marco aurélio fraga borges neurologista agosto, 2015 · marco aurélio fraga borges neurologista...
TRANSCRIPT
Marco Aurélio Fraga Borges Neurologista
Agosto, 2015
JACC March 17, 2015
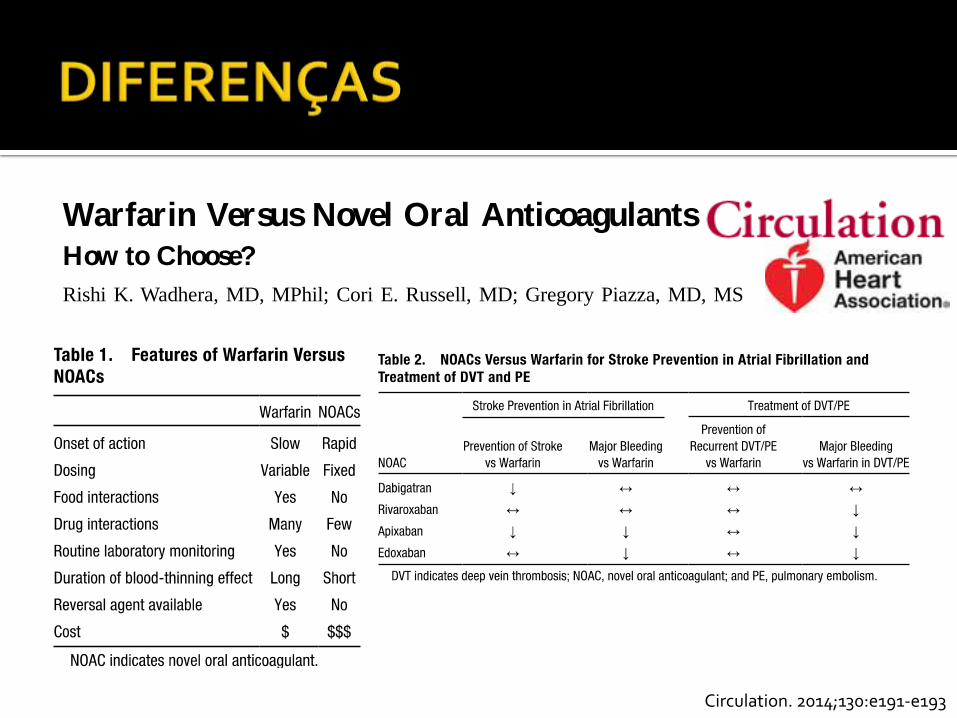
Circulation. 2014;130:e191-e193
e191
Anticoagulants (commonly called
blood thinners) are medications that
interact with the body’s natural blood-
clotting system to treat and prevent
abnormal blood clots. Anticoagulants are
used in patients who have blood clots in
the legs (called deep vein thrombosis or
DVT) or in the lungs (called pulmonary
embolism or PE), other types of blood
clots in the arteries or veins, an irregular
heart rhythm called atrial fibrillation that
increases the risk of stroke, and mechan-
ical heart valves. For decades, warfarin
(also known as Coumadin) was the pri-
mary anticoagulant used. Recently, sev-
eral other medications known as novel
oral anticoagulants (NOACs) have been
studied and released on the market as
alternatives to warfarin. Given the num-
ber of choices now available for patients
who need anticoagulants, the benefits,
risks, side effects, and convenience of
each anticoagulant must be carefully
considered.
How Do NOACs Differ From Warfarin?
Warfarin treats and prevents blood
clots by decreasing the production of
several clotting proteins that rely on
vitamin K. Warfarin is taken by mouth
once daily, and the dose varies depend-
ing on inherited factors, reason for the
medication, and diet (Table 1). Because
of the variations in doses needed for
each patient, warfarin requires frequent
laboratory monitoring and dose adjust-
ment to maintain blood levels within
the target range (called the international
normalized ratio or INR). Below target
blood levels, patients have an increased
risk of clotting. Above target blood lev-
els, the risk of bleeding increases. As
with all anticoagulants, warfarin use
increases the risk of bleeding. If this
happens, vitamin K or various blood
products can be given to replace the
clotting factors affected by warfarin.
NOACs work by targeting individual
clotting proteins. They do not require
laboratory monitoring or dose adjust-
ment because they reach predictable
levels in most patients (Table 1). They
are also shorter-acting than warfarin. If
a dose of warfarin is missed, a patient’s
blood may still be adequately thinned
because it takes several days for the
anticoagulant effect to wear off. In con-
trast, if a dose of a NOAC is missed,
patients quickly lose the anticoagulant
effect and are unprotected from blood
clots. Unlike warfarin, no specific anti-
dotes are currently available to reverse
the blood-thinning effect of NOACs
in patients who are bleeding. Because
its anticoagulant effect lasts for days,
warfarin must be stopped several days
before surgery and certain other proce-
dures. During interruption of warfarin
treatment, patients may need to give
themselves injections with shorter-act-
ing anticoagulants or be admitted to the
hospital for intravenous anticoagulants
to prevent blood clots (often called
bridging). The NOACs rarely require
bridging because they are shorter act-
ing and can be safely stopped a day or
two before surgery or procedures.
NOACs are taken once or twice daily
(depending on the NOAC being used and
the condition being treated). Although
NOACs have been evaluated for stroke
prevention in atrial fibrillation and treat-
ment and prevention of DVTs and PEs,
they are contraindicated for treatment in
patients with mechanical heart valves.
WarfarinWarfarin has been used for decades to
treat patients with atrial fibrillation,
(Circulation. 2014;130:e191-e193.)© 2014 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.114.010426
The information contained in this Circulation Cardiology Patient Page is not a substitute for medical advice, and the American Heart Association recommends consultation with your doctor or healthcare professional.
From the Cardiovascular Division (G.P.) and Department of Medicine (R.K.W., C.E.R.), Brigham and Women’s Hospital, Harvard Medical School, Boston, MA.
Correspondence to Gregory Piazza, MD, MS, Cardiovascular Division, Brigham and Women’s Hospital, 75 Francis St, Boston, MA 02115. E-mail [email protected]
Warfarin Versus Novel Oral AnticoagulantsHow to Choose?
Rishi K. Wadhera, MD, MPhil; Cori E. Russell, MD; Gregory Piazza, MD, MS
CARDIOLOGY PATIENT PAGE
by guest on August 17, 2015http://circ.ahajournals.org/Downloaded from
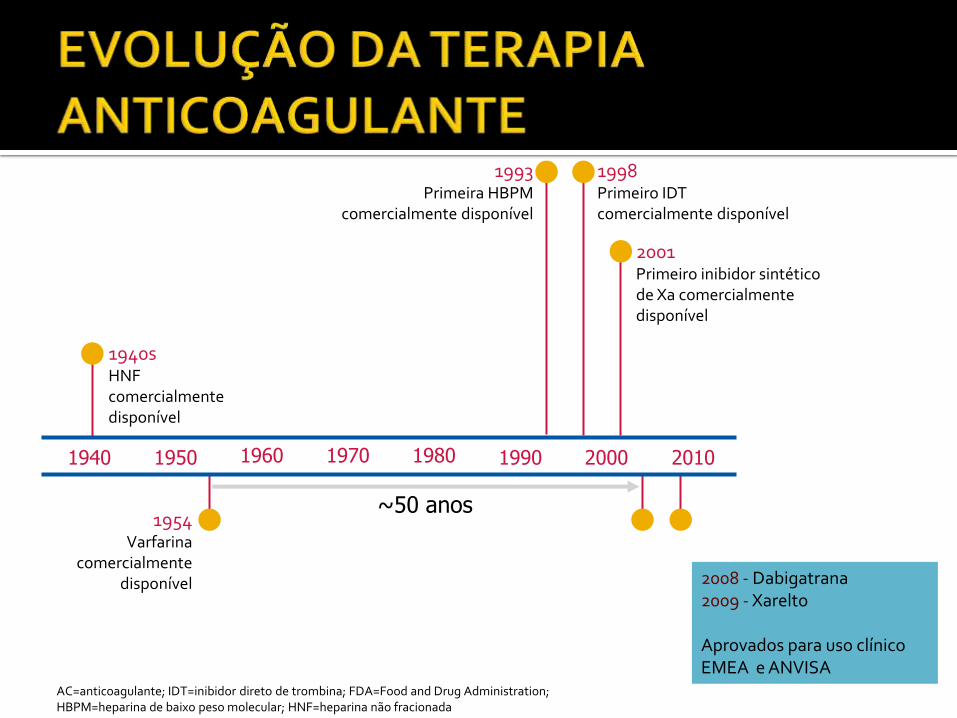
1960 1970 1980 1940 2010 1950 1990 2000
1940s HNF comercialmente disponível
1954 Varfarina
comercialmente disponível
1993 Primeira HBPM
comercialmente disponível
1998 Primeiro IDT comercialmente disponível
2001 Primeiro inibidor sintético de Xa comercialmente disponível
~50 anos
2008 - Dabigatrana 2009 - Xarelto Aprovados para uso clínico EMEA e ANVISA
AC=anticoagulante; IDT=inibidor direto de trombina; FDA=Food and Drug Administration; HBPM=heparina de baixo peso molecular; HNF=heparina não fracionada
Journal of Thrombosis and Haemostasis 2013, 11: 177–179
Escolher o indivíduo ADEQUADO para ser anticoagulado na intensidade ADEQUADA com
a droga ADEQUADA.
J Am Coll Cardiol. 2014;64(21):2246-2280
RECOMENDAÇÕES CLASSE I
RECOMENDAÇÕES CLASSE III
Stroke. 2014;45:2160-2236 Lancet. 2009 Oct 10;374(9697):1271-83
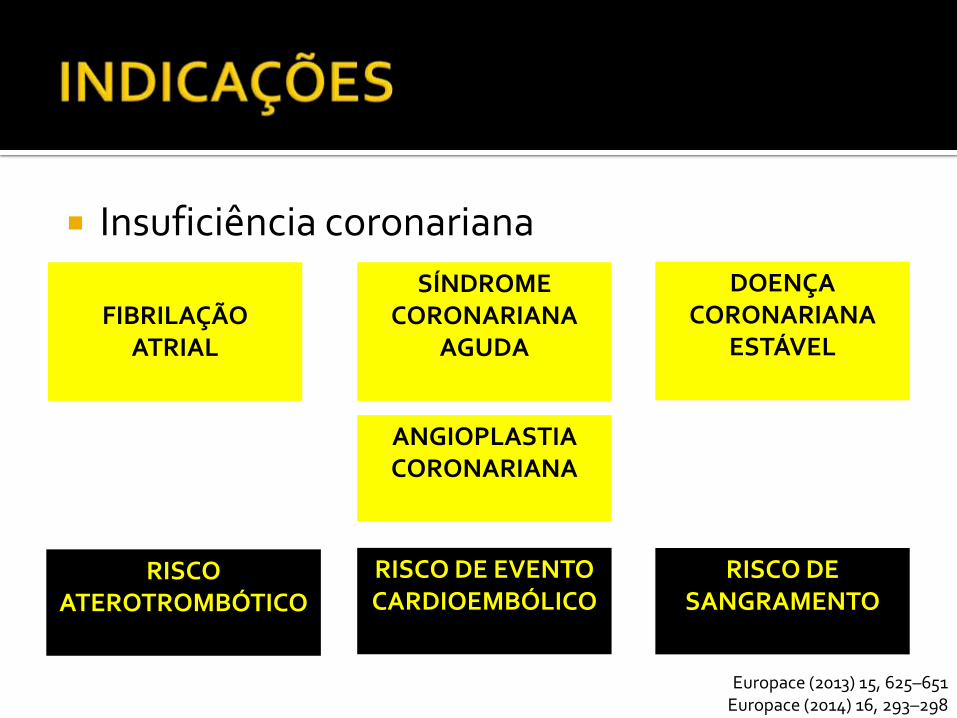
Insuficiência coronariana
FIBRILAÇÃO
ATRIAL
SÍNDROME CORONARIANA
AGUDA
DOENÇA CORONARIANA
ESTÁVEL
Europace (2013) 15, 625–651 Europace (2014) 16, 293–298
ANGIOPLASTIA CORONARIANA
RISCO DE EVENTO CARDIOEMBÓLICO
RISCO ATEROTROMBÓTICO
RISCO DE SANGRAMENTO
Lancet. 2009 Oct 10;374(9697):1271-83 Europace (2013) 15, 625–651
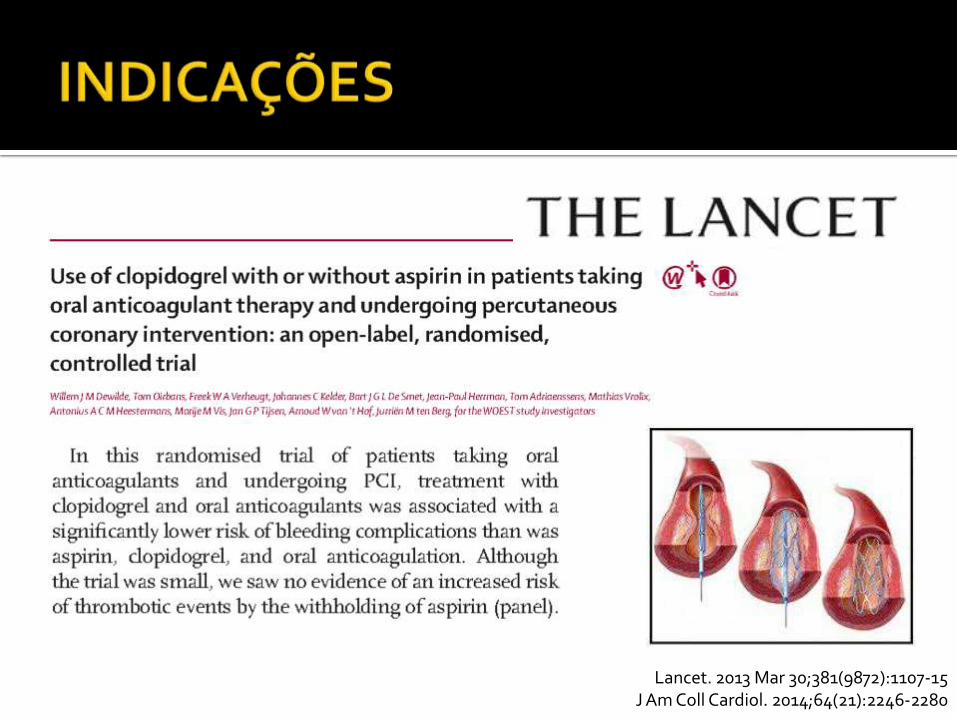
Lancet. 2013 Mar 30;381(9872):1107-15 J Am Coll Cardiol. 2014;64(21):2246-2280
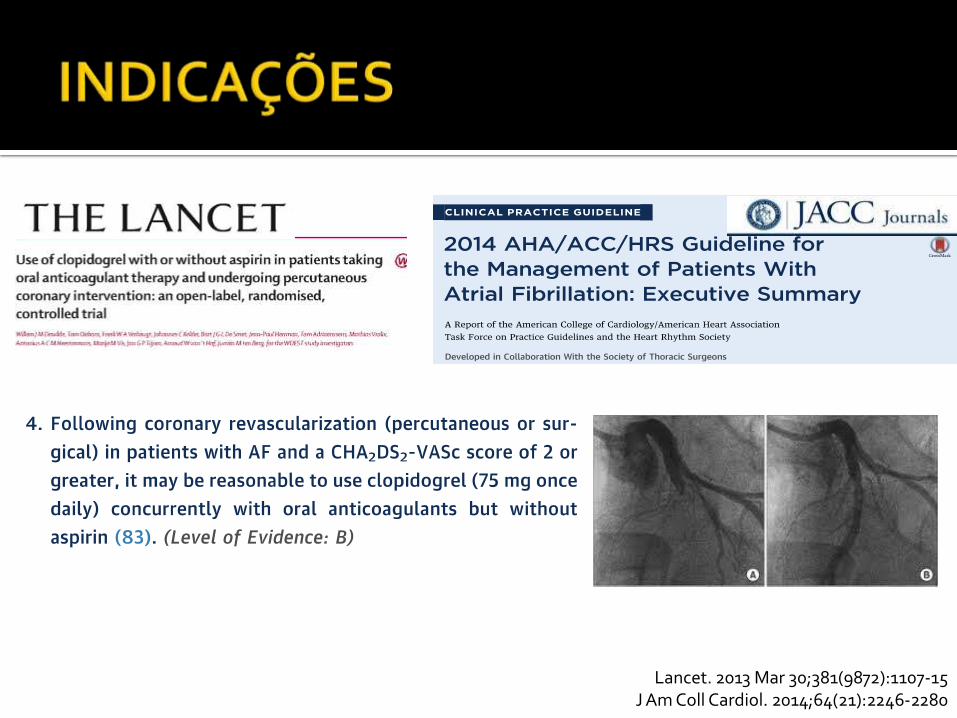
Lancet. 2013 Mar 30;381(9872):1107-15 J Am Coll Cardiol. 2014;64(21):2246-2280
Europace (2013) 15, 625–651
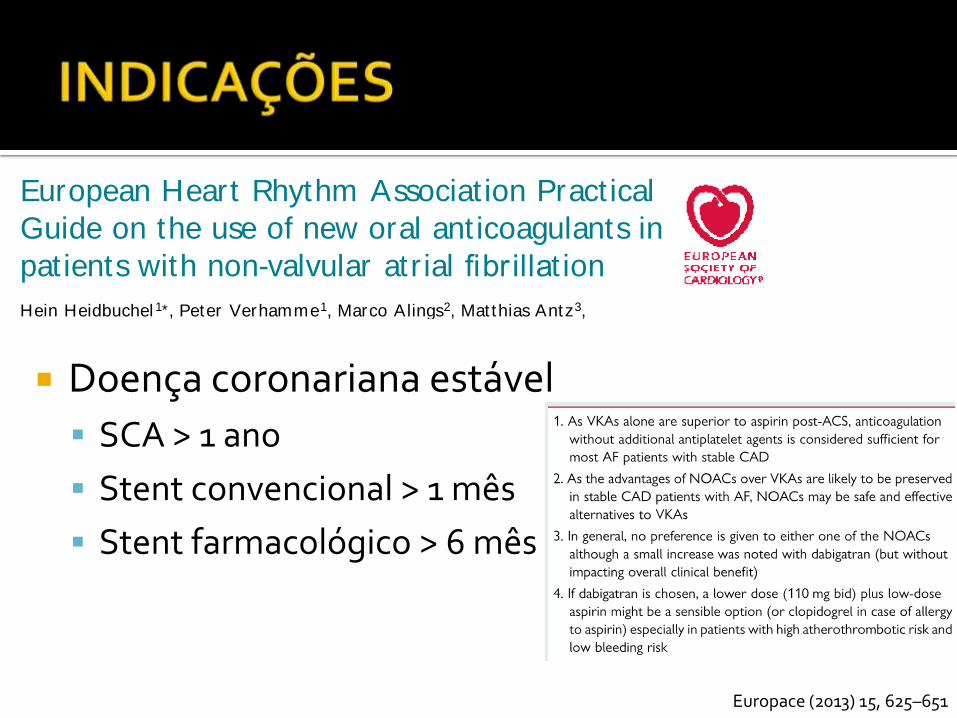
EHRA PRACTICAL GUIDE
European Heart Rhythm Associat ion Pract ical
Guide on the use of new oral ant icoagulants in
pat ients with non-valvular atr ial fibrillat ion
Hein Heidbuchel 1*, Peter Verhamme1, Marco Alings2, Mat thias Antz3,
W erner Hacke4, Jonas Oldgren5, Peter Sinnaeve1, A. John Camm 6,
and Paulus Kirchhof7,8
1Department of Cardiovascular Medicine, University Hospital Gasthuisberg, University of Leuven, Leuven, Belgium; 2Department of Cardiology, Amphia Ziekenhuis, Breda,
Netherlands; 3Department of Cardiology, Klinikum Oldenburg, Oldenburg, Germany; 4Department of Neurology, Ruprecht Karls Universitat, Heidelberg, Germany; 5Uppsala
Clinical Research Center and Dept of Medical Sciences, Uppsala University, Uppsala, Sweden; 6Clinical Cardiology, St George’s University, London, UK; 7University of Birmingham
Centre for Cardiovascular Sciences, Birmingham, UK; and 8Department of Cardiology and Angiology, University of Munster, Germany
Received 7 November 2012; accepted after revision 18 March 2013
New oral anticoagulants (NOACs) are an alternative for vitamin K antagonists (VKAs) to prevent stroke in patients with non-valvular atrial
fibrillation (AF). Both physiciansand patientswill have to learn how to use these drugseffectively and safely in clinical practice. Many unresolved
questions on how to optimally use these drugs in specific clinical situations remain. The European Heart Rhythm Association set out to co-
ordinate aunified way of informingphysicianson the use of the different NOACs. A writinggroup listed 15 topicsof concrete clinical scenarios
and formulated as practical answers as possible based on available evidence. The 15 topics are: (1) Practical start-up and follow-up scheme for
patientson NOACs; (2) How to measure the anticoagulant effect of NOACs; (3) Drug–druginteractionsand pharmacokineticsof NOACs; (4)
Switching between anticoagulant regimens; (5) Ensuring compliance of NOAC intake; (6) How to deal with dosing errors; (7) Patients with
chronic kidney disease; (8) What to do if there is a (suspected) overdose without bleeding, or a clotting test is indicating a risk of bleeding?
(9) Management of bleeding complications; (10) Patients undergoing a planned surgical intervention or ablation; (11) Patients undergoing an
urgent surgical intervention; (12) Patients with AF and coronary artery disease; (13) Cardioversion in a NOAC-treated patient; (14) Patients
presenting with acute stroke while on NOACs; (15) NOACs vs. VKAs in AF patients with a malignancy. Since new information is becoming
available at a rapid pace, an EHRA Web site with the latest updated information accompanies this text (www.NOACforAF.eu).- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywor ds Atrial fibrillation † Anticoagulation † Stroke † Bleeding † Pharmacology
Int roduct ion
New oral anticoagulants (NOACs) have emerged as an alternative
for vitamin K antagonists (VKAs) for thromboembolic prevention
in patients with non-valvular atrial fibrillation (AF). This will have
an impact on many practical considerations in the daily manage-
ment of these patients. Although very promising in many regards
(predictable effect without need for monitoring, fewer food and
drug interactions, shorter plasma half-life, and an improved effi-
cacy/safety ratio), the proper use of NOACs will require new
approaches in many daily aspects. Whereas the 2010 ESC Guide-
lines (and the 2012 Update)1,2 mainly discuss the indications for
anticoagulation in general (e.g. based on the CHA2DS2-VASc
score) and of NOAC in particular, they guide less on how to
* Corresponding author. Tel: + 32-16-34 42 48; fax: + 32-16-34 42 40, Email: [email protected]
Advisors: Azhar Ahmad, M.D. (Boehringer Ingelheim Pharma), Susanne Hess, M.D. (Bayer Healthcare Pharmaceuticals), Felix Munzel, Ph.D. (Daiichi Sankyo Europe), Markus
Schwertfeger, M.D. (Daiichi Sankyo Europe), Martin van Eickels, M.D. (Bayer Healthcare Pharmaceuticals), Jean-Philippe Verbist, M.D. (Bristol Myers Squibb/Pfizer).
Document reviewers: Coordinator: Antonio Raviele, Alliance to Fight Atrial Fibrillation (ALFA), Venice-Mestre, Italy.
Leandro Zimerman, M.D. (Hospital deClınicas de Porto Alegre, Brasil), Chern-En Chiang, Ph.D. (Taipei VeteransGeneral Hospital, Taiwan), HansDiener, Ph.D. (University of Essen,
Germany), Giuseppe Di Pasquale, Ph.D. (Ospedale Maggiore, Bologna, Italy), Stephan Hohnloser, Ph.D. (Klinikum der J.-W.-Goethe-Universitat, Frankfurt, Germany), Jean-Yves Le
Heuzey, Ph.D. (Hopital Europeen Georges Pompidou, Paris, France), Jose Lopez-Sendon, Ph.D. (Hospital Universitario La Paz. Madrid, Spain, Jonas Bjerring Olesen, Ph.D. (Copen-
hagen University Hospital Gentofte, Denmark), Frans H Rutten, Ph.D. (Julius Center UMC Utrecht, The Netherlands), Marco Valgimigli, Ph.D. (University Hospital of Ferrara, Italy),
Freek W.A. Verheugt, Ph.D. (Onze Lieve Vrouwe Gasthuis, Amsterdam, The Netherlands), Michael Brainin, Ph.D. (Klinische Medizin Und Praeventionsmedizin, Danube University
Krems, Austria), Kennedy Lees, Ph.D. (University of Glasgow, UK).
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2013. For permissions please email: [email protected].
Europace (2013) 15, 625–651
doi:10.1093/europace/eut083
by guest on January 19, 2015D
ownloaded from
Doença coronariana estável
SCA > 1 ano
Stent convencional > 1 mês
Stent farmacológico > 6 mês
Stroke. 2014;45:2160-2236 J Am Coll Cardiol. 2014;64(21):2246-2280
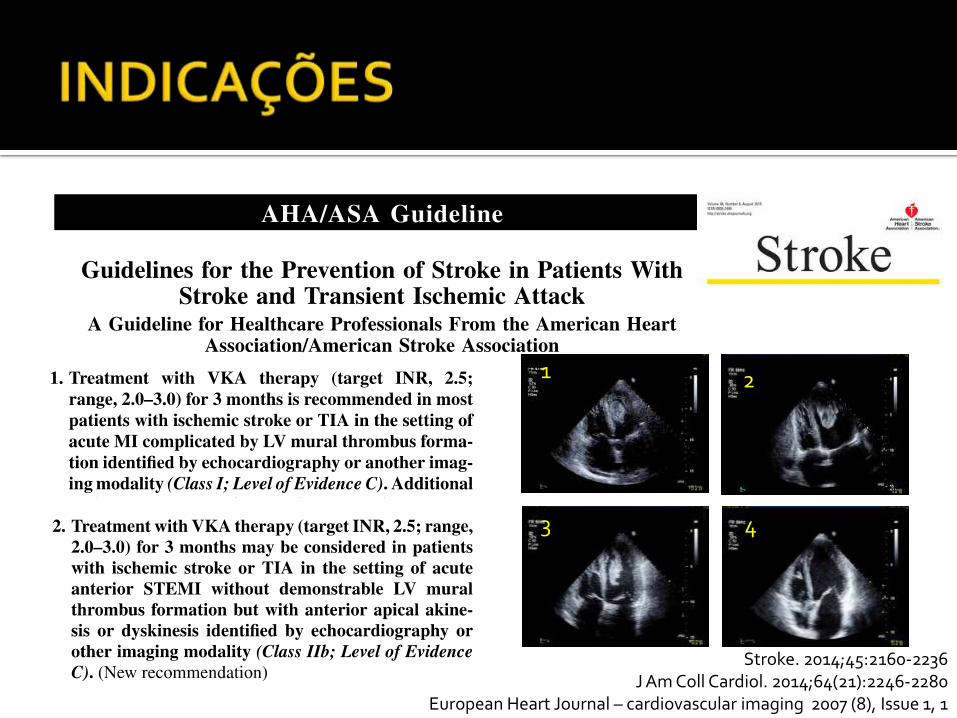
European Heart Journal – cardiovascular imaging 2007 (8), Issue 1, 1
1 2
4 3
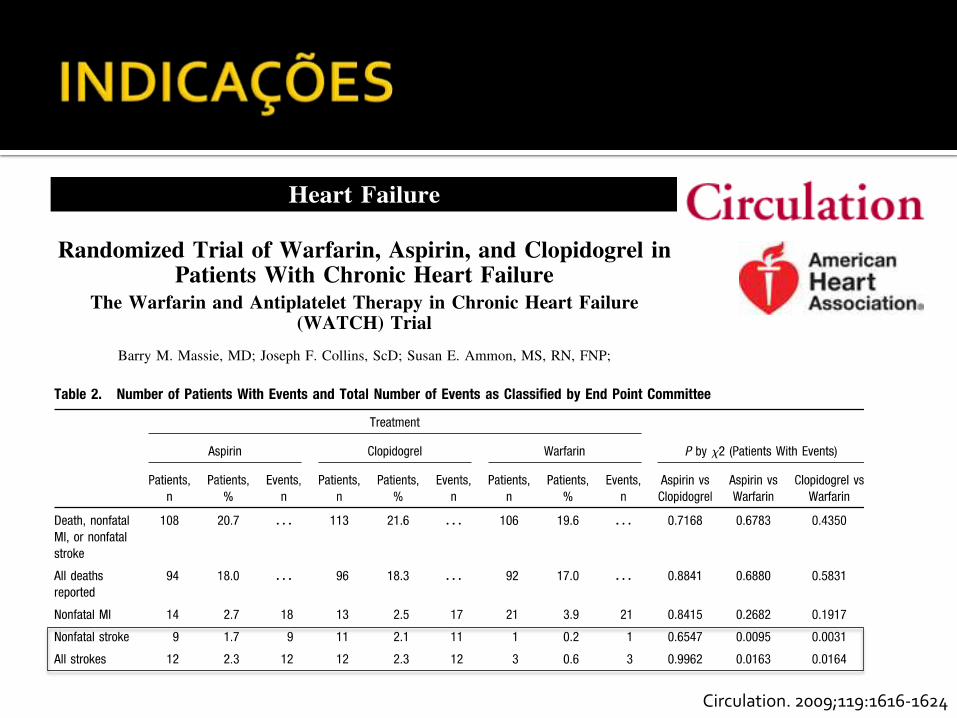
Circulation. 2009;119:1616-1624
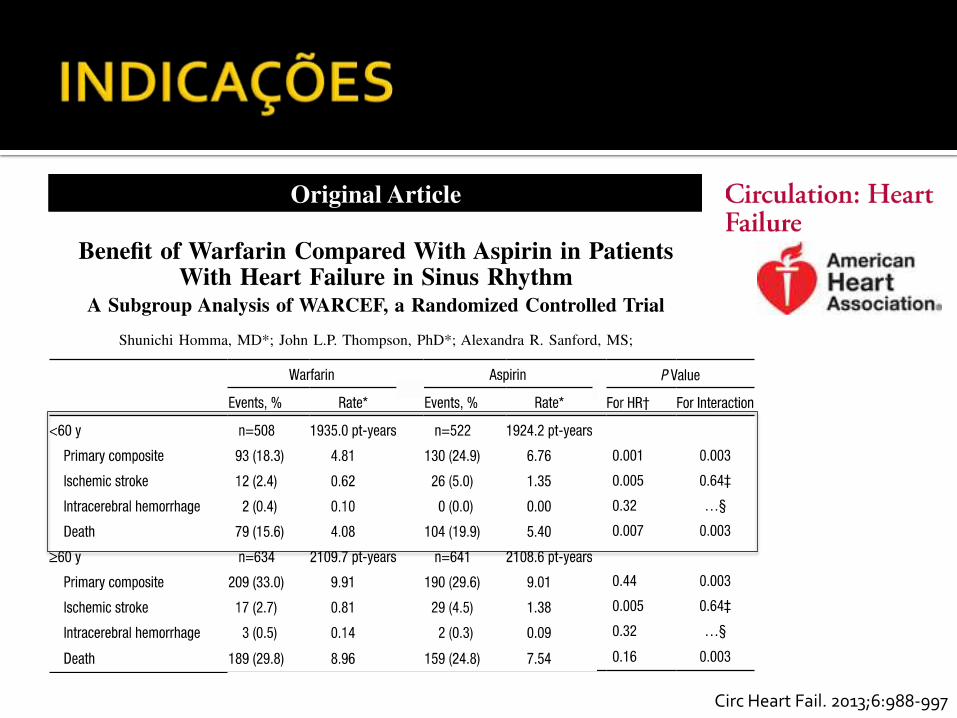
Circ Heart Fail. 2013;6:988-997
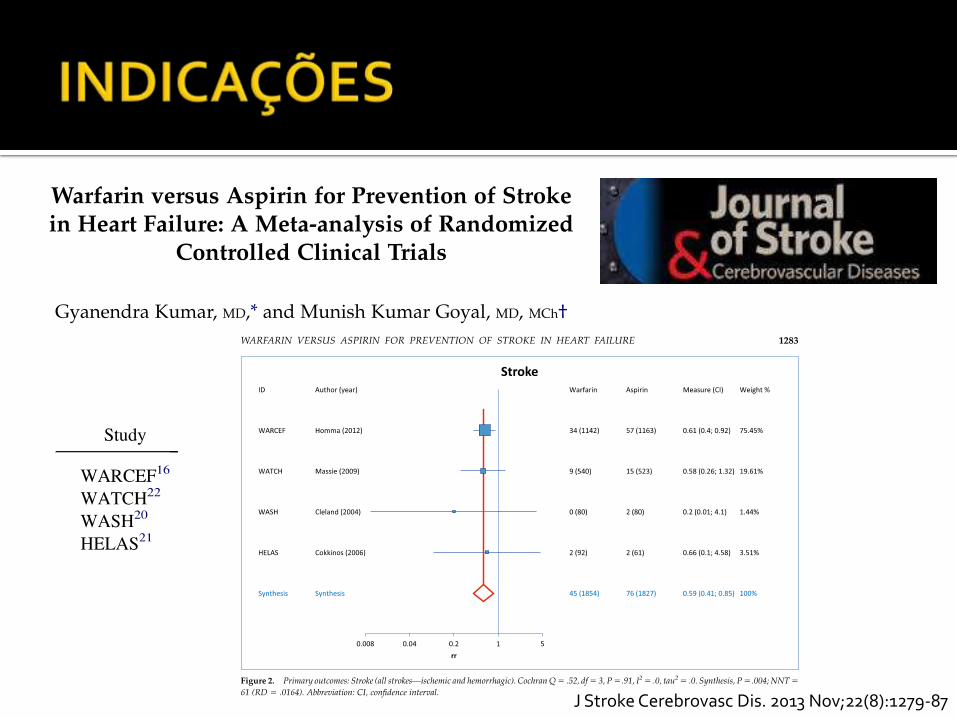
J Stroke Cerebrovasc Dis. 2013 Nov;22(8):1279-87
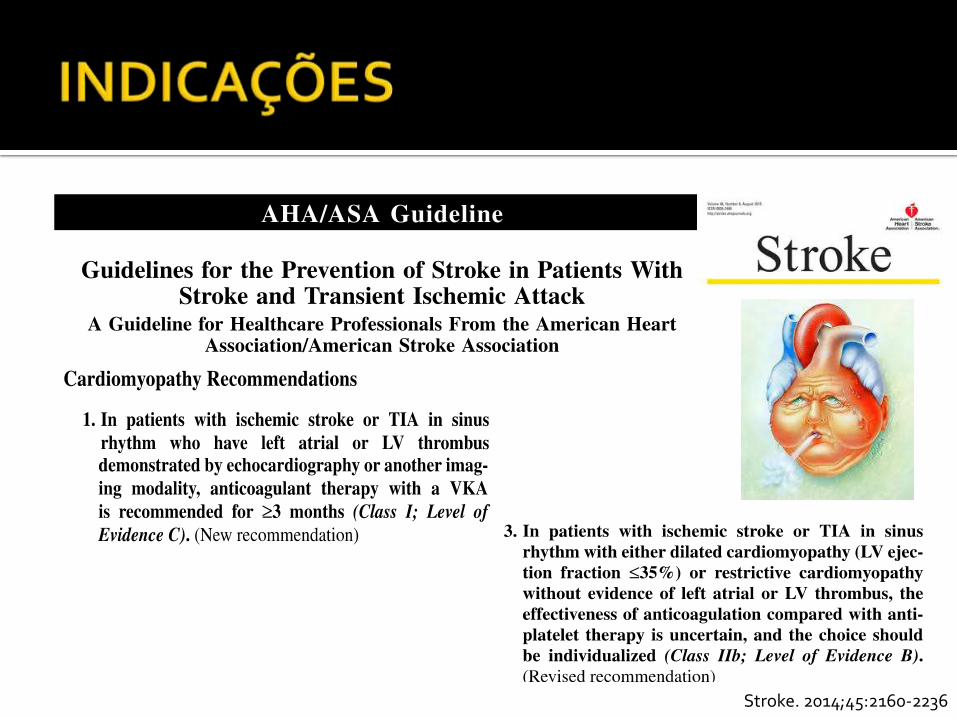
Stroke. 2014;45:2160-2236
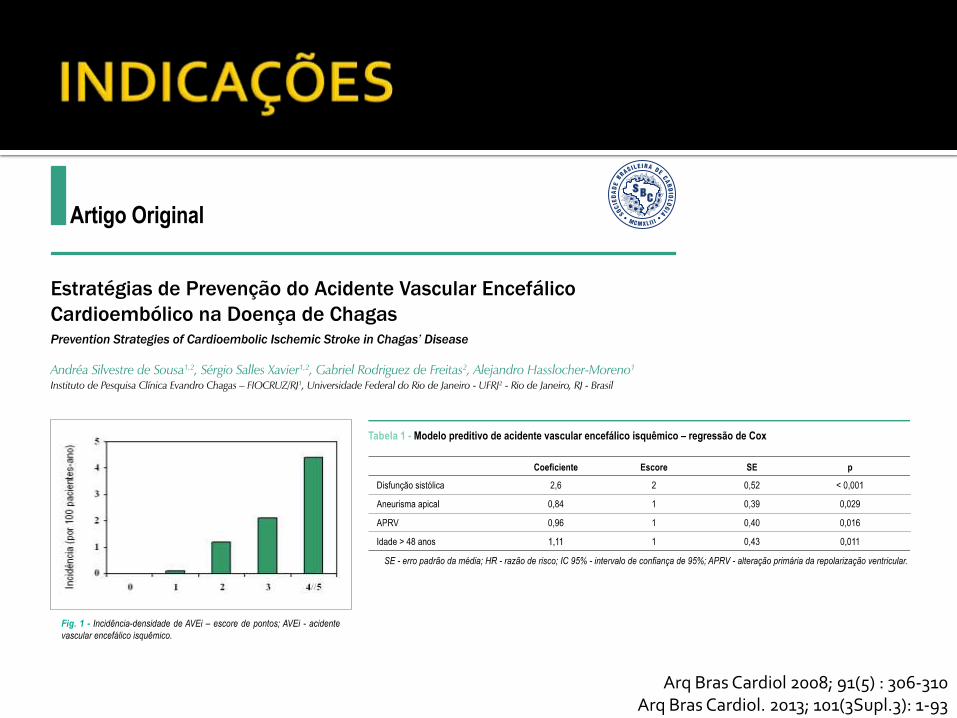
Arq Bras Cardiol 2008; 91(5) : 306-310 Arq Bras Cardiol. 2013; 101(3Supl.3): 1-93
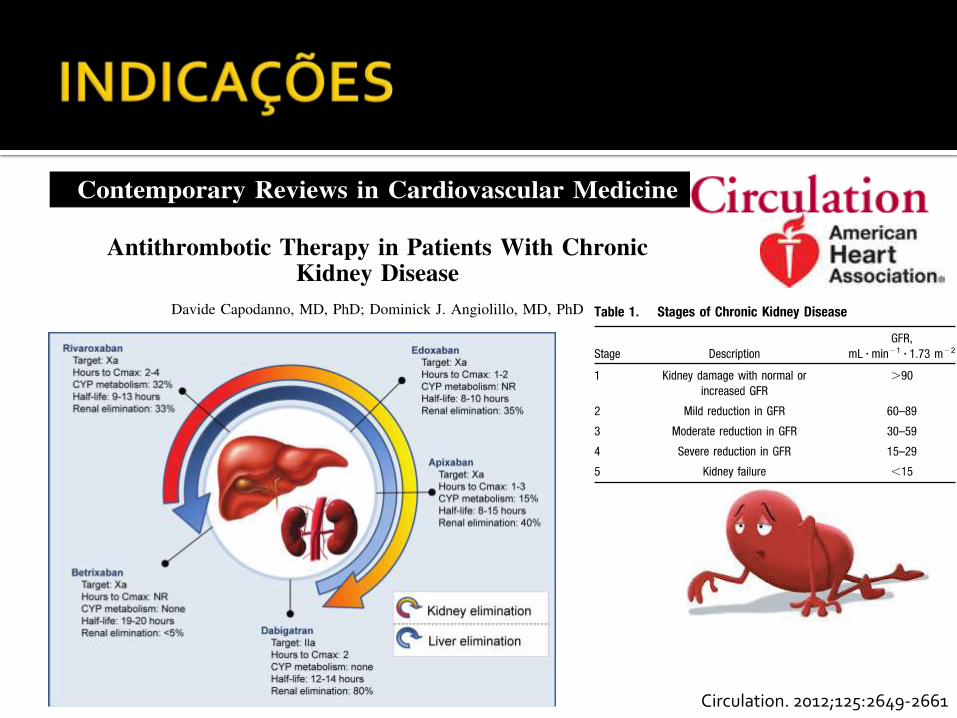
Circulation. 2012;125:2649-2661
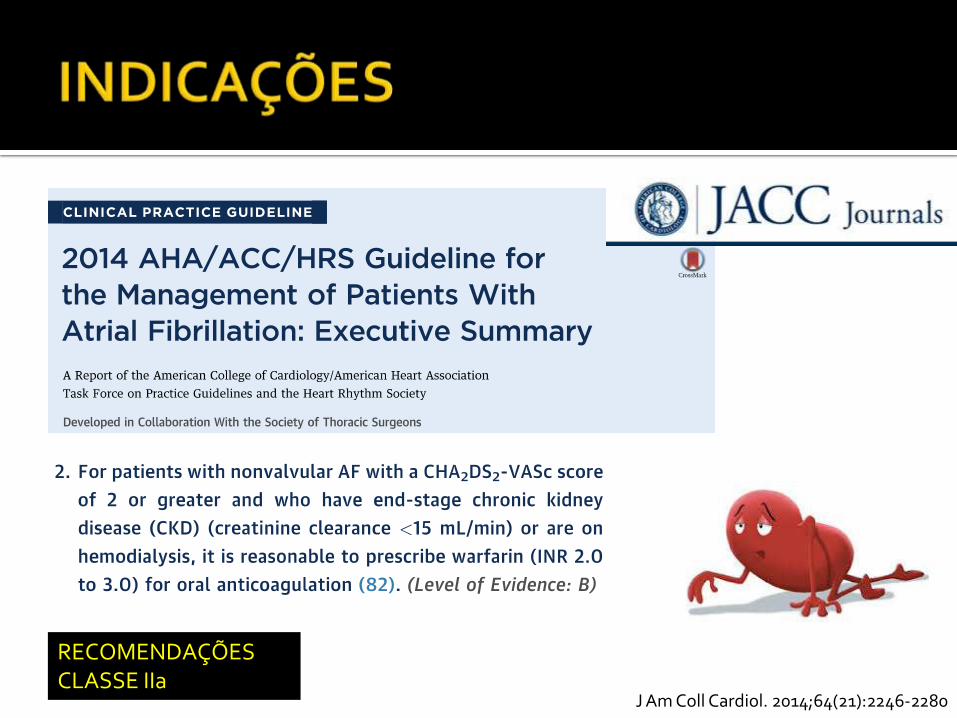
J Am Coll Cardiol. 2014;64(21):2246-2280
RECOMENDAÇÕES CLASSE IIa
Síndrome de anticorpo antifosfolípede
Diagnóstico confirmado e AVC/AIT prévio
Trombose venosa cerebral Gestação e amamentação
Heparina
Shimoli V. Shah and Brian F. GageCost-Effectiveness of Dabigatran for Stroke Prophylaxis in Atrial Fibrillation
ISSN: 1524-4539 Copyright © 2011 American Heart Association. All rights reserved. Print ISSN: 0009-7322. Online
72514Circulation is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX
doi: 10.1161/CIRCULATIONAHA.110.9856552011, 123:2562-2570: originally published online May 23, 2011Circulation
http://circ.ahajournals.org/content/123/22/2562located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://www.lww.com/reprintsReprints: Information about reprints can be found online at [email protected]. E-mail:
Fax:Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters http://circ.ahajournals.org//subscriptions/Subscriptions: Information about subscribing to Circulation is online at
at CONS AUSTRIAN NAT CONSORTIUM on July 12, 2011http://circ.ahajournals.org/Downloaded from
Baixo risco de AVC (CHADS2 = 0)
Alto risco de AVC (CHADS2 > 3)
Médio risco de AVC (CHADS2 = 1-2)
Risco de sangramento 6% ao ano
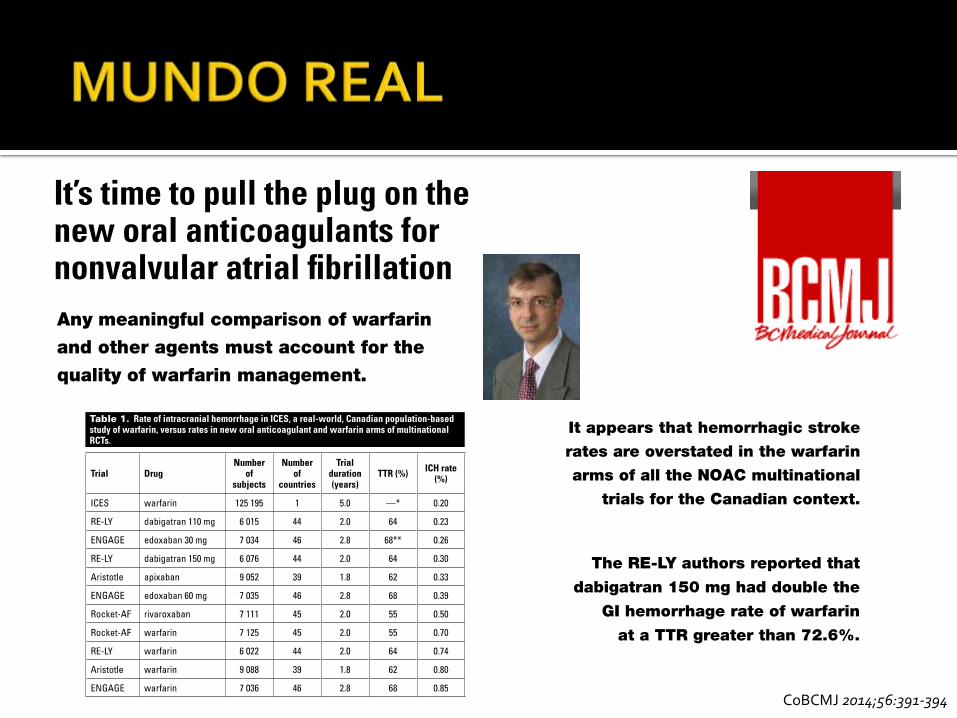
CoBCMJ 2014;56:391-394
Avaliação de custo efetividade É efetiva e segura Sem bem tolerada previamente não há
necessidade de troca, que inclusive nesse caso não é recomendada
Prezar mais a discussão de tratamento com o paciente