mestrado integrado em medicina the impact of covid-19 …
TRANSCRIPT

MESTRADO INTEGRADO EM MEDICINA
The Impact of COVID-19 on Cancer Therapy
André Jorge Moniz Garcia
M 2021

The Impact of COVID-19 on Cancer Therapy
Dissertação de candidatura ao grau de Mestre em Medicina, submetida ao Instituto de Ciências Biomédicas Abel Salazar – Universidade do Porto
André Jorge Moniz Garcia Aluno do 6º ano profissionalizante de Mestrado Integrado em Medicina
Afiliação: Instituto de Ciências Biomédicas Abel Salazar – Universidade do Porto
Endereço: Rua de Jorge Viterbo Ferreira nº228, 4050-313 Porto
Endereço eletrónico: [email protected]
Orientador: Professor Doutor António Araújo
Professor Catedrático Convidado, Director do Serviço de Oncologia Médica,
Centro Hospitalar Universitário do Porto
Afiliação: Instituto de Ciências Biomédicas Abel Salazar – Universidade do Porto
Endereço: Largo Professor Abel Salazar, 4099-001 Porto

Porto, 02 de Junho de 2021

Dedication
I dedicate this dissertation, to my beloved parents, for endowing in me their hopes, and the means to accomplish my goals.

i
Acknowledgments I would like to thank Professor António Araujo, for the opportunity and counsel, that was of utmost importance to accomplishing this task. Then, I would like to thank my dear brothers, Diogo Paulo Moniz Garcia, and Tiago Moniz Garcia, for their priceless insight and guidance, for without them I would have been lost. And finally, to my always present and patient friends, Hugo Marinho, Jorge Teixeira, Maria Cunha, Pedro Almeida and Simão Bessa, for preserving my tenacity to persevere, through this hardship and this especially hard year.
ii
Abstract Background: The COVID-19 (Coronavirus Disease 2019) pandemic began in December of 2019 in Wuhan, China, and was considered a pandemic by the World Health Organization (WHO) on March 11 of 2020. Since then, after more than a year, it has claimed many lives and has destabilized health care systems worldwide, leaving special groups of patients even more vulnerable, being cancer patients one of these groups. Purpose: This review seeks to assess how cancer therapy was affected by the COVID-19 pandemic. Mainly in ascertaining if cancer patients, particularly those under anticancer treatment, are especially vulnerable to SARS-COV-2 (Severe Acute Respiratory Syndrome Coronavirus 2) infection, ascertain the therapy recommendations made to respond to the pandemic, and how cancer care centers or departments implemented them. This study focused mainly on adult patients, solid cancer, and high-income countries. Methods: This study reviews published literature that was selected following research using PubMed, based on all possible combinations of the keywords described below. The selection process also included inclusion and exclusion criteria established per the purpose of this study. The references of the initially added articles were analyzed to add further articles. Results: 408 articles were initially analyzed. Of these 55, were included, and a further 4 were added, ending with 59 articles included. Some articles analyzed populations in specific regions, others nationwide or worldwide. Among these articles, 20 were prospective or retrospective articles that described how a population of cancer patients was affected by the SARS-COV-2 infection, 17 articles disclosed initial therapy recommendations, and in 24 cancer care activity changes were reported, mainly through the analysis of a survey. Conclusions: Cancer patients are likely to be more vulnerable to a SARS-CoV-2 infection than non-cancer patients, in terms of transmission, as the prevalence of cancer in COVID-19 patients was 1-8.5% vs. 5-year prevalence of cancer worldwide in 2020 of 0.65%, and in prognosis, 40-90% of cancer patients with COVID-19 are hospitalized vs. 20% in general COVID-19 patients, with a case fatality rate in hospitalized COVID-19 cancer patients of 17%-55% vs. 15-20% in general hospitalized patients with COVID-19. Initial recommendations sought to balance the risk of infection with that of undertreatment. Priority was given to urgent and curative treatments, with elective and non-urgent procedures, such as routine and follow-up visits, being delayed. At the same time, there were efforts to maintain a safe in-hospital or clinic environment, with patient triaging before visits and procedures and adherence to infection prevention measures. Cancer care activity was generally decreased with fewer outpatient visits and an increase in treatment delays, while the use of telemedicine, remote technology for medical practice, was mostly broadened. The long-term effects of treatment delays are still unknown. However, it will likely have lasting repercussions on cancer patient’s prognosis with the possibility of a higher prevalence of more advanced and unresectable tumors in the future. Keywords: COVID-19; Medical Oncology; Neoplasm; Disease Management; Therapy; Patient Care Management; Delivery of Health Care; Global Burden of Disease; Telehealth;

iii
Resumo Cenário: A pandemia do COVID-19 (Doença por Coronavirus 2019), começou em Dezembro de 2019, na cidade Wuhan, Chinam e foi considerada pela Organização Mundial de Saúde (OMS), como uma pandemia a 11 de Março de 2020. Desde então, após mais de um ano, várias doentes faleceram desta doença e muitos sistemas de saúde foram destabilizados por todo o mundo, deixado certos grupos específicos de doentes ainda mais vulneráveis, nomeadamente doentes oncológicos. Objetivo: Esta revisão, tem como objetivo avaliar como a terapia oncológica foi afetada, pela pandemia do COVID-19. Especialmente, ao verificar se os doentes oncológicos, nomeadamente os tratados com terapia anticancerígena, são mais vulneráveis à infeção do SARS-CoV-2 (Coronavirus da Sindrome Respiratória Grave 2), que recomendações terapêuticas foram criadas como resposta à pandemia e como foram implementadas em centros oncológicos. Foco foi primariamente a doentes adultos, com cancro sólido e de países com rendimento elevado. Resultados: Inicialmente foram analisados 408 artigos, destes 55 foram selecionados, aos quais 4 foram adicionados. posteriormente, com base em referências de artigos selecionados, para um total de 59. Alguns artigos estudavam populações de uma região específicos, outros analisavam a população geral de certos países ou mundial. Dentro destes artigos, 20 eram estudos prospetivos ou retrospetivos que descreviam como a população oncológica foi afetada pela infeção do SARS-CoV-2, 17 informavam sobre quais foram as recomendações iniciais, e 24 analisaram, a partir de inquéritos, alterações registadas no impacto oncológico. Conclusões: Doentes oncológicos, são presumivelmente mais vulneráveis a infeção de SARS-CoV-2 que doentes não oncológicos, quer em termos de transmissão, dado que nos estudos a prevalência de cancro nos doentes com COVID-19 foi entre 1-8.5% e a prevalência mundial de cancro em 5 anos foi de 0.65%, em 2020, quer de prognóstico com hospitalizações nos estudos selecionados de 40-90% em doentes oncológicos com COVID-19 comparado com 20% na população geral com COVID-19, nos doentes hospitalizados com cancro e COVID-19, e verificou-se uma taxa de letalidade de 17%-55%, comparado com a da população geral hospitalizada com COVID-19, de 15-20%. Recomendações iniciais, tentaram equilibrar o potencial risco de infeção com o de sub-tratamento, tratamentos curativos e urgentes foram priorizados e os tratamentos eletivos adiados, tal como procedimentos não urgentes, como visitas de rotina e seguimento, e ao mesmo tempo, zelando pela segurança do tratamento prestado. A atividade dos cuidados oncológicos foi globalmente diminuída, com menos visitas de ambulatório e aumento de adiamento de tratamentos, com um aumento paralelo de telemedicina, uso de tecnologias remotas para cuidados médicos. Os efeitos a longo termo dos adiamentos nos tratamentos, ainda não é compreendido, contudo é provável que terão repercussões nefastas no prognóstico destes doentes, como aumento de prevalência de cancros mais avançados e irressecáveis, nos próximos anos. Palavras-chave: COVID-19; Medical Oncology; Neoplasm; Disease Management; Therapy; Patient Care Management; Delivery of Health Care; Global Burden of Disease; Telehealth;

iv
Abreviations
§ Adj.- adjuvant § AKT- protein kinase B § Anti-CT- anti-cancer therapy § ARDS- acute respiratory distress syndrome§ ASTRO- American Society for Radiation
Oncology § AUS- Australia § CAR-T- chimeric antigen receptor T cell § ChT- chemotherapy § CI- confidence interval § CKD- chronic kidney disease § CP- cancer patient § CO- compositeoutcome § CoV- coronavirus § COVID-19- Coronavirus Disease 2019 § CT- computer tomography § dNLR- derived neutrophil-to-
lymphocyte ratio § DOAC- direct oral anti-coagulant § Dx - diagnosis § ECOG PS- Eastern Cooperative
Oncology Group performance status score
§ ESMO- European Society for Medical Oncology
§ ESTRO- European Society for Radiotherapy and Oncology
§ FN- febrile neutropenia § G-CSF- granulocyte colony-stimulating
factors § GI- gastro-intestinal § H- high § HC- hematologic cancer § HCP- hematologic cancer patient § HCW- health care worker § HR- hazard ratio § HT- hormone therapy § ICI- immune checkpoint inhibitor § ICU- intensive care unit § IL-6- interleukin-6 § IMV-invasive mechanical ventilation § ir-AE – immune-related adverse event § IT- immunotherapy § L- low § LC- lung cancer § LMWH- low molecular weight heparin
§ M- medium § MC- metastatic cancer § MEK- mitogen-activated extracellular
signal-regulated kinase § MERS-CoV - Middle East Respiratory
Syndrome Coronavirus § MR- magnetic resonance imaging § N/A- Not available § NCP- non-cancer patient § NPS- nasopharyngeal swab § NSCLC- Non-small-cell lung carcinoma § NT pro-BNP- N-terminal prohormone
of brain natriuretic peptide § NY- New York § NZ- New Zealand § OR- odds ratio § OS- overall survival § PD-L1- Programmed death-ligand 1 § PET- Positron emission tomography § PI3K- Phosphoinositide 3-kinases § PPE- Personal protective equipment § R0- basic reproductive rate § ROI- Radiation oncology institution § RR- relative risk § RT- Radiotherapy § RT-PCR- Reverse transcription
polymerase chain reaction § RTT – radiotherapy technician § TKI- Tyrosine kinase inhibitor § TNF – tumor necrosis factor § SACT- systemic anti-cancer therapy § SARS-CoV- Severe Acute Respiratory
Syndrome Coronavirus § SARS-CoV-2- Severe Acute Respiratory
Syndrome Coronavirus 2 § SC- solid cancer § SCP- solid cancer patient § UK- United Kingdom § USA- United States of America § WHO- World Health Organization § WBC- white blood cel

v
Index
Acknowledgments ...................................................................................................... i
Abstract .................................................................................................................... ii
Resumo .................................................................................................................... iii
Abreviations ............................................................................................................. iv
Index ......................................................................................................................... v
Introduction .............................................................................................................. 1
Methodology ............................................................................................................. 3
Results ...................................................................................................................... 4 Perceiving cancer patients’ vulnerability to Covid-19 ........................................................ 4 Initial management recommendations ............................................................................ 10 Impact on Cancer care ..................................................................................................... 13
Discussion and Conclusions ...................................................................................... 25
References ............................................................................................................... 47 Figure i – Flowchart of article selection ......................................................................... 32 Table i- Inclusion and exclusion criteria used ................................................................ 32 Table I- Perceiving cancer patients’ vulnerability to COVID-19- Characteristics of studies selected……………………………………………………………………………………………………………………..34 Table II- Perceiving cancer patients’ vulnerability to COVID-19- Characteristics and risk factors of the population, in corresponding study. ....................................................... 35 Table III- Initial management recommendations - Resource allocation ........................ 36 Table III.1- ESMO cancer patient prioritization…………………………………………………………..37 Table IV- Initial management recommendations- Outpatient setting ........................... 38 Table V- Initial management recommendations- Inpatient setting ............................... 39 Table VI- Initial management recommendations- Anticancer Treatment . ................... 40 Table VII- Initial management recommendations- Measures for staff .......................... 42 Table VIII- Initial management recommendations- Telemedicine recommendations, uses and limitations ....................................................................................................... 43 Table IX- Initial management recommendations- Other general and support recommendations .......................................................................................................... 44 Table X- Impact in Cancer care- Characteristics of studies selected .............................. 45 Table XI- Impact in Cancer care- Recommendations followed, impact in activity and infection transmission of corresponding study ............................................................. 46

1
Introduction
The COVID-19 (Coronavirus Disease 2019) pandemic, caused by the SARS-CoV-2 (Severe
Acute Respiratory Syndrome Coronavirus 2) virus, began in December of 2019 in the Chinese
city of Wuhan of the Hubei province and was considered a pandemic by the World Health
Organization (WHO) at March 11 20201,2 . As of December 20 of 2020, a year after it began, it
has already infected 75 129 306 people and caused 1 680 794 deaths worldwide (approximately
2.24% of cases), mainly in the Americas (32 437 597; 809 105) and in Europe (23 691 857;
527 719).3 It is part of the coronavirus family (CoV), which includes the SARS-CoV and MERS-CoV
viruses, which also caused outbreaks in 2002-2004 and 2012-2015, respectively1. The main mean
of spread is through respiratory droplets, especially from the cough or sneezes of symptomatic
cases. Aerosols and surface contact spread are also other means of transmission but to a lesser
degree1,4. As such, there is a high human-to-human transmission capacity, with an R0 (basic
reproductive rate) of 2.52. The incubation period (time between exposure and symptoms) of
SARS-CoV-2 is 2 to 14 days, with a mean of 3 days1. The most common symptoms at onset are
fever and cough, with dyspnea typically appearing seven days later1. The disease course tends
to be heterogeneous. Some are asymptomatic, others have mild or severe disease with the
possibility of severe pneumonia or acute respiratory distress syndrome (ARDS)1,4, and about 20%
need to be hospitalized2. Nearly 5% of patients and 20% of those hospitalized will have severe
symptoms needing admission to the ICU4, including septic shock, acute respiratory failure and
multiple organ failure1,4. COVID-19 is also associated with many complications, including venous
and arterial thromboembolism, which occurs in a significant proportion of hospitalized patients
(10-25%)4. In hospitalized COVID-19 cases, up to 15-20% of cases end up dying, and 40% of those
in the ICU4. The risk of severe disease or mortality is associated with older age 2,4 and
comorbidities2, mainly cardiovascular, diabetes and hypertension1.
In this setting, one crucial group to mention is that of oncological patients. These
account for 6-8% of hospitalized positive cases4, while the 5-year cancer prevalence worldwide
in 2020 was 50 550 287, nearly 0.65% of the world population5. Not only are they frailer and, in
general, have a suppressed immune system, but these patients are also older and have a higher
number of comorbidities than the non-oncologic population6,7. As such, they are likely to be
more vulnerable to infections like SARS-CoV-2, which are then more severe and associated with
a worse prognosis, having a higher risk of complications and death.6,7

2
This increased vulnerability of cancer patients (CPs) revolves not only around the disease
itself, but it is also due to its treatment7,8. One of the prominent diverse effects of systemic
anticancer therapy and surgery is that of immunosuppression8, especially in cytotoxic
treatments, that increases the risk of infection and can also lead to febrile neutropenia (FN)9.
This alarming complication can be mitigated with the use of hematopoietic growth factors, such
as recombinant granulocyte colony-stimulating factors (G-CSF)9. Although its use for prophylaxis
was formerly reserved for patients at high risk, after the pandemic, it is foreseeable that it will
be extended to be used in more patients9. One the most noticeable side effects in
immunotherapy is pneumonitis, which can be hard to differentiate with COVID-19 pneumonia
that typically has ground glass-opacities. Furthermore, to treat this complication,
immunosuppressants like high-dose corticosteroids might be employed, which, if used in a
COVID-19 patient, could reveal to be disastrous10. Additionally, reports of cytokine storm (a
hyperinflammatory state with increased cytokine levels that may lead to ARDS) have also been
associated with the use of ICI6,10 or CAR-T therapy6. It is expected that the use of anticancer
treatments (AntiCTs) will be delayed as a precaution measure, especially in those with more
stable cancers8.
There is another aspect that increases the risk of CPs, the need for routine visits and
treatment sessions to the hospital or cancer clinics may lead to increased risk of exposure and
infection11. As such, it might be expected that follow-up visits and non-urgent treatments might
be delayed or canceled in selected patients, along with the implementation of triaging systems
to detect signs of possible infection6. Another increasing trend is that of the implementation of
telemedicine, in other words, the substitution of in-person visits by remote ones (phone or
video)12, especially in those where the risk of exposure outweighs the need for a visit8,13. Other
uses of telemedicine include remote screenings for signs of infection, and oral treatment
supervision, reported to be increasing13. Telemedicine permits an increase of access to care12,13,
decreased treatment inequality12, and allows for a more multidisciplinary care12,13, by permitting
professionals of different fields to interact without time or space limitations12.
Furthermore, this pandemic applied stress and destabilized worldwide health care
systems11, especially in countries more affected by the pandemic, like Italy during the first wave7.
The need to allocate resources to the treatment of COVID-19 patients eventually leading to a
decreased capacity to deal with other patients as is the case with CPs, possibly leading to the
undertreatment and worse prognosis in some patients, with the possibility of some cancers
becoming unresectable8. This stress can also lead to shortages of crucial resources like personal

3
protective equipment (PPE) and staff7, which are even more crucial to maintaining treatment
safety during this period.
This study aims to evaluate the impact that the COVID-19 pandemic had on cancer
therapy, firstly by ascertaining how CPs are more vulnerable than NCPs and if anticancer therapy
affects the outcome. Then to perceive what recommendations were initially made to prepare
for the outcomes of the pandemic. Moreover, finally, how the changes were implemented and
their impact on therapy activity and infection transmission in CPs and health care workers
(HCW). The focus was on solid cancer patients and high-income countries.
Methodology
In order to realize this review, research was made using PubMed on December 20 of 2020,
using the following keywords ((Covid-19) AND (Medical Oncology) AND ((Disease Management)
OR (therapy) OR (Global Burden of Disease) OR (Telehealth) OR (Patient Care Management) OR
(Delivery of Health Care))) AND (neoplasm). With this search, 603 results were obtained. A filter
for studies with an available abstract, those written in English and those based on humans,
dropped results to 408. There were no duplicates, and there was no restriction in the year of
publication, but studies released after the date of research were not included. Afterward, case
reports, clinical trials, and editorials were removed. By analyzing the title and the abstract of
these studies, those that approached cancer cases as a whole were included, and those that
focused on specific cancers or groups of cancers such as breast, digestive, endocrine,
gynecological, head and neck, hematologic, neurologic, oral, prostate, renal cell, skin, thoracic
or lung, and urological cancers were excluded as were studies that focused on the pediatric
population. Of the remaining studies, those that analyzed the outcome of COVID-19 in cancer
patients and had a sample size of more than ten patients were included. Articles focusing on
recommendations for cancer care facing COVID-19 were also included, with those focusing
solely on one type of treatment excluded, and other reviews except for those about guidelines
and recommendations were also excluded. Studies that analyzed differences in activity in cancer
care departments, facilities, or institutions were included. Finally, studies focusing on low-
income or developing countries were excluded. Later, some articles present in the references of
selected articles were also added, resulting in 58 studies and a webpage being selected. Figure i
shows a flowchart that demonstrates the selection process, and table i summarizes the inclusion
and exclusion criteria.

4
Results
Perceiving cancer patients’ vulnerability to Covid-19
Of the selected articles, 19 assessed the clinical interactions between cancer patients
and Covid-19 and had a study sample of more than ten patients and sought to understand if
cancer patients (CP) are more vulnerable than the general population. It was also evaluated
what other risk factors exist and if anticancer therapy (AntiCT) affects the prognosis (see table I
and II).
China’s and, in particular, Wuhan’s population were the basis of many studies. In one of
the first14, among 1590 COVID-19 cases, 18 (1%) had a history of cancer (higher than the cancer
incidence in China 0.28%). A composite outcome (admittance to the ICU, requiring mechanical
ventilation and death) happened to 7 (39%) of CPs and 124 (8%) non-cancer patients (NCP)
(Fisher’s exact p=0·0003). There were 4 CPs submitted to recent surgery or chemotherapy (ChT);
3 (75%) of them had a severe outcome [OR=5.34,p=0.0026)] having a significantly higher risk.
They recommended considering postponing adjuvant ChT or elective surgery in stable CPs of
endemic areas. Nevertheless, attention should fall to the fact that the sample size of CPs of this
study is small. Studies of larger sample sizes should be assessed to more faithfully interpret the
results.
In regards to this region, the other studies that followed analyzed patients mainly
through the first trimester of 2020. In the following study15, 105 CPs with COVID-19 were paired
with 536 age-matched NCPs of the same hospital (total 641). CPs were significantly more likely
to have been infected in a hospital setting than NCPs (19.04% vs. 1.49% p<0.01). CP case
mortality rate was 11.43%. having significantly higher risk of death than NCP [OR= 2.34 (p
=0.03)] in univariate analysis, (not when adjusted for multivariable p = 0.06) and of ICU
admission [OR=3.13 (p < 0.01), of having at least one severe or critical symptom [OR=1.99 (p <
0.01)] and of needing invasive mechanical ventilation OR 2.71 (p= 0.04), when adjusted for
multivariables. Hematologic, lung and metastatic cancer (HC, LC and MC) had higher risks of
death and worse outcomes, being in the latter [OR=5.58 (p=0.01); [OR=6.59 (p<0.01)]; [OR 5.97
(p<0.01)]; [OR=55.42 (p<0.01)], while non metastatic cancer had similar rates to NCPs p>0.05.
Patients that received surgery had a higher risk of death and worse outcomes, while those who
received radiotherapy (RT) had similar rates to NCPs.
In a succeeding study 16, 28 (2.2%) out of 1276 patients admitted to 3 hospitals for
COVID-19 had cancer. Among them, 15(53.6%) had severe events, with 6 (21.4%) requiring
admission to the ICU, with 8 (28.6%) of them dying. CPs at stage IV were more likely to have
5
severe events (70%vs 44.4%). Those that had recently (within 14 days) received AntiCT had a
significantly increased risk of severe events occurring, having a hazard ratio (HR) of 4.079 (p =
0.037), and the same was seen in those with patch consolidation on CT scan at admission [HR=
5.438, (p=0.010)].
In a study17 that analyzed 232 adult CPs and 519 matched NCPs (751 total), admitted
with confirmed COVID-19, the case fatality rate in CPs was 20%(n=46) and in NCPs was 11%
(n=56) which was significantly different (p=0.0012). CPs had also a significantly higher risk of
severe disease (64% v. 32%); [OR 3.61 (p<0.0001)] and in this regard, severe patients had a
mortality rate of 26% (10% in non-severe, p<0.05), they were significantly older p=0.024, had
higher Eastern Cooperative Oncology Group performance status score (ECOG PS score)
(p<0.0001) and more advanced cancer p=0.048. Risk of a severe COVID-19 was associated with
advanced tumor stage [OR 2.60, p=0.039)], increased TNF factor α [OR=1.22, (p=0.037)], NT pro-
BNP [OR 1.65, (p=0.032) interleukin-6 [OR=1.03 (p=0.019)], procalcitonin [OR=2.76 (p=0.0015)],
and D-dimer [OR=1.12 (p=0.0074)] and diminished CD4+ T cells [OR=0.84; (p=0.031)], and
albumin–globulin ratio [OR 0.12 (p=0.024)]. Severe COVID-19 CPs were more likely have been
treated with surgery 78 (93%)vs 119 (80%), p=0.018, ChT or RT p=0.042 and target therapy (TKI)
or immunotherapy (IT) 6 (7%) vs 26 (18%), p=0.044. When using surgical treatment as reference,
ChT or RT use was not a significant risk factor for COVID-19 severity [OR=1.28 (p=0.24) ] while
on the other hand, receiving TKI or IT was OR 3.29 p=0.015. The risk of disease severity in ChT
was higher when last treatment was within 2 weeks of hospitalization. CPs were also more likely
than NCPs to have ground glass opacity p=0.00070 or patchy shadows p= 0.0027 in CT scan.
A further study18 analyzed 3559 hospitalized patients with COVID-19. Among them, 107
(3.0%) had cancer. More than half of CPs had a severe course (n=56;52.3%), with 18 (16.8%)
requiring IMV. The case fatality rate due to COVID-19 was 21.5%. The risk of mortality even when
adjusted for multivariables was significantly associated with age [HR= 1.053;(p = .023) ] and
having recently or currently treated with AntiCT [HR= 3.56; (p = .003) ] or [HR= 3.117; (p = .016)
] if without patients in palliative setting. AntiCT effect in mortality was seen in both systemic
(e.g., ChT) and non-systemic therapies(e.g., RT or surgery). Patients receiving AntiCT had more
pronounced lymphopenia, anemia, elevated C-reactive protein, procalcitonin, a more severe
course (64.9% vs. 45.7%) of disease, and a higher need for mechanical ventilation (29.7% vs.
10%).
205 (2.5%) CPs among 8161 patients with COVID-19 admitted in 9 hospitals from the
Hubei province were included in another study19. Of the cancer patients, almost all 200(98%)
had symptoms, 30(15%) were admitted to the ICU, and 40 (20%) died, being higher than the 1%
in the general Chinese population. Of those who developed ARDS, 67% died. Significant risk

6
factors for mortality in this population shown using multivariable regression analysis were being
male [OR= 3.86 (p=0.0033) ] and having been treated with recent (within four weeks) ChT [OR=
3.51 (p=0.026) ]. Having HC [OR=2.07, (p=0.20) ] and age were not significant risk factors for
death in multivariate analysis with the latter also not being in the univariable analysis
[OR=0.99CI(0.97-1.01), (p=0.44) ] That said, HC patients (HCP) still had a higher case fatality rate
when compared with solid tumor patients (SCP) [HR=3.28; (log-rank p=0.0009) ]
In the final chinese study selected,20 207 SCPs with COVID-19 admitted in 32 hospitals
nationwide were analysed. Case fatality rate was 17% (n= 37). Significant risk factors for death
identified in univariate and used for multivariate logistic analysis that documented increased
age [OR=1.08 (p=0.043) ], recent (within 3 months) AntiCT [OR=28.65 (p=0.002) ], white blood
cell (WBC) count ≥6.93 ×109/L [OR=14.52 (p=0.003), derived neutrophil-to-lymphocyte ratio
(dNLR) ≥4.19 [OR=18.99 (p=0.001) ] and having dyspnea when admited [OR=20.38 (p=0.001) ],
as significant risk factors.
Countries in Europe and North America also followed oncologic patients with COVID-19,
but at a later period encompassing the middle of the first trimester of 2020 (February and
March) and through most of the second trimester (April and May).
In Madrid, Spain, two studies were selected. The first21 reviewed 1069 CP records
admitted in a hospital oncological department. Among them, 45 were positive (4.2%), being
higher than the incidence of COVID-19 in the Community of Madrid’s population
42,450/6,662,000 (0,64%) p < 0.00001 during that time. The fatality rate of COVID-19 in CPs of
42.2% was significantly higher than in NCPs 13.2%(p = 0.0001), and significantly associated with
increased age when adjusted for cancer stage and histology (74 vs. 63.5 years old, [OR=1.06, (CI
1.00–1.12, p = 0.03) ]. There was no significant difference in overall survival (OS) if patients were
under ChT (p=0.44). Compared with other studies, the higher mortality rate in these patients
may be due to a high percentage of metastatic cancer patients among the CP with COVID-
19(n=26;57.8%).
In Madrid, the other study 22, analyzed 63 cancer patients undergoing active treatment
admitted due to COVID-19. 61 (93%) of these patients had received recent (within four weeks
of infection) AntiCT. The overall case-fatality rate was 25.4% (n=16). In this population 54%
(n=34) developed respiratory failure with 47% (n=16) dying , and 38% (n=24) developed ARDS
and 67% (n=16) of them died. Multivariate analysis recognized severe neutropenia [OR=16.54,
(p= 0.025) ], bilateral lung infiltrates [OR=32.83, (p=0.002) ] and tumor lung involvement, be it
primary or metastatic tumor, [OR=4.34, (p=0.02) ] as risk factors of mortality. As such, the
authors concluded that hospitalized CPs under AntiCT had worse outcomes than the general
population, but similar death rate to hospitalized NCPs, using China’s general population

7
mortality 1.4% and using NY and China’s (25%; 24.5%) hospitalized NCP’s case fatality rate as a
comparison.
In NY, USA, three studies were selected. The first23 analyzed electronic medical records
of Mount Sinai Health System (MSHS) of 5688 patients with COVID-19. Among them, 334 (6%)
had cancer. The overall case fatality rate in CPs was 11.1% (n=37), and in NCPs 9.68%(n=518)
with a relative risk (RR) of 1.15 95% CI(0.84-1.57) that was not significant (p >0.05), but when
assessing the younger patients of 50 years the RR is significant p<0.05 of 5.01 CI(1.55-16.2). The
overall risk of CPs needing to be intubated is also significantly higher with 11.1% (n=37) CPs and
5.86% (n=314) of NCPs [RR=1.89(1.37-2.61) and especially for the 66-80 years age group
[RR=1.76 CI(1.15-2.70).
At the time of the second study24 (10 April 2020), 180 458 cases had been diagnosed in
NY with 9385 deaths, of those 8.4% were comprised of CPs. In this study 423 cases of
symptomatic COVID-19 CPs were evaluated, 168 (40%) were hospitalized, 87 (20%) developed
severe respiratory illness with 47 (11%) requiring high-flow oxygen and 40 (9%) required IMV.
The 30 day fatality rate of all symptomatc COVID-19 patients was 12% having 51 died, from
those admitted to the hospital was 24% (41/168) and 35% (17/48) patients admitted to the ICU.
Age above 65 [OR=1.53 (p=0.072) ] , treatment with ICIs [OR=2.84 (p=0.013) ], HC [OR=2.49
(p=0.003) ], non-caucasian [OR=1.62 (p=0.029) ] and chronic lymphopenia and/or use of
corticosteroid [OR=1.85 (p=0.030) ], were a associated with increase risk of hospitalization and
age [OR=1.67 (p= 0.024) ] and ICIs [OR=2.74 (p=0.004) ] were also a preditors of severe
respiratory disease, after multivariate adjustment. Mestatic cancer [OR 0.89 (p=0.647) ], major
surgery [OR=1.24 (p=0.612) ] and systemic ChT [OR=1.04 (p=0.845) ] both within 30 days did not
confer significant risk of hospitalization or severe disease.
Lastly 25, 117 hospitalized adult patients with COVID-19 and active malignancy were
matched with 468 NCPs (4 each) based on age, sex, and comorbid conditions, being in 585 total.
The death rate in hospitalized CPs (24.8%) was similar to that of matched hospitalized NCPs
(21.4%) p=0.894. The primary outcome in this study was a composite of admission to the ICU,
intubation, and death, which was not significantly different between hospitalized CP and NCPs
p=0.0814. Age and obesity were both associated with a significantly worse composite outcome
[HR, 1.15 95% (CI, 1.03 to 1.28) ] and [HR, 1.64 95% (CI, 1.21 to 2.21)] with age was also being
associated with a significantly higher risk of death [HR 2.04 95% (CI, 1.72 to 2.42)]. The presence
of active malignancy was not associated with a significant difference in composite outcome [HR
0.80 95% (CI, 0.50 to 1.13)] or death [HR=0.98 95% (CI, 0.58 to 1.67)] and the recent (within

8
90days) receipt of cytotoxic ChT also did no significantly alter the outcome [HR, 0.99 (95% CI,
0.52 to 1.88)].
In Germany, a study26 analysed 167 COVID-19 patients hospitalized at the University
Hospital Freiburg , 39 (23.4%) being CPs. A control group of 39 age matched patients, admitted
at the same time, was created. Among the CPs 8 (21%) died and in the NCPs 14 (36%) ,with HR
multivariable ajusted nearly 1 [HR = 0.99, 95%CI 0.40-2.43, (p= 0.98) ] and 30 day OS also similiar
78.6% (95% CI: 61.6%-88.7%) and 64.1% (95% CI: 47.0%-76.9%), respectively. Admission in the
ICU between both groups (41% CPs and 36% NCPs) was smilar p>0.05. The OS between SC and
HC was also similar (30dOS: 78.2% vs 80.0%, p = 0.95). 24/39 (60%) of CPs have active cancer 14
(36%) and received AntiCT . The 30 day OS of active cancer 83.1% (95% CI: 61.0%-93.3%) was
similar to that of non active cancer 70.9% (95% CI: 39.5%-88.1%). The risk factors associated
with worse prognosis were high IL-6 levels at COVID-19 diagnosis [HR = 6.95, (p= 0.0121) ], age
≥ 65 years [HR = 6.22 (p= .0156) ], and chronic kidney disease (CKD) [HR = 2.00, (p = 0.1176) ].
The authors advise caution in interpreting the results suggesting that other studies with larger
samples should be created.
In Italy, three studies were selected. The earliest 27 was where 21(3.1%) among the 675
CPs referred for consultation or therapy were diagnosed with COVID-19. 17(81%) of the 21
patients got infected during a hospital stay or soon after discharge, and 1 (4.8%) during
chemoradiotherapy session, afterward 18 patients (86%) were hospitalized due to COVID-19,
with 1(4.8%) admitted to the ICU. As soon as the patients were diagnosed, those under active
(n=9; 43%) anticancer halted it. The case fatality rate was 29%(n=6) and higher in those that
were under AntiCT during the diagnosis 44% (n=4) than does not under 16.7% (n=2) but not
significantly (p = 0,066, Fisher exact test, 2-sided), which the authors concluded that it could be
due to the small population. It was also noted that most of the infections were in the initial
stages of the pandemic. Once protection measures such as the use of PPE were implemented,
the infections diminished. Thus, not only could the CPs be more vulnerable due to the effect of
AntiCT, but hospital admissions and recurrent visits also put these patients at risk of infection.
A retrospective study 28, of a radiation oncology department located in Lombardy, where
402 cancer patients underwent active anticancer therapy, 23 had suggestive symptoms, and
13(3.23%) were positive, 5(1.24%) of patients died being 38.5% of Covid-19 patients. This high
mortality was explained to be due to the high patient age ( median 69.7 years, range 59.7–
84.9)and the high percentage of advanced cancer in patients infected (11;84.6% stage III or IV),
of male patients (11;84.6%), of patients with smoking history (69.2% smoking; 15.4% former
smokers) and of severe comorbidities (7.7% had none and 38.5% had three or more). Among
the positive cases, 6 (46.2%) developed severe disease, and none received mechanical

9
ventilation. This lack of use could have occurred due to an overwhelmed ICU or poor patient
prognosis and clinical condition.
The final Italian study selected was the COVINT study29, in Milan, which analyzed the
incidence of COVID-19 in cancer patients treated with anticancer therapy. Among the 1081
patients studied that had confirmed COVID-19, all of them were symptomatic, 10 (90.9%)
needed to be hospitalized, and 6(55%) eventually died. Only 1 (9.1%) was admitted to the ICU.
Of the five that survived, 3 (60%) fully recovered. There was no significant difference in COVID-
19 positive, suspect, and negative groups regarding cancer type, stage, type, and treatment
regimen.
From the UK, two studies were selected. First, a study 30 where 800 patients diagnosed
with cancer and had symptomatic Covid-19 were assessed, it was shown that 226 (28%) of the
patients had died. The risk of death was associated to certain risk factors such as age [OR=9.42,
(p<0.0001)], male gender [OR=1.67, (p=0.003)], and comorbidities such as cardiovascular
disorder [OR=2.32 (p= 0.0019) ], and hypertension [OR=1.95 (p<0.001)]. Of these patients, 281
(35%) had been treated with cytotoxic chemotherapy within four weeks of their COVID-19
diagnoses, and when adjusted to the other risk factors, it revealed that it had no significant
effect on their risk of death [OR=1.18 (p=0.380)], other AntiCT were also not seen as conveying
significantly different risk.
The second British study31 was a prospective cohort study with 1044 adult CPs in the UK
Coronavirus Cancer Monitoring Project (UKCCMP) with active cancer and infected with SARS-
CoV2 or had COVID-19, and the UK’s cancer population (without COVID-19) data of 2017 was
used as control. All-cause mortality was of 319 patients (30.6%), and due to COVID-19 295
(28,3%), it was associated with increased age (10% in patients with 40-49 years vs. 48% in those
older than 80) and male sex [OR=1.92 (p<0.0001)]. Male patients were more likely to get
infected, having a significant difference in distribution between UKCCMP and the control groups
[OR 1.57; (p<0.0043)] HCPs had a more severe disease course [OR=1.57 (p<0·0043)]. Moreover,
HCPs who had recent (within four weeks) ChT had an increased risk of death, being 47.6%
[OR=2.09 (p=0.028)] when adjusted for age and sex. This study also noted a low rate of ICU
admissions in this population, which was pondered due to a perceived less worth in admitting
CPs than NCPs.
In Belgium, a nationwide study32 analyzed 10486 adult patients hospitalized with COVID-
19, 892 (8.5%) with SC, and the risks were adjusted for multivariable (table). SCPs had a
significant higher 30 day death rate (31.7% vs 20.0%; [OR=1.34; (95% CI 1.13 to 1.58)] than NCPs.
This difference in the 30day mortality was more felt in the younger demographic <60 years
[OR=3.84; (95% CI 1.94 to 7.59)] and in the population without other comorbidities [OR=2.27;

10
(95% CI 1.41 to 3.64)]. It was reasoned that a higher prevalence of other comorbidities besides
cancer in the older population was mitigating the cancer impact. Curiously the difference in
mortality was inversed to the rate of admission to ICU (13.2%NC vs. 8.6%C), [OR=0.70; (95% CI
0.55 to 0.90)] and of receiving IMV (8.1%NCP vs. 4.9% CP), [OR=0.70; 95% CI 0.55 to 0.90), as
such composite outcome of ICU admission, IMV or death was similar in both groups (36.7%CP
vs 28.8% NCP), [OR=1.10; (95% CI 0.95 to 1.29)], the authors pondered if it could be due to higher
non-resuscitation demand in the cancer population, especially that of palliative care..
A study from the COVID-19 and Cancer Consortium (CCC19) database33 that comprised
USA, Canada, and Spain assessed data from 928 adult patients with active or history of
malignancy infected with SARS-CoV-2. The all-cause 30-day mortality was 13% (121 patients
died). Approximately half (466; 50.2%) of the patients were hospitalized, and 23% (n=106) died.
14%(n=132) of all patients were admitted to the ICU, with 38% (n=50) of these died, and 116
(12%) required mechanical ventilation 43% (50) died. The risk factors for increased 30-day
mortality (partially adjusted age, sex, smoking status, and obesity) were age (per 10 years;
[OR=1.84, (95% CI 1·53–2·21)]), male sex [OR=1.63, (CI 1.07–2.48) ] smoking status (former
smoker vs. no smoking history [OR=1.60, (CI 1.03–2.47) ], number of comorbidities (two vs. none
[OR=4.50, (CI 1.33–15.28) ] ECOG performance status ³ 2 [OR 3.89, (CI 2.11–7.18)] and active
cancer (stable vs. remission [OR=1.79 (CI 1.09-2.95)] (progressing vs. remission [OR=5.20, (CI
2.77–9.77)]. Obesity [OR=0.99 (0.58–1.71)], and recent (within 4 weeks of diagnosis) AntiCT
(cytotoxic [OR=1.47(0.84-2.56)]; non cytotoxic [OR=1.04(0.62-1.76)]) or surgery [OR=1.52( 0.58-
3.96)]) was not associated with significant increase in 30 day mortality. Lastly, it should be
noticed that most patients that died were not admitted to the ICU, 71 (59%) of the 121. .
Initial management recommendations
To evaluate early recommendations on the general treatment of cancer patients, mainly
those with a solid tumor, tables were made to consolidate these recommendations. These were
based on resource allocation (Table III), outpatient and inpatient setting (Table IV and V),
anticancer treatment as a whole, and by type of procedure (except in ChT that was included
mainly in the outpatient setting) (table VI), staff measures (table VII), telemedicine use
implementations and limitations (table VIII) and other general measures (table IX).
One of the main challenges to the treatment of CPs during the COVID-19 pandemic is
that of resource allocation that may limit treatment to cancer patients. It is imperative to ensure
that the disruption to cancer treatment is reduced to a minimum, especially to those of curative
intent34-37. Elective surgeries and non-urgent outpatient visits were delayed and canceled,

11
especially when there was an increased workload or resource shortage 34,35. As such, treatment
prioritization and care intensity were to be adapted based mainly on the pandemic scenario38,
treatment priority level38,39, health care capacity38, and resources available38,40. Other
recommendations for the allocation of resources are in table III. An example of cancer patient
prioritization is the one used by ESMO, which is used to stratify the treatment approaches based
on patients’ condition and the intervention’s benefit41, seen in table III.1.
In the outpatient setting, activity also needs to be altered. In general, outpatient visits
should be reduced, especially those non- urgent34,36,39,40,42 such as in routine and follow-up
visits39,40,42,43 and for at special risk populations, such as older patients44. When possible, in-
person visits should be substituted by remote ones such as by phone or video36,37,40,42,43,45.
Patients should be educated 34,37,42 on how to diminish risk of exposure. It can be with hygiene
34,37 and infection control measures34 such as reporting to HCW in case of symptoms34. Entry and
exit points should be limited34, 31 as well as visitors accompanying the patient,34,39,43,45 . For the
patients planned to be admitted, they should be screened before admission to detect possible
infection,34-39,42,43,45,46, this can be done the day before by phone infection,34-37,39,42,43,47 and/or
before entry,34-39,48, mainly regarding contact34,36,38,43,45, or travel history,34,36,38,45 and existing
fever or respiratory symptoms34,36,38,39,42,43,45,48. If feasible, RT-PCR tests should be implemented
to all patients before a treatment session38,40 (e.g.,48h before each treatment cycle) or all
suspect cases38,43, with the latter barred from entering the center38, their visits are canceled, they
are put in isolation/quarantine39 and if positive should be transferred to a specialized unit 37,40,43
or considered for home or community care in mild cases43. In the case of ChT infusion sessions,
in general, delays should be avoided 34 , but it could be considered in patients with stable or
slow-progressing tumor26. Another approach is switching from intravenous to an adequate oral
substitute therapy 34,36,39,40,46,48 and reducing the number of visits 34,40. To avoid ChT’s cytotoxicity
and the potential of inducing neutropenia, prophylaxis with hemopoietic-stimulating factors
such as G-CSF35,36,38,39,42 could be expanded from those of high risk (>20%) to also those of
intermediate risk (10-20%)38 and the elderly38. Home infusion 34 and courier 34,36,39,40,43,44,47 could
also be considered to avoid vulnerable patients from unnecessary exposure 43. Cancer survivors
should adhere to general population recommendations to diminish possible exposures34,37,
reduce the number of surveillance visits34,37, and remain at home for the time being37. Inside the
clinic or hospital, social distancing should be followed 36, and the use of PPE, such as masks,
should be mandatory36-38 . Other recommendations in the outpatient setting are included in
table IV.
For the inpatient setting, the recommendations assessed have been summarized in table
V. Hospitalizations are to be expected, be it from medical emergencies or uncontrolled

12
symptoms 34 so specialized wards34,36-38,40,46 for the treatment of COVID-19 patients 36-38 with
HCW dedicated to only their care are recommended 34, while other patients should be treated
in COVID-19 “free” institutions or wards 36-38 . However, with the ensuing pandemic and possible
destabilizing of healthcare systems, this may become more and more difficult to implement, and
triaging should be put in place34,38,43 to ascertain patients with suspect symptoms34,38,43,48 and
whose urgency requires admission34,38, limiting non-urgent inpatient admissions 34,39,48. In
COVID-19 wards, a team with a lead infectious disease specialist qualified for cancer care should
be created. Patients and HCW should have access to PPE 34,36,37 ,38,48,49, masks should always be
worn34, and HCW in COVID-19 ward should wear full PPE38, as well as patients when they are
being transferred to other departments or wards 36-38
Anticancer therapy measures in table VI are considered in general and then in individual
procedures besides chemotherapy (summarized in table IV). Patients should be informed of
possible therapy risks during the pandemic 34 and given the option to change to a less myelotoxic
treatment 34 . As for altering anticancer treatment, it should be decided in a case-by-case
basis39,42-44 according to treatment intent43, patients’ clinical characteristics43, prognosis40,43, and
preference43. Priority should be given to the treatment of symptomatic cancer cases43 and
procedures with a high impact on prognosis43. As for positive COVID-19 cases, some articles
argue that postponing treatment should be considered on a case-by-case basis43, while others
recommend ceasing and postponing anticancer treatment in symptomatic49 or all positive
cases34,35,37.
In regards to surgery, recommendations are present in table VI.1. Due to potentially
exposing patients to risks and resource allocation due to the pandemic, treatment prioritization
is implemented with elective and non-urgent surgeries being promptly delayed34,35,37,39,44,45. As
such treatment prioritization should be based on urgency35,45,46, efficacy35, post-op use of
resources such as ICU bed and ventilators35,45, type of procedure based on possible exposure
and its perceived duration45, alternative treatment 36, cancer characteristics, such as histology 36,
location40 and progression rate46. HCWs are also at potential risk of exposure, especially during
some procedures like intubation and extubating 36 . As such, all patients should be tested and
screened before an invasive procedure 36,37,, and due to the possibility of false negatives, a
second test can be considered36,37. In the post-op, fewer lab work and image scans can be
considered 36 and fewer adjuvant treatments following surgery or of lower duration and oral
systemic AntiCT are preferred 36. In radiotherapy patients need to attend treatments daily, and
interruption of ongoing therapy is not recommended 34. RT measures recommended are present
in table VI.3. It can be used as an alternative treatment to surgery39. Other measures
recommended in the activity of radiotherapy can be summarized according to ESTRO as safety,

13
avoidance, rescheduling, and shortening (SARS) 50. As for immunotherapy and target therapy,
measures are present in tables VI.2 and VI.4, respectively.
Measures recommended regarding the staff are present in table VII. In general, if
exposed, staff may need to self-isolate34,39 , so to limit these absences, PPE should be provided
to all HCW and used accordingly along with other hygiene and infection control measures;36-38,49.
These include practicing hand hygiene36-38 and avoiding crowded places37;, HCW should be
allocated to only one facility36, and it is recommended to rotate staff36. Triaging among staff
should be implemented mainly at hospital or facilities entry points36, routine tests can be
implemented 36, and those suspected of being infected should also self-isolate until a negative
test38.
Telemedicine use recommendations and limitations are present in table VIII. Table IX,
includes other general measures, such as implementing nutritional support to patients51, and
implementing psychological support34,36,37,39,42-44 for patients;34,37,39,42-44 and HCW 36,37,42,44; as
they are more susceptible to symptoms of anxiety and distress34,42,43, in this tough
unprecedented period.
Impact on Cancer care
To understand how the pandemic affected cancer therapy care, we must see how the
activity was adapted and its impact. Twenty-four studies were selected that disclosed these
changes. Two of them also mentioned the impact on CPs and one disclosed recommendations
in the previous section. These are listed in Table X. Table XI presents the recommendations taken
or assessed that coincide with those previously mentioned, along with the impact the pandemic
had in cancer activity and how the measures affected infection transmission in the departments
or centers present in each study.
Many of the studies selected centered on Italy. The earliest52 analyzed the difference in
activity in an oncological department in Verona (Italy) between January 1 to March 31, 2020,
from the same period in 2019. On March 13, the oncology ward was turned into a COVID-19
unit, with the previous inpatients relocated to a surgical ward. Different teams dedicated to
positive and negative cases were established and separated, resulting in a temporary decrease
of 40% - 43% of HCW dedicated to cancer patients. During this time, maintaining ongoing
systemic treatment was prioritized over new treatment. Overall oncologic procedure admissions
decreased 8% during this period reaching 40% in March, with a 6 % decrease in total ChT
administrations, reaching 14% in March( p<0.05), 3% decrease in specialist visits, reaching less
35% in March <0.05. Of the 471 COVID-19 patients admitted, 75 (15.9%) had a history of cancer,

14
15(3.2%) were on active treatment, being 7 (1.5%)in this unit and encompassing 1.3% of the 525
treated during this period. Of these cases 2 (28.6%) died, 5 (71.4%) were discharged and 3
(42.8%) resumed AntiCT. Of the 85 HCW, (9.4% 8 (9.4%) got infected, 7 (7/40; 17.5%) worked
at some point in the COVID-19 unit, of the remainder 1 (1/45; 2.22%), none were due to non-
adherence to prevention measure or in hospital contagion, and none were severe. Most
prevention measures, such as double triage (by phone and before entry), adherence to PPE by
staff and patients, and limitations to visitors were implemented in March.
The next study 53, evaluated how activity changed in an ROI in Rovigo, Italy, during
February and March of 2020 and 2019. On the day before follow-up, patients were contacted
regarding health and cancer status. Stable cases were postponed, patients with progressing
cancer were admitted after another phone triaged for possible COVID-19 infection, based on
symptoms, contact history, and residency. Non-suspect cases were permitted admission, along
with that of one caregiver. If an infection was suspected, the national dedicated telephone
number was activated, or patients were referred to their general practitioner. Urgent conditions
were to be treated within 24 to 48h and non-urgent palliative RT within seven days. Elective
treatments with high priority were promptly admitted after phone triage, and those of lower
priority were delayed up to 3 months. HCWs were mandated to use appropriate PPE in cases of
high-risk contact. All visits were evenly dispersed throughout the day. Activity in 2020 increased
in first visits 8.8%, and patients treated 13.0% (130 vs. 115). The HCW absence is comparable in
both years. No patient or HCW was infected during this period.
The COVINT study 29 also analyzed changes in treatment activity between 2020 and 2019
during the same period. Of the five that recovered, 1 (33.3%) resumed anticancer therapy after
55 days. Patients were suspected (n=73 ;6.7%) of infection, if they had symptoms (86.3%) or
signs like suggestive findings in CT scan (n=23;31.5%) and negative or no RT-PCR test, which was
only performed in 41.1 % of suspect cases. Of the suspect cases, 35 (45.2%) were quarantined
for at least 14 days, and 28(38.4%) stopped anticancer treatment, with 22(30.1%) later resuming
in a median of 50 days. In a whole, 96(8.9%) patients’ anticancer treatment was postponed as a
precautionary measure. On average, in both years, each patient received two treatment
administrations during this time, but in 2020 there were 15% fewer patients and a resulting
decrease in treatments administered of 9.5%). In the inpatient setting there were 130 (22%
decrease; 166 in 2019) patients treated, 181 hospitalizations(20% decrease; 226 in 2019), 4
(3.1%) of them developed COVID-19-like symptoms, 1(0.8%) had ground glass in CT scan and
1(0.8%) was positive for COVID-19. Prophylactic myeloid growth factors were given to 58 (5.8%)

15
patients if they were negative for COVID-19 and more frequently in non-suspect than suspect
cases (5.3% vs. 2.7%; p<0.001).
The treatment activity changes of the Brescia University Radiation Oncology
Department were studied28, in a selected article. The total RT performed decreased, reaching a
maximum of 17% decrease, being at 11% decrease at the end of the period, while systemic
therapy maintained nearly the same level. Treatment planning in March decreased
approximately 50% due to treatment delays and restricted patient flow in the center. There was
a relative decrease in brachytherapy thanks to the postponement in the treatment of low-risk
prostate tumors. Among the 87 HCW, 12 (13.7%) were positive, and 7 (8.0%) had suggestive
symptoms but a negative test. The staff shortage was at its highest from mid-March to early
April. Most patients deaths and infections occurred until March (12 of 13 positive cases occurred
until March 24 and 4 of 5 deaths until March 16). The authors attributed this to an initial
underestimation of the outbreak, followed by tighter adherence to PPE and prevention
measures that helped contain the infection. After March 24 infection rate was 0.43% (total
3.23%). Therapy was maintained in 46.2% (6/13) of positive cases and 50% (5/10) of suspected
patients, with no pauses.
Also, in Italy, a study54 where the activity of an ROI in the region of Abruzzo, at the time
one of the least hit (had 1.39% of national cases) of Italy, was compared with that of 2019. The
activity was altered in two phases, during lockdown (phase I) from March 9 to May 3 and after
lockdown (phase II) from May 4. Comparing both years (2019 vs. 2020) in that period (phase I),
there was no significant change in overall function. First radiotherapy visits (123 vs. 121),
simulation computed tomography (137 vs. 135), and linear acceleration treatment (151 vs. 170)
remained nearly the same. Among the 42 active staff members, all were tested in the week of
May 25 to May 31 with RT-PCR, and none were infected. Measures of prevention transmission
control and safety are reported to have been adhered to and implemented mainly by the Italian
Society of Radiotherapy and Clinical Oncology. In phase I, telemedicine was the primary tool for
patient consultation, while in phase II, the follow-up clinic was reopened but only allowed one
patient appointment every 45 minutes. They also report that Italian centers decreased clinical
activity <10% in 32%, 10-30% and in 30.4% and in Lombardia (the most hit region, 38.38% of
cases) cancer radiotherapy was reduced 10%-50%, meaning that in Italy, RT activity reduction is
directly affected by the impact of COVID-19 on the region.
Reported changes in radiotherapy activity in their unit of the University Hospital of Pisa,
Italy, between 2020 and 2019 during the same time period, were analysed in a selected study55.

16
Hypofractionated regimens were preferred, and treatment was delayed in patients with a better
prognosis and benign disease. Compared with 2019, there was an 18% decrease in first-time
visits, a 5% increase in RT procedures, and an increase of 29.8% in patients under palliative
treatment, and the latter was a result of the restructuring of departments that led to the
shutting of palliative therapy and surgery. Among the 52 HCW, none were infected, and among
the 365 patients in active treatment, 2 (0.55%) became infected, with one during treatment that
was shortly postponed until having a negative RT-PCR test. The low infection rate was reasoned
to be a result of the preventive measures taken. Some of the reasons for the decreased number
of visits were pondered to be due to delays in diagnostic and histologic/cytologic tests.
A study56 on the changes made on Italy’s nationwide medical oncology departments
with a survey responded by 122 physicians head of oncological departments. One of the most
widespread measures was the vaccination of patients (93%), especially if the patient is under
active treatment, mainly for seasonal flu (64%), pneumococcal (7%), or both (37%). Before visits,
triage to detect suspicious COVID-19 patients was also generally adhered to (95%), be it in all
patients (70%) patients with fever (19%), respiratory symptoms (12%) or both (7%) and 65% of
responders reported preventive isolation followed by RT-PCR and imaging if the patients were
symptomatic. In terms of treatment changes, there were mainly treatments and visit delays in
non-urgent patients. Around 20% of establishments reported a considerable change in activity,
60% a small change, and 9% reported virtually none. In order to counter this decrease, 80% of
responders used other means, mainly telemedicine (by phone). Of the responders, 24% reported
that at least one of their patients had COVID-19, mainly those in Italy’s red zone with 46%. On
the effectiveness of the measures, 53% of responders think that they can significantly reduce
the risk of infection, while 39% think its effect is insufficient.
The impact that the pandemic, during its first five weeks, had on urgent and elective
surgeries in Italy by a survey on March 27 (when Italy had 86,498 positive cases and 3732 in the
ICU) responded by 54 surgical units (30% in Lombardy), in 36 hospitals, was analyzed in a
selected study57. At the time, 32 (89%) hospitals had positive cases, 33 (92%) created a
department exclusively for COVID-19 patients’ care, and 33(92%) had COVID-free ICUs with an
average of 8 beds. Positive cases occupied a median of 14% of hospital beds (>30% in Lombardy).
Non-urgent and non-oncologic surgeries were canceled, and resources reallocated (e.g., HCW,
ventilators) to the care of positive cases. There was a decrease of hospital beds in 38(70%)units,
of surgical activity in 41(76%) with a median of 50%, of ICU beds available in 45(83%), and
outpatient clinics in 52(96%). Temporary blood component shortages occurred in 19 (35%) units.
17
Surgeries performed declined from 3.8 a week to 2.6 (p=0.036). There were 8 positive patients
operated in 7 units (13.0%), and 31 surgeons at 18 units (33.3%) contracted the disease, 12 of
them in Lombardy (12/31; 38.7%). The time between a multidisciplinary discussion and the
surgery went up, from 3 to 7 weeks (2.3x), which were repeated in 31 (64%) of the units. 13(24%)
preferred non-surgical alternatives. Patient prioritization for surgery was based mainly on the
type of tumor (aggressiveness) (80%), the time that elapsed from the neoadjuvant treatment
(61%), the demand for post-op ICU (57%), probability of becoming inoperable (57%) or if the
tumor was symptomatic (52%). The PS score, complexity of the surgery, and the lack of
alternative therapies were also considered. Imaging was restricted in 31% for CT scans, 24% for
MR, and 13% for PET CT scans. Radiotherapy was also limited in 11% of units. In 42(78%) units,
pre-surgery testing was implemented, 21(38.9%) with RT-PCR using NPS, 6(11.1%) with CT scan,
and 10(18.5%) with both, with 4(7.4%) only if the patients were symptomatic. Post-op testing in
patients presenting with fever was implemented with chest imaging in 25(46%) and adding RT-
PCR testing in 5(9%).
A nationwide Italian study 58, based on a survey responded by 125 directors of Italian
radiological departments. Within the first weeks of the outbreak, 68% of the facilities were
converted to COVID-19 centers. Hypofractionated RT regimens were preferred in 73.6% of
departments, especially in larger centers. Waiting lists were reorganized to ensure prioritization
in 62.4%. Outpatient first-visits were generally maintained (98.6%), but almost all non-urgent
routine follow-up visits were stopped (92%), and teleconsultations were increased by 62.4%. In
terms of overall clinical activities, only 28%(n=35) reported no change, while 32%(n=40)
reported a decrease in <10%, 30.4%(n=38) of 10 to 30% and 8.8%(n=11) of 30 to 50%. Triages
were done initially by phone in 48.8%, then at hospital entrance 54.4% and 75% before entering
the radiation department. Almost all centers imposed masks and social distance (98.4% and
94.4%), 76% of departments completely restricted visitors, and 84.8% implemented cleaning
protocols, particularly of surfaces. During this period, 62.3% of centers reported no infected
patient, and 26.2%(n=32) had 1-3 patients, with most cases in Lombardy and northern Italy.
Nearly 2/3 of centers postponed RT treatment in positive cases, with half of these resuming right
after two negative RT-PCR tests. PPE was generally given to HCWs, primarily surgical masks and
gloves, in almost all departments (>90%). Teleworking was adhered to in administrative HCWs
in 48.8% of departments. Quarantined HCWs were present in 45.5% of departments, with 11%
having more than five, being more felt in areas with more cases. In 16% of centers, HCW were
drafted to the care of COVID-19 patients (ward or triage). Nearly 50% of centers implemented
psychological support for HCWs.
18
The Italian immunotherapy activity changes and a comparison between different
regions by COVID-19 prevalence (high H, medium M, low L) were reported via a survey,
responded by 75 (17H; 51M; 7L) young oncologists and analyzed in a selected article59. CPs in H
and M were mainly triaged the day before admission by phone and then before entry (82.4%;
58.8%), whereas in L, most (57.1%) reported screening only before admission p=0.03. Generally,
treatment would start after triage and not delayed upfront, be it for metastatic (92%) or in
adjuvant treatment (80%), and treatment in suspect cases was generally halted (96%) until a
negative test. The use of telemedicine for follow-up in patients that completed or fully
responded to ICI was present in H (88.2%), M(90.2%), and L(85.7%). In those treated with ICI,
positive cases occurred in 29.4%, 31.4%, and 0% (overall 28%). Most 76.5%, 74.5%, and 100%
opted for longer interval schedules, and no responder selected shorter intervals. The dose of
steroids used in ir-AEs was seldom changed (4%), and almost all would not substitute ICI
treatment for ChT (92%) or TKI (88%). G-CSF was largely used in the case of febrile neutropenia
(H=88.2%, M=92.2%, L=100%). Lung cancer was not seen as a reason to delay (89.3%). Surgeries
were delayed by 46.7%. The only significant difference between regions was in the patient
screening method.
In the Netherlands, a study 60, where 5302 cancer patients responded to a survey
between March 29 and April 18 on how in their perspective, their treatment changed in
response to COVID-19. Half remained in contact with the hospital during this period, 36% from
those in follow-up, 52% of those awaiting treatment, and 69% of those receiving treatment
(p<0.05). These visits were significantly higher between April 4th and 17th (57% vs. 48%, <0.05),
even with the country being more heavily hit, by the pandemic, during that time. Among those
in contact with the hospital, 30% reported changes in treatment, with 52% of them switching in-
person visits to remote visits using telemedicine by phone or video. Treatment changes included
therapy adjustment (3%; 7%), delay (16%; 12%), and discontinuations happened in overall 20%
(49/250) of those awaiting and 20%(480/2391) of those under treatment. The therapies
adjusted were primarily chemotherapy (30%)and immunotherapy (32%). In areas more hit by
the pandemic (code red), visit cancelation and treatment adjustments were higher but not
significantly than in the other areas, but the patients’ concern over getting infected was
significantly greater (51% vs. 46%, p < 0.05).
In a german hotspot University Hospital, the changes in radiation oncology management
were analyzed in a selected article 61. Patients with benign disease treatment were unanimously
postponed and curative in the radiation setting, and definitive and palliative treatment was
19
prioritized over postoperative adjuvant treatment. Hypofraction regiment was preferred
whenever possible. Every inpatient had a COVID-19 PCR-RT test done on admission and needed
a negative test done in the last 72 hours before an invasive procedure. In the public outpatient
setting, the rate of patients showing for their first visit was maintained at 85.5%, similar to the
88.9% of 2019 p=0.165. However, there was a significant decrease of 10.3% in the number of
daily appointments compared with 2019 (6.4 vs. 7.1) (p=0.004) and 14.7 % of those presenting
(5.4 vs. 6.3) (p=0.0024). In a private outpatient setting, there were no significant changes in
scheduling (2.7vs 2.8 p=0.331) or showing (2.5 vs. 2.5 p=0.468) patients. Because more severe
cancers were selected, CT scans planned and performed were increased by 13.9% (10.6 vs. 9.4
p=0.0001) and 20.1% (10.0 vs. 8.2% p=0.0001), respectively, and the ratio of performed and
scheduled CT scan increased from 88.2% in 2019 to 93.7% in 2020. The start of radiation
treatment increased 18.5% in 2020 (8.8 vs 7.5 p=0.024). Hypofractionated and acceleration
regiments were more widely used p=0.0043). Stereotactic radiosurgery (SRS) was used more
often in 2020 (2.23 vs. 1.45 p = 0.0043), while the number of patients treated with CyberKnife
was similar in both years p=0.364. The aftercare clinic had fewer patients presenting both in
public 98% (6 vs. 318, p = 0.0001) and private 73% (13 vs 48 p = 0.001) divisions. PCR-RT test for
SARS-CoV2 was done on 74 (45.1%) of the 164 inpatients, and none were infected.
A selected study62 investigated the pandemic’s impact on radiation oncology care,
though ROIs responded to a questionnaire in Germany, Austria, and Switzerland. Among the
106, 24 (22.6%) had had patients infected with SARS-CoV-2. In positive cases with few or no
symptoms, most ROIs (76.7%) maintained treatment. If symptomatic most centers would stop
treatment or have a break of RT for longer than one week and then continue treatment
afterward (68.8%). HCW tested positive in 16.5% of ROIs, with a cumulative incidence of 0.56%
(vs 0.25% in general population). The patient screening was employed in 50.5% of ROIs, with
questionnaires (47%), temperature checks (27%), and PCR-RT test (10%), only 23.3% screened
HCW mainly with temperature and other symptom checks. HCW groups were restricted in
number, mainly in RT technicians (RTTs) (66.3%), physicists (59.3%), and physicians(51.2%), and
less frequently in nurses (32.6%) with work at home established and done by 18.3%, 52.3%,
32.6%, and 9.3%, respectively, especially for those more vulnerable (e.g., older, with
comorbidities). In terms of PPE, the most used were surgical masks, in 88.4% of RTTs, 66% of
nurses, 86.0% of physicians, and 93% of patients in ROIs, 34.9% of which reported a temporary
shortage. Curative RT activity remained unchanged significantly more in curative than palliative
in 68.4% vs. 53.6% of ROIs (p<0.001), and for preference of hypofractionated regimens 18.1%
vs. 28.1% in moderate hypofraction and 7.6 vs. 14% in ultra-hypofraction overall significantly

20
more in palliative (p<0.001). In benign cases, RT was mostly postponed (69.0%). For ChT and
other systemic therapies, almost all maintained their treatment unaltered (90.8% and 92.1%),
but follow-up visits were mostly postponed or replaced by telephone/video visits (42.2%; 43.6%;
0.5%). Having positive cases did not alter the treatment for curative setting nor impact overall
follow-up approaches.
RT centers from Germany, Austria, and Switzerland, the COVID-19 impact analyzed in
study63 through a survey responded by 154 medical physicists. Of responders, 56.2 % work for a
public hospital, 5.9% a private hospital, and 33.3% a private RT center. Ambulatory treatment is
preferred, and patients with malignant cancer are prioritized over benign CPs. 72.4% of
responders reported that the pandemic impacted RT activity. 54.2% due to practices taking
longer than usual, since added safety measures, 36.7% due to reduced number of HCWs
working, 42.5% due to increased patient absence for consultations, this eventually led to
increased workload and strain for staff present. Most adhered measures were giving specific
information for patients at the entrance (89.6%) or by phone (73.6%), limiting visitors/caregivers
(77.4%), and canceling/delaying visits (69.8%). As precautions for eventual treatment
restrictions, prioritization of treatment had already been implemented, mainly based on
urgency 41%, hypofractionated regimens were increased by 33.7%, or added treatment
fractions to compensate breaks in 14.5%. Projections are that this will rise in implementation to
61.5%, 48.2%, and 39.8% of responders.
The results from a survey conducted by the European Society for Radiotherapy and
Oncology (ESTRO) responded by 139 heads of RO departments in 29 European countries were
revealed in a selected study50 and compared with that reported by the American Society for
Radiation Oncology (ASTRO). During this period, all departments maintained active, but 58%
reported treatment delays in new cancer cases, with the percentage differing for each country,
being lesser in Italy (40%)and higher in the UK (100%). Telemedicine was generally used (78%),
having most of these centers (76%) specifically introduced it in response to the COVID-19
pandemic, 22% (0% Belgium; 88%UK) used it for clinical evaluation of patients in active
treatment, and 72% (41% Germany; 100% Netherlands and Belgium) used for patients in follow-
up. In 60% of departments (50% Netherlands; 88%UK), there was an average decrease of 25%
inpatient volume resulting from treatment postponements (65%), decreased referrals (75%),
and reduced staff (15%). In 57% staff was diminished due to the pandemic, be it for contracting
COVID-19 in 26% (0% Netherlands; 71% Spain and UK), need to care for family members in 29%
(0% Belgium;71%UK), response to a lower number of patient visits in 11% (0%Switzerland and

21
UK; 33% Belgium) or because of staff transfers 13% (0% Belgium; 29% Spain and UK). Treatment
delays were mainly benign or early cancers, most prominently for low and intermediate-risk
prostate cancer (62%;40%) and non-urgent palliative treatments (25%). In terms of protective
measures, in staff most prominent were the use of masks and social distancing (89%;88%), but
the use of other PPE such as gloves (69%) and screening before each shift (60%) was also widely
used. In terms of patient screening, 82% reported performing before admission at the entrance,
with complete restriction on visitors in 88%. In 48% occurred PPE shortages, and in 6%, there
was a lack of medications. ASTRO’s results though similar, there were some changes mainly in
that 84% reported a decrease in volume of at least 20% inpatient volume, while in ESTRO, only
38% decreased that amount. 78% in ASTRO reported a supply shortage vs. 52% in ESTRO.
The Canadian medical oncologist responses in a survey on the impact in medical care
were also analyzed64 . Only one (0.6%) of the surveyed was diagnosed with COVID-19, seven had
been exposed (3 in the work environment), with 5 in self-isolation. Regarding the use of PPE and
adherence to hygiene, it was reported by 33% that no routine use was in place, by 13% of used
them scarcely or were even sometimes discouragement (those besides masks and hygiene),
while 54% used PPE regularly. Symptoms suggestive of burnout were highly reported, mainly
increased anxiety (54%) and decreased attention (33%). In cancer care, telemedicine was used
by 82% in most of their patients, mainly by phone (100%) and video conferencing (42%). In terms
of follow-up visits, 22% maintained frequency, 64% maintained partial frequency, and all were
delayed or canceled in 14%. In clinical trials, 54% reported stopping new patients’ accrual and
were restricted in 34%. In terms of chemotherapy regimens, 26% responded to unaltered
activity, in 38% changes were in a low percentage of patients (<20%), in 25% in a moderate
percentage (20-40%), and 10% in a significant percentage (>40%). The main factors for
treatment change are patient prognosis, treatment effect, risk of treatment toxicity, and risk of
SARS-CoV2 infection.
A study 65 monitored 121 patients’ activities, in a RO department in Texas early in the
pandemic. Patients included were being treated with RT and were tested for SARS-CoV-2 with
RT-PCR. Motives for testing were symptoms (fever or RS) 55%, screening before a procedure
30%, travel history 11%, imaging findings 4%. Other measures include delaying routine visits in
non-urgent patients for ³2 months, increased use of telemedicine, referring patients to
establishments nearer home. Screening for fever and RS for all patients and HCW on the
entrance with different sites for each group. PPE use of surgical masks became mandatory in
HCW and patients in the middle of the investigated period, with other PPE such as gowns, gloves,

22
respirators, and goggles were also given to HCWs. Among the 121 patients, 7 (5.8%) were
positive. In 40 (33%) patients, RT was deferred or stopped in those awaiting test results, which
lasted an average of 3.5 or 1 days, depending on the time it took for a result (1.5 or £1 days,
respectively) . During this period, 39 HCW were quarantined for an average of 3 days, with a
peak of 17 HCWs absent at the same time, right before implementing mandatory PPE use, which
resulted in a six-fold reduction in new HCW quarantines from 2.9 to 0.5 a day. No HCW tested
positive.
A nationwide cross-sectional survey in the USA, responded by 411 physicians, 241
(58.6%) surgeons, 106 (25.8%) medical oncologists, and 64 (15.6%) radiation oncologists, was
analyzed in a selected article66. Among the responders, 57% sustained that the PPE available was
sufficient for clinical activity. Of the responders, 68.6% stated to have changed treatment
regimens, with 71.5% of surgeons delaying or canceling surgeries (70.2% maintained with
alternative treatment), 73.4% of the radiation oncologist, and 64.4% of medical oncologists
doing the same for RT and ChT, respectively. Similar reasons for treatment alteration were
present in all groups, but medical oncologists were significantly more likely to change than
radiation oncologists or surgeons due to the higher risk of patient exposure and infection to
SARS-CoV2 (91%; 78.7%; 69.1% p=0.002). Surgeons were significantly more likely to change than
medical or radiation oncologists due to the need to conserve PPE, due to institutional directives
and due to medical recommendations (67.9%; 10.5%; 25.5%; p<0.0001, 71.4%; 34.3%; 25.5%; p
< 0.0001 and 73.8%; 34.3%; 51.1%; P < 0.001). And finally, radiation oncologists were
significantly more likely than surgeons and medical oncologist to alter treatment regimens due
to logistic problems, like the restriction in visitors (34.0%; 13.7%; 26.9%; p=0.003) and more
likely to alter due to risk of exposure and infection to HCWs (61.7%; 51.2%; 40.3%, p = 0.08).
A survey responded by oncological centers in 10 countries (from Europe and the USA),
to assess how their activity changed, it was also analyzed67. In 19/21 (90.5%), patients were
triaged before visits, 20/21(95.2%) before outpatient infusion at daycare, and 20/20 (100%)
before inpatient hospitalization. This triage was mostly by phone the day before(81%;85.7%,
and 90%). Before entry, symptoms were checked for 17(81%), 20(95.2%), and 19/20 (95%),
respectively. Visitors were only allowed in 8(38.1%), 4(19%), and 8(40%), with few exceptions.
Only 2/21(9.5%) did RT-PCR tests routinely for outpatients, but 13/20 in ( 65%) inpatients. In
90.5%, surgical masks were mandatory to patients and in 100% to HCW. Increased disinfection
practice in 17(81%) for consultation rooms, 18(85.7%) daycare units, 17/20(85%) inpatient units.
Physical exams were stopped in 16(76.2%) of centers, along with reduction of non-necessary

23
exams, blood pressure control, blood sampling, and radiological response evaluations, the latter
two reduced > 25% in 10(47.6%) and 11/21 (52.4%). In the inpatient palliative setting, patients
decreased in 10/20 (50%) of centers, and inpatient ChT was referred for outpatient use in 5/20
(25%). In inpatient treatment, 13(65%) tested all patients before admission, with half (10) only
allowing negative cases to be admitted. HCW were seldom routinely tested, with only two (10%)
implementing to all HCW (one weekly another biweekly). Different units for COVID-19 positive
or negative were implemented in 20(95.2%) centers, with members unable to coincide in
12(57.1%). Specific pathways were created if cases were positive or negative in 20(90.2%).
Inpatients, positive and suspect cases were transferred to COVID-19 positive units in 18(90%).
Day care positive or suspect cases were treated in specific units in 9(42.9%). Increased use of
telemedicine was seen in 16(76.2%) centers by phone or video consultations. Video board
meetings were implemented in 17(81%) centers. HCW had to isolate if they had a fever
20(95.2%) or living with someone self-isolating 13(61.9%). For the return to work in positive
cases, most 16(76.2%) required 14 days of isolation and a negative test. Work from home was
allowed in 1(4.8%) center for those vulnerable or living with vulnerable people..
The activity from Korea University Anam Hospital in 2020 was compared with that of
2019 during the same period68. There was a reduction of 14.7% in the number of diagnoses (
1445 vs. 1694), 3.6% in surgeries performed, 24.3% in RT performed. However, in metastatic
cancer patients, ChT activity increased 12.6%), especially in outpatients with a 73% increase,
while there was a decrease of 8.1% in inpatients (1742 vs. 1896). In 2020, patients were tested
for COVID-19 based on suggestive signs or symptoms with 33% because they presented with
fever, 28% for respiratory symptoms, 14% for suspicious pneumonia, 7% before the transfer, 5%
before surgeries, and 13% in those who visited or lived in heavily hit areas, none of the patients
treated nor any HCWs tested positive for SARS-CoV2.
A study evaluated the global pharmacologic in oncology response to COVID-1969
through a survey responded by 42 practice leaders in 28 countries. PPE shortage was one of the
main issues expressed in 12(42.9%) countries. Difficulty to access anticancer medication was
also reported by 12(42.9%), especially in Africa and Europe. In regards to treatment changes in
the curative setting, clinical trial referrals were reduced in 10 (35.7%), increased use of
supportive medications were in 9(32.1%), and treatments were delayed or changed their
interval timing between cycles in 9(32.1%). For palliative care, 12(42.9%) decided to opt more in
oral SACTs, 8(28.6%) changed to less myelotoxic ChT, and 8(28.6%) decreased clinical trial
referrals. Increased use of telemedicine was seen in 13 (46.4%) for consultation with patients
24
and 15 (53.6%) for the contact between HCW, and this was less seen in African and Asian
countries, due in part to lower resources. 17(60.7%) of the surveyed countries defend that
psychological support programs should be implemented for HCW as they are more vulnerable
to adverse mental health outcomes. The changes between regions and countries were pondered
to reflect the different levels that the COVID-19 pandemic hit them.
An article selected 70 sought to evaluate the preventive measures taken by oncologists
in response to the pandemic through a survey responded by 343 oncologists in 28 countries. In
80% use, telemedicine was implemented for consultations, be it phone or video. In terms of PPE,
mainly surgical masks 90%, gloves 52%, and glasses 39% were given. Of 266 answers, 58% did
not routinely test patients, 39% did routine RT-PCR tests in select patients, and 3% on every
patient. Points that most affect treatment choices were ECOG PS score of 2 or higher (93.5%),
age (88.8%), and the presence of comorbidities (92%), mainly COPD(84.1%) and Diabetes
mellitus (63.4%). TKI and hormonal therapy were regarded as comparatively safe. At the same
time, cytotoxic ChT and ICI were deemed less safe or harmful, and responders would be more
cautious of using them along with the use of steroids. 78% were more likely to use G-CSF than
before. There was an overall therapy reduction, but it was more pronounced for second-line and
third-line ChT in metastatic cancer treatment (>70% altered) and to a lesser extent in adjuvant
(50%) and neoadjuvant (30%) settings, prioritizing curative intent. Most responders (>50%)
would use longer intervals in first-line ChT of metastatic cases, second-line ChT, and ICI and to a
lesser extent (<40%) to TKI, neoadjuvant and adjuvant therapy. Moreover, most (>50%) would
decrease the dosage in first-line ChT of metastatic cases, second-line ChT, and the rest to a lesser
extent (<40%). These alterations were not significantly different across nations. In terms of PPE,
most used face masks (89.8%) and gloves (51.9%), with some also using goggles(39.7%), N95
masks (32.4%), and surgical gowns (16.6%).
A global collaborative study71, evaluated the impact COVID-19 had on cancer care
worldwide, using survey responses by 356 centers. Clinical activity was reduced in most care
centers (88.2%), mainly as a precaution approach (55.34%) but also due to an overwhelmed
healthcare system (19.94%), shortage of PPE (19.10%), staff (17.98%), or medications (9.83) and
lockdown or travel bans (8.71%). In 46.35% of care centers, more than 10% of patients missed
at least one ChT session. Only 11.52 % reported no change in surgery activity, with most (62.08%)
being partly affected and 9.52% fully canceled during an average of 5.5 weeks. Similar results
occurred for radiation therapy, systemic therapy, and palliative care, with percentages in table
10. Only 6.74% of centers did not change outpatient visit activity, with most remaining switching
25
to virtual clinics (89.05%). Increased use of telemedicine was implemented via virtual clinics in
84.27%, be it by telephone (66.57%) or video (17.55%). Virtual tumor boards were implemented
in 77.53% of centers. In 68.26% of centers, medications were delivered to patients’ homes,
mainly hormonal therapy (79.98%) and oral ChT (67.98%). Only 16% of centers have returned to
levels before the pandemic by the time of the survey. Of the responders, 48.03% reported
COVID-19 diagnosis in a cancer inpatient setting and 46.35% in outpatient settings, lower than
those of nononcologic patients (76.40%; 70.79%) 44.38% of centers reported diagnosis in HCW.
Shortage of PPE was seen in most centers 48.32%, with masks the main PPE lacking, 48.31% in
N95 masks, and 29.21% in surgical masks. The impact was more felt in countries of lower-income
as they more often reduced activity due to resource shortage (PPE p<0.001; medications
p<0.001), had more patient missing ChT sessions p<0.001 and lacked means for the use of
telemedicine by virtual clinics p<0.001 or virtual tumor boards p<0.001, and home medication
delivery p<0.001.
A survey on how clinical activity changed as a response to COVID-19, responded by 501
clinicians of 70 countries worldwide, was assessed in a selected article72. 88.9% reported change
in their activity, which was similar across the continents p=0.26, despite being differently hit by
the pandemic. The main common reasons for activity change were presence of respiratory
comorbidities (74.7% p=020), patients age (74% p=0.33) and institutional guidelines (70.2%
p=0.056). As for significant different reasons between continents, the fear of the impact on the
health care (34.9% ) was most answered in Asia (41.5%) p=0.03, with lack of general resources
(28.3%) HCW (28.3%) and PPE (21.9%) also more responded in Asia (49.2%; 44.6% 35.4%)
p<0.001, p<0.001 and p=0.013 . The percentage of responders who had patients diagnosed with
COVID-19 and then died was 66.1% and 31.5 % in Europe, 27.8% and 8.3% in Asia, and 4.8% and
1.2 % in AUS and NZ significantly more in Europe p<0.001. Having patients diagnosed with
COVID-19 made responders more likely to change their way of practice (93% vs. 86%)p=0.03.
There was an overall decrease of 5010 outpatient visits a week by the surveyed during the
pandemic. This decrease was lower in AUS and NZ with a mean of 4 fewer patients a week,
fewer 10 in Europe, and 20 in Asia p <0.001. There was an increase in telemedicine by 11.8 times
in AUS and NZ, 7.2 in Europe, and 3.8 in Asia (in general 7.7x). The changes reported occurred in
the curative setting and palliative setting for SACT and RT, with decreased administrations,
altered intervals, delays, or even interruptions (latter only in SACT). In terms of urgent surgeries,
some reported delaying them (40%) or not performing them (12%), being both higher in the nor-
urgent setting (80%; 32%). 190 (52.6%) of HCW suffered an adverse psychological impact due to
the pandemic.

26
Discussion and Conclusions
This study aimed to understand the impact that the COVID-19 pandemic had on cancer
therapy, mainly that of high-income and developed countries and in patients with solid cancer.
It was essential to understand the impact of the infection on cancer patients, especially those
under anticancer therapy.
Cancer patient vulnerability
Overall, in the studies selected, it is seen that the prevelence of malignancy, among
COVID-19 patients, is higher than that of the overall population, and therefore, it is likely that
COVID-19 is transmitted relatively more, in patients with cancer. In the case of the studies from
China, where cancer in 2020 had a 0.28% incidence14 and a 0.64% 5-year prevelence5, CPs
encompassed 1%14 to 3%18 of infected patients with COVID-19 in the studies selected. This
tendency can be seen in studies from other countries, with cancer being present in 1%29 to
8.5%32 of overall COVID-19 cases, higher than the worldwide 5-year cancer prevalence of 0.65%.
One crucial factor seen was that of a higher rate of in-hospital infection15 than in the general
population, which may result from a potential immunosuppressed state coupled with more
regular hospital visits21.
Another point is that CPs reveal more likely than NCPs to be hospitalized due to COVID-
19, as they correspond to 4.2%21 to 23.4%26 of overall hospitalized COVID-19 cases and 40%24 to
90.9%29 of positive COVID-19 CPs are hospitalized, being higher than the 20% in NCPs4. This is
important because while the overall mortality rate in hospitalized COVID-19 cancer patients was
from 17%20 to 55%29, in some studies, like Kuderer et al33 , hospitalized cancer patients had a
case fatality rate of 23% which was not far from that of overall hospitalized patients 15-20%4.
Knowing that 50.2% of those CPs had been hospitalized33, makes its overall death rate 13%,
which is much higher than the world-wide overall COVID-19 case fatality rate of nearly 2.24%3.
This might explain why in studies like those by Brar et al25 and Shoumariyeh, K et al26,
hospitalized CPs and NCPs have similar case fatalities, while in others such as in Liang, W et al14,
Dai et al15, Tian, J et al17, Rogado et al 21 and de Azambuja E et al 32 the case fatality rate or
composite outcome, that includes death, are significantly higher in CPs than in NCPs. As for other
outcomes, cancer was associated with a significantly increased risk of severe disease or
symptom in Dai et al15 and Tian, J et al17, and in none it was associated with lower or similar risk,
being present in 34.29%15 to 64%17 of hospitalized CPs, among the articles selected. That said,
in the ICU, cancer can be used as a criterion to bar entry. For example, de Azambuja et al32 CPs

27
had fewer admissions to ICU and significantly fewer IMV use, even with them being associated
with higher mortality. While in other studies, an increased risk of being admitted to the ICU was
seen, such as in Dai et al15 and Shoumariyeh, K et al26, occurring in 8.6%32 to 41%26.
In CPs, one vital factor in ascertaining is if the anticancer treatment makes them more
susceptible to a severe form of COVID-19 and ultimately dying. Among the selected studies,
anticancer therapy had varying levels of impact. However, in most, it was associated with a
higher risk of worse outcomes14,16,18-20,24, or the patients with worse outcomes had been more
widely treated with AntiCT17, even after being adjusted for other risk factors. Significant worse
outcomes were seen when recent ChT was administered in Yang, K. et al19. It was also seen in
ICIs, for instance, in the study by Robilotti, E.V et al24. In Liang, W et al14 with recent ChT or
surgery. Finally, overall AntiCT worse outcomes were seen in Zhang, L et al16, Zhang, H. et al18,
and Liu, C. et al20 . In most studies that showed no significant risk, they still had those treated
with recent AntiCT having a higher risk24,30,33 or percentage15,27 of worse outcome, except for the
study by Brar, G et al25. Possible reasons for some of these results not being significant could be
a small population sample size25 or the fact that cancers are a heterogeneous group of diseases
with heterogeneous populations25. Regardless, the results suggest that the receipt of recent
AntiCT at diagnosis will likely be associated with a worse outcome than in other cancer patients.
Other risk factors that were identified as significant for worse outcomes in the selected studies
and as such require attention, include increased age18,20,21,24-26,30,33, being male19,30,31,33, smoking
history33, active cancer33, metastatic cancer15,17, hematological cancer24,31, tumor lung
involvement (metastatic or primary)22, patchy consolidation16 or bilateral infiltrates22 in imaging
at admission, high white blood cell count20, severe neutropenia22, a higher number of
comorbidities33, cardiovascular disorder30, hypertension30, obesity25, and CKD26.
Recommendations
The focus of this study was on general oncological care, so more broad and general
recommendations were addressed. Articles that focused solely on recommendations of one
type of procedure, one type of cancer or hematological cancers, and pediatric population were
generally excluded. There was an attempt to summarize and assemble all measures taken or
assessed in the articles selected, but some, not present in tables, were not considered.
In the recommendations, a key theme found was the balance between the risk of
exposure and infection and the risk of undertreatment and its repercussions (cancer progression
and worse prognosis)6,73 . In order to achieve this balance, it should also be regarded how the

28
region and the hospital in which the CP occupies was affected by the pandemic, mainly in the
way of supply and resource capacity, such as ICU beds, medications, PPEs, and workforce38,40.
Patient treatment was prioritized mainly in those with curative intent40. When the infection risk
outweighed potential benefits, procedures and visits were recommended to be canceled or
postponed34,36,39,40,42, such as follow-up or routine visits39,40,42,43 and in-person visits in vulnerable
patients44. Whenever possible, efforts to curtail undertreatment were incentivized, be it with
the implementation of telemedicine (by phone or video)36,37,40,42,43,45 and home visits, or
treatment courier systems47. Another crucial point in mind is maintaining the treatment offered
safe for each patient without compromising the health of other patients and HCWs. This was
especially seen in attempts to bar potential or confirmed Covid-19 CPs from outpatient setting38
and isolating those in the inpatient setting in a dedicated ward36-38, treated by HCW committed
to only their care34. To identify these patients, triaging34-39 and subsequent testing in suspicious
individuals38,43 was vital for maintaining efficient care. Other measures include limiting visitors
and caregivers present in outpatient34,39,43,45 and inpatient settings34-36, implementation of PPE,
hand hygiene35,43 and social distancing35,36 measures in patients and staff, were also essential.
In regards to specific cancer treatment, some changes were also recommended. Mostly,
systemic anticancer treatments (SACTs) such as chemotherapy or immunotherapy, when
feasible, were preferred as oral treatments instead of IV36,39, along with regiments that included
fewer visits and were less toxic36,39,40. As for surgeries, elective or non-urgent were generally
delayed34,35,37,39, and those that would have a reduced benefit in the patient’s prognosis and in
patients with stable slow-growing cancer35,45. In radiotherapy, hypofractionated regiments are
to be prefered36,39,50, and may be used as a substitute to surgery in some cases39. Cancer patients
are vulnerable to complications such as febrile neutropenia, especially as a consequence of
cytotoxic cancer treatment, so some studies advise extending the use of G-CSF to patients of
intermediate-risk or more vulnerable38 . In inpatient care, due to higher risk of thromboembolic
events in cancer that only increases with concomitant COVID-19 4,38 , prophylaxis with low
molecular weight heparin (LMWH) or direct oral anticoagulants (DOACs) have also been
advised38 .
Impact on cancer care
Of the articles selected, a large portion (10 of 24; 41.67%) comprised only Italian cancer
centers. This most likely results from Italy being one of the most hit countries during the first
stages of the pandemic, mainly in its northern regions that include Lombardy, Emilia Romagna,
and Veneto56 (called red zones). On April 1, 2020, Italy was the second country in the world with

29
the most confirmed cases (105 792, 12.8% of all cases) and the country with the most confirmed
deaths (12 430, 30.6% of all deaths)74. Overall in Italy, it was reported a decreased clinical activity
nationwide, it was seen treatment delays and fewer visits in 80% of centers, being considerable
in 20% of them, and the wide implementation of telemedicine in 80% of centers and although
most agreed that the measures were effective, CPs were still getting infected mainly in red zones 56. The surgical activity was also decreased, along with reduced hospital and ICU beds available,
outpatient clinics, and restricted imaging and invasive procedures57. Radiotherapy had
decreased activity, mainly with delays of non-urgent follow-up visits, and hypofractionated
regiments were prefered58. In immunotherapy, most CPs were screened for a possible infection
and delayed predominantly only if suspected or infected, and telemedicine was used to
substitute follow-up in those who completed or responded to therapy59.
Regarding studies of specific areas or centers in Italy, most concluded that prevention
measures were paramount in limiting the spread of infection in CPs and HCWs and maintaining
a safe treatment28,29,52,54,55. In the studies selected, most followed the nationwide trend of
treatment and visit delays or cancelations28,29,52,55, but in some, activity was able to be
maintained54 or increased 53. Montesi, G et al53, reported the activity the radiotherapy
department in Rovigo situated in the region of Verato, one of the red zone, there was rather an
increase of first visits and treatments, with none of the patients and HCW being infected during
that time. In the study by Carvatta, L et al54, its similar activity with that of 2019 can be because
the region of the center studied, Abruzzo, was one of the least hit areas. In the same study, areas
with more cases, mainly Lombardy, suffered a higher impact on cancer RT activity54.
In other European countries, it was also seen a decrease in clinical activity. With
decreased or delayed visits, mainly in follow-up50,60-62, treatment delays50,60, fewer patients in
the outpatient setting and aftercare clinics61, changes in ChT and other SACT administration
regimens62, lower RT activity62,63 with preferred hypofraction regimens62,63 and increased
implementation of telemedicine mainly in order to replace the delayed in-person visits50,60,62.
Another impact seen was that of HCW getting infected50,62 or absent due to self-isolation or
quarantine50,63.
When added studies with Nothern America centers, same trends of visit and treatment
delay64,66, including for surgeries66, and RT66, telemedicine64,67 and staff absences64,65 were seen.
However, they also mention an increase in burnout symptoms in staff members such as anxiety,
lower attention, and depression64, lower clinical trial accrual64, decreased physical exams, blood

30
samplings, radiological response evaluations67and reduced inpatients, with ChT inpatients
referred for the outpatient setting and fewer palliative inpatients67.
When finally, we look at the worldwide impact in cancer care activity due to COVID-19,
we see that it changed in similar ways. With general lower activity reported by 88.2% of
responders in the study by Jazieh, A. R. et al71 and 88.9% altered treatment regimen (alternative
treatment implementation, lower dose, delay, and interruption) in the study by Chazan, G et
al72. ChT and other SACT were delayed, mainly for metastatic cancer70, adjuvant or palliative69-72
and second or third line treatments70. Surgeries were also delayed, especially non-urgent72and
RT hypofraction was prefered72. There were increased telemedicine implementation69-72,
decreased clinical trial referrals69, an increase of psychological impact among staff69,72, as well as
the presence of resource shortages, including PPE and medications, being more felt in Africa and
Europe69 . As for differences in implementing telemedicine, it was more widely adhered to in
high-income countries, including countries in Europe, Australia, and New Zealand72, and less in
asian69,72 and African countries69, in part due to lack of resources69.
Another important point is the way anticancer treatment is conducted in positive
COVID-19 CPs. As mentioned above there is a likely association between its use and worse
outcomes, not to mention their admission could put other patients and HCWs at risk of infection.
Patient screening for potential infection were widely adhered be it by phone29,52,53,55,58,59,67 the
day before or at admission29,50,52,55,56,58,59,67 and creation of wards dedicated for COVID-19
patients, separated from other COVID-19 “clean” zones28,29,52,57,67,68, along with other prevention
and hygiene measures. That said, among the studies selected, in patients suspected of infection
or in positive cases, centers opted in delaying treatment to all until deemed safe58,59, postponed
based on risk-benefit in a case by case basis28,62 or generally maintained treatment unaltered in
a safely manner58, being the presence of symptoms28,62 and cancer stage28 major criteria in the
decision. In the study Nichetti et al29, all positive cases had their treatment postponed, and less
than half of suspect cases had their treatment delayed. In the study by Buglione, M. et al28,
almost half of the positive cases and half of the suspect cases maintained RT. Reasons for this
discrepancy include the lack of concrete evidence on the impact COVID-19 had on patients under
anticancer therapy28,59,62, as well as the type of therapy28, with RT interruptions being generally
not recommended34.
At the moment of selecting these articles, it is still unknown the magnitude in which
these delays will have in CPs’ life expectancy72, but it will likely have ramifications for years to
come. Treatment delays were not only a method to compensate a strained health care system71,

31
they were also a measure of precaution against unnecessary exposure29,71. That said, decreased
cancer therapy activity can result in an unwanted increase of more advanced and unresectable
tumors in the future, with worse prognosis61,75 followed by an increase in deaths due to cancer72
and further strains in the health care budgets72 . A study in England75, reveals that a delay of 3
to 6 months in cancer surgery can result in the loss of life years gained of 0.97 to 2.19 per patient,
being comparable to 19% to 43%, respectively, of those gained by the hospitalization of the
same number of COVID-19 cases, and 26% to 59% if adjusted for resources used, revealing likely
long-lasting repercussions in cancer care due to the pandemic. As such, treatment prioritization
was crucial in mitigating that impact75, with adjuvant and curative treatment being prioritized
over palliative treatments67.
The articles evaluated comprise mainly the early stages of the pandemic, since then the
scenery has changed dramatically, mainly through the introduction of vaccination to combat
COVID-19 and the emergence of new COVID-19 variants, that also need to be evaluated on how
they impacted cancer care, but this is beyond the scope of this article. Nevertheless, this crisis
is unique in the way that it reveals how in a worldwide emergency, high-income countries deal
with an unforeseen emergency that burdens their healthcare systems and leads to the
compromise of the care of other sectors like oncological care, which will have a lasting impact,
and how to buffer said impact in the future while maintaining the patients safe.
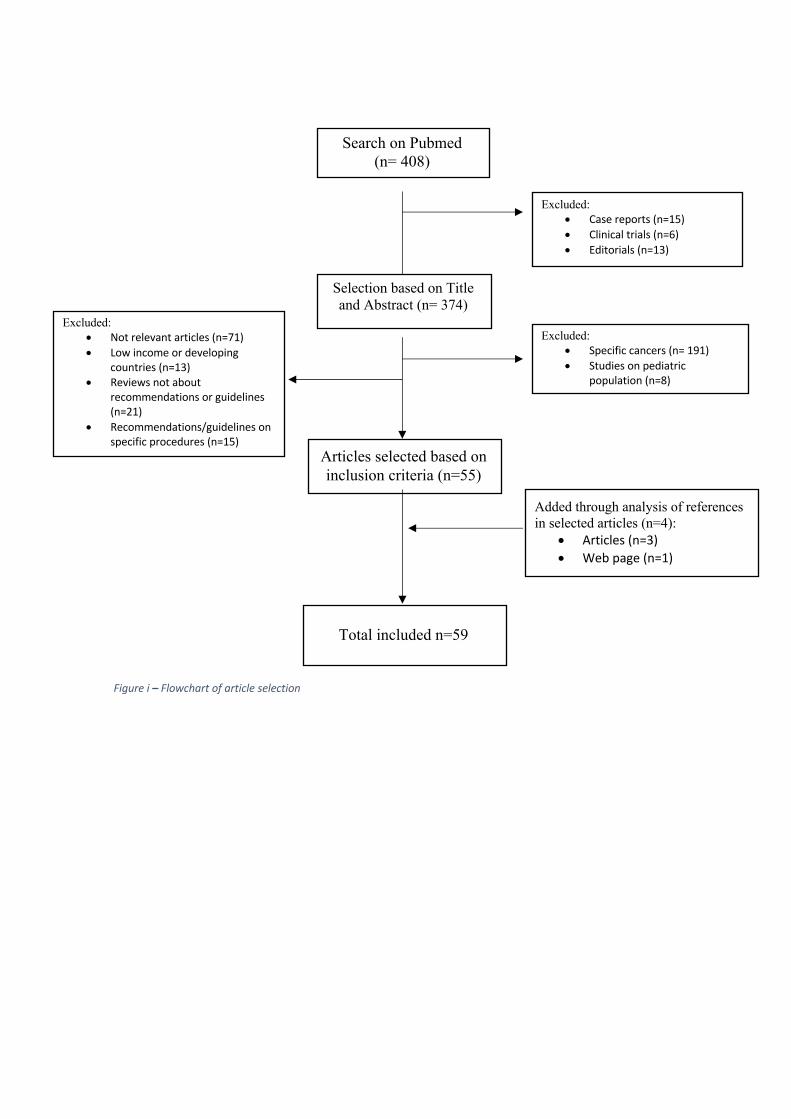
Figure i – Flowchart of article selection
Excluded: • Case reports (n=15) • Clinical trials (n=6) • Editorials (n=13)
Selection based on Title and Abstract (n= 374)
Excluded: • Specific cancers (n= 191) • Studies on pediatric
population (n=8)
Excluded: • Not relevant articles (n=71) • Low income or developing
countries (n=13) • Reviews not about
recommendations or guidelines (n=21)
• Recommendations/guidelines on specific procedures (n=15)
Articles selected based on inclusion criteria (n=55)
Added through analysis of references in selected articles (n=4):
• Articles (n=3) • Web page (n=1)
Total included n=59
Search on Pubmed (n= 408)

33
Table i- Inclusion and exclusion criteria used
Inclusion Criteria Exclusion criteriageneral cancer patients case reportsstudies analyzed the outcome of COVID-19 in cancer patients with a sample size of more than 10 patients
clinical trials
Articles focusing on recommendations for cancer care during COVID-19 pandemic
editorials
Studies that analyzed differences in activity in cancer care departments, facilities or institutions
focused on specific cancers or groups of cancers
studies that focused on pediatric populationnon- recomendation reviewRecommendations or guidelines focused on a specific procedureStudies focusing on low-income or developing countries, except China

34
Table I- Perceiving cancer patients’ vulnerability to COVID-19- Characteristics of studies selected.
1st Author Region type of study population Time period followedLiang, W Wuhan,
Chinaretrospective study
1590 records of COVID-19 patient from 575 hospitals
until January 31st 2020
Dai, M Wuhan, China
prospective, observational multicentre study
641 Covid patients from 14 hospitals: 105 cancer patients paired with 536 age matched non cancer patients
January 1, 2020, to February 24, 2020
Zhang, L Wuhan, China
retrospective case study
1276 treated for COVID-19 in 3 hospitals, 28 (2.2%) with cancer
January 13 to February 26
Tian, J Wuhan, China
multicentre, retrospective, cohort study
751 Covid patients from 9 hospitals: 232 cancer patients paired with 519 age, gender and comorbitie matched non cancer patients
January 13 to March 18
Zhang, H Wuhan, China
multicenter retrospective observational study
3559 hospitalized patients with COVID-19 in 5 hospitals, 107(3%) with cancer
January 5 to March 18
Yang, K Hubei, China
retrospective, cohort study
205(2.5%) cancer patients among 8161 COVID-19 patients admitted in 9 hospitals
January 13 to March 18
Liu, C China multicenter retrospective cohort study
207 solid cancer patients with COVID-19 admitted in 32 hospitals
December 17, 2020, and March 18
Rogado Madrid, Spain
retrospective study
1069 cancer patient records who were admited in an hospital oncological department during this period
February 1 to April 7, 2020
Yarza, R Madrid, Spain
retrospective study
63 cancer patients undergoing active treatment admited due to COVID-19
March 9 to April 19
Miyashita, H
NY, USA retrospective study
electronic medical records of Mount Sinai Health System (MSHS) of 5688 patients with COVID-19
March 1 to of April 6
Robilotti, E.V.
NY, USA retrospective cohort study
423 cases of symptomatic COVID-19 cancer patients diagnosed at Memorial Sloan Kettering Cancer Center
March 10 to April 7, 2020
Brar, G NY, USA retrospective observational cohort study
585 patients COVID-19 patients admitted two New York–Presbyterian (NYP) hospitals: 117 with active malignancy matched with 468 non cancer patients based on age, sex and comorbidities
March 3 to May 15, 2020
Shoumariyeh, K
Germany retrospective single center cohort study
39 (23.4%) cancer patients with COVID-19 among a total of 167 COVID-19 patients hospitalized at the University Hospital Freiburg
February 27 to April 10
Garrone, O Italy retrospective/prospective observational study
21(3.1%) COVID-19 patients among the 675 cancer patients that were referred to a medical oncology unit at the general hospital of Piedmont region in nothern Italy for cosultation or therapy
mid-March to April 23
Buglione, M Lombardy, Italy
retrospective study
Brescia University Radiation Oncology Department were 402 cancer patients were undergoing active anticancer therapy
February 24 to April 24
Nichetti, F Milan, Italy observational study
1081 cancer patients treated with antiancer therapy in outpatient and inpatient setting in the COVINT study
February 16 and April 10 of 2019 and 2020
Lee, L. Y. UK prospective cohort study
800 patients with a diagnosis of cancer and symptomatic COVID-19
March 18 to April 26, 2020
Lee, L.Y.W. UK prospective cohort study
1044 adult patients in the UK Coronavirus Cancer Monitoring Project (UKCCMP) with active cancer and infected with SARS-CoV2 or with COVID-19; UK’s cancer population data of 2017 was used as contro
March 18 to May 8, 2020
Azambuja, E
Belgium population-based nationwide cohort study
10486 hospitalized adult COVID-19 patients, 892 with solid cancer, 9594 without cancer
until May 24th
Kuderer NM USA, Canada and Spain (CCC19)
retrospective cohort study
928 patients with active or history of cancer infected with SARS-CoV-2, in the CCC19 database
March 17 to April 16, 2020
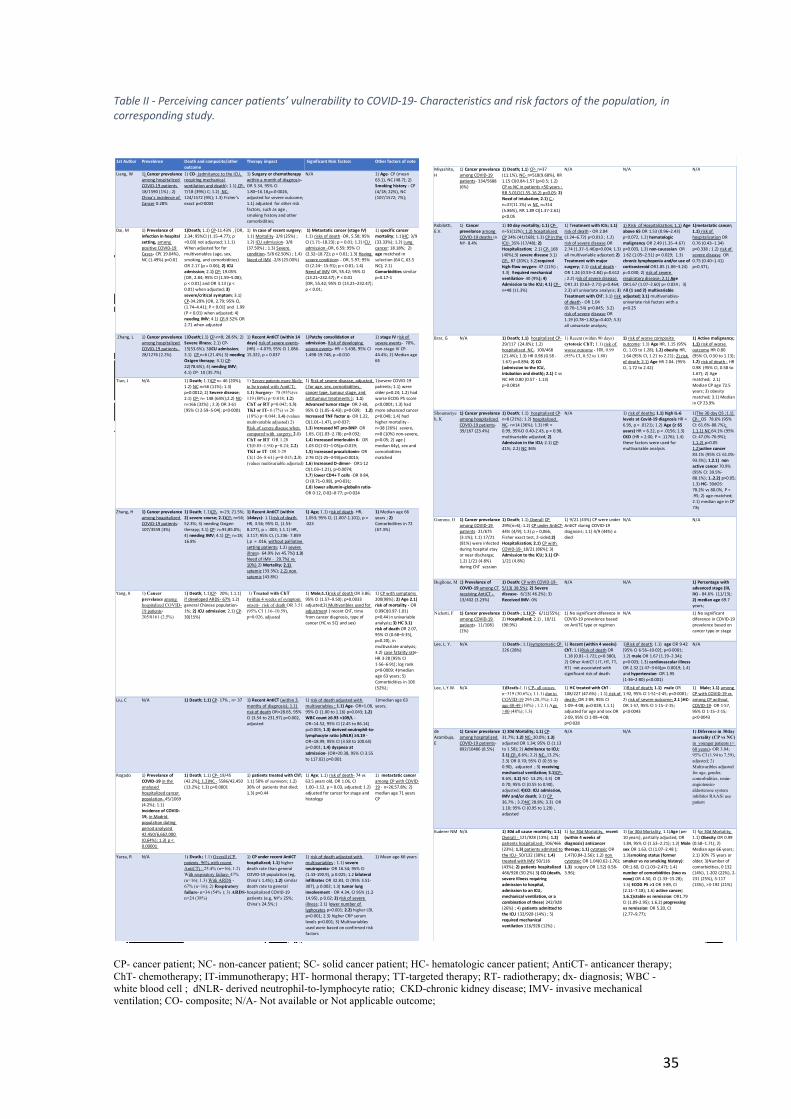
35
Table II - Perceiving cancer patients’ vulnerability to COVID-19- Characteristics and risk factors of the population, in corresponding study.
CP- cancer patient; NC- non-cancer patient; SC- solid cancer patient; HC- hematologic cancer patient; AntiCT- anticancer therapy; ChT- chemotherapy; IT-immunotherapy; HT- hormonal therapy; TT-targeted therapy; RT- radiotherapy; dx- diagnosis; WBC - white blood cell ; dNLR- derived neutrophil-to-lymphocyte ratio; CKD-chronic kidney disease; IMV- invasive mechanical ventilation; CO- composite; N/A- Not available or Not applicable outcome;
Miyashita, H
1) Cancer prevelance among COVID-19 patients- 334/5688 (6%)
1) Death; 1.1) CP- n=37 (11.1%), NC- n=518(9.68%), RR 1.15 CI(0.84-1.57 )p>0.5; 1.2) CP vs NC in patients <50 years : RR 5.01CI(1.55-16.2) p<0.05; 2) Need of intubation; 2.1) C -n=37(11.1%) vs NC n=314 (5.86%), RR 1.89 CI(1.37-2.61) p<0.05
N/A N/A N/A
Robilotti, E.V.
1) Cancer prevelance among COVID-19 deaths in NY- 8.4%
1) 30 day mortality; 1.1) CP- n=51(12%); 1.2) hospitalized CP 24% (41/168); 1.3) CP in the ICU- 35% (17/48); 2) Hospitalization; 2.1) CP- 168 (40%);3) severe disease 3.1) CP- 87 (20%); 3.2)required high-flow oxygen- 47 (11%) ; 3.3) Required mechanical ventilation- 40 (9%); 4) Admission to the ICU; 4.1) CP- n=48 (11.3%)
1) Treatment with ICIs; 1.1) risk of death - OR 2.84 (1.24–6.72) p=0.013 ; 1.2) risk of severe disease OR 2.74 (1.37–5.46)p=0.004; 1.3) all multivariable adjusted; 2) Treatment with major surgery; 2.1) risk of death - OR 1.24 (0.53–2.84) p=0.612 ; 2.2) risk of severe disease OR1.31 (0.63–2.71) p=0.464; 2.3) all univariate analysis; 3) Treatment with ChT; 3.1) risk of death - OR 1.04 (0.70–1.54) p=0.845; 3.2) risk of severe disease OR 1.19 (0.78–1.82)p=0.407; 3.3) all univariate analysis;
1) Risk of Hospitalization; 1.1) Age above 65 OR 1.53 (0.96–2.43) p=0.072, 1.2) hematologic malignancy OR 2.49 (1.35–4.67) p=0.003, 1.3) non-caucasian OR 1.62 (1.05–2.51) p= 0.029; 1.3) chronic lymphopenia and/or use of corticosteroid OR1.85 (1.06–3.24) p=0.030; 2) risk of severe respiratory disease; 2.1) Age OR1.67 (1.07–2.60) p= 0.024 ; 3) All (1 and 2) multivariable adjusted; 3.1) multivariables- univariate risk factors with a p<0.25
1)metastatic cancer; 1.1) risk of hospitalization OR 0.76 (0.43–1.34) p=0.338 ; 1.2) risk of severe disease OR 0.75 (0.40–1.41) p=0.371;
Brar, G N/A 1) Death; 1.1) hospitalized CP-29/117 (24.8%); 1.2) hospitalized NC- 100/468 (21.4%); 1.3) HR 0.98 (0.58 - 1.67) p=0.894; 2) CO (admission to the ICU, intubation and death); 2.1) C vs NC HR 0.80 (0.57 - 1.13) p=0.0814
1) Recent (within 90 days) cytotoxic ChT; 1.1) risk of worse outcome - HR, 0.99 (95% CI, 0.52 to 1.88)
1) risk of worse composite outcome: 1.1) Age HR, 1.15 (95% CI, 1.03 to 1.28); 1.2) obesity HR, 1.64 (95% CI, 1.21 to 2.21); 2) risk of death; 2.1) Age HR 2.04. (95% CI, 1.72 to 2.42)
1) Active malignancy; 1.1) risk of worse outcome HR 0.80 (95% CI, 0.50 to 1.13); 1.2) risk of death - HR 0.98 (95% CI, 0.58 to 1.67); 2) Age matched; 2.1) Median CP age 72.5 years; 3) obesity matched; 3.1) Median in CP 23.9%
Shoumariyeh, K
1) Cancer prevelance among hoapitalized COVID-19 patients- 39/167 (23.4%)
1) Death; 1.1) hospitalized CP- n=8 (21%); 1.2) hospitalized NC- n=14 (36%); 1.3) HR = 0.99, 95%CI 0.40-2.43, p = 0.98, multivariable adjusted; 2) Admission in the ICU; 2.1) CP- 41%; 2.2) NC 36%
N/A 1) risk of deaths; 1.1) high IL-6 levels at Covid-19 diagnosis HR = 6.95, p = .0121); 1.2) Age (≥ 65 years) HR = 6.22, p = .0156; 1.3) CKD (HR = 2.00, P = .1176); 1.4) these factors were used for multivariable analysis
1)The 30 day OS ;1.1) CP- OS 78.6% (95% CI: 61.6%-88.7%); 1.1.1) NC 64.1% (95% CI: 47.0%-76.9%); 1.1.2) p>0.05 1.2)active cancer 83.1% (95% CI: 61.0%-93.3%); 1.2.1) non active cancer 70.9% (95% CI: 39.5%-88.1%); 1..2.2) p>0.05; 1.3) HC- 30dOS: 78.2% vs 80.0%, P = .95; 2) age-matched; 2.1) median age in CP 73y
Garrone, O 1) Cancer prevelance among COVID-19 patients- 21/675 (3.1%); 1.1) 17/21 (81%) were infected during hospital stay or near discharge; 1.2) 1/21 (4.8%) during ChT session
1) Death; 1.1) Overall CP 29%(n=6); 1.2) CP under AntiCT- 44% (4/9); 1.3) p = 0,066, Fisher exact test, 2-sided;2) Hospitalization; 2.1) CP with COVID-19- 18/21 (86%); 3) Admission to the ICU; 3.1) CP- 1/21 (4.8%)
1) 9/21 (43%) CP were under AntiCT during COVID-19 diagnosis; 1.1) 4/9 (44%) o died
N/A N/A
Buglione, M 1) Prevelance of COVID-19 among CT receiving AntiCT - 13/402 (3.23%)
1) Death: CP with COVID-19- 5/13( 38.5%); 2) Severe disease- 6/13( 46.2%); 3) Received IMV- 0%
N/A N/A 1) Percentage with advanced stage (III, IV) - 84.6% (11/13); 2) median age 69.7 years;
Nichetti, F 1) Cancer prevelance among COVID-19 patients- 11/1081 (1%)
1) Death-; 1.1)CP- 6/11(55%); 2) Hospitalized; 2.1) , 10/11 (90.9%)
1) No significant diference in COVID-19 prevelence based on AntiTC type or regimen
N/A 1) No significant diference in COVID-19 prevelence based on cancer type or stage
Lee, L. Y. N/A 1) Death-; 1.1)symptomatic CP - 226 (28%)
1) Recent (within 4 weeks) ChT; 1.1)Risk of death OR 1.18 [0.81–1.72]; p=0·380), 2) Other AntiCT ( IT, HT, TT, RT) not associated with significant risk of death
1)Risk of death; 1.1) age OR 9·42 [95% CI 6·56–10·02]; p<0·0001; 1.2) male OR 1.67 (1.19–2.34); p=0·003; 1.3) cardiovascular illness OR 2.32 [1·47–3·64]p= 0.0019; 1.4) and hypertension- OR 1.95 (1·36–2·80) p<0.001)
N/A
Lee, L.Y.W. N/A 1)Death-1.1) CP- all causes n=319 (30.6%); 1.1.1) due to COVID-19 295 (28,3%); 1.2) age 40-49 (10%) ; 1.2.1) Age >80 (48%); 1.3)
1) HC treated with ChT - 108/227 (47.6%) ; 1.1) risk of death- OR 2·09, 95% CI 1·09–4·08; p=0·028; 1.1.1) adjusted for age and sex OR 2·09, 95% CI 1·09–4·08; p=0·028
1)Risk of death; 1.1) male OR 1.92, 95% CI 1·51–2·45; p<0·0001; 2) risk of severe outcome; 2.1 )HC- OR 1·57, 95% CI 1·15–2·15; p<0·0043
1) Male; 1.1) among CP with COVID-19 vs among CP without COVID-19- OR 1·57, 95% CI 1·15–2·15; p<0·0043
de Azambuja, E
1) Cancer prevelance among hospitalized COVID-19 patients- 892/10486 (8.5%)
1) 30d Mortality; 1.1) CP- 31.7%; 1.2) NC- 20.0%; 1.3) adjusted OR 1.34; 95% CI (1.13 to 1.58); 2) Admitance to ICU; 2.1) CP- 8.6%; 2.2) NC- 13.2%; 2.3) OR 0.70; 95% CI (0.55 to 0.90), adjusted ; 3) receiving mechanical ventilation; 3.1)CP- 8.6%; 3.2) NC- 13.2%; 3.3) OR 0.70; 95% CI (0.55 to 0.90), adjusted; 4)CO: ICU admission, IMV and/or death; 3.1) CP 36.7% ; 3.2)NC 28.8%; 3.3) OR 1.10; 95% CI (0.95 to 1.29) , adjusted
N/A N/A 1) Diference in 30day mortality (CP vs NC) in younger patients (< 60 years)- OR 3.84; 95% CI (1.94 to 7.59), adjusted; 2) Multivaribles adjusted for age, gender, comorbidities, renin-angiotensin-aldosterone system inhibitor RAASi use patient
Kuderer NM N/A 1) 30d all cause mortality; 1.1) Overall - 121/928 (13%); 1.2) patients hospitalized- 106/466 (23%); 1.3) patients admited to the ICU- 50/132 (38%); 1.4) treated with IMV 50/116 (43%); 2) patients hospitalized 466/928 (50.2%) 3) CO (death, severe illness requiring admission to hospital, admission to an ICU, mechanical ventilation, or a combination of these) 242/928 (26%) ; 4) patients admitted to the ICU 132/928 (14%) ; 5) required mechanical ventilation 116/928 (12%) ;
1) for 30d Mortality, recent (within 4 weeks of diagnosis) anticancer therapy; 1.1) cytotoxic OR 1.47(0.84-2.56); 1.2) non cytotoxic OR 1.04(0.62-1.76); 1.3) surgery OR 1.52( 0.58-3.96);
1) for 30d Mortality 1.1)Age (per 10 years), partially adjusted, OR 1.84, 95% CI (1.53–2.21); 1.2) Male sex OR 1.63, CI (1.07–2.48 ); 1.3)smoking status (former smoker vs no smoking history): OR:1.60, CI (1.03–2.47); 1.4) number of comorbidities (two vs none) OR 4.50, CI (1.33–15.28); 1.5) ECOG PS >1 OR 3·89, CI (2.11–7.18); 1.6) active cancer; 1.6.1)stable vs remission: OR1.79 CI (1.09-2.95); 1.6.2) progressing vs remission: OR 5.20, CI (2.77–9.77);
1) for 30d Mortality; 1.1) Obesity OR 0.99 (0.58–1.71); 2) Median age 66 years; 2.1) 30% 75 years or older; 3)Number of comorbidities, 0 132 (14%), 1-202 (22%), 2-231 (25%), 3-117 (13%), >3-192 (21%)
1st Author Prevelence Death and composite/other
outcome
Therapy impact Significant Risk factors Other factors of note
Liang, W 1) Cancer prevelance
among hospitalized
COVID-19 patients
18/1590 (1%) ; 2)
China's incidence of
Cancer 0.28%
1) CO- (admitance to the ICU,
requiring mechanical
ventilation and death); 1.1) CP-
7/18 (39%) C; 1.2) NC-
124/1572 (9%); 1.3) Fisher’s
exact p=0·0003
1) Surgery or chemotherapy
within a month of diagnosis-
OR 5.34, 95% CI
1.80–16.18,p=0·0026,
adjusted for severe outcome;
1.1) adjusted for other risk
factors, such as age ,
smoking history and other
comorbidities;
N/A 1) Age- CP (mean
63.1), NC (48.7); 2)
Smoking history - CP
(4/18; 22%), NC
(107/1572; 7%);
Dai, M 1) Prevelance of
infection in hospital
setting, among
positive COVID-19
Cases- CP( 19.04%),
NC (1.49%) p<0.01
1)Death; 1.1) CP-11.43% , [OR,
2.34; 95%CI (1.15–4.77); p
=0.03] not adjusted; 1.1.1)
When adjusted for for
multivariables (age, sex,
smoking, and comorbidities)
OR 2.17 (p = 0.06); 2) ICU
admission; 2.1) CP- 19.05%
[OR, 2.84; 95% CI (1.59–5.08);
p < 0.01] and OR 3.13 (p <
0.01) when adjusted; 3)
severe/critical symptom; 3.1)
CP-34.29% [OR, 2.79; 95% CI,
(1.74–4.41); P < 0.01] and 1.99
(P < 0.01) when adjusted; 4)
needing IMV; 4.1) CP-9.52% OR
2.71 when adjusted
1) In case of recent surgery;
1.1) Mortality- 2/8 (25%) ;
1.2) ICU admission- 3/8
(37.50%) ; 1.3) Severe
condition- 5/8 62.50%) ; 1.4)
Need of IMV -2/8 (25.00%)
1) Metastatic cancer (stage IV)
1.1) risks of death -OR, 5.58; 95%
CI (1.71–18.23); p = 0.01; 1.2) ICU
admission -OR, 6.59; 95% CI
(2.32–18.72); p < 0.01; 1.3) Having
severe conditions - OR, 5.97; 95%
CI (2.24– 15.91); p < 0.01; 1.4)
Need of IMV OR, 55.42; 95% CI
(13.21–232.47); P < 0.01
[OR, 55.42; 95% CI (13.21–232.47);
p < 0.01;
1) specific cancer
mortality; 1.1)HC: 3/9
(33.33%); 1.2) Lung
cancer: 18.18%; 2)
age matched in
selection (64 C, 63.5
NC); 2.1)
Comorbidities similar
p=0.17-1
Zhang, L 1) Cancer prevelance
among hospitalized
COVID-19 patients-
28/1276 (2.2%)
1)Death;1.1) CP-n=8; 28.6%; 2)
Severe illness; 2.1) CP-
15(53.6%); 3)ICU admission;
3.1) CP n=6 (21.4%) 3) needing
Oxigen therapy; 3.1) CP-
22(78.6%); 4) needing IMV;
4.1) CP- 10 (35.7%)
1) Recent AntiCT (within 14
days) risk of severe events-
(HR) = 4.079, 95% CI 1.086-
15.322, p = 0.037
1)Patchy consolidation at
admission- Risk of developing
severe events- HR = 5.438, 95% CI
1.498-19.748, p =0.010
1) stage IV risk of
severe events- 70%,
non-stage IV CP-
44.4%; 2) Median age
65
Tian, J N/A 1) Death; 1.1)CP n= 46 (20%);
1.2) NC n=56 (11%); 1.3)
p=0.0012; 2) Severe disease;
2.1) CP- n= 148 (64%);2.2) NC-
n=166 (32%) ; 2.3) OR 3·61
[95% CI 2·59–5·04]; p<0·0001
1) Severe patients more likely to be treated with AntiCT; 1.1) Surgery- 78 (93%)vs 119 (80%) p=0.018; 1.2) ChT or RT p=0.042; 1.3) TKI or IT- 6 (7%) vs 26 (18%) p=0.044; 1.4) (values multivariable adjusted) 2) Risk of severe disease when compared with surgery; 2.1) ChT or RT OR 1.28 CI(0.85–1.94) p=0.24; 2.2) TKI or IT OR 3·29 CI(1·26–8·61) p=0·015; 2.3) (values multivariable adjusted)
1) Risk of severe disease, adjusted
( for age, sex, comorbidities,
cancer type, tumour stage, and
antitumour treatments ); 1.1)
Advanced tumor stage- OR 2·60,
95% CI (1.05–6.43); p=0·039; 1.2)
Increased TNF factor α- OR 1.22,
CI(1.01–1.47), p=0·037;
1.3) Increased NT pro-BNP- OR
1.65, CI(1.03–2.78); p=0·032;
1.4) Increased interleukin 6- OR
1.03 CI(1·01–1·05)p=0.019;
1.5) Increased procalcitonin- OR
2·76 CI(1·25–3·93)p=0.0015;
1.6) Increased D-dimer- OR1·12
CI(1.03–1.21), p=0.0074;
1.7) lower CD4+ T cells -OR 0·84,
CI (0.71–0.98), p=0·031;
1.8) lower albumin–globulin ratio-
OR 0·12, 0·02–0·77; p=0·024
1)severe COVID-19
patients; 1.1) were
older p=0.24; 1.2) had
worse ECOG PS score
p<0.0001; 1.3) had
more advanced cancer
p=0.048; 1.4) had
higher mortality -
n=38 (26%) severe,
n=8 (10%) non-severe,
p<0.05; 2) age (
median 64y), sex and
comorbidities
matched
Zhang, H 1) Cancer prevelance
among hoapitalized
COVID-19 patients-
107/3559 (3%)
1) Death; 1.1)CP- n=23; 21.5%;
2) severe course; 2.1)CP- n=56;
52.3%; 3) needing Oxigen
therapy; 3.1) CP- n=91;85.0%;
4) needing IMV; 4.1) CP- n=18;
16.8%
1) Recent AntiCT (within
14days)- 1.1)risk of death
HR, 3.56; 95% CI, (1.53-
8.277), p = .003; 1.1.1) HR,
3.117; 95% CI, (1.236- 7.859
),p = .016, without palliative
setting patients; 1.2) severe
illness- 64.9% (vs 45.7%) 1.3)
Need of IMV - 29.7%( vs
10%) 2) Mortality; 2.1)
sytemic (33.3%); 2.2) non
sytemic (43.8%)
1) Age; 1.1) risk of death- HR,
1.053; 95% CI, (1.007-1.101), p =
.023
1) Median age 66
years ; 2)
Comorbidities in 72
(67.3%)
Yang, K 1) Cancer prevelance among hoapitalized COVID-19 patients- 205/8161 (2.5%)
1) Death; 1.1)CP- 20%; 1.1.1)
if developed ARDS- 67% 1.2)
general Chinese population-
1%; 2) ICU admission; 2.1) CP-
30(15%)
1) Treated with ChT (within 4 weeks of symptom onset)- risk of death OR 3.51 (95% CI 1.16–10.59), p=0.026, adjusted
1) Male;1.1)risk of death OR 3.86;
95% CI (1.57–9.50); p=0.0033
adjusted;2) Multivaribles used for
adjustment ( recent ChT, time
from cancer diagnosis, type of
cancer (HC vs SC) and sex)
1) CP with symptoms
200(98%); 2) Age 2.1)
risk of mortality - OR
0.99CI(0.97-1.01)
p=0.44 in univariable
analysis; 3) HC 3.1)
risk of death OR 2.07,
95% CI (0.68–6·35),
p=0.20), in
multivariate analysis;
3.2) case fatality rate-
HR 3·28 [95% CI
1·56–6·91]; log rank
p=0·0009; 4)median
age 63 years; 5)
Comorbidities in 106
(52%);
Liu, C N/A 1) Death; 1.1) CP- 17% , n= 37 1) Recent AntiCT (within 3
months of diagnosis); 1.1)
risk of death OR=28.65, 95%
CI (3.54 to 231.97) p=0.002,
adjusted
1) risk of death adjusted with
multivariables ; 1.1) Age- OR=1.08,
95% CI (1.00 to 1.16) p=0.043; 1.2)
WBC count ≥6.93 ×109/L -
OR=14.52, 95% CI (2.45 to 86.14)
p=0.003; 1.3) derived neutrophil-to-
lymphocyte ratio (dNLR) ≥4.19 -
OR=18.99, 95% CI (3.58 to 100.65)
p=0.001; 1.4) dyspnea at
admission- (OR=20.38, 95% CI 3.55
to 117.02) p=0.001
1)median age 63
years;
Rogado 1) Prevelance of
COVID-19 in the
analysed
hospitalized cancer
population- 45/1069
(4.2%); 1.1)
Incidence of COVID-
19, in Madrid
population duting
period analysed
42,450/6,662,000
(0,64%); 1.3) p <
0.00001
1) Death; 1.1) CP- 19/45
(42.2%); 1.2)NC - 5586/42,450
(13.2%); 1.3) p=0.0001
1) patients treated with ChT;
1.1) 50% of survivors; 1.2)
36% of patients that died;
1.3) p=0.44
1) Age; 1.1) risk of death- 74 vs
63.5 years old, OR 1.06, CI
1.00–1.12, p = 0.03, adjusted; 1.2)
adjusted for cancer for stage and
histology
1) metastatic cancer
among CP with COVID-
19 - n=26;57.8%; 2)
median age 71 years
CP
Yarza, R N/A 1) Death; 1.1) Overall (CP patients, 96% with recent AntiCT) - 25.4% (n=16); 1.2) With respiratory failure- 47% (n=16); 1.3) With ARDS - 67% (n=16); 2) Respiratory failure- n=34 (54% ); 3) ARDS- n=24 (38%)
1) CP under recent AntiCT
hospitalized; 1.1) higher
death rate than general
COVID-19 population (eg,
China's 1.4%); 1.2) similar
death rate to general
hospitalized COVID-19
patients (e.g, NY's 25%;
China's 24.5%; )
1) risk of death adjusted with
multivariables ; 1.1) severe
neutropenia- OR 16.54; 95% CI
(1.43-190.9), p 0.025; 1.2 bilateral
infiltrates OR 32.83, CI (95% 3.51-
307), p 0.002; 1.3) tumor lung
involvement - OR 4.34, CI 95% (1.2-
14.95), p 0.02; 2) risk of severe
illness; 2.1) lower number of
lyphocytes p=0.001; 2.2) higher LDL
p<0.001; 2.3) higher CRP serum
levels p<0.001; 3) Multivariables
used were based on confirmed risk
factors
1) Mean age 66 years

36
Table III- Initial management recommendations - Resource allocation
Measure tag Intervention RefencesResource Allocation (R)
R1 The interruption to cancer treatment should be as low as possible, specially to patients treated with curative intent
34;35;36;37;
R2 Recommended defer/delay elective surgery and non-urgent outpatient visits, specialy in increased workload and resource shortage cenarios
34;35;
R3 In drug shortage cenario: 34;R3.1 Connect with other sites/ health systems 34;R3.1.1 Shift drug inventory between other institutions 34;R3.2 Search for alternate treatments 34;R3.3 Develop a patient priorization criteria 34;R4 Adapt treatment prioritization and care intensity
according to:R4.1 Pandemic scenario ( e.g., a cording to European Center fo
Disease Prevention and Control (ECDC) 1 to 4)38;
R4.2 local R0 index 38;R4.3 health care facilities capacity (e.g., ICU ventilation
capacity)38;
R4.4 Priority/urgency level of treatment (which should be established)
38; 39;
R4.5 Resources available (e.g, Medication; workforce ; PPE)
38;40;
R4.5.1 If there are no shortage of resources, therapies that cannot be postponed should be promptly adressed and the remainder delayed for at least 3 months and resheduled as quick as possible.
38;
R4.5.2 if exhausted: only promptly adress emergencies 38; 40;R5 All patients patients should be stratified acording to
their risk if infected36;
R5.1 Consider deferring patients at "high risk" (e.g, cardiovascular comorbidities)
35;
R6 Hospital policy on use of critical resources (e.g. ICU beds, ventilators) should be determined upfront
36;37;42;
R7 Patients admission to the ICU, depends on: 38;R7.1 ICU resource strain 38;R7.2 R0 index and ECDC pandemic scenario 38;R7.3 Ethics 37;38;R7.3.1 Increased survival for patients with reasonable life expectancy is the main priority38;R7.3.2 Need to balance need of patient tranfer with prognosis 37;38;42;R7.3.2.1 Disease (e,g,. Location/type of tumor) 38;R7.3.2.2 Cancer Stage 38;42;R7.3.2.3 Treatment intent 38;R7.3.2.4 Life expectancy 38;42;R7.3.2.5 comorbidities present 37;R8 Goals of care and advance directives should be
discussed with all patients and recorded (reducing unneded inpatient admissions and transfers to the ICU)
36;39;45;
R8.1 also discuss likely prognosis 42;R9 Treatment Priorization should follow principals of
Survival, Beneficence and Justice42;
R10 treatment intent (curative or palliative) is an important factor in treatment prioritization
40;
R10.1 In general, focus of resources should be in patients with curative intent
36;42;
R10.2 symptomatic patients in palliative setting should still be cared for36;R11 In case of limited operating room or ICU capacity,
focus should be on neoadjuvant therapies and curative surgeries
39;
R12 A Hospital-wide crisis team should be formed to organize and coordinate measures between departments
39;
R13 Allocation of ample resources, crucial for cancer treatment, should be maintained37;42;R14 Treatment of emergencies should always be guaranteed 47;48;

37
Table III.1- Initial management recommendations – ESMO cancer patient prioritization (removed from https://www.esmo.org/guidelines/cancer-patient-management-during-the-covid-19-pandemic. Accessed 21/04/2021.)
Priority level Characteristic for selection
High
Patient's condition is immediately life threatening, clinically unstable, and/or the magnitude of benefit qualifies the intervention as high priority (e.g. significant overall survival [OS] gain and/or substantial improvement in quality of life [QoL]);
Medium
Patient's situation is non-critical but delay beyond 6 weeks could potentially impact overall outcome and/or the magnitude of benefit qualifies for intermediate priority;
Low
Patient's condition is stable enough that services can be delayed for the duration of the COVID-19 pandemic and/or the intervention is non-priority based on the magnitude of benefit (e.g. no survival gain with no change nor reduced QoL).

38
Table IV- Initial management recommendations- Outpatient setting
Measure tag Intervention RefencesOutpatient clinics (O)O1 Reduce/cancel non-urgent outpatient visits,
without compromising patient care 34; 36;39;40;42;
O1.1Delay when feasible, routine and follow-up visits 39;40;42;43;
O1.1.1when possible substitute to remotely (e.g,phone call or telemedicine)
36; 37; 40; 42; 43; 45;
O1.1.1.1 Specialy in those receiving oral SACT 40;O1.2 Delay/cancel non-urgent surgeries 39;
O1.2.1and surgeries with associated high morbidity and mortality 39;
O1.3
Consider alternative therapies, mainly with associated with fewer visits and that has similar effectiveness 42;
O1.4
Consider postponing maintenance/adjuvant systemic anticancer treatment of advanced cancer 48;
O1.5
It is not recoomended in person visits in at risk patients, like older patients (e.g, >70 years) 44;
O2 Educate/ communicate to patients 34; 37; 42;O2.1 hygiene measures (e.g. hand washing) 34; 37;
O2.2Infection control measures (e.g. social distance, use of mask) 34;
O2.3 Signs and symptoms of COVID-19 34;
O2.4 Ways of exposure and travel destinations of high risk 34;
O2.5Report in case of suspicious symptom onset
34;O2.6 How to act in case of symptoms 42;O2.7 Their potencial increased vunerability to 42;
O2.7.1exposure/infection due to anticancer treatment 39;
O2.7.2treatment changes due to pandemic impact to healthcare 42;
O3Limit visitors/careguivers present (e,g, one;none) 34;39; 43; 45;
O4Limit entry/exit points for patients and HCW 34; 45;
O4.1 Should be diferent point for each group 42;45;
O5
Screening/triaging should be employed, to detect potencial COVID-19 infected patients, before visit
34; 35; 36; 37; 38;39; 42;45;46;
O5.0.1 (including home visits) 47;
O5.1 by phone (e.g., a day before) 34;35;36;37;39;42
;43;47;
O5.2at the hospital/clinic before entry 34;35;36;37;38;39
;48;O5.3 Based on:O5.3.1 Travel history 34; 36;38;45;O5.3.2 contact history 34; 36; 38; 43;45;
O5.3.3symptoms (e.g,Fever (>37.5ºC) or Respiratory symptoms)
34;36;38;39;42;43;45;48;
O5.3.4 Procedure/treatment planned 38;
O5.3.5Presence of relatives/cohabiters in sharing same livining space 47;
O5.3.6 other
O5.4Consider testing anyone suspicious, mainly those with COVID-like symptoms 38;43;
O5.4.1 Bar entry to suspicious cases 38;
O5.4.2If feasible, only allow patients wih negative tests to enter 38;
O5.5 Patients with suspicious symptoms should be evaluated according to their risk if infected, and then triaged at: 42;
O5.5.1 General COVID-19 clinic 42;O5.5.2 Specialized clinic for patients at high risk 42;O5.6 Consider to delay treatment in suspicious
patients, until deemed safe 35; 39;O5.6.1 Until disapearence of symptoms and
radiological signs and/or a negative RT-PCR test 37;49;
O5.7 Isolate patients that meet criteria of highly communicable disease, such as COVID-19
34;39;46;O5.8 Suspicious patients, mainly those with
symptoms, are advised not to go to the clinic and should follow isolation/quarantine measures 39;
O5.9 If resources available, consider implementing a RT-PCR test to all patients in active treatment (e.g.,48h before each treatment cycle) 38; 40;
O5.9.1 In case of testing shortage test at least everyone undergoing chemotherapy 38;
O5.10 In case of positive COVID-19 in oncological patients 43;
O5.10.1 If mild disease, should be isolated and may be treated in: 43;
O5.10.1.1 community care 43;O5.10.1.2 at home if in palliative/supportive care 43;O5.10.2 Admission to specific COVID-19 care unit 37;40;43;O5.10.2.1 Or inpatient transfer 40;
O6 In Chemotherapy infusion/ other SACT avoid treatment delays, as much as possible 34;
O6.1 Consider delay, especialy adjuvant and in stable/slow progressing tumors 40;
O6.2Consider switching to aceptable oral therapy
34; 36; 39; 40;46; 48;
O6.2.1also consider oral substitutes for other systemic anticancer treatments 36; 39;42;
O6.2.2Subcutaneous treatment can also be an option 39;
O6.3Prefer infusion facilities near patient's home 36; 46;
O6.3.1 If feasible, consider home infusion 34;O6.4 If feasible, use longer regiments with
longer intervals and less visits 36; 39; 42; 48;O6.4.1 reduce total duration 36; 39;O6.5 Prefer use of less toxic (e.g., cytotoxic)
regimes if they are as effective 36; 39; O6.5.1 Consider monotherapy 39;O6.6 Lower doses can be considered if feasible
and necessary to avoid severe myelotoxicity46;
O6.7 Recommended reducing combination with immunotherapy (associated with higher rate of admissions) 42;
O6.8 Consider use of oral premeditations to shorten the stay in the clinic, such as antiemetics, steroids or antihistamines 42;
O6.9 Delay when feasible, non-essential scans/lab work and routine follow-ups 42;
O7 In case of oral chemotherapy reduce visits to safest minimum
34; 40;
O7.1Consider treatent breaks or holidays (case-by-case basis) 34;36;
O7.2Consider implementing a drive-through facility for drug collection 34;
O8
Consider use of hemopoietic colony-stimulating factors (e.g., G-CSF) as prophylaxis for febrile neutropenia 35; 36;38; 39;42;
08.1For patients intermidiate (10-20%) and high (>20%) risk of febrile neutropenia 38;
O8.2 In elderly with significant comorbidities 38;
O9
Minimize patient visits for imaging/blood/lab work assessment 34; 36;
O9.1 If feasible be home-drawn 34; 39;
O9.2When possible drawn/taken in external facilities near patient's residence 36; 39;42;44;
O9.3 Consider prolonging intervals 34; 36;O10 Increase use of telemedicine to support
patients remotely 34; 36;37;
38;42;43; 44; 45;
O11
Cancer survivor should adhere to general WHO and CDC recommendations 34; 37;
O11.1Consider deferring or reducing surveilence visits 34; 37;
O11.1.1Must not be lost to follow-up, track deferred visits 34; 43;
O11.1.2Consider follow-up with the use of telemedicine 37;43;
O11.2Should maintain at home during the time being 37;
O12 Consultations for routine screening and genetics oncology can be considered for deferral until the end of pandemic wave 34; 40;
O12.1 unless results before the pandemic had been abnormal 34;
O13 Consider delivering/shipping treatments to patients' homes
34;36;39;40;43;44;47;
O13.1Oral chemotherapy agents/other anticancer therapy 36;39;43;44;
O13.2Intramuscular or subcutaneous cancer treatment 43;
O13.3 IV maintenance treatment 39;
O13.4Specially in patients with higher risk (e.g.,older with more comorbidities) 43;
O14 In the cancer center/outpatient clinic
O14.1 social distance must be adhered 36;O14.1.1 from other patients 36;38;O14.1.2 from HCW 36;38;O14.1.3 awainting rooms should be avoided 37;
O14.2Apropriate PPE (e.g. wear masks) should be used by all 36;37;38;
O14.2.1 especially during treatment 38;
O14.3Patients should avoid arriving early for a visit 39;
O14.4 Reduce duration of the stay 37;O14.5 Use hydroalcoholic solutions for hands 37;
O14.6disinfection measures, mainly of surfaces, should be set in place 37; 42;
O15
Appointment scheduling and registration should be done, preferably online 36; 48;
O16
Radiological-response evaluations should be when feasible, reduced or postponed 39;
O17
Consider testing asymptomatic patients in these cases: 43;
O17.1 before immunosupressive treatment 43;
O17.2imunocomprimised patient that needs to be hospitalized 43;

39
Table V- Initial management recommendations- Inpatient setting
Measure tag Intervention RefencesInpatient (I)I1 Designated units with cohort of COVID-
19 patients to specific wards should be implemented for:
34;36;37;38;40;46;
I1.1 Covid-19 positive 36;37;38;I1.2 Covid-19 negative "free" 36;37;38;I1.3 A third ward for potential/suspected
cases 37;46;
I1.a Comunication/mixing between wards should be avoided
37;46;
I2 Where possible dedicate health care professionals, in the COVID-19 ward, to the care of only COVID-19 patients
34;
I2.1 Create a COVID-19 team with a lead infectious disease specialist qualified for cancer care
34;49;
I2.2 The number of HCW in the COVID-19 ward should be limited
46;
I3 Triaging measures should be implemented at entry points based on:
34;38;43;
I3.1 COVID-19-like symptoms or signs (e.g. chest imaging findings)
34;38;43;48;
I3.2 Urgency and need for hospitalization 34;38;I3.2.1 Limit admissions, mainly non-urgent
hospitalization34;39;48;
I3.3 if resources available to RT-PCR tests to every patient within 48h of admission
38;
I3.3.1 if not feasible, every patient with fever or respiratory symptoms
38;
I4 Suspect cases should be intially admitted in a specific isolation room
34;38;
I4.1 with negative pressure room/HEPA filter 36;
I4.2 If tested negative consider tranfer to COVID-19 "free" ward
34;38;
I4.3 if the patient was exposed to a close contact of a positive case, quarantine should be considered
34;
I4.4 If confirmed positive, isolation measures should proceede
34;
I5 Patients and HCW should have acess to PPE
34;36;37;38;48;49;
I5.1 Masks should be worn at all times 48;I5.2 HCW in COVID-19 ward should wear full
PPE 38;
I5.3 When transferred across hospital departments/wards a patient should wear full PPE
36;37;38;
I5.4 PPE corservation measures should be put in place, especially in case of resource restraints.
34;38;43;
I6 Restrict visitors 34;35;36;I7 Appropriate disinfection measures
should be put in place34;
36;37;42;46;I8 Routine TC lung scan and blood tests can
be implemented48;
I8.1 In case of suspect CT, nucleic acid tests must be done
48;
I9 Patients with high risk of SARS-CoV-2 related death in case of infection, should be tested, regardless of symptoms or signs if they need to be admitted and there are available resources
38;
I10 COVID-19 patients with cancer are at na increased risk of tromboembolic events
38;
I10.1 Prophylaxis with LMWH or DOACs are recommended
38;
I10.1.1 Monitor and prevent possible bleeding complications
38;
I11 HCW should frequently wash their hands 36;
I12 HCW and visitors should be screened for fever
42;

40
Table VI- Initial management recommendations- Anticancer Treatment; 6.1 - Surgery
Measure tag Intervention RefencesAnticancer
treatment
(A)
A1Inform patients of possible risks of therapy during the pandemic 34;
A2
Give patients the option for a potentially less effective but less myelosuppressive treatment 34;
A3
Decision of altering vs maintaining anticancer therapy should be done in a case-by-case basis and based on: 39;42;43;44;
A3.1
Treatment intent (curative vs
palliative) 43;
A3.2 Prognosis/life expectancy 40;43;
A3.3 Patient comorbidities 43;
A3.4 Patient preference 43;
A3.5 symptoms/ clinical condition 43;
A3.6
type of treatment/ Associated
toxicity 39;42;43;
A3.7
risk /probability of infection
transmission 39;42;43;
A3.8 Patient age 40;
A3.9 tumor location 40;
A3.10 number of treatment lines 40;
A3.11 Magnitude of treatment effect 43;
A3.12 other reasons
A4Treatment prioritization should be established 43;
A4.1
prioritize symptomatic cancer cases
and/or interventions with high
magnitude of effect 43;
A4.2
palliative interventions are of lesser
priority and curative are of higher
priority 43;
A5
Curative adjuvant treatment delay can be considered, if for a reasonable duration 34;
A6
In confirmed COVID-19 cancer patients a case-by-case risk-benefict evaluation of maintaining anticancer therapy should be done. 43;
A7
Consider postponing any anticancer treatment in positive cases, as soon as deemed safe 34;35;37;
A7.0.1 if symptomatic 49;
A7.1
Until disapearence of symptoms and
radiological signs and/or a negative
RT-PCR test 37;49;
A8
Treatment decisions (e.g., delay vs maintain) should be done by a multidisciplinary team 44;
A9
Adverse effects of treatments need to be surveilled and treated accordingly (e.g. irAE in IT; nausea and vomits ChT) 43;
A9.1 identify those at higher risk 43;
A10
Consider if feasible maintaining delayed surgeries or RT with neoadjuvant SACT, if feasible 36;37;40;
A10.1
Consider delaying surgeries or RT, if
they can be maintained with
neoadjuvant SACT 36;
Anticancer
treatment,
Surgery (AS)
AS1
Consider delaying/deferring elective
surgeries
34;35;37;39;
44;45;
AS1.1
Until more manageable pandemic
wave 34;39;
AS1.2
Specialy in benign, stable cancer
patients with no complications 37;45;46;
AS2
Surgeries should rationed and
prioritized based on
AS2.1 Urgency 35;45;46;
AS2.1.1
presence of severe organ failure/ life
theatning condition 46;
AS2.2 efficacy 35;
AS2.3
need of post-op ICU beds or other
resources (e.g. PPE; manpower;) 35;45;
AS2.4 tyoe of procedure 45;
AS2.5 Duration 45;
AS2.6
expected time elapsed after
rescheduling 36;
AS2.7 presence of alternative treatment 36;
AS2.8 cancer type 36;
AS2.8.1 progression rate 46;
AS2.9 cancer location 40;
AS2.10 other
AS3
In confirmed COVID-19 cancer
patients should only be operated for
life-threatening conditions 36;
AS4
Special concern for the protection of
HCW with PPE 36;
AS4.1 Specially during procedures like: 36;
AS4.1.1 intubation 36;
AS4.1.2 extubating 36;
AS4.1.3 mask ventilation 36;
AS4.1.4 bronchoscopy 36;
AS4.1.5 chest drain placement 36;
AS4.1.6
electric scalpel treatment especially
of the digestive tract organs 36;
AS4.1.7 laparoscopic surgery 36;
AS4.2
All Patients (even if asymptomatic)
should be tested with RT-PCR,
before surgery/invasive procedure 36;37;
AS4.2.1
and screened for symptoms, travel
and contact history 36;
AS4.2.2
If needed add a second test to
increase sensitivity 36;37;
AS4.3
some surgeries due to being
problementic can be delayed or
replaced with other treatments 36;
AS4.3.1 head and neck 36;
AS4.3.2 upper respiratory/digestive tract 36;
AS5
Surgery for GI, urological, or
gynecologic cancers may be delayed
in assymptomatic or minimally
symtomatic patients 36;
AS6 For post op consider 36;
AS6.1 fewer lab work 36;
AS6.2 fewer image scans 36;
AS6.3
adjuvant chemotherapy of reduced
duration 36;
AS6.4
Systemic anticancer therapy changed
oral , when feasible 36;
AS7
Surgery after neoadjuvant
treatments shoud be performed
after an acceptable time 46;
AS8
When feasible, diagnostic or staging
surgeries should be replaced by
radiologic exams 37;

41
Table VI (Continued)- Initial management recommendations – Anticancer treatment; VI.2- Immunotherapy; VI.3- Radiotherapy; VI.4- Target Therapy
Anticancer treatment, radiotherapy (AR)
AR1
Patients in ongoing radiotherapy
should not interrupt their treatment 34;
AR2 To ensure safety:
AR2.1PPE should be used by patients and HCW 50;
AR2.2 Screen patients before session 50;
AR2.3establish absolute restriction on visitors 50;
AR3
Avoid RT in those were the risk of
severe COVID-19 outcome are
greater than the benefits of the
therapy (e.g. elderly) 50;
AR4
Consider reschedulling RT in those
that delay won’t or mostly won´t
impact their life expectancy 50;
AR5
Consider hypo fractionated
radiotherapy or shorter sessions 50;36;39;
AR5.1
With a simpler treatment plan and delivery 36;
AR5.2
Especially to those that had similar benefit with regular course
AR6
Consider reducing the number of
sessions 36;39;
AR7
Patients who are known contacts or
suspected to be infected should be
treated in diferent rooms of other
patients 34;
AR8
Radiotherapy can in some cases be
considered as a substitute to surgery39;
AR9 Disinfect RT equipment accordingly 37;
Anticancer treatment, Target Therapy (AT)
AT1
PI3K/AKT/mTOR or RAS/RAF/MEK
axis can affect with immune
response capability 38;
AT1.1
The decision to deffer treatment should be based on risk-benefit balance with use of ESMO-Magnitude of Clinical Benefit Scale. 38;
AT1.1.1 depends especialy on cancer type 38;
AT2
In covid-19 patients, with stable
cancer course can withhold TKI until
medically clear 38;
AT3
In positive cases TKI can be
maintained if: 38;
AT3.1 COVID-19 with mild course 38;
AT3.2
patients have sizeable, targetable-oncogene addicted tumors that are likely to flare upon TKI interruption. 38;
AT4 Refrain from using TKI 39;
Anticancer treatment, Immunotherapy (AI)
AI1
Neoadjuvant or adjuvant treatment of ICIs with approved indication, that has with high benefit magnitude in the survival of the patient, should not be suspended or postponed in patients without SARS-CoV-2 infection 38;
AI1.1
In cases of some cases of stable cancer delay can be considered (e.g., associations like nivolumab-ipilinumab) 38;40;
AI2
In positive cases of SARS-CoV-2 infection, treatment should be deferred until recovery. 38;
AI3
In positive COVID-19 cases of stage IV melanoma, intermediate/poor-risk metastatic renal cell carcinoma, programmed death-ligand 1 (PD-L1)-positive and non- small-cell lung cancer (NSCLC) and hepatocellular carcinoma, should suspend ICI treatment, even if it has clear survival benefit, until having a complete recovery and a negative RT-PCR test. 38;
AI3.0.1 should be maintained in lung cancer 39;
AI4
In the case of a very probable irAE, immunosuppressants should be promptly administered as well as a rapid COVID-19 test 42;
AI5
Due to lack of clear evidence of harm due to corticosteroid use, high dose steroid therapy should be discouraged 39;40;42;
AI5.1Its use as an antiemetic should be used less than usual 42;
AI5.1.1 or avoided 40;
AI5.2its use for anti-allergy can also be reduced 42;
AI6
In order to manage irAE, high-dose steroids should be avoided in SARS-CoV-2 infected patients 38;42;
AI6.0 or evaluated in a case-to-case basis 40;
AI6.1
To manage grade 3-4 irAE, if possible, switch to another immunosuppressive medication 38;
AI7 Diminish the use of combined ICIs 42;
AI7.1
Anti-CTLA4 + anti-PD-(L)1 should be administered combined (not sequenced) , if indicated itreatment . 38;
AI7.2
Anti-CTLA4 plus anti-PD-(L)1 combined are associated with high incidence of grade 3-4 irAE. They should be saved for a select group of patients. 42;
AI8
in case of pneumonitis to differentiate between a irAE from a COVID-19 complication, a multidisciplinary aproach should be employed . 35;38;42;
AI8.1employ RT-PCR test and high-resolution CT scan 38;
AI9Consider the use of higher doses with a longer interval period 42;
AI10
when possible replace ciplastin with carboplatin, for it is less toxic and quicker to administer 40;
AI11
Consider replacing treatments with associated lung toxicity such as bleomycin 40;
AI12In case of neutropenia consider use of G-CSF 40;

42
Table VII- Initial management recommendations- Measures for staff
Measure tag Intervention RefencesStaff (S)
S1
In case of contact with confirmed/suspect case, staff may need to self-isolate 34;39;
S2
PPE should be provided to all HCW, and used accordingly allong with other hygiene and infection control measures 36;37;38;
49;S2.1 Surgical mask/Filtering face piece FFP 38;S2.2 Gloves 38;S2.3 Gown 38;S2.4 Eye protection 38;S2.5 Should practice hand hygiene 36;37;38;S2.6 avoid crowded areas/ social distancing 37;S2.7 hidroalcoholic solution use 37;S2.8 other
S3
HCW must be allocated to one area/facility to ensure reduced spread to other locations 36;
S4
Rotate staff/ stagger shift to minimize risk of infection transmission to all HCW 36;
S5Triage staff (e.g., at hospital/facility entry points) 36;
S5.1 for fever 42;S5.2 other
S6
Routine testing should be established should be established, especialy for staff working with positive COVID-19 patients. 36;
S7
HCW suspected of being infected should self-isolate/quarantine at home until testing negative 38;
S8
RT-PCR tests from NPS should be offered to all HCW with symptoms suggestive of SARS-CoV-2 infection 38;
S8.1or if directly exposed to a suspect/positive patient 49;
S9 Clear policies should be established 36;
S9.1 how to manage symptomatic or infected staff 36;
S9.2 return-to-work 36;
S10 HCW should be instructed and train on infection prevention measures 36;37;
S11 Implement travel restrictions to all HCW 45;
S12
Establishment of clear pathways in order to maintain productivity even after significant number of HCWs were absent (e.g., become ill or in self-isolation/ quarantine) 34;39;42;
S12.1
Use telemedicine to help mitigate impact of fewer HCW in the hospital/clinic or protect them from exposure 34;39;
S13
Consider drafting HCW from non-essential cancer services ( e.g.cancer genetics) to substitute in needed services 42;
S14Multidisciplinary team consultations should be done remotely when possible 39;42;
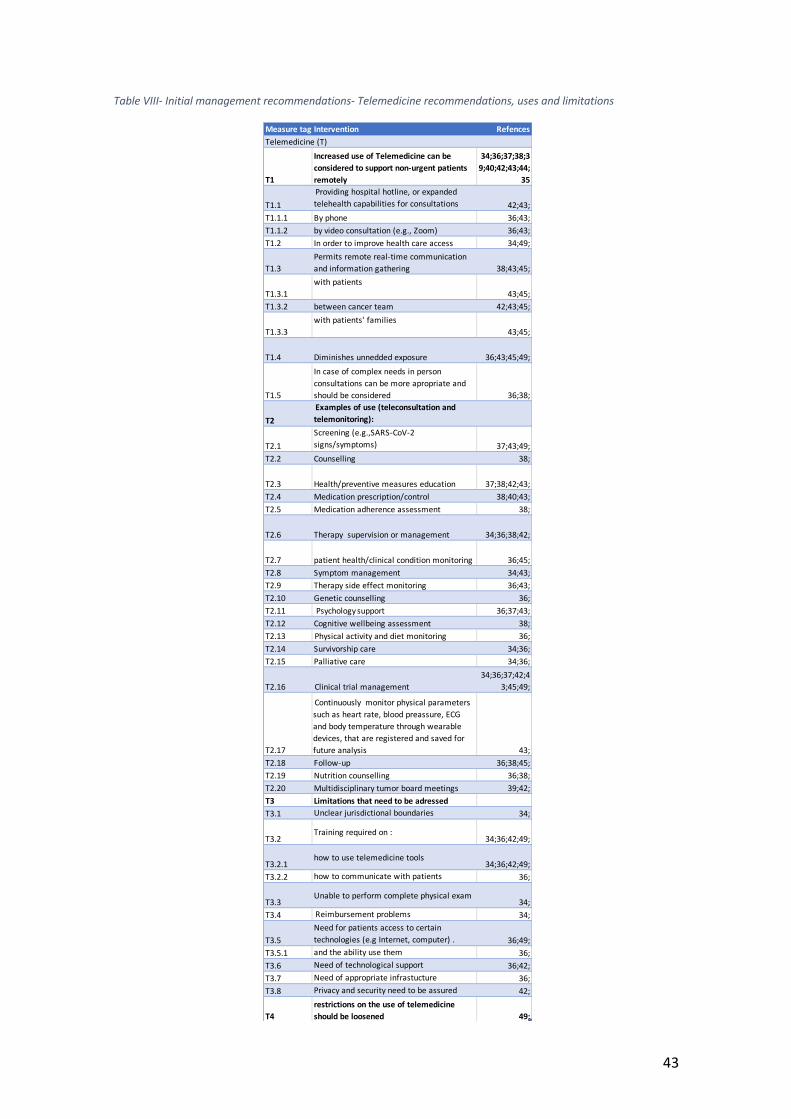
43
Table VIII- Initial management recommendations- Telemedicine recommendations, uses and limitations
Measure tag Intervention RefencesTelemedicine (T)
T1
Increased use of Telemedicine can be considered to support non-urgent patients remotely
34;36;37;38;39;40;42;43;44;
35
T1.1 Providing hospital hotline, or expanded telehealth capabilities for consultations 42;43;
T1.1.1 By phone 36;43;T1.1.2 by video consultation (e.g., Zoom) 36;43;T1.2 In order to improve health care access 34;49;
T1.3Permits remote real-time communication and information gathering 38;43;45;
T1.3.1with patients
43;45;T1.3.2 between cancer team 42;43;45;
T1.3.3with patients' families
43;45;
T1.4 Diminishes unnedded exposure 36;43;45;49;
T1.5
In case of complex needs in person consultations can be more apropriate and should be considered 36;38;
T2 Examples of use (teleconsultation and telemonitoring):
T2.1Screening (e.g.,SARS-CoV-2 signs/symptoms) 37;43;49;
T2.2 Counselling 38;
T2.3 Health/preventive measures education 37;38;42;43;T2.4 Medication prescription/control 38;40;43;T2.5 Medication adherence assessment 38;
T2.6 Therapy supervision or management 34;36;38;42;
T2.7 patient health/clinical condition monitoring 36;45;T2.8 Symptom management 34;43;T2.9 Therapy side effect monitoring 36;43;T2.10 Genetic counselling 36;T2.11 Psychology support 36;37;43;T2.12 Cognitive wellbeing assessment 38;T2.13 Physical activity and diet monitoring 36;T2.14 Survivorship care 34;36;T2.15 Palliative care 34;36;
T2.16 Clinical trial management34;36;37;42;4
3;45;49;
T2.17
Continuously monitor physical parameters such as heart rate, blood preassure, ECG and body temperature through wearable devices, that are registered and saved for future analysis 43;
T2.18 Follow-up 36;38;45;T2.19 Nutrition counselling 36;38;T2.20 Multidisciplinary tumor board meetings 39;42;T3 Limitations that need to be adressedT3.1 Unclear jurisdictional boundaries 34;
T3.2Training required on :
34;36;42;49;
T3.2.1how to use telemedicine tools
34;36;42;49;T3.2.2 how to communicate with patients 36;
T3.3Unable to perform complete physical exam
34;T3.4 Reimbursement problems 34;
T3.5Need for patients access to certain technologies (e.g Internet, computer) . 36;49;
T3.5.1 and the ability use them 36;T3.6 Need of technological support 36;42;T3.7 Need of appropriate infrastucture 36;T3.8 Privacy and security need to be assured 42;
T4restrictions on the use of telemedicine should be loosened 49;

44
Table IX- Initial management recommendations- Other general and support recommendations
Measure tag Intervention Refences
General and support (G)
G1
Recommended hygiene and infection prevention measures
(e.g., regular hand washing and use of masks) 43;35;
G2 Social distancing should be advocated for HCW and patients 35;36;
G2.1Crowded areas (e.g., waiting rooms) should be avoided by patients and HCW 37;
G3 Psychological suppport must be provided
34;36;37;39;4
2;43;44;
G3.1 for patients34;37;39;42;4
3;44;G3.2 For HCW 36;37;42;44;G3.2.1 assess burnout or distress, and act accordingly 36;37;42;
G3.3Assess levels of distress and need for psychological treatment, 34;42;43;
G3.3.1 act promptly and appropriately 34;42;43;
G3.4 Telemedicine/telepsychiatry can help mitigate symptoms in patients and HCW 36;42;
G4
Testing RT-PCR test is the gold standard for the diagnosis of
acute infection 37;38;39;43;
G4.1 Imaging (e.g., CT) of the chest, can also be considered 36;38;43;G4.1.1 Especialy used in regions with high prevelence 43;
G4.1.2 It is not used for routine screening or diagnosis of COVID-19 43;G4.1.3 Can be considered for preoperative screening 36;
G4.2Serological assays may help identify who has already been infected 38;39;43;
G4.2.1 not usefull in detection of acute infection 38;43;
G4.2.2May help surveil the dissemination of infection in the cancer patient population 38;43;
G4.2.3 May identify possible immunity 38;39;43;G4.2.4 Can also be implemented among HCW 38;
G5
Cacer patients are recommended to self isolate and
minimize outside activities
36;
G6
Focus should be in reducing the number and duration of
consultations, anticancer treatment sessions and
admissions, without comprimising patients treatment
40;
G6.1treatment adjustment, to acomplish this goal, should be discussed by a multidisciplinary team 39;
G7
More rigorous screenings and assessments should be
implemented for the older patients in regards to: 42;
G7.1 Function 42;
G7.2 Comorbidities 42;
G7.3 Falls 42;
G7.4 Depression 42;
G7.5 Cognition 42;
G7.6 Nutrition 42;
G7.7 treatment toxicities 42;
G8 Nutrition support should be maintained 42;51;G8.1 Prevent malnutrition and its consequences 51;
G8.2preferably remotely using telemedicine/telehealth and phone calls, when feasible 51;
G8.3 in all patients (oupatient and inpatient) 51;
G8.4In case of critical conditions such as poor nutritional status, consider hospital admission. 51;
G8.5Consider the use of oral nutritional supplements (ONS) in patients at risk of malnutrition 51;
G9 Promote exercise and nutrition measures 42;
G10 Ensure patients are vacinated for influenza/seasonal flu 35;42;
G10.1 Especialy in the southern hemisthere 42;G11 restrict in hospital/clinic patient flow 36;
G12
All patients with advanced cancer should be screened and
tested 49;
G12.1
screening also extended in elderly patients before chemotherapy session or surgery and all imunocomprimised patients 49;
G13
Besides age, special atention should be given to patients
with certain risk factors like lyphopenia, neutropenia and
comorbidities 40;
G14 Clinical trial referrals/accrual decision should be based on 38;
G14.0.1 as a general rule referrals/accruals should be reduced 35;39;46;
G14.1 R0 index 38;
G14.2 Pandemic case load 38;
G14.3 Health care organization characteristics and resources 38;48; G14.4 Patients risk by not entering 38;G14.5 Patient’s risk of being infected 38;46;

45
Table X- Impact in Cancer care- Characteristics of studies selected
1st author Region type of study Population Time period followedZuliani, S Verona,
Italyretrospective study
the oncological department from the University Hospital Trust of Verona (Italy)
January 1 to March 31 of 2019 and 2020
Montesi, G Rovigo, Italy retrospective study
a ROI in Rovigo, Italy (Maria della Misericordia Hospital)
February 1 to March 31 of 2019 and 2020
Nichetti, F Milan, Italy observational study
1081 cancer patients treated with antiancer therapy in outpatient and inpatient setting in the COVINT study
February 16 and April 10 of 2019 and 2020
Buglione, M Lombardy, Italy
retrospective study
Brescia University Radiation Oncology Department were 402 cancer patients were undergoing active anticancer therapy
February 24 to April 24
Caravatta, L Abruzzo, Italy
retrospective study
the Radiation Center of Chieti March 9 to May 4 2019 and 2020
Gonnelli, A Pisa, Italy retrospective study
unit of radiotherapy (Operative Unit of Radiotherapy; OUR) of the University Hospital of Pisa
March 9 to May 31
Indini, A Italy nation wide cross-sectional survey
responded by 122 physicians head of oncological departments
March 12 to 15
Torzilli,G Italy nation wide cross-sectional survey
responded by 54 surgical units in 36 Hospitals. 30% of the units were in Lombardy
March 27
Jereczek-Fossa, B. A
Italy nation wide cross-sectional survey
responded by 125 directors of italian radiological departments (20% in Lobardy)
April 6 to 16
Ottaviano, M
Italy nation-wide cross-sectional survey
responded by 75 young oncologists, most specialists(49;65.3%) and the remaining trainees(26;34.7%)
April 10 to May 8
Joode, K Netherlands nation wide cross-sectional survey
responded by 5302 cancer patients
March 29 to April 18
Akuamoa-Boateng, D
Heinsberg, Germany
retrospective study
a german hotspot University between weeks 12 and 19 of 2019 and 2020 (March 18 to May 10, 2019; March 16, to May 08, 2020)
Matuschek,
C
Germany, Austria and Switzerland
cross-sectional survey
responded by 106 radiation
oncologic institutions (ROI) in
Germany(83), Austria (13) and
Switzerland (10)
April 26 to May 22
Reuter-
Oppermann,
M
Germany,
Austria and
Switzerland
cross-sectional survey
responded by 154 medical
physiscists (82 complete and 72
partially complete)
23 to 26 of March
Slotman, B.
J
Europe cross-sectional survey
responded by 139 members, heads of RO departments in 29 european contries (mainly Italy (20; 14%), Germany (17; 12%), Spain (15; 11%), the Nether- lands (10; 7%), Switzerland (9; 6%), the United Kingdom (8; 6%) and Belgium (7; 5%)
May 6 to May 21
Gill, S Canada nation wide
cross-sectional
survey
responded by 159 canadian medical oncologist
March 30 to April 4
Ning, M. S Texas, USA Prospective cohort study
in a RO department in Texas
USA, 121 patients’ activities
were monitored
March 19 to April 22
Hui, J. Y. C USA nation wide
cross-sectional
survey
responded by 411 physicians,
241 (58.6%) surgeons, 106
(25.8%) medical oncologists,
and 64 (15.6%) radiation
oncologists
March 27 to April 10
Onesti, C.E Europe and USA
observational
study
responded by 21 oncological centers in 10 countries (from Europe and the USA)
April 10 to May 6
Lee, S South Korea retrospective study
Korea University Anam
Hospital
January 1 to April 30 of
2019 and 2020
Alexander,
M
worldwide (28 countries from Africa, Europe, Australasia, South and Norther America)
cross-
sectional
survey
42 practice leaders in 28
countries/regions
10 to 22 of April
Ürün, Y worldwide cross-
sectional
survey
responded by 343 oncologists in 28 countries, mostly from Turkey (49.27%
Mach 24 to April 29
Jazieh, A.
R.
worldwide cross-sectional study
responded by 356 centers throughout 54 countries woldwide (mainly european 41.01%)
April 21 to May 8
Chazan, G worldwide cross sectional international survey
501 clinicians of 70 countries mostly european (39%), with Australia(AUS) as the most represented country (33.5%), and the remainder from New Zealand (NZ) and Asia
between May 4 and June 19
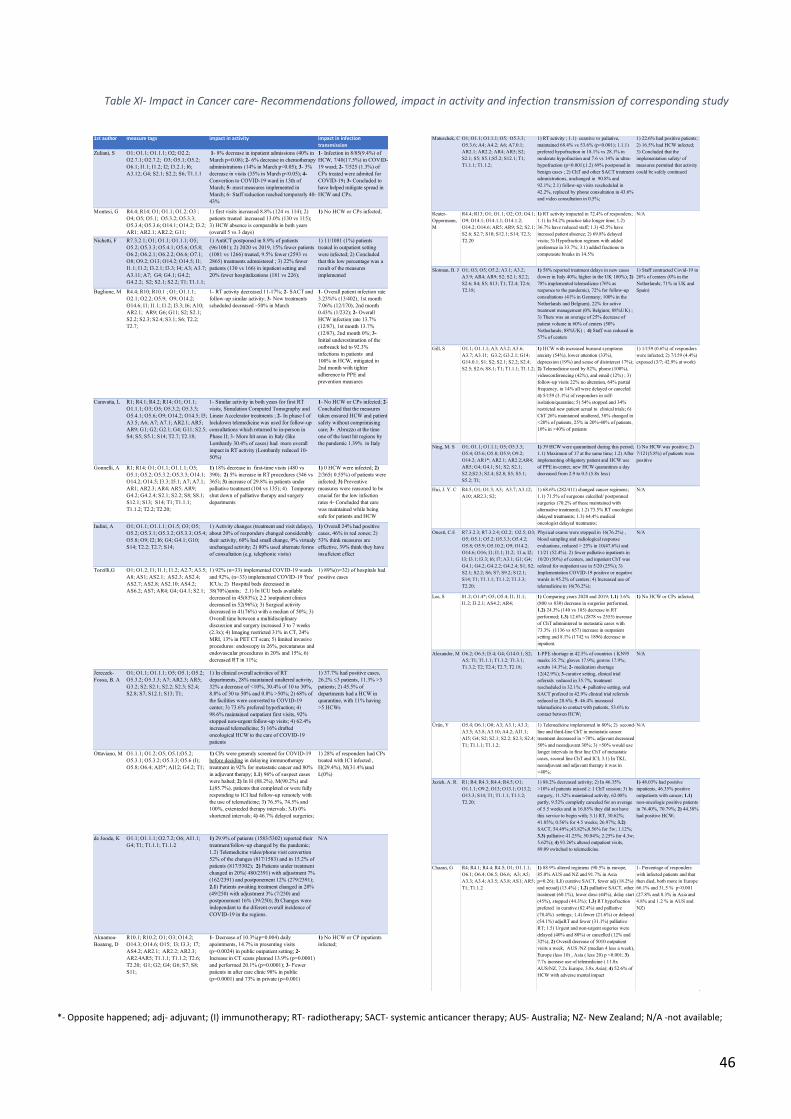
46
Table XI- Impact in Cancer care- Recommendations followed, impact in activity and infection transmission of corresponding study
*- Opposite happened; adj- adjuvant; (I) immunotherapy; RT- radiotherapy; SACT- systemic anticancer therapy; AUS- Australia; NZ- New Zealand; N/A -not available;
1st author measure tags impact in activity impact in infection transmission
Zuliani, S O1; O1.1; O1.1.1; O2; O2.2; O2.7.1; O2.7.2; O3; O5.1; O5.2; O6.1; I1.1; I1.2; I2; I3.2.1; I6; A3.12; G4; S2.1; S2.2; S6; T1.1.1
1- 8% decrease in inpatient admissions (40% in March p=0.08); 2- 6% decrease in chemotherapy administrations (14% in March p<0.05); 3- 3% decrease in visits (35% in March p<0.05); 4- Convertion to COVID-19 ward in 13th of March; 5- most measures implemented in March; 6- Staff reduction reached temporarly 40-43%
1- Infection in 8/85(9.4%) of HCW, 7/40(17.5%) in COVID-19 ward; 2- 7/525 (1.3%) of CPs treated were admited for COVID-19; 3- Concluded to have helped mitigate spread in HCW and CPs.
Montesi, G R4.4; R14; O1; O1.1; O1.2; O3 ; O4; O5; O5.1; O5.3.2; O5.3.3; O5.3.4; O5.3.6; O14.1; O14.2; I3.2; AR1; AR2.1; AR2.2; G11;
1) first visits increased 8.8% (124 vs 114); 2) patients treated increased 13.0% (130 vs 115); 3) HCW absence is comparable in both years (overall 5 vs 3 days)
1) No HCW or CPs infected;
Nichetti, F R7.3.2.1; O1; O1.1; O1.1.1; O5; O5.2; O5.3.3; O5.4.1; O5.6; O5.8; O6.2; O6.2.1; O6.2.2; O6.6; O7.1; O8; O9.2; O13; O14.2; O14.5; I1; I1.1; I1.2; I3.2.1; I3.3; I4; A3; A3.7; A3.11; A7; G4; G4.1; G4.2; G4.2.2; S2; S2.1; S2.2; T1; T1.1.1;
1) AntiCT postponed in 8.9% of patients (96/1081); 2) 2020 vs 2019, 15% fewer patients (1081 vs 1266) treated, 9.5% fewer (2593 vs 2865) treatments admnistered ; 3) 22% fewer patients (130 vs 166) in inpatient setting and 20% fewer hospitalizations (181 vs 226);
1) 11/1081 (1%) patients treated in outpatient setting were infected; 2) Concluded that this low percentage was a result of the measures implemented
Buglione, M R4.4; R10; R10.1 ; O1; O1.1.1; O2.1; O2.2; O5.9; O9; O14.2; O14.6; I1; I1.1; I1.2; I3.3; I6; A10; AR2.1; AR9; G6; G11; S2; S2.1; S2.2; S2.3; S2.4; S3.1; S6; T2.2; T2.7;
1- RT activity decreased 11-17%; 2- SACT and follow-up similar activity; 3- New treatments scheduled decreased ~50% in March
1- Overall patient infection rate 3.23%% (13/402), 1st month 7.06% (12/170), 2nd month 0.43% (1/232); 2- Overall HCW infection rate 13.7% (12/87), 1st month 13.7% (12/87), 2nd month 0%; 3- Initial underestimation of the outbreack led to 92.3% infections in patients and 100% in HCW, mitigated in 2nd month with tighter adherence to PPE and prevention measures
Caravatta, L R1; R4.1; R4.2; R14; O1; O1.1; O1.1.1; O3; O5; O5.3.2; O5.3.3; O5.4.1; O5.6; O9; O14.2; O14.5; I5; A3.5; A6; A7; A7.1; AR2.1; AR5; AR9; G1; G2; G2.1; G4; G11; S2.5; S4; S5; S5.1; S14; T2.7; T2.18;
1- Similar activity in both years for first RT visits, Simulation Computed Tomography and Linear Accelerator treatments ; 2- In phase I of lockdown telemedicine was used for follow-up consultations which returned to in-person in Phase II; 3- More hit areas in Italy (like Lombardy 30.4% of cases) had more overall impact in RT activity (Lombardy reduced 10-50%)
1- No HCW or CPs infected; 2- Concluded that the measures taken ensured HCW and patient safety without comprimising care; 3- Abruzzo at the time one of the least hit regions by the pandemic 1.39% in Italy
Gonnelli, A R1; R14; O1; O1.1; O1.1.1; O5; O5.1; O5.2; O5.3.2; O5.3.3; O14.1; O14.2; O14.5; I3.3; I5.1; A7; A7.1; AR1; AR2.3; AR4; AR5; AR9; G4.2; G4.2.4; S2.1; S2.2; S8; S8.1; S12.1; S13; S14; T1; T1.1.1; T1.1.2; T2.2; T2.20;
1) 18% decrease in first-time visits (480 vs 390); 2) 5% increase in RT procedures (346 vs 365); 3) increase of 29.8% in patients under palliative treatment (104 vs 135); 4) Temporary shut down of palliative therapy and surgery departments
1) 0 HCW were infected; 2) 2/365( 0.55%) of patients were infected; 3) Preventive measures were reasoned to be crucial for the low infection rates 4- Concluded that care was maintained while being safe for patients and HCW
Indini, A O1; O1.1; O1.1.1; O1.5; O3; O5; O5.2; O5.3.1; O5.3.2; O5.3.3; O5.4; O5.8; O9; I2; I6; G4; G4.1; G10; S14; T2.2; T2.7; S14;
1) Activity changes (treatment and visit delays), about 20% of responders changed considerably their activity, 60% had small change, 9% virtualy unchanged activity; 2) 80% used alternate forms of consultation (e.g. telephonic visits)
1) Overall 24% had positive cases, 46% in red zones; 2) 53% think measures are effective, 39% think they have insuficient effect
Torzilli,G O1; O1.2; I1; I1.1; I1.2; A2.7; A3.5; A8; AS1; AS2.1; AS2.3; AS2.4; AS2.7; AS2.8; AS2.10; AS4.2; AS6.2; AS7; AR4; G4; G4.1; S2.1;
1) 92% (n=33) implemented COVID-19 wards and 92%, (n=33) implemented COVID-19 'free' ICUs; 2) Hospital beds decreased in 38(70%)units; 2.1) In ICU beds available decreased in 45(83%); 2.2 )outpatient clinics decreased in 52(96%); 3) Surgical activity decreased in 41(76%) with a median of 50%; 3) Overall time between a multidisciplinary discussion and surgery increased 3 to 7 weeks (2.3x); 4) Imaging restricted 31% in CT, 24% MRI, 13% in PET CT scan; 5) limited invasive procedures: endoscopy in 26%, percutaneus and endovascular procedures in 20% and 15%; 6) decreased RT in 11%;
1) 89%(n=32) of hospitals had positive cases
Jereczek-Fossa, B. A
O1; O1.1; O1.1.1; O5; O5.1; O5.2; O5.3.2; O5.3.3; A7; AR2.3; AR5; G3.2; S2; S2.1; S2.2; S2.3; S2.4; S2.8; S7; S12.1; S13; T1;
1) In clinical overall activities of RT departments, 28% maintained unaltered activity, 32% a decrease of <10%, 30.4% of 10 to 30%, 8.8% of 30 to 50% and 0.8% >50%; 2) 68% of the facilities were converted to COVID-19 center; 3) 73.6% prefered hypofraction; 4) 98.6% maintained outpatient first visits, 92% stopped non-urgent follow-up visits; 4) 62.4% increased telemedicine; 5) 16% drafted oncological HCW to the care of COVID-19 patients
1) 37.7% had positive cases, 26.2% ≤3 patients, 11.3% >3 patients; 2) 45.5% of departments had a HCW in quarantine, with 11% having >5 HCWs
Ottaviano, M O1.1.1; O1.2; O5; O5.1;O5.2; O5.3.1; O5.3.2; O5.3.3; O5.6 (I); O5.8; O6.4; AI5*; AI12; G4.2; T1;
1) CPs were generaly screened for COVID-19 before deciding in delaying immunotherapy treatment in 92% for metastatic cancer and 80% in adjuvant therapy; 1.1) 96% of suspect cases were halted; 2) In H (88.2%), M(90.2%) and L(85.7%), patients that completed or were fully responding to ICI had follow-up remotely with the use of telemedicine; 3) 76.5%, 74.5% and 100%, extenteded therapy intervals; 3.1) 0% shortened intervals; 4) 46.7% delayed surgeries;
1) 28% of responders had CPs treated with ICI infected , H(29.4%), M(31.4%)and L(0%)
de Joode, K O1.1; O1.1.1; O2.7.2; O6; AI1.1; G4; T1; T1.1.1; T1.1.2
1) 29.9% of patients (1583/5302) reported their treatment/follow-up changed by the pandemic; 1.2) Telemedicine video/phone visit convertion 52% of the changes (817/1583) and in 15.2% of patients (817/5302); 2) Patients under treatment changed in 20%( 480/2391) with adjustment 7% (162/2391) and postponement 12% (279/2391); 2.1) Patients awaiting treatment changed in 20% (49/250) with adjustment 3% (7/250) and postponement 16% (39/250); 3) Changes were independant to the diferent overall incidence of COVID-19 in the regions.
N/A
Akuamoa-Boateng, D
R10.1; R10.2; O1; O3; O14.2; O14.3; O14.6; O15; I3; I3.3; I7; AS4.2; AR2.1; AR2.2; AR2.3; AR2.4AR5; T1.1.1; T1.1.2; T2.6; T2.20; G1; G2; G4; G6; S7; S8; S11;
1- Decrease of 10.3%(p=0.004) daily apointments, 14.7% in presenting visits (p=0.0024) in public outpatient setting; 2- Increase in CT scans planned 13.9% (p=0.0001) and performed 20.1% (p=0.0001); 3- Fewer patients in after care clinic 98% in public (p=0.0001) and 73% in private (p=0.001)
1) No HCW or CP inpatients infected;
Matuschek, C O1; O1.1; O1.1.1; O5; O5.3.3; O5.3.6; A4; A4.2; A6; A7.0.1; AR2.1; AR2.2; AR4; AR5; S2; S2.1; S5; S5.1;S5.2; S12.1; T1; T1.1.1; T1.1.2;
1) RT activity ; 1.1) curative vs paliative, maintained 68.4% vs 53.6% (p<0.001); 1.1.1) prefered hypofraction in 18.1% vs 28.1% in moderate hypofraction and 7.6 vs 14% in ultra-hypofraction (p<0.001);1.2) 69% postponed in benign cases ; 2) ChT and other SACT treatment admnistrations, unchanged in 90.8% and 92.1%; 2.1) follow-up visits rescheduled in 42.2%, replaced by phone consultation in 43.6% and video consultation in 0.5%;
1) 22.6% had positive patients; 2) 16.5% had HCW infected; 3) Concluded that the implementation safety/ of measures permited that activity could be safely continued
Reuter-Oppermann, M
R4.4; R13; O1; O1.1; O2; O3; O4.1; O9; O14.1; O14.1.1; O14.1.2; O14.2; O14.6; AR5; AR9; S2; S2.1; S2.6; S2.7; S10; S12.1; S14; T2.3; T2.20
1) RT activity impacted in 72.4% of responders; 1.1) In 54.2% practice take longer time; 1.2) 36.7% have reduced staff; 1.3) 42.5% have incresed patient absence; 2) 69.8% delayed visits; 3) Hypofraction regimen with added preference in 33.7%; 3.1) added fractions to compensate breaks in 14.5%
N/A
Slotman, B. J O1; O3; O5; O5.2; A3.1; A3.2; A3.9; AR4; AR9; S2; S2.1; S2.2; S2.6; S4; S5; S13; T1; T2.4; T2.6; T2.18;
1) 58% reported treatment delays in new cases (lower in Italy 40%; higher in the UK 100%); 2) 78% implemented telemedicine (76% as responce to the pandemic), 72% for follow-up consultations (41% in Germany; 100% in the Netherlands and Belgium), 22% for active treatment management (0% Belgium; 88%UK) ; 3) There was an average of 25% decrease of patient volume in 60% of centers (50% Netherlands; 88%UK) ; 4) Staff was reduced in 57% of centers
1) Staff contracted Covid-19 in 26% of centers (0% in the Netherlands; 71% in UK and Spain)
Gill, S O1.1; O1.1.1; A3; A3.2; A3.6; A3.7; A3.11; G3.2; G3.2.1; G14; G14.0.1; S1; S2; S2.1; S2.2; S2.4; S2.5; S2.6; S8.1; T1; T1.1.1; T1.1.2;
1) HCW with increased burnout symptoms anxiety (54%), lower attention (33%), depression (19%) and sense of disinterest 17%); 2) Telemedicine used by 82%, phone (100%), videoconferencing (42%), and email (12%) ; 3) follow-up visits 22% no alteration, 64% partial frequency, in 14% all were delayed or canceled 4) 5/159 (3.1%) of responders in self-isolation/quaratine; 5) 54% stopped and 34% restricted new patient acrual to clinical trials; 6) ChT 26% maintained unaltered, 38% changed in <20% of patients, 25% in 20%-40% of patients, 10% in >40% of patients
1) 1/159 (0.6%) of responders were infected; 2) 7/159 (4.4%) exposed (3/7; 42.9% at work)
Ning, M. S O1; O1.1; O1.1.1; O5; O5.3.3; O5.4; O5.6; O5.8; O5.9; O9.2; O14.2; AR1*; AR2.1; AR2.2;AR4; AR5; G4; G4.1; S1; S2; S2.1; S2.2;S2.3; S2.4; S2.8; S5; S5.1; S5.2; T1;
1) 39 HCW were quarantined during this period; 1.1) Maximum of 17 at the same time; 1.2) After implementing obligatory patient and HCW use of PPE in-center, new HCW quarantines a day decreased from 2.9 to 0.5 (5.8x less)
1) No HCW was positive; 2) 7/121(5.8%) of patients were positive
Hui, J. Y. C R4.5; O1; O1.3; A3; A3.7; A3.12; A10; AR2.3; S2;
1) 68.6% (282/411) changed cancer regimens; 1.1) 71.5% of surgeons calcelled/ postponned surgeries (70.2% of these maintained with alternative treatment); 1.2) 73.5% RT oncologist delayed treatments; 1.3) 64.4% medical oncologist delayed treatments;
N/A
Onesti, C.E R7.3.2.3; R7.3.2.4; O2.2; O2.5; O3; O5; O5.1; O5.2; O5.3.3; O5.4.2; O5.8; O5.9; O5.10.2; O9; O14.2; O14.6; O16; I1; I1.1; I1.2; I1.a; I2; I3; I3.1; I3.3; I6; I7; A3.1; G1; G4; G4.1; G4.2; G4.2.2; G4.2.4; S1; S2; S2.1; S2.2; S6; S7; S9.2; S12.1; S14; T1; T1.1.1; T1.1.2; T1.3.3; T2.20;
Physical exams were stopped in 16(76.2%) , blood sampling and radiological response evaluations, reduced > 25% in 10(47.6%) and 11/21 (52.4%). 2) fewer palliative inpatients in 10/20 (50%) of centers, and inpatient ChT was refered for outpatient use in 5/20 (25%); 3) Implementation COVID-19 positive or negative wards in 95.2% of centers; 4) Increased use of telemedicine in 16(76.2%);
N/A
Lee, S 01.2; O1.4*; O5; O5.4; I1; I1.1; I1.2; I3.2.1; AS4.2; AR4;
1) Comparing years 2020 and 2019; 1.1) 3.6% (800 vs 830) decrease in surgeries performed, 1.2) 24.3% (140 vs 185) decrease in RT performed; 1.3) 12.6% (2878 vs 2555) increase of ChT admnintered to metastatic cases with 73.3% (1136 vs 657) increase in outpatient setting and 8.1% (1742 vs 1896) decrease in inpatient.
1) No HCW or CPs infected;
Alexander, M O6.2; O6.5; I5.4; G4; G14.0.1; S2; A5; T1; T1.1.1; T1.1.2; T1.3.1; T1.3.2; T2; T2.4; T2.7; T2.18;
1-PPE shortage in 42.5% of countries ( KN95 masks 35.7%; gloves 17.9%; gowns 17.9%; scrubs 14.3%); 2- medication shortage 12(42.9%); 3-curative setting, clinical trial referrals reduced in 35.7%, treatment rescheduled in 32.1%; 4- palliative setting, oral SACT prefered in 42.9% clinical trial referrals reduced in 28.6%; 5- 46.4% increased telemedicine to contact with patients, 53.6% to contact betwen HCW;
N/A
Ürün, Y O5.4; O6.1; O8; A3; A3.1; A3.3; A3.5; A3.8; A3.10; A4.2; AI1.1; AI5; G4; S2; S2.1; S2.2; S2.3; S2.4; T1; T1.1.1; T1.1.2;
1) Telemedicine implemented in 80%; 2) second-line and third-line ChT in metastatic cancer treatment decreased in >70%, adjuvant decreased 50% and neoadjuvant 30%; 3) >50% would use longer intervals in first line ChT of metastatic cases, second line ChT and ICI; 3.1) In TKI, neoadjuvant and adjuvant therapy it was in <40%;
N/A
Jazieh, A. R. R1; R4; R4.3; R4.4; R4.5; O1; O1.1.1; O9.2; O13; O13.1; O13.2; O13.3; S14; T1; T1.1.1; T1.1.2; T2.20;
1) 88.2% decreased activity; 2) In 46.35% >10% of patients missed ≥ 1 ChT session; 3) In surgery, 11.52% maintained activity, 62.08% partly, 9.52% completly canceled for an average of 5.5 weeks and in 16.85% they did not have this service to begin with; 3.1) RT, 30.62%; 41.85%; 0.56% for 4.5 weeks; 26.97%; 3.2) SACT, 54.49%;;43.82%;0.56% for 5w; 1.12%; 3.3) palliative 41.25%; 50.84%; 2.25% for 4.3w; 5.62%); 4) 93.26% altered outpatient visits, 89.09 switched to telemedicine.
1) 48.03% had positive inpatients, 46.35% positive outpatients with cancer; 1.1) non-oncologic positive patients in 76.40%, 70.79%; 2) 44.38% had positive HCW;
Chazan, G R4; R4.1; R4.4; R4.5; O1; O1.1.1; O6.1; O6.4; O6.5; O6.6; A3; A5; A3.3; A3.4; A3.5; A3.8; AS1; AR5; T1; T1.1.2
1) 88.9% altered regimens (90.5% in europe, 85.0% AUS and NZ and 91.7% in Asia p=0.26); 1.1) curative SACT, fewer adj (18.2%) and neoadj (13.4%) ; 1.2) palliative SACT, other treatment (60.1%), lower dose (44%), delay start (45%), stopped (44.3%); 1.3) RT hypofraction prefered in curative (82.4%) and palliative (78.4%) settings; 1.4) fewer (21.6%) or delayed (54.1%) adjuRT and fewer (31.1%) palliative RT; 1.5) Urgent and non-urgent sugeries were delayed (40% and 80%) or cancelled (12% and 32%); 2) Overall decrease of 5010 outpatient visits a week, AUS /NZ (median 4 less a week), Europe (less 10) , Asia ( less 20) p <0.001; 3) 7.7x increase use of telemedicine ( 11.8x AUS/NZ, 7.2x Europe, 3.8x Asia); 4) 52.6% of HCW with adverse mental impact
1- Percentage of responders with infected patients and that then died, both more in Europe 66.1% and 31.5 % p<0.001 (27.8% and 8.3% in Asia and 4.8% and 1.2 % in AUS and NZ)

47
References 1. Kakodkar P, Kaka N, Baig MN. A Comprehensive Literature Review on the Clinical
Presentation, and Management of the Pandemic Coronavirus Disease 2019 (COVID-19). Cureus. 2020;12(4):e7560-e7560.
2. Petersen E, Koopmans M, Go U, et al. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. The Lancet Infectious Diseases. 2020;20(9):e238-e244.
3. World Health Organizarion (WHO); Genebra, Switzerland; Weekly epidemiological update - 22 December 2020. 2020; https://www.who.int/publications/m/item/weekly-epidemiological-update---22-december-2020. Accessed 25/12/2020.
4. Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA. 2020;324(8):782-793.
5. International Agency for Research on Cancer (IARC); Lyon, France; CANCER TODAY. 2020; https://gco.iarc.fr/today/home. Accessed 25/04/2021.
6. Bakouny Z, Hawley JE, Choueiri TK, et al. COVID-19 and Cancer: Current Challenges and Perspectives. Cancer Cell. 2020;38(5):629-646.
7. Lambertini M, Toss A, Passaro A, et al. Cancer care during the spread of coronavirus disease 2019 (COVID-19) in Italy: young oncologists' perspective. ESMO Open. 2020;5(2).
8. Cortiula F, Pettke A, Bartoletti M, Puglisi F, Helleday T. Managing COVID-19 in the oncology clinic and avoiding the distraction effect. Ann Oncol. 2020;31(5):553-555.
9. Lyman GH, Kuderer NM. Personalized cancer supportive care in COVID-19 era. Annals of oncology : official journal of the European Society for Medical Oncology. 2020;31(7):835-837.
10. Rossi E, Schinzari G, Tortora G. Pneumonitis from immune checkpoint inhibitors and COVID-19: current concern in cancer treatment. J Immunother Cancer. 2020;8(2).
11. Schrag D, Hershman DL, Basch E. Oncology Practice During the COVID-19 Pandemic. JAMA. 2020;323(20):2005-2006.
12. Mulvey TM, Jacobson JO. COVID-19 and Cancer Care: Ensuring Safety While Transforming Care Delivery. Journal of Clinical Oncology. 2020;38(28):3248-3251.
13. Pareek P, Vishnoi JR, Kombathula SH, Vyas RK, Misra S. Teleoncology: The Youngest Pillar of Oncology. JCO Glob Oncol. 2020;6:1455-1460.
14. Liang W, Guan W, Chen R, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol. 2020;21(3):335-337.
15. Dai M, Liu D, Liu M, et al. Patients with Cancer Appear More Vulnerable to SARS-CoV-2: A Multicenter Study during the COVID-19 Outbreak. Cancer Discov. 2020;10(6):783-791.
16. Zhang L, Zhu F, Xie L, et al. Clinical characteristics of COVID-19-infected cancer patients: a retrospective case study in three hospitals within Wuhan, China. Ann Oncol. 2020;31(7):894-901.
17. Tian J, Yuan X, Xiao J, et al. Clinical characteristics and risk factors associated with COVID-19 disease severity in patients with cancer in Wuhan, China: a multicentre, retrospective, cohort study. Lancet Oncol. 2020;21(7):893-903.

48
18. Zhang H, Wang L, Chen Y, et al. Outcomes of novel coronavirus disease 2019 (COVID-19) infection in 107 patients with cancer from Wuhan, China. Cancer. 2020;126(17):4023-4031.
19. Yang K, Sheng Y, Huang C, et al. Clinical characteristics, outcomes, and risk factors for mortality in patients with cancer and COVID-19 in Hubei, China: a multicentre, retrospective, cohort study. Lancet Oncol. 2020;21(7):904-913.
20. Liu C, Li L, Song K, et al. A nomogram for predicting mortality in patients with COVID-19 and solid tumors: a multicenter retrospective cohort study. J Immunother Cancer. 2020;8(2).
21. Rogado J, Obispo B, Pangua C, et al. Covid-19 transmission, outcome and associated risk factors in cancer patients at the first month of the pandemic in a Spanish hospital in Madrid. Clin Transl Oncol. 2020;22(12):2364-2368.
22. Yarza R, Bover M, Paredes D, et al. SARS-CoV-2 infection in cancer patients undergoing active treatment: analysis of clinical features and predictive factors for severe respiratory failure and death. Eur J Cancer. 2020;135:242-250.
23. Miyashita H, Mikami T, Chopra N, et al. Do patients with cancer have a poorer prognosis of COVID-19? An experience in New York City. Ann Oncol. 2020;31(8):1088-1089.
24. Robilotti EV, Babady NE, Mead PA, et al. Determinants of COVID-19 disease severity in patients with cancer. Nat Med. 2020;26(8):1218-1223.
25. Brar G, Pinheiro LC, Shusterman M, et al. COVID-19 Severity and Outcomes in Patients With Cancer: A Matched Cohort Study. J Clin Oncol. 2020;38(33):3914-3924.
26. Shoumariyeh K, Biavasco F, Ihorst G, et al. Covid-19 in patients with hematological and solid cancers at a Comprehensive Cancer Center in Germany. Cancer Med. 2020;9(22):8412-8422.
27. Garrone O, Denaro N, Ruatta F, et al. Treating patients with cancer amidst the COVID-19 pandemic: experience of a regional hospital in the Piedmont region in northern Italy. Tumori. 2020;106(5):427-431.
28. Buglione M, Spiazzi L, Guerini AE, et al. Two months of radiation oncology in the heart of Italian "red zone" during COVID-19 pandemic: paving a safe path over thin ice. Radiat Oncol. 2020;15(1):191.
29. Nichetti F, Bini M, Ambrosini M, et al. COVID-19 risk for patients undergoing anticancer treatment at the outpatient clinic of the National Cancer Institute of Milan: the COVINT study. ESMO Open. 2020;5(Suppl 3).
30. Lee LY, Cazier JB, Angelis V, et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: a prospective cohort study. Lancet. 2020;395(10241):1919-1926.
31. Lee LYW, Cazier JB, Starkey T, et al. COVID-19 prevalence and mortality in patients with cancer and the effect of primary tumour subtype and patient demographics: a prospective cohort study. Lancet Oncol. 2020;21(10):1309-1316.
32. de Azambuja E, Brandão M, Wildiers H, et al. Impact of solid cancer on in-hospital mortality overall and among different subgroups of patients with COVID-19: a nationwide, population-based analysis. ESMO Open. 2020;5(5).
33. Kuderer NM, Choueiri TK, Shah DP, et al. Clinical impact of COVID-19 on patients with cancer (CCC19): a cohort study. Lancet. 2020;395(10241):1907-1918.
34. Al-Shamsi HO, Alhazzani W, Alhuraiji A, et al. A Practical Approach to the Management of Cancer Patients During the Novel Coronavirus Disease 2019 (COVID-

49
19) Pandemic: An International Collaborative Group. Oncologist. 2020;25(6):e936-e945.
35. El-Shakankery KH, Kefas J, Crusz SM. Caring for our cancer patients in the wake of COVID-19. Br J Cancer. 2020;123(1):3-4.
36. Jazieh AR, Chan SL, Curigliano G, et al. Delivering Cancer Care During the COVID-19 Pandemic: Recommendations and Lessons Learned From ASCO Global Webinars. JCO Glob Oncol. 2020;6:1461-1471.
37. Raymond E, Thieblemont C, Alran S, Faivre S. Impact of the COVID-19 Outbreak on the Management of Patients with Cancer. Target Oncol. 2020;15(3):249-259.
38. Curigliano G, Banerjee S, Cervantes A, et al. Managing cancer patients during the COVID-19 pandemic: an ESMO multidisciplinary expert consensus. Ann Oncol. 2020;31(10):1320-1335.
39. van de Haar J, Hoes LR, Coles CE, et al. Caring for patients with cancer in the COVID-19 era. Nat Med. 2020;26(5):665-671.
40. Slimano F, Baudouin A, Zerbit J, et al. Cancer, immune suppression and Coronavirus Disease-19 (COVID-19): Need to manage drug safety (French Society for Oncology Pharmacy [SFPO] guidelines). Cancer Treat Rev. 2020;88:102063.
41. European Society for Medical Oncology (ESMO); Lugano Switzerland; Cancer Patient
Management During the COVID-19 Pandemic. 2020;
https://www.esmo.org/guidelines/cancer-patient-management-during-the-covid-19-pandemic. Accessed 21/04/2021.
42. Segelov E, Underhill C, Prenen H, et al. Practical Considerations for Treating Patients With Cancer in the COVID-19 Pandemic. JCO Oncol Pract. 2020;16(8):467-482.
43. Consoli F, Cristini C, Guarinoni MG, et al. New models of care and multidimensional solutions for oncological patients in the post-acute SARS-COV-2 period: a "Second Phase" also for cancer patients. Eur Rev Med Pharmacol Sci. 2020;24(21):11445-11454.
44. Burki TK. Cancer guidelines during the COVID-19 pandemic. The Lancet. Oncology. 2020;21(5):629-630.
45. Overton J, Denton K, Frumovitz M, et al. Coronavirus (COVID-19): Patient experience-Administrative services on the frontline during crisis. Head Neck. 2020;42(7):1477-1481.
46. Tan J, Yang C. Prevention and control strategies for the diagnosis and treatment of cancer patients during the COVID-19 pandemic. Br J Cancer. 2020;123(1):5-6.
47. Porzio G, Cortellini A, Bruera E, et al. Home Care for Cancer Patients During COVID-19 Pandemic: The Double Triage Protocol. J Pain Symptom Manage. 2020;60(1):e5-e7.
48. Wang Z, Wang J, He J. Active and Effective Measures for the Care of Patients With Cancer During the COVID-19 Spread in China. JAMA Oncol. 2020;6(5):631-632.
49. Spiess PE, Greene J, Keenan RJ, Paculdo D, Letson GD, Peabody JW. Meeting the challenge of the 2019 novel coronavirus disease in patients with cancer. Cancer. 2020;126(14):3174-3175.
50. Slotman BJ, Lievens Y, Poortmans P, et al. Effect of COVID-19 pandemic on practice in European radiation oncology centers. Radiother Oncol. 2020;150:40-42.
51. Lobascio F, Caccialanza R, Monaco T, et al. Providing nutritional care to cancer patients during the COVID-19 pandemic: an Italian perspective. Support Care Cancer. 2020;28(9):3987-3989.

50
52. Zuliani S, Zampiva I, Tregnago D, et al. Organisational challenges, volumes of oncological activity and patients' perception during the severe acute respiratory syndrome coronavirus 2 epidemic. Eur J Cancer. 2020;135:159-169.
53. Montesi G, Di Biase S, Chierchini S, et al. Radiotherapy during COVID-19 pandemic. How to create a No fly zone: a Northern Italy experience. Radiol Med. 2020;125(6):600-603.
54. Caravatta L, Rosa C, Di Sciascio MB, et al. COVID-19 and radiation oncology: the experience of a two-phase plan within a single institution in central Italy. Radiat Oncol. 2020;15(1):226.
55. Gonnelli A, Montrone S, Cocuzza P, et al. Radiotherapy in the COVID-19 Pandemic Era. In Vivo. 2020;34(6):3731-3734.
56. Indini A, Aschele C, Cavanna L, et al. Reorganisation of medical oncology departments during the novel coronavirus disease-19 pandemic: a nationwide Italian survey. Eur J Cancer. 2020;132:17-23.
57. Torzilli G, Viganò L, Galvanin J, et al. A Snapshot of Elective Oncological Surgery in Italy During COVID-19 Emergency: Pearls, Pitfalls, and Perspectives. Ann Surg. 2020;272(2):e112-e117.
58. Jereczek-Fossa BA, Pepa M, Marvaso G, et al. COVID-19 outbreak and cancer radiotherapy disruption in Italy: Survey endorsed by the Italian Association of Radiotherapy and Clinical Oncology (AIRO). Radiother Oncol. 2020;149:89-93.
59. Ottaviano M, Curvietto M, Rescigno P, et al. Impact of COVID-19 outbreak on cancer immunotherapy in Italy: a survey of young oncologists. J Immunother Cancer. 2020;8(2).
60. de Joode K, Dumoulin DW, Engelen V, et al. Impact of the coronavirus disease 2019 pandemic on cancer treatment: the patients' perspective. Eur J Cancer. 2020;136:132-139.
61. Akuamoa-Boateng D, Wegen S, Ferdinandus J, Marksteder R, Baues C, Marnitz S. Managing patient flows in radiation oncology during the COVID-19 pandemic : Reworking existing treatment designs to prevent infections at a German hot spot area University Hospital. Strahlenther Onkol. 2020;196(12):1080-1085.
62. Matuschek C, Fischer JC, Combs SE, et al. Measures of infection prevention and incidence of SARS-CoV-2 infections in cancer patients undergoing radiotherapy in Germany, Austria and Switzerland. Strahlenther Onkol. 2020;196(12):1068-1079.
63. Reuter-Oppermann M, Müller-Polyzou R, Wirtz H, Georgiadis A. Influence of the pandemic dissemination of COVID-19 on radiotherapy practice: A flash survey in Germany, Austria and Switzerland. PLoS One. 2020;15(5):e0233330.
64. Gill S, Hao D, Hirte H, Campbell A, Colwell B. Impact of COVID-19 on Canadian medical oncologists and cancer care: Canadian Association of Medical Oncologists survey report. Curr Oncol. 2020;27(2):71-74.
65. Ning MS, McAleer MF, Jeter MD, et al. Mitigating the impact of COVID-19 on oncology: Clinical and operational lessons from a prospective radiation oncology cohort tested for COVID-19. Radiother Oncol. 2020;148:252-257.
66. Hui JYC, Yuan J, Teoh D, et al. Cancer Management During the COVID-19 Pandemic in the United States: Results From a National Physician Cross-sectional Survey. Am J Clin Oncol. 2020;43(10):679-684.
67. Onesti CE, Rugo HS, Generali D, et al. Oncological care organisation during COVID-19 outbreak. ESMO Open. 2020;5(4).

51
68. Lee S, Lim AR, Kim MJ, et al. Innovative countermeasures can maintain cancer care continuity during the coronavirus disease-2019 pandemic in Korea. Eur J Cancer. 2020;136:69-75.
69. Alexander M, Jupp J, Chazan G, O'Connor S, Chan A. Global oncology pharmacy response to COVID-19 pandemic: Medication access and safety. J Oncol Pharm Pract. 2020;26(5):1225-1229.
70. Ürün Y, Hussain SA, Bakouny Z, et al. Survey of the Impact of COVID-19 on Oncologists' Decision Making in Cancer. JCO Glob Oncol. 2020;6:1248-1257.
71. Jazieh AR, Akbulut H, Curigliano G, et al. Impact of the COVID-19 Pandemic on Cancer Care: A Global Collaborative Study. JCO Glob Oncol. 2020;6:1428-1438.
72. Chazan G, Franchini F, Alexander M, et al. Impact of COVID-19 on cancer service delivery: results from an international survey of oncology clinicians. ESMO Open. 2020;5(6).
73. Chakraborty M, Pandey M. Caring for cancer patients in the Covid pandemic: choosing between the devil and deep sea. World J Surg Oncol. 2020;18(1):220.
74. World Health Organizarion (WHO); Genebra, Switzerland; Coronavirus disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. 2021; https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports. Accessed 21/04/2021.
75. Sud A, Jones ME, Broggio J, et al. Collateral damage: the impact on outcomes from cancer surgery of the COVID-19 pandemic. Ann Oncol. 2020;31(8):1065-1074.