jembi health systems - moasis.org.mz · improving hospital systems in mozambique ... afecções do...
TRANSCRIPT

Designing Better Hospital Mortality Systems
Improving hospital systems in Mozambique ACHIEVEMENTS, CHALLENGES & OPPORTUNITIES
2006-2015
Dra Cidália Baloi, MOH
Dra. Esperança Nhagumbe, MOJ
Mr. Ivan Mabote, UEM-Moasis/Jembi
(on behalf of Dr. Alessandro Campione)
Ministério da Saude
CAIRO, EGYPT 2015
Ministério da Justiça

MOASIS is a non-profit organization of University Eduardo Mondlane, Living Lab created and
supported entirely by JEMBI with support of IDRC, CDC, WHO, Rockefeller and others ORG. We
aim to:
Strengthen HIS local capabilities involving the public, private and academic sectors
Reference and link between the MOH and public/private partners
Set up a South-South cooperation model
JEMBI/MOASIS model

Rationale
Before 2006: Mortality data collected through census/surveys and ad hoc studies
2006: pilot implementations of mortality and morbidity reporting using ICD-10
coding in 2 hospitals
MOH recognized the need for mortality statistics at hospital level and lacking of vital
statistics in the country
Strategy to address the need
MOH and partners revised entirely the national death registration system aiming to:
Strategic Priority: National level system for hospital mortality registration
Contribute to CRVS national reform (medium/long term)
Expansion to extra-hospital deaths in coordination with all CRVS stakeholders (Long
term)

Little pilot
Review of mortality system
In health sector
First ICD-10 Hospital Mortality System
Enhancement of electronic tool for
intra-hospital mortality register (SIS-ROH)
SIS-ROH expanding to all Mozambique
(till Sept 2015 = 44 sites, >100,000 records)
Strengthening of the whole
CRVS system and inter-institutional cooperation
Revision of Mortality registration System
2007
2008
2009
2013
2010
2015
Background (cont.)

CRVS COMPONENT
UEM-Moasis supported the creation Inter-institutional Group for Civil Registration and
Vital Statistics
Mozambique is one of the few African country that have this formalized and with a
Work Plan and is considered a best practice in the field of Mortality System
implementation.
Set up cooperation with Medical Research Council, WHO and STAT-SA
Promoted MoH as active member of WHO-FIC community
Constituted the Inter-institutional Vital Statistics Working Group (MoU) MOH, MOJ,
UEM/MOASIS, INE, MI.
Performed the In-depth assessment of CRVS and plan of action for CRVS Reform in
Mozambique
Participate to the CRVS reform
and working group
Visit to Stats SA
WHO-FIC
Conference
Cape Town
Planning stage (including the revision of the inquiry form for death registry
and cause of death)
Technical and financial support in the filed work (e.g. Boane)
Support and facilitated the consolidation meeting and training of the 2
components)
Support the draft, conclusion and approval from GITEV of the CRVS
operational plan
JEMBI-MOASIS active role in the CRVS in-depth
assessment
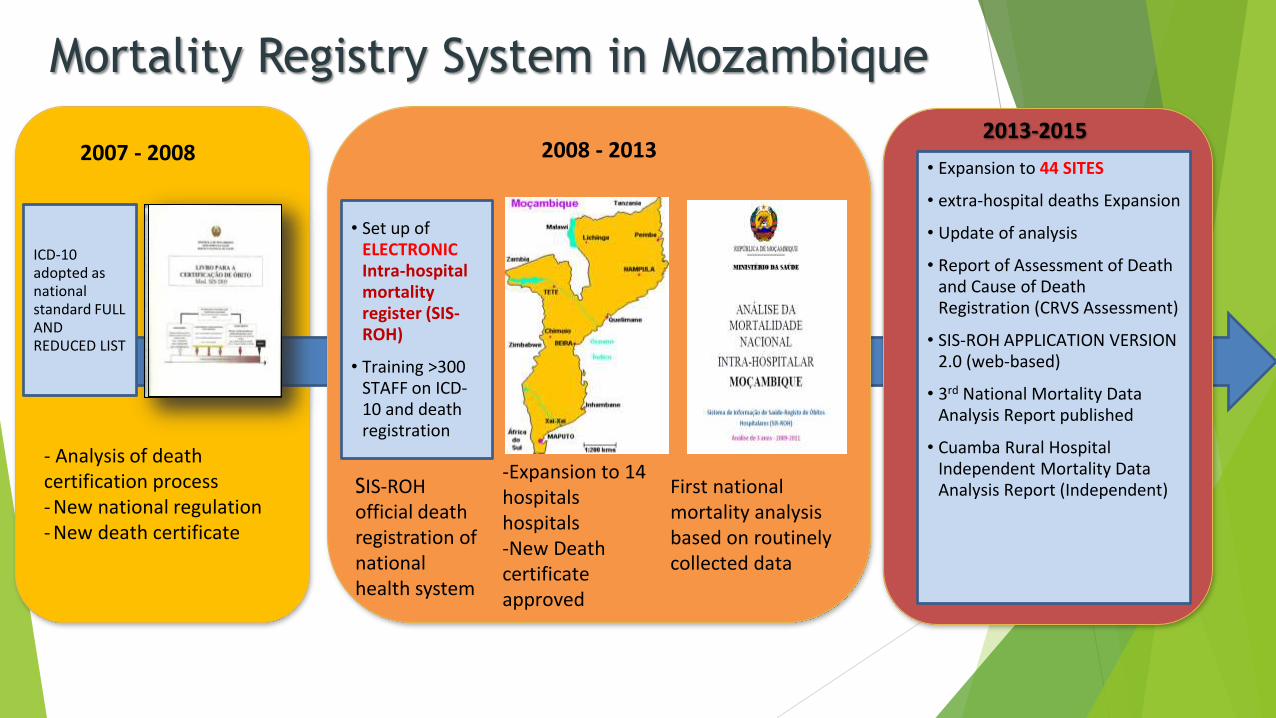
Mortality Registry System in Mozambique
- Analysis of death certification process - New national regulation - New death certificate
ICD-10 adopted as national standard FULL AND REDUCED LIST
2007 - 2008 2013-2015
• Expansion to 44 SITES
• extra-hospital deaths Expansion
• Update of analysis
• Report of Assessment of Death and Cause of Death Registration (CRVS Assessment)
• SIS-ROH APPLICATION VERSION 2.0 (web-based)
• 3rd National Mortality Data Analysis Report published
• Cuamba Rural Hospital Independent Mortality Data Analysis Report (Independent)
• Set up of ELECTRONIC Intra-hospital mortality register (SIS-ROH)
• Training >300 STAFF on ICD-10 and death registration
First national mortality analysis based on routinely collected data
2008 - 2013
-Expansion to 14 hospitals hospitals -New Death certificate approved
SIS-ROH official death registration of national health system

SUCCESS FACTORS

IT PROBLEM &
TECHNOLOGY
MANY FOCUS HERE
CLINIC/PUBLIC
HEALTH PROBLEM
NEED ASSESSMENT
PROJECT,
AGREEMENTS
FUNDRISING
COMMITMENT
REQUIREMENTS TRAINING
DEPLOYMENT
INTEGRATION
DATA QUALITY
PUBLICATION AND USE
MAINTENANCE
SUPPORT AND
SUSTAINABILITY
1. FOCUS ON THE WHOLE SYSTEM
CLINIC/PUBLIC
HEALTH PROBLEM
PROJECT,
AGREEMENTS
FUNDRISING
COMMITMENT
DEPLOYMENT
INTEGRATION

2. Institutional and Stakeholder support
Bottom-up approach
Start little, be pragmatic
Respond to needs of health workers first
Obtain concrete results and grow based on success
Local ownership and MOH commitment
Informatics solutions suitable to the country setting
basic computer technology
modular design, open source
minimum data set and introduction of standards
Creation of high level WG was a milestone to reach governmental
commitment to strengthen the overall CRVS
MOH/ UEM-MOASIS/JEMBI Collaboration for SIS-ROH
MOH has the ownership and provide overall direction and
supervision to all joint projects
UEM-MOASIS: UEM project design an all aspects, supports
development of system and software, implementation and
maintenance of all tools and training at the national level
Jembi: South African NGO, provides technical and financial
support to UEM-MOASIS
Institutional and Stakeholder support (cont.)
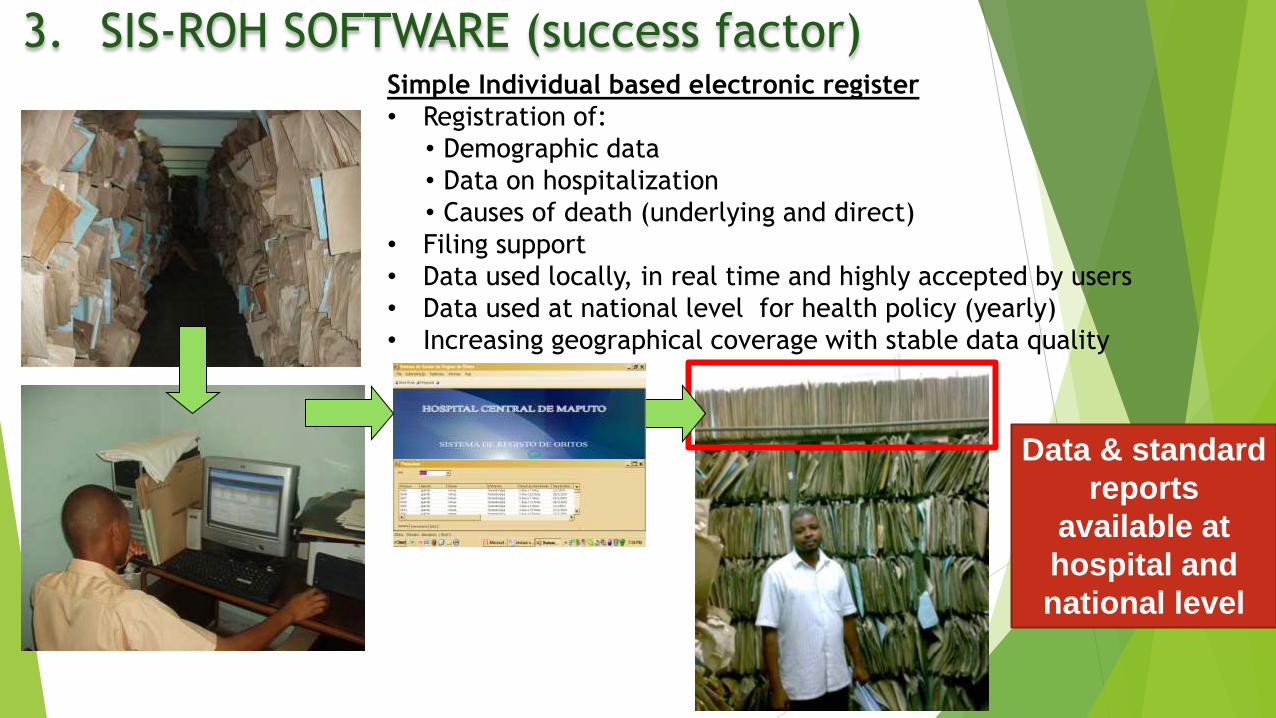
3. SIS-ROH SOFTWARE (success factor) Simple Individual based electronic register
• Registration of:
• Demographic data
• Data on hospitalization
• Causes of death (underlying and direct)
• Filing support
• Data used locally, in real time and highly accepted by users
• Data used at national level for health policy (yearly)
• Increasing geographical coverage with stable data quality
Data & standard
reports
available at
hospital and
national level

4. Country specific solutions
mICD SIS Compact
Station (Internet 3G) – Connectivity
issues mitigated, low virus
contamination, dedicated
to national HIS
ICD-10
Short list

5. IT In the Provinces
IT technicians supporting Health
facilities at the district and
provincial
Constant IT support and
maintenance, correction of bugs and
errors, helpdesk, troubleshooting to
ensure proper functioning of the HIS
and infrastructure at HF level
1 technician present in every
province of the country (MOH/DIS
with support from UEM-
MOASIS/JEMBI).
6. Quality Assurance
Mechanisms
Training:
At central and provincial level:
TOT on death certification and ICD-10
Training on SIS-ROH software for long term
maintenance
In each new implementation site:
Training on death certification and ICD-10 for clinical staff and Statistical unit staff
Training on SIS-ROH software for data management, filing, backup, maintenance
• SIS-ROH inbuilt data validations (cause of death coding according to age, gender, etc.)
• Routine data analyses, presentation/discussion and publication
• Data Quality assessments and supervision
Use of data at local and national level

OPPORTUNITIES &
FUTURE PROSPECTS
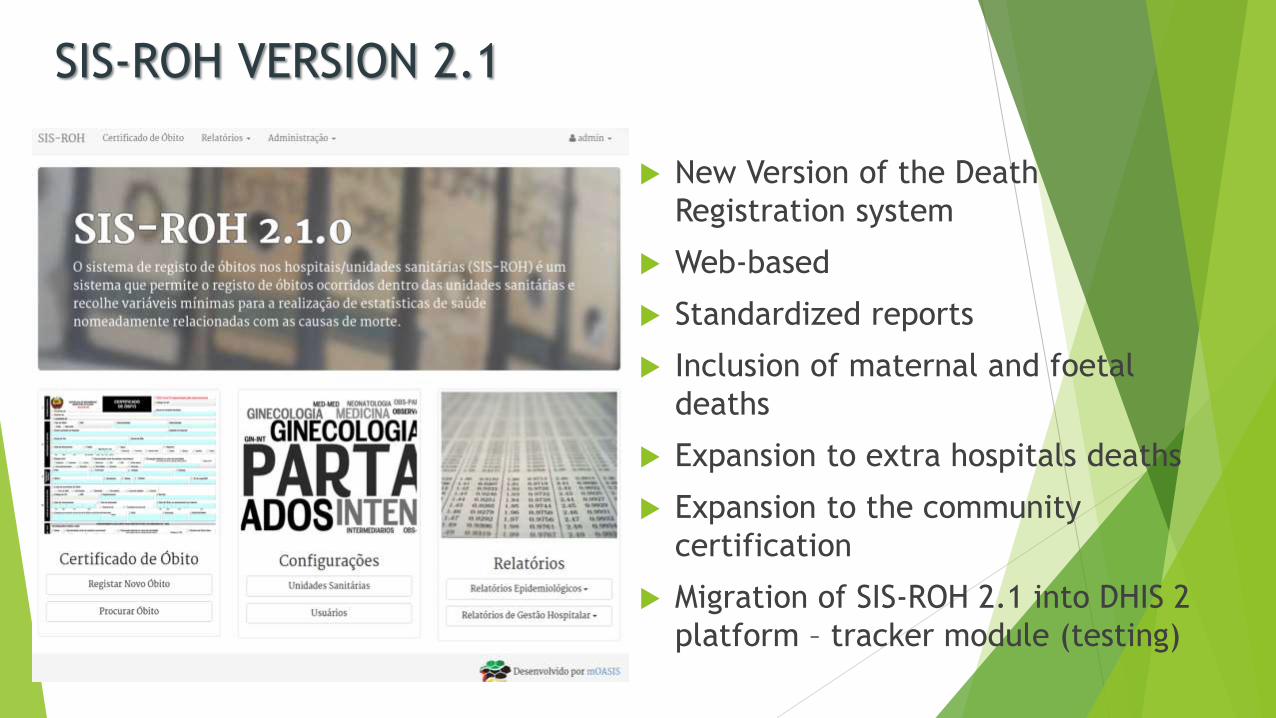
SIS-ROH VERSION 2.1
New Version of the Death
Registration system
Web-based
Standardized reports
Inclusion of maternal and foetal
deaths
Expansion to extra hospitals deaths
Expansion to the community
certification
Migration of SIS-ROH 2.1 into DHIS 2
platform – tracker module (testing)
Integration of SIS-ROH with other HIS
in Mozambique
Ongoing the SIS-ROH2 interoperability and
integration with some national HIS including
the greater national CRVS System, supported
by UEM-MOASIS/JEMBI including: • SIS-H = hospital IS based on short lists of ICD-10 for morbidity
reporting
• SIBI = patient based system for chronic patients
• SIS-MA = national M&E information system

Systems Integration & Interoperability
(CRVS)
CURRENT STATUS IN MOZAMBIQUE
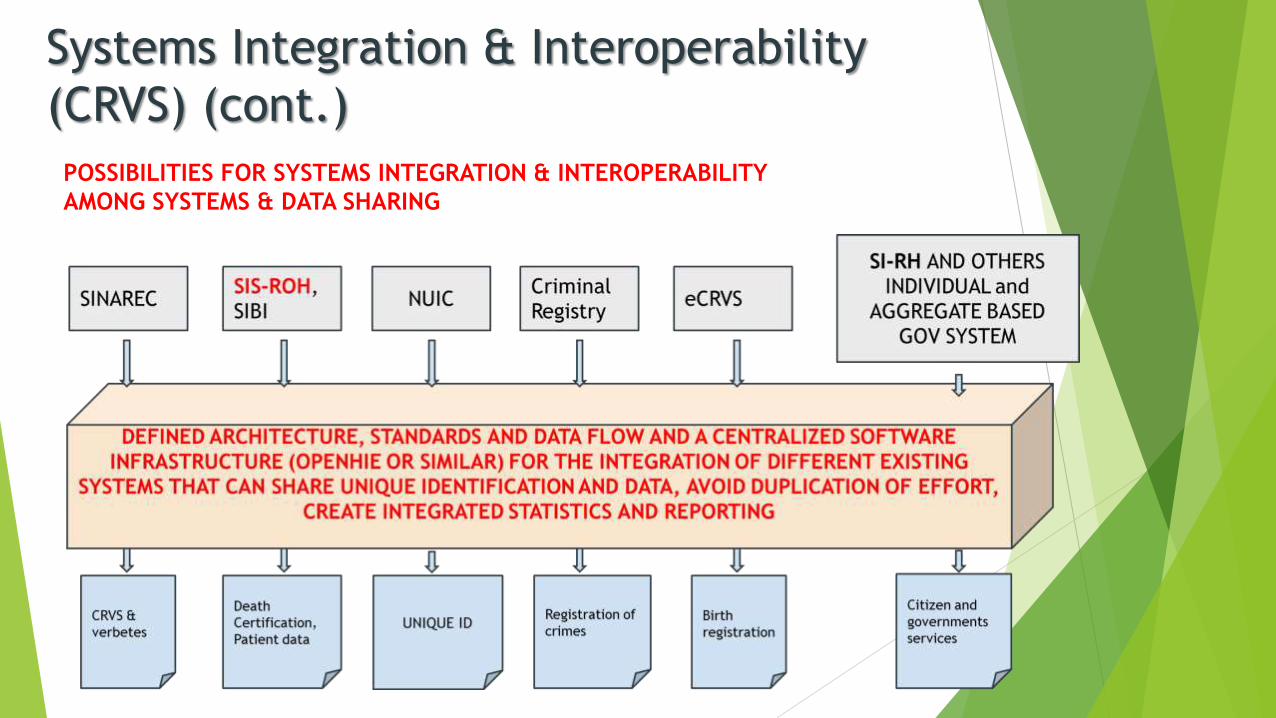
Systems Integration & Interoperability
(CRVS) (cont.)
POSSIBILITIES FOR SYSTEMS INTEGRATION & INTEROPERABILITY
AMONG SYSTEMS & DATA SHARING
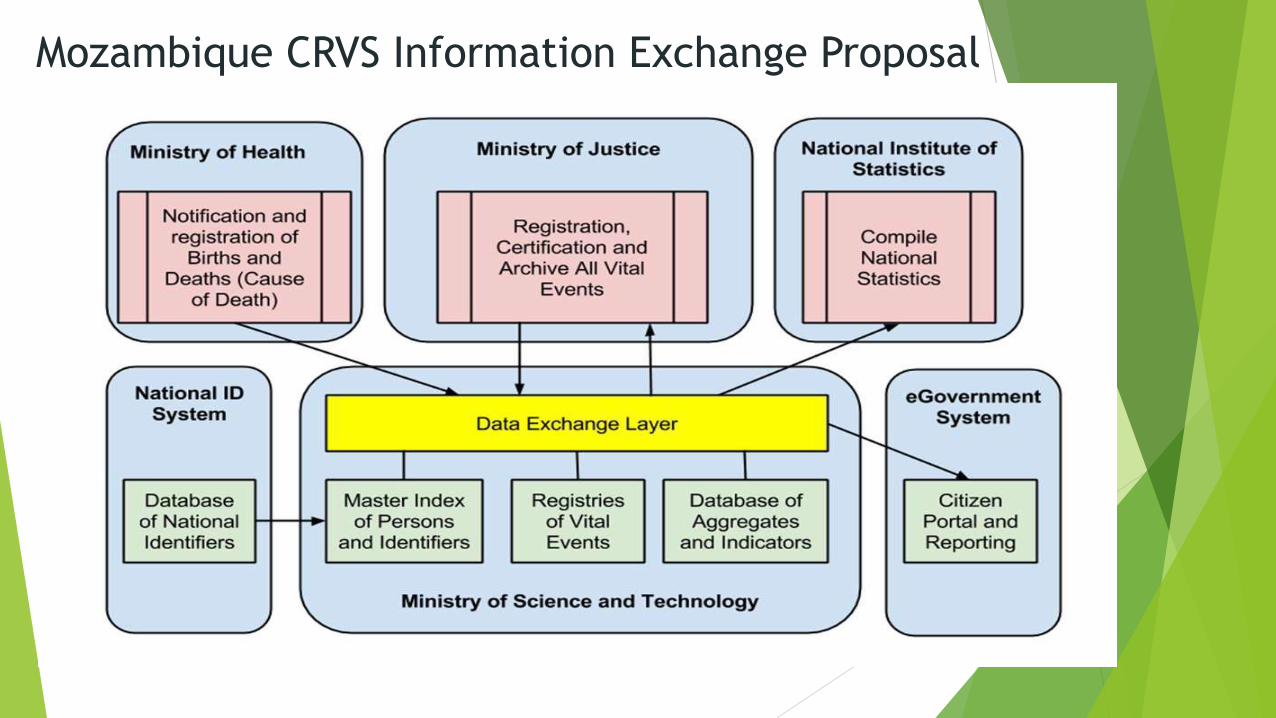
Mozambique CRVS Information Exchange Proposal

ACHIEVEMENTS AND IMPACT
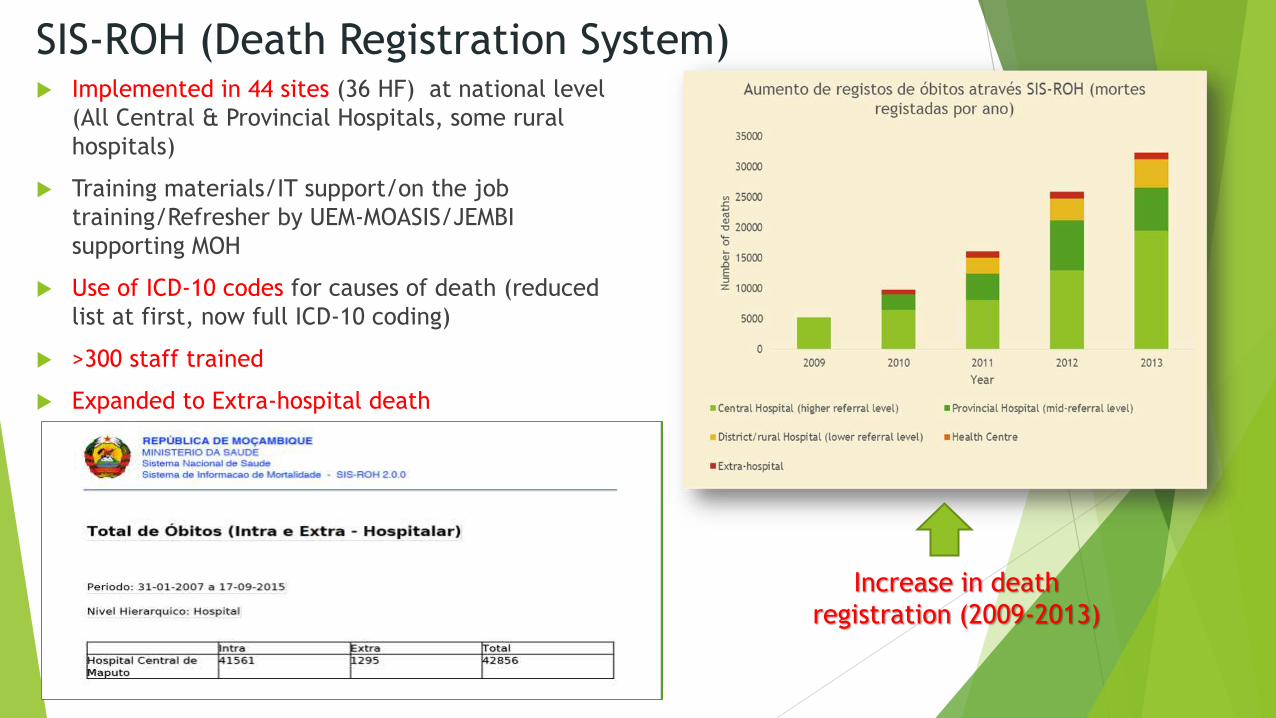
SIS-ROH (Death Registration System)
Implemented in 44 sites (36 HF) at national level
(All Central & Provincial Hospitals, some rural
hospitals)
Training materials/IT support/on the job
training/Refresher by UEM-MOASIS/JEMBI
supporting MOH
Use of ICD-10 codes for causes of death (reduced
list at first, now full ICD-10 coding)
>300 staff trained
Expanded to Extra-hospital death
Increase in death
registration (2009-2013)

IMPACT
SIS-ROH
training
Before 2006, mortality data was acquired from
census and surveys
2009: Mozambique produced first data analysis
mortality report (extracted from SIS-ROH)
3 National reports to date have been produced
(The latest published data from 2009-2013)
Cuamba Rural Hospital Report (done by national
staff at own initiative)
>100.000 deaths registered
Data are also shared and used by INE for
specific epidemiological and statistical analyses
Regular use in Health Units for quality of care
and planning
DATA ANALYSIS, PUBLICATION AND USE AT NATIONAL AND
LOCAL LEVEL:
posters national and international, articles, regular
governmental statistic publications, specific study etc.

SIS-ROH NEW SIMPLIFIED DATA FLOW CYCLE PROCESS
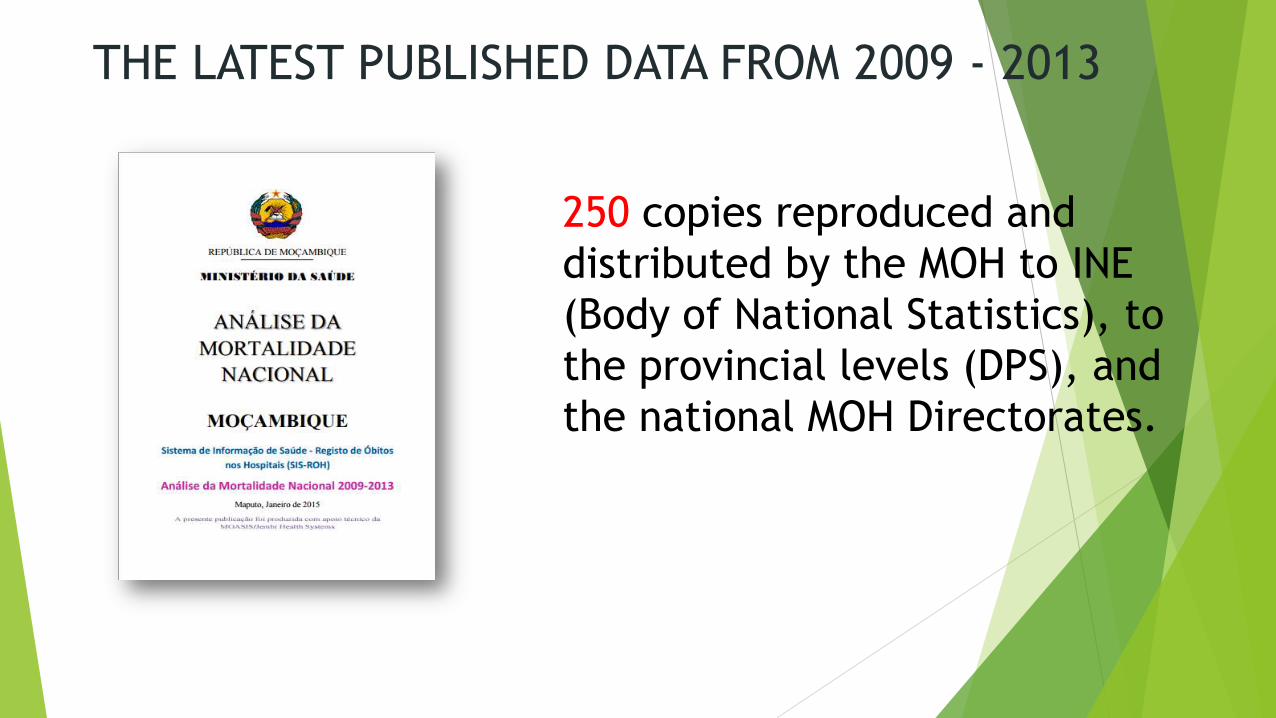
250 copies reproduced and
distributed by the MOH to INE
(Body of National Statistics), to
the provincial levels (DPS), and
the national MOH Directorates.
THE LATEST PUBLISHED DATA FROM 2009 - 2013

0
2
4
6
8
10
12
14
16
18
Surgery Gyneco/Obst Medicine Orthopedics Pediatrics
2008 2009 2010 2011 2012 2013
Intra-hospital mortality rates in Central
Hospital of Maputo by department, 2008-
2013
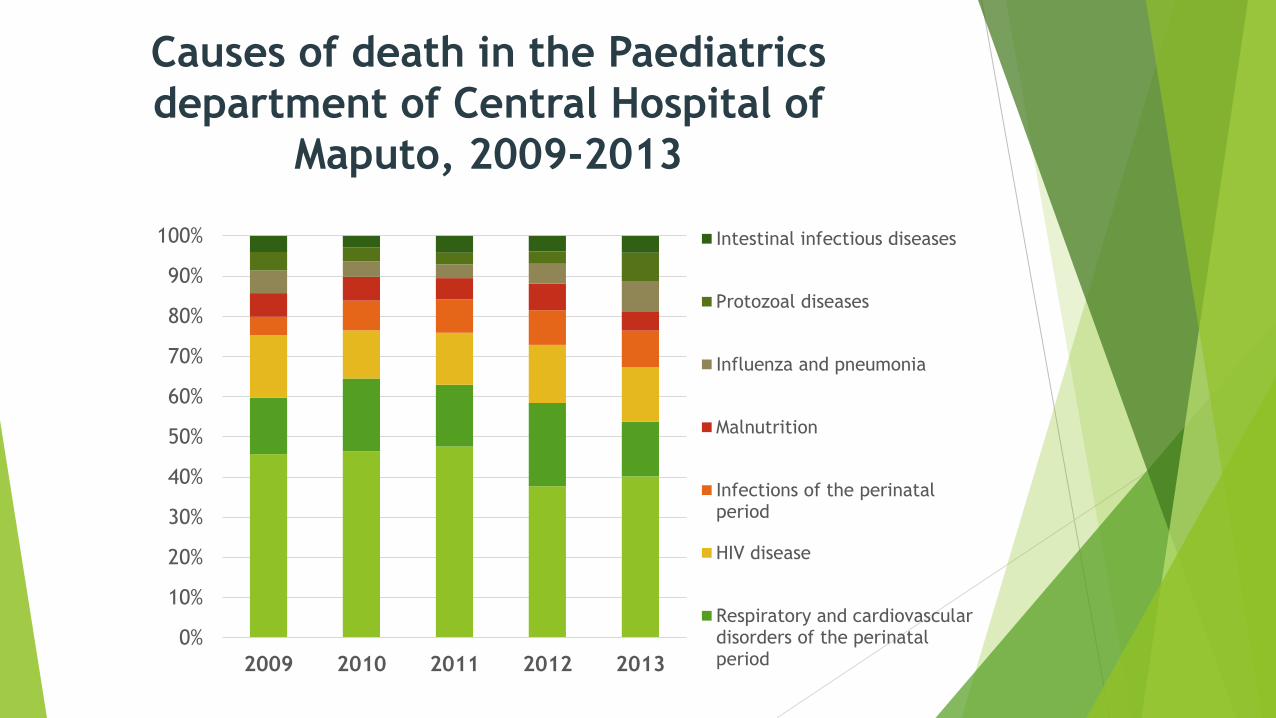
Causes of death in the Paediatrics
department of Central Hospital of
Maputo, 2009-2013
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2009 2010 2011 2012 2013
Intestinal infectious diseases
Protozoal diseases
Influenza and pneumonia
Malnutrition
Infections of the perinatalperiod
HIV disease
Respiratory and cardiovasculardisorders of the perinatalperiod
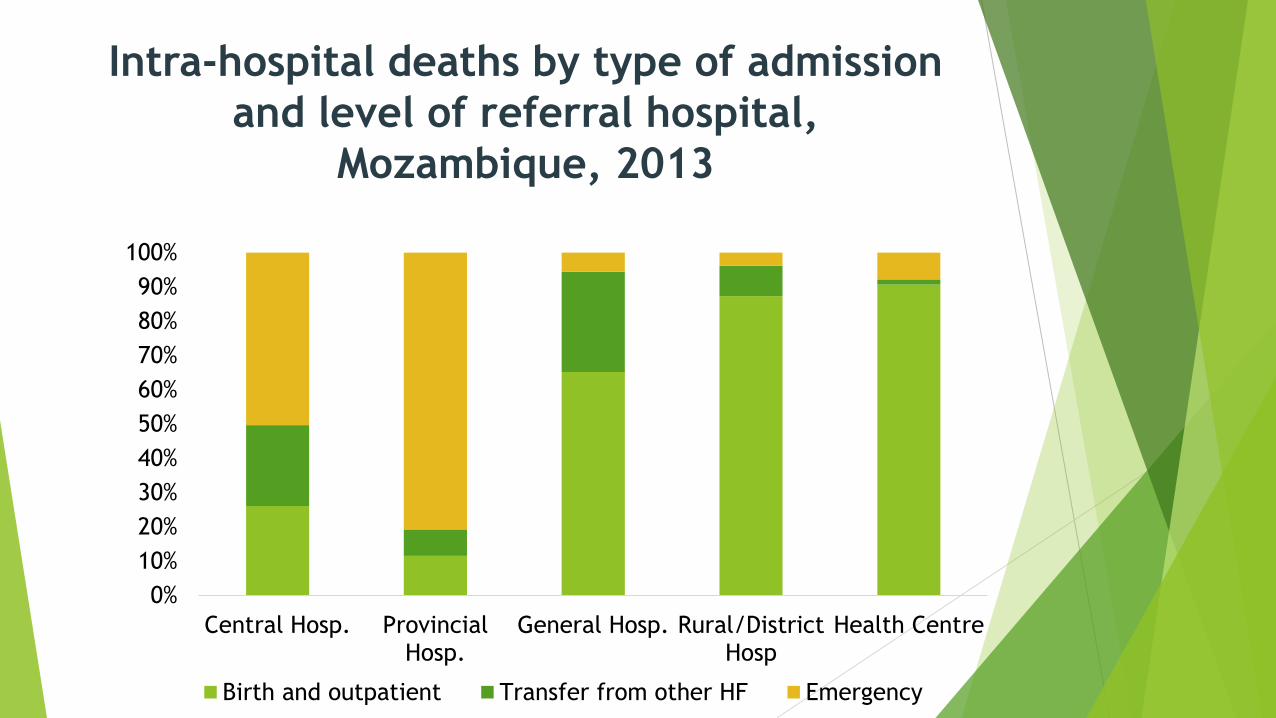
Intra-hospital deaths by type of admission
and level of referral hospital,
Mozambique, 2013
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Central Hosp. ProvincialHosp.
General Hosp. Rural/DistrictHosp
Health Centre
Birth and outpatient Transfer from other HF Emergency

Mortality by cause of death, Mozambique
2009-2011 – Broad Category
Infectious
and parasitic
dis.
37%
Disorders
of perinatal
period
19%
Cardio-
vascular dis.
8%
External
causes
6%
Respiratory
dis.
5%
Neoplasms
5%
Endocrine and
metabolic dis.
4%
Nervous
system dis.
3%
Hematological
dis.
2%
Digestive dis.
2%
Pregnancy,
delivery,
puerp.
2% Other causes
7%
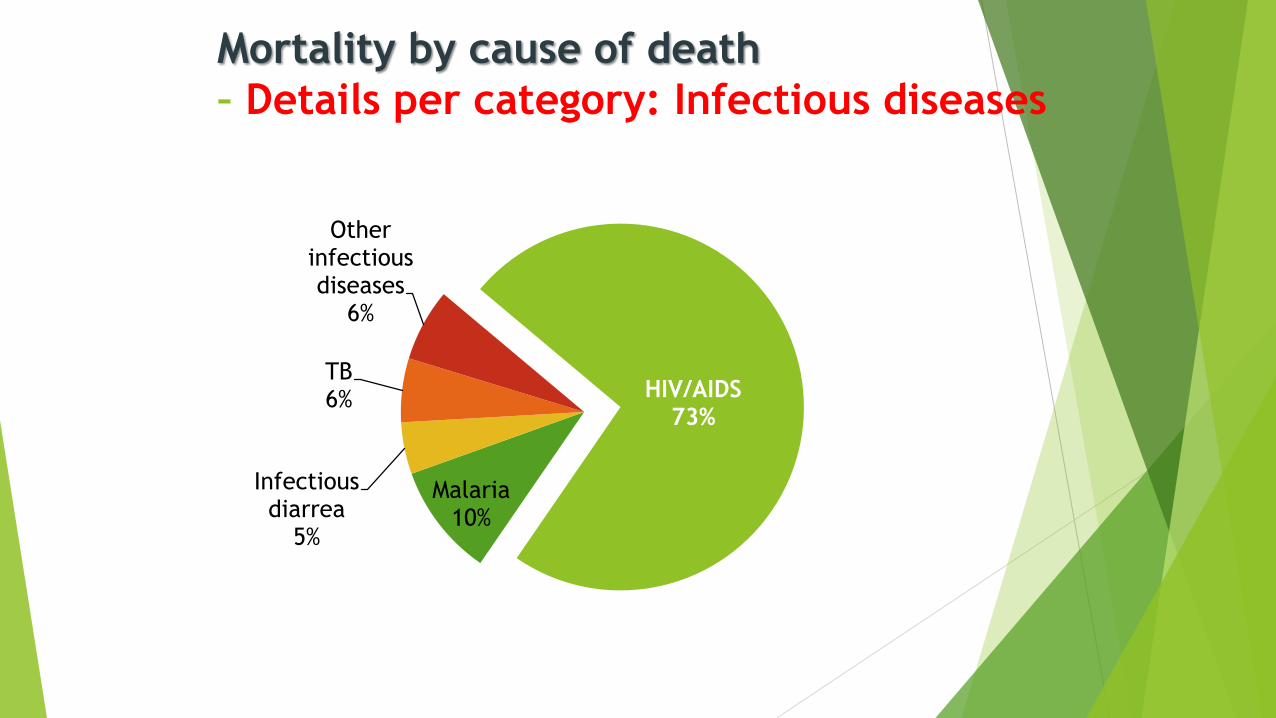
Mortality by cause of death
– Details per category: Infectious diseases
HIV/AIDS 73%
Malaria 10%
Infectious diarrea
5%
TB 6%
Other infectious diseases
6%

Mortality by cause of death
– Details per sub-category: HIV/AIDS
71,9%
11,2%
5,0%
4,2%
2,9%
2,5%
0,4% 0,2%
0,3%
1,1% 0,4%
HIV not specified
HIV + TB
HIV + multiple infections
HIV + encephalopathy
HIV + bacterial infections
HIV + Kaposi sarcoma
HIV + mycotic infections
HIV + Burkitt lynphoma
HIV + other malignantneoplasmHIV + pneumonia(pneumocystis)
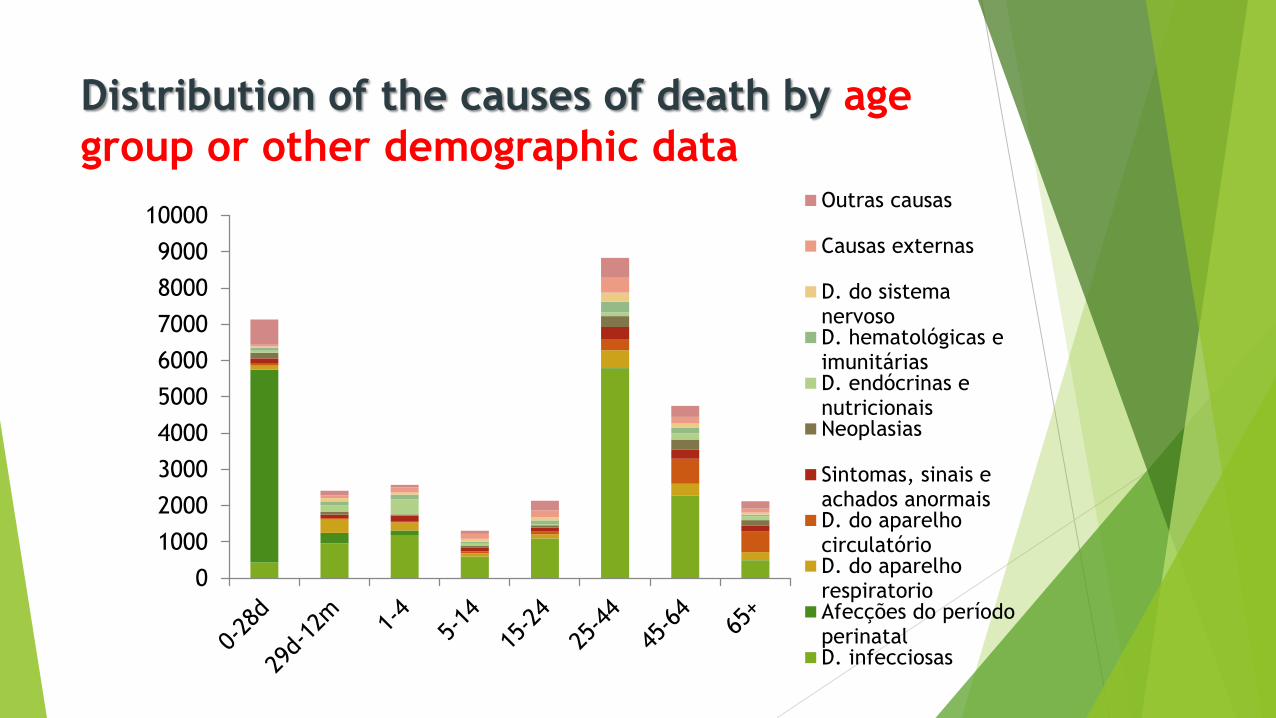
Distribution of the causes of death by age
group or other demographic data
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000Outras causas
Causas externas
D. do sistemanervosoD. hematológicas eimunitáriasD. endócrinas enutricionaisNeoplasias
Sintomas, sinais eachados anormaisD. do aparelhocirculatórioD. do aparelhorespiratorioAfecções do períodoperinatalD. infecciosas
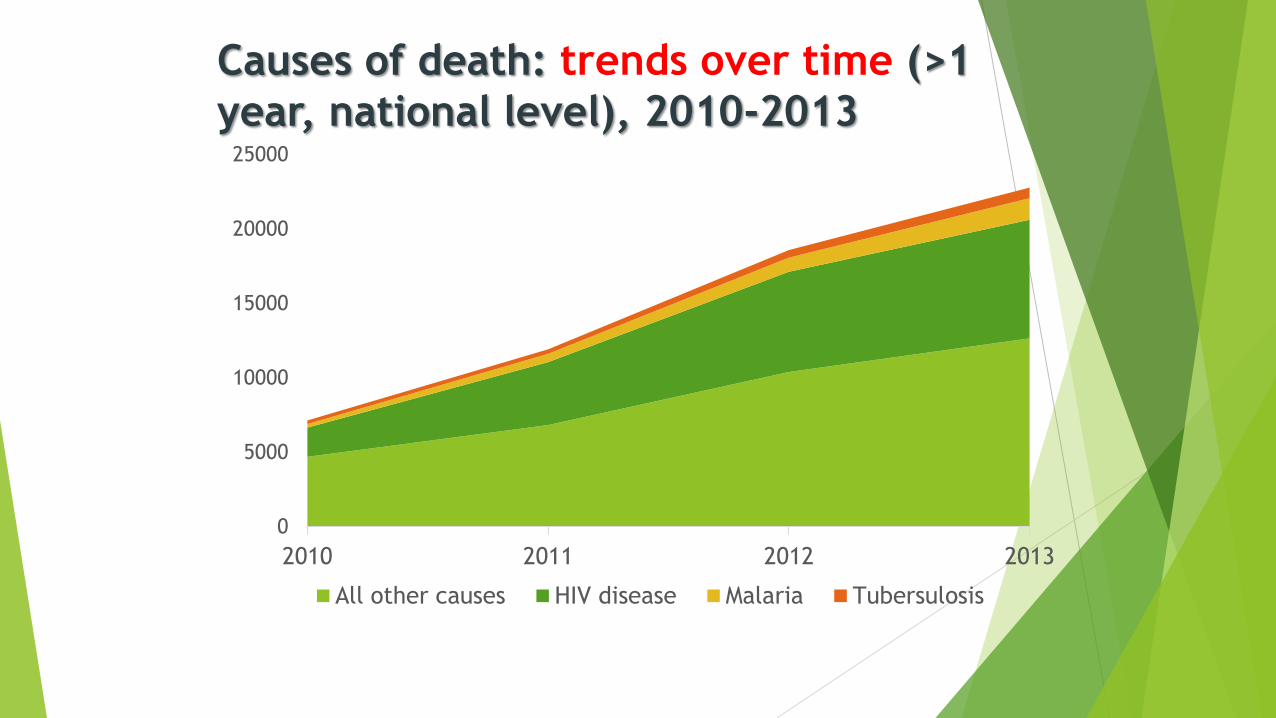
Causes of death: trends over time (>1
year, national level), 2010-2013
0
5000
10000
15000
20000
25000
2010 2011 2012 2013
All other causes HIV disease Malaria Tubersulosis

CHALLENGES

• Expansion to all Health Facilities, out of the Health System at
community level (cultural barriers, poor access to information, low
coverage health and civil registration services)
• Full implementation of Mother and child section of the SIS-ROH2 system
• Full integration in the national M&E system (SIS-MA)
• Full Connection and integration with the Civil Registration system
• Conduct regular training on death certification and ICD-10
• Ensure improvements in Data Quality
• Boost IT Infrastructure, other equipment and materials (ICD-10 manuals)
Kanimambo!
Obrigado!
Dra. Cidália Baloi
Dra. Esperança Nhagumbe
Mr. Ivan Mabote
Ministério da Saude
Ministério da Justiça