novas tecnologias para ablação de fibrilação atrial ... d'or/sabad'or/05... ·...
TRANSCRIPT
Novas Tecnologias para Ablação de Fibrilação Atrial:
São elas quentes ou frias?
Nilson Araujo
Pontos Chave• Conceitos fisiopatológicos relevantes para
entender o papel da ablação da FA
• Ablação por RF hoje
• Crioablação
• Novas fronteiras

Por que nós precisamos da Ablação no tratamento de nosso paciente com FA?
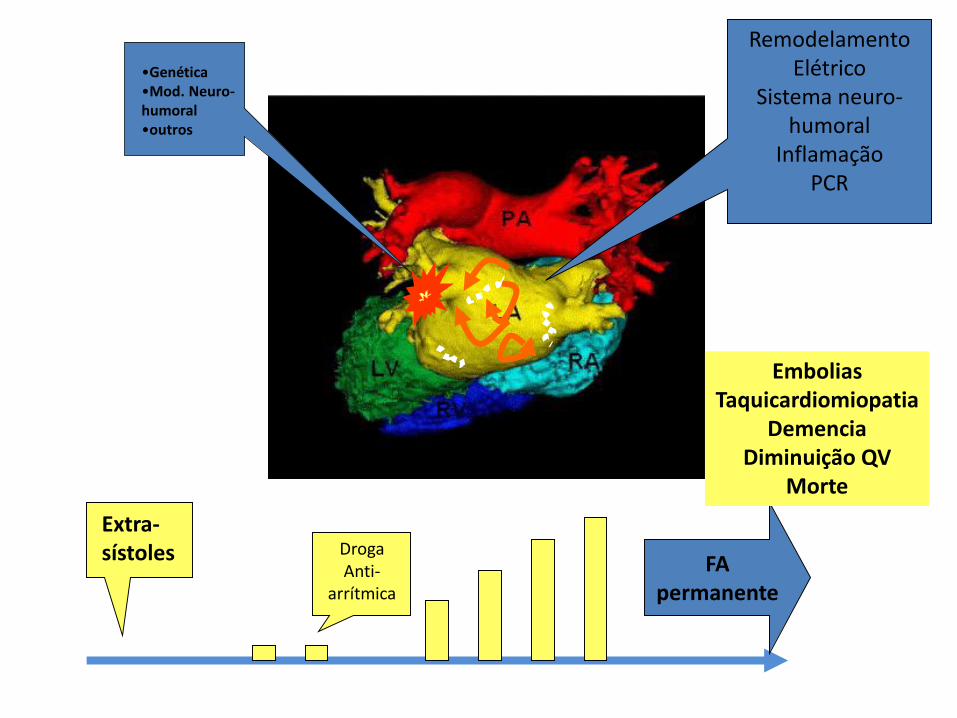
•Genética•Mod. Neuro-humoral•outros
Extra-sístoles
RemodelamentoElétrico
Sistema neuro-humoral
InflamaçãoPCR
DrogaAnti-
arrítmica
FApermanente
EmboliasTaquicardiomiopatia
DemenciaDiminuição QV
Morte

A FA é uma doença:
• Multifatorial
• Evolutiva
• Sintomática
• Causadora de lesões em órgãos alvo
• Impacta na sobrevida

• O modelo de doença da FA é desfavorável para a existência de um tratamento CURATIVO.
• No entanto, há espaço para tratamentos que visem o CONTROLE DE SINTOMAS e de COMPLICAÇÕES. Podendo haver impacto em aumento de QUANTIDADE E QUALIDADE de Vida

Sucesso de Ablação por RF da FA

Um caso de insucesso:
• Feminina, 55 anos com história de surtos paroxísticos de palpitação com sensação de escurecimento visual frequentes. Em abril de 2009 foi submetida a ablação com radiofrequência apresentando recorrência no terceiro mês pós-procedimento, segundo registrado no monitor de eventos.
• Foi inicialmente controlada com drogas mas os sintomas foram se intensificando, sendo submetida a nova ARF em 08/15




•Genética•Mod. Neuro-humoral•outros
Extra-sístoles Droga
Anti-arrítmica
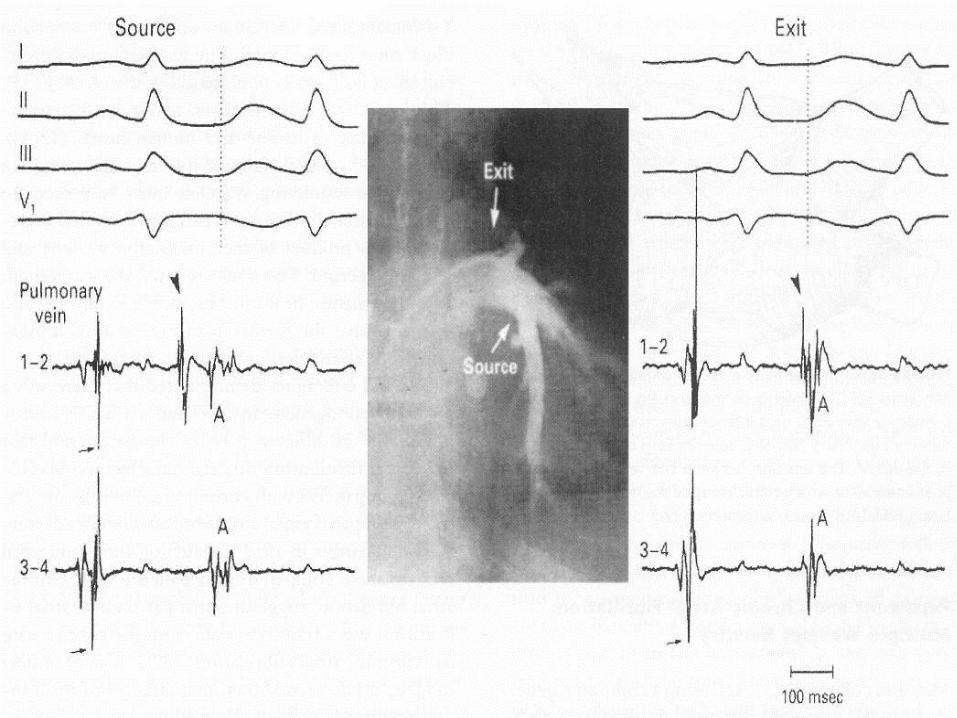
Ablação por RF da FA

Haïssaguerre, M. et al. N Engl J Med 1998;339:659-666
Tehran Arrhythmia Clinic


Resultados: 60-65% sucesso40% re-intervenção
Arch Mal Coeur Vaiss. 2001 Oct;94(10):1087-92.

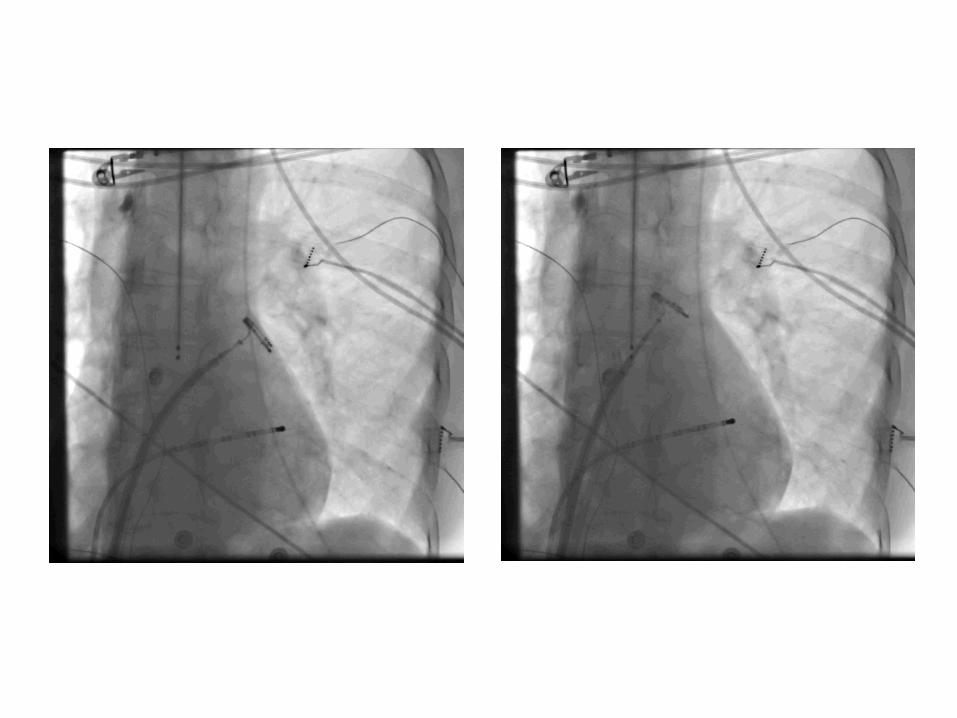
What you see in a 2D projection...May not be true in a 3D view
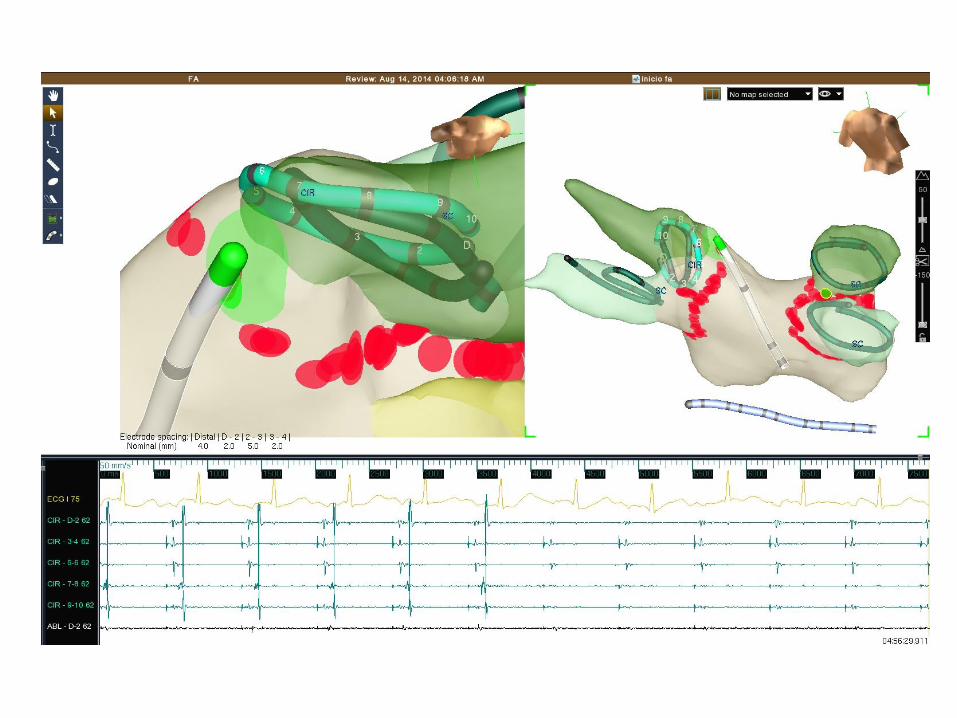

EAM mappingsystem ON but
blind to theoperator
This guy havedone
more than 300 AF ablations





Contact force

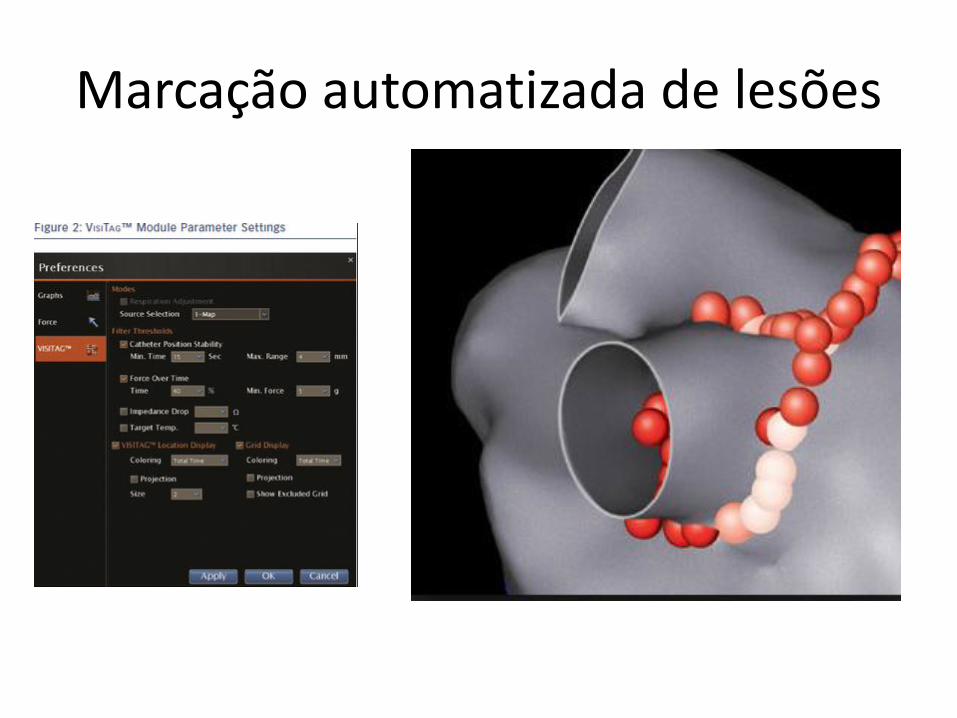
Marcação automatizada de lesões
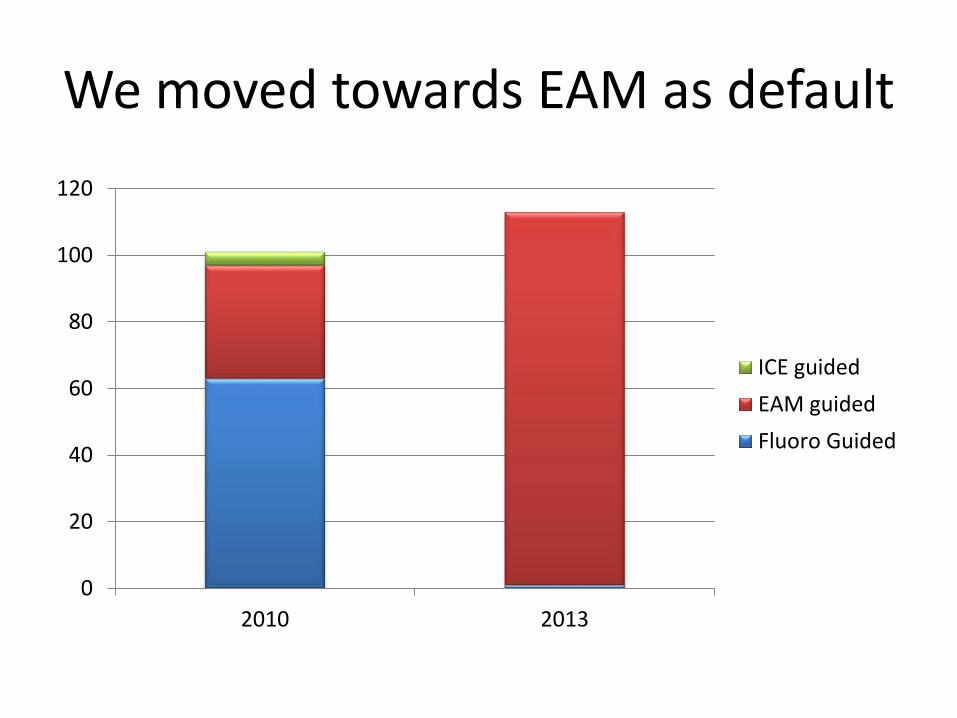
We moved towards EAM as default
0
20
40
60
80
100
120
2010 2013
ICE guided
EAM guided
Fluoro Guided

Sucesso X Complicações de Ablação de FA Rede D´Or 2012 (123 pt)
Sem complicações 109AVC 0Fistula AE 0Estenose VVPP 0Tamponamento 0TA por Abl 7Choque cardiogênico 1Edema pulmonar 0Bradiarritmia 1vasculares 2Miscelanea 3
70% paroxísticos sem droga90% com droga AA55% persistentes com droga AA

Hoje nós temos um procedimento padronizado:
• Exequível em 2 h totais
• Uso aceitável de RX (10-15 min)
• Dentro dos melhores padrões de qualidade internacionais
• Seguro
• Eficaz

Novas tendências em Ablação de FA
https://www.google.com.br/trends/
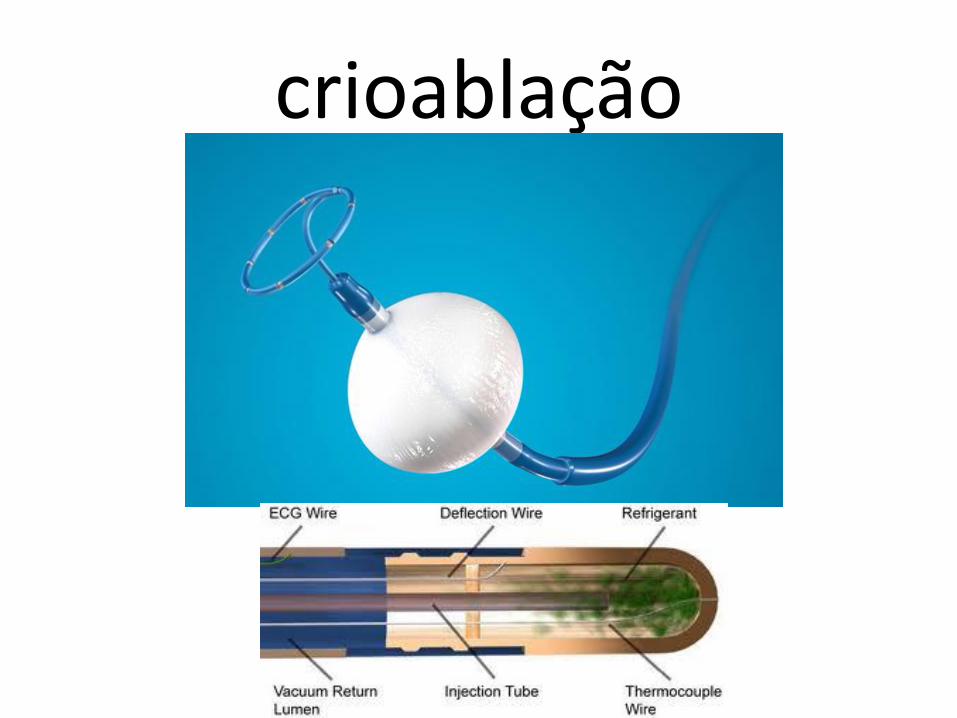
crioablação

4. O Console de Crioentrega N2O aocateter e retorna o vapor de maneirasegura. Váriossistemas de segurançamitigam perigospotenciais.
2. Dentro do balão, o N2O líquidovaporiza e absorve o calor do tecido vizinho. 3. O vapor retorna ao console através do
lúmen mantido sob vácuo.
Teoria da Operação:Como o Balão de Crio Ablaciona?
1. N2O líquido é entregue a partir do Console de Crio através de um tubode injeção no interior do balão.
35


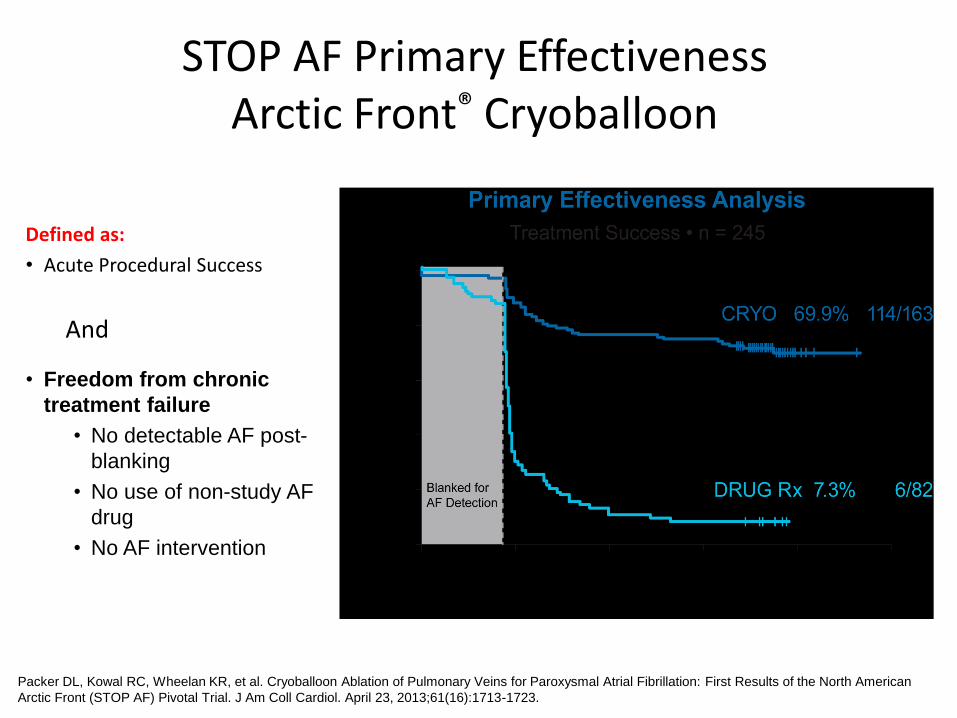
Defined as:
• Acute Procedural Success
• Freedom from chronic
treatment failure
• No detectable AF post-
blanking
• No use of non-study AF
drug
• No AF intervention
And
STOP AF Primary EffectivenessArctic Front® Cryoballoon
Packer DL, Kowal RC, Wheelan KR, et al. Cryoballoon Ablation of Pulmonary Veins for Paroxysmal Atrial Fibrillation: First Results of the North American
Arctic Front (STOP AF) Pivotal Trial. J Am Coll Cardiol. April 23, 2013;61(16):1713-1723. 38

Cryo vs. RF Trial HRS 2014 Late Breaking Trial 5/9/14 - St. Bartholomew Hospital (London
UK)
• 237 patients with paroxysmal AF were randomized 1:1:1 to RF WACA ablation1, Cryo2 or a combined approach3
• Procedure time was 211 (IQR 174-256) mins for RF compared to 167 (136 - 202) mins for Cryo (p<0.001)
1. RF WACA: Wide encirclement of the PVs using an irrigated radiofrequency ablation catheter guided by a 3D mapping system.
2. Cryo: Pulmonary vein isolation using the Arctic Front Cryoballoon. 3. Combined: RF WACA wide encirclement of the PVs to achieve PV isolation, followed by 2 empirical
applications of the cryoballoon to each PV ostia.
Hunter, et al. HRS 2014, San Francisco. Lecture ID 9526.
Cryo vs. RF P<0.015
RF vs. Combined p<0.001
Cryo vs. Combined P=0.166
47%
67%76%
0%
20%
40%
60%
80%
RF (n=77) Cryo (n=78) Combined (n=79)
1-Year Single Procedure Freedom From AF, off AADs
39

Pulmonary Vein Isolation with Arctic Front and Arctic Front Advance – 28 mm
Pre and Post Procedure Voltage Maps
Chierchia, et al. Kenigsberg, et al.
Patients 4 43
Balloon and Application Time CB1 28 mm, 5 min CB2 28 mm, 3 min
Extent of posterior wall ablation 40% 73%
6 month Freedom from AF 75% 95%
Chierchia, et al. Cardiovasc Med (Hagerstown). 2011; 12(3): 162-166. Kenigsberg, et al. Heart Rhythm 2014; In press 40

Durability of Pulmonary Vein Isolation with Cryoballoon Ablation: Results from the SUstained PV Isolation with ARctic Front Advance (SUPIR) Study
41
• 3 months after the Arctic Front Advance index procedure, a second PV remapping procedure was performed to assess PVI durability in 21 patient
• 91% of veins remained electrically isolated
• All PVs remained durably isolated in 78% of patients
• Clinical AF recurrence was detected in 2 patients (11%) at follow up
Analysis of Gaps in Patients with PV Reconduction
Subject ID# of PVs with
GapsLocation of Gap(s)
Clinical AF Recurrence
7 3LSPV Ridge area, LIPV anterior LAA area, RSPV posterior-superior area
yes
13 1 RIPV inferior aspect no
14 2RSPV anterio-middle aspect, RIPV inferior aspect
yes
22 1 RIPV inferior aspect no
Petru, et al. International Symposium on Progress in Clinical Pacing 2014

PV Lesion Durability with RF and CryoStudies evaluating PV re-conduction using repeat electrophysiology and
mapping after the index procedure
30%
23%
8%
35%
67%
78%
0%
20%
40%
60%
80%
100%
GAP-AF Willems Jiang EFFICAS I Ahmed SUPIR
% of Patients with PVI* During Remapping Procedure
Follow-up** 3 Months 3 Months 12 months 3 months 3 months 3 months
(n=117) (n=40) (n=75)(n=75) (n=21)
1Late Breaking Clinical Trials session I at the EHRA EUROPACE 2013 meeting in Athens, Greece 2 Williems, et al. J Cardiovasc Electrophysiol 2010; 21(10):1079-84. 3 Jiang, et al. Heart Rhythm. 2014;11(6):969-76 4 Neuzil et al. Circ Arrhythm Electrophysiol.(2):327-33 5 Ahmed, et al. J Cardiovasc Electrophysiol, 2010;21(7):731-7, 6 Petru, et al. International Symposium on Progress in Clinical Pacing 2014
RF: Contact SensingRF Arctic Front
1 2 3 4
(n=12)
Arctic Front Advance
5 6
**All 4 veins were isolated in invasive remapping procedure *Time between index procedure and re-mapping procedure. All patients were evaluated regardless of clinical symptoms
Phased array ablation

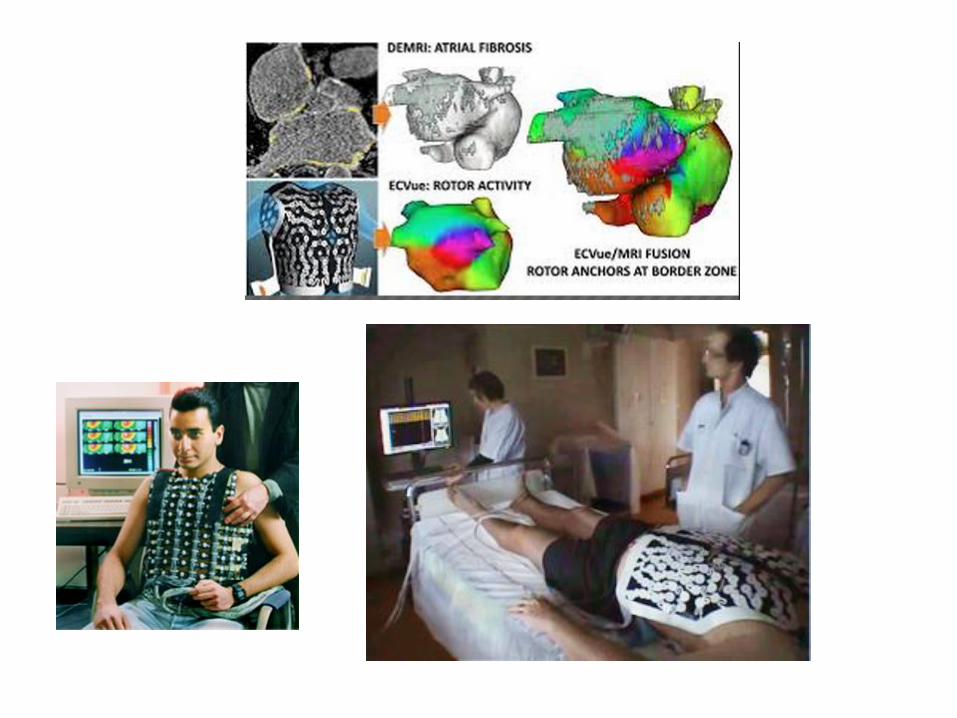
Ablação de rotores


Frigidarium, Pedro Weingartner1897.
Caldarium, Pedro Weingartner
1900.