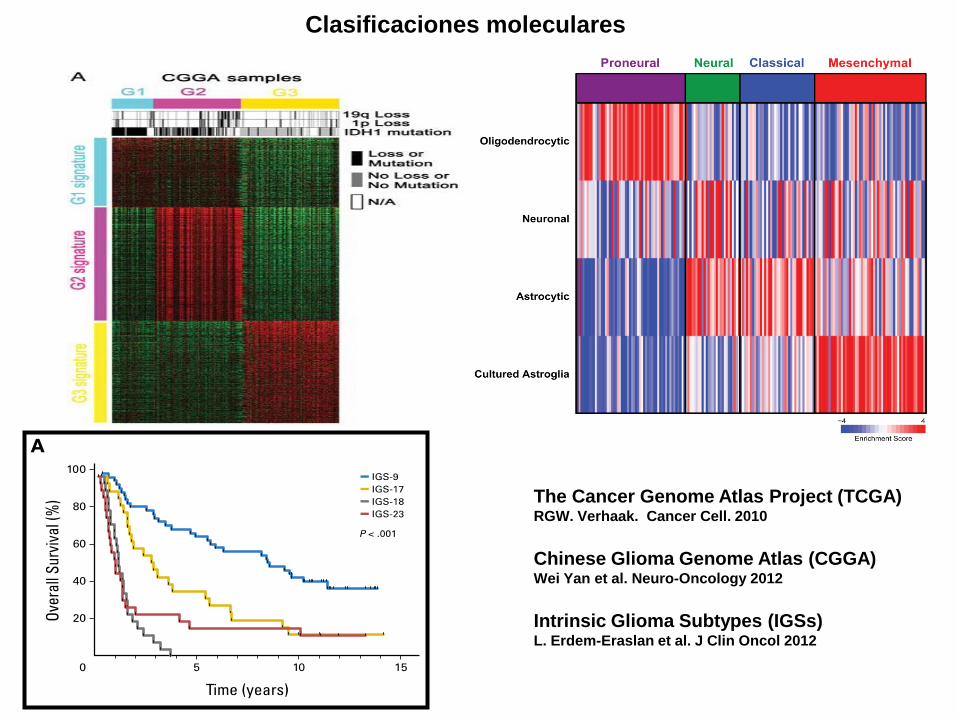
Clasificaciones moleculares
The Cancer Genome Atlas Project (TCGA) RGW. Verhaak. Cancer Cell. 2010
Chinese Glioma Genome Atlas (CGGA) Wei Yan et al. Neuro-Oncology 2012
Intrinsic Glioma Subtypes (IGSs) L. Erdem-Eraslan et al. J Clin Oncol 2012
Figure 4.
Single sample GSEA scores of GBM subtypes show a relation to specific cell types. Gene
expression signatures of oligodendrocytes, astrocytes, neurons and cultured astroglial cells
were generated from murine brain cell types (Cahoy et al., 2008). Single sample GSEA was
used to project the four gene sets on samples on the Proneural, Classical, Neural and
Mesenchymal subtypes. A positive enrichment score indicates a positive correlation between
genes in the gene set and the tumor sample expression profile; a negative enrichment score
indicates the reverse. Also see FigureS6.
Verhaak et al. Page 19
Cancer Cell . Author manuscript; available in PMC 2011 January 19.
NIH
-PA
Au
tho
r Ma
nu
scrip
tN
IH-P
A A
uth
or M
anu
scrip
tN
IH-P
A A
uth
or M
anu
scrip
t
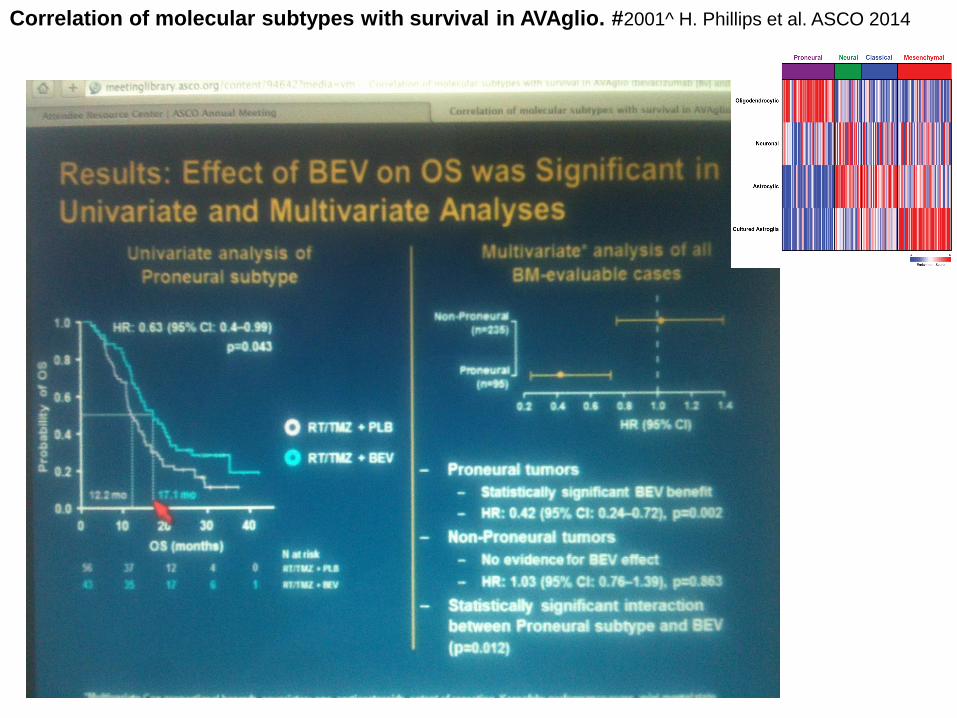
Correlation of molecular subtypes with survival in AVAglio. #2001^ H. Phillips et al. ASCO 2014
Figure 4.
Single sample GSEA scores of GBM subtypes show a relation to specific cell types. Gene
expression signatures of oligodendrocytes, astrocytes, neurons and cultured astroglial cells
were generated from murine brain cell types (Cahoy et al., 2008). Single sample GSEA was
used to project the four gene sets on samples on the Proneural, Classical, Neural and
Mesenchymal subtypes. A positive enrichment score indicates a positive correlation between
genes in the gene set and the tumor sample expression profile; a negative enrichment score
indicates the reverse. Also see FigureS6.
Verhaak et al. Page 19
Cancer Cell . Author manuscript; available in PMC 2011 January 19.
NIH
-PA
Au
tho
r Manu
scrip
tN
IH-P
A A
uth
or M
anu
scrip
tN
IH-P
A A
uth
or M
anu
scrip
t
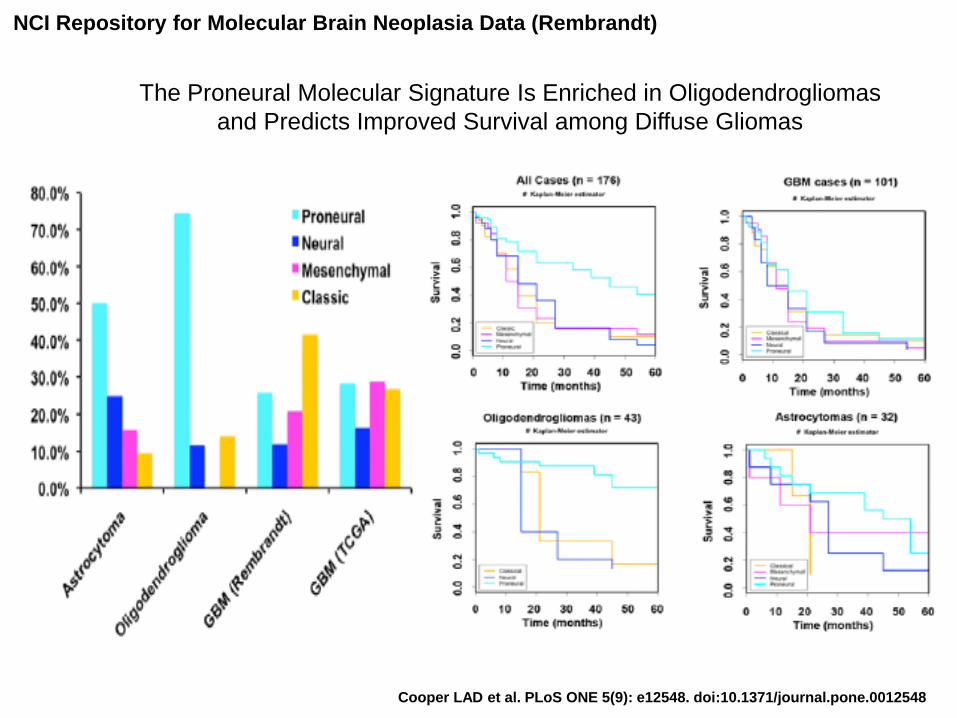
Cooper LAD et al. PLoS ONE 5(9): e12548. doi:10.1371/journal.pone.0012548
The Proneural Molecular Signature Is Enriched in Oligodendrogliomas
and Predicts Improved Survival among Diffuse Gliomas
NCI Repository for Molecular Brain Neoplasia Data (Rembrandt)
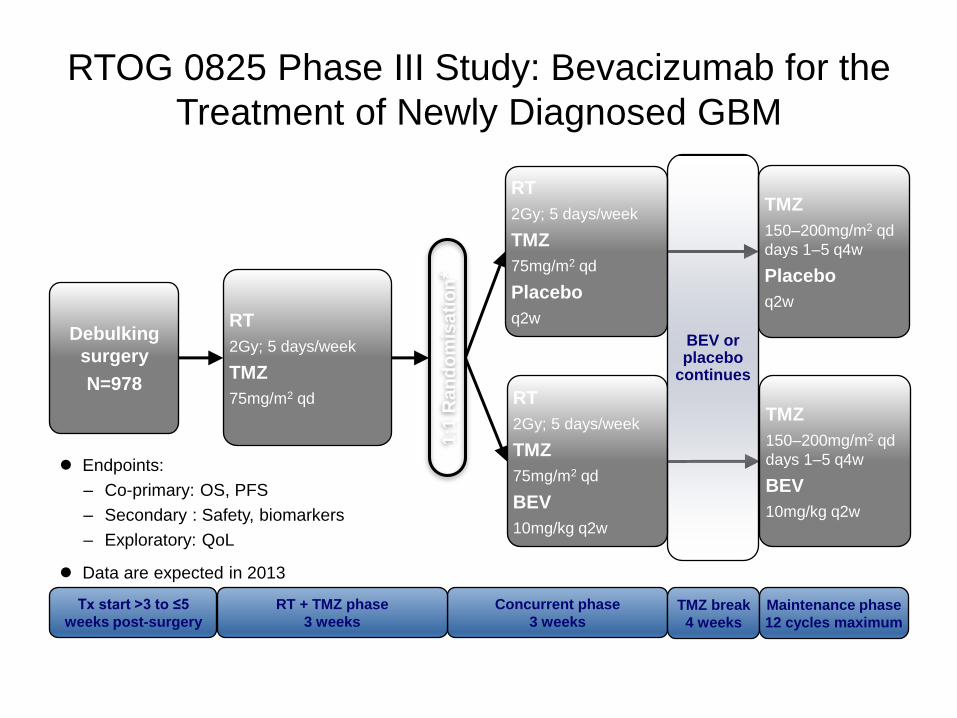
RTOG 0825 Phase III Study: Bevacizumab for the
Treatment of Newly Diagnosed GBM
Endpoints:
– Co-primary: OS, PFS
– Secondary : Safety, biomarkers
– Exploratory: QoL
Data are expected in 2013
Cycle = 28 days. *≤10 days after start of RT; Stratification by MGMT methylation status and molecular profile BEV = bevacizumab; GBM = glioblastoma; MGMT = O6-methylguanine-DNA methyltransferase; OS = overall survival; PFS = progression-
free survival; q2w = every 2 weeks; q4w = every 4 weeks; qd = daily; QoL = quality of life; RT = radiotherapy, TMZ = temozolomide NCT00884741
Debulking
surgery
N=978
RT
2Gy; 5 days/week
TMZ
75mg/m2 qd
1:1
Ra
nd
om
isa
tio
n*
RT
2Gy; 5 days/week
TMZ
75mg/m2 qd
Placebo
q2w
TMZ
150–200mg/m2 qd
days 1–5 q4w
Placebo
q2w
RT
2Gy; 5 days/week
TMZ
75mg/m2 qd
BEV
10mg/kg q2w
TMZ
150–200mg/m2 qd
days 1–5 q4w
BEV
10mg/kg q2w
Tx start >3 to ≤5
weeks post-surgery
Concurrent phase
3 weeks TMZ break
4 weeks
Maintenance phase
12 cycles maximum
RT + TMZ phase
3 weeks
BEV or placebo
continues
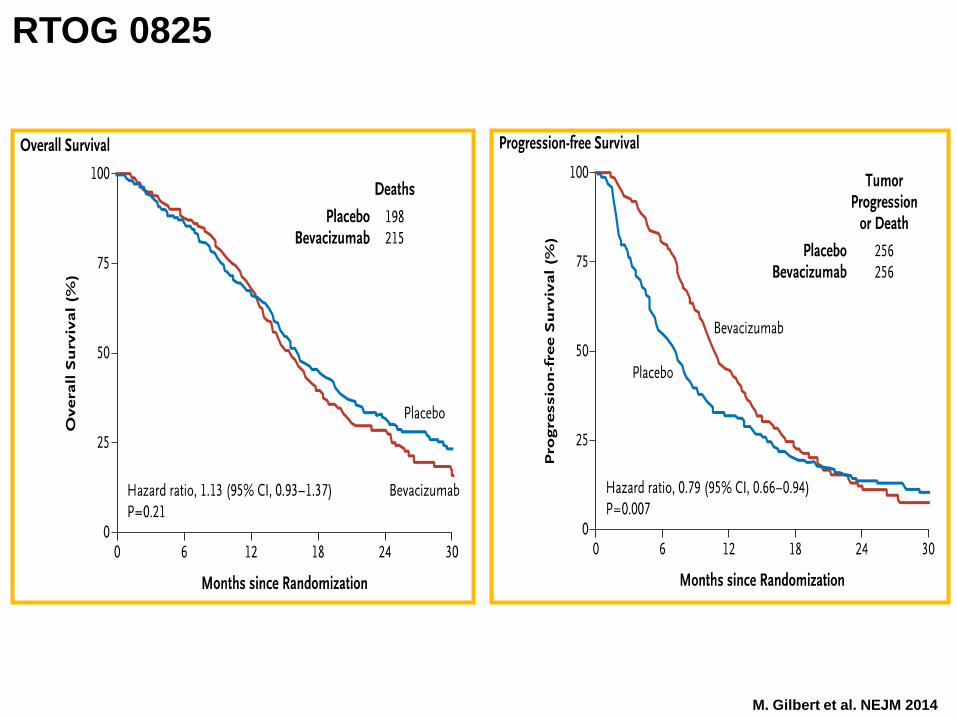
M. Gilbert et al. NEJM 2014
RTOG 0825
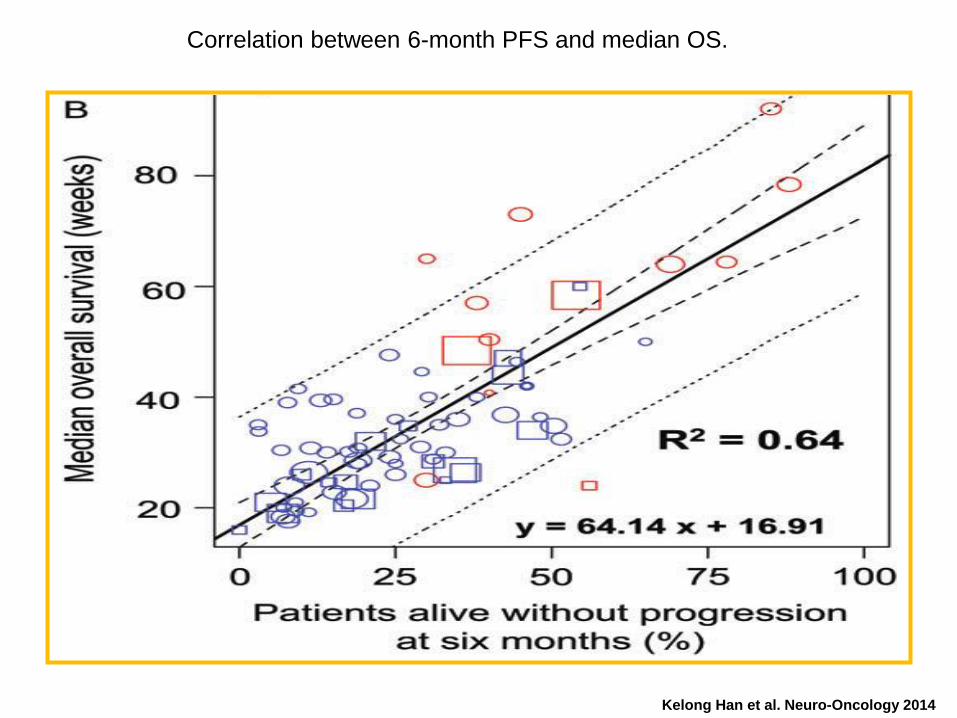
Correlation between 6-month PFS and median OS.
Kelong Han et al. Neuro-Oncology 2014
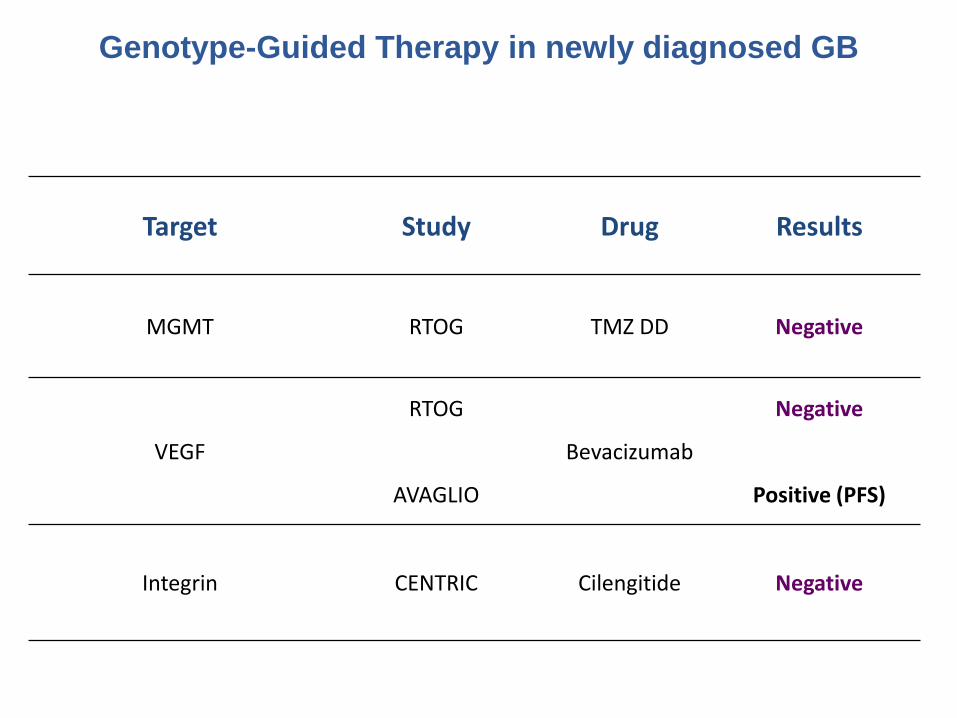
Target Study Drug Results
MGMT RTOG TMZ DD Negative
VEGF
RTOG
AVAGLIO
Bevacizumab
Negative
Positive (PFS)
Integrin CENTRIC Cilengitide Negative
Genotype-Guided Therapy in newly diagnosed GB
OMS
Bajo Grado Alto Grado
II III IV
Astrocitoma Astrocitoma anaplásico
med SG: ≈ 2-3 años Glioblastoma
Oligodendroglioma Oligodendroglioma
anaplásico
Meduloblastoma,
PNET, Pineoblastoma
Oligoastrocitoma Oligoastrocitoma anaplásico
Aspectos
Novedosos
2ª línea
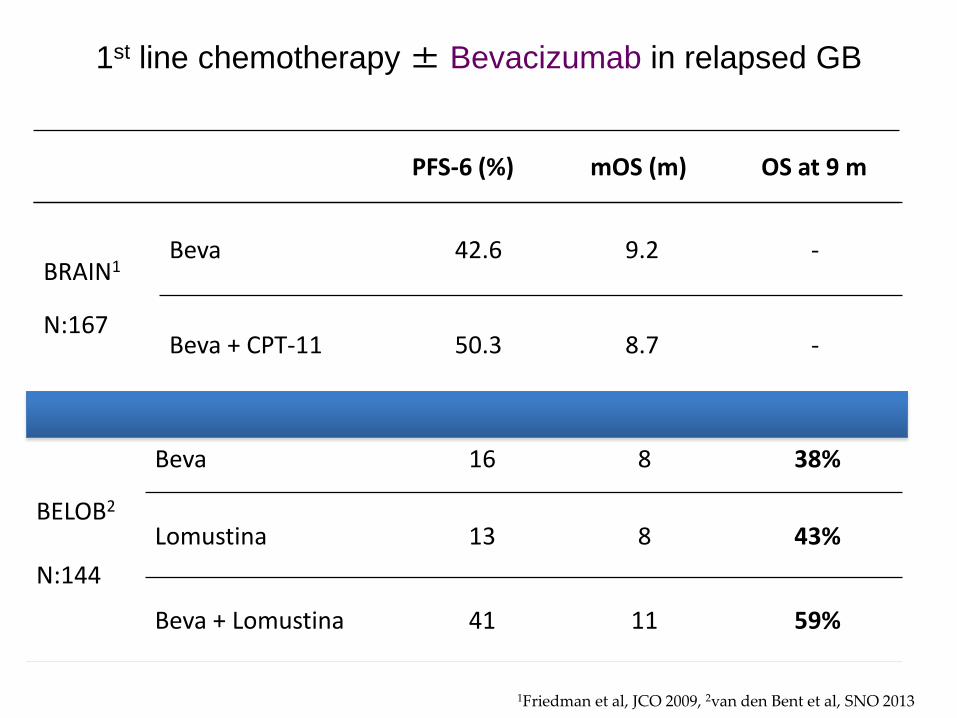
PFS-6 (%) mOS (m) OS at 9 m
1Friedman et al, JCO 2009, 2van den Bent et al, SNO 2013
BRAIN1
N:167
Beva 42.6 9.2 -
Beva + CPT-11 50.3 8.7 -
1st line chemotherapy ± Bevacizumab in relapsed GB
BELOB2
N:144
Beva 16 8 38%
Lomustina 13 8 43%
Beva + Lomustina 41 11 59%
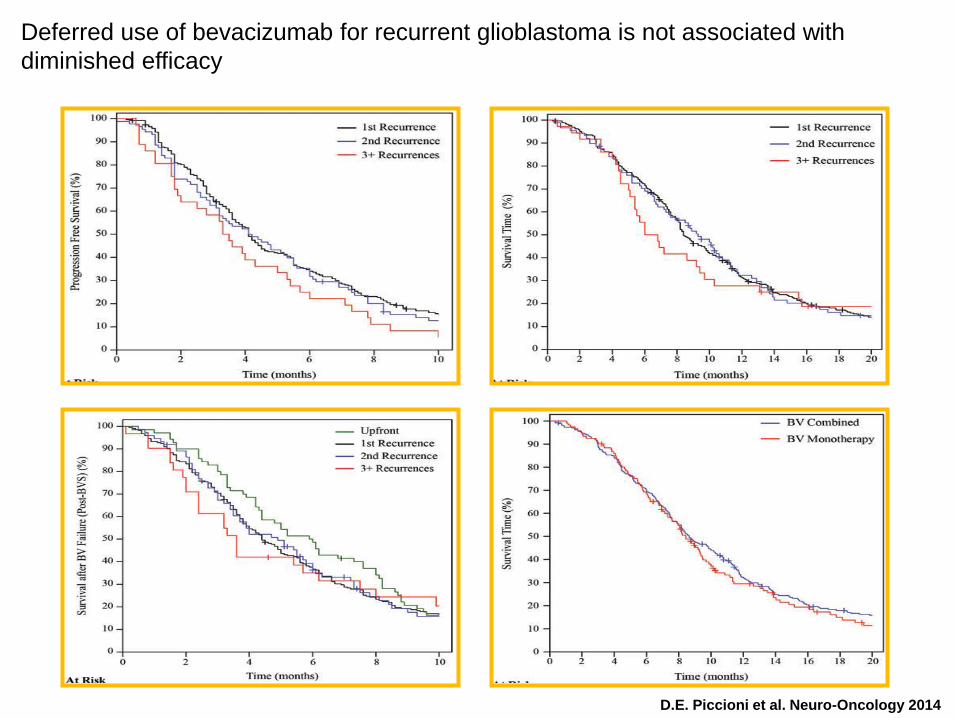
Deferred use of bevacizumab for recurrent glioblastoma is not associated with
diminished efficacy
D.E. Piccioni et al. Neuro-Oncology 2014
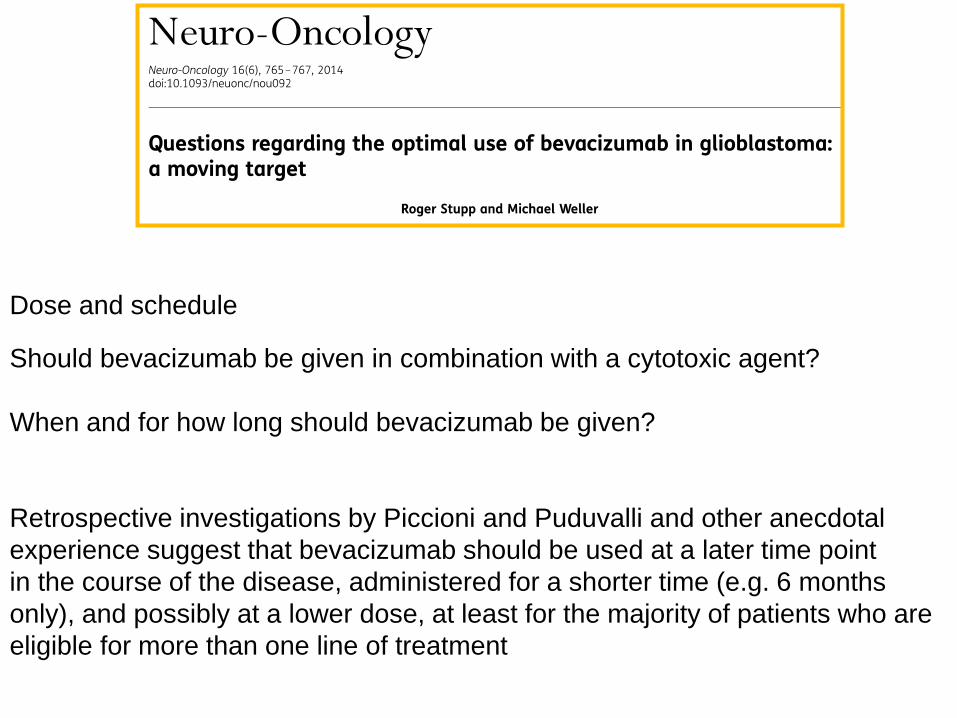
Dose and schedule
Should bevacizumab be given in combination with a cytotoxic agent?
When and for how long should bevacizumab be given?
Retrospective investigations by Piccioni and Puduvalli and other anecdotal
experience suggest that bevacizumab should be used at a later time point
in the course of the disease, administered for a shorter time (e.g. 6 months
only), and possibly at a lower dose, at least for the majority of patients who are
eligible for more than one line of treatment
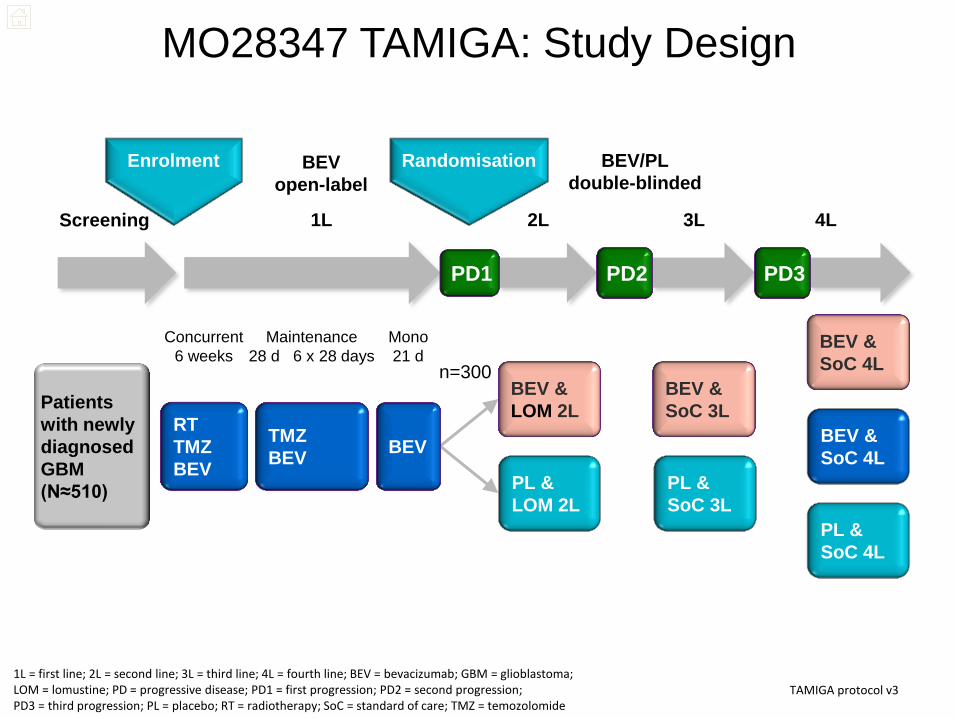
MO28347 TAMIGA: Study Design
TAMIGA protocol v3 1L = first line; 2L = second line; 3L = third line; 4L = fourth line; BEV = bevacizumab; GBM = glioblastoma; LOM = lomustine; PD = progressive disease; PD1 = first progression; PD2 = second progression; PD3 = third progression; PL = placebo; RT = radiotherapy; SoC = standard of care; TMZ = temozolomide
Patients
with newly
diagnosed
GBM
(N≈510)
TMZ
BEV
RT
TMZ
BEV
Screening 1L 2L 3L
Randomisation
Concurrent
6 weeks
4L
BEV &
SoC 4L
BEV &
SoC 4L
n=300
PD1 PD3 PD2
PL &
SoC 4L
BEV
open-label
BEV/PL
double-blinded
Maintenance
28 d 6 x 28 days
Mono
21 d
Enrolment
BEV
BEV &
LOM 2L
PL &
LOM 2L
BEV &
SoC 3L
PL &
SoC 3L
Quimioterapia “adyuvante” establecida en Gliomas
- Bajo grado: PCV
- Alto grado:
- Anaplásicos: PCV / TMZ
- Glioblastoma: TMZ / RT
Caracterización molecular pronóstica / predictiva:
IDH - 1p19q - MGMT
Tumores SNC: aspectos novedosos

MUCHAS GRACIAS A TOD@S