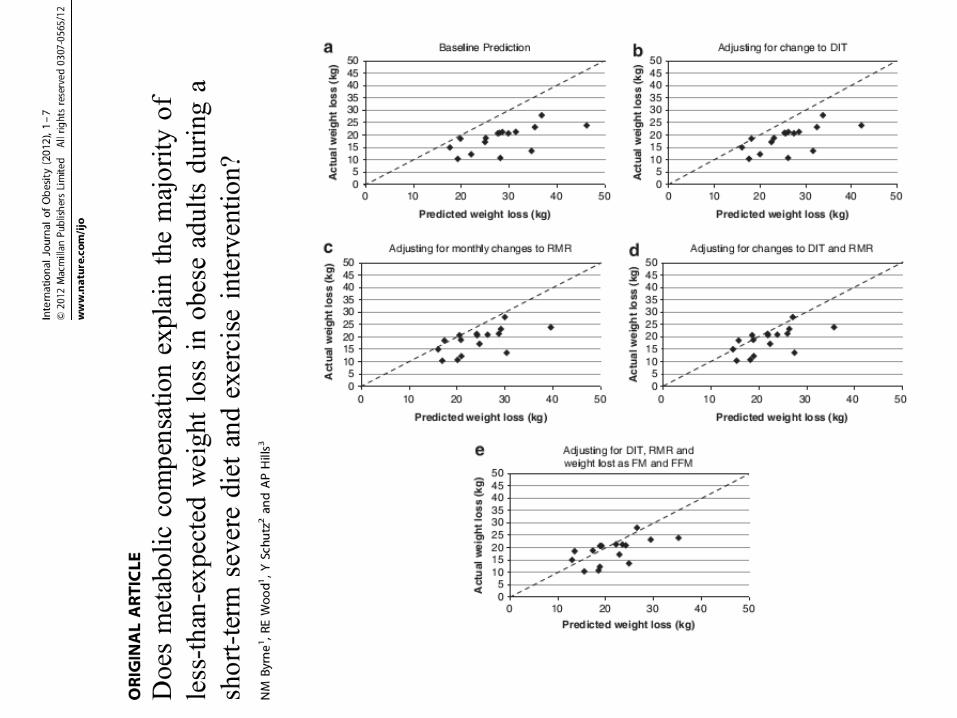
taller 3: estudio del gasto energético. - seedo.es · taller 3: estudio del gasto energético. p...
TRANSCRIPT
Taller 3: Estudio del gasto energético.
P Matía Martín Servicio de Endocrinología y Nutrición Unidad de Nutrición Hospital Clínico San Carlos Madrid.
ESQUEMA DEL TALLER
• 1.-Componentes del gasto energético • 2.-Utilidad práctica de la estimación del gasto energético • 3.-Estimación del gasto energético basal y en reposo
– Fórmulas – Calorimetría indirecta – Sensores
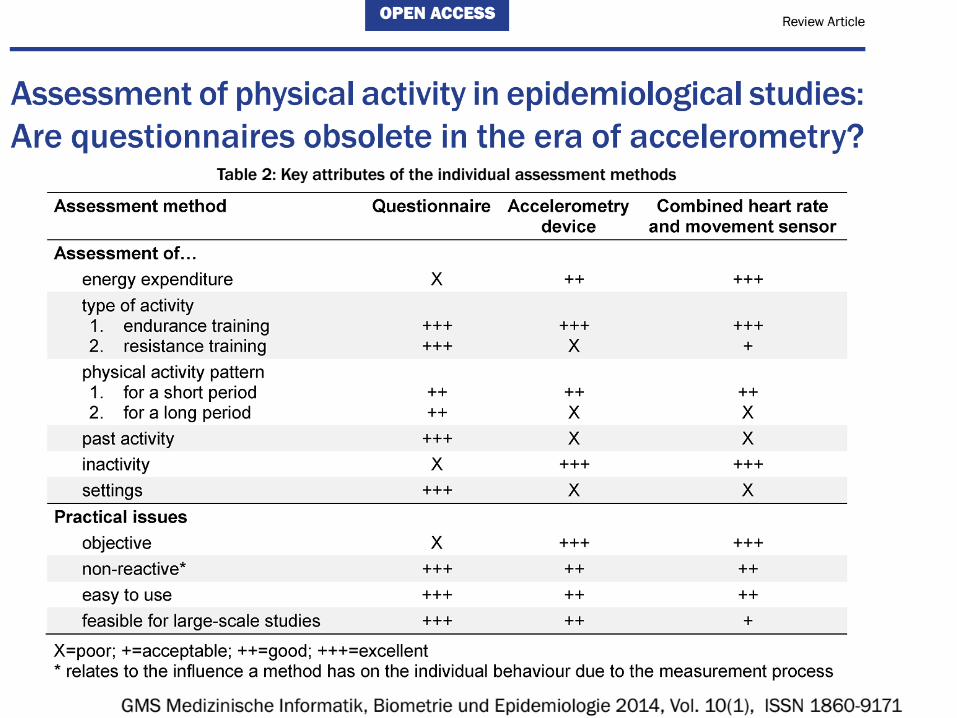
• 4.-Estimación del gasto energético por actividad física – Cuestionarios – Sensores
• 5.-Estimación del consumo de calorías por la dieta • 6.-Estimación del gasto energético en la agresión (el
paciente hospitalizado) • 7.-Nuevas aplicaciones de interés
GASTO ENERGÉTICO
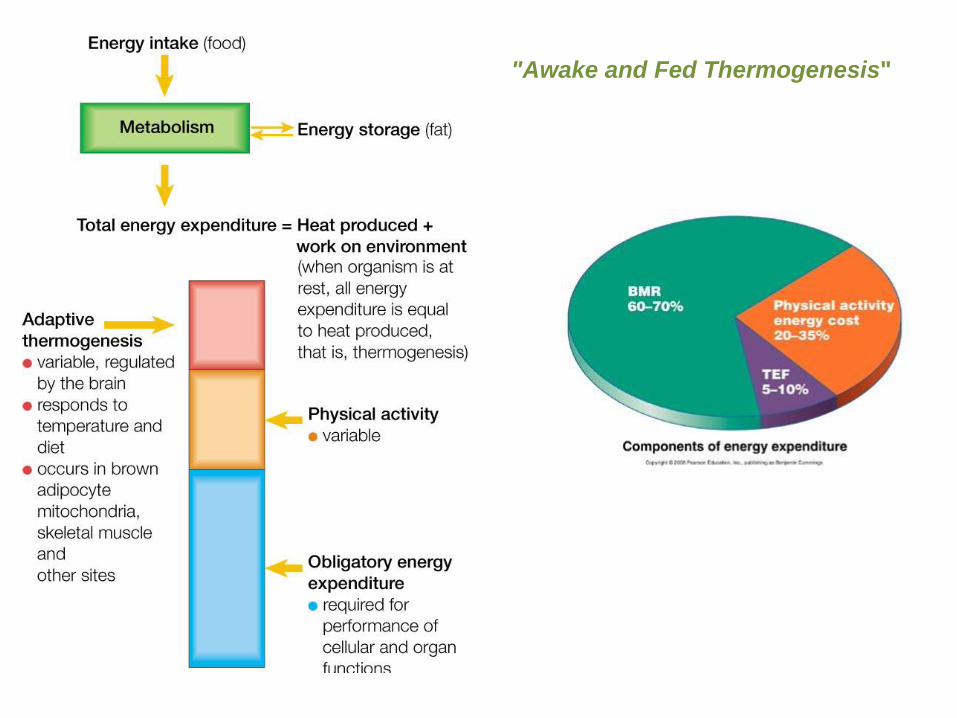
"Awake and Fed Thermogenesis"
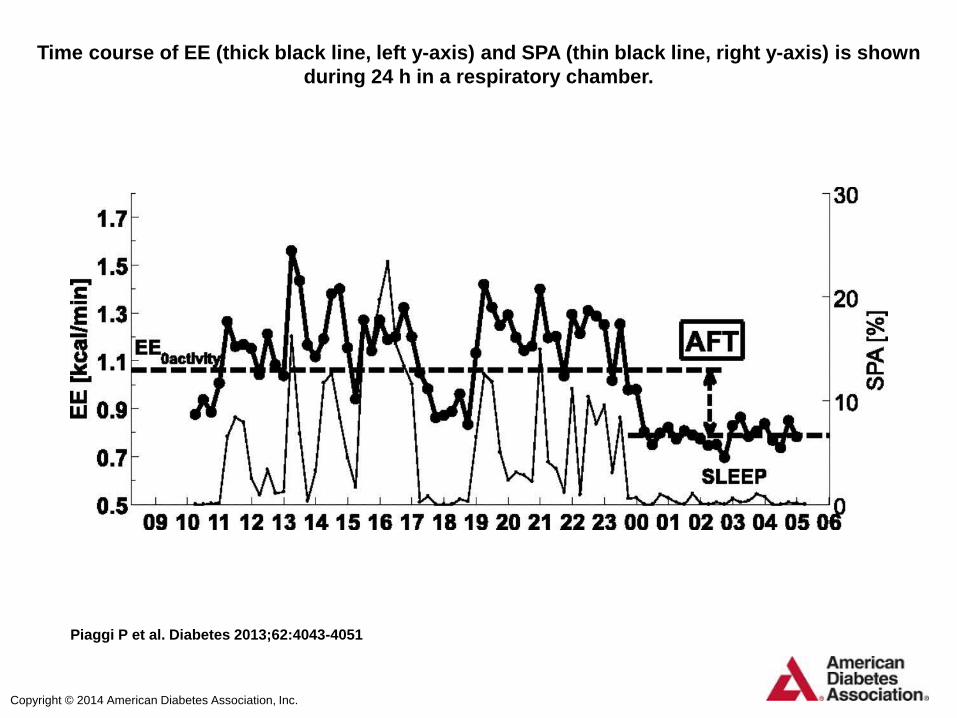
Time course of EE (thick black line, left y-axis) and SPA (thin black line, right y-axis) is shown
during 24 h in a respiratory chamber.
Piaggi P et al. Diabetes 2013;62:4043-4051
Copyright © 2014 American Diabetes Association, Inc.
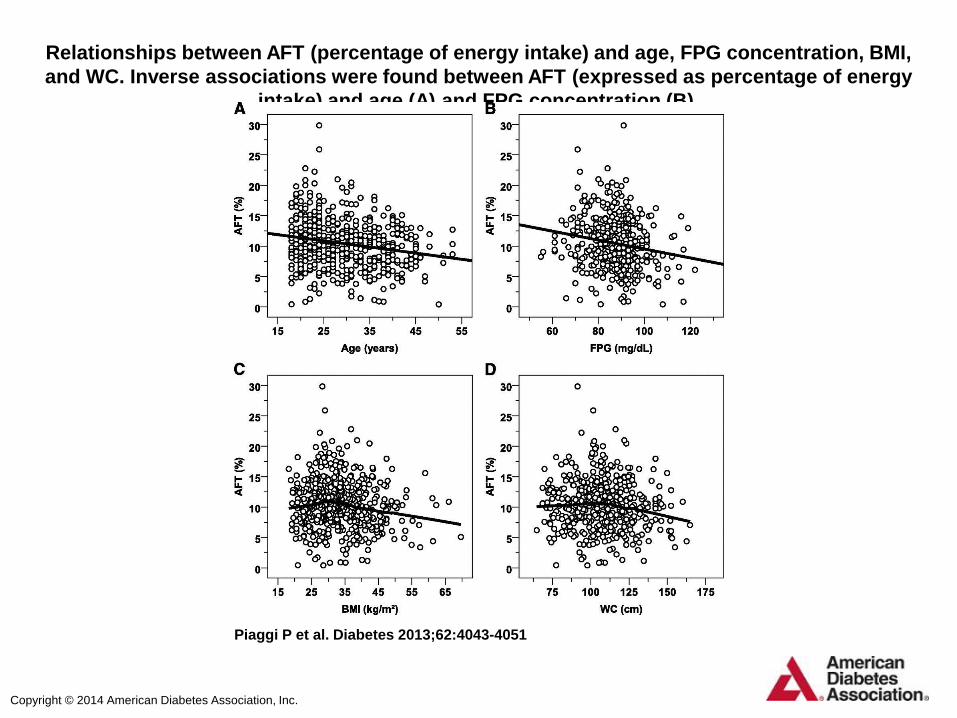
Relationships between AFT (percentage of energy intake) and age, FPG concentration, BMI,
and WC. Inverse associations were found between AFT (expressed as percentage of energy
intake) and age (A) and FPG concentration (B).
Piaggi P et al. Diabetes 2013;62:4043-4051
Copyright © 2014 American Diabetes Association, Inc.
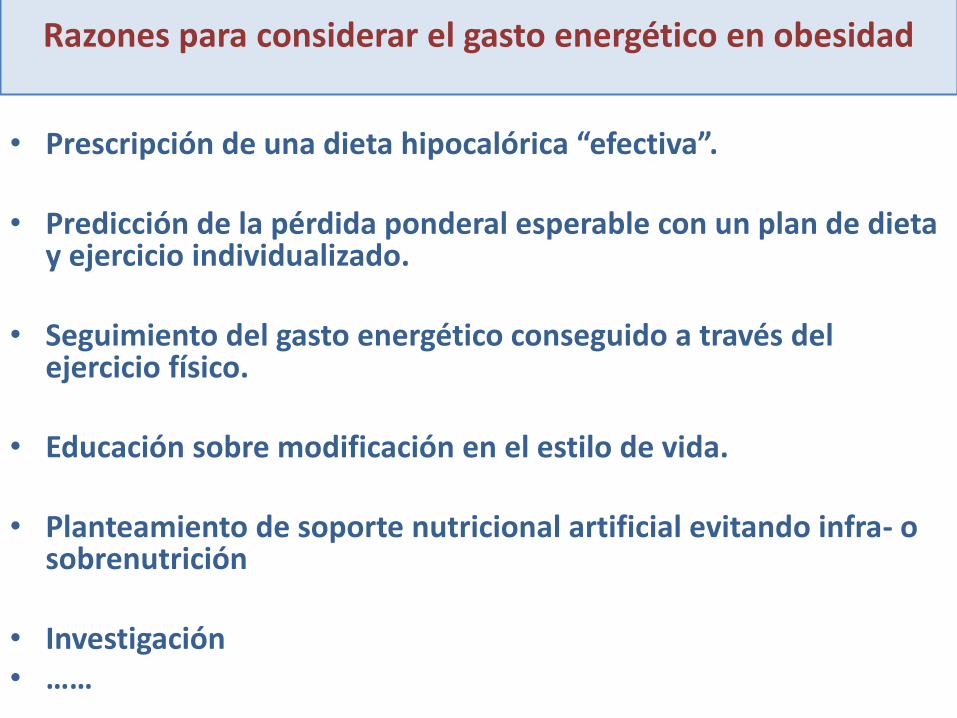
Razones para considerar el gasto energético en obesidad
• Prescripción de una dieta hipocalórica “efectiva”.
• Predicción de la pérdida ponderal esperable con un plan de dieta y ejercicio individualizado.
• Seguimiento del gasto energético conseguido a través del ejercicio físico.
• Educación sobre modificación en el estilo de vida.
• Planteamiento de soporte nutricional artificial evitando infra- o sobrenutrición
• Investigación • ……
CASO 1.-
Mujer de 35 años: • HTA, dislipemia
• Insuficiencia renal (GN extracapilar, p. de Scholein-Henoch). Cuarto
trasplante renal en 2009 –rechazo de los tres previos-. Buena función renal actual –Cl creatinina 77,1 ml/min-. Hiperparatiroidismo secundario.
• ITUs de repetición
• Leucotrombopenia atribuida a enalapril.
• Episodio de TSV controlado con atenolol.
• Queratitis punctata a estudio.
• No consumo de alcohol. No tabaquismo.
• Tratamiento habitual:
– Prednisona 5mg: 1-0-0 –desde primeros trasplantes-
– Prograf (Tacrolimus)
– Rapamune (Sirolimus)
– Coropres: 1-0-1 (Carvedilol)
– Zemplar 1-3 días a la semana (Paricalcitol)
– Atorvastatina 20 mg: 0-0-1
– Nitrofurantoína diaria
– Preparado de arándano
• Motivo de consulta:
Aumento ponderal progresivo desde hace 1 año. Peso habitual: 57 kg
La paciente no refiere cambio de hábitos previos.
La única modificación terapéutica ha sido la introducción de Sirolimus.
CASO 1.-
• Exploración:
Peso 73,25 kg, talla 1,53 m,IMC 31,3 kg/m2. TA 100/70 mmHg. Perímetro cintura: 99 cm. No edemas.
Resto sin alteraciones.
• En análisis:
Glucemia 91 mg/dl, HOMA 1, HbA1c 5,4%.
Función tiroidea normal
Triglicéridos 170 mg/dl.
CASO 1.-
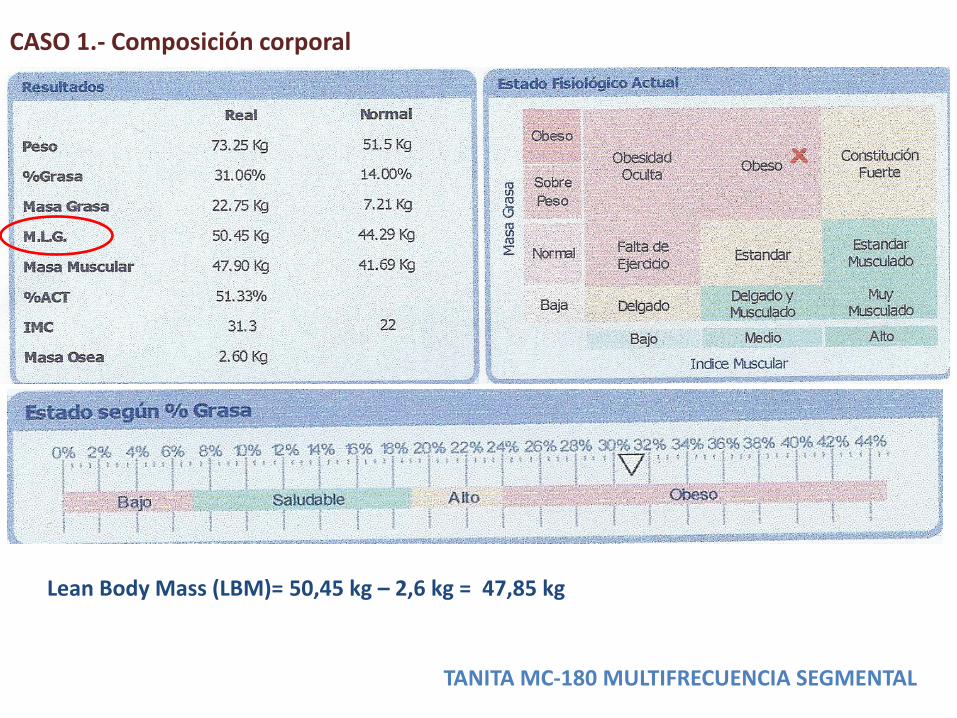
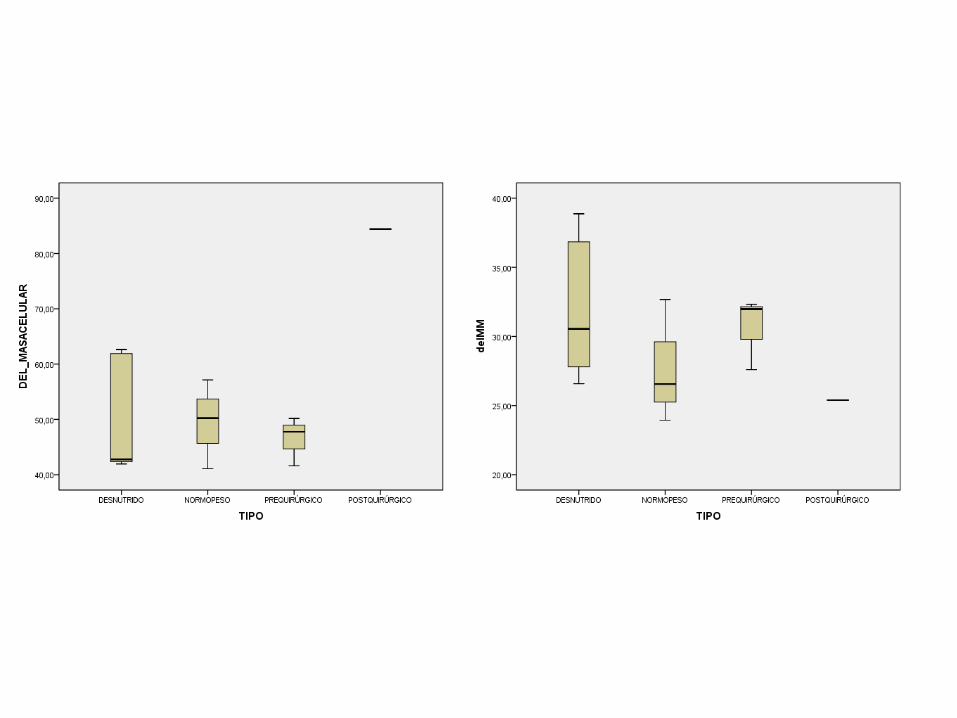
CASO 1.- Composición corporal
TANITA MC-180 MULTIFRECUENCIA SEGMENTAL
Lean Body Mass (LBM)= 50,45 kg – 2,6 kg = 47,85 kg

CALORIMETRÍA DIRECTA

AGUA DOBLEMENTE MARCADA free-living conditions

CÁLCULO DEL GASTO ENERGÉTICO BASAL
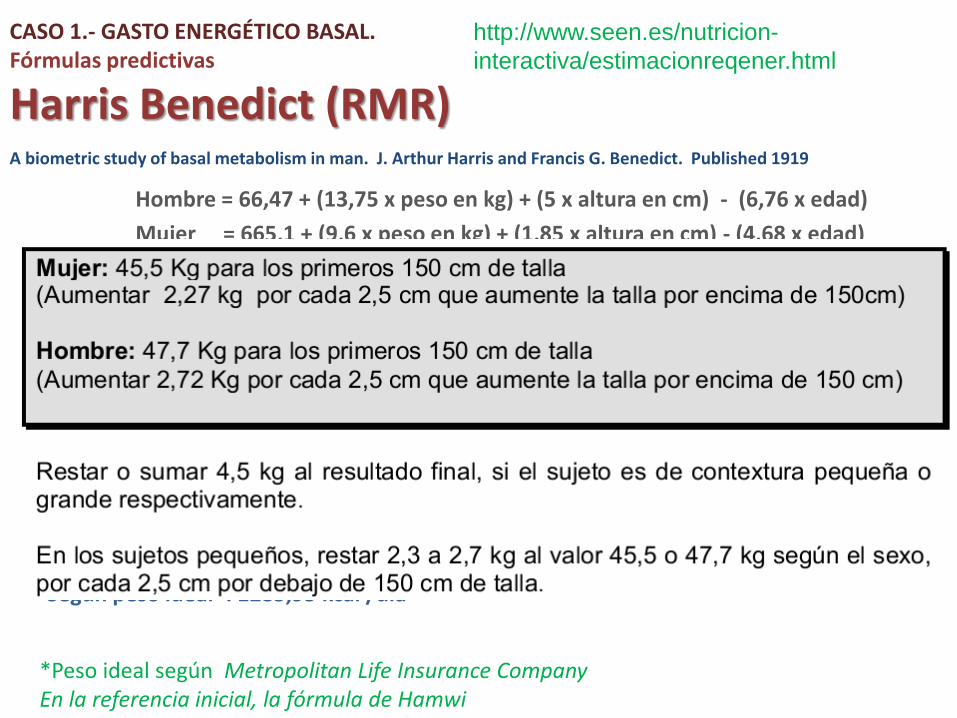
CASO 1.- GASTO ENERGÉTICO BASAL. Fórmulas predictivas
Harris Benedict (RMR)
Hombre = 66,47 + (13,75 x peso en kg) + (5 x altura en cm) - (6,76 x edad)
Mujer = 665,1 + (9,6 x peso en kg) + (1,85 x altura en cm) - (4,68 x edad)
A biometric study of basal metabolism in man. J. Arthur Harris and Francis G. Benedict. Published 1919
-Según peso real: 1815,15 kcal /día -Según peso ajustado: 1336,35 kcal /día -Según peso ideal*: 1285,95 kcal /día
*Peso ideal según Metropolitan Life Insurance Company En la referencia inicial, la fórmula de Hamwi
http://www.seen.es/nutricion-
interactiva/estimacionreqener.html

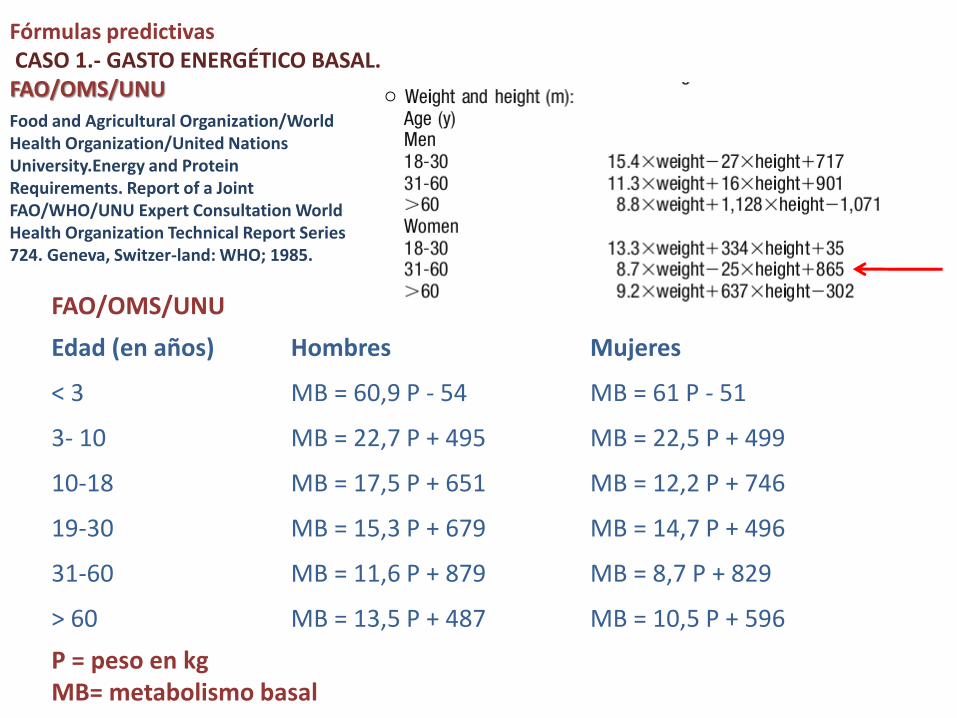
FAO/OMS/UNU
Edad (en años) Hombres Mujeres
< 3 MB = 60,9 P - 54 MB = 61 P - 51
3- 10 MB = 22,7 P + 495 MB = 22,5 P + 499
10-18 MB = 17,5 P + 651 MB = 12,2 P + 746
19-30 MB = 15,3 P + 679 MB = 14,7 P + 496
31-60 MB = 11,6 P + 879 MB = 8,7 P + 829
> 60 MB = 13,5 P + 487 MB = 10,5 P + 596
P = peso en kg MB= metabolismo basal
Fórmulas predictivas CASO 1.- GASTO ENERGÉTICO BASAL. FAO/OMS/UNU
Food and Agricultural Organization/World Health Organization/United Nations University.Energy and Protein Requirements. Report of a Joint FAO/WHO/UNU Expert Consultation World Health Organization Technical Report Series 724. Geneva, Switzer-land: WHO; 1985.
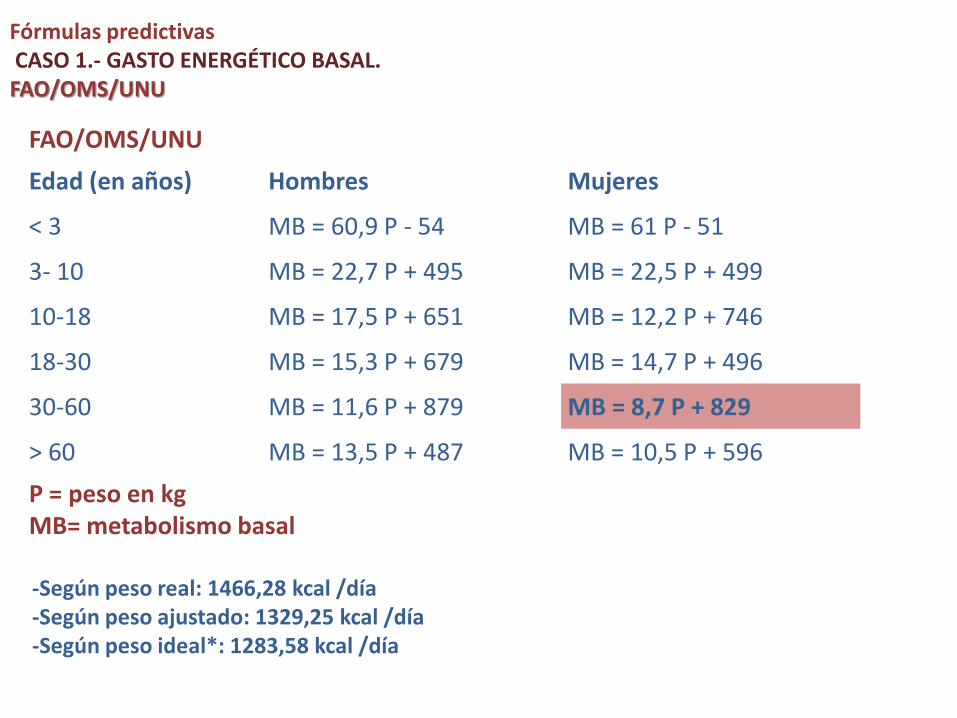
Fórmulas predictivas CASO 1.- GASTO ENERGÉTICO BASAL. FAO/OMS/UNU
FAO/OMS/UNU
Edad (en años) Hombres Mujeres
< 3 MB = 60,9 P - 54 MB = 61 P - 51
3- 10 MB = 22,7 P + 495 MB = 22,5 P + 499
10-18 MB = 17,5 P + 651 MB = 12,2 P + 746
18-30 MB = 15,3 P + 679 MB = 14,7 P + 496
30-60 MB = 11,6 P + 879 MB = 8,7 P + 829
> 60 MB = 13,5 P + 487 MB = 10,5 P + 596
P = peso en kg MB= metabolismo basal
-Según peso real: 1466,28 kcal /día -Según peso ajustado: 1329,25 kcal /día -Según peso ideal*: 1283,58 kcal /día
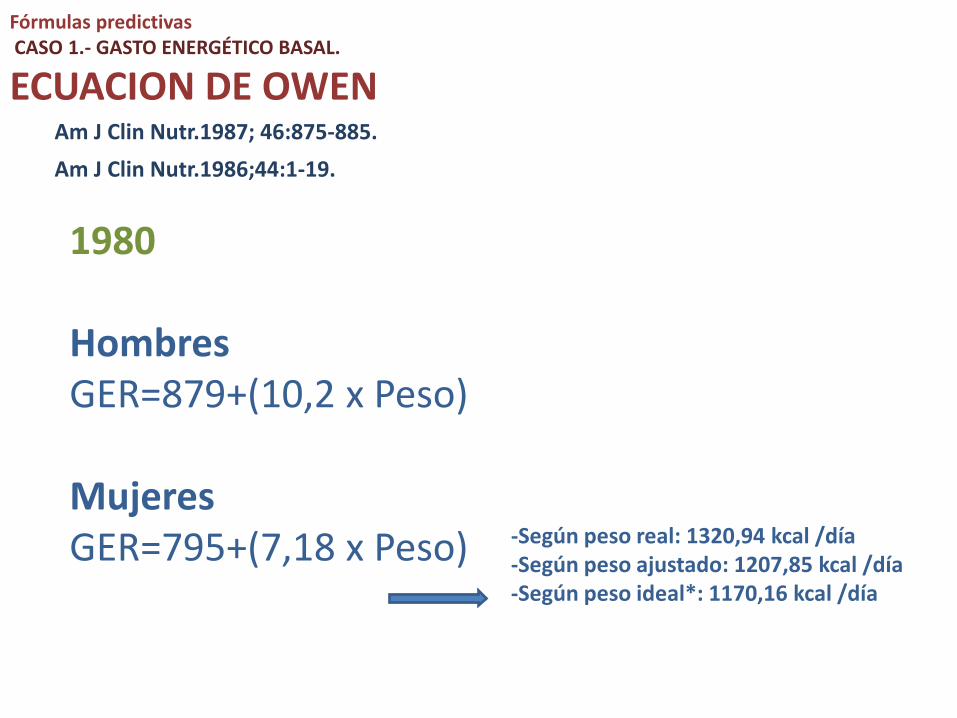
Fórmulas predictivas CASO 1.- GASTO ENERGÉTICO BASAL.
ECUACION DE OWEN
1980 Hombres GER=879+(10,2 x Peso) Mujeres GER=795+(7,18 x Peso)
Am J Clin Nutr.1987; 46:875-885. Am J Clin Nutr.1986;44:1-19.
-Según peso real: 1320,94 kcal /día -Según peso ajustado: 1207,85 kcal /día -Según peso ideal*: 1170,16 kcal /día

ECUACION DE MIFFLIN-ST. JEOR • Hombres
GER= 9,99 x peso + 6,25 x talla -4,92 x edad + 5
• Mujeres GER= 9,99 x peso + 6,25 x talla -4,92 x edad -161
Mifflin, MD; St Jeor, ST; Hill, LA; Scott, BJ; Daugherty, SA; Koh, YO (1990). "A new predictive equation for resting energy expenditure in healthy individuals". The American journal of clinical nutrition 51 (2): 241–7.
(RMR)
-Según peso real: 1354,82 kcal /día -Según peso ajustado: 1197,48 kcal /día -Según peso ideal*: 1145,03 kcal /día
CASO 1.- GASTO ENERGÉTICO BASAL. Fórmulas predictivas
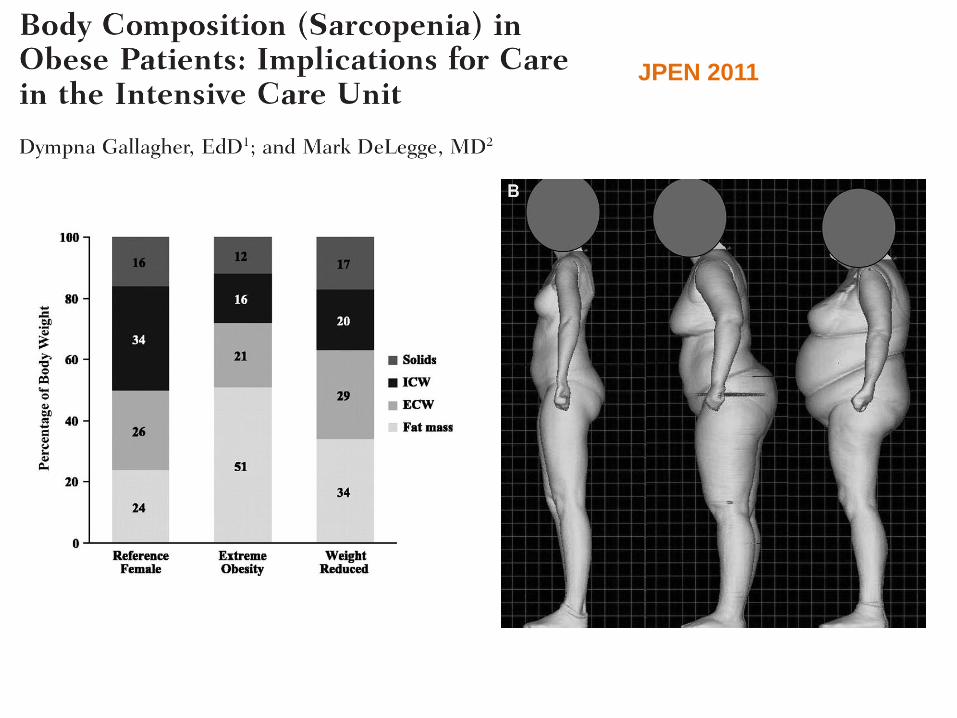
JPEN 2011
Fórmula de Katch-McArdle (BMR):
GER=370+(21,6 x LBM* –kg-)
*Lean Body Mass
1403,56 kcal /día
CASO 1.- GASTO ENERGÉTICO BASAL. Fórmulas predictivas
ECUACION DE CUNNINGHAM
GER=500+(22 x LBM* –kg-)
Reanalysis of the factors influencing basal metabolic rate in normal adults.Am J Clin Nutr. 1980;33: 2372– 4.
*Lean Body Mass
1552,70 kcal /día
CASO 1.- GASTO ENERGÉTICO BASAL. Fórmulas predictivas
10-18 años, GER= 8,4 P + 4,5 T + 200
18-30 años, GER= 13,7 P + 2,8 T + 99
30-60 años, GER= 8,2 P + 0,01 T + 847
Schofield WN: Predicting basal metabolic rate, new standards and review of previous work. Human Nutrition: Clinical Nutrition 1985; 39C (Supl. 1): 5-41
CASO 1.- GASTO ENERGÉTICO BASAL. Fórmulas predictivas
-Según peso real: 1449,18 kcal /día -Según peso ajustado: 1320,03 kcal /día -Según peso ideal*: 1276,98 kcal /día
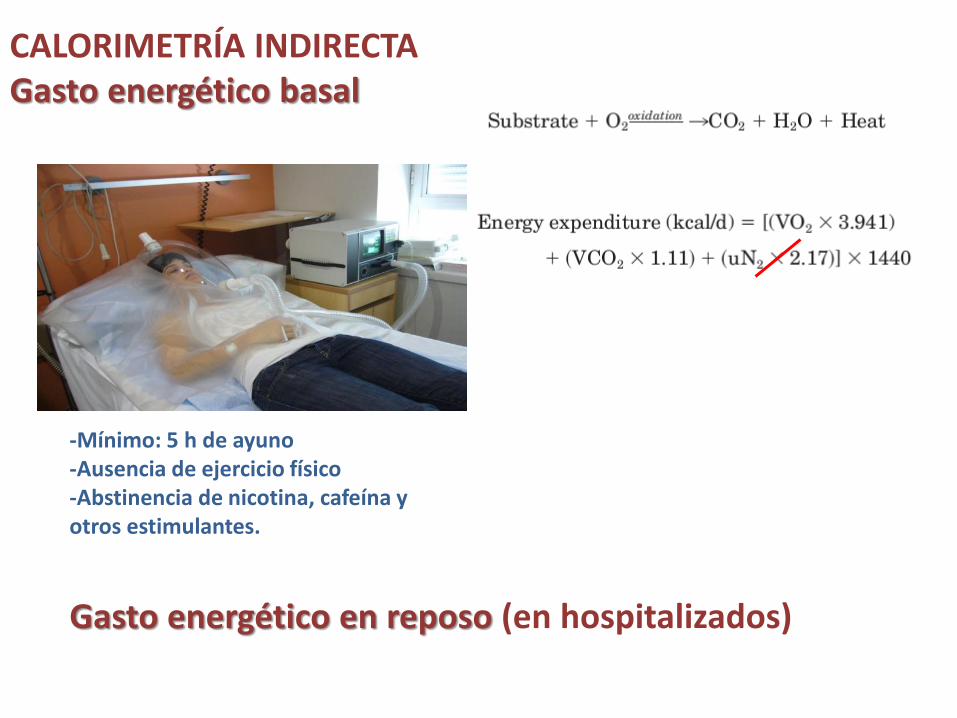
CALORIMETRÍA INDIRECTA Gasto energético basal
-Mínimo: 5 h de ayuno -Ausencia de ejercicio físico -Abstinencia de nicotina, cafeína y otros estimulantes.
Gasto energético en reposo (en hospitalizados)
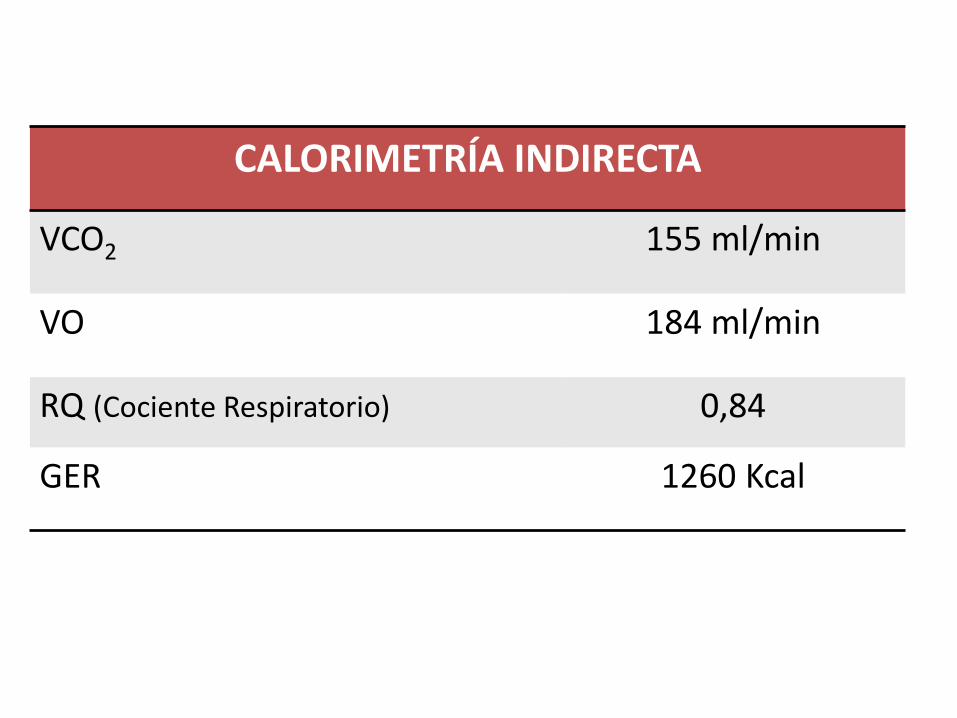
CALORIMETRÍA INDIRECTA
VCO2 155 ml/min
VO 184 ml/min
RQ (Cociente Respiratorio) 0,84
GER 1260 Kcal
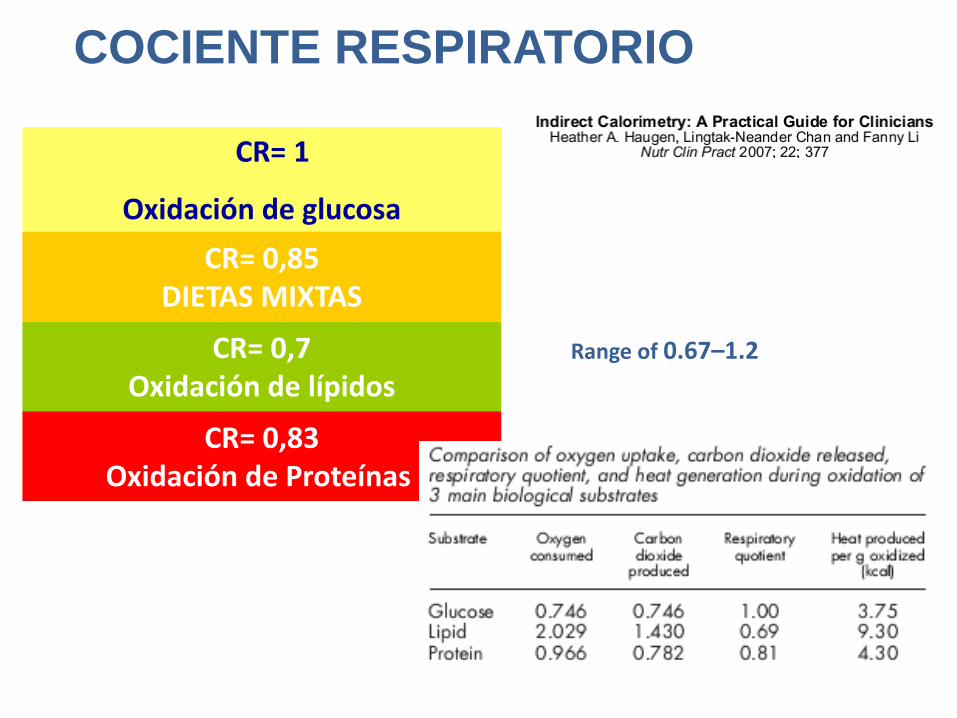
COCIENTE RESPIRATORIO
CR= 1
Oxidación de glucosa
CR= 0,7 Oxidación de lípidos
CR= 0,83 Oxidación de Proteínas
CR= 0,85 DIETAS MIXTAS
Range of 0.67–1.2
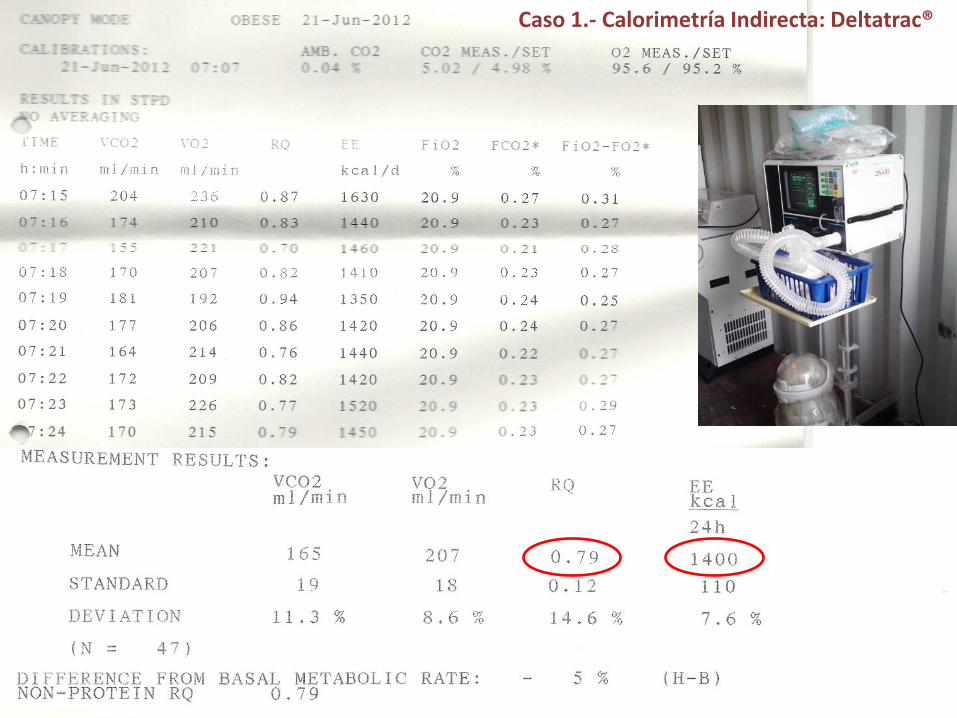
Caso 1.- Calorimetría Indirecta: Deltatrac®

Fitmate®

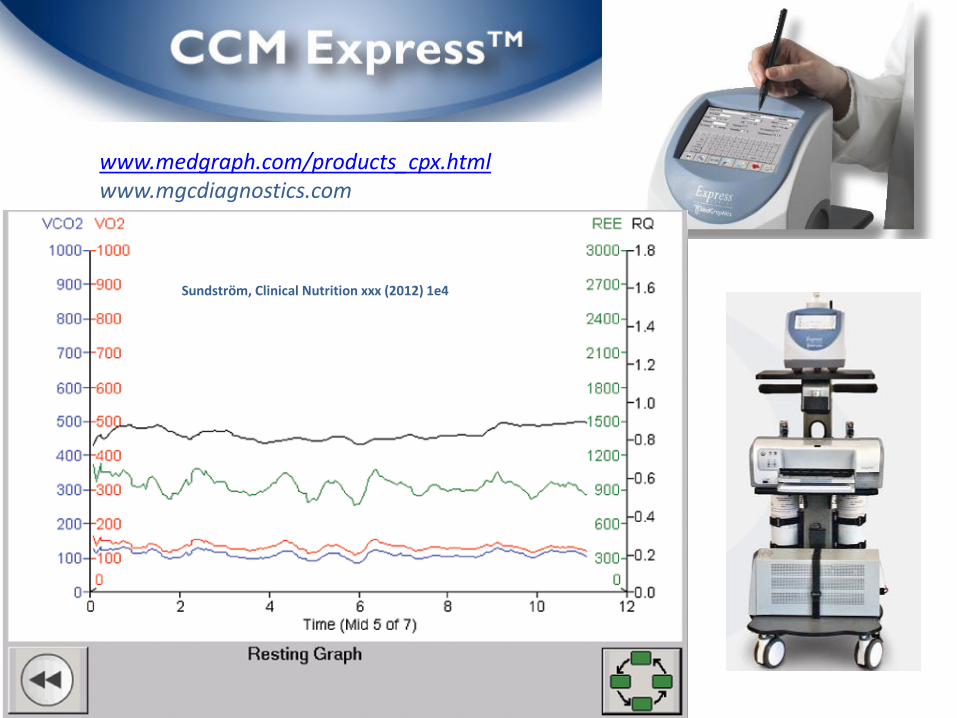
www.medgraph.com/products_cpx.html www.mgcdiagnostics.com
Sundström, Clinical Nutrition xxx (2012) 1e4
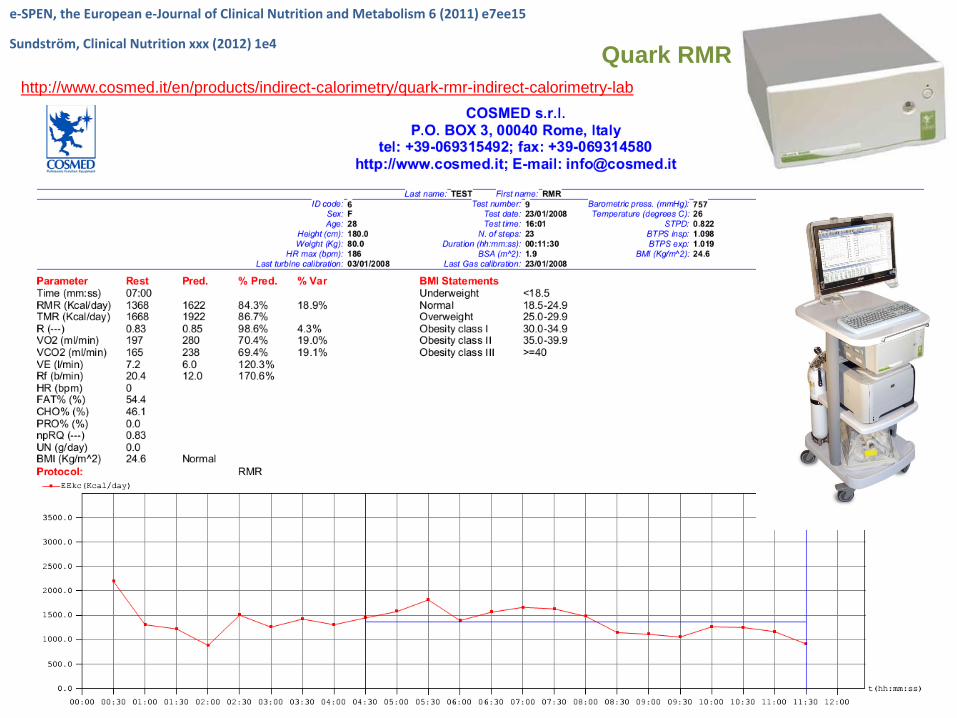
e-SPEN, the European e-Journal of Clinical Nutrition and Metabolism 6 (2011) e7ee15
Sundström, Clinical Nutrition xxx (2012) 1e4 Quark RMR
http://www.cosmed.it/en/products/indirect-calorimetry/quark-rmr-indirect-calorimetry-lab

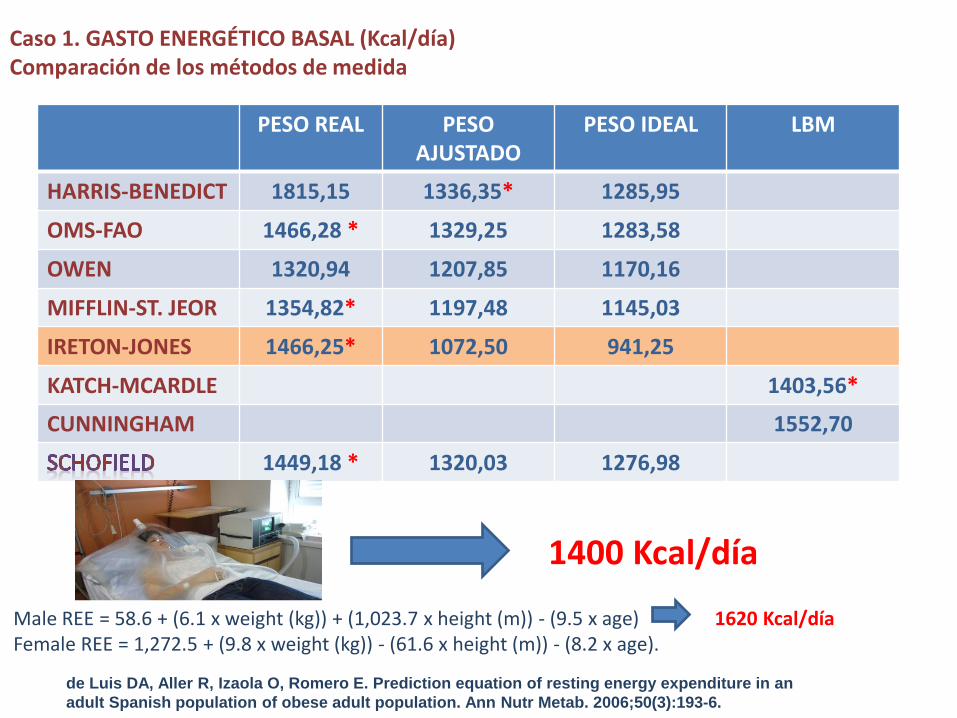
Caso 1. GASTO ENERGÉTICO BASAL (Kcal/día) Comparación de los métodos de medida
PESO REAL PESO AJUSTADO
PESO IDEAL LBM
HARRIS-BENEDICT 1815,15 1336,35* 1285,95
OMS-FAO 1466,28 * 1329,25 1283,58
OWEN 1320,94 1207,85 1170,16
MIFFLIN-ST. JEOR 1354,82* 1197,48 1145,03
IRETON-JONES 1466,25* 1072,50 941,25
KATCH-MCARDLE 1403,56*
CUNNINGHAM 1552,70
1449,18 * 1320,03 1276,98
1400 Kcal/día
de Luis DA, Aller R, Izaola O, Romero E. Prediction equation of resting energy expenditure in an
adult Spanish population of obese adult population. Ann Nutr Metab. 2006;50(3):193-6.
Male REE = 58.6 + (6.1 x weight (kg)) + (1,023.7 x height (m)) - (9.5 x age) Female REE = 1,272.5 + (9.8 x weight (kg)) - (61.6 x height (m)) - (8.2 x age).
1620 Kcal/día
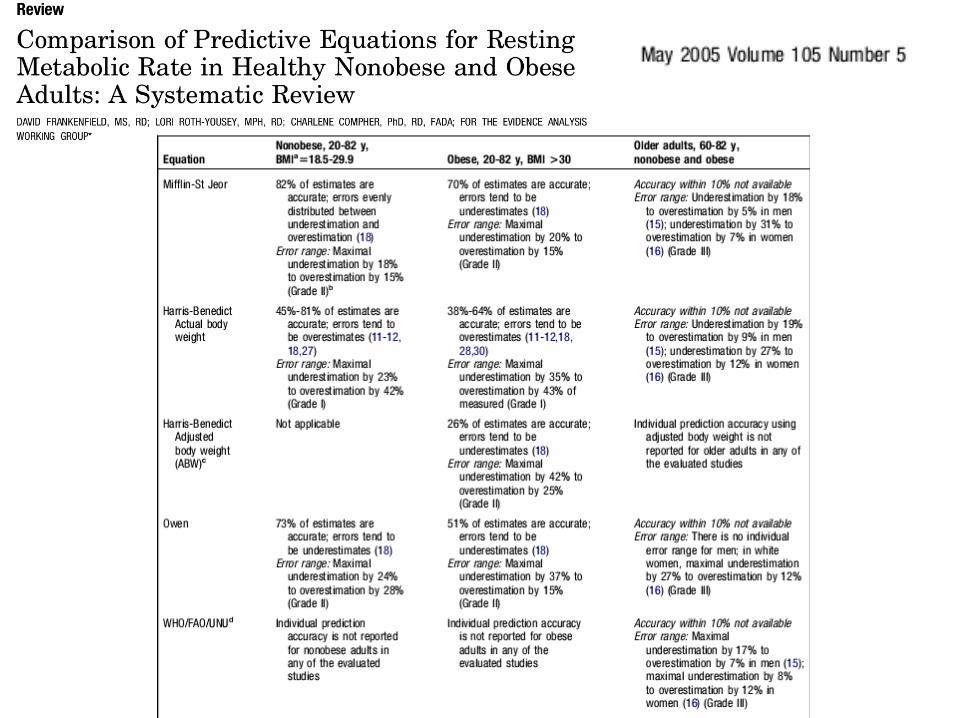
ECUACION DE MIFFLIN-ST. JEOR*** ECUACIÓN DE HARRIS-BENEDICT ECUACIÓN DE OWEN FAO/OMS/UNU ?
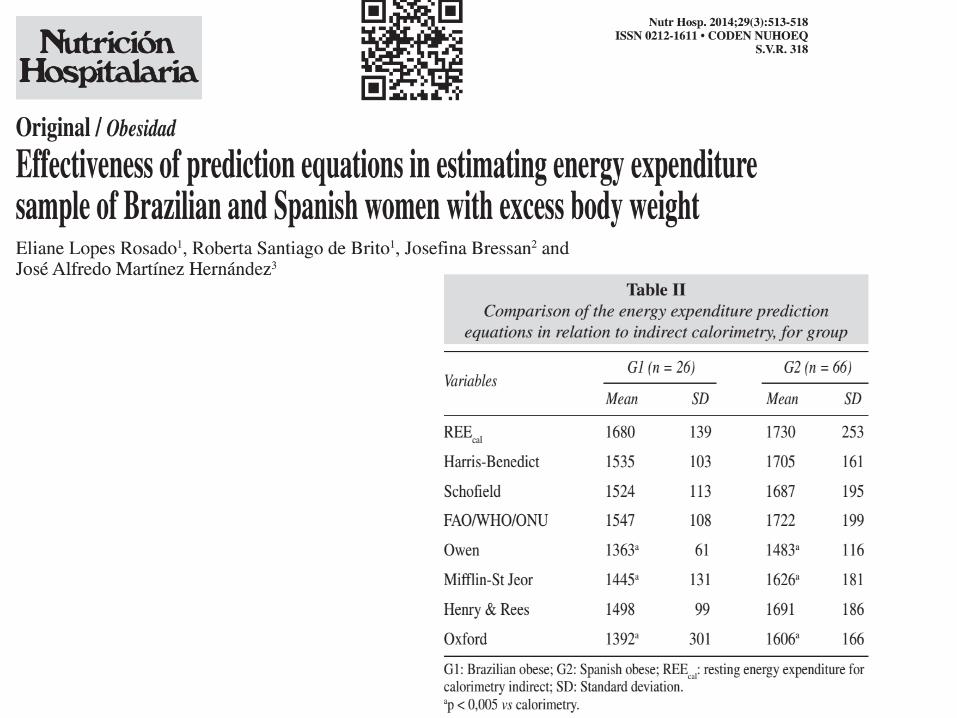
Nutr Hosp. 2007;22:410-6
JPEN.31:217–227,2007
http://www.sediabetes.org/calculadoraGCB.asp
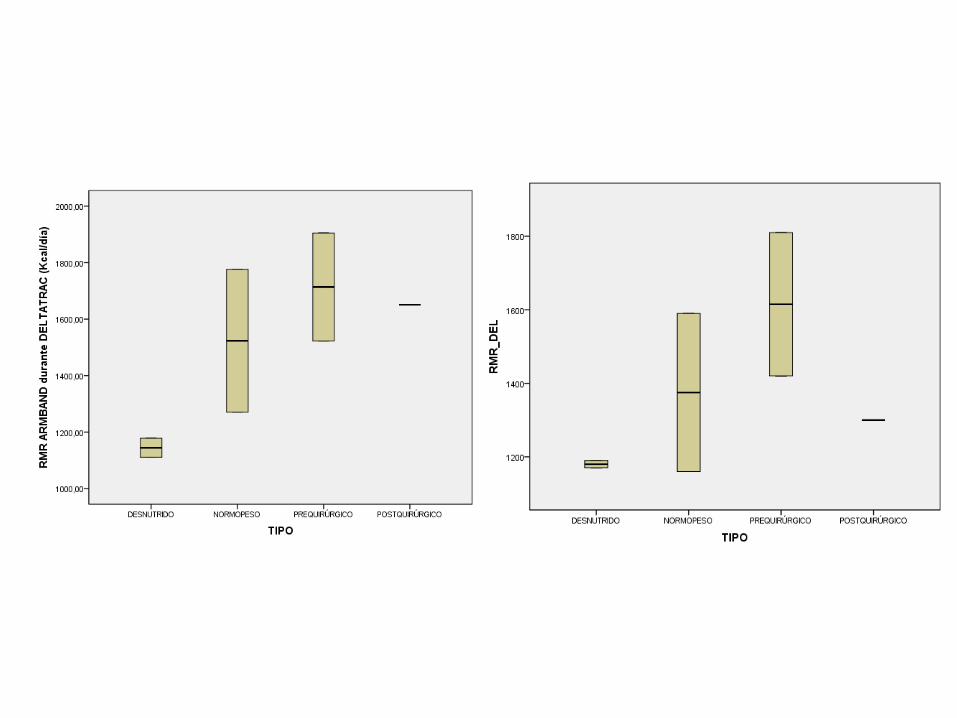
Estimación del gasto energético basal mediante
calorimetría indirecta portátil y holter calórico
Rubio MA, Hernández G, Martín Rojas-Marcos P, Lorenzo L, Matía P, Khreshi W, Sánchez-Pernaute A*, Torres AJ*, Cabrerizo L.
Servicio de Endocrinología y Nutrición y Cirugía General y Digestiva*.
Hospital Clínico San Carlos. Madrid.
Becas: FMM y Vegenat S.A.

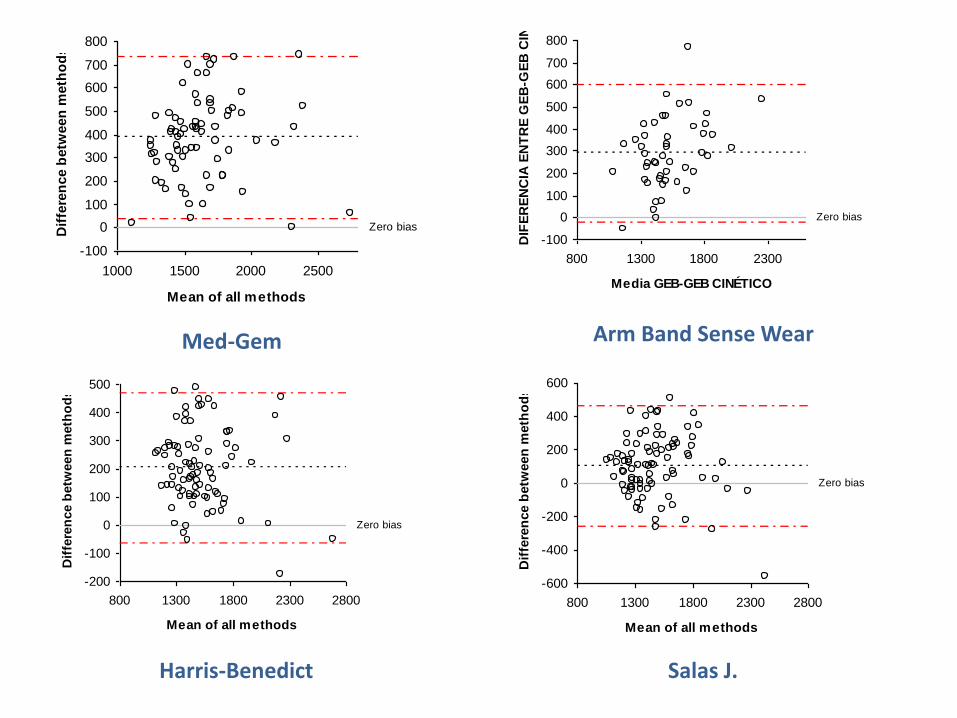
Fórmulas de estimación del GEB • Harris-Benedict
– Hombres: 66 + (13,7 x peso) + (5 x talla) - (6,8 x edad)
– Mujeres: 655 + (9,6 x peso) + (1,9 x talla) – (4,7 x edad)
• Salas J, et al – (12,3 x peso) - (3,4 x talla) – (4,2 x edad) + 1215
• Rubio MA, et al – (12,52 x peso) + 369
Zero bias
-100
0
100
200
300
400
500
600
700
800
1000 1500 2000 2500
Mean of all methods
Dif
fere
nce b
etw
een
meth
od
s
Med-Gem
Zero bias
-100
0
100
200
300
400
500
600
700
800
800 1300 1800 2300
Media GEB-GEB CINÉTICO
DIF
ER
EN
CIA
EN
TR
E G
EB
-GE
B C
INÉ
TIC
O
Arm Band Sense Wear
Zero bias
-200
-100
0
100
200
300
400
500
800 1300 1800 2300 2800
Mean of all methods
Dif
fere
nce b
etw
een
meth
od
s
Harris-Benedict
Zero bias
-600
-400
-200
0
200
400
600
800 1300 1800 2300 2800
Mean of all methods
Dif
fere
nce b
etw
een
meth
od
s
Salas J.

CÁLCULO DEL GASTO ENERGÉTICO POR ACTIVIDAD FÍSICA
Ejercicio físico: 3 veces a la semana gimnasio (mixto; 1,5-2 horas diarias). Resto de los días: caminata. A ritmo moderado. Trabaja en una oficina caminando, subiendo y bajando escaleras durante 7 horas diarias, 5 días a la semana.
CASO 1.-
http://www.fundaciondelcorazon.com/ejercicio/calculadoras.html
http://deportesinquimica.blogspot.com.es/2011/02/calculo-gasto-
calorico-diario-tmb-
gasto.html?Weight=73&WeightUnit=2.2&Time=100&TimeUnit=6
0&Activity=2&Calories=535

Ligera Moderada Alta
Hombres 1.60 1.78 2.10
Mujeres 1.50 1.64 1.90
Fuente: FAO/WHO-OMS/UNU Expert Consultation Report. Energy and Protein Requirements.
Technical Report Series 724. Ginebra:WHO/OMS. 1985
Factores de actividad física
GEB x F actividad física (moderada)= 1400 kcal x 1,64 = 2296 kcal
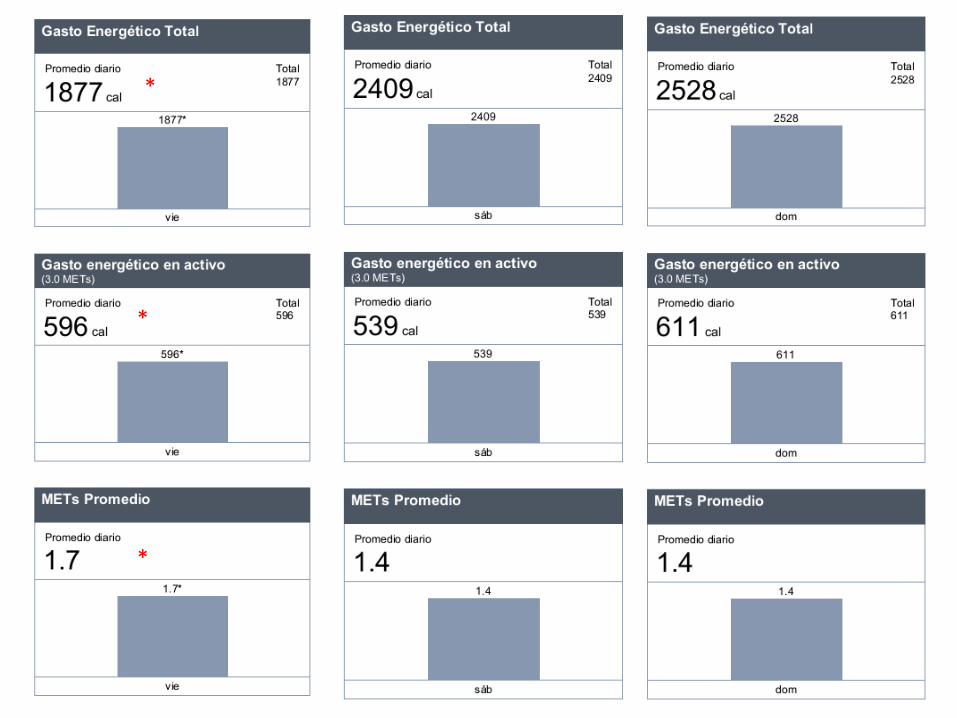
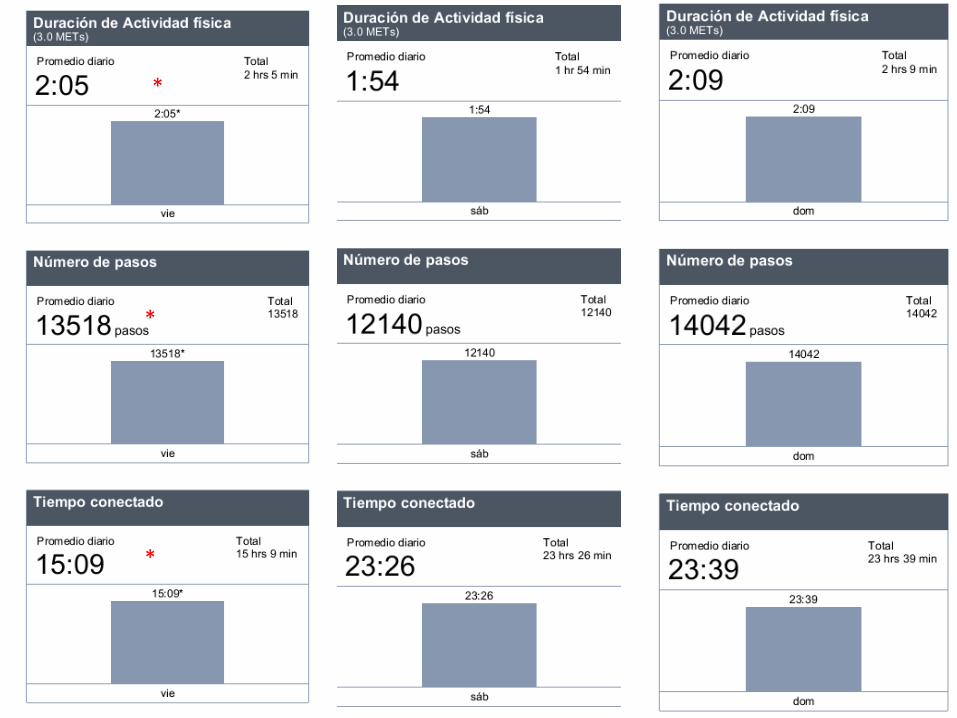
CASO 1.- GASTO ENERGÉTICO TOTAL. Corrección por ACTIVIDAD FÍSICA
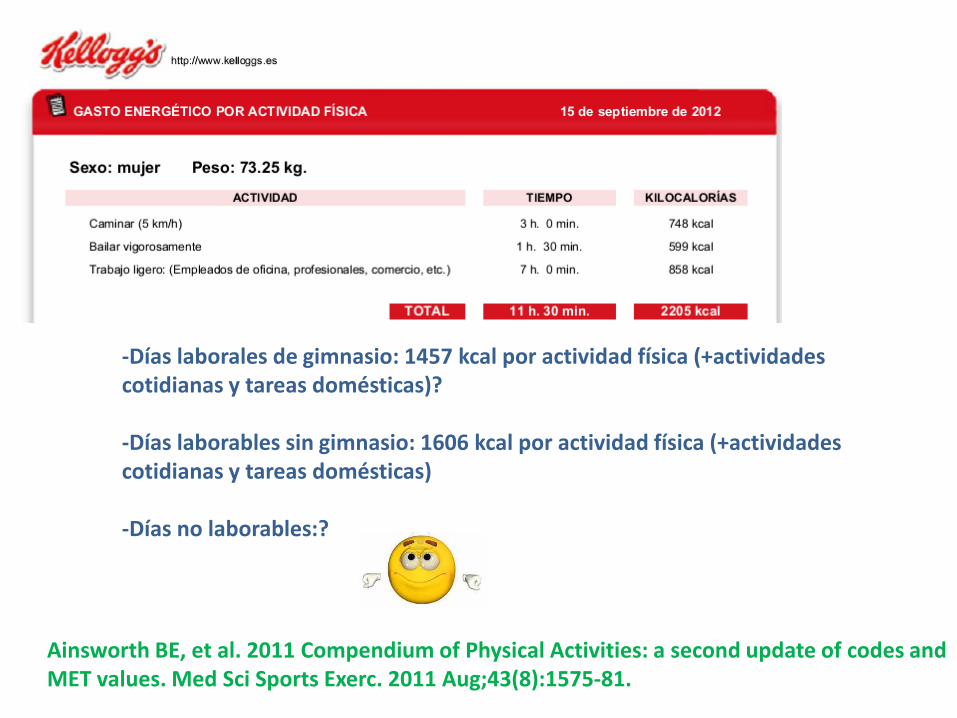
-Días laborales de gimnasio: 1457 kcal por actividad física (+actividades cotidianas y tareas domésticas)? -Días laborables sin gimnasio: 1606 kcal por actividad física (+actividades cotidianas y tareas domésticas) -Días no laborables:?
Ainsworth BE, et al. 2011 Compendium of Physical Activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011 Aug;43(8):1575-81.
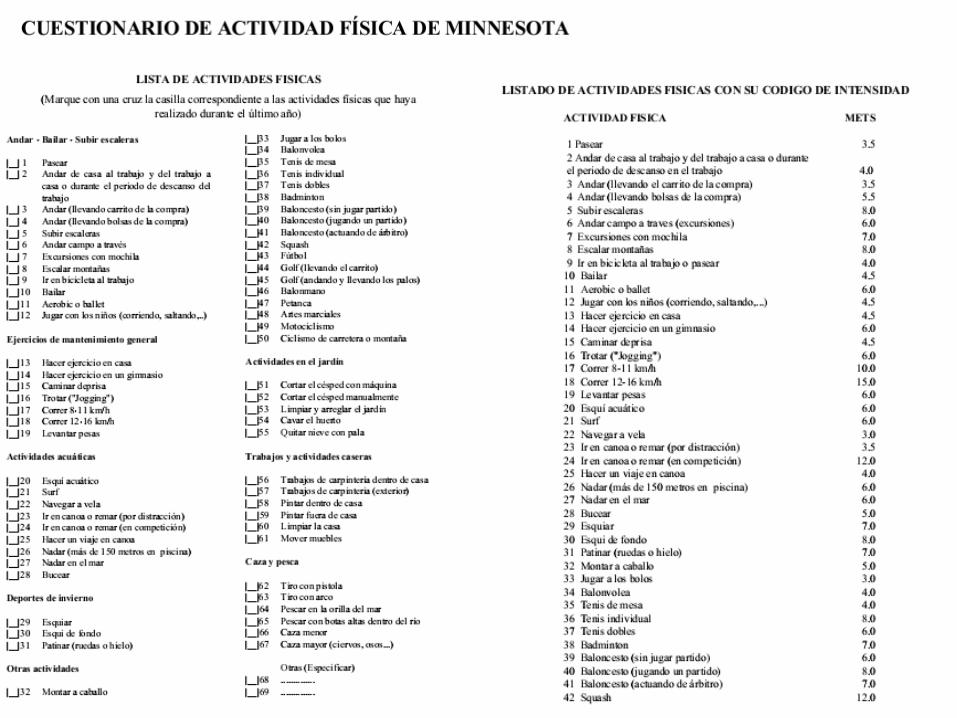

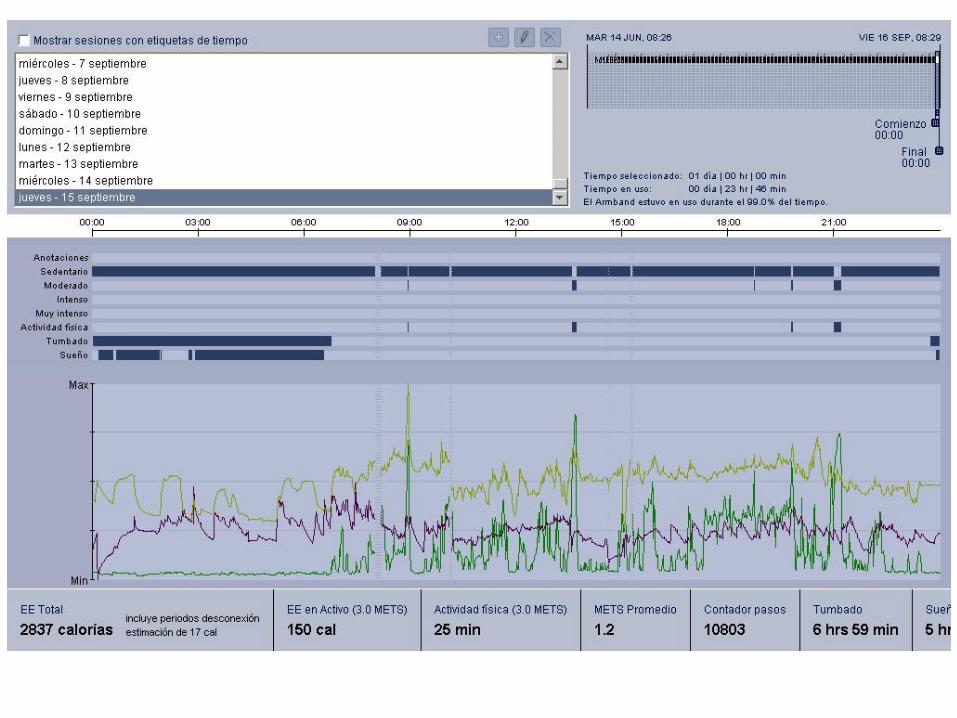
Se consideran dos definiciones de persona activa: a) tener un gasto energético total diario en tiempo libre >300 equivalentes metabólicos (MET) y b) realizar ejercicio físico en actividades ≥4 MET al menos 25min diarios las mujeres y 30 los hombres
Gac Sanit. 2009;23(2):127–132
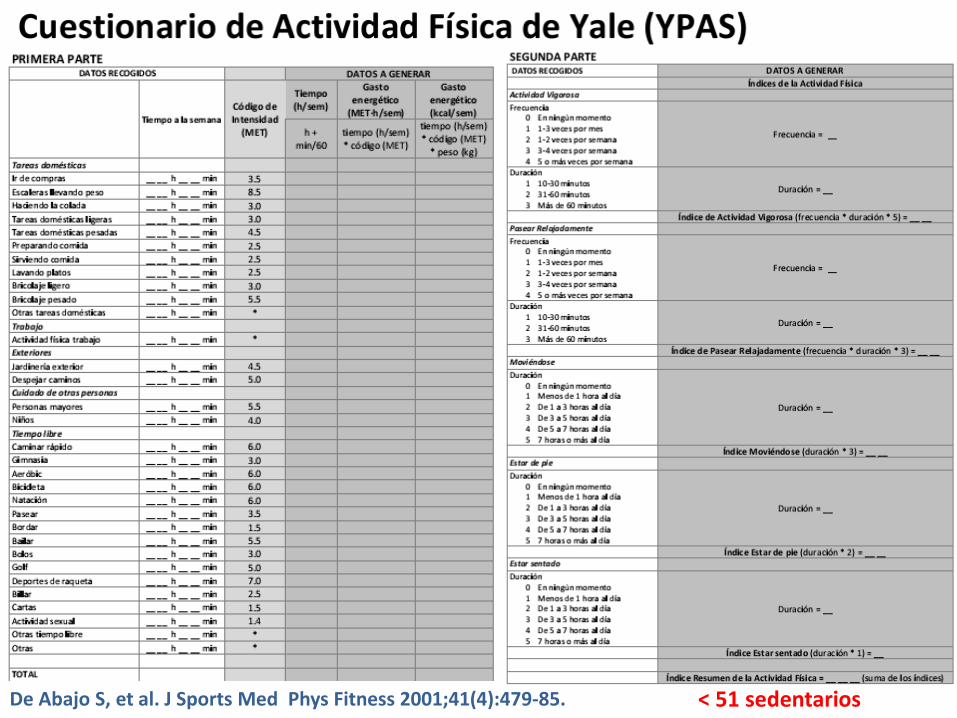
De Abajo S, et al. J Sports Med Phys Fitness 2001;41(4):479‐85. < 51 sedentarios
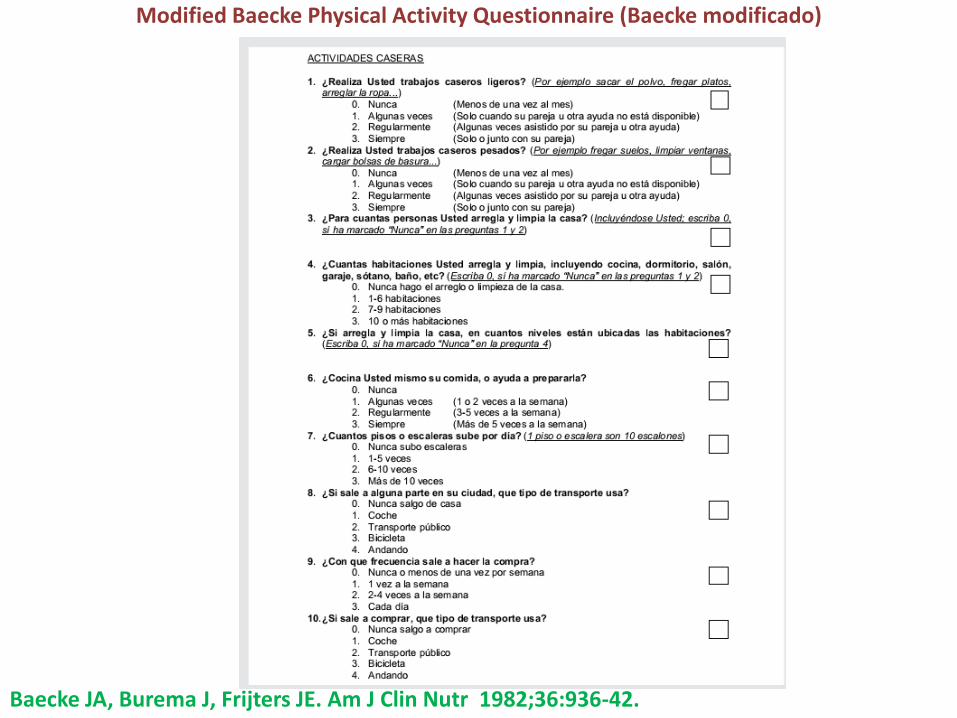
Modified Baecke Physical Activity Questionnaire (Baecke modificado)
Baecke JA, Burema J, Frijters JE. Am J Clin Nutr 1982;36:936-42.

Los sujetos con valores inferiores a 9 se
consideran sedentarios, entre 9-16, sedentarios
moderados, y por encima de 16, activos
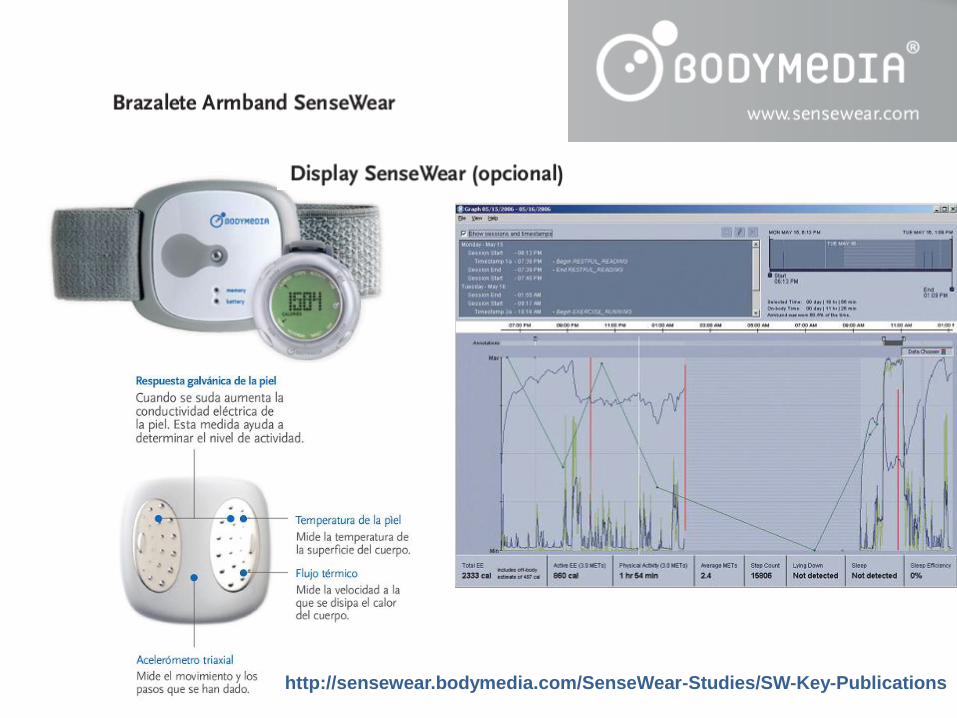
http://sensewear.bodymedia.com/SenseWear-Studies/SW-Key-Publications
*
*
*
*
*
*

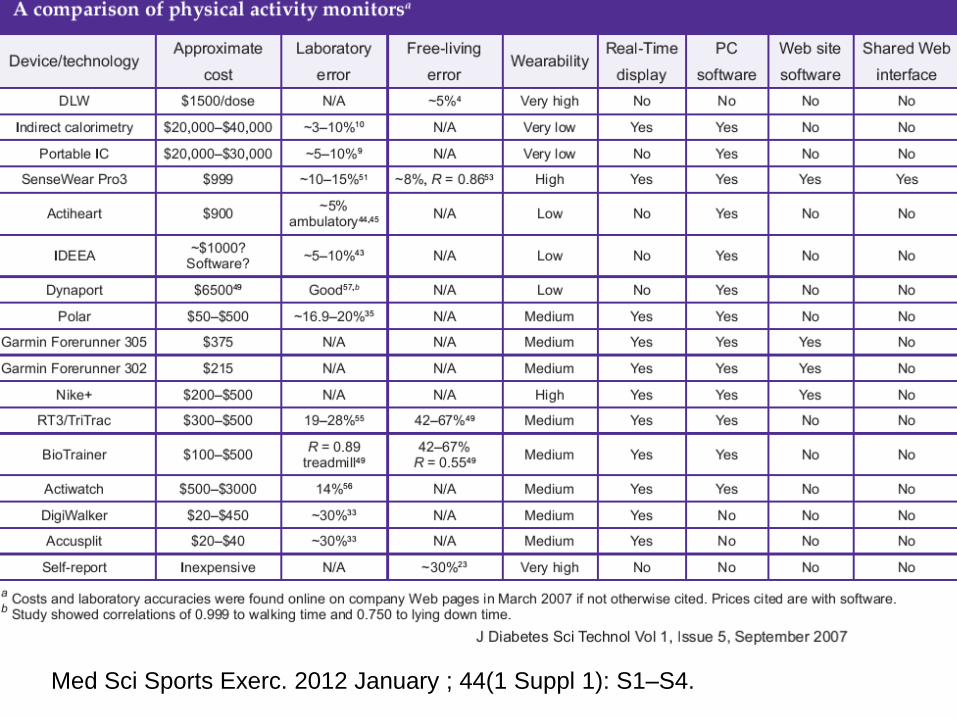
Med Sci Sports Exerc. 2012 January ; 44(1 Suppl 1): S1–S4.

El mundo de las “Apps”
Contador de
Calorías FatSecret MyFitnessPal, LLC
Runtastic Runtastic Pedometer
Calorie Counter

CÁLCULO DE LA INGESTA DE CALORÍAS CON LA
DIETA
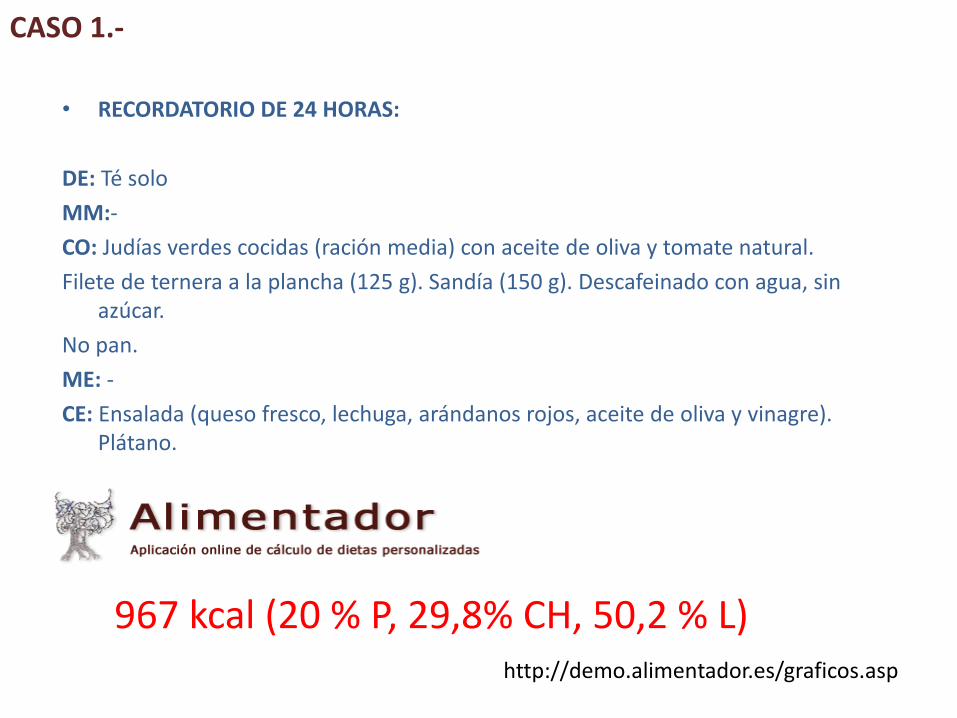
• RECORDATORIO DE 24 HORAS:
DE: Té solo
MM:-
CO: Judías verdes cocidas (ración media) con aceite de oliva y tomate natural.
Filete de ternera a la plancha (125 g). Sandía (150 g). Descafeinado con agua, sin azúcar.
No pan.
ME: -
CE: Ensalada (queso fresco, lechuga, arándanos rojos, aceite de oliva y vinagre). Plátano.
CASO 1.-
967 kcal (20 % P, 29,8% CH, 50,2 % L) http://demo.alimentador.es/graficos.asp
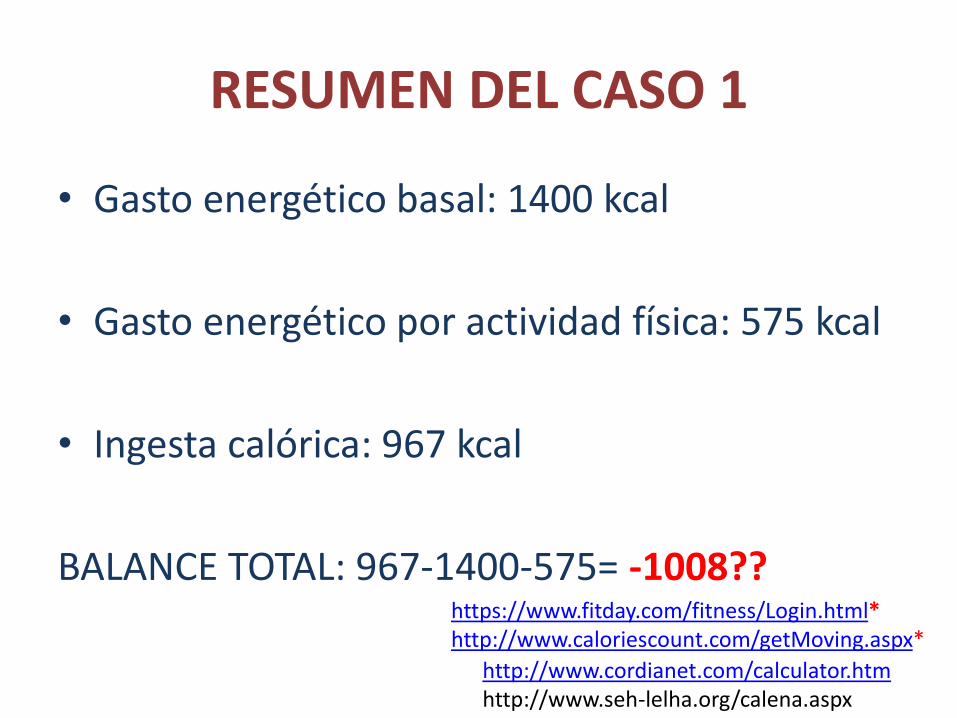
RESUMEN DEL CASO 1
• Gasto energético basal: 1400 kcal
• Gasto energético por actividad física: 575 kcal
• Ingesta calórica: 967 kcal
BALANCE TOTAL: 967-1400-575= -1008?? https://www.fitday.com/fitness/Login.html* http://www.caloriescount.com/getMoving.aspx* http://www.cordianet.com/calculator.htm
http://www.seh-lelha.org/calena.aspx
CASO 2.-
• Varón de 52 años Acude a consulta 4 meses después de cirugía bariátrica (SADIs -Single
Anastomosis Duodeno-Ileal Bypass with Sleeve Gastrectomy-)
Peso precirugía: 168 kg, talla 1,81 m, IMC 51,3 kg/m2
Comorbilidades previas: HTA, SAOS/CPAP, dislipemia
Actualmente:
No complicaciones postquirúrgicas.
No síntomas digestivos
Peso: 130,9 kg (-22 %), talla 1,81 m, IMC 40,4 kg/m2
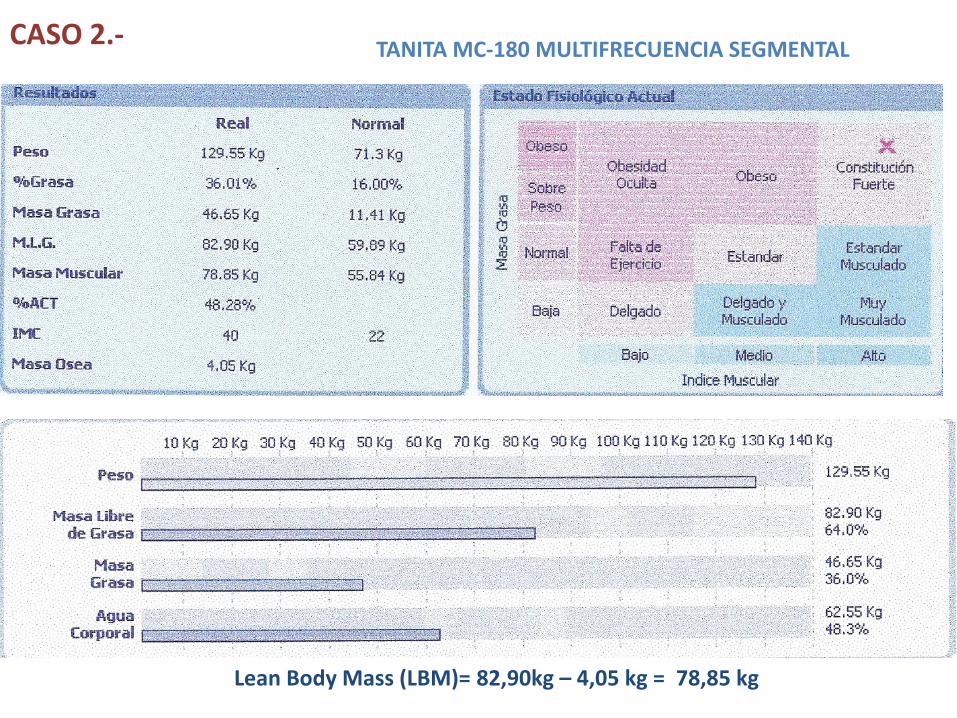
CASO 2.-
Lean Body Mass (LBM)= 82,90kg – 4,05 kg = 78,85 kg
TANITA MC-180 MULTIFRECUENCIA SEGMENTAL
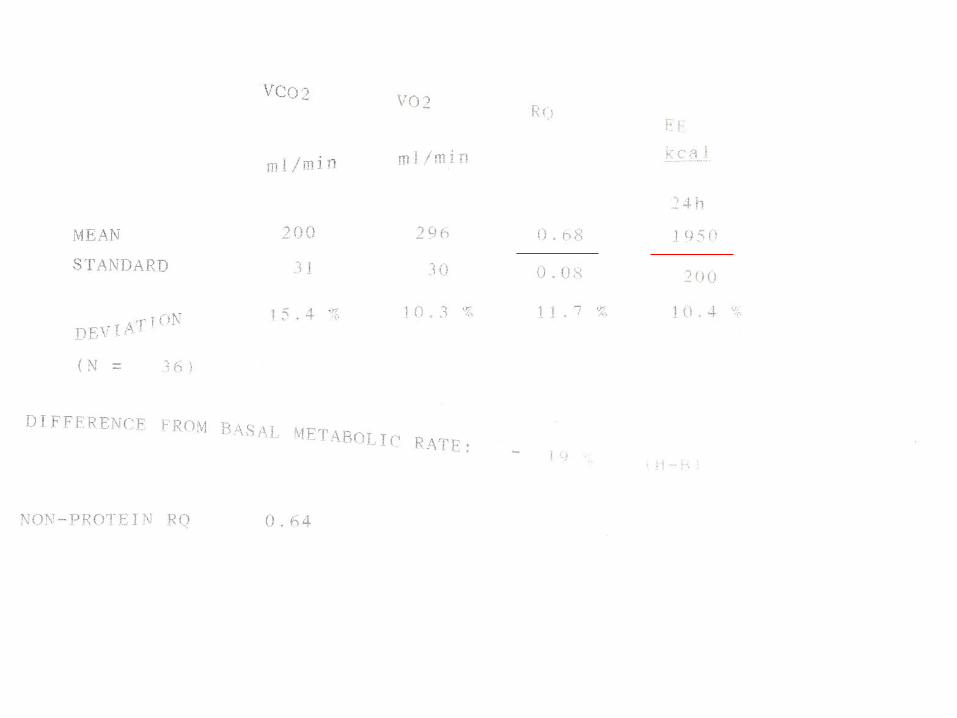
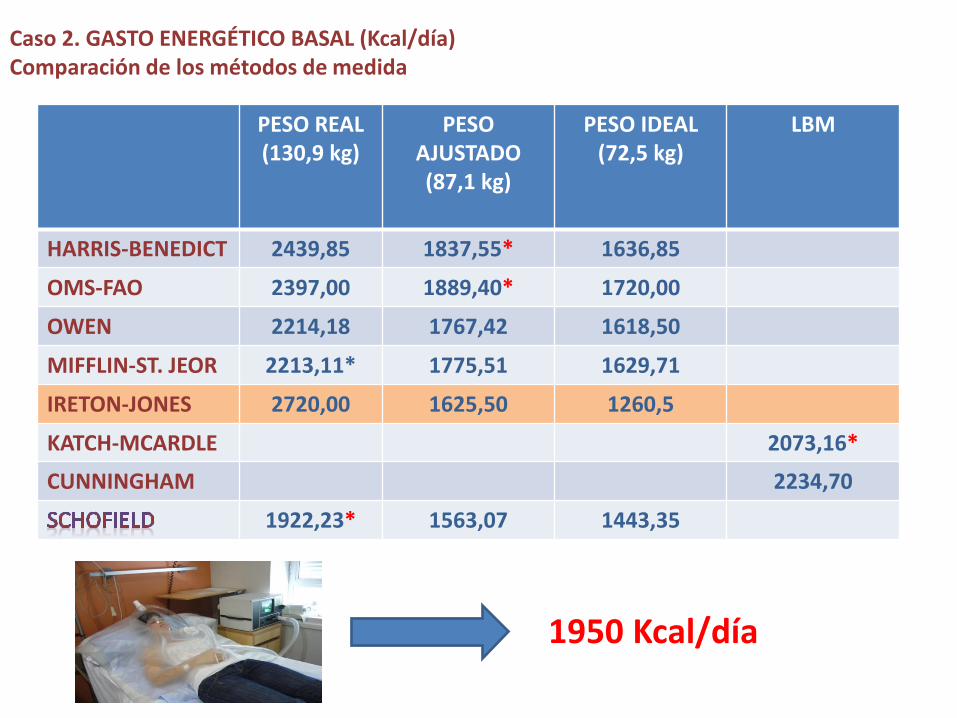
Caso 2. GASTO ENERGÉTICO BASAL (Kcal/día) Comparación de los métodos de medida
PESO REAL (130,9 kg)
PESO AJUSTADO (87,1 kg)
PESO IDEAL (72,5 kg)
LBM
HARRIS-BENEDICT 2439,85 1837,55* 1636,85
OMS-FAO 2397,00 1889,40* 1720,00
OWEN 2214,18 1767,42 1618,50
MIFFLIN-ST. JEOR 2213,11* 1775,51 1629,71
IRETON-JONES 2720,00 1625,50 1260,5
KATCH-MCARDLE 2073,16*
CUNNINGHAM 2234,70
1922,23* 1563,07 1443,35
1950 Kcal/día

20 artículos IMC 40-50 kg/m2 : 1800-2000 Kcal/día 1600 Kcal/día ↑2300 Kcal/día IMC 50-60 kg/m2 : 2300 Kcal/día 2000 Kcal/día ↑2600-3000 Kcal/día IMC ≥ 60 kg/m2 : 2400-3000 Kcal/día (menor nivel de evidencia)
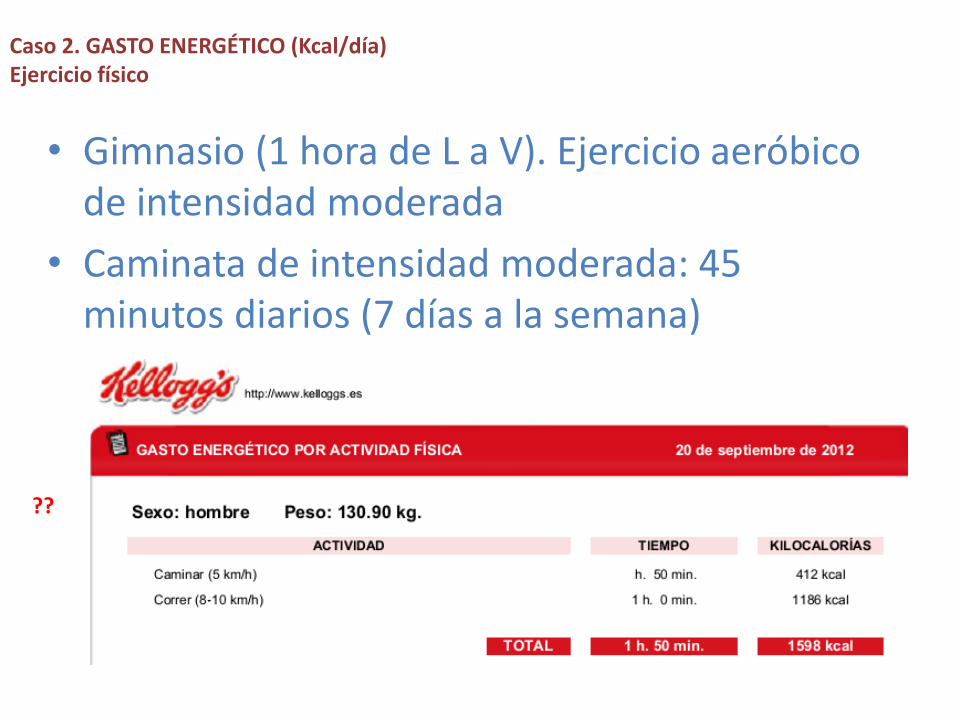
• Gimnasio (1 hora de L a V). Ejercicio aeróbico de intensidad moderada
• Caminata de intensidad moderada: 45 minutos diarios (7 días a la semana)
Caso 2. GASTO ENERGÉTICO (Kcal/día) Ejercicio físico
??
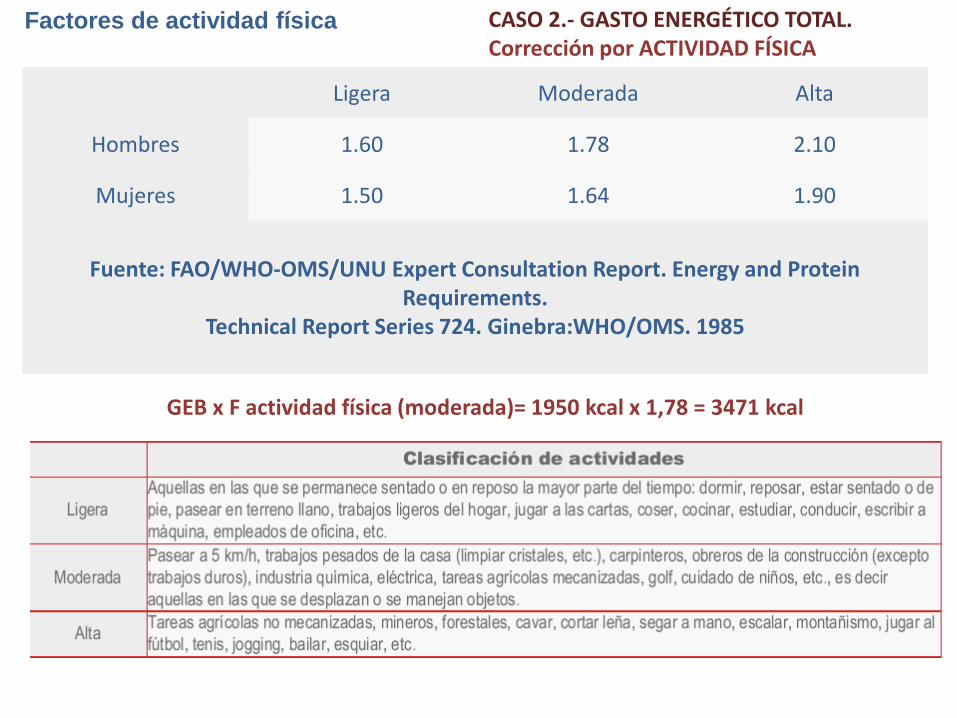
Ligera Moderada Alta
Hombres 1.60 1.78 2.10
Mujeres 1.50 1.64 1.90
Fuente: FAO/WHO-OMS/UNU Expert Consultation Report. Energy and Protein Requirements.
Technical Report Series 724. Ginebra:WHO/OMS. 1985
Factores de actividad física
GEB x F actividad física (moderada)= 1950 kcal x 1,78 = 3471 kcal
CASO 2.- GASTO ENERGÉTICO TOTAL. Corrección por ACTIVIDAD FÍSICA
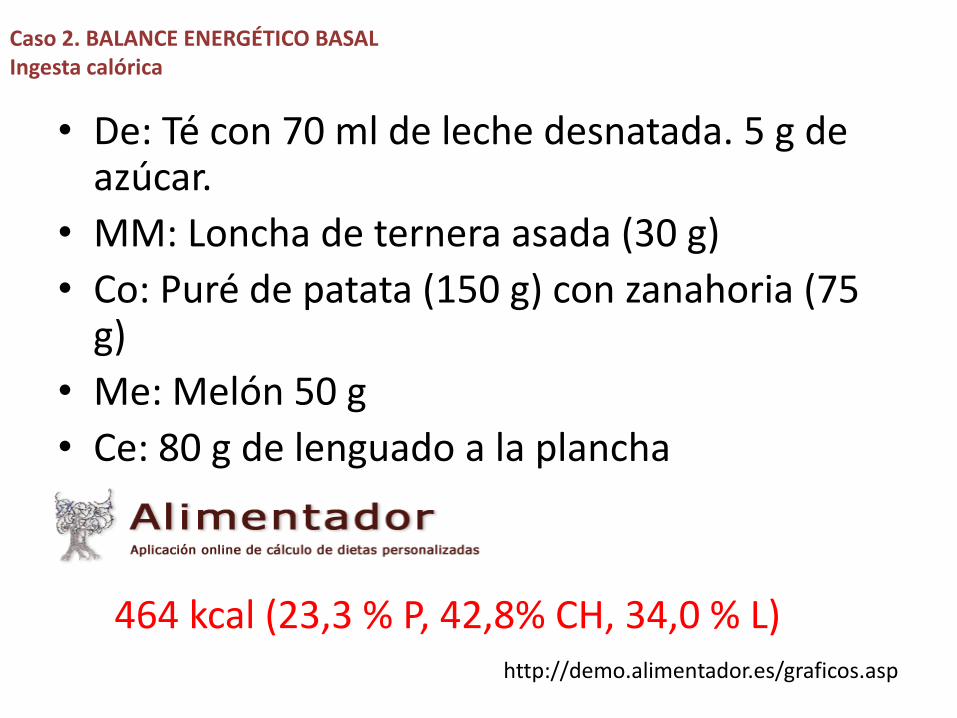
• De: Té con 70 ml de leche desnatada. 5 g de azúcar.
• MM: Loncha de ternera asada (30 g)
• Co: Puré de patata (150 g) con zanahoria (75 g)
• Me: Melón 50 g
• Ce: 80 g de lenguado a la plancha
Caso 2. BALANCE ENERGÉTICO BASAL Ingesta calórica
464 kcal (23,3 % P, 42,8% CH, 34,0 % L) http://demo.alimentador.es/graficos.asp
CÁLCULO DEL GASTO ENERGÉTICO EN
PACIENTES HOSPITALIZADOS
GEB X FACTOR DE AGRESIÓN?
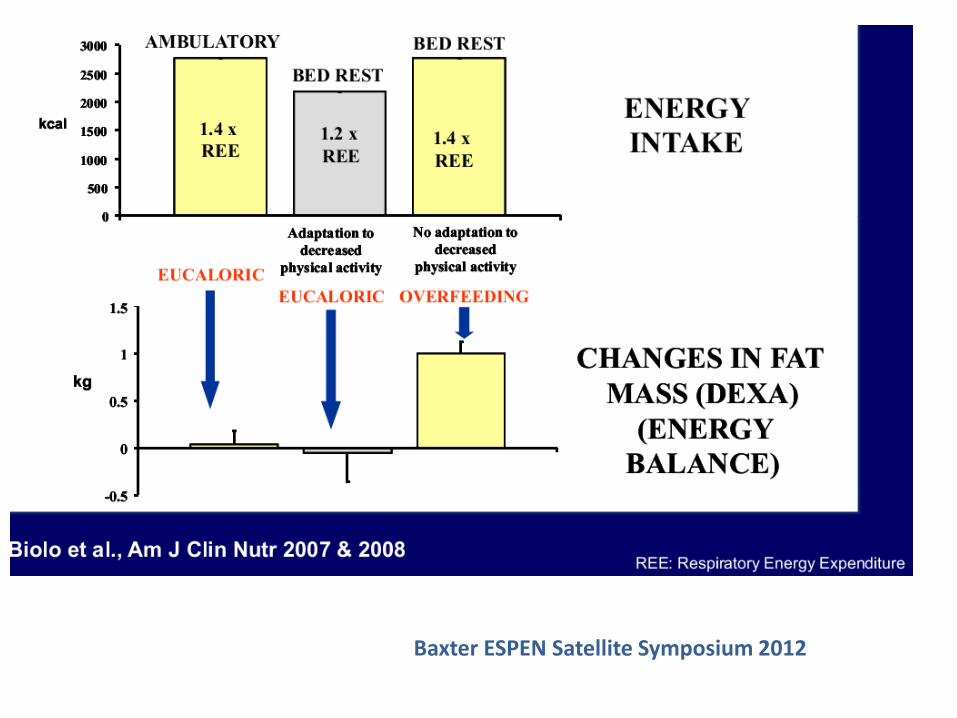
Baxter ESPEN Satellite Symposium 2012
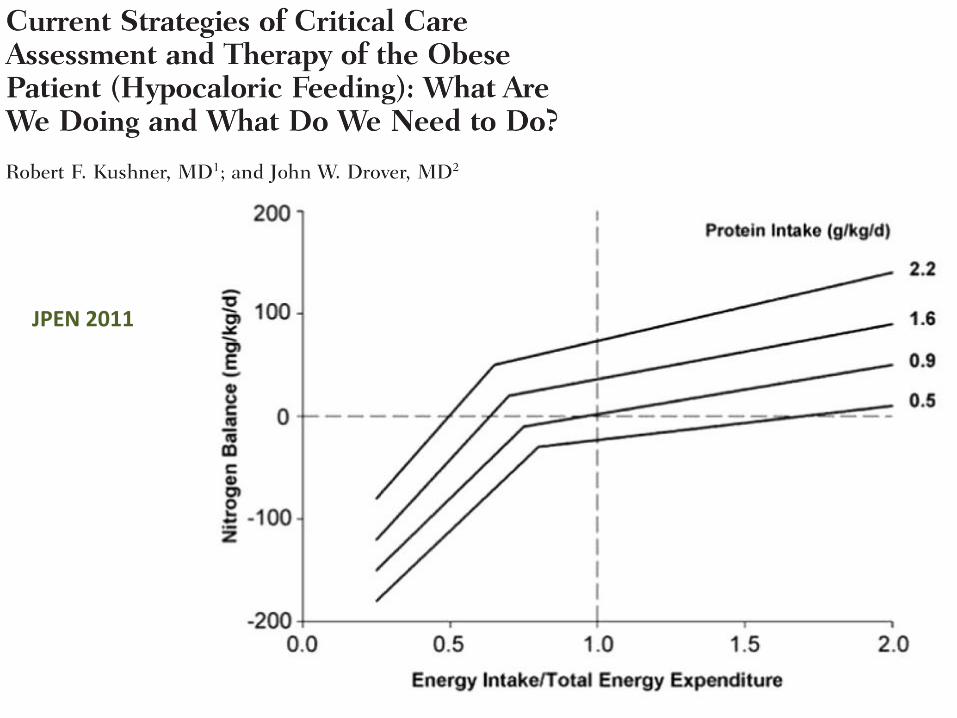
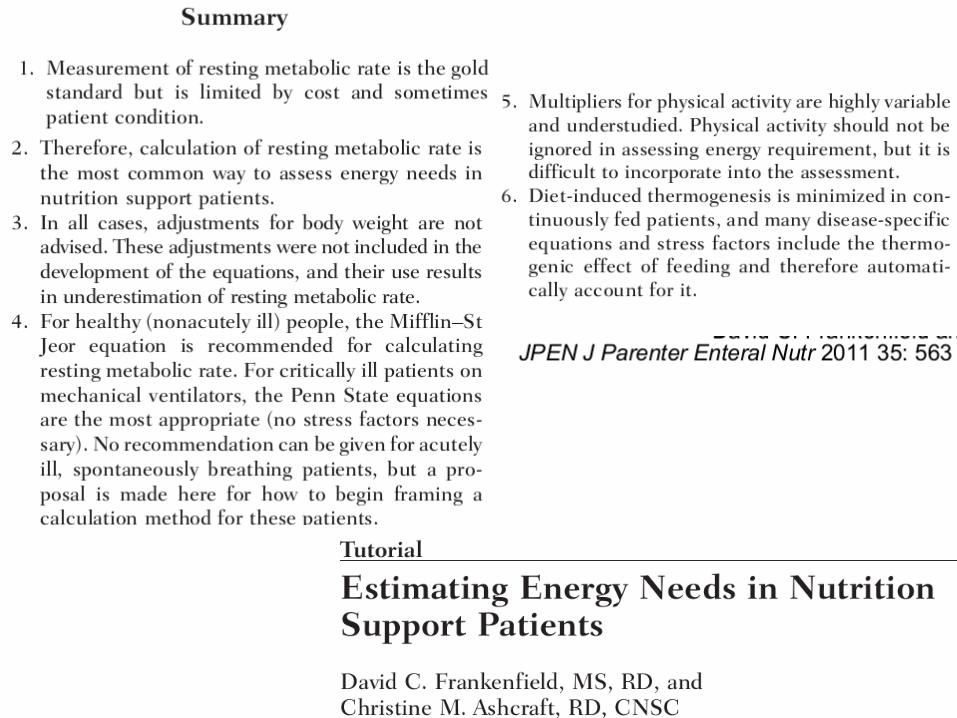
JPEN 2011
-La calorimetría indirecta continua es el
patrón oro para el cálculo de los requerimientos
energéticos del paciente obeso crítico (A).
-Las necesidades energéticas del obeso crítico
son altamente variables, lo que dificulta su
cálculo con las ecuaciones predictivas (C).
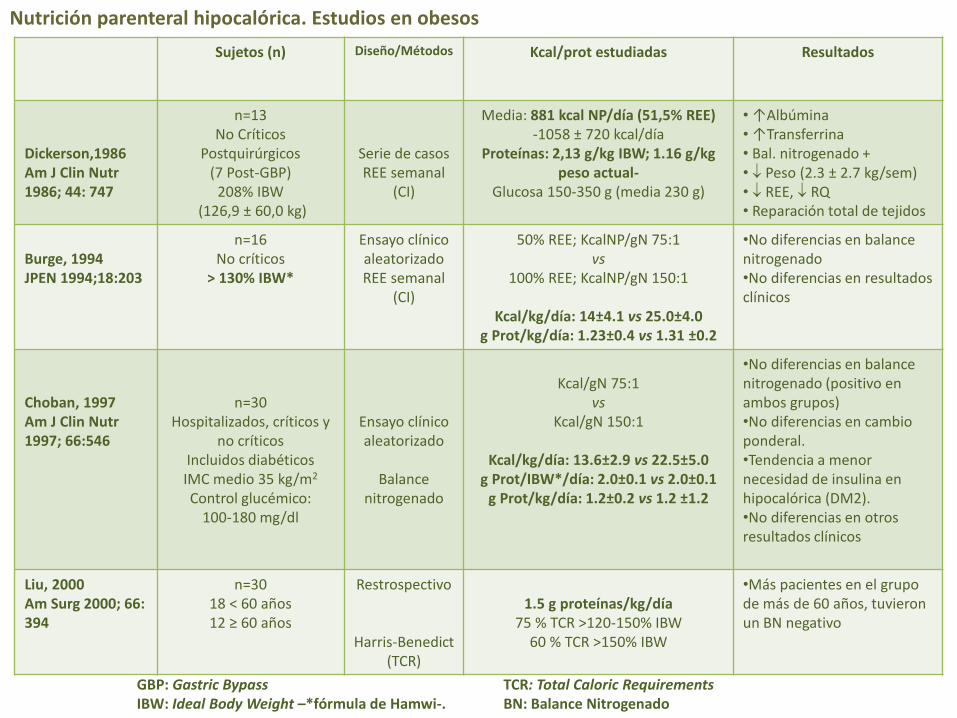
Nutrición parenteral hipocalórica. Estudios en obesos
Sujetos (n) Diseño/Métodos Kcal/prot estudiadas Resultados
Dickerson,1986 Am J Clin Nutr 1986; 44: 747
n=13 No Críticos
Postquirúrgicos (7 Post-GBP)
208% IBW (126,9 ± 60,0 kg)
Serie de casos REE semanal
(CI)
Media: 881 kcal NP/día (51,5% REE) -1058 ± 720 kcal/día
Proteínas: 2,13 g/kg IBW; 1.16 g/kg peso actual-
Glucosa 150-350 g (media 230 g)
• ↑Albúmina • ↑Transferrina • Bal. nitrogenado + • Peso (2.3 ± 2.7 kg/sem) • REE, RQ • Reparación total de tejidos
Burge, 1994 JPEN 1994;18:203
n=16 No críticos
> 130% IBW*
Ensayo clínico aleatorizado REE semanal
(CI)
50% REE; KcalNP/gN 75:1 vs
100% REE; KcalNP/gN 150:1
Kcal/kg/día: 14±4.1 vs 25.0±4.0 g Prot/kg/día: 1.23±0.4 vs 1.31 ±0.2
•No diferencias en balance nitrogenado •No diferencias en resultados clínicos
Choban, 1997 Am J Clin Nutr 1997; 66:546
n=30 Hospitalizados, críticos y
no críticos Incluidos diabéticos IMC medio 35 kg/m2 Control glucémico:
100-180 mg/dl
Ensayo clínico aleatorizado
Balance
nitrogenado
Kcal/gN 75:1
vs Kcal/gN 150:1
Kcal/kg/día: 13.6±2.9 vs 22.5±5.0
g Prot/IBW*/día: 2.0±0.1 vs 2.0±0.1 g Prot/kg/día: 1.2±0.2 vs 1.2 ±1.2
•No diferencias en balance nitrogenado (positivo en ambos grupos) •No diferencias en cambio ponderal. •Tendencia a menor necesidad de insulina en hipocalórica (DM2). •No diferencias en otros resultados clínicos
Liu, 2000 Am Surg 2000; 66: 394
n=30 18 < 60 años 12 ≥ 60 años
Restrospectivo
Harris-Benedict (TCR)
1.5 g proteínas/kg/día
75 % TCR >120-150% IBW 60 % TCR >150% IBW
•Más pacientes en el grupo de más de 60 años, tuvieron un BN negativo
GBP: Gastric Bypass IBW: Ideal Body Weight –*fórmula de Hamwi-.
TCR: Total Caloric Requirements BN: Balance Nitrogenado
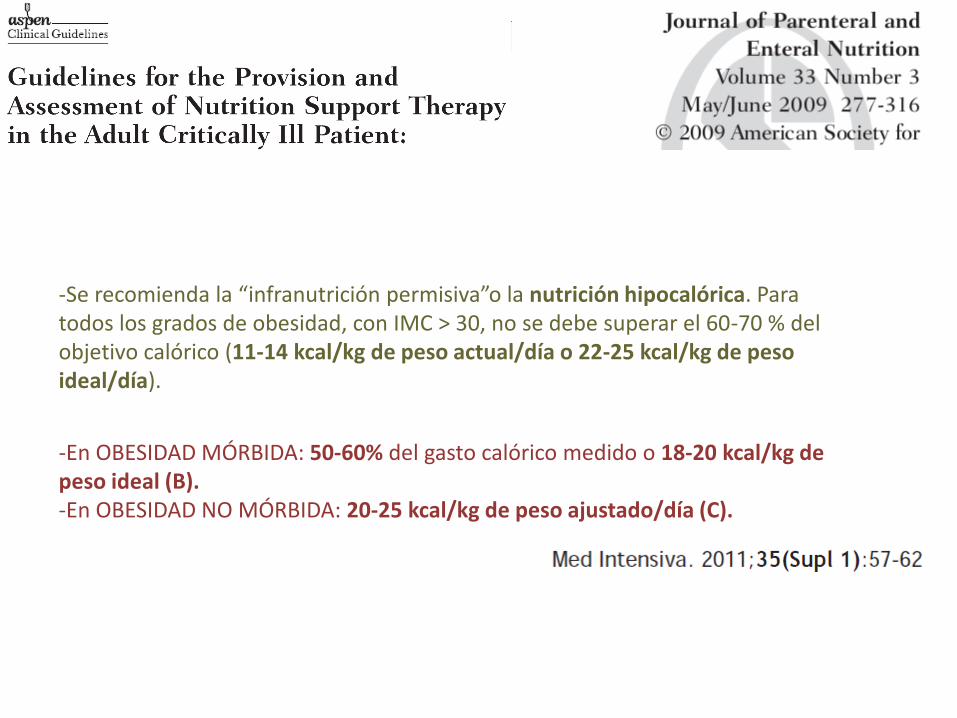
-Se recomienda la “infranutrición permisiva”o la nutrición hipocalórica. Para todos los grados de obesidad, con IMC > 30, no se debe superar el 60-70 % del objetivo calórico (11-14 kcal/kg de peso actual/día o 22-25 kcal/kg de peso ideal/día).
-En OBESIDAD MÓRBIDA: 50-60% del gasto calórico medido o 18-20 kcal/kg de peso ideal (B). -En OBESIDAD NO MÓRBIDA: 20-25 kcal/kg de peso ajustado/día (C).
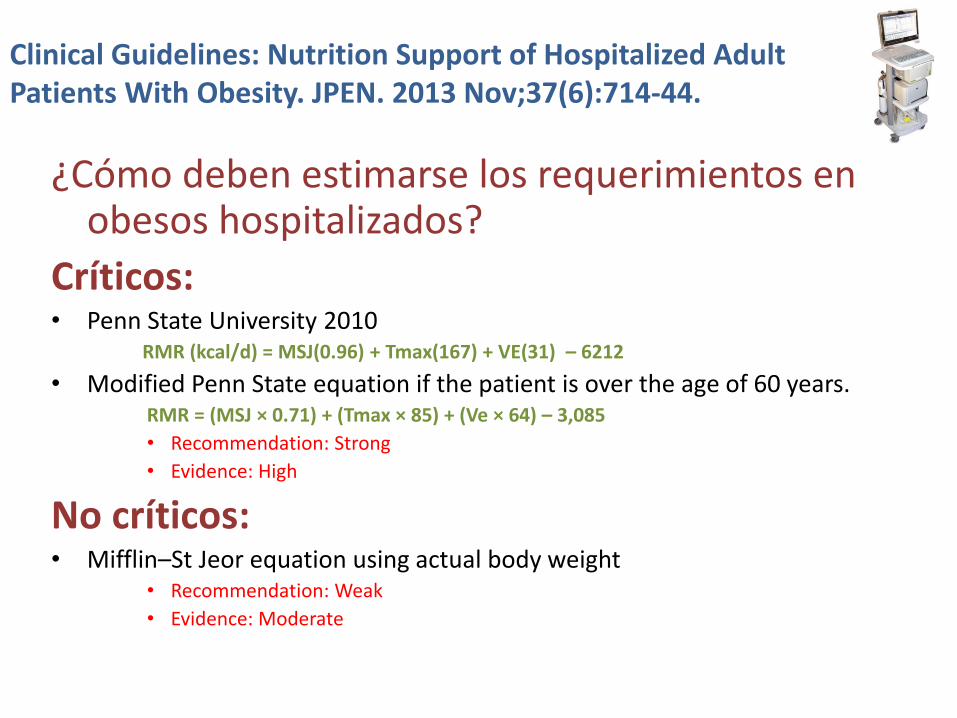
Clinical Guidelines: Nutrition Support of Hospitalized Adult Patients With Obesity. JPEN. 2013 Nov;37(6):714-44.
¿Cómo deben estimarse los requerimientos en obesos hospitalizados?
Críticos: • Penn State University 2010
RMR (kcal/d) = MSJ(0.96) + Tmax(167) + VE(31) – 6212
• Modified Penn State equation if the patient is over the age of 60 years. RMR = (MSJ × 0.71) + (Tmax × 85) + (Ve × 64) – 3,085
• Recommendation: Strong
• Evidence: High
No críticos: • Mifflin–St Jeor equation using actual body weight
• Recommendation: Weak
• Evidence: Moderate
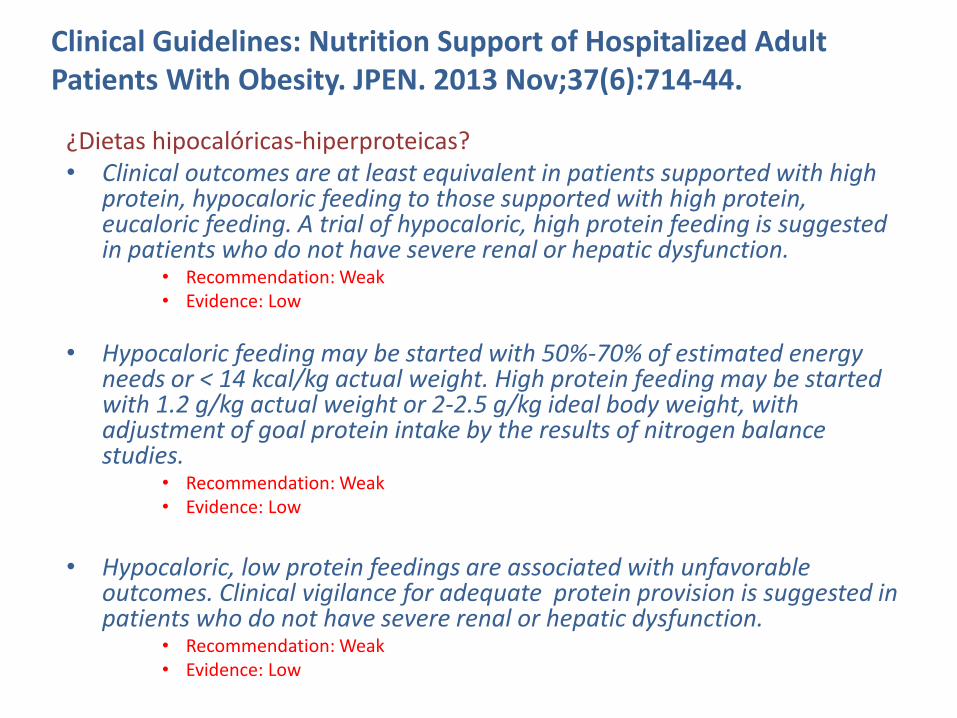
¿Dietas hipocalóricas-hiperproteicas? • Clinical outcomes are at least equivalent in patients supported with high
protein, hypocaloric feeding to those supported with high protein, eucaloric feeding. A trial of hypocaloric, high protein feeding is suggested in patients who do not have severe renal or hepatic dysfunction.
• Recommendation: Weak • Evidence: Low
• Hypocaloric feeding may be started with 50%-70% of estimated energy needs or < 14 kcal/kg actual weight. High protein feeding may be started with 1.2 g/kg actual weight or 2-2.5 g/kg ideal body weight, with adjustment of goal protein intake by the results of nitrogen balance studies.
• Recommendation: Weak • Evidence: Low
• Hypocaloric, low protein feedings are associated with unfavorable
outcomes. Clinical vigilance for adequate protein provision is suggested in patients who do not have severe renal or hepatic dysfunction.
• Recommendation: Weak • Evidence: Low
Clinical Guidelines: Nutrition Support of Hospitalized Adult Patients With Obesity. JPEN. 2013 Nov;37(6):714-44.
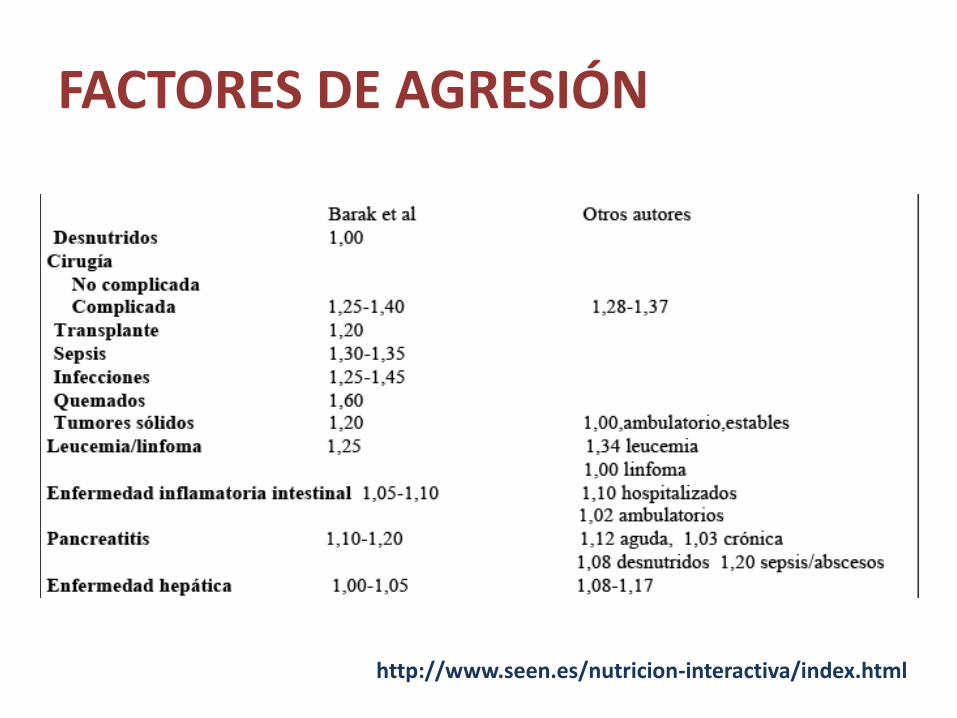
FACTORES DE AGRESIÓN
http://www.seen.es/nutricion-interactiva/index.html

CRÍTICOS

Referencias bibliográficas (I) • Anderegg BA, Worrall C, Barbour E, Simpson KN, Delegge M. Comparison of
resting energy expenditure prediction methods with measured resting energy expenditure in obese, hospitalized adults. JPEN J Parenter Enteral Nutr. 2009 ;33:168-75.
• Stucky CC, Moncure M, Hise M, Gossage CM, Northrop D. How accurate are resting energy expenditure prediction equations in obese trauma and burn patients? JPEN J Parenter Enteral Nutr. 2008; 32:420-6.
• Dobratz JR, Sibley SD, Beckman TR, Valentine BJ, Kellogg TA, Ikramuddin S, Earthman CP. Predicting energy expenditure in extremely obese women. JPEN J Parenter Enteral Nutr. 2007; 31:217-27.
• Frankenfield D. Validation of an equation for resting metabolic rate in older obese, critically ill patients. JPEN J Parenter Enteral Nutr. 2011;35:264-9.
• Spears KE, Kim H, Behall KM, Conway JM. Hand-held indirect calorimeter offers advantages compared with prediction equations, in a group of overweight women, to determine resting energy expenditures and estimated total energy expenditures during research screening. J Am Diet Assoc. 2009;109:836-45.
• Ireton-Jones C. Adjusted body weight, con: why adjust body weight in energy-expenditure calculations? Nutr Clin Pract. 2005;20:474-9.
• Krenitsky J. Adjusted body weight, pro: evidence to support the use of adjusted body weight in calculating calorie requirements. Nutr Clin Pract. 2005;20:468-73.
• Donahoo WT, Levine JA, Melanson EL. Variability in energy expenditure and its components. Curr Opin Clin Nutr Metab Care. 2004;7:599-605.
• O'Riordan CF, Metcalf BS, Perkins JM, Wilkin TJ. Reliability of energy expenditure prediction equations in the weight management clinic. . J Hum Nutr Diet. 2010;23:169-75.
• Renee N Walker and Roschelle A Heuberger. Predictive Equations for Energy Needs for the Critically Ill. Respir Care. 2009; 54: 509-521.
• Choban P, Dickerson R, Malone A, Worthington P, Compher C; and the American Society for Parenteral and Enteral Nutrition. A.S.P.E.N. Clinical Guidelines: Nutrition Support of Hospitalized Adult Patients With Obesity. JPEN J Parenter Enteral Nutr. 2013 Aug 23. [Epub ahead of print] PubMed PMID: 23976769.
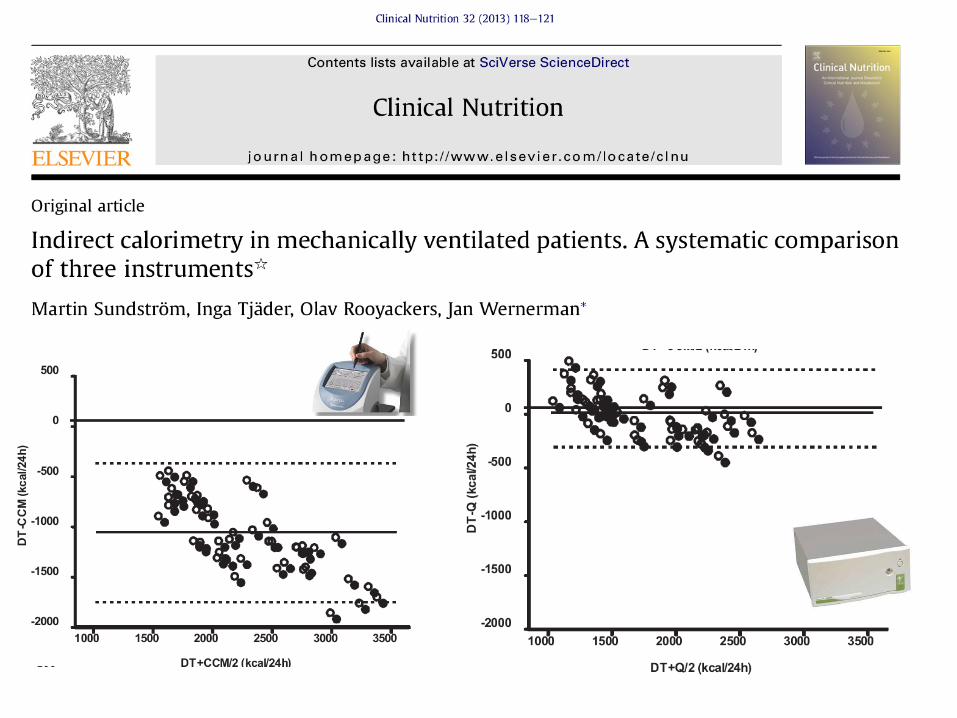
• Sundström M, Tjäder I, Rooyackers O, Wernerman J. Indirect calorimetry in mechanically ventilated patients. A systematic comparison of three instruments. Clin Nutr. 2013 Feb;32(1):118-21.
Referencias bibliográficas (II)
