· sociedade brasileira de cardiologia • issn-0066-782x • volume 103, nº 3, september 2014...
TRANSCRIPT
www.arquivosonline.com.br Sociedade Brasileira de Cardiologia • ISSN-0066-782X • Volume 103, Nº 3, September 2014
EditorialPercutaneous Treatment of Functional Mitral Regurgitation in Heart
Failure
Original ArticlesEfficacy and Safety of Drug-Eluting Stents in the Real World: 8-Year
Follow-Up
Do Diabetic Patients with Acute Coronary Syndromes Have a Higher
Threshold for Ischemic Pain?
Investigation Route of the Coronary Patient in the Public Health
System in Curitiba, São Paulo and in Incor – IMPACT Study
Effects of Exercise Training on Heart Rate Variability in Chagas Heart
Disease
Survival and Predictive Factors of Lethality in Hemodyalisis: D/I
Polymorphism of The Angiotensin I-Converting Enzyme and of the
Angiotensinogen M235T Genes
Combination Therapy for the Cardiovascular Effects of Perinatal Lead
Exposure in Young and Adult Rats
Assessing Strategies for Heart Failure with Preserved Ejection Fraction
at the Outpatient Clinic
Elevated Blood Pressure and Obesity in Childhood: A Cross-Sectional
Evaluation of 4,609 Schoolchildren
Comparison of Postprandial Lipemia between Women who are on Oral
Contraceptive Methods and Those who are not
Review ArticleMultimodality Imaging of Heart Valve Disease
Letter to the EditorIs Sildenafil a Therapeutic Option for Noncompaction?
Eletronic Pages
Anatomopathological SessionCase 4/2014 - A 66-Year-Old Man with Acute Myocardial Infarction
and Death in Asystole after Primary Coronary Angioplasty
Case ReportSudden Cardiac Death and Short QT Syndrome
ViewpointCylinder Mania in Valvulopathy Back to the Future
Figure 1 – Echocardiographic appearances of the aortic valve in short axis. Figure 1A shows the three-dimensional appearance of a tricuspid aortic valve on transoesophageal echocardiography; Figure 1B shows the appearance of a bicuspid aortic valve on transthoracic echocardiography; and Figures 1C and 1D shows the appearances of a quadricuspid aortic valve in systole and diastole. Page: 253

Arquivos Brasileiros de Cardiologia - Volume 103, Nº 3, September 2014
A JOURNAL OF SOCIEDADE BRASILEIRA DE CARDIOLOGIA - Published since 1948
Contents
Editorial
Percutaneous Treatment of Functional Mitral Regurgitation in Heart FailureGuilherme F. Attizzani and Pedro A. Lemos.....................................................................................................................................................................page 172
Original Articles
Coronary Angioplasty with and without Stent
Efficacy and Safety of Drug-Eluting Stents in the Real World: 8-Year Follow-UpDenise Oliveira Pellegrini, Vitor Osorio Gomes, Ricardo Lasevitch, Luis Smidt, Marco Aurelio Azeredo, Priscila Ledur, Rodrigo Bodanese, Leonardo Sinnott, Emílio Moriguchi, Paulo Caramori.....................................................................................................................................................................page 174
Acute Coronary Artery Disease
Do Diabetic Patients with Acute Coronary Syndromes Have a Higher Threshold for Ischemic Pain?Jose Carlos Nicolau, Carlos Jose Dornas Gonçalves Barbosa, Andre Franci, Luciano Moreira Baracioli, Marcelo Franken, Felipe Gallego Lima, Roberto Rocha Giraldez, Roberto Kalil Filho, Jose Antônio Franchini Ramires, Robert P. Giugliano.....................................................................................................................................................................page 183
Chronic Coronary Artery Disease
Investigation Route of the Coronary Patient in the Public Health System in Curitiba, São Paulo and in Incor – IMPACT StudyJuliano J. Cerci, Evelinda Trindade, Rodrigo Julio Cerci, Daniel Preto, Pedro A. Lemos, Luiz Antonio Machado Cesar, Luís Preto, Luiz Stinghen, Cátia Martinez, Jose Claudio Meneghetti.....................................................................................................................................................................page 192
Chagas’ Disease
Effects of Exercise Training on Heart Rate Variability in Chagas Heart DiseaseBruno Ramos Nascimento, Márcia Maria Oliveira Lima, Maria do Carmo Pereira Nunes, Maria Clara Noman de Alencar, Henrique Silveira Costa, Marcelo Martins Pinto Filho, Vitor Emanuel Serafim Cota, Manoel Otávio da Costa Rocha, Antonio Luiz Pinho Ribeiro.....................................................................................................................................................................page 201
Epidemiology
Survival and Predictive Factors of Lethality in Hemodyalisis: D/I Polymorphism of The Angiotensin I-Converting Enzyme and of the Angiotensinogen M235T GenesMauro Alves, Nelson Albuquerque de Souza e Silva, Lucia Helena Alvares Salis, Basilio de Bragança Pereira, Paulo Henrique Godoy, Emília Matos do Nascimento, Jose Mario Franco Oliveira.....................................................................................................................................................................page 209

Arquivos Brasileiros de Cardiologia - Volume 103, Nº 3, September 2014
Pharmacology/Toxicology
Combination Therapy for the Cardiovascular Effects of Perinatal Lead Exposure in Young and Adult RatsAndreia Fresneda Gaspar e Sandra Cordellini.....................................................................................................................................................................page 219
Ventricular Function/Cardiac Remodeling
Assessing Strategies for Heart Failure with Preserved Ejection Fraction at the Outpatient ClinicAntonio Jose Lagoeiro Jorge, Maria Luiza Garcia Rosa, Mario Luiz Ribeiro, Luiz Claudio Maluhy Fernandes, Monica Di Calafiori Freire, Dayse Silva Correia, Patrick Duarte Teixeira, Evandro Tinoco Mesquita.....................................................................................................................................................................page 231
Hypertension
Elevated Blood Pressure and Obesity in Childhood: A Cross-Sectional Evaluation of 4,609 SchoolchildrenCaroline Filla Rosaneli, Cristina Pellegrio Baena, Flavia Auler, Alika Terumi Arasaki Nakashima, Edna Regina Netto-Oliveira, Amauri Bássoli Oliveira, Luiz Cesar Guarita-Souza, Marcia Olandoski, Jose Rocha Faria-Neto.....................................................................................................................................................................page 238
Systemic Hypertension
Comparison of Postprandial Lipemia between Women who are on Oral Contraceptive Methods and Those who are notJefferson Petto, Leila Monique Reis Vasques, Renata Leão Pinheiro, Beatriz de Almeida Giesta, Alan Carlos Nery dos Santos, Mansueto Gomes Neto, Ana Marice Teixeira Ladeia.....................................................................................................................................................................page 245
Review Article
Multimodality Imaging of Heart Valve DiseaseRonak Rajani, Rajdeep Khattar, Amedeo Chiribiri, Kelly Victor, John Chambers.....................................................................................................................................................................page 251
Letter to the Editor
Is Sildenafil a Therapeutic Option for Noncompaction?Josef Finsterer e Claudia Stöllberger.....................................................................................................................................................................page 264

Arquivos Brasileiros de Cardiologia - Volume 103, Nº 3, September 2014
Arquivos Brasileiros de Cardiologia - Eletronic Pages
Anatomopathological Session
Case 4/2014 - A 66-Year-Old Man with Acute Myocardial Infarction and Death in Asystole after Primary Coronary AngioplastyWilma Noia Ribeiro, Alice Tatsuko Yamada, Luiz Alberto Benvenuti..................................................................................................................................................................page e31
Case Report
Sudden Cardiac Death and Short QT SyndromeMaria Lícia Ribeiro Cury Pavão, Viviane Cristina Ono, Elerson Arfelli, Marcus Vinícius Simões, Jose Antonio Marin Neto, Andre Schmidt..................................................................................................................................................................page e37
Viewpoint
Cylinder Mania in Valvulopathy Back to the FutureMax Grinberg..................................................................................................................................................................page e41
* Indicate manuscripts only in the electronic version. To view them, visit: http://www.arquivosonline.com.br/2014/english/10303/edicaoatual.asp
Editorial BoardBrazilAguinaldo Figueiredo de Freitas Junior (GO)Alfredo Jose Mansur (SP)Aloir Queiroz de Araújo Sobrinho (ES)Amanda G. M. R. Sousa (SP)Ana Clara Tude Rodrigues (SP)Andre Labrunie (PR)Andrei Sposito (SP)Angelo A. V. de Paola (SP)Antonio Augusto Barbosa Lopes (SP) Antonio Carlos C. Carvalho (SP) Antonio Carlos Palandri Chagas (SP) Antonio Carlos Pereira Barretto (SP) Antonio Claudio L. Nobrega (RJ) Antonio de Padua Mansur (SP)Ari Timerman (SP)Armenio Costa Guimaraes (BA)Ayrton Pires Brandao (RJ)Beatriz Matsubara (SP)Brivaldo Markman Filho (PE)Bruno Caramelli (SP)Carisi A. Polanczyk (RS)Carlos Eduardo Rochitte (SP)Carlos Eduardo Suaide Silva (SP) Carlos Vicente Serrano Júnior (SP) Celso Amodeo (SP)Charles Mady (SP)Claudio Gil Soares de Araujo (RJ) Claudio Tinoco Mesquita (RJ)Cleonice Carvalho C. Mota (MG)Clerio Francisco de Azevedo Filho (RJ)Dalton Bertolim Precoma (PR)Dario C. Sobral Filho (PE)Decio Mion Junior (SP)Denilson Campos de Albuquerque (RJ) Djair Brindeiro Filho (PE)Domingo M. Braile (SP)Edmar Atik (SP)Emilio Hideyuki Moriguchi (RS)
Enio Buffolo (SP)Eulogio E. Martinez Filho (SP) Evandro Tinoco Mesquita (RJ) Expedito E. Ribeiro da Silva (SP)Fabio Vilas-Boas (BA)Fernando Bacal (SP)Flavio D. Fuchs (RS) Francisco Antonio Helfenstein Fonseca (SP)Gilson Soares Feitosa (BA)Glaucia Maria M. de Oliveira (RJ)Hans Fernando R. Dohmann (RJ)Humberto Villacorta Junior (RJ)Ines Lessa (BA)Iran Castro (RS)Jarbas Jakson Dinkhuysen (SP)Joao Pimenta (SP)Jorge Ilha Guimaraes (RS)Jose Antonio Franchini Ramires (SP)Jose Augusto Soares Barreto Filho (SE)Jose Carlos Nicolau (SP)Jose Lazaro de Andrade (SP)Jose Pericles Esteves (BA)Leonardo A. M. Zornoff (SP)Leopoldo Soares Piegas (SP)Lucia Campos Pellanda (RS)Luis Eduardo Rohde (RS)Luis Claudio Lemos Correia (BA)Luiz A. Machado Cesar (SP)Luiz Alberto Piva e Mattos (SP)Marcia Melo Barbosa (MG)Maria da Consolaçao Moreira (MG)Mario S. S. de Azeredo Coutinho (SC)Mauricio I. Scanavacca (SP)Max Grinberg (SP)Michel Batlouni (SP)Murilo Foppa (RS)Nadine O. Clausell (RS)Orlando Campos Filho (SP)Otavio Rizzi Coelho (SP)
Otoni Moreira Gomes (MG)Paulo Andrade Lotufo (SP)Paulo Cesar B. V. Jardim (GO)Paulo J. F. Tucci (SP)Paulo R. A. Caramori (RS)Paulo Roberto B. Évora (SP)Paulo Roberto S. Brofman (PR)Pedro A. Lemos (SP)Protasio Lemos da Luz (SP)Reinaldo B. Bestetti (SP)Renato A. K. Kalil (RS)Ricardo Stein (RS)Salvador Rassi (GO)Sandra da Silva Mattos (PE)Sandra Fuchs (RS)Sergio Timerman (SP)Silvio Henrique Barberato (PR)Tales de Carvalho (SC)Vera D. Aiello (SP)Walter Jose Gomes (SP)Weimar K. S. B. de Souza (GO)William Azem Chalela (SP)Wilson Mathias Junior (SP)
ExteriorAdelino F. Leite-Moreira (Portugal)Alan Maisel (Estados Unidos)Aldo P. Maggioni (Italia)Cândida Fonseca (Portugal)Fausto Pinto (Portugal)Hugo Grancelli (Argentina)James de Lemos (Estados Unidos) Joao A. Lima (Estados Unidos)John G. F. Cleland (Inglaterra)Maria Pilar Tornos (Espanha)Pedro Brugada (Belgica)Peter A. McCullough (Estados Unidos)Peter Libby (Estados Unidos)Piero Anversa (Italia)
Scientific Director Maria da Consolaçao Vieira Moreira
Chief Editor Luiz Felipe P. Moreira
Associated Editors
Clinical Cardiology Jose Augusto Barreto-Filho
Surgical Cardiology Paulo Roberto B. Evora
Interventionist Cardiology Pedro A. Lemos
Pediatric/Congenital Cardiology Antonio Augusto Lopes
Arrhythmias/Pacemaker Mauricio Scanavacca
Non-Invasive Diagnostic Methods Carlos E. Rochitte
Basic or Experimental Research Leonardo A. M. Zornoff
Epidemiology/Statistics Lucia Campos Pellanda
Arterial Hypertension Paulo Cesar B. V. Jardim
Ergometrics, Exercise and Cardiac Rehabilitation Ricardo Stein
First Editor (1948-1953) † Jairo Ramos
A JOURNAL OF SOCIEDADE BRASILEIRA DE CARDIOLOGIA - Published since 1948www.arquivosonline.com.br
PresidentAngelo Amato V. de Paola
Vice-PresidentSergio Tavares Montenegro
Financial DirectorJacob Atie
Scientific DirectorMaria da Consolaçao Vieira Moreira
Administrative DirectorEmilio Cesar Zilli
Assistance Quality DirectorPedro Ferreira de Albuquerque
Communication DirectorMauricio Batista Nunes
Information Technology DirectorJose Carlos Moura Jorge
Government Liaison DirectorLuiz Cesar Nazario Scala
Director of State and Regional AffairsAbrahao Afiune Neto
Cardiovascular Health Promotion Director - SBC/FuncorCarlos Costa Magalhaes
Department DirectorEspecializados - Jorge Eduardo Assef
Research DirectorFernanda Marciano Consolim Colombo
Chief Editor of the Brazilian Archives of CardiologyLuiz Felipe P. Moreira
Special Advisor to the PresidencyFabio Sândoli de Brito
Adjunct Coordination
SBC Newsletter EditorNabil Ghorayeb e Fernando Antonio Lucchese
Continuing Education Coordination Estevao Lanna Figueiredo
Norms and Guidelines Coordination Luiz Carlos Bodanese
Governmental Integration Coordination Edna Maria Marques de Oliveira
Regional Integration Coordination Jose Luis Aziz
Presidents of State and Regional Brazilian Societies of Cardiology
SBC/AL - Carlos Alberto Ramos Macias
SBC/AM - Simao Gonçalves Maduro
SBC/BA - Mario de Seixas Rocha
SBC/CE - Ana Lucia de Sa Leitao Ramos
SBC/CO - Frederico Somaio Neto
SBC/DF - Wagner Pires de Oliveira Junior
SBC/ES - Marcio Augusto Silva
SBC/GO - Thiago de Souza Veiga Jardim
SBC/MA - Nilton Santana de Oliveira
SBC/MG - Odilon Gariglio Alvarenga de Freitas
SBC/MS - Mercule Pedro Paulista Cavalcante
SBC/MT - Julio Cesar De Oliveira
SBC/NNE - Jose Itamar Abreu Costa
SBC/PA - Luiz Alberto Rolla Maneschy
SBC/PB - Catarina Vasconcelos Cavalcanti
SBC/PE - Helman Campos Martins
SBC/PI - Joao Francisco de Sousa
SBC/PR - Osni Moreira Filho
SBC/RJ - Olga Ferreira de Souza
SBC/RN - Rui Alberto de Faria Filho
SBC/RS - Carisi Anne Polanczyk
SBC/SC - Marcos Venicio Garcia Joaquim
SBC/SE - Fabio Serra Silveira
SBC/SP - Francisco Antonio Helfenstein Fonseca
SBC/TO - Hueverson Junqueira Neves
Sociedade Brasileira de Cardiologia
Presidents of the Specialized Departaments and Study GroupsSBC/DA - Jose Rocha Faria Neto
SBC/DECAGE - Josmar de Castro Alves
SBC/DCC - Jose Carlos Nicolau
SBC/DCM - Maria Alayde Mendonça da Silva
SBC/DCC/CP - Isabel Cristina Britto Guimaraes
SBC/DIC - Arnaldo Rabischoffsky
SBC/DERC - Nabil Ghorayeb
SBC/DFCVR - Ricardo Adala Benfati
SBC/DHA - Luiz Aparecido Bortolotto
SOBRAC - Luiz Pereira de Magalhaes
SBCCV - Marcelo Matos Cascado
SBHCI - Helio Roque Figueira
SBC/DEIC - Dirceu Rodrigues Almeida
GERTC - Clerio Francisco de Azevedo Filho
GAPO - Danielle Menosi Gualandro
GEECG - Joel Alves Pinho Filho
GEECABE - Mario Sergio S. de Azeredo Coutinho
GECETI - Gilson Soares Feitosa Filho
GEMCA - Alvaro Avezum Junior
GECC - Mauricio Wanjgarten
GEPREC - Glaucia Maria Moraes de Oliveira
Grupo de Estudos de Cardiologia Hospitalar - Evandro Tinoco Mesquita
Grupo de Estudos de Cardio-Oncologia - Roberto Kalil Filho
GEEC - Claudio Jose Fuganti
GECIP - Gisela Martina Bohns Meyer
GECESP - Ricardo Stein
GECN - Ronaldo de Souza Leao Lima
GERCPM - Artur Haddad Herdy

Arquivos Brasileiros de Cardiologia
Affiliated at the Brazilian Medical Association
Volume 103, Nº 3, September 2014Indexing: ISI (Thomson Scientific), Cumulated Index Medicus (NLM), SCOPUS,
MEDLINE, EMBASE, LILACS, SciELO, PubMed
The ads showed in this issue are of the sole responsibility of advertisers, as well as the concepts expressed in signed articles are of the sole responsibility of their
authors and do not necessarily reflect the views of SBC.
This material is for exclusive distribution to the medical profession. The Brazilian Archives of Cardiology are not responsible for unauthorized access to its contents and
that is not in agreement with the determination in compliance with the Collegiate Board Resolution (DRC) N. 96/08 of the National Sanitary Surveillance Agency
(ANVISA), which updates the technical regulation on Drug Publicity, Advertising, Promotion and Information. According to Article 27 of the insignia, "the advertisement or publicity of prescription drugs should be restricted solely and exclusively to health
professionals qualified to prescribe or dispense such products (...)".
To ensure universal access, the scientific content of the journal is still available for full and free access to all interested parties at:
www.arquivosonline.com.br.
Commercial Department
Phone: (11) 3411-5500
E-mail: [email protected]
Editorial Production
SBC - Internal Publication Department
Graphic Design and DiagrammingSBC - Internal Design Department
Address: Av. Marechal Câmara, 160 - 3º andar - Sala 330 20020-907 • Centro • Rio de Janeiro, RJ • Brasil
Phone.: (21) 3478-2700
E-mail: [email protected]
www.arquivosonline.com.br
SciELO: www.scielo.br

Editorial
Percutaneous Treatment of Functional Mitral Regurgitation in Heart FailureGuilherme F. Attizzani1 and Pedro A. Lemos2
Harrington Heart and Vascular Institute - University Hospitals Case Medical Center1, Cleveland, OH - USA; Instituto do Coração - Hospital das Clínicas - Faculdade de Medicina - Universidade de São Paulo2, São Paulo - Brazil
Mailing Address: Pedro A. Lemos •Avenida Doutor Eneas de Carvalho Aguiar, 255, Cerqueira Cesar. Postal Code 05403-000, São Paulo, SP − BrazilE-mail: [email protected]
KeywordsHeart Failure/mortality; Mitral Valve Insufficiency/
physiopathology; Ventricular Remodeling; Cardiac Catheterization/instrumentation.
DOI: 10.5935/abc.20140143
Congestive heart failure (HF) remains one of the most important and challenging clinical problems in cardiovascular medicine in Brazil and worldwide. Evidence suggests that mortality in this setting has decreased in Brazil over recent years1, which may be related, at least partially, to a more intense and widespread use of neurohormonal blockade (with angiotensin-converting-enzyme inhibitors and beta-blockers) in patients with advanced HF2. To better evaluate the characteristics of end-stage heart disease in Brazil, the ongoing I Brazilian Registry of Heart Failure (BREATHE registry) will evaluate the profile of 1,200 patients admitted with decompensated HF to 60 hospitals representative of the different Brazilian regions3. Final results of the BREATHE registry are expected to be available within the next months. In spite of recent improvements in medical therapy, advanced HF continues to impose an ominous prognosis; in some subsets, mortality rates can reach up to 30% to 50% in the first year of disease, according to contemporary series of Brazilian centers4. In this context, therapeutic alternatives have been intensively investigated in an attempt to improve the outcomes of patients with HF.
Mitral regurgitation (MR) is a frequent finding among individuals with end-stage HF5,6. Indeed, observational studies revealed that most patients with HF and severe (≥ 3+) MR have functional (74%), rather than degenerative (21%), MR7. While surgery is the gold-standard therapy in patients with organic (i.e., degenerative) mitral valve disease associated with symptoms or evidence of left ventricle dysfunction8, its benefit to patients with MR secondary
to underlying ventricular dysfunction (i.e., functional MR) remains unclear9. Therefore, individuals with functional MR are frequently referred to isolated clinical management, carrying poor long-term prognosis7.
Percutaneous mitral valve transcatheter therapies, such as direct and indirect annuloplasty, leaflet repairing devices, and valve replacement, have recently emerged as potential alternatives for patients with MR. Percutaneous edge-to-edge mitral valve repair with the MitraClip system (Abbott Vascular, Abbott Park, Illinois) exhibits the largest body of data available among transcatheter therapies for MR10. The procedure has consistently demonstrated to be safe, coupled with efficacious MR reduction, left ventricle reverse remodeling, and improvement in congestive HF symptoms and in the quality of life of patients with either functional or degenerative MR11,12. In fact, MitraClip implantation has been approved for commercial use for many years in Europe, but, in the United States, the approval has been recently given. In Brazil, the system has been just approved by the Brazilian Health Surveillance Agency (Anvisa) and is expected to be available in the near future.
The only prospective, randomized, controlled trial comparing MitraClip therapy and conventional surgery mostly for patients with organic MR (i.e., EVEREST II trial) has shown that the percutaneous procedure had superior safety and similar improvement in clinical outcomes, although the latter led to more effective reduction in the magnitude of MR10. It is currently under intense investigation whether catheter-based therapies could be offered as a minimally invasive strategy also for patients with severe MR secondary to left ventricular dysfunction. Recently, non-randomized studies including high-risk patients with functional MR have confirmed excellent safety and efficacy profiles of MitraClip implantation in more complex clinical scenarios, thus contributing to refine the understanding on the role of this novel therapy in patients with different MR etiologies13,14.
Minimally invasive catheter-based therapies aimed at correcting (or minimizing) functional MR represent a whole new and promising therapeutic strategy for patients with advanced HF15. Notwithstanding its potential, the novel treatment must be scrutinized in the context of studies specifically designed to evaluate its clinical value in improving short- and long-term clinical outcomes.
172

Editorial
Attizzani & LemosPercutaneous treatment of mitral regurgitation
Arq Bras Cardiol. 2014; 103(3):172-173
1. Gaui EN, Oliveira GM, Klein CH. Mortality by heart failure and ischemic heart disease in Brazil from 1996 to 2011. Arq Bras Cardiol. 2014;102(6):557-65.
2. Carlo CH, Cardoso JN, Ochia ME, Oliveira MT Jr, Ramires JA, Pereira-Barretto AC. Temporal variation in the prognosis and treatment of advanced heart failure - before and after 2000. Arq Bras Cardiol. 2014;102(5):495-504.
3. BREATHE investigators. Rationale and design: BREATHE registry--I Brazilian Registry of Heart Failure. Arq Bras Cardiol. 2013;100(5):390-4.
4. Pereira-Barretto AC, Carlo CH, Cardoso JN, Ochiai ME, Lima MV, Curiati MC, et al. Role of BNP levels on the prognosis of decompensated advanced heart failure. Arq Bras Cardiol. 2013;100(3):281-7.
5. Mancuso FJ, Moises VA, Almeida DR, Oliveira WA, Poyares D, Brito FS, et al. Criteria for mitral regurgitation classification were inadequate for dilated cardiomyopathy. Arq Bras Cardiol. 2013;101(5):457-65.
6. Mornos C, Petrescu L, Cozma D, Ionac A. A new tissue Doppler index to predict cardiac death in patients with heart failure. Arq Bras Cardiol. 2014;102(1):19-29.
7. Goel SS, Bajaj N, Aggarwal B, Gupta S, Poddar KL, Ige M, et al. Prevalence and outcomes of unoperated patients with severe symptomatic mitral regurgitation and heart failure: comprehensive analysis to determine the potential role of MitraClip for this unmet need. J Am Coll Cardiol. 2014;63(2):185-6.
8. Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC)1; European Association for Cardio-Thoracic Surgery (EACTS), Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H,et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J. 2012;33(19):2451-96.
9. Mihaljevic T, Lam BK, Rajeswaran J, Takagaki M, Lauer MS, Gillinov AM, et al. Impact of mitral valve annuloplasty combined with revascularization in patients with functional ischemic mitral regurgitation. J Am Coll Cardiol. 2007;49(22):2191-201.
10. Feldman T, Foster E, Glower DD, Kar S, Rinaldi MJ, Fail PS, et al. EVEREST II Investigators. Percutaneous repair or surgery for mitral regurgitation. N Engl J Med. 2011;364(15):1395-406.
11. Attizzani GF, Ohno Y, Capodanno D. Extended use of percutaneous edge-to-edge mitral valve repair beyond EVEREST Criteria: thirty-day and twelve-month clinical and echocardiographic outcomes from the GRASP Registry. J Am Coll Cardiol Interv. [In Press]
12. Glower DD, Kar S, Trento A, Lim DS, Bajwa T, Quesada R, et al. Percutaneous mitral valve repair for mitral regurgitation in high-risk patients: results of the EVEREST II Study. J Am Coll Cardiol. 2014;64(2):172-81.
13. Maisano F, Franzen O, Baldus S, Schäfer U, Hausleiter J, Butter C, et al. Percutaneous mitral valve interventions in the real world: early and 1-year results from the ACCESS-EU, a prospective, multicenter, nonrandomized post-approval study of the MitraClip therapy in Europe. J Am Coll Cardiol. 2013;62(12):1052-61.
14. Taramasso M, Denti P, Buzzatti N, De Bonis M, La Canna G, Colombo A, et al. Mitraclip therapy and surgical mitral repair in patients with moderate to severe left ventricular failure causing functional mitral regurgitation: a single-centre experience. Eur J Cardiothorac Surg. 2012;42(6):920-6.
15. Franzen O, van der Heyden J, Baldus S, Schlüter M, Schillinger W, Butter C, et al. MitraClip(R) therapy in patients with end-stage systolic heart failure. Eur J Heart Fail. 2011;13(5):569-76
References
173

Original Article
Efficacy and Safety of Drug-Eluting Stents in the Real World: 8-Year Follow-UpDenise Oliveira Pellegrini, Vitor Osorio Gomes, Ricardo Lasevitch, Luis Smidt, Marco Aurelio Azeredo, Priscila Ledur, Rodrigo Bodanese, Leonardo Sinnott, Emílio Moriguchi, Paulo CaramoriHospital São Lucas PUC, Porto Alegre, RS, Brazil
Mailing Address: Denise Machado de Oliveira Pellegrini •Avenida Alegrete 423/1601, Petropolis. Postal Code 90460-100, Porto Alegre, RS, BrazilEmail: [email protected]; [email protected] Manuscript received November 21, 2013; revised manuscript March 5, 2014; accepted March 14, 2014.
DOI: 10.5935/abc.20140110
Abstract
Background: Drug-eluting stents have been used in daily practice since 2002, with the clear advantages of reducing the risk of target vessel revascularization and an impressive reduction in restenosis rate by 50%–70%. However, the occurrence of a late thrombosis can compromise long-term results, particularly if the risks of this event were sustained. In this context, a registry of clinical cases gains special value.
Objective: To evaluate the efficacy and safety of drug-eluting stents in the real world.
Methods: We report on the clinical findings and 8-year follow-up parameters of all patients that underwent percutaneous coronary intervention with a drug-eluting stent from January 2002 to April 2007. Drug-eluting stents were used in accordance with the clinical and interventional cardiologist decision and availability of the stent.
Results: A total of 611 patients were included, and clinical follow-up of up to 8 years was obtained for 96.2% of the patients. Total mortality was 8.7% and nonfatal infarctions occurred in 4.3% of the cases. Target vessel revascularization occurred in 12.4% of the cases, and target lesion revascularization occurred in 8% of the cases. The rate of stent thrombosis was 2.1%. There were no new episodes of stent thrombosis after the fifth year of follow-up. Comparative subanalysis showed no outcome differences between the different types of stents used, including Cypher®, Taxus®, and Endeavor®.
Conclusion: These findings indicate that drug-eluting stents remain safe and effective at very long-term follow-up. Patients in the “real world” may benefit from drug-eluting stenting with excellent, long-term results. (Arq Bras Cardiol. 2014; 103(3):174-182)
Keywords: Drug-Eluting Stents/trends; Treatment Outcome; Effectiveness; Long-Term Effect.
IntroductionDrug-eluting stents (DES) have been used in clinical practice
since 2002. Multicenter clinical trials have clearly demonstrated the advantages of these stents in reducing major cardiovascular outcomes, particularly target vessel revascularization (TVR), compared with bare metal stents1. Randomized clinical trials have not included DES, despite their increased use; thus, their efficacy and safety in the real world has been questioned. Considerations regarding DES safety have increased since 2006, when preliminary data indicated higher rates of in-stent thrombosis with DES compared with bare metal stents2-5. Despite the widespread use of DES in subsequent years, there is still a lack of long-term studies of patients who have received these devices.
A patient registry was created within this scenario. All the patients from two Brazilian institutions who received DES between 2002 and 2007, often with off-label indications, were clinically followed up for 8 years. Patient outcomes were analyzed based on the current definitions, and the efficacy and safety of this technology were assessed.
Methods
PopulationThis study included all patients who underwent
percutaneous coronary intervention using at least 1 DES (Costar®, Cypher®, Endeavor®, Infinnium®, Janus®, Supralimus®, and Taxus®) from January 2002 to April 2007 at the São Lucas and Mãe de Deus hospitals in Porto Alegre (RS). Every patient that presented with acute coronary syndrome and stable angina, with or without ST-segment elevation, was included. The type of DES used during the procedure was left to the discretion of the interventional cardiologist. Given the predominant use of the Cypher®, Endeavor®, and Taxus® stents, a sub-analysis comparing the performance of these stents was conducted.
174

Original Article
Pellegrini et al.Drug-eluting stents: long-term follow-up
Arq Bras Cardiol. 2014; 103(3):174-182
Definitions and clinical follow-upData regarding the patients’ clinical presentations at the
time of the procedure were collected through a detailed review of medical records. The patient groups were defined as follows: stable angina, unstable angina, nonST elevation myocardial infarction, ST segment elevation, and recent myocardial infarction (MI) (<3 months before the procedure). Data regarding the procedure and in-hospital outcomes were prospectively collected. Chronic renal failure was defined as a glomerular filtration rate (GFR) of <60 ml/min/1.73 m2 6.
Clinical outcomes were defined as follows: mortality due to any cause; nonfatal MI; CK-MB increase greater than or equal to three times the upper normal limit, and/or electrocardiographic changes compatible with infarction (i.e., ST-segment elevation or new inactive zone); or in patients who underwent coronary artery bypass graft surgery, CK-MB increase greater than or equal to five times the upper normal limit; target lesion revascularization (TLR) (i.e., percutaneous or surgical revascularization to treat lesions in the segment of the stent or 5 mm proximal or distal to the prior implant); and TVR (i.e., any revascularization of the vessel treated with DES in the index procedure).
Stent thrombosis was classified according to the definition given by the Academic Research Consortium (ARC) as follows: defined (i.e., acute coronary syndrome with visualization of a thrombus in the segment where the DES was deployed), probable (i.e., unexplained death within 30 days or target vessel infarction), and possible (i.e., any unexplained death after 30 days). Based on the time of occurrence, stent thrombosis was defined as follows: acute (i.e., within the first 24 h), subacute (i.e., within 30 days), late (i.e., after 30 days), and very late (i.e., after 1 year)7.
Total mortality, nonfatal MI, and TVR that occurred during the follow-up period were defined as major adverse cardiac events (MACEs).
Angiographic success was defined as stenosis < 20% and thrombolysis in myocardial infarction (TIMI) flow grade 3 by the end of the procedure. Clinical success was defined as angiographic success and the absence of clinical complications such as death, MI, urgent revascularization, and stroke during the index hospitalization.
The first intervention was considered the index procedure for patients with more than one intervention during the study period.
Clinical follow-up was conducted through medical appointments, phone interviews with the patient, reviews of outpatient and in-hospital medical records, and contact with the attending physician. All the clinical events were adjudicated by analysis of the documentation’s sources by a cardiologist who was blinded to the other clinical data. The first clinical follow-up was performed 12 months after the index procedure and a biannual clinical follow-up was performed thereafter.
Quantitative coronary angiographic analysisAn experienced interventional cardiologist analyzed the
baseline and post-procedure coronary angiograms. Offline quantitative coronary angiography of the index intervention was performed using a guiding catheter for calibration of
the image magnification (CardioNow Websend DICOM Study Sharing Software, HeartLab, Inc., Westerly, Rhode Island). The minimal luminal diameter and the reference vessel diameter were measured, both before and after the intervention, from a single shot showing the smaller luminal diameter. Coronary lesions were classified according to the American Heart Association and the American College of Cardiology (AHA / ACC) guidelines8.
Statistical AnalysisStatistical analysis was performed using the SPSS 19.0
software, assuming a significance level of 5%. Quantitative variables were expressed as a mean ± standard deviation. Categorical variables were presented as absolute and relative frequencies and were compared by the chi-square test or Fisher’s exact test, as appropriate. Adjusted residuals greater than 1.96 (α = 0.05) were considered statistically significant, thereby indicating a positive association between the categories. Kaplan-Meier curves were developed for analysis of the clinical outcomes. Cox regression analysis was used to investigate the association between explanatory variables and outcomes. The multivariate analysis initially included all of the variables, for which the p value was < 0.20 in the univariate analysis. Those with the highest p values were removed one by one and only the variables with p values < 0.05 were maintained in the final model.
ResultsIn total, 611 patients were included in the registry. Clinical
follow-up was available for 96.2% of the patients, with an average follow-up of 84 (±12) months and a maximum of 96 months. The demographic characteristics and clinical presentations of the patients are presented in Table 1.
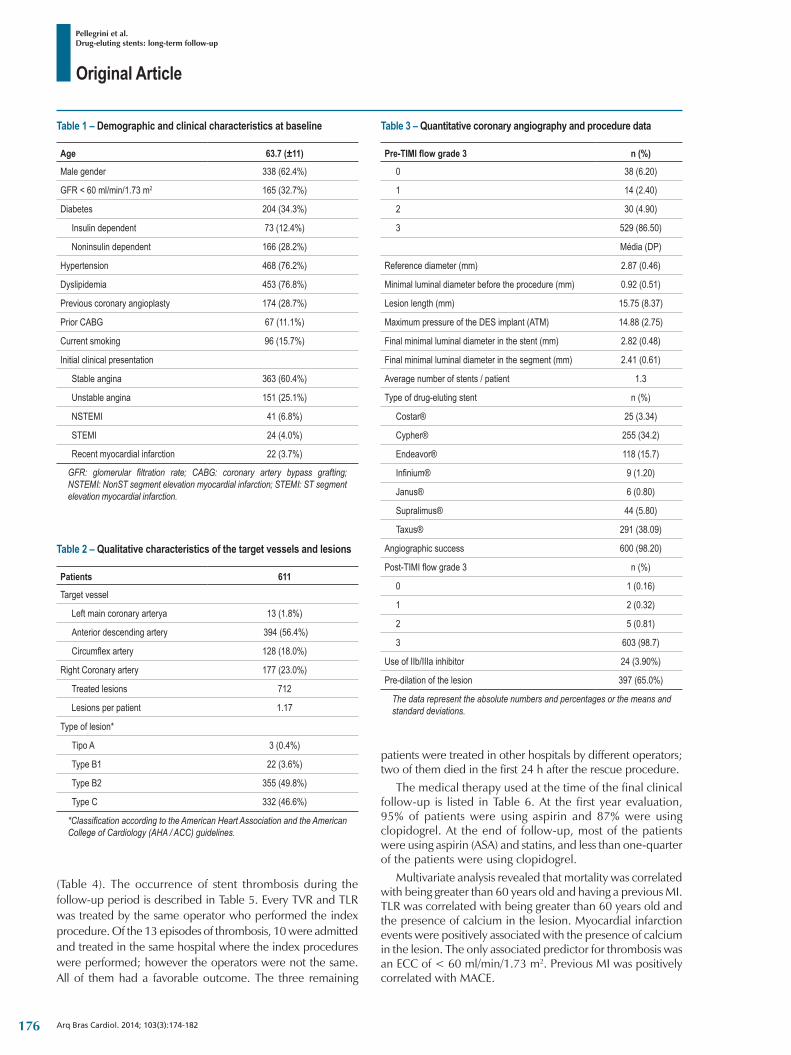
The mean average age was 63.7 years, and the male gender was predominant (63%). One-third of the subjects exhibited renal failure or diabetes, more than two-thirds had hypertension and dyslipidemia, and slightly more than one-half were smokers. Stable angina was the most common clinical presentation.
Regarding the angiographic characteristics, most of the lesions were located in the left anterior descending artery (in 348 patients or 56.4%). The majority of the lesions (96.4%) were either type B2 or type C lesions (Table 2).
The mean reference diameter of the target vessel before the procedure was 2.87 mm (± 0.46), with a minimal luminal diameter of 0.92 mm (± 0.51) and a mean lesion length of 15.75 mm (± 8.37). A total of 748 DES and 83 bare metal stents were used in the index procedure. Angiographic success was observed in 98.2% of the cases. Additional angiographic characteristics are presented in Table 3.
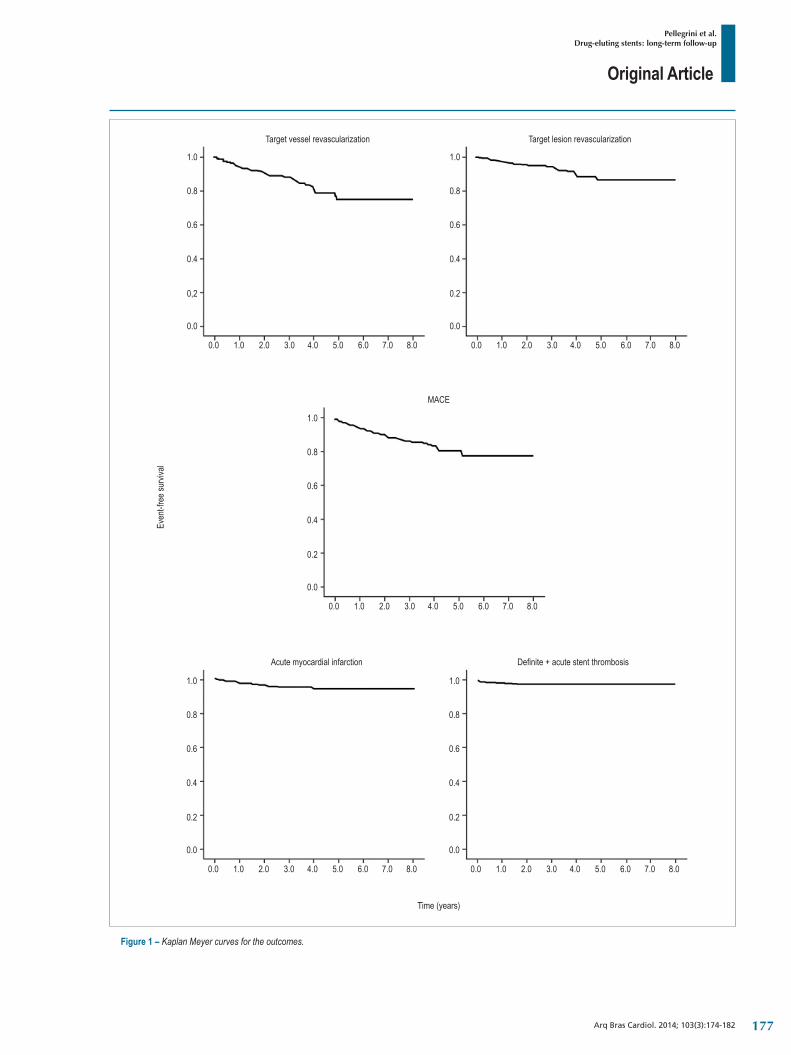
The event-free Kaplan Meier curves are shown in Figure 1. Total mortality was 8.7% at an average follow-up of 84 months (± 12). Only 4.3% of the patients experienced a new nonfatal MI. Eight percent of the patients required new revascularization of the target lesion; 5.4% of the procedures were percutaneous and 2.6% were performed via bypass surgery. The incidence of defined or probable DES thrombosis was 2.1%. Target vessel revascularization and TLR were 12.4% and 8.0%, respectively
175
Original Article
Pellegrini et al.Drug-eluting stents: long-term follow-up
Arq Bras Cardiol. 2014; 103(3):174-182
Table 1 – Demographic and clinical characteristics at baseline
Age 63.7 (±11)
Male gender 338 (62.4%)
GFR < 60 ml/min/1.73 m2 165 (32.7%)
Diabetes 204 (34.3%)
Insulin dependent 73 (12.4%)
Noninsulin dependent 166 (28.2%)
Hypertension 468 (76.2%)
Dyslipidemia 453 (76.8%)
Previous coronary angioplasty 174 (28.7%)
Prior CABG 67 (11.1%)
Current smoking 96 (15.7%)
Initial clinical presentation
Stable angina 363 (60.4%)
Unstable angina 151 (25.1%)
NSTEMI 41 (6.8%)
STEMI 24 (4.0%)
Recent myocardial infarction 22 (3.7%)
GFR: glomerular filtration rate; CABG: coronary artery bypass grafting; NSTEMI: NonST segment elevation myocardial infarction; STEMI: ST segment elevation myocardial infarction.
Table 2 – Qualitative characteristics of the target vessels and lesions
Patients 611
Target vessel
Left main coronary arterya 13 (1.8%)
Anterior descending artery 394 (56.4%)
Circumflexartery 128 (18.0%)
Right Coronary artery 177 (23.0%)
Treated lesions 712
Lesions per patient 1.17
Type of lesion*
Tipo A 3 (0.4%)
Type B1 22 (3.6%)
Type B2 355 (49.8%)
Type C 332 (46.6%)
*Classification according to the American Heart Association and the American College of Cardiology (AHA / ACC) guidelines.
Table 3 – Quantitative coronary angiography and procedure data
Pre-TIMI flow grade 3 n (%)
0 38 (6.20)
1 14 (2.40)
2 30 (4.90)
3 529 (86.50)
Média (DP)
Reference diameter (mm) 2.87 (0.46)
Minimal luminal diameter before the procedure (mm) 0.92 (0.51)
Lesion length (mm) 15.75 (8.37)
MaximumpressureoftheDESimplant(ATM) 14.88 (2.75)
Final minimal luminal diameter in the stent (mm) 2.82 (0.48)
Final minimal luminal diameter in the segment (mm) 2.41 (0.61)
Average number of stents / patient 1.3
Type of drug-eluting stent n (%)
Costar® 25 (3.34)
Cypher® 255 (34.2)
Endeavor® 118 (15.7)
Infinium® 9 (1.20)
Janus® 6 (0.80)
Supralimus® 44 (5.80)
Taxus® 291 (38.09)
Angiographic success 600 (98.20)
Post-TIMIflowgrade3 n (%)
0 1 (0.16)
1 2 (0.32)
2 5 (0.81)
3 603 (98.7)
Use of IIb/IIIa inhibitor 24 (3.90%)
Pre-dilation of the lesion 397 (65.0%)
The data represent the absolute numbers and percentages or the means and standard deviations.
(Table 4). The occurrence of stent thrombosis during the follow-up period is described in Table 5. Every TVR and TLR was treated by the same operator who performed the index procedure. Of the 13 episodes of thrombosis, 10 were admitted and treated in the same hospital where the index procedures were performed; however the operators were not the same. All of them had a favorable outcome. The three remaining
patients were treated in other hospitals by different operators; two of them died in the first 24 h after the rescue procedure.
The medical therapy used at the time of the final clinical follow-up is listed in Table 6. At the first year evaluation, 95% of patients were using aspirin and 87% were using clopidogrel. At the end of follow-up, most of the patients were using aspirin (ASA) and statins, and less than one-quarter of the patients were using clopidogrel.
Multivariate analysis revealed that mortality was correlated with being greater than 60 years old and having a previous MI. TLR was correlated with being greater than 60 years old and the presence of calcium in the lesion. Myocardial infarction events were positively associated with the presence of calcium in the lesion. The only associated predictor for thrombosis was an ECC of < 60 ml/min/1.73 m2. Previous MI was positively correlated with MACE.
176
Original Article
Pellegrini et al.Drug-eluting stents: long-term follow-up
Arq Bras Cardiol. 2014; 103(3):174-182
1.0
0.8
0.6
0.4
0,2
0.0
0.0 1.0 2.0 3.0 4.0 5.0 6.0
Target vessel revascularization Target lesion revascularization
MACE
Time (years)
Even
t-fre
e sur
vival
Acute myocardial infarction Definite+acutestentthrombosis
7.0 8.0
1.0
0.8
0.6
0.4
0.2
0.0
0.0 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0
1.0
0.8
0.6
0.4
0.2
0.0
0.0 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0
1.0
0.8
0.6
0.4
0.2
0.0
0.0 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0
1.0
0.8
0.6
0.4
0.2
0.0
0.0 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0
Figure 1 – Kaplan Meyer curves for the outcomes.
177
Original Article
Pellegrini et al.Drug-eluting stents: long-term follow-up
Arq Bras Cardiol. 2014; 103(3):174-182
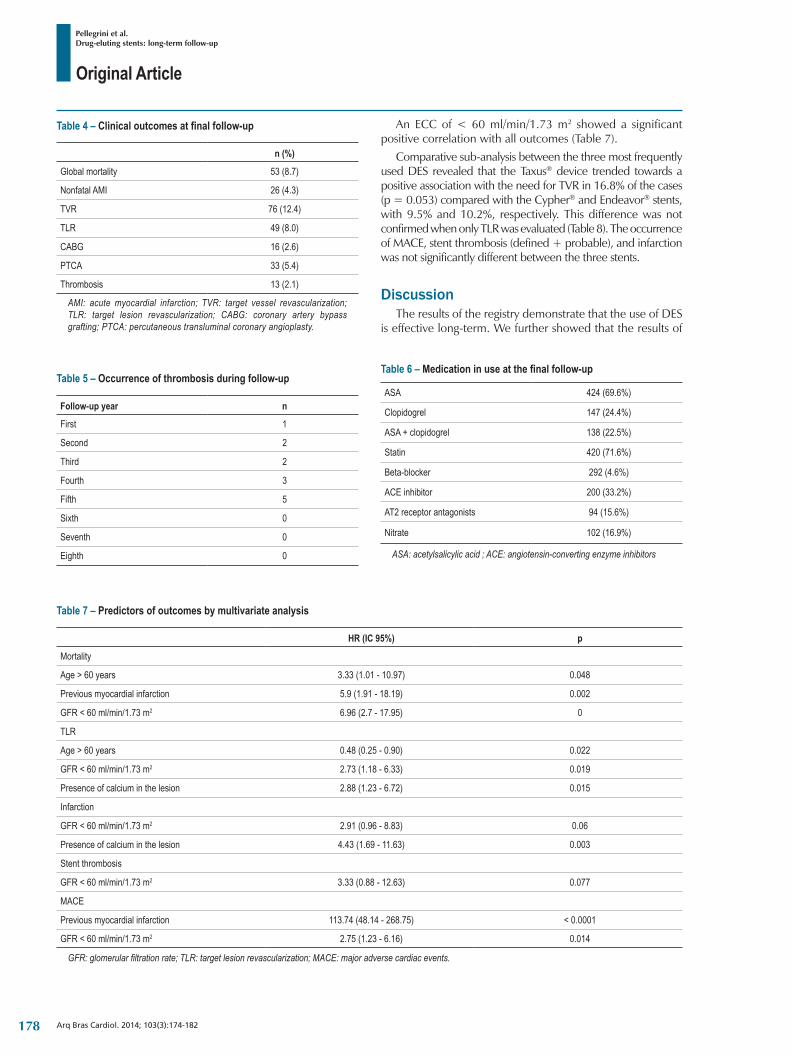
Table 4 – Clinical outcomes at final follow-up
n (%)
Global mortality 53 (8.7)
Nonfatal AMI 26 (4.3)
TVR 76 (12.4)
TLR 49 (8.0)
CABG 16 (2.6)
PTCA 33 (5.4)
Thrombosis 13 (2.1)
AMI: acute myocardial infarction; TVR: target vessel revascularization; TLR: target lesion revascularization; CABG: coronary artery bypass grafting; PTCA: percutaneous transluminal coronary angioplasty.
Table 6 – Medication in use at the final follow-up
ASA 424 (69.6%)
Clopidogrel 147 (24.4%)
ASA+clopidogrel 138 (22.5%)
Statin 420 (71.6%)
Beta-blocker 292 (4.6%)
ACE inhibitor 200 (33.2%)
AT2 receptor antagonists 94 (15.6%)
Nitrate 102 (16.9%)
ASA: acetylsalicylic acid ; ACE: angiotensin-converting enzyme inhibitors
Table 5 – Occurrence of thrombosis during follow-up
Follow-up year n
First 1
Second 2
Third 2
Fourth 3
Fifth 5
Sixth 0
Seventh 0
Eighth 0
Table 7 – Predictors of outcomes by multivariate analysis
HR (IC 95%) p
Mortality
Age > 60 years 3.33 (1.01 - 10.97) 0.048
Previous myocardial infarction 5.9 (1.91 - 18.19) 0.002
GFR < 60 ml/min/1.73 m2 6.96 (2.7 - 17.95) 0
TLR
Age > 60 years 0.48 (0.25 - 0.90) 0.022
GFR < 60 ml/min/1.73 m2 2.73 (1.18 - 6.33) 0.019
Presence of calcium in the lesion 2.88 (1.23 - 6.72) 0.015
Infarction
GFR < 60 ml/min/1.73 m2 2.91 (0.96 - 8.83) 0.06
Presence of calcium in the lesion 4.43 (1.69 - 11.63) 0.003
Stent thrombosis
GFR < 60 ml/min/1.73 m2 3.33 (0.88 - 12.63) 0.077
MACE
Previous myocardial infarction 113.74 (48.14 - 268.75) < 0.0001
GFR < 60 ml/min/1.73 m2 2.75 (1.23 - 6.16) 0.014
GFR: glomerular filtration rate; TLR: target lesion revascularization; MACE: major adverse cardiac events.
An ECC of < 60 ml/min/1.73 m2 showed a significant positive correlation with all outcomes (Table 7).
Comparative sub-analysis between the three most frequently used DES revealed that the Taxus® device trended towards a positive association with the need for TVR in 16.8% of the cases (p = 0.053) compared with the Cypher® and Endeavor® stents, with 9.5% and 10.2%, respectively. This difference was not confirmed when only TLR was evaluated (Table 8). The occurrence of MACE, stent thrombosis (defined + probable), and infarction was not significantly different between the three stents.
DiscussionThe results of the registry demonstrate that the use of DES
is effective long-term. We further showed that the results of
178

Original Article
Pellegrini et al.Drug-eluting stents: long-term follow-up
Arq Bras Cardiol. 2014; 103(3):174-182
Table 8 – Differences between the stents regarding outcomes
Cypher® Endeavor® Taxus®p value
n 255 118 291
Mortality 11 (4.3) 2 (1.7) 10 (3.4) 0.47
TVR 19 (9.5) 9 (10.2) 39 (16.8) 0.05
TLR 14 (7.0) 7 (8.0) 22 (9.5) 0.63
Infarction 24 (12.0) 12 (13.6) 41 (17.7) 0.24
Stent thrombosis 3 (1.5) 1 (1.1) 7 (3.0) 0.42
MACE 21 (8.20) 9 (7.6) 27 (9.2) 0.88
TVR: target vessel revascularization; TLR: target lesion revascularization; MACE: major adverse cardiac event.
randomized trials can be replicated in clinical practice, despite the inclusion of patients with a wide variety of clinical and angiographic characteristics that are high risk and complex9-17.
In the present study, the low incidence of adverse events, such as new revascularization and stent thrombosis, is similar to recent data that have demonstrated reduced occurrence of these events with DES long-term. The mortality rate observed during the 8 years of follow-up is similar to that demonstrated in most randomized trials with up to 6 years of follow-up9-13.
The long-term follow-up of patients is a key differentiator of this registry. The first report of the efficacy and safety of DES in unselected consecutive patients with complex disease came from the RESEARCH Registry. It demonstrated that the use of the Cypher® stent is associated with significantly lower rates of MACE and TVR compared with bare metal stents during a 6 month follow-up12.
The reduced incidence of new revascularizations at the 8 year follow-up reported in the present investigation also corroborates the data observed in several other clinical studies. They observed a reduced requirement for new revascularization of the target lesion, especially after 1 year9-20. Therefore, the hypothesis that DES would merely delay the phenomenon of restenosis has been rejected.
The incidence of stent thrombosis associated with DES was low in our study. The low number of patients using clopidogrel by the end of the follow-up period was expected because dual antiplatelet therapy has been recommended for only 12 months after DES.
The duration of dual antiplatelet therapy is a point of debate when discussing the risk of stent thrombosis21-24. A higher incidence of thrombosis with DES has been demonstrated when dual antiplatelet therapy is interrupted within the first 6 months after angioplasty24. Nevertheless, the impact of long-term use of dual antiplatelet therapy is debatable. The incidence of stent thrombosis was low in our study, despite the low number of patients using antiplatelet drugs at the end of the follow-up period. The highest rate of stent thrombosis was observed within the first year after the index angioplasty.
Studies comparing the incidence of stent thrombosis between DES and bare metal stents have generated conflicting data. Clinical trials have not included stent thrombosis as a primary outcome due to the low incidence of stent thrombosis
(0.5 to 1% per year). In a meta-analysis25,26, the incidence of stent thrombosis was found to be similar for both DES and bare metal stents during the first year. After 1 year, the risk of thrombosis with DES was reported to be higher26. In another study, no difference in stent thrombosis between DES and a bare metal stent was observed during a 15-month follow-up27. In a meta-analysis of trials limited to primary angioplasty for acute MI, the stent thrombosis rate observed with DES and bare metal stents was similar at 1 year of follow-up27.
The frequency of various clinical outcomes of bare metal stents and DES differs between clinical trial data and observational studies. Although clinical trials have demonstrated similar mortality and MI rates for DES and bare metal stents, observational real-world studies indicate a reduction in mortality in the DES group21-25. Recent studies indicate a significant reduction in the occurrence of stent thrombosis in second-generation DES versus bare metal stents9,28.
The effect of different generations of DES on clinical outcomes must also be considered. Few comparisons have been made between the Cypher®, Taxus®, and Endeavor® stents. One study indicated that the Endeavor® stent was not inferior to the Cypher® stent and was superior to the Taxus® stent when mortality from all causes, MI, and TVR were assessed at 12 months29,30. In our registry, the incidence of thrombosis, MI, and TLR was similar among those three stents. We observed a significant difference in the incidence of TVR between the groups, with a higher incidence in the Taxus® group.
Head-to-head comparisons between the Cypher® and Taxus® stents indicate a lower occurrence of stent thrombosis and TLR with the Cypher® stent31. Another head-to-head study comparing the Endeavor® and Taxus® stents with a follow-up period of > 1 year indicated a lower incidence of stent thrombosis with the Endeavor® stent32. Although these studies suggested a higher incidence of thrombosis with the Taxus® stent compared with other first-generation stents, the results were variable and inconclusive when stent thrombosis was assessed as the primary outcome21. Recent studies comparing the second-generation stent Xience V® versus Taxus® have demonstrated a lower incidence of stent thrombosis with Xience V®9,22,23, despite equal patient adherence to dual antiplatelet therapy during the first year of follow-up. A recent meta-analysis of clinical trials revealed a lower incidence of
179

Original Article
Pellegrini et al.Drug-eluting stents: long-term follow-up
Arq Bras Cardiol. 2014; 103(3):174-182
1. Daemen J, Serruys PW. Drug-eluting stent update 2007: part II: Unsettled issues. Circulation. 2007;116(8):961-8.
2. Holmes DR Jr, Kereiakes DJ, Laskey WK, Colombo A, Ellis SG, Henry TD, et al. Thrombosis and drug-eluting stents: an objective appraisal. J Am Coll Cardiol. 2007;50(2):109-18.
3. Jensen LO, Maeng M, Kaltoft A, Thayssen P, Hansen HH, Bottcher M, et al. Stent thrombosis, myocardial infarction, and death after drug-eluting and bare-metal stent coronary interventions. J Am Coll Cardiol. 2007;50(5):463-70.
4. Stettler C, Wandel S, Allemann S, Kastrati A, Morice MC, Schomig A, et al. Outcomes associated with drug-eluting and bare-metal stents: a collaborative network meta-analysis. Lancet. 2007;370(9591):937-48.
5. Pfisterer M, Brunner-La Rocca HP, Buser PT, Rickenbacher P, Hunziker P, Mueller C, et al; BASKET-LATE Investigators. Late clinical events after clopidogrel discontinuation may limit the benefit of drug-eluting stents: an observational study of drug-eluting versus bare-metal stents. J Am Coll Cardiol. 2006;48(12):2584-91.
6. Osorio Gomes V, Blaya P, Lasevitch R, Oliveira D, Hickmann P, Smidt L, et al. Impact of chronic kidney disease on the efficacy of drug-eluting stents: long-term follow-up study. Arq Bras Cardiol. 2011;96(5):346-51.
7. Laskey WK, Yancy CW, Maisel WH. Thrombosis in coronary drug-eluting stents: report from the meeting of the Circulatory System Medical Devices Advisory Panel of the Food and Drug Administration Center for Devices and Radiologic Health, December 7-8, 2006. Circulation. 2007;115(17):2352-7.
8. Ryan TJ, Faxon DP, Gunnar RM, Kennedy JW, King SB 3rd, Loop FD, et al. Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee on Percutaneous Transluminal Coronary Angioplasty). Circulation. 1988;78(2):486-502.
9. Bangalore S, Kumar S, Fusaro M, Amoroso N, Attubato MJ, Feit F, et al. Short- and long-term outcomes with drug-eluting and bare-metal coronary stents: a mixed-treatment comparison analysis of 117 762 patient-years of follow-up from randomized trials. Circulation. 2012;125(23):2873-91.
10. Bangalore S, Kumar S, Fusaro M, Amoroso N, Kirtane AJ, Byrne RA, et al. Outcomes with various drug eluting or bare metal stents in patients with diabetes mellitus: mixed treatment comparison analysis of 22,844 patient years of follow-up from randomised trials. BMJ. 2012;345:e5170.
11. Vogt A, Schoelmerich A, Pollner F, Schlitt M, Raaz U, Maegdefessel L, et al. Comparison of outcome in 1809 patients treated with drug-eluting stents or bare-metal stents in a real-world setting. Vasc Health Risk Manag. 2011;7:693-9.
12. Lemos PA, Hoye A, Goedhart D, Arampatzis CA, Saia F, van der Giessen WJ, et al. Clinical, angiographic, and procedural predictors of angiographic restenosis after sirolimus-eluting stent implantation in complex patients: an evaluation from the Rapamycin-Eluting Stent Evaluated At Rotterdam Cardiology Hospital (RESEARCH) study. Circulation. 2004;109(11):1366-70.
13. Costa JR Jr, Sousa A, Moreira AC, Costa RA, Cano M, Maldonado G, et al. Incidence and predictors of very late (>or=4 years) major cardiac adverse events in the DESIRE (Drug-Eluting Stents in the Real World)-Late registry. JACC Cardiovasc Interv. 2010;3(1):12-8.
14. Sousa A, Costa JR Jr, Moreira AC, Cano M, Maldonado G, Costa RA, et al. Long-term clinical outcomes of the Drug-Eluting Stents in the Real World (DESIRE) Registry. J Interv Cardiol. 2008;21(4):307-14.
15. Saia F, Piovaccari G, Manari A, Guastaroba P, Vignali L, Varani E, et al. Patient selection to enhance the long-term benefit of first generation drug-eluting stents for coronary revascularisation procedures. Insights from a large multicentre registry. EuroIntervention. 2009;5(1):57-66.
16. Ortolani P, Balducelli M, Marzaroli P, Piovaccari G, Menozzi A, Guiducci V, et al. Two-year clinical outcomes with drug-eluting stents for diabetic patients with de novo coronary lesions: results from a real-world multicenter registry. Circulation. 2008;117(7):923-30.
17. Marzocchi A, Saia F, Piovaccari G, Manari A, Aurier E, Benassi A, et al. Long-term safety and efficacy of drug-eluting stents: two-year results of the REAL (REgistro AngiopLastiche dell’Emilia Romagna) multicenter registry. Circulation. 2007 Jun 26;115(25):3181-8.
References
thrombosis with the Xience V®, compared with the Taxus® stent30. Thus, differences in stent thrombosis rates between the types of DES might exist, however, the magnitude of these differences is difficult to measure34-36.
Data from studies of this nature cannot be compared with those from clinical trials due to the nonrandomized, all-comers design. However, real world registries allow for the assessment of outcomes in clinical scenarios that are not tested in randomized studies.
The present study revealed adequate safety and efficacy of DES during a long-term clinical follow-up period in the real world. It included a significant proportion of patients at high cardiovascular risk, thereby validating the use of these stents for routine treatment of patients with coronary artery disease.
Author contributionsConception and design of the research: Gomes VO,
Lasevitch R, Caramori P, Pellegrini DO; Acquisition of data: Gomes VO, Lasevitch R, Ledur P, Caramori P, Pellegrini DO;
Analysis and interpretation of the data: Smidt L, Azeredo MA, Bodanese R, Sinnott L, Caramori P, Pellegrini DO; Statistical analysis: Ledur P, Caramori P, Pellegrini DO; Writing of the manuscript: Moriguchi E, Caramori P, Pellegrini DO; Critical revision of the manuscript for intellectual content: Moriguchi E, Caramori P.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This article is part of the thesis of master submitted by Denise Oliveira Pellegrini, from Universidade Federal do Rio Grande do Sul.
180
Original Article
Pellegrini et al.Drug-eluting stents: long-term follow-up
Arq Bras Cardiol. 2014; 103(3):174-182
18. Marroquin OC, Selzer F, Mulukutla SR, Williams DO, Vlachos HA, Wilensky RL, et al. A comparison of bare-metal and drug-eluting stents for off-label indications. N Engl J Med. 2008;358(4):342-52.
19. Morice MC, Serruys PW, Sousa JE, Fajadet J, Ban Hayashi E, Perin M, et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med. 2002;346(23):1773-80.
20. Dawkins KD, Grube E, Guagliumi G, Banning AP, Zmudka K, Colombo A, et al. Clinical efficacy of polymer-based paclitaxel-eluting stents in the treatment of complex, long coronary artery lesions from a multicenter, randomized trial: support for the use of drug-eluting stents in contemporary clinical practice. Circulation. 2005;112(21):3306-13.
21. Stone GW, Ellis SG, Cannon L, Mann JT, Greenberg JD, Spriggs D, et al; TAXUS V Investigators. Comparison of a polymer-based paclitaxel-eluting stent with a bare metal stent in patients with complex coronary artery disease: a randomized controlled trial. JAMA. 2005;294(10):1215-23.
22. Stone GW, Moses JW, Ellis SG, Schofer J, Dawkins KD, Morice MC, et al. Safety and efficacy of sirolimus- and paclitaxel-eluting coronary stents. N Engl J Med. 2007;356(10):998-1008.
23. Fajadet J, Wijns W, Laarman GJ, Kuck KH, Ormiston J, Baldus S, et al. Long-term follow-up of the randomised controlled trial to evaluate the safety and efficacy of the zotarolimus-eluting driver coronary stent in de novo native coronary artery lesions: five year outcomes in the ENDEAVOR II study. EuroIntervention. 2010;6(5):562-7.
24. Venkitachalam L, Lei Y, Stolker JM, Mahoney EM, Amin AP, Lindsey JB, et al. Clinical and economic outcomes of liberal versus selective drug-eluting stent use: insights from temporal analysis of the multicenter Evaluation of Drug Eluting Stents and Ischemic Events (EVENT) registry. Circulation. 2011;124(9):1028-37.
25. Holmes DR Jr, Kereiakes DJ, Garg S, Serruys PW, Dehmer GJ, Ellis SG, et al. Stent thrombosis. J Am Coll Cardiol. 2010;19;56(17):1357-65.
26. Gwon HC, Hahn JY, Park KW, Song YB, Chae IH, Lim DS, et al. Six-month versus 12-month dual antiplatelet therapy after implantation of drug-eluting stents: the Efficacy of Xience/Promus Versus Cypher to Reduce Late Loss After Stenting (EXCELLENT) randomized, multicenter study. Circulation. 2011;125(3):505-13.
27. Stefanini GG, Holmes DR Jr. Drug-eluting coronary-artery stents. N Engl J Med. 2013;368(3):254-65.
28. Ko DT, Chiu M, Guo H, Austin PC, Goeree R, Cohen E, et al. Safety and effectiveness of drug-eluting and bare-metal stents for patients with off- and on-label indications. J Am Coll Cardiol. 2009;53(19):1773-82.
29. Roukoz H, Bavry AA, Sarkees ML, Mood GR, Kumbhani DJ, Rabbat MG, et al. Comprehensive meta-analysis on drug-eluting stents versus bare-metal stents during extended follow-up. Am J Med. 2009;122(6):581.e1-10.
30. Fuchs AT, Kuehnl A, Pelisek J, Rolland PH, Mekkaoui C, Netz H, et al. Meta-analysis shows similar risk of thrombosis after drug-eluting stent, bare-metal stent, or angioplasty. Endothelium. 2008;15(1):93-100.
31. Brodie B, Pokharel Y, Fleishman N, Bensimhon A, Kissling G, Hansen C, et al. Very late stent thrombosis after primary percutaneous coronary intervention with bare-metal and drug-eluting stents for ST-segment elevation myocardial infarction: a 15-year single-center experience. JACC Cardiovasc Interv. 2011;4(1):30-8.
32. Palmerini T, Biondi-Zoccai G, Della Riva D, Stettler C, Sangiorgi D, D’Ascenzo F, et al. Stent thrombosis with drug-eluting and bare-metal stents: evidence from a comprehensive network meta-analysis. Lancet. 2012;379(9824):1393-402.
33. Jaffery Z, Prasad A, Lee JH, White CJ. Drug-eluting coronary stents - focus on improved patient outcomes. Patient Relat Outcome Meas. 2011;2:161-74.
34. Park DW, Kim YH, Yun SC, Kang SJ, Lee SW, Lee CW, et al. Comparison of zotarolimus-eluting stents with sirolimus- and paclitaxel-eluting stents for coronary revascularization: the ZEST (comparison of the efficacy and safety of zotarolimus-eluting stent with sirolimus-eluting and paclitaxel-eluting stent for coronary lesions) randomized trial. J Am Coll Cardiol. 2010;56(15):1187-95.
35. Schomig A, Dibra A, Windecker S, Mehilli J, Suarez de Lezo J, Kaiser C, et al. A meta-analysis of 16 randomized trials of sirolimus-eluting stents versus paclitaxel-eluting stents in patients with coronary artery disease. J Am Coll Cardiol. 2007;50(14):1373-80.
36. Leon MB, Nikolsky E, Cutlip DE, Mauri L, Liberman H, Wilson H, et al. Improved late clinical safety with zotarolimus-eluting stents compared with paclitaxel-eluting stents in patients with de novo coronary lesions: 3-year follow-up from the ENDEAVOR IV (Randomized Comparison of Zotarolimus- and Paclitaxel-Eluting Stents in Patients With Coronary Artery Disease) trial. JACC Cardiovasc Interv. 2010;3(10):1043-50.
181

Original Article
Pellegrini et al.Drug-eluting stents: long-term follow-up
Arq Bras Cardiol. 2014; 103(3):174-182182

Original Article
Do Diabetic Patients with Acute Coronary Syndromes Have a Higher Threshold for Ischemic Pain?Jose Carlos Nicolau1, Carlos Jose Dornas Gonçalves Barbosa1, Andre Franci, Luciano Moreira Baracioli1, Marcelo Franken1, Felipe Gallego Lima1, Roberto Rocha Giraldez1, Roberto Kalil Filho1, Jose Antônio Franchini Ramires1, Robert P. Giugliano2
Instituto do Coração (InCor) – Faculdade de Medicina da Universidade de São Paulo1, São Paulo, Brazil; Cardiovascular Division, Brigham and Women’s Hospital, Harvard Medical School2, Boston, MA, USA
Mailing Address: José Carlos Nicolau •Aureliano Coutinho, 355/1401, Higienopolis. Postal Code 01224-020, São Paulo, SP - Brazil.Email: [email protected]; [email protected] received April 17, 2014; revised manuscript April 17, 2014; accepted April 29, 2014.
DOI: 10.5935/abc.20140106
Abstract
Background: Data from over 4 decades have reported a higher incidence of silent infarction among patients with diabetes mellitus (DM), but recent publications have shown conflicting results regarding the correlation between DM and presence of pain in patients with acute coronary syndromes (ACS).
Objective: Our primary objective was to analyze the association between DM and precordial pain at hospital arrival. Secondary analyses evaluated the association between hyperglycemia and precordial pain at presentation, and the subgroup of patients presenting within 6 hours of symptom onset.
Methods: We analyzed a prospectively designed registry of 3,544 patients with ACS admitted to a Coronary Care Unit of a tertiary hospital. We developed multivariable models to adjust for potential confounders.
Results: Patients with precordial pain were less likely to have DM (30.3%) than those without pain (34.0%; unadjusted p = 0.029), but this difference was not significant after multivariable adjustment, for the global population (p = 0.84), and for subset of patients that presented within 6 hours from symptom onset (p = 0.51). In contrast, precordial pain was more likely among patients with hyperglycemia (41.2% vs 37.0% without hyperglycemia, p = 0.035) in the overall population and also among those who presented within 6 hours (41.6% vs. 32.3%, p = 0.001). Adjusted models showed an independent association between hyperglycemia and pain at presentation, especially among patients who presented within 6 hours (OR = 1.41, p = 0.008).
Conclusion: In this non-selected ACS population, there was no correlation between DM and hospital presentation without precordial pain. Moreover, hyperglycemia correlated significantly with pain at presentation, especially in the population that arrived within 6 hours from symptom onset. (Arq Bras Cardiol. 2014; 103(3):183-191)
Keywords: Diabetes Mellitus; Acute Coronary Syndrome; Chest Pain; Hyperglycemia.
IntroductionSince the 1960’s several investigators have reported a
correlation between the presence of diabetes mellitus (DM) and a higher threshold for ischemic pain1,2. Necropsy data demonstrated a higher incidence of lesions at afferent nerves that conduct pain3, supporting the hypothesis that patients with DM have impaired sensation of precordial pain. However, subsequent clinical data have provided conflicting results4-12.
For example, in analyses of patients undergoing exercise stress testing and 48-hour continuous electrocardiographic
monitoring to evaluate ischemia, Caracciolo et al.5 found a similar prevalence of asymptomatic ischemia using both modalities in diabetics compared with non-diabetics. Meanwhile, Falcone et al6 found an even higher incidence of angina during daily activities in patients with DM, while others reported a higher prevalence of painless ischemia among patients with DM7.
Another method to explore the association between DM and symptomatic ischemia is to analyze the rate of unrecognized (silent) myocardial infarction in longitudinal studies. The majority of the publications report an absence of correlation between the presence of DM and silent MI, even when taking into account the presence of diabetic neuropathy8-11. These findings led Sheffer et al. to comment in a review of the topic that, “none of the existing epidemiologic analyses have identified diabetes as an independent predictor of infarct recognition”12.
Analyses of the presence of chest pain at hospital arrival in patients with or without diabetes with acute coronary syndromes (ACS) represent a third opportunity to explore this question –
183

Original Article
Nicolau et al.Diabetes and ischemic pain
Arq Bras Cardiol. 2014; 103(3):183-191
results to date have been conflicting13,14. Since hyperglycemia is a strong predictor of in-hospital mortality15-18, and admission with ACS often represents the unmasking of previously undiagnosed DM19, exploration of the association between hyperglycemia at presentation and presence or absence of pain with ACS represents another venue to explore this issue.
The main purpose of this study was to analyze the associations between prior diabetes and the presence or absence of precordial pain in patients presenting at the hospital with ACS. The secondary aims included exploring the association between hyperglycemia and precordial pain, as well as analyzing the same associations in the subgroup of patients arriving at the hospital within 6 hours of symptom onset.
MethodsWe analyzed data from a cohort of 3544 consecutive
non-selected patients with ACS (1405 with ST-segment elevation myocardial infarction (STEMI), 1425 with non-STEMI, and 724 unstable angina) from a prospective registry of patients admitted to a coronary care unit of a tertiary hospital from 02/1998 to 04/2012. The registry included patients whose symptom onset started within 7 days, and included patients who were transferred from another hospital. We have used standard definitions to diagnose AMI as described in the concurrent guidelines, with measurement of creatine-kinase myocardial band (CK-MB) mass and cardiac troponin I on a routine basis from 2001 onward.
The presence of precordial pain at hospital arrival was determined by review of the patient’s information obtained by the admitting physician(s) in the coronary care unit. Patient who were unconscious or disoriented were excluded. Patients who experienced other symptoms, such as dyspnea, fatigue, or other “ischemic equivalents” were classified as not having precordial pain. We defined the presence of diabetes mellitus from the medical history and/or use of glucose lowering drugs. Patients who had newly diagnosed diabetes during hospitalization were classified as not having diabetes at presentation. We defined hyperglycemia as the presence of a blood glucose level of > 125 mg/dL measured in the local hospital laboratory on the first measurement after hospital arrival.
Statistical analysesThe Chi-square and Fisher exact test were used for the
comparison between categorical variables as appropriate. The Mann-Whitney (non-normal distribution, as determined by the Kolmogorov-Smirnov test) or Student’s t-test (normal distribution) was used for comparisons between continuous variables.
Model developmentSeveral adjusted models were developed to analyze the
association between history of diabetes or hyperglycemia and presence of absence of pain at hospital arrival, using the backward stepwise logistic regression method. Those variables were chosen to develop a broad scenario regarding
patient information at hospital arrival. The first 3 models tested the correlation between history of diabetes and pain at hospital arrival. Model 1A included as independent variables those listed in Table 1, except time from symptom onset and hyperglycemia. Model 1B included the same variables, plus time from symptom onset (as a continuous variable). Finally, model 1C was similar to model 1A, but was restricted to the population arriving at the hospital within 6 hours of symptom onset. Because history of diabetes was excluded in the first steps of the development of models 1A, 1B and 1C, similar additional models were developed, forcing the variable (history of diabetes) into the model. In order to analyze the association between hyperglycemia and pain at hospital arrival, we substituted history of diabetes by hyperglycemia in models 1A, 1B and 1C, generating models 2A, 2B and 2C respectively. Because hyperglycemia was excluded in the early steps of model 2A development, an additional model forcing the variable hyperglycemia until the last step was developed.
SPSS version 20.0 software (IBM, USA) was used for the analyses and a p-value < 0.05 (2-tailed) was considered statistically significant, with no corrections for multiple comparisons.
ResultsThe characteristics of the population are shown in
Table 1. The mean age was 64.1 years and 68.6% were men. As commonly seen in tertiary hospitals, the incidence of risk factors was high, including 31.5% with known diabetes. As expected, significant differences were observed between the groups with vs. without precordial pain. For example, patients in the painless group were older and more likely to be smokers; on the other hand, this group had lower rates of previous heart failure, hypertension, coronary artery bypass graft surgery and were less likely to present with STEMI.
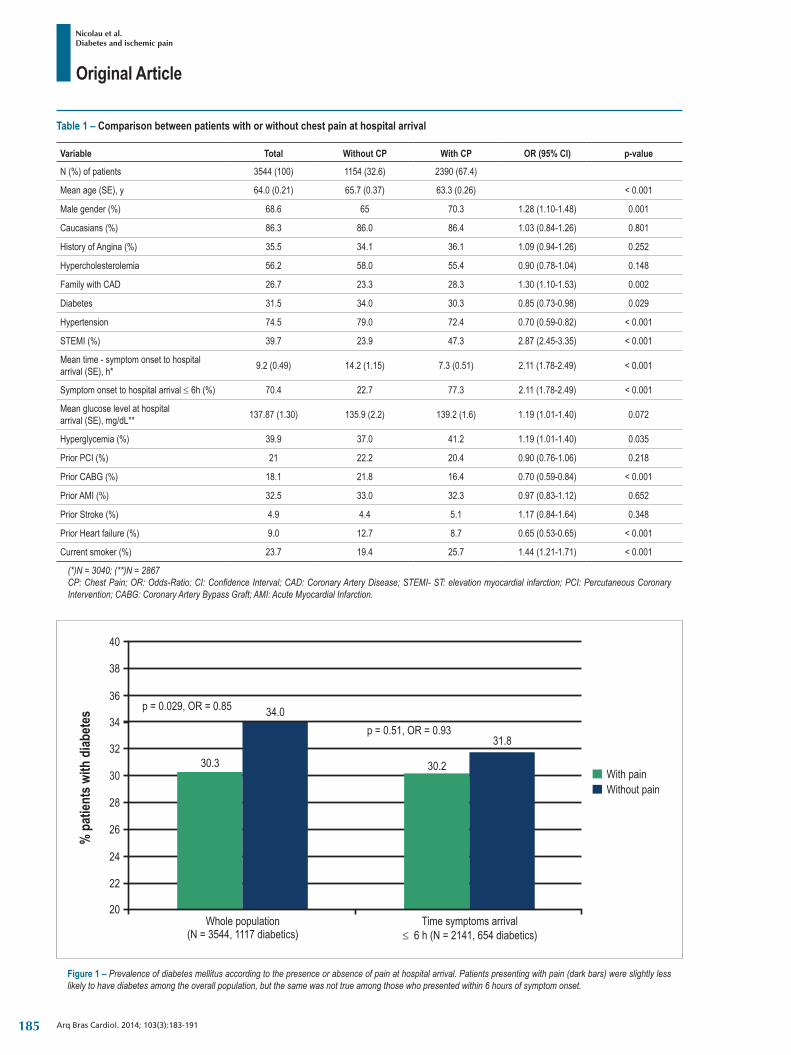
Figure 1 shows the unadjusted associations between a history of diabetes and presence of precordial pain at hospital arrival in the overall population (diabetes present in 30.3% with vs. 34.0% without pain, p = 0.029), as well as the subgroup who presented within 6 hours of symptom onset (30.2% vs 31.8%, p = 0.51).
There was no significant correlation between the presence of pain and in-hospital deaths (overall population: 8.8% for the painless group vs. 8.0% for the group with precordial pain, p = 0.44; subgroup within 6 hours from symptom onset: 7.6% vs. 7.2%, p = 0.74). Meanwhile, there was a higher rate of in-hospital mortality among patients with history of diabetes (overall population: DM 10.1% vs 7.4% for no DM, p = 0.006; subgroup within 6 hours of symptom onset 9.5% vs. 6.3%, p = 0.010).
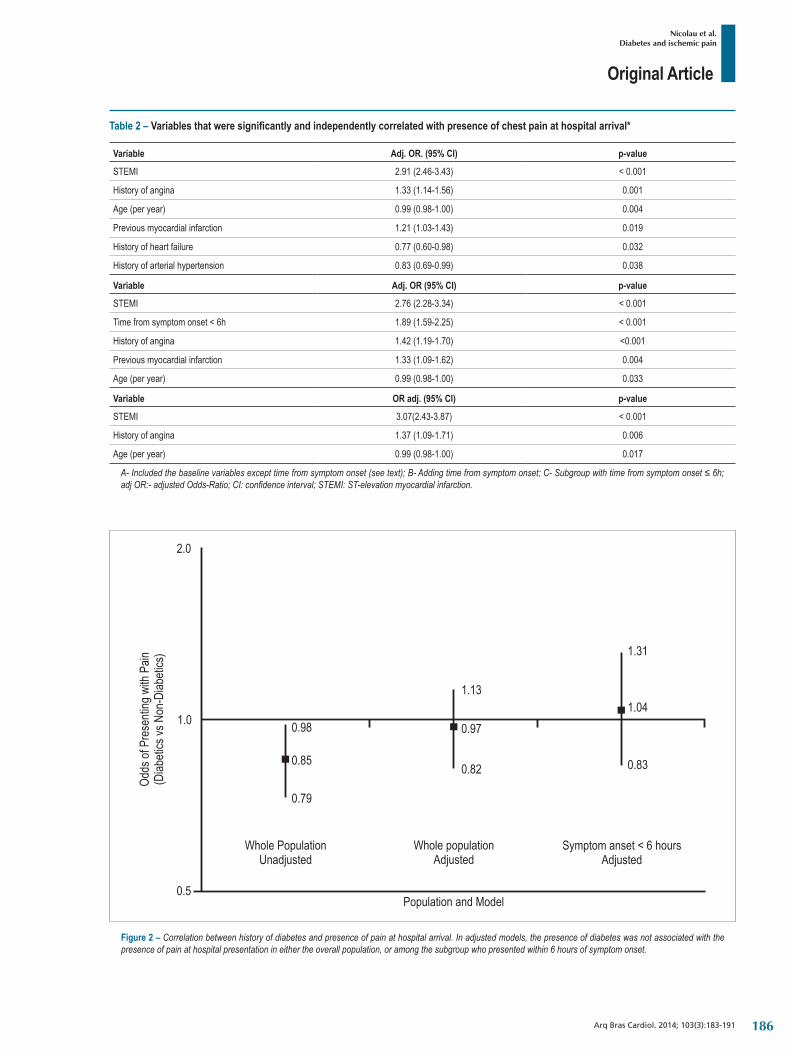
Table 2 shows the variables that independently correlated with the presence of pain at hospital arrival in models 1A, 1B and 1C. Notably, a history of diabetes was not a significant predictor in any of the 3 models, with ORs of 0.97 (p = 0.67), 0.98 (p = 0.84) and 1.04 (p = 0.72), respectively when forced into models 1A, 1B and 1C. Figure 2 depicts the unadjusted and adjusted odds-ratios for the correlation between a history of diabetes and the presence of pain at hospital arrival.
184
Original Article
Nicolau et al.Diabetes and ischemic pain
Arq Bras Cardiol. 2014; 103(3):183-191
Figure 1 – Prevalence of diabetes mellitus according to the presence or absence of pain at hospital arrival. Patients presenting with pain (dark bars) were slightly less likely to have diabetes among the overall population, but the same was not true among those who presented within 6 hours of symptom onset.
Table 1 – Comparison between patients with or without chest pain at hospital arrival
Variable Total Without CP With CP OR (95% CI) p-value
N (%) of patients 3544 (100) 1154 (32.6) 2390 (67.4)
Mean age (SE), y 64.0 (0.21) 65.7 (0.37) 63.3 (0.26) < 0.001
Male gender (%) 68.6 65 70.3 1.28 (1.10-1.48) 0.001
Caucasians (%) 86.3 86.0 86.4 1.03 (0.84-1.26) 0.801
History of Angina (%) 35.5 34.1 36.1 1.09 (0.94-1.26) 0.252
Hypercholesterolemia 56.2 58.0 55.4 0.90 (0.78-1.04) 0.148
FamilywithCAD 26.7 23.3 28.3 1.30 (1.10-1.53) 0.002
Diabetes 31.5 34.0 30.3 0.85 (0.73-0.98) 0.029
Hypertension 74.5 79.0 72.4 0.70 (0.59-0.82) < 0.001
STEMI (%) 39.7 23.9 47.3 2.87 (2.45-3.35) < 0.001
Mean time - symptom onset to hospital arrival (SE), h* 9.2 (0.49) 14.2 (1.15) 7.3 (0.51) 2.11 (1.78-2.49) < 0.001
Symptom onset to hospital arrival ≤ 6h (%) 70.4 22.7 77.3 2.11 (1.78-2.49) < 0.001
Mean glucose level at hospital arrival (SE), mg/dL** 137.87 (1.30) 135.9 (2.2) 139.2 (1.6) 1.19 (1.01-1.40) 0.072
Hyperglycemia (%) 39.9 37.0 41.2 1.19 (1.01-1.40) 0.035
Prior PCI (%) 21 22.2 20.4 0.90 (0.76-1.06) 0.218
Prior CABG (%) 18.1 21.8 16.4 0.70 (0.59-0.84) < 0.001
Prior AMI (%) 32.5 33.0 32.3 0.97 (0.83-1.12) 0.652
Prior Stroke (%) 4.9 4.4 5.1 1.17 (0.84-1.64) 0.348
Prior Heart failure (%) 9.0 12.7 8.7 0.65 (0.53-0.65) < 0.001
Current smoker (%) 23.7 19.4 25.7 1.44 (1.21-1.71) < 0.001
(*)N = 3040; (**)N = 2867CP: Chest Pain; OR: Odds-Ratio; CI: Confidence Interval; CAD: Coronary Artery Disease; STEMI- ST: elevation myocardial infarction; PCI: Percutaneous Coronary Intervention; CABG: Coronary Artery Bypass Graft; AMI: Acute Myocardial Infarction.
185
Original Article
Nicolau et al.Diabetes and ischemic pain
Arq Bras Cardiol. 2014; 103(3):183-191
Table 2 – Variables that were significantly and independently correlated with presence of chest pain at hospital arrival*
Variable Adj. OR. (95% CI) p-value
STEMI 2.91 (2.46-3.43) < 0.001
History of angina 1.33 (1.14-1.56) 0.001
Age (per year) 0.99 (0.98-1.00) 0.004
Previous myocardial infarction 1.21 (1.03-1.43) 0.019
History of heart failure 0.77 (0.60-0.98) 0.032
History of arterial hypertension 0.83 (0.69-0.99) 0.038
Variable Adj. OR (95% CI) p-value
STEMI 2.76 (2.28-3.34) < 0.001
Time from symptom onset < 6h 1.89 (1.59-2.25) < 0.001
History of angina 1.42 (1.19-1.70) <0.001
Previous myocardial infarction 1.33 (1.09-1.62) 0.004
Age (per year) 0.99 (0.98-1.00) 0.033
Variable OR adj. (95% CI) p-value
STEMI 3.07(2.43-3.87) < 0.001
History of angina 1.37 (1.09-1.71) 0.006
Age (per year) 0.99 (0.98-1.00) 0.017
A- Included the baseline variables except time from symptom onset (see text); B- Adding time from symptom onset; C- Subgroup with time from symptom onset ≤ 6h; adj OR:- adjusted Odds-Ratio; CI: confidence interval; STEMI: ST-elevation myocardial infarction.
Figure 2 – Correlation between history of diabetes and presence of pain at hospital arrival. In adjusted models, the presence of diabetes was not associated with the presence of pain at hospital presentation in either the overall population, or among the subgroup who presented within 6 hours of symptom onset.
186

Original Article
Nicolau et al.Diabetes and ischemic pain
Arq Bras Cardiol. 2014; 103(3):183-191
There was a significant correlation (unadjusted) between hyperglycemia at presentation and the presence of precordial pain at hospital arrival in the overall population and also in the subgroup that arrived in the hospital within 6 hours of symptom onset (Figure 3). Moreover, hyperglycemia was associated with a significantly higher rate of in-hospital mortality: 13.9% vs. 5.0% for patients with vs. without hyperglycemia (OR = 3.07, p < 0.001) for the overall population and 12.9% vs. 4.1% (OR = 3.43, p < 0.001) for those within 6 hours of symptom onset. Finally, hyperglycemia was significantly associated with STEMI (OR = 1.53, p < 0.001), presence of precordial pain at hospital arrival (OR = 1.49, p = 0.001) and history of diabetes (OR = 7.44, p < 0.001).
In the three adjusted models (Table 3), there was a positive correlation between hyperglycemia and presence of precordial pain in models 2B and 2C, but not in 2A, where the OR for hyperglycemia was 1.14 (p = 0.14). Figure 4 shows the unadjusted and adjusted odds-ratios for the association between hyperglycemia and presence of precordial pain at hospital arrival. Overall, considering all 6 models developed, the variables that best correlated with the presence of precordial pain at hospital arrival were presentation with STEMI and previous angina (significant correlation in all the 6 models), while older age and prior MI were significant correlated with precordial pain in 5 out of the 6 models.
DiscussionWe showed in this analysis of 3544 consecutive and
unselected patients with ACS admitted to the coronary care unit of a tertiary hospital that:
(1) A history of DM was not independently associated with precordial pain at hospital arrival in any of the adjusted models;
(2) The presence of hyperglycemia was independently correlated with precordial pain in 2 of the 3 adjusted models;
(3) Presentation with STEMI and a prior history of angina were most strongly associated with presentation with precordial pain at hospital arrival.
Potential causes of blunted perception of ACS in patients with DM include receptor and afferent neuron dysfunction, gating mechanisms and neuropsychiatric factors. While autonomic neuropathy has been proposed by some as the possible explanation for the relatively high incidence of painless ischemia in diabetic patients3, others have failed to demonstrate cardiac denervation in patients with DM20. As noted by Sheifer et al12, diabetic neuropathy may impair recognition of pain, but significant neurological dysfunction typically appears only in patients with advanced disease.
In 1973, Margolis et a8 published their classic paper, showing that out of 259 patients with electrocardiographically documented MI, 23% were discovered only by routine ECG at the time of the patient’s bi-annual routine examination. Moreover, they showed that unrecognized MI is rare in patients with prior angina pectoris and despite a numerically higher incidence in patients with diabetes or hypertension, the difference did not reach statistical significance8. In 1995 Sigurdsson et al10 obtained similar results: at least one third
of all MI were unrecognized, there was a strong correlation between absence of angina and unrecognized MI and risk factor profiles were similar in recognized or unrecognized MI. In a recently published review, the prevalence of silent MI in the general population varied from 22% to 64% and from 29% to 79% in diabetic patients11.
Specifically among patients with acute myocardial infarction, 33% of patients did not have precordial pain in a North-American registry (National Registry of Myocardial Infarction 2)13, while the incidence was much lower (10%) in a report from South Korea21. However, it is noteworthy that this difference could be explained, at least in part, by the fact that the South Korean registry included only patients with STEMI undergoing primary PCI, whereas the North-American registry included an unselected population of AMI patients. The present study was more similar to the North-American registry in that we analyzed data from an unselected population, and indeed found a similar percentage of patients who did not experience precordial pain (32.7%).
We did not find a strong correlation between the absence of precordial pain and diabetes in our registry of patients with ACS. Similar findings were first described by Christensen et al in 198522 in a population of patients with AMI, and were subsequently replicated in recent registries14. However, the aforementioned North-American registry did find a significant and independent association between the absence of precordial pain and presence of diabetes (adjusted OR 1.21, 95% CI 1.19-1.23)13, contrary to the findings in our study and the others described above. Importantly, the North American registry did not adjust for STEMI as a potential confounder, despite the strong correlation between the presence of precordial pain and presentation with STEMI.
To the best of our knowledge, our analysis is one of the first to report the association between hyperglycemia at presentation and the presence of precordial pain. We found a positive correlation, especially for patients arriving to the hospital within 6 hours from symptom onset. One possible explanation for the finding could be related to the highly significant correlation between hyperglycemia at presentation and STEMI, the most acute of all manifestations of coronary artery disease.
We recognize several limitations to our analyses. First, although the registry sample was prospectively collected, the present analyses were retrospective and, therefore, they have the limitations of this type of clinical investigation. Secondly, only one question regarding the presence or absence of precordial pain at hospital arrival was ascertained in the dataset, with no information obtained regarding other symptoms such as dyspnea, nausea, syncope, fatigue or regarding the characteristics of the pain. Thirdly, we did not collect information on the type of diabetic therapy; however, it is important to note that Kentsch et al14 did not find any correlation between the use of insulin and presence of angina. Lastly, we cannot exclude the possibility of bias in the selection of patients included in this registry, as one might expect a higher rate of hospitalization for patients who experience precordial pain compared with those without pain.
187
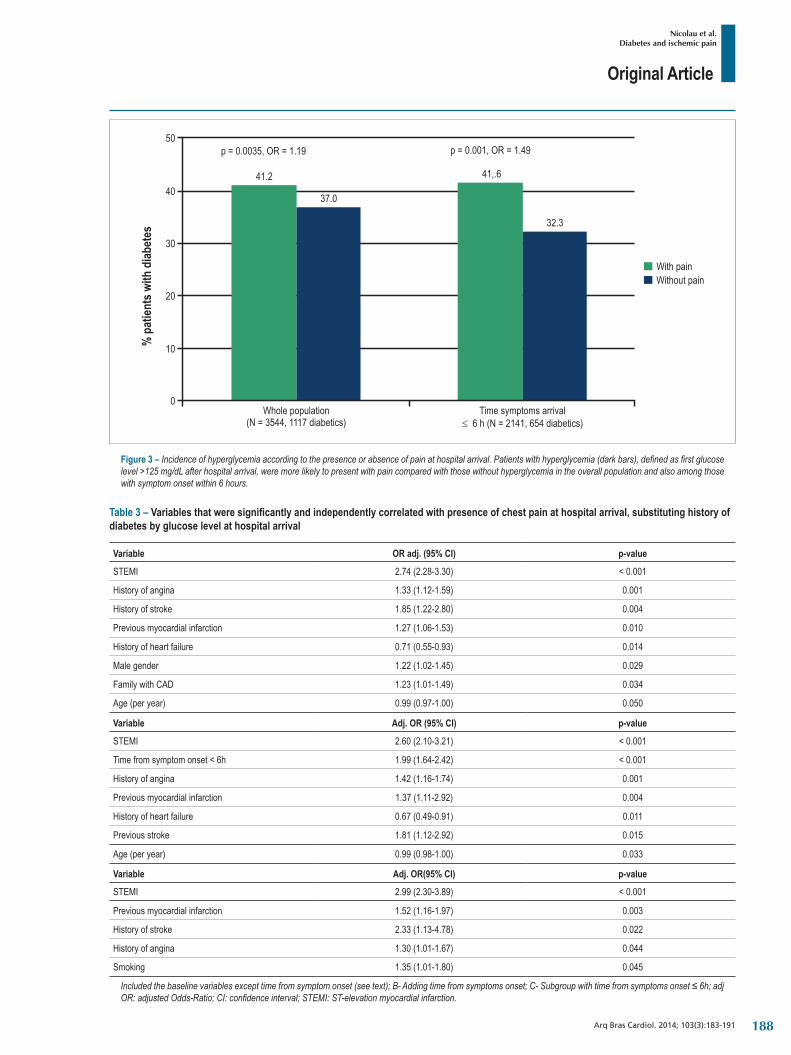
Original Article
Nicolau et al.Diabetes and ischemic pain
Arq Bras Cardiol. 2014; 103(3):183-191
Figure 3 – Incidence of hyperglycemia according to the presence or absence of pain at hospital arrival. Patients with hyperglycemia (dark bars), defined as first glucose level >125 mg/dL after hospital arrival, were more likely to present with pain compared with those without hyperglycemia in the overall population and also among those with symptom onset within 6 hours.
Table 3 – Variables that were significantly and independently correlated with presence of chest pain at hospital arrival, substituting history of diabetes by glucose level at hospital arrival
Variable OR adj. (95% CI) p-value
STEMI 2.74 (2.28-3.30) < 0.001
History of angina 1.33 (1.12-1.59) 0.001
History of stroke 1.85 (1.22-2.80) 0.004
Previous myocardial infarction 1.27 (1.06-1.53) 0.010
History of heart failure 0.71 (0.55-0.93) 0.014
Male gender 1.22 (1.02-1.45) 0.029
FamilywithCAD 1.23 (1.01-1.49) 0.034
Age (per year) 0.99 (0.97-1.00) 0.050
Variable Adj. OR (95% CI) p-value
STEMI 2.60 (2.10-3.21) < 0.001
Time from symptom onset < 6h 1.99 (1.64-2.42) < 0.001
History of angina 1.42 (1.16-1.74) 0.001
Previous myocardial infarction 1.37 (1.11-2.92) 0.004
History of heart failure 0.67 (0.49-0.91) 0.011
Previous stroke 1.81 (1.12-2.92) 0.015
Age (per year) 0.99 (0.98-1.00) 0.033
Variable Adj. OR(95% CI) p-value
STEMI 2.99 (2.30-3.89) < 0.001
Previous myocardial infarction 1.52 (1.16-1.97) 0.003
History of stroke 2.33 (1.13-4.78) 0.022
History of angina 1.30 (1.01-1.67) 0.044
Smoking 1.35 (1.01-1.80) 0.045
Included the baseline variables except time from symptom onset (see text); B- Adding time from symptoms onset; C- Subgroup with time from symptoms onset ≤ 6h; adj OR: adjusted Odds-Ratio; CI: confidence interval; STEMI: ST-elevation myocardial infarction.
188
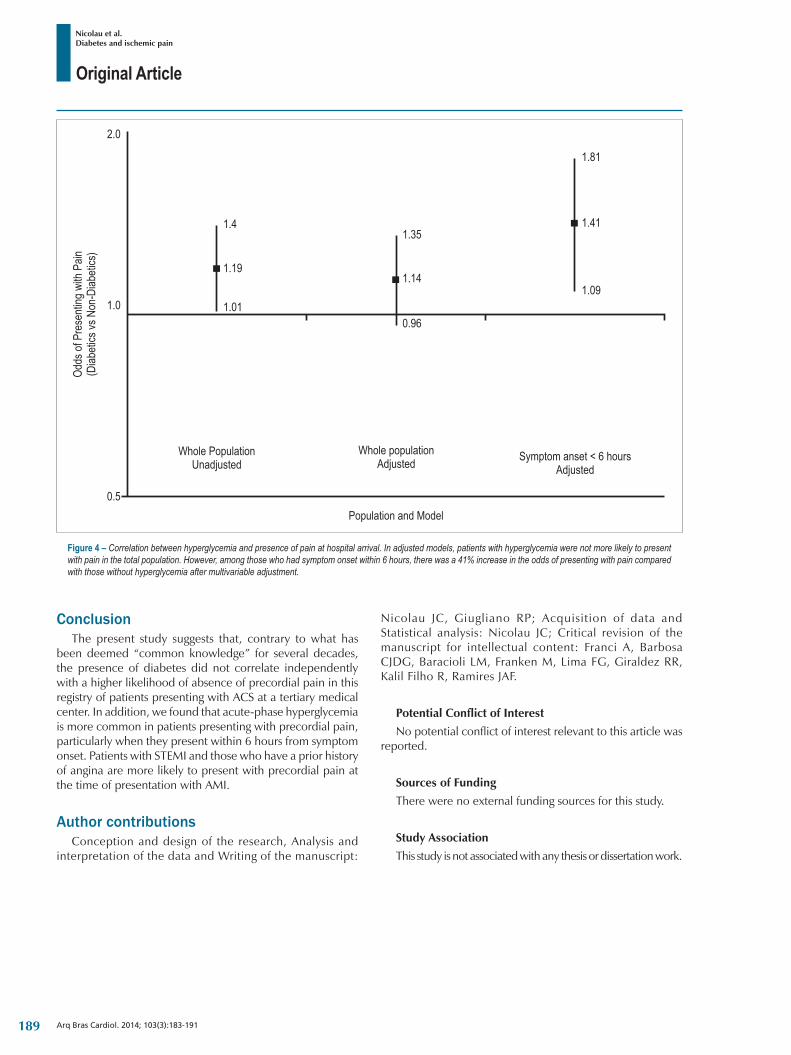
Original Article
Nicolau et al.Diabetes and ischemic pain
Arq Bras Cardiol. 2014; 103(3):183-191
Figure 4 – Correlation between hyperglycemia and presence of pain at hospital arrival. In adjusted models, patients with hyperglycemia were not more likely to present with pain in the total population. However, among those who had symptom onset within 6 hours, there was a 41% increase in the odds of presenting with pain compared with those without hyperglycemia after multivariable adjustment.
ConclusionThe present study suggests that, contrary to what has
been deemed “common knowledge” for several decades, the presence of diabetes did not correlate independently with a higher likelihood of absence of precordial pain in this registry of patients presenting with ACS at a tertiary medical center. In addition, we found that acute-phase hyperglycemia is more common in patients presenting with precordial pain, particularly when they present within 6 hours from symptom onset. Patients with STEMI and those who have a prior history of angina are more likely to present with precordial pain at the time of presentation with AMI.
Author contributionsConception and design of the research, Analysis and
interpretation of the data and Writing of the manuscript:
Nicolau JC, Giugliano RP; Acquisition of data and Statistical analysis: Nicolau JC; Critical revision of the manuscript for intellectual content: Franci A, Barbosa CJDG, Baracioli LM, Franken M, Lima FG, Giraldez RR, Kalil Filho R, Ramires JAF.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis study is not associated with any thesis or dissertation work.
189
Original Article
Nicolau et al.Diabetes and ischemic pain
Arq Bras Cardiol. 2014; 103(3):183-191
1. Bradley RF, Schonfeld A. Diminished pain in diabetic patients with acute myocardial infarction. Geriatrics. 1962;17:322-6.
2. Vaisrub S. Painless myocardia l infarct ion in diabetes. JAMA. 1978;239(17):1790.
3. Faerman I, Faccio E, Milei J, Nunez R, Jadzinsky M, Fox D, et al. Autonomic neuropathy and painless myocardial infarction in diabetic patients: histologic evidence of their relationship. Diabetes. 1977;26(12):1147-58.
4. Chiariello M, Indolfi C. Silent myocardial ischemia in patients with diabetes mellitus. Circulation. 1996;93(12):2089-91.
5. Caracciolo EA, Chaitman BR, Forman SA, Stone PH, Bourassa MG, Sopko G, et al. Diabetics with coronary disease have a prevalence of asymptomatic ischemia during exercise treadmill testing and ambulatory ischemia monitoring similar to that of nondiabetic patients. An ACIP database study. ACIP Investigators. Asymptomatic Cardiac Ischemia Pilot Investigators. Circulation. 1996;93(12):2097-105.
6. Falcone C, Nespoli L, Geroldi D, Gazzaruso C, Buzzi MP, Auguadro C, et al. Silent myocardial ischemia in diabetic and nondiabetic patients with coronary artery disease. Int J Cardiol. 2003;90(2-3):219-27.
7. Nesto RW, Phillips RT, Kett KG, Hill T, Perper E, Young E, et al. Angina and exertional myocardial ischemia in diabetic and nondiabetic patients: assessment by exercise thallium scintigraphy. Ann Intern Med. 1988;108(2):170-5.
8. Margolis JR, Kannel WS, Feinleib M, Dawber TR, McNamara PM. Clinical features of unrecognized myocardial infarction--silent and symptomatic. Eighteen year follow-up: the Framingham study. Am J Cardiol. 1973;32(1):1-7.
9. Burgess DC, Hunt D, Li L, Zannino D, Williamson E, Davis TM, et al. Incidence and predictors of silent myocardial infarction in type 2 diabetes and the effect of fenofibrate: an analysis from the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) study. Eur Heart J. 2010;31(1):92-9.
10. Sigurdsson E, Thorgeirsson G, Sigvaldason H, Sigfusson N. Unrecognized myocardial infarction: epidemiology, clinical characteristics, and the prognostic role of angina pectoris. The Reykjavik Study. Ann Intern Med. 1995;122(2):96-102.
11. Valensi P, Lorgis L, Cottin Y. Prevalence, incidence, predictive factors and prognosis of silent myocardial infarction: a review of the literature. Arch Cardiovasc Dis. 2011;104(3):178-88.
12. Sheifer SE, Manolio TA, Gersh BJ. Unrecognized myocardial infarction. Ann Intern Med. 2001;135(9):801-11.
13. Canto JG, Shlipak MG, Rogers WJ, Malmgren JA, Frederick PD, Lambrew CT, et al. Prevalence, clinical characteristics, and mortality among patients with myocardial infarction presenting without chest pain. JAMA. 2000;283(24):3223-9.
14. Kentsch M, Rodemerk U, Gitt AK, Schiele R, Wienbergen H, Schubert J, et al. Angina intensity is not different in diabetic and non-diabetic patients with acute myocardial infarction. Z Kardiol. 2003;92(10):817-24.
15. Nicolau JC, Serrano CV Jr, Giraldez RR, Baracioli LM, Moreira HG, Lima F, et al. In patients with acute myocardial infarction, the impact of hyperglycemia as a risk factor for mortality is not homogeneous across age-groups. Diabetes Care. 2012;35(1):150-2.
16. Qaseem A, Humphrey LL, Chou R, Snow V, Shekelle P. Use of intensive insulin therapy for the management of glycemic control in hospitalized patients: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2011;154(4):260-7.
17. Jneid H, Anderson JL, Wright RS, Adams CD, Bridges CR, Casey DE, et al. 2012 ACCF/AHA Focused Update of the Guideline for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction (Updating the 2007 Guideline and Replacing the 2011 Focused Update): A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(7):645-81.
18. O’Gara PT, Kushner FG, Ascheim DD, Casey DE, Chung MK, de Lemos JA, et al. 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61(4):485-510.
19. Ladeira RT, Baracioli LM, Faulin TE, Abdalla DS, Seydell TM, Maranhão RC, et al. Unrecognized diabetes and myocardial necrosis: predictors of hyperglycemia in myocardial infarction. Arq Bras Cardiol. 2013;100(5):404-11.
20. Park AM, Armin S, Azarbal A, Lai A, Chen PS, Fishbein MC. Distribution of cardiac nerves in patients with diabetes mellitus: an immunohistochemical postmortem study of human hearts. Cardiovasc Pathol. 2002;11(6):326-31.
21. Cho JY, Jeong MH, Ahn YK, Kim JH, Chae SC, Kim YJ, et al. Comparison of outcomes of patients with painless versus painful ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention. Am J Cardiol. 2012;109(3):337-43.
22. Christensen PD, Kofoed PE, Seyer-Hansen K. Painless myocardial infarction in diabetes mellitus--a myth? Dan Med Bull. 1985;32(5):273-5.
References
190

Original Article
Nicolau et al.Diabetes and ischemic pain
Arq Bras Cardiol. 2014; 103(3):183-191191
Original Article
Investigation Route of the Coronary Patient in the Public Health System in Curitiba, São Paulo and in Incor – IMPACT StudyJuliano J. Cerci1,4, Evelinda Trindade1,3, Daniel Preto1, Rodrigo Julio Cerci4, Pedro A. Lemos1, Luiz Antonio Machado Cesar4, Luís Preto2, Luiz Stinghen5, Cátia Martinez3, Jose Claudio Meneghetti4 Incor-FMUSP1; Secretaria Municipal de Saúde de São Paulo2; Secretaria Estadual da Saúde de São Paulo3, São Paulo, SP; Quanta Diagnostico Nuclear4; Secretaria Municipal de Curitiba5, Curitiba, PR - Brazil
Mailing Address: Juliano Julio Cerci •Av. Sete de Setembro, 4.699, Batel. Postal Code 80240-001, Curitiba, PR – BrazilE-mail: [email protected]; [email protected] December 18, 2013; revised manuscript April 22, 2014; accepted April 29, 2014.
DOI: 10.5935/abc.20140107
Abstract
Background: The investigation of stable coronary artery disease (CAD) and its treatment depend on risk stratification for decision-making on the need for cardiac catheterization and revascularization.
Objective: To analyze the procedures used in the diagnosis and invasive treatment of patients with CAD, at the Brazilian Unified Health System (SUS) in the cities of Curitiba, São Paulo and at InCor-FMUSP.
Methods: Retrospective, descriptive, observational study of the diagnostic and therapeutic itineraries of the Brazilian public health care system patient, between groups submitted or not to prior noninvasive tests to invasive cardiac catheterization. Stress testing, stress echocardiography, perfusion scintigraphy, catheterization and percutaneous or surgical revascularization treatment procedures were quantified and the economic impact of the used strategies.
Results: There are significant differences in the assessment of patients with suspected or known CAD in the metropolitan region in the three scenarios. Although functional testing procedures are most often used the direct costs of these procedures differ significantly (6.1% in Curitiba, 20% in São Paulo and 27% in InCor-FMUSP). Costs related to the procedures and invasive treatments represent 59.7% of the direct costs of SUS in São Paulo and 87.2% in Curitiba. In InCor-FMUSP, only 24.3% of patients with stable CAD submitted to CABG underwent a noninvasive test before the procedure.
Conclusion: Although noninvasive functional tests are the ones most often requested for the assessment of patients with suspected or known CAD most of the costs are related to invasive procedures/treatments. In most revascularized patients, the documentation of ischemic burden was not performed by SUS. (Arq Bras Cardiol. 2014; 103(3):192-200)
Keywords: Coronary Artery Disease / therapy; Coronary Artery Disease / surgery; Investigative Techniques; Unified Health System.
IntroductionIn the last decade, major clinical studies have reassessed
the issue of stable coronary artery disease (CAD) investigation and its treatment1,2. Currently, the assessment of patients with suspected or established stable obstructive CAD depends on the risk stratification for proper decision-making on the need for cardiac catheterization (CC) and clinical benefits of revascularization3-7.
Interventional cardiac procedures have high cost and technological adjustments are necessary to operate these services at high levels of resolution and efficiency. Thus, non-invasive stress tests are recommended as screening tests in patients at risk for CAD, being important to select higher-risk patients who
may benefit from invasive, higher-cost treatments. These tests also provide relevant prognostic information8 with treatment implications, by defining the need for revascularization in patients with significant ischemia9.
To evaluate the sequence of diagnostic investigation and currently used treatment in patients with suspected or established CAD in two major metropolitan areas, São Paulo and Curitiba, as well as a referral cardiology institution, is an important step towards understanding how the resources of the Brazilian Unified Health System (SUS) are being used and identify whether there are opportunities for improvement.
MethodsThis was a retrospective, descriptive, observational study
of the diagnostic and therapeutic routes of patients with suspected or known CAD, treated by SUS in the cities of Curitiba and Sao Paulo, between the groups submitted or not to noninvasive tests prior to invasive cardiac catheterization. The respective economic impact of the strategies observed from the perspective of SUS was also evaluated. Similarly, patients treated at Instituto do Coração
192

Original Article
Cerci et al.IMPACT Study
Arq Bras Cardiol. 2014; 103(3):192-200
of Hospital das Clínicas da Faculdade de Medicina of Universidade de São Paulo (Incor-FMUSP), were evaluated, due to having the largest population of patients with CAD and Latin America, as well as a structured database that allows this type of survey, including the report of procedures in a computerized system.
A survey was carried out in DATASUS regarding the number of procedures performed by SUS during the investigation of CAD in Curitiba and São Paulo, data that were corrected and cross-analyzed with a review of the High Complexity Outpatient Procedure Authorization (HCOPA) forms.
Outpatient treatment reports (OTRs), High Complexity Outpatient Procedures Authorization forms (HCOPAs) and hospital admission authorization forms (HAAs) in the period 2008-2010, of patients undergoing stress test, scintigraphy, stress echocardiography, angioplasty and coronary artery bypass grafting by SUS in the cities of Curitiba and São Paulo were assessed. Starting with the name of the patients, it was possible to determine which and how many procedures each patient was longitudinally submitted to during the study period. According to directions from the Municipal Health Secretariat of Curitiba, this survey was accompanied by auditors from the secretariat itself, and cross-checked with the costs of examinations.
The same survey was carried out in InCor-FMUSP, in patients treated by SUS, only. When evaluating HCOPA, HAA and OTR forms, we analyzed the National Registry of Health Care Institutions (CNES) to verify whether there was no overlapping with data from InCor-USP and other centers in the city of São Paulo. Empirical data observed in the realities of the health departments of Curitiba and São Paulo, as well as the InCor-USP were compared. Considering the currently prevailing conditions at InCor-USP in each year of the study, we analyzed the assessment and monitoring of approximately four thousand patients undergoing cardiac catheterization.
The distribution of absolute and relative frequencies of the study procedures allows estimating the probabilities of use of these diagnostic and therapeutic resources, according to the observed diagnostic and comorbidity strata, age and gender of the patients. The final outcome (death) in each identified investigation stratum has been reported in the Mortality Information System (MIS) up to the date of 12/31/2012, and the annual mortality rate was calculated.
Administrative data were received from municipal health secretariats and data mining techniques were used, which, regardless of the activity met, are divided into seven steps10,11: cleaning, integration, selection, data processing and mining, evaluation of standards and representation of knowledge.
In parallel with these development activities, we also evaluated data from electronic medical records of patients from InCor-FMUSP. It is a known fact that InCor receives patients from many other cities and states and this study included all patients treated by SUS, regardless of city of origin. In both databases, the evaluation of diagnostic and therapeutic standards was performed based on the quantities and qualities of assistance resources used to in both groups of patients: those undergoing prior noninvasive tests and those referred directly to invasive cardiac catheterization.
The model of the decision tree was used to allow the observation and quantification of examinations and health resources required by each group of patients. The procedure costs were calculated in each group of patients according to Datasus surveys and the empirical reality observed in InCor-FMUSP.
Statistical analyses were performed using Microsoft Excel 2007 (Microsoft, USA) and STATA version 11.0 (Stata Corp, College Station, United States), with a level of significance < 0.05. The descriptive analysis was performed by calculating the percentage of patients who underwent stress test, scintigraphy or CC as the initial diagnostic test. The frequency of the following tests, the overall incidence of revascularization and incidence of revascularization after CC in each strategy group was also calculated. The chi-square test was used to test differences between groups.
Results
SUS in the metropolitan region of CuritibaIt is estimated that the metropolitan region of Curitiba has
3,168,980 inhabitants. Among the 66,987 procedures for cardiac evaluation and treatment of CAD in the period of January 2008 to December 2010, the exercise test was the most frequent examination, followed by the percutaneous and surgical revascularization procedures. These same procedures accounted for 1.5% and 87.2% of total direct costs involved in the diagnosis and invasive treatment of patients with CAD in the metropolitan region of Curitiba.
It is noteworthy that, while there were 10,809 percutaneous and surgical revascularization procedures, only 6,517 catheterizations were performed in the same period.
After excluding transthoracic and transesophageal echocardiography procedures, which can be used in other indications in addition to CAD, the number of procedures has a final direct cost of nearly 60 million reais, taking into account the estimated population of about 3.1 million inhabitants, with an average cost per capita of R$ 18.90 (Table 1). Figure 1 shows the number of procedures and their respective costs.
Among the HAAs and HCOPA, which data were provided by the Municipal Health Secretariat, of 6,076 catheterization procedures, only 14.5% of cases were assessed with functional imaging exams prior to catheterization. It was not possible to assess how many of these patients underwent a stress test, as there was no record of the name of the patients submitted to the examination in the reports of the health departments (municipal or state and even the Ministry of Health registry, which included only the identification number of the health care provider and the total value spent on stress test during the period).
Regarding the HAAs of 6,489 revascularization procedures analyzed, only 13.5% had been previously assessed with functional imaging exams.
In the group of patients subsequently submitted to percutaneous revascularization, the annual mortality rate was 4.8%, whereas for patients undergoing CABG it was 5.6%. In patients undergoing catheterization, but not
193
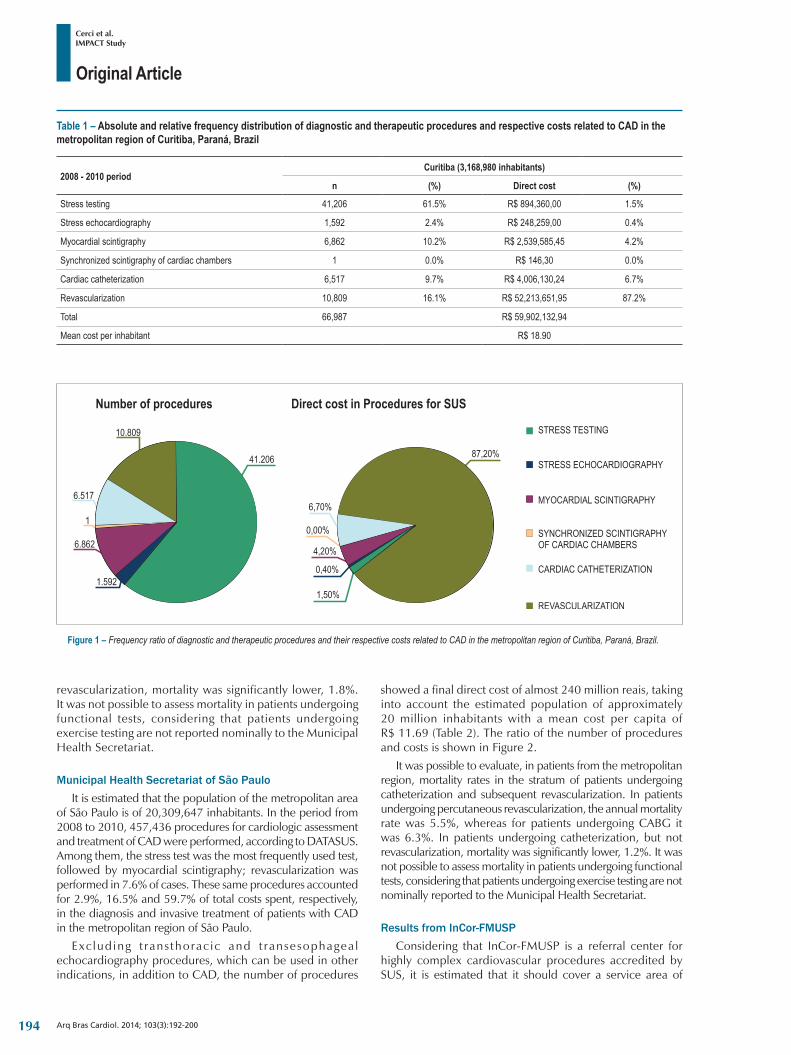
Original Article
Cerci et al.IMPACT Study
Arq Bras Cardiol. 2014; 103(3):192-200
Figure 1 – Frequency ratio of diagnostic and therapeutic procedures and their respective costs related to CAD in the metropolitan region of Curitiba, Paraná, Brazil.
Table 1 – Absolute and relative frequency distribution of diagnostic and therapeutic procedures and respective costs related to CAD in the metropolitan region of Curitiba, Paraná, Brazil
2008 - 2010 periodCuritiba (3,168,980 inhabitants)
n (%) Direct cost (%)
Stress testing 41,206 61.5% R$ 894,360,00 1.5%
Stress echocardiography 1,592 2.4% R$ 248,259,00 0.4%
Myocardial scintigraphy 6,862 10.2% R$ 2,539,585,45 4.2%
Synchronized scintigraphy of cardiac chambers 1 0.0% R$ 146,30 0.0%
Cardiac catheterization 6,517 9.7% R$ 4,006,130,24 6.7%
Revascularization 10,809 16.1% R$ 52,213,651,95 87.2%
Total 66,987 R$ 59,902,132,94
Mean cost per inhabitant R$ 18.90
revascularization, mortality was significantly lower, 1.8%. It was not possible to assess mortality in patients undergoing functional tests, considering that patients undergoing exercise testing are not reported nominally to the Municipal Health Secretariat.
Municipal Health Secretariat of São PauloIt is estimated that the population of the metropolitan area
of São Paulo is of 20,309,647 inhabitants. In the period from 2008 to 2010, 457,436 procedures for cardiologic assessment and treatment of CAD were performed, according to DATASUS. Among them, the stress test was the most frequently used test, followed by myocardial scintigraphy; revascularization was performed in 7.6% of cases. These same procedures accounted for 2.9%, 16.5% and 59.7% of total costs spent, respectively, in the diagnosis and invasive treatment of patients with CAD in the metropolitan region of São Paulo.
Exc lud ing t rans thorac ic and t ransesophagea l echocardiography procedures, which can be used in other indications, in addition to CAD, the number of procedures
showed a final direct cost of almost 240 million reais, taking into account the estimated population of approximately 20 million inhabitants with a mean cost per capita of R$ 11.69 (Table 2). The ratio of the number of procedures and costs is shown in Figure 2.
It was possible to evaluate, in patients from the metropolitan region, mortality rates in the stratum of patients undergoing catheterization and subsequent revascularization. In patients undergoing percutaneous revascularization, the annual mortality rate was 5.5%, whereas for patients undergoing CABG it was 6.3%. In patients undergoing catheterization, but not revascularization, mortality was significantly lower, 1.2%. It was not possible to assess mortality in patients undergoing functional tests, considering that patients undergoing exercise testing are not nominally reported to the Municipal Health Secretariat.
Results from InCor-FMUSPConsidering that InCor-FMUSP is a referral center for
highly complex cardiovascular procedures accredited by SUS, it is estimated that it should cover a service area of
194
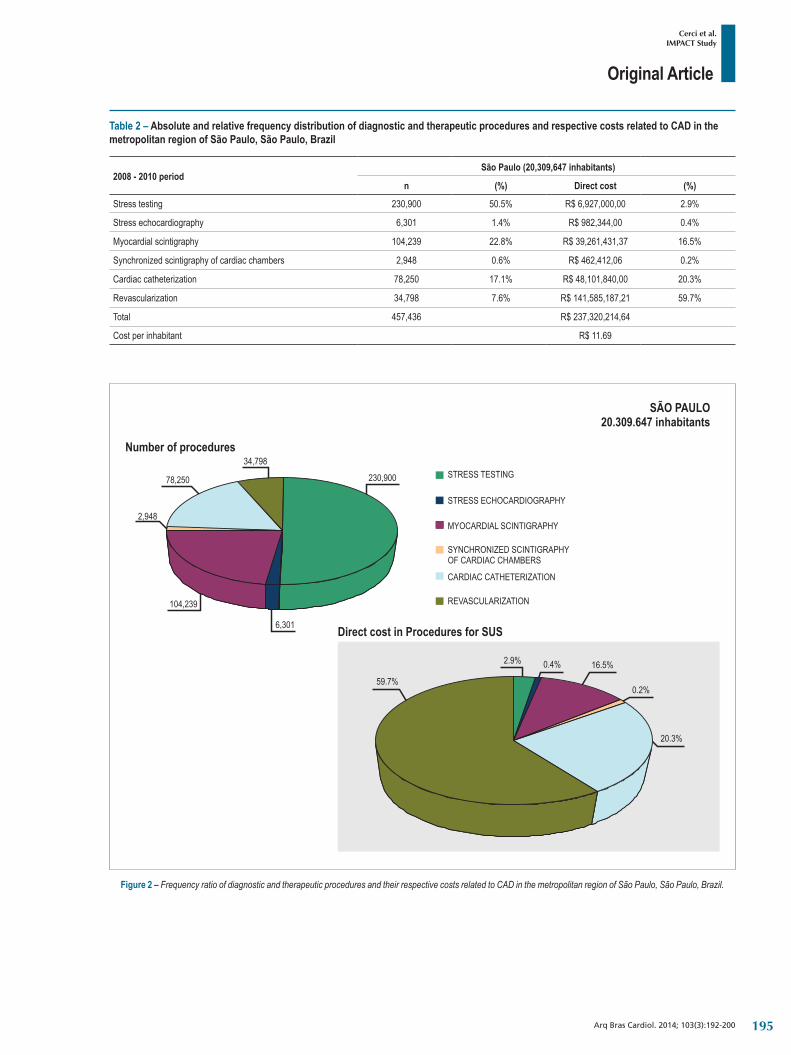
Original Article
Cerci et al.IMPACT Study
Arq Bras Cardiol. 2014; 103(3):192-200
Table 2 – Absolute and relative frequency distribution of diagnostic and therapeutic procedures and respective costs related to CAD in the metropolitan region of São Paulo, São Paulo, Brazil
2008 - 2010 periodSão Paulo (20,309,647 inhabitants)
n (%) Direct cost (%)
Stress testing 230,900 50.5% R$ 6,927,000,00 2.9%
Stress echocardiography 6,301 1.4% R$ 982,344,00 0.4%
Myocardial scintigraphy 104,239 22.8% R$ 39,261,431,37 16.5%
Synchronized scintigraphy of cardiac chambers 2,948 0.6% R$ 462,412,06 0.2%
Cardiac catheterization 78,250 17.1% R$ 48,101,840,00 20.3%
Revascularization 34,798 7.6% R$ 141,585,187,21 59.7%
Total 457,436 R$ 237,320,214,64
Cost per inhabitant R$ 11.69
Figure 2 – Frequency ratio of diagnostic and therapeutic procedures and their respective costs related to CAD in the metropolitan region of São Paulo, São Paulo, Brazil.
195
Original Article
Cerci et al.IMPACT Study
Arq Bras Cardiol. 2014; 103(3):192-200
approximately five million inhabitants. In the period 2008-2010, 78,792 patients were evaluated in the institution with suspected or established CAD. Of these, 18,994 were excluded because they were admitted to an emergency unit, transferred from another institution or due to a diagnosis of acute myocardial infarction or high-risk unstable angina. The final cohort consisted of 59,798 patients with suspected or stable CAD.
Of the 59,798 patients, 34,626 (57.9%) were first evaluated by stress test (Group 1), 16,221 (27.1%) were initially submitted to scintigraphy (Group 2), whereas 8,951 (14.9%) were initially submitted to CC (Group 3).
Patients initially assessed by stress test (ST)Of the total cohort, 34,626 (57.9%) patients were initially
evaluated by ST. The annual mortality rate in this group was 0.5%. These patients were divided into three subgroups:
1. CC: in 797 patients (2.3%) CC was performed after ST. Of these, 410/797 (51.4%) did not undergo CABG. While 387/797 patients (48.6%) underwent CABG, 256 underwent elective PCI, 98 patients underwent CABG and 33 underwent PCI and CABG.
2. Scintigraphy: It was the next test in 1,865 patients (5.4%). Of these, 1.748/1.865 (93.7%) did not undergo CC. Of 117/1.865 (6.3%) patients submitted to CC, 69/117 (59.0%) underwent CABG, 46 patients underwent PCI, 20 underwent CABG and three CABG and PCI.
3. The remaining 31,964 patients (92.3%) were followed clinically without subsequent CC or scintigraphy.
The incidence of overall coronary artery bypass grafting was 1.3% (456/34.626), whereas the incidence of revascularization after CC was 49.9% (456/914) in this diagnostic strategy group.
Patients initially evaluated by myocardial perfusion scintigraphy
Of the 16,221 patients initially evaluated by myocardial perfusion scintigraphy, 1,959 (12.1%) were subsequently submitted to CC with an overall revascularization incidence of 6.0% (971/16.221). The annual mortality rate in this group was 2.7%.
The incidence of myocardial revascularization after CC was 49.6% (971/1.959) in myocardial perfusion scintigraphy group, with 760 patients undergoing PCI, 179 CABG and 32 CABG and PCI.
Patients initially evaluated by cardiac catheterizationCardiac catheterization was the initial diagnostic test in
8,951 patients, with a revascularization incidence of 28.9% (2.583/8.951) in this group, of which 1,624 (62.9%) patients underwent PCI, 857 (33.2%) underwent CABG and 102 (3.9%) both. The annual mortality rate in this group was 3.8%.
Proportion of CC, prior noninvasive testing and subsequent revascularization rates
Of the 12,132 patients undergoing catheterization, in 8951 (73.8%), no prior functional test was performed to
document ischemia; 914/12.132 in patients (7.5%), ST was the first examination performed, and in 1.959/12.132 patients (16.1%), myocardial perfusion scintigraphy was performed initially. Thus, only 2.873/12.132 (23.7%) of the patients submitted to elective CC underwent a stress test in the 180 days before the procedure.
The incidence of CC that did not result in revascularization was not significantly different between the groups initially submitted the ST and myocardial perfusion scintigraphy (50.1% versus 50.4%, respectively, p = 0.74), but this incidence was significantly higher in the group initially assessed by CC (71.1%, p < 0.001) - Figure 3. Finally, a third of the 4,010 patients who underwent revascularization – 1.427/4.010 (35.6%) – underwent a noninvasive stress test before the procedure.
Direct costs related to the investigation procedures and invasive treatment in patients with known or suspected CAD in InCor-FMUSP are shown in Table 3 and Figure 4.
DiscussionCoronary angioplasty and coronary artery bypass grafting
are treatment options for patients with stable CAD, with established benefits in high-risk populations. Guidelines for elective coronary intervention published jointly by the American College of Cardiology, American Heart Association and the Society of Cardiovascular Angiography and Intervention indicate that for patients with stable angina, the revascularization intervention is indicated when stenosis is “associated with moderate or high-degree ischemia at noninvasive testing”12. Previous studies have shown that patients undergoing elective angioplasty in accordance with these guidelines have better therapeutic outcomes13.
In fact, in patients from InCor-FMUSP with suspected or diagnosed CAD, those with the highest mortality rates are the ones submitted to tests of higher complexity: patients initially evaluated by ST have an annual mortality of 0.5%, whereas patients initially evaluated by scintigraphy, the mortality rate was 2.7% and in patients initially evaluated by cardiac catheterization, 3.8%. This is important because interventional cardiology laboratories have high operational costs and must be operated at the highest levels of efficiency and resolution.
Thus, when there is high probability of revascularization need, it is cost-effective to directly initiate the diagnostic evaluation with cardiac catheterization and, if possible, percutaneous revascularization intervention in the same procedure. However, in lower risk patients, the noninvasive evaluation test prior to CC is associated with lower overall cost of diagnosis, shorter hospital stays and lower rates of revascularization, without increase in adverse events, such as cardiac death or myocardial infarction14,15.
To assess whether invasive tests, such as CC, are being performed in appropriately selected patients is critical to providing high quality medical care. In this sense, our results suggest that current diagnostic strategies can be substantially improved in SUS, as even in InCor-FMUSP, a high-level educational institution, only 23.7% of patients with confirmed or suspected stable CAD submitted to
196
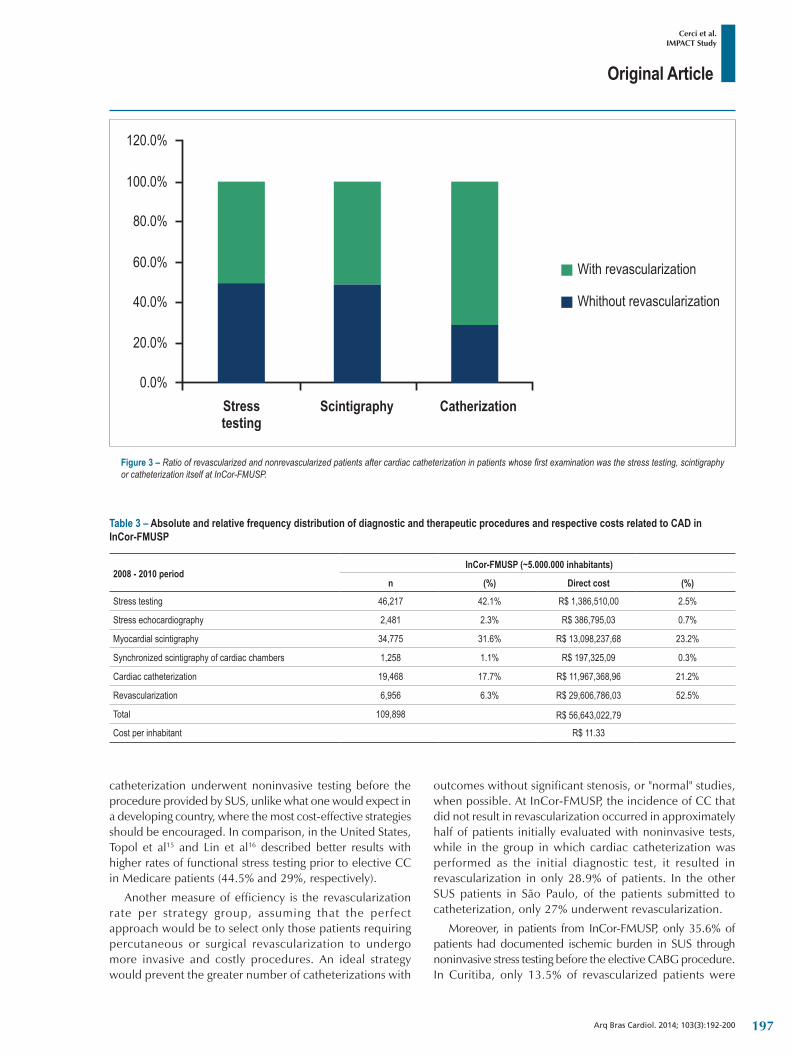
Original Article
Cerci et al.IMPACT Study
Arq Bras Cardiol. 2014; 103(3):192-200
Figure 3 – Ratio of revascularized and nonrevascularized patients after cardiac catheterization in patients whose first examination was the stress testing, scintigraphy or catheterization itself at InCor-FMUSP.
catheterization underwent noninvasive testing before the procedure provided by SUS, unlike what one would expect in a developing country, where the most cost-effective strategies should be encouraged. In comparison, in the United States, Topol et al15 and Lin et al16 described better results with higher rates of functional stress testing prior to elective CC in Medicare patients (44.5% and 29%, respectively).
Another measure of efficiency is the revascularization rate per strategy group, assuming that the perfect approach would be to select only those patients requiring percutaneous or surgical revascularization to undergo more invasive and costly procedures. An ideal strategy would prevent the greater number of catheterizations with
outcomes without significant stenosis, or "normal" studies, when possible. At InCor-FMUSP, the incidence of CC that did not result in revascularization occurred in approximately half of patients initially evaluated with noninvasive tests, while in the group in which cardiac catheterization was performed as the initial diagnostic test, it resulted in revascularization in only 28.9% of patients. In the other SUS patients in São Paulo, of the patients submitted to catheterization, only 27% underwent revascularization.
Moreover, in patients from InCor-FMUSP, only 35.6% of patients had documented ischemic burden in SUS through noninvasive stress testing before the elective CABG procedure. In Curitiba, only 13.5% of revascularized patients were
Table 3 – Absolute and relative frequency distribution of diagnostic and therapeutic procedures and respective costs related to CAD in InCor-FMUSP
2008 - 2010 periodInCor-FMUSP (~5.000.000 inhabitants)
n (%) Direct cost (%)
Stress testing 46,217 42.1% R$ 1,386,510,00 2.5%
Stress echocardiography 2,481 2.3% R$ 386,795,03 0.7%
Myocardial scintigraphy 34,775 31.6% R$ 13,098,237,68 23.2%
Synchronized scintigraphy of cardiac chambers 1,258 1.1% R$ 197,325,09 0.3%
Cardiac catheterization 19,468 17.7% R$ 11,967,368,96 21.2%
Revascularization 6,956 6.3% R$ 29,606,786,03 52.5%
Total 109,898 R$ 56,643,022,79
Cost per inhabitant R$ 11.33
197
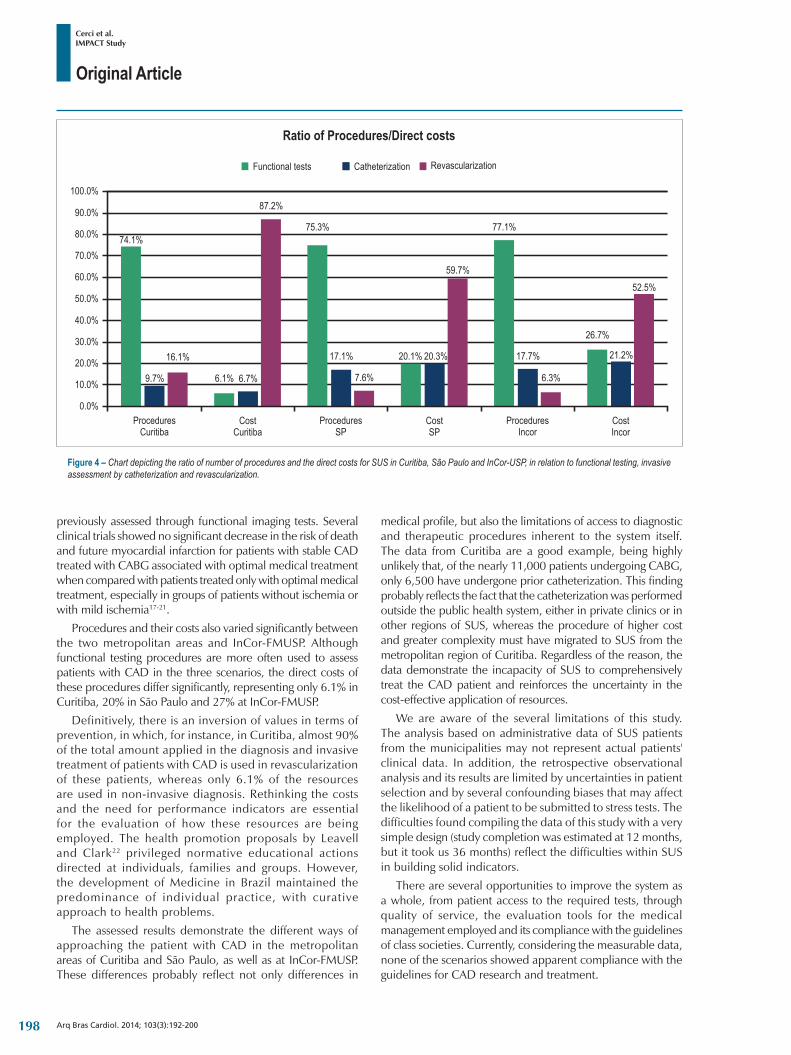
Original Article
Cerci et al.IMPACT Study
Arq Bras Cardiol. 2014; 103(3):192-200
Figure 4 – Chart depicting the ratio of number of procedures and the direct costs for SUS in Curitiba, São Paulo and InCor-USP, in relation to functional testing, invasive assessment by catheterization and revascularization.
previously assessed through functional imaging tests. Several clinical trials showed no significant decrease in the risk of death and future myocardial infarction for patients with stable CAD treated with CABG associated with optimal medical treatment when compared with patients treated only with optimal medical treatment, especially in groups of patients without ischemia or with mild ischemia17-21.
Procedures and their costs also varied significantly between the two metropolitan areas and InCor-FMUSP. Although functional testing procedures are more often used to assess patients with CAD in the three scenarios, the direct costs of these procedures differ significantly, representing only 6.1% in Curitiba, 20% in São Paulo and 27% at InCor-FMUSP.
Definitively, there is an inversion of values in terms of prevention, in which, for instance, in Curitiba, almost 90% of the total amount applied in the diagnosis and invasive treatment of patients with CAD is used in revascularization of these patients, whereas only 6.1% of the resources are used in non-invasive diagnosis. Rethinking the costs and the need for performance indicators are essential for the evaluation of how these resources are being employed. The health promotion proposals by Leavell and Clark22 privileged normative educational actions directed at individuals, families and groups. However, the development of Medicine in Brazil maintained the predominance of individual practice, with curative approach to health problems.
The assessed results demonstrate the different ways of approaching the patient with CAD in the metropolitan areas of Curitiba and São Paulo, as well as at InCor-FMUSP. These differences probably reflect not only differences in
medical profile, but also the limitations of access to diagnostic and therapeutic procedures inherent to the system itself. The data from Curitiba are a good example, being highly unlikely that, of the nearly 11,000 patients undergoing CABG, only 6,500 have undergone prior catheterization. This finding probably reflects the fact that the catheterization was performed outside the public health system, either in private clinics or in other regions of SUS, whereas the procedure of higher cost and greater complexity must have migrated to SUS from the metropolitan region of Curitiba. Regardless of the reason, the data demonstrate the incapacity of SUS to comprehensively treat the CAD patient and reinforces the uncertainty in the cost-effective application of resources.
We are aware of the several limitations of this study. The analysis based on administrative data of SUS patients from the municipalities may not represent actual patients' clinical data. In addition, the retrospective observational analysis and its results are limited by uncertainties in patient selection and by several confounding biases that may affect the likelihood of a patient to be submitted to stress tests. The difficulties found compiling the data of this study with a very simple design (study completion was estimated at 12 months, but it took us 36 months) reflect the difficulties within SUS in building solid indicators.
There are several opportunities to improve the system as a whole, from patient access to the required tests, through quality of service, the evaluation tools for the medical management employed and its compliance with the guidelines of class societies. Currently, considering the measurable data, none of the scenarios showed apparent compliance with the guidelines for CAD research and treatment.
198

Original Article
Cerci et al.IMPACT Study
Arq Bras Cardiol. 2014; 103(3):192-200
A simple measure such as the use of patient identification on all examinations performed and not only those of higher cost/complexity, would be more accurate indicators of health. Without precise indicators about which patients are submitted to which procedures, whether these procedures are well indicated and the mortality related to different strata of patients, it is not possible to assess whether the nearly 354 million reais were used in the most cost-effective way.
However, the start of the current situation analysis, supported by the acknowledged cross-validation strategies, such as the described sensitivity analyses, is an essential and viable first step. In the absence of more reliable databases, we believe that starting this analytical process was more important than not starting it due to the several current limitations.
ConclusionThere are clear differences in the management of patients
with suspected or known DAC in the metropolitan regions of Curitiba and São Paulo, and InCor-FMUSP. Although noninvasive functional tests are the tests most frequently used in the evaluation of patients with CAD in the three evaluated scenarios, the percentage of resources employed to perform the functional tests is much lower in Curitiba than in the other scenarios. Most of the costs are related to invasive procedures / treatments. Significant differences were observed in InCor-FMUSP regarding rates of revascularization when comparing the initial investigation strategies by invasive and noninvasive methods. When starting with non-invasive techniques (stress test and myocardial
perfusion) one attains lower rates of catheterization that do not lead to revascularization in this population.
Author contributionsConception and design of the research: Cerci JJ, Trindade
E, Cerci RJ, Preto D, Cesar LAM, Preto L, Stinghen L, Martinez C, Meneghetti JC; Acquisition of data: Cerci JJ, Trindade E, Cerci RJ, Preto D, Lemos PA, Cesar LAM, Preto L, Stinghen L, Martinez C, Meneghetti JC; Analysis and interpretation of the data: Cerci JJ, Trindade E, Cerci RJ, Meneghetti JC; Statistical analysis: Cerci JJ, Trindade E, Cerci RJ; Writing of the manuscript: Cerci JJ, Trindade E, Cerci RJ, Preto D, Lemos PA, Cesar LAM, Preto L, Stinghen L, Martinez C, Meneghetti JC; Critical revision of the manuscript for intellectual content: Cerci JJ, Trindade E, Cerci RJ, Preto D, Lemos PA, Cesar LAM, Preto L, Stinghen L, Martinez C, Meneghetti JC.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis article is part of the thesis of Post-doctoral submitted
by Juliano Julio Cerci, from USP.
1. Dagenais GR, Lu J, Faxon DP, Kent K, Lago RM, Lezama C, et al; Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) Study Group. Effects of optimal medical treatment with or without coronary revascularization on angina and subsequent revascularizations in patients with type 2 diabetes mellitus and stable ischemic heart disease. Circulation. 2011;123(14):1492-500.
2. Maron DJ, Boden WE, Spertus JA, Hartigan PM, Mancini GB, Sedlis SP, et al; COURAGE Trial Research Group. Impact of metabolic syndrome and diabetes on prognosis and outcomes with early percutaneous coronary intervention in the COURAGE (Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation) trial. J Am Coll Cardiol. 2011; 58(2):131-7.
3. Messerli FH, Mancia G, Conti CR, Pepine CJ. Guidelines on the management of stable angina pectoris: executive summary: the task force on the management of stable angina pectoris of the European society of cardiology. Eur Heart J. 2006;27(23):2902-3.
4. Cheitlin MD, Armstrong WF, Aurigemma GP, Beller GA, Bierman FZ, Davis JL, et al. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASE Committee to Update the 1997 Guidelines for the Clinical Application of Echocardiography). J Am Soc Echocardiogr. 2003;16(10):1091-110.
5. Fraker Jr TD, Fihn SD, Gibbons RJ, Abrams J, Chatterjee K, Daley J, et al. 2007 chronic angina focused update of the ACC/AHA 2002 guidelines
for the management of patients with chronic stable angina: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Writing Group to develop the focused update of the 2002 guidelines for the management of patients with chronics able angina. J Am Coll Cardiol. 2007;50(23):2264-74. Erratum in J Am Coll Cardiol. 2007;50(23):e1.
6. Klocke FJ, Baird MG, Lorell BH, Baterman TM, Messer JV, Berman DS, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging – executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASNC Committee to Revise the 1995 Guidelines for the Clinical Use of Cardiac Radionuclide Imaging). J Am Coll Cardiol. 2003;42(7):1318-33.
7. Hendel RC, Berman DS, Di Carli MF, Heidenreich PA, Henkin RE, Pell ikka PA, et al; American College of Cardiology Foundation Appropr i a te Use Cr i t e r i a Ta sk Fo rce , Amer i can Soc ie t y o f Nuclear Cardiology, American College of Radiology, American Heart Association, American Society of Echocardiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, Society of Nuclear Medicine. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 appropriate use criteria for cardiac radionuclide imaging: a report of the American College of Cardiology Foundation appropriate use criteria task force, the American Society of Nuclear Cardiology, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the Society of Cardiovascular Computed Tomography, the Society for Cardiovascular Magnetic Resonance, and the Society of Nuclear Medicine. J Am Coll Cardiol. 2009;53(23):2201-29.
References
199
Original Article
Cerci et al.IMPACT Study
Arq Bras Cardiol. 2014; 103(3):192-200
8. Cerci MS, Cerci JJ, Cerci RJ, Pereira Neto CC, Trindade E, Delbeke D, et al. Myocardial perfusion imaging is a strong predictor of death in women. JACC Cardiovasc Imaging. 2011;4(8):880-8.
9. Shaw LJ, Berman DS, Maron DJ, Mancini GB, Hayes SW, Hartigan PM, et al. COURAGE Investigators. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation. 2008;117(10):1283-91.
10. Soibelman L. Data preparation process for construction knowledge generation through knowledge discovery from databases. J Comput Civil Engineer. 2002;16:39-48.
11. Fayyad U, Piatetsky-Shapirio G, Smyth P. The KDD process for extracting useful knowledge from volumes data. Association for Computing Machinery. Communications ACM. 1996;39(11):27-34.
12. Smith SC Jr, Feldman TE, Hirshfeld JW Jr, Jacobs AK, Jern MJ, King SB, et al. ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAIWriting Committee to Update 2001 Guidelines for Percutaneous Coronary Intervention). Circulation. 2006;113(7):e166-e286.
13. Anderson HV, Shaw RE, Brindis RG, Klein LW, Mc Kay CR, Kutcher MA, et al. Relationship between procedure indications and outcomes of percutaneous coronary interventions by American College of Cardiology/American Heart Association Task Force Guidelines. Circulation. 2005;112(18):2786-91.
14. Shaw LJ, Hachamovitch R, Berman DS, Marwick TH, Lauer MS, Heller GV, et al; Economics of Noninvasive Diagnosis (END) Multicenter Study Group. The economic consequences of available diagnostic and prognostic strategies for the evaluation of stable angina patients: an observational assessment of the value of precatheterization ischemia. J Am Coll Cardiol. 1999;33(3):661-9.
15. Topol EJ, Ellis SG, Cosgrove DM, Bates ER, Muller DW, Schork NJ, et al. Analysis of coronary angioplasty practice in the United States with an insurance-claims data base. Circulation. 1993;87(5):1489-97.
16. Lin GA, Dudley RA, Lucas FL, Malenka DJ, Vittinghoff E, Redberg RF. Frequency of stress testing to document ischemia prior to elective percutaneous coronary intervention. JAMA. 2008;300(15):1765-73.
17. Folland ED, Hartigan PM, Parisi AF; Veterans Affairs ACME Investigators. Percutaneous transluminal coronary angioplasty versus medical therapy for stable angina pectoris: outcomes for patients with double-vessel versus single-vessel coronary artery disease in a Veterans Affairs Cooperative randomized trial. J Am Coll Cardiol. 1997;29(7):1505-11.
18. Pitt B, Waters D, Brown WV, van Boven AJ, Schwartz L, Title LM, et al; Atorvastatin versus Revascularization Treatment Investigators. Aggressive lipid-lowering therapy compared with angioplasty in stable coronary artery disease. N Engl JMed. 1999;341(2):70-6.
19. Henderson RA, Pocock SJ, Clayton TC, Knight R, Fox KA, Julian DG, et al. Seven year outcome in the RITA-2 trial: coronary angioplasty versus medical therapy. J Am Coll Cardiol. 2003;42(7):1161-70.
20. Hueb W, Lopes NH, Gersh BJ, Soares P, Machado LA, Jatene FB, et al. Five-year follow-up of the Medicine, Angioplasty, or Surgery Study (MASS II): a randomized controlled clinical trial of 3 therapeutic strategies for multivessel coronary artery disease. Circulation. 2007;115(9):1082-9.
21. Hueb W, Soares PR, Gersh BJ, Cesar LA, Luz PL, Puig LB, et al. The medicine, angioplasty, or surgery study (MASS-II): a randomized, controlled clinical trial of three therapeutic strategies for multivessel coronary artery disease: one-year results. J Am Coll Cardiol. 2004;43(10):1743-51.
22. Leavell & Clark. Principles of epidemiology. 2nd ed. Atlanta: U.S Dept. of H&H Serv; 1992.
200

Original Article
Effects of Exercise Training on Heart Rate Variability in Chagas Heart DiseaseBruno Ramos Nascimento1,2,3, Márcia Maria Oliveira Lima3,4, Maria do Carmo Pereira Nunes1,2,3, Maria Clara Noman de Alencar2, Henrique Silveira Costa3, Marcelo Martins Pinto Filho1,2, Vitor Emanuel Serafim Cota1, Manoel Otávio da Costa Rocha1,3, Antonio Luiz Pinho Ribeiro1,2,3
Faculdade de Medicina da Universidade Federal de Minas Gerais1; Serviço de Cardiologia e Cirurgia Cardiovascular do Hospital das Clínicas da UFMG2; Pos-graduação em Infectologia e Medicina Tropical - Faculdade de Medicina da UFMG3, Belo Horizonte, MG; Escola de Fisioterapia da Universidade Federal dos Vales do Jequitinhonha e Mucuri4, Diamantina, MG - Brazil
Mailing Address: Bruno Ramos Nascimento •Rua Tenente Garro, 137, apt. 1202, Santa Efigenia. Postal Code 30240-360, Belo Horizonte, MG - BrazilE-mail: [email protected]; [email protected] received December 27, 2013; revised manuscript May 12, 2014; accepted may 13, 2014.
DOI: 10.5935/abc.20140108
Abstract
Background: Heart rate variability (HRV) is a marker of autonomic dysfunction severity. The effects of physical training on HRV indexes in Chagas heart disease (CHD) are not well established.
Objective: To evaluate the changes in HRV indexes in response to physical training in CHD.
Methods: Patients with CHD and left ventricular (LV) dysfunction, physically inactive, were randomized either to the intervention (IG, N = 18) or control group (CG, N = 19). The IG participated in a 12-week exercise program consisting of 3 sessions/week.
Results: Mean age was 49.5 ± 8 years, 59% males, mean LVEF was 36.3 ± 7.8%. Baseline HRV indexes were similar between groups. From baseline to follow-up, total power (TP): 1653 (IQ 625 – 3418) to 2794 (1617 – 4452) ms, p = 0.02) and very low frequency power: 586 (290 – 1565) to 815 (610 – 1425) ms, p = 0.047) increased in the IG, but not in the CG. The delta (post – pre) HRV indexes were similar: SDNN 11.5 ± 30.0 vs. 3.7 ± 25.1 ms. p = 0.10; rMSSD 2 (6 – 17) vs. 1 (21 – 9) ms. p = 0.43; TP 943 (731 – 3130) vs. 1780 (921 – 2743) Hz. p = 0.46; low frequency power (LFP) 1.0 (150 – 197) vs. 60 (111 – 146) Hz. p = 0.85; except for high frequency power, which tended to increase in the IG: 42 (133 – 92) vs. 79 (61 – 328) Hz. p = 0.08).
Conclusion: In the studied population, the variation of HRV indexes was similar between the active and inactive groups. Clinical improvement with physical activity seems to be independent from autonomic dysfunction markers in CHD. (Arq Bras Cardiol. 2014; 103(3):201-208)
Keywords: Chagas Cardiomyopathy; Exercise; Heart Rate.
IntroductionChagas disease is an infection caused by the Trypanosoma
cruzi, transmitted primarily by insects of the Triatominae family. It is estimated than 8-10 million people are infected worldwide, especially in Latin America, where the disease is still endemic1,2. Chagas cardiomyopathy (CHD) affects 20-40% of patients with the chronic form, and its pathogenesis is closely linked to neurogenic mechanisms, microvascular dysfunction, autoimmune processes and direct injury by the parasite2-4.
Cardiac autonomic dysfunction is known to be a characteristic and early finding of Chagas disease5-9, possibly related to deposits of autoantibodies10, causing desensitization of cardiac neurotransmitter receptors, early affecting cardiac vagal control11. The heart rate variability (HRV) is an indirect measure of the interactions between the sympathetic and parasympathetic systems, mediated by several physiological mechanisms such as reflex arcs, release of cytokine and vasoactive substances, among others. The values of HRV measurements in the time and frequency domains are known diagnostic, prognostic markers and predictors of complications, including mortality, in several systemic diseases, such as heart failure and sepsis12-14.
Among the non-pharmacological measures in the treatment of cardiovascular diseases, regular physical activity as a factor of vagal tone increase has shown a major impact on HRV indices and association with training intensity15,16. Significant HRV impairment has been demonstrated in CHD17, but studies suggest that, unlike other forms of heart failure, there seems to be a change in the association between physical exercise and HRV18, with no significant improvement of their indices being observed after supervised training programs5.
201

Original Article
Nascimento et al.Heart rate variability in Chagas disease
Arq Bras Cardiol. 2014; 103(3):201-208
The objective of this study is to evaluate the changes of HRV indexes in the time and frequency domains in patients with Chagas heart disease and left ventricular dysfunction undergoing supervised exercise training for 12 weeks, compared with the inactive group of patients with the same clinical characteristics.
Methods
Study population and inclusion criteriaA complete description of the study design has been
published previously19. Briefly, 145 subjects were recruited from the Cardiology and Chagas Disease Outpatient Clinics of Hospital das Clinicas, Universidade Federal de Minas Gerais. The volunteers were interviewed to obtain clinical history and current life habits. To be eligible for the study, patients had to have a previous diagnosis of CHD, based on at least two positive serologic tests for Trypanosoma cruzi antibodies, along with the presence of left ventricular dysfunction and capacity to attend the training program fully4. Patients with comorbidities, patients with pacemaker or resynchronization device and those that self-reported to be physically active were excluded. Forty patients met the inclusion criteria.
All patients had been clinically stable for at least three months, had sinus rhythm and were receiving standard medical therapy20. After randomization, carried out through an electronic system, patients were allocated to the intervention group (IG) or control group (CG). Informed consent was obtained from all patients, and the study was approved by the Research Ethics Committee of Universidade Federal de Minas Gerais, in accordance with the Declaration of Helsinki.
Study design and proceduresAt the moment of inclusion, all patients underwent clinical
examination, laboratory tests, 12-lead ECG, symptom-limited exercise stress test to establish training heart rate (HR) intensity, 6-minute walk test (6MWT), echocardiography and 24-h Holter monitoring to assess HRV indices. Functional capacity was assessed by Goldman and New York Heart Association (NYHA) criteria. Severity of cardiac impairment was determined by echocardiographic indices (ejection fraction, EF, and left ventricular end diastolic volume, LVEDV). All tests were performed in a two-week period before and after aerobic training. Examiners were blinded to the results of the other tests.
A symptom-limited exercise stress was performed on a treadmill (Digistress Pulsar Micromed, Brasilia, Brazil) using the Bruce protocol. Continuous monitoring was performed with 12-lead ECG, recorded every minute. Blood pressure was measured manually with a cuff in the standing position in the last 30 seconds of each stage and for four minutes in the recovery period. Heart rate was determined by ECG and the chronotropic response was calculated as the achieved percentage of heart rate predicted for age, according to the Astrand formula (220 - age) at peak exercise. The 6-minute walk test (6MWT) was performed according to standard protocol21 with two walks at maximum walking speed in a 30-meter corridor, separated by a 15-minute interval. A HR monitor (Polar FS2, Electro, Kempele, Finland) and a pulse
oximeter (NoninOnyx 9500, Plymouth, Minnesota, USA) were used in the assessment.
24 h-Holter monitoring was performed using a portable three-channel tape recorder (Dynamics, Cardios, São Paulo, Brazil), at the beginning and end of the study. Subjects were instructed to maintain their normal daily activities during the recording. HRV analysis was performed when a good quality tracing of at least 18 h was available on a Burdick/DMI/Cardios Hospital Holter System (Spacelabs Burdick, Deerfield, Wisconsin, Sao Paulo, Brazil). Tracings were analyzed for five minutes every hour, and the sleep period with the loweat HR was used as reference.
The HRV indices were calculated in the time domain (SDNN: standard deviation of normal RR intervals; rMSSD: Root Mean Square of Successive Differences) and frequency domain (TP, total power; VLFP: very low frequency power; LFP: low frequency power; HFP, high frequency power).
Physical training protocolThe IG patients participated in a supervised program
consisting of three sessions per week, on alternate days, totaling 36 sessions in 12 weeks, as detailed in a previous publication19. Briefly, the protocol consisted of warm-up exercises for 15 minutes, followed by a 30 minute-walk and 15 minutes of cooling down. Exercise intensity was based on peak HR achieved on a treadmill test limited by symptoms and calculated by the Karvonen formula (maximal HR - HR at rest) 50-70% + resting HR22 and was adjusted throughout the program. The CG patients were instructed to maintain their daily routines and were asked about physical activities during consultations.
Statistical Analysis Statistical analysis was performed using SPSS software
version 20.0 for Mac OSX (SPSS Inc., Chicago, Illinois, United States of America). For this analysis, a sample of 36 patients was calculated to detect a 15% difference in SDNN variation between groups, with α error = 5% and β error = 20%. Descriptive analysis of continuous and categorical variables was performed. The presence or absence of normal distribution of variables was performed with the Shapiro-Wilk’s test. Continuous data were expressed as mean ± standard deviation or as median and interquartile (IQ) range Q1 - Q3 (25-75%) when presenting with non-normal distribution. Categorical variables were expressed as absolute values and percentages. Variations in measurements at the beginning and end of the study were expressed as delta values (Δ).
To evaluate the changes in continuous variables in relation to baseline, the paired Student’s t test was used for normally distributed variables or paired Wilcoxon test if the distribution was not normal. The comparison of means between groups was performed using Student's t test for continuous variables with normal distribution and the Mann-Whitney test for those with non-normal distribution. The comparison of categorical variables between groups was performed by Chi-square test. When necessary, analysis of variance transformations were performed. A two-tailed significance level of 0.05 was considered statistically significant.
202
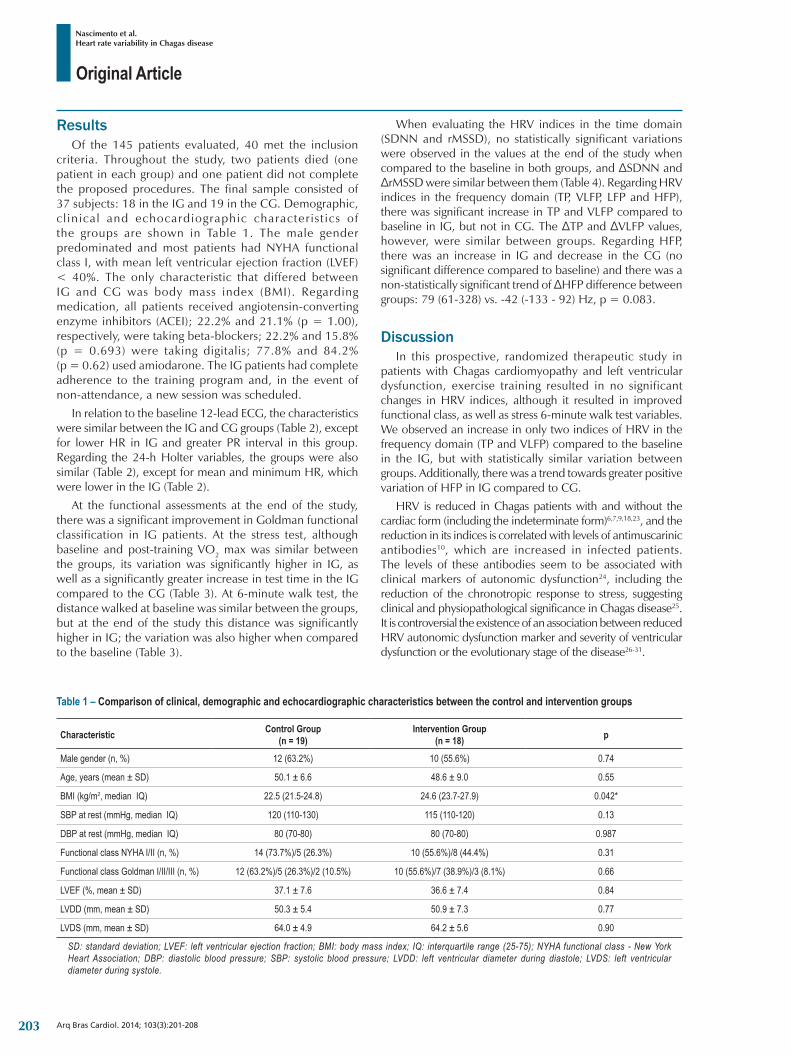
Original Article
Nascimento et al.Heart rate variability in Chagas disease
Arq Bras Cardiol. 2014; 103(3):201-208
ResultsOf the 145 patients evaluated, 40 met the inclusion
criteria. Throughout the study, two patients died (one patient in each group) and one patient did not complete the proposed procedures. The final sample consisted of 37 subjects: 18 in the IG and 19 in the CG. Demographic, c l inical and echocardiographic character is t ics of the groups are shown in Table 1. The male gender predominated and most patients had NYHA functional class I, with mean left ventricular ejection fraction (LVEF) < 40%. The only characteristic that differed between IG and CG was body mass index (BMI). Regarding medication, all patients received angiotensin-converting enzyme inhibitors (ACEI); 22.2% and 21.1% (p = 1.00), respectively, were taking beta-blockers; 22.2% and 15.8% (p = 0.693) were taking digitalis; 77.8% and 84.2% (p = 0.62) used amiodarone. The IG patients had complete adherence to the training program and, in the event of non-attendance, a new session was scheduled.
In relation to the baseline 12-lead ECG, the characteristics were similar between the IG and CG groups (Table 2), except for lower HR in IG and greater PR interval in this group. Regarding the 24-h Holter variables, the groups were also similar (Table 2), except for mean and minimum HR, which were lower in the IG (Table 2).
At the functional assessments at the end of the study, there was a significant improvement in Goldman functional classification in IG patients. At the stress test, although baseline and post-training VO2 max was similar between the groups, its variation was significantly higher in IG, as well as a significantly greater increase in test time in the IG compared to the CG (Table 3). At 6-minute walk test, the distance walked at baseline was similar between the groups, but at the end of the study this distance was significantly higher in IG; the variation was also higher when compared to the baseline (Table 3).
When evaluating the HRV indices in the time domain (SDNN and rMSSD), no statistically significant variations were observed in the values at the end of the study when compared to the baseline in both groups, and ΔSDNN and ΔrMSSD were similar between them (Table 4). Regarding HRV indices in the frequency domain (TP, VLFP, LFP and HFP), there was significant increase in TP and VLFP compared to baseline in IG, but not in CG. The ΔTP and ΔVLFP values, however, were similar between groups. Regarding HFP, there was an increase in IG and decrease in the CG (no significant difference compared to baseline) and there was a non-statistically significant trend of ΔHFP difference between groups: 79 (61-328) vs. -42 (-133 - 92) Hz, p = 0.083.
DiscussionIn this prospective, randomized therapeutic study in
patients with Chagas cardiomyopathy and left ventricular dysfunction, exercise training resulted in no significant changes in HRV indices, although it resulted in improved functional class, as well as stress 6-minute walk test variables. We observed an increase in only two indices of HRV in the frequency domain (TP and VLFP) compared to the baseline in the IG, but with statistically similar variation between groups. Additionally, there was a trend towards greater positive variation of HFP in IG compared to CG.
HRV is reduced in Chagas patients with and without the cardiac form (including the indeterminate form)6,7,9,18,23, and the reduction in its indices is correlated with levels of antimuscarinic antibodies10, which are increased in infected patients. The levels of these antibodies seem to be associated with clinical markers of autonomic dysfunction24, including the reduction of the chronotropic response to stress, suggesting clinical and physiopathological significance in Chagas disease25. It is controversial the existence of an association between reduced HRV autonomic dysfunction marker and severity of ventricular dysfunction or the evolutionary stage of the disease26-31.
Table 1 – Comparison of clinical, demographic and echocardiographic characteristics between the control and intervention groups
Characteristic Control Group (n = 19)
Intervention Group (n = 18) p
Male gender (n, %) 12 (63.2%) 10 (55.6%) 0.74
Age, years (mean ± SD) 50.1 ± 6.6 48.6 ± 9.0 0.55
BMI (kg/m2, median IQ) 22.5 (21.5-24.8) 24.6 (23.7-27.9) 0.042*
SBP at rest (mmHg, median IQ) 120 (110-130) 115 (110-120) 0.13
DBP at rest (mmHg, median IQ) 80 (70-80) 80 (70-80) 0.987
Functional class NYHA I/II (n, %) 14 (73.7%)/5 (26.3%) 10 (55.6%)/8 (44.4%) 0.31
Functional class Goldman I/II/III (n, %) 12 (63.2%)/5 (26.3%)/2 (10.5%) 10 (55.6%)/7 (38.9%)/3 (8.1%) 0.66
LVEF (%, mean ± SD) 37.1 ± 7.6 36.6 ± 7.4 0.84
LVDD (mm, mean ± SD) 50.3 ± 5.4 50.9 ± 7.3 0.77
LVDS (mm, mean ± SD) 64.0 ± 4.9 64.2 ± 5.6 0.90
SD: standard deviation; LVEF: left ventricular ejection fraction; BMI: body mass index; IQ: interquartile range (25-75); NYHA functional class - New York Heart Association; DBP: diastolic blood pressure; SBP: systolic blood pressure; LVDD: left ventricular diameter during diastole; LVDS: left ventricular diameter during systole.
203
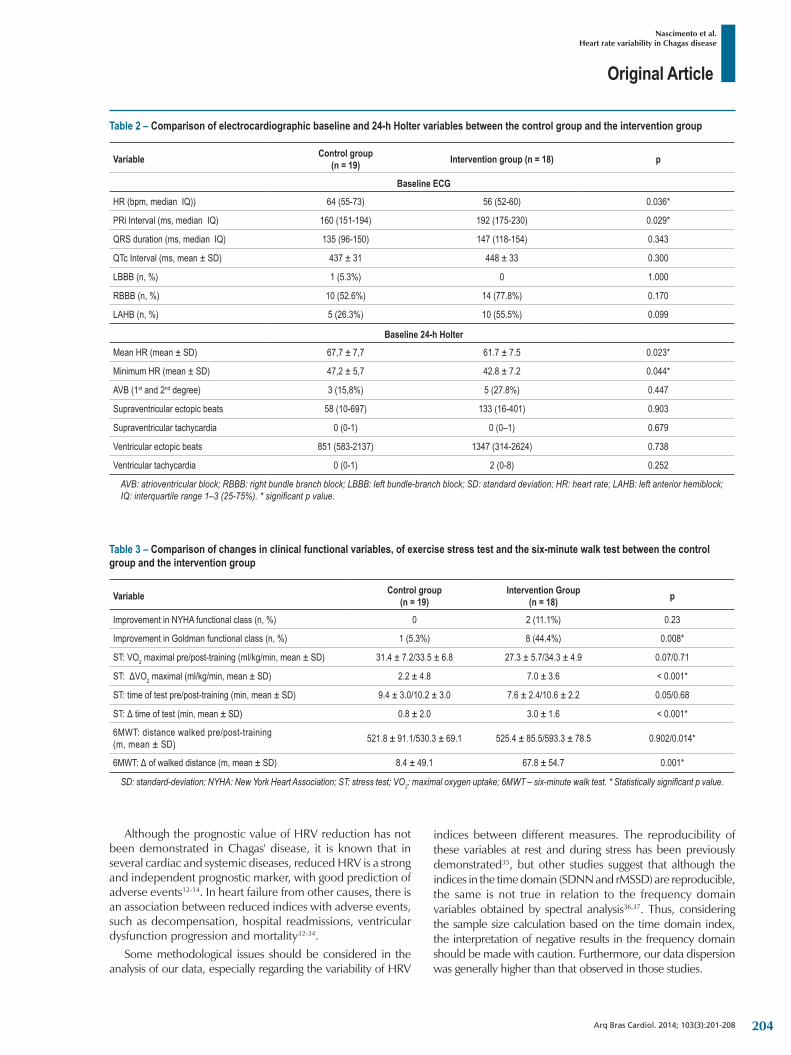
Original Article
Nascimento et al.Heart rate variability in Chagas disease
Arq Bras Cardiol. 2014; 103(3):201-208
Although the prognostic value of HRV reduction has not been demonstrated in Chagas' disease, it is known that in several cardiac and systemic diseases, reduced HRV is a strong and independent prognostic marker, with good prediction of adverse events12-14. In heart failure from other causes, there is an association between reduced indices with adverse events, such as decompensation, hospital readmissions, ventricular dysfunction progression and mortality32-34.
Some methodological issues should be considered in the analysis of our data, especially regarding the variability of HRV
indices between different measures. The reproducibility of these variables at rest and during stress has been previously demonstrated35, but other studies suggest that although the indices in the time domain (SDNN and rMSSD) are reproducible, the same is not true in relation to the frequency domain variables obtained by spectral analysis36,37. Thus, considering the sample size calculation based on the time domain index, the interpretation of negative results in the frequency domain should be made with caution. Furthermore, our data dispersion was generally higher than that observed in those studies.
Table 2 – Comparison of electrocardiographic baseline and 24-h Holter variables between the control group and the intervention group
Variable Control group (n = 19) Intervention group (n = 18) p
Baseline ECG
HR (bpm, median IQ)) 64 (55-73) 56 (52-60) 0.036*
PRi Interval (ms, median IQ) 160 (151-194) 192 (175-230) 0.029*
QRS duration (ms, median IQ) 135 (96-150) 147 (118-154) 0.343
QTc Interval (ms, mean ± SD) 437 ± 31 448 ± 33 0.300
LBBB (n, %) 1 (5.3%) 0 1.000
RBBB (n, %) 10 (52.6%) 14 (77.8%) 0.170
LAHB (n, %) 5 (26.3%) 10 (55.5%) 0.099
Baseline 24-h Holter
Mean HR (mean ± SD) 67,7 ± 7,7 61.7 ± 7.5 0.023*
Minimum HR (mean ± SD) 47,2 ± 5,7 42.8 ± 7.2 0.044*
AVB (1st and 2nd degree) 3 (15,8%) 5 (27.8%) 0.447
Supraventricular ectopic beats 58 (10-697) 133 (16-401) 0.903
Supraventricular tachycardia 0 (0-1) 0 (0–1) 0.679
Ventricular ectopic beats 851 (583-2137) 1347 (314-2624) 0.738
Ventricular tachycardia 0 (0-1) 2 (0-8) 0.252
AVB: atrioventricular block; RBBB: right bundle branch block; LBBB: left bundle-branch block; SD: standard deviation; HR: heart rate; LAHB: left anterior hemiblock; IQ: interquartile range 1–3 (25-75%). * significant p value.
Table 3 – Comparison of changes in clinical functional variables, of exercise stress test and the six-minute walk test between the control group and the intervention group
Variable Control group (n = 19)
Intervention Group (n = 18) p
Improvement in NYHA functional class (n, %) 0 2 (11.1%) 0.23
Improvement in Goldman functional class (n, %) 1 (5.3%) 8 (44.4%) 0.008*
ST: VO2maximalpre/post-training(ml/kg/min,mean±SD) 31.4 ± 7.2/33.5 ± 6.8 27.3 ± 5.7/34.3 ± 4.9 0.07/0.71
ST:ΔVO2maximal(ml/kg/min,mean±SD) 2.2 ± 4.8 7.0 ± 3.6 < 0.001*
ST: time of test pre/post-training (min, mean ± SD) 9.4 ± 3.0/10.2 ± 3.0 7.6 ± 2.4/10.6 ± 2.2 0.05/0.68
ST:Δtimeoftest(min,mean±SD) 0.8 ± 2.0 3.0 ± 1.6 < 0.001*
6MWT:distancewalkedpre/post-training (m, mean ± SD) 521.8 ± 91.1/530.3 ± 69.1 525.4 ± 85.5/593.3 ± 78.5 0.902/0.014*
6MWT:Δofwalkeddistance(m,mean±SD) 8.4 ± 49.1 67.8 ± 54.7 0.001*
SD: standard-deviation; NYHA: New York Heart Association; ST: stress test; VO2: maximal oxygen uptake; 6MWT – six-minute walk test. * Statistically significant p value.
204
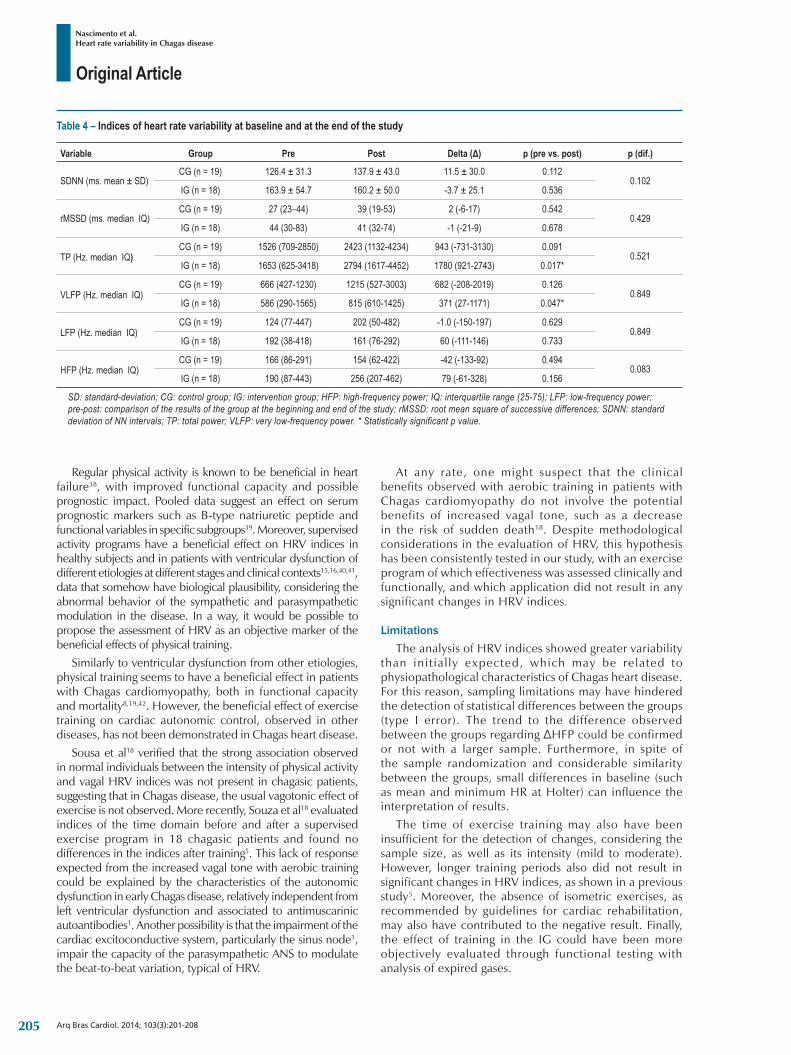
Original Article
Nascimento et al.Heart rate variability in Chagas disease
Arq Bras Cardiol. 2014; 103(3):201-208
Regular physical activity is known to be beneficial in heart failure38, with improved functional capacity and possible prognostic impact. Pooled data suggest an effect on serum prognostic markers such as B-type natriuretic peptide and functional variables in specific subgroups39. Moreover, supervised activity programs have a beneficial effect on HRV indices in healthy subjects and in patients with ventricular dysfunction of different etiologies at different stages and clinical contexts15,16,40,41, data that somehow have biological plausibility, considering the abnormal behavior of the sympathetic and parasympathetic modulation in the disease. In a way, it would be possible to propose the assessment of HRV as an objective marker of the beneficial effects of physical training.
Similarly to ventricular dysfunction from other etiologies, physical training seems to have a beneficial effect in patients with Chagas cardiomyopathy, both in functional capacity and mortality8,19,42. However, the beneficial effect of exercise training on cardiac autonomic control, observed in other diseases, has not been demonstrated in Chagas heart disease.
Sousa et al18 verified that the strong association observed in normal individuals between the intensity of physical activity and vagal HRV indices was not present in chagasic patients, suggesting that in Chagas disease, the usual vagotonic effect of exercise is not observed. More recently, Souza et al18 evaluated indices of the time domain before and after a supervised exercise program in 18 chagasic patients and found no differences in the indices after training5. This lack of response expected from the increased vagal tone with aerobic training could be explained by the characteristics of the autonomic dysfunction in early Chagas disease, relatively independent from left ventricular dysfunction and associated to antimuscarinic autoantibodies1. Another possibility is that the impairment of the cardiac excitoconductive system, particularly the sinus node1, impair the capacity of the parasympathetic ANS to modulate the beat-to-beat variation, typical of HRV.
At any rate, one might suspect that the clinical benefits observed with aerobic training in patients with Chagas cardiomyopathy do not involve the potential benefits of increased vagal tone, such as a decrease in the risk of sudden death18. Despite methodological considerations in the evaluation of HRV, this hypothesis has been consistently tested in our study, with an exercise program of which effectiveness was assessed clinically and functionally, and which application did not result in any significant changes in HRV indices.
LimitationsThe analysis of HRV indices showed greater variability
than init ial ly expected, which may be related to physiopathological characteristics of Chagas heart disease. For this reason, sampling limitations may have hindered the detection of statistical differences between the groups (type I error). The trend to the difference observed between the groups regarding ΔHFP could be confirmed or not with a larger sample. Furthermore, in spite of the sample randomization and considerable similarity between the groups, small differences in baseline (such as mean and minimum HR at Holter) can influence the interpretation of results.
The time of exercise training may also have been insufficient for the detection of changes, considering the sample size, as well as its intensity (mild to moderate). However, longer training periods also did not result in significant changes in HRV indices, as shown in a previous study5. Moreover, the absence of isometric exercises, as recommended by guidelines for cardiac rehabilitation, may also have contributed to the negative result. Finally, the effect of training in the IG could have been more objectively evaluated through functional testing with analysis of expired gases.
Table 4 – Indices of heart rate variability at baseline and at the end of the study
Variable Group Pre Post Delta (Δ) p (pre vs. post) p (dif.)
SDNN (ms. mean ± SD)CG (n = 19) 126.4 ± 31.3 137.9 ± 43.0 11.5 ± 30.0 0.112
0.102IG (n = 18) 163.9 ± 54.7 160.2 ± 50.0 -3.7 ± 25.1 0.536
rMSSD (ms. median IQ)CG (n = 19) 27 (23–44) 39 (19-53) 2 (-6-17) 0.542
0.429IG (n = 18) 44 (30-83) 41 (32-74) -1 (-21-9) 0.678
TP (Hz. median IQ)CG (n = 19) 1526 (709-2850) 2423 (1132-4234) 943 (-731-3130) 0.091
0.521IG (n = 18) 1653 (625-3418) 2794 (1617-4452) 1780 (921-2743) 0.017*
VLFP (Hz. median IQ)CG (n = 19) 666 (427-1230) 1215 (527-3003) 682 (-208-2019) 0.126
0.849IG (n = 18) 586 (290-1565) 815 (610-1425) 371 (27-1171) 0.047*
LFP (Hz. median IQ)CG (n = 19) 124 (77-447) 202 (50-482) -1.0 (-150-197) 0.629
0.849IG (n = 18) 192 (38-418) 161 (76-292) 60 (-111-146) 0.733
HFP (Hz. median IQ)CG (n = 19) 166 (86-291) 154 (62-422) -42 (-133-92) 0.494
0.083IG (n = 18) 190 (87-443) 256 (207-462) 79 (-61-328) 0.156
SD: standard-deviation; CG: control group; IG: intervention group; HFP: high-frequency power; IQ: interquartile range (25-75); LFP: low-frequency power; pre-post: comparison of the results of the group at the beginning and end of the study; rMSSD: root mean square of successive differences; SDNN: standard deviation of NN intervals; TP: total power; VLFP: very low-frequency power. * Statistically significant p value.
205

Original Article
Nascimento et al.Heart rate variability in Chagas disease
Arq Bras Cardiol. 2014; 103(3):201-208
ConclusionsIn the studied population, exercise training did not significantly
alter HRV indices in Chagas patients with LV dysfunction, although it resulted in functional improvement. The only changes observed in relation to baseline were increased TP and VLFP in the IG, with no significant difference in changes between groups. The data are consistent with previous publications and suggest that the clinical benefits of physical conditioning in Chagas heart disease are independent from HRV indices. Future studies in larger populations are needed in order to reach more definitive conclusions about the behavior of HRV during physical conditioning in Chagas heart disease.
Author contributionsConception and design of the research: Nascimento BR,
Lima MMO, Rocha MOC, Ribeiro AL; Acquisition of data: Lima, MMO, Nunes MCP, Alencar MCN, Costa HS, Pinto Filho MM, Cota VES; Analysis and interpretation of the
data: Nascimento BR, Lima MMO, Pinto Filho MM, Cota VES; Obtaining financing: Rocha MOC, Ribeiro AL; Writing of the manuscript: Nascimento BR, Lima MMO; Critical revision of the manuscript for intellectual content: Rocha MOC, Ribeiro AL.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThis study was funded by CNPq, FAPEMIG and CAPES.
Study AssociationThis article is part of the thesis of Doctoral submitted by
Márcia Maria Oliveira Lima, from Universidade Federal de Minas Gerais.
1. Nunes MC, Dones W, Morillo CA, Encina JJ, Ribeiro AL; Council on Chagas Disease of the Interamerican Society of Cardiology. Chagas disease: an overview of clinical and epidemiological aspects. J Am Coll Cardiol. 2013;62(9):767-76.
2. Biolo A, Ribeiro AL, Clausell N. Chagas cardiomyopathy: where do we stand after a hundred years? Prog Cardiovasc Dis. 2010;52(4):300-16.
3. Ribeiro AL, Nunes MP, Teixeira MM, Rocha MO. Diagnosis and management of Chagas disease and cardiomyopathy. Nat Rev Cardiol. 2012;9(10):576-89.
4. Rocha MO, Teixeira MM, Ribeiro AL. Anupdateonthe management of Chagas cardiomyopathy. Expert Rev Anti Infect Ther. 2007;5(4):727-43.
5. Amaral da Silva Souza MV, Santos Soares CC, Rega de Oliveira J, Rosa de Oliveira C, Hargreaves Fialho P, Cunha DM, et al. [Heart rate variability: analysis of time-domain indices in patients with chronic Chagas disease before and after an exercise program]. Rev Port Cardiol. 2013;32(3):219-27.
6. Resende LA, Carneiro AC, Ferreira BD, Silva RA, Silva VJ, Prata A, et al. Análise temporal da variabilidade da frequencia cardíaca no estado basal em idosos chagásicos na forma indeterminada em área endemica. Rev Soc Bras Med Trop. 2003;36(6):703-6.
7. Guzzetti S, Iosa D, Pecis M, Bonura L, Prosdocimi M, Malliani A. Impaired heart rate variability in patients with chronic Chagas’ disease. Am Heart J. 1991;121(6 Pt 1):1727-34.
8. Ritt LE, Carvalho AC, Feitosa GS, Pinho-Filho JA, Andrade MV, Feitosa-Filho GS, et al. Cardiopulmonary exercise and 6-min walk tests as predictors of quality of life and long-term mortality among patients with heart failure due to Chagas disease. Int J Cardiol. 2013;168(4):4584-5.
9. Rocha AL, Lombardi F, da Costa Rocha MO, Barros MV, Val Barros Vda C, Reis AM, et al. Chronotropic incompetence and abnormal autonomic modulation in ambulatory Chagas disease patients. Ann Noninvasive Electrocardiol. 2006;11(1):3-11.
10. Ribeiro AL, Gimenez LE, Hernandez CC, Carvalho AC, Teixeira MM, Guedes VC, et al. Early occurrence of anti-muscarinic autoantibodies and abnormal vagal modulation in Chagas disease. Int J Cardiol. 2007;117(1):59-63.
11. Ribeiro AL, Moraes RS, Ribeiro JP, Ferlin EL, Torres RM, Oliveira E, et al. Parasympathetic dysautonomia precedes left ventricular systolic dysfunction in Chagas disease. Am Heart J. 2001;141(2):260-5.
12. Bauer A, Barthel P, Schneider R, Ulm K, Muller A, Joeinig A, et al. Improved stratification of autonomic regulation for risk prediction in post-infarction patients with preserved left ventricular function (ISAR-risk). Eur Heart J. 2009;30(5):576-83.
13. La Rovere MT, Pinna GD, Maestri R, Barlera S, Bernardinangeli M, Veniani M, et al; GISSI-HF Investigators. Autonomic markers and cardiovascular and arrhythmic events in heart failure patients: still a place in prognostication? Datafromthe GISSI-HF trial. Eur J Heart Fail. 2012;14(12):1410-9.
14. Nascimento BR, Coelho TO, Ribeiro AL. Variabilidade da frequencia cardíaca em pacientes criticamente enfermos. In: Botoni FA, Dias FS. (eds.). PROAMI. Programa de atualização em medicina intensiva. Porto Alegre: Artmed Panamericana; 2009.
15. Larsen AI, Gjesdal K, Hall C, Aukrust P, Aarsland T, Dickstein K. Effect of exercise training in patients with heart failure: a pilot study on autonomic balance assessed by heart rate variability. Eur J Cardiovasc Prev Rehabil. 2004;11(2):162-7.
16. Iellamo F, Manzi V, Caminiti G, Sposato B, Massaro M, Cerrito A, et al. Dose-response relationship of baroreflex sensitivity and heart rate variability to individually-tailored exercise training in patients with heart failure. Int J Cardiol. 2013;166(2):334-9.
17. Vasconcelos DF, Junqueira Jr LF. Distinctive impaired cardiac autonomic modulation of heart rate variability in chronic Chagas’ indeterminate and heart diseases. J Electrocardiol. 2009;42(3):281-9.
18. Sousa L, Rocha MO, Britto RR, Lombardi F, Ribeiro AL. Chagas disease alters the relationship between heart rate variability and daily physical activity. Int J Cardiol. 2009;135(2):257-9.
19. Lima MM, Rocha MO, Nunes MC, Sousa L, Costa HS, Alencar MC, et al. A randomized trial of the effects of exercise training in Chagas cardiomyopathy. Eur J Heart Fail. 2010;12(8):866-73.
20. Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ, Ponikowski P, Poole-Wilson PA, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: The task force for the diagnosis and treatment of acute and chronic heart failure 2008 of the European Society of Cardiology. Developed in collaboration with the heart failure association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur Heart J. 2008;29(19):2388-442. Erratum in: Eur Heart J. 2010;12(4):416, Eur Heart J. 2010;31(5):624.
References
206
Original Article
Nascimento et al.Heart rate variability in Chagas disease
Arq Bras Cardiol. 2014; 103(3):201-208
21. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS Statement: guidelines for the six-minute test. Am J Respir Crit Care Med. 2002;166(1):111-7.
22. Myers J. Principles of exercise prescription for patients with chronic heart failure. Heart Fail Rev. 2008;13(1):61-8.
23. Ribeiro AL, Cassini P, Peixoto SV, Lima-Costa MF. Vagal impairment in elderly Chagas disease patients: a population-based study (the Bambui study). Int J Cardiol. 2011;147(3):359-65.
24. Thiers CA, Barbosa JL, Pereira Bde B, Nascimento EM, Nascimento JH, Medei EH, et al. Autonomic dysfunction and anti-M2 and anti-beta 1 receptor antibodies in Chagas disease patients. Arq Bras Cardiol. 2012;99(2):732-9.
25. Talvani A, Rocha MO, Ribeiro AL, Borda E, Sterin-Borda L, Teixeira MM. Levels of anti-M2 and anti-beta1 autoantibodies do not correlate with the degree of heart dysfunction in Chagas’ heart disease. Microbes Infect. 2006;8(9-10):2459-64.
26. Ribeiro AL, Lombardi F, Sousa MR, Lins Barros MV, Porta A, Costa Val Barros V, et al. Power-law behavior of heart rate variability in Chagas’ disease. Am J Cardiol. 2002;89(4):414-8.
27. Villar JC, Leon H, Morillo CA. Cardiovascular autonomic function testing in asymptomatic T. cruzi carriers: a sensitive method to identify subclinical Chagas’ disease. Int J Cardiol. 2004;93(2-3):189-95.
28. Tundo F, Lombardi F, Rocha MC, Botoni F, Schmidt G, Barros VC, et al. Heart rate turbulence and left ventricular ejection fraction in Chagas disease. Europace. 2005;7(3):197-203.
29. Vasconcelos DF, Junqueira Jr LF. Funções autonômica e mecânica ventricular na cardiopatia chagásica crônica assintomática. Arq Bras Cardiol. 2012;98:111-119.
30. Davila DF, Inglessis G, Mazzei de Davila CA. Chagas’ heart disease and the autonomic nervous system. Int J Cardiol. 1998;66(2):123-7.
31. Molina RB, Matsubara BB, Hueb JC, Zanati SG, Meira DA, Cassolato JL, et al. Dysautonomia and ventricular dysfunction in the indeterminate form of Chagas disease. Int J Cardiol. 2006;113(2):188-93.
32. Tanindi A, Olgun H, Celik B, Boyaci B. Heart rate variability in patients hospitalized for decompensated diastolic heart failure at admission and after clinical stabilization. Future Cardiol. 2012;8(3):473-82.
33. Arsenos P, Gatzoulis K, Manis G, Gialernios T, Dilaveris P, Tsiachris D, et al. Decreased scale-specific heart rate variability after multi resolution wavelet analysis predicts sudden cardiac death in heart failure patients. Int J Cardiol. 2012;154(3):358-60.
34. Ho YL, Lin C, Lin YH, Lo MT. The prognostic value of non-linear analysis of heart rate variability in patients with congestive heart failure: a pilot study of multiscale entropy. PloS One. 2011;6(4):e18699.
35. McNarry MA, Lewis MJ. Heart rate variability reproducibility during exercise. Physiol Meas. 2012;33(7):1123-33.
36. Tannus LR, Sperandei S, Montenegro Júnior RM, Carvalho VR, Pedrosa HC, Felix MT, et al. Reproducibility of methods used for the assessment of autonomous nervous system’s function. Auton Neurosci. 2013;177(2):275-9.
37. Ginsburg P, Bartur G, Peleg S, Vatine JJ, Katz-Leurer M. Reproducibility of heart rate variability during rest, paced breathing and light-to-moderate intense exercise in patients one month after stroke. Eur Neurol. 2011;66(2):117-22.
38. McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, et al; ESC Committee for Practice Guidelines. Esc guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The task force for the diagnosis and treatment of acute and chronic heart failure 2012 of the European Society of Cardiology. Developed in collaboration with the heart failure association (HFA) of the ESC. Eur J Heart Fail. 2012;14(8):803-69. Erratum in Eur J Heart Fail. 2013;15(3):361-2.
39. Cipriano G Jr, Cipriano VT, da Silva VZ, Cipriano GF, Chiappa GR, de Lima AC, et al. Aerobic exercise effect on prognostic markers for systolic heart failure patients: a systematic review and meta-analysis. Heart Fail Rev. 2013 Oct 16. [Epub ahead of print].
40. Murad K, Brubaker PH, Fitzgerald DM, Morgan TM, Goff DC Jr, Soliman EZ, et al. Exercise training improves heart rate variability in older patients with heart failure: a randomized, controlled, single-blinded trial. Congest Heart Fail. 2012;18(4):192-7.
41. Routledge FS, Campbell TS, McFetridge-Durdle JA, Bacon SL. Improvements in heart rate variability with exercise therapy. Can Jo Cardiol. 2010;26(6):303-12.
42. Fialho PH, Tura BR, Sousa AS, Oliveira CR, Soares CC, Oliveira JR, et al. Efeitos de um programa de exercícios sobre a capacidade funcional de pacientes com cardiopatia chagásica crônica, avaliados por teste cardiopulmonar. Rev Soc Bras Med Trop. 2012;45(2):220-4.
207

Original Article
Nascimento et al.Heart rate variability in Chagas disease
Arq Bras Cardiol. 2014; 103(3):201-208 208
Original Article
Survival and Predictive Factors of Lethality in Hemodyalisis: D/I Polymorphism of The Angiotensin I-Converting Enzyme and of the Angiotensinogen M235T GenesMauro Alves1, Nelson Albuquerque de Souza e Silva1, Lucia Helena Alvares Salis1, Basilio de Bragança Pereira1, Paulo Henrique Godoy1, Emília Matos do Nascimento1, Jose Mario Franco Oliveira2
Universidade Federal do Rio de Janeiro1, Rio de Janeiro, RJ; Universidade Federal Fluminense2, Niteroi, RJ - Brazil
Mailing Address: Mauro Alves •Rua Paraim, 54/201, Freguesia, Ilha do Governador. Postal Code 21911-050, Rio de Janeiro, RJ – BrazilE-mail: [email protected], [email protected] received October 12, 2013; revised manuscript February 16, 2014; accepted March 27, 2014.
DOI: 10.5935/abc.20140105
Abstract
Background: End-stage kidney disease patients continue to have markedly increased cardiovascular disease morbidity and mortality. Analysis of genetic factors connected with the renin–angiotensin system that influences the survival of the patients with end-stage kidney disease supports the ongoing search for improved outcomes.
Objective: To assess survival and its association with the polymorphism of renin-angiotensin system genes: angiotensin I-converting enzyme insertion/deletion and angiotensinogen M235T in patients undergoing hemodialysis.
Methods: Our study was designed to examine the role of renin-angiotensin system genes. It was an observational study. We analyzed 473 chronic hemodialysis patients in four dialysis units in the state of Rio de Janeiro. Survival rates were calculated by the Kaplan–Meier method and the differences between the curves were evaluated by Tarone–Ware, Peto-Prentice, and log rank tests. We also used logistic regression analysis and the multinomial model. A p value ≤ 0.05 was considered to be statistically significant. The local medical ethics committee gave their approval to this study.
Results: The mean age of patients was 45.8 years old. The overall survival rate was 48% at 11 years. The major causes of death were cardiovascular diseases (34%) and infections (15%). Logistic regression analysis found statistical significance for the following variables: age (p = 0.000038), TT angiotensinogen (p = 0.08261), and family income greater than five times the minimum wage (p = 0.03089), the latter being a protective factor.
Conclusions: The survival of hemodialysis patients is likely to be influenced by the TT of the angiotensinogen M235T gene. (Arq Bras Cardiol. 2014; 103(3):209-218)
Keywords: Survival Analysis; Lethality; Renal Dialysis; Polymorphism, Genetic; Peptidyl-Dipeptidase A; Kidney Failure, Chronic.
IntroductionThe number of patients undergoing renal replacement
therapy is on the increase all over the world, including Brazil1-3. Data from the Brazilian Society of Nephrology shows that between 1994 and 2009, the number of patients enrolled in chronic dialysis programs in Brazil more than tripled from 24,000, to 77,5893. Of these, 89.6% were on hemodialysis3.
On July 1st, 2010, the number of Brazilian dialysis patients was 92,091. The annual crude mortality rate for patients with end-stage chronic kidney failure was 17.1% in 20093, and 17.9% in 20104. Despite major advances in recent decades in the treatment of chronic kidney disease,
cardiovascular disease is still the main cause of death for these patients, especially among those on dialysis. The cardiovascular mortality of hemodyalized patients is high (40% to 50% of the population of chronic kidney patients), significantly higher than for the general population5,6. The general population trend for cardiovascular mortality is decreasing , but, among hemodialyzed patients, it is increasing4-8.
Traditional cardiovascular risk factors alone are not capable of explaining the high mortality rate for chronic kidney disease, dialysis population. Other factors need to be taken into consideration. Our view is that the key to improving survival is better knowledge of prognostic risk factors, be they traditional or not.
The primary objective of this study was to assess the survival of patients with end-stage chronic kidney failure who received hemodialysis in four centers in the State of Rio de Janeiro. patients were followed up for 11 years and compared to the general population to look at the correlation between mortality for those with cardiovascular risk factors and D/I and M235T polymorphisms of the angiotensin I-converting enzyme and the angiotensinogen genes, respectively. The secondary objective was to analyze cause of death by sex and age group.
209

Original Article
Alves et al.Survival among hemodyalized patients and polymorphism
Arq Bras Cardiol. 2014; 103(3):209-218
Methods
Study Diagram:
Population of4 HD centers(1997/98)
-------- 11 years ------
• Death
• Survival on HD
• Transplanted
• TransferredThe initial study cohort comprised 473 chronic hemodialyzed
patients from four hemodialysis centers. Three from the city of Niteroi and one from Rio Bonito. This represented all eligible patients in those hemodialysis centers from July 15, 1997 to July 15, 1998.
Inclusion criteria: All adult patients (aged 18 years old or more at the time of selection for this study), regardless of age at the time hemodialysis treatment began, who had been on chronic hemodialysis for at least one year during the period between July 15, 1997 and July 15, 1998.
Exclusion criteria: Exclusion criteria included the presence of Acute Kidney Failure; refusal to participate in this study; and the fact that patients had already been submitted to kidney transplant before selection.
Death records: We used the Mortality Information System. Survival analysis used information from the study population data bases, and death records (1998 to 2008) in the State of Rio de Janeiro, with the objective of identifying individuals who passed away and to determine cause of death. Analysis was conducted with RecLink III software and consisted of six steps:
1. Standardizing the format of data variables.2. Grouping records using identification keys. 3. Using algorithms to compare chains of characters.4. Scoring record pairs on their level of global concordance. 5. Using threshold definitions to determine whether each
pair was real, doubtful, borderline, or non-paired.6. Manual revision of the doubtful or borderline pairs,
aiming to reclassify as real pairs or non-pairs.Study duration: Follow-up: 11 years; recruitment: July
15, 1997 to July 15, 1998; conclusion: December 31, 2008.Variables: The variables studied were defined as follows:1. Systolic Blood Pressure before the hemodialysis
session: The first measurement recorded in the medical history was used in the recruiting stage of this study.
2. Length of hemodialysis in months at the time of recruiting. From this variable, it was possible to calculate the date hemodialysis started and the time of survival on hemodialysis. This was calculated by the sum of the time of hemodialysis at the beginning of the treatment, plus the time until the event (death, kidney transplant or conclusion of the study).
3. Body Mass Index. Calculated using the formula, weight in kg, divided by the squared height in meters. Weight was obtained prior to hemodialysis.
4. Monthly family income, as provided by the patient when he or she was admitted to the hemodialysis center. This information was registered in the medical record or it
was collected from the patient. The variable was measured in number of minimum wages at the time the treatment began in the hemodialysis center. Afterwards, we created the following categories: less than two times the minimum wage; from two to five times the minimum wage; and more than five times the minimum wage.
5. Age at the beginning of hemodialysis (in years).6. Gender.7. Basic cause of death: using data from the Mortality
Information System of the State Secretariat of Health in the State of Rio de Janeiro, we identified the basic cause of death recorded in the Mortality Information System through selection rules.
8. Triglycerides: measured by the enzymathic method, at the time of recruiting.
9. Total cholesterol: measured by the enzymathic method, at the time of recruiting.
10. High-density lipoprotein: measured by the enzymathic method, at the time of recruiting.
11. Hematocrit: Percentage occupied by red blood cells in the total blood volume, at the time of recruiting.
12. Diabetes mellitus, diagnosis registered on the medical record at the time of admission in the hemodialysis center, and collected by us during recruiting.
13. History of ischemic heart disease, characterized by acute myocardial infarction, angina pectoris, or by some previous invasive coronary procedures. This information was collected from medical records.
14. History of stroke, collected from medical records.15. History of smoking or former smoking, recorded in medical
records at the time of admission to the hemodialysis center.16. Polymorphism of genes of the angiotensin I-converting
enzyme (I/D) and angiotensinogen (M235T). Samples of 5 mL of blood were drawn from patients at the time of recruiting and stored in tubes containing ethylenediaminetetraacetic acid, which were sent to São Paulo. The genetic polymorphism of the angiotensin I-converting enzyme (I/D) was determined by using a standardized essay with three primers. The variable M235T of the angiotensinogen gene was determined by the polymerase chain reaction method, followed by enzymatic digestion. The team who conducted the genotypic assessments did not have access to the clinical information of the study patients.
Patients who had undergone kidney transplant and patients who were alive on December 31, 2008, when the study was concluded, were censored to their respective dates.
The analyzed outcomes were: primary, time of survival; and secondary, basic cause of death.
The Research Ethics Committee in the University Hospital Clementino Fraga Filho, at Universidade Federal do Rio de Janeiro, approved this study.
Statistical AnalysisEach variable was analyzed and its distribution, mean,
and standard deviation was calculated. The Chi-Square test was used for categorical variables and the unpaired Student’s
210
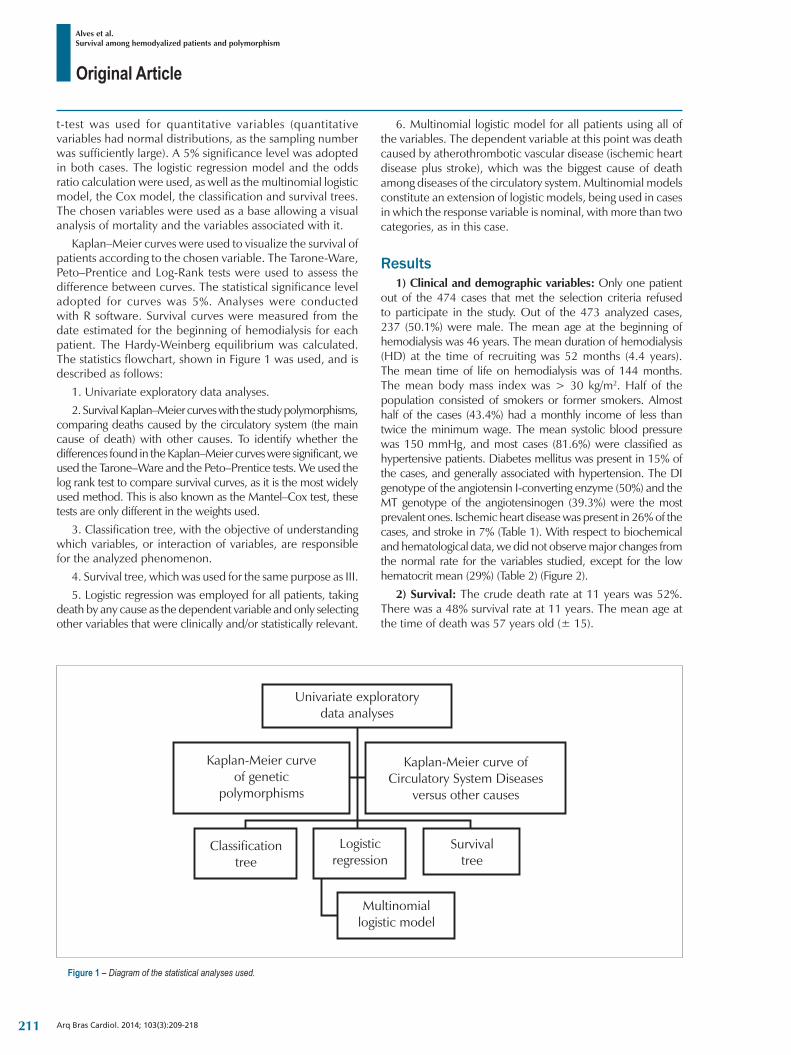
Original Article
Alves et al.Survival among hemodyalized patients and polymorphism
Arq Bras Cardiol. 2014; 103(3):209-218
Figure 1 – Diagram of the statistical analyses used.
t-test was used for quantitative variables (quantitative variables had normal distributions, as the sampling number was sufficiently large). A 5% significance level was adopted in both cases. The logistic regression model and the odds ratio calculation were used, as well as the multinomial logistic model, the Cox model, the classification and survival trees. The chosen variables were used as a base allowing a visual analysis of mortality and the variables associated with it.
Kaplan–Meier curves were used to visualize the survival of patients according to the chosen variable. The Tarone-Ware, Peto–Prentice and Log-Rank tests were used to assess the difference between curves. The statistical significance level adopted for curves was 5%. Analyses were conducted with R software. Survival curves were measured from the date estimated for the beginning of hemodialysis for each patient. The Hardy-Weinberg equilibrium was calculated. The statistics flowchart, shown in Figure 1 was used, and is described as follows:
1. Univariate exploratory data analyses.2. Survival Kaplan–Meier curves with the study polymorphisms,
comparing deaths caused by the circulatory system (the main cause of death) with other causes. To identify whether the differences found in the Kaplan–Meier curves were significant, we used the Tarone–Ware and the Peto–Prentice tests. We used the log rank test to compare survival curves, as it is the most widely used method. This is also known as the Mantel–Cox test, these tests are only different in the weights used.
3. Classification tree, with the objective of understanding which variables, or interaction of variables, are responsible for the analyzed phenomenon.
4. Survival tree, which was used for the same purpose as III. 5. Logistic regression was employed for all patients, taking
death by any cause as the dependent variable and only selecting other variables that were clinically and/or statistically relevant.
6. Multinomial logistic model for all patients using all of the variables. The dependent variable at this point was death caused by atherothrombotic vascular disease (ischemic heart disease plus stroke), which was the biggest cause of death among diseases of the circulatory system. Multinomial models constitute an extension of logistic models, being used in cases in which the response variable is nominal, with more than two categories, as in this case.
Results1) Clinical and demographic variables: Only one patient
out of the 474 cases that met the selection criteria refused to participate in the study. Out of the 473 analyzed cases, 237 (50.1%) were male. The mean age at the beginning of hemodialysis was 46 years. The mean duration of hemodialysis (HD) at the time of recruiting was 52 months (4.4 years). The mean time of life on hemodialysis was of 144 months. The mean body mass index was > 30 kg/m2. Half of the population consisted of smokers or former smokers. Almost half of the cases (43.4%) had a monthly income of less than twice the minimum wage. The mean systolic blood pressure was 150 mmHg, and most cases (81.6%) were classified as hypertensive patients. Diabetes mellitus was present in 15% of the cases, and generally associated with hypertension. The DI genotype of the angiotensin I-converting enzyme (50%) and the MT genotype of the angiotensinogen (39.3%) were the most prevalent ones. Ischemic heart disease was present in 26% of the cases, and stroke in 7% (Table 1). With respect to biochemical and hematological data, we did not observe major changes from the normal rate for the variables studied, except for the low hematocrit mean (29%) (Table 2) (Figure 2).
2) Survival: The crude death rate at 11 years was 52%. There was a 48% survival rate at 11 years. The mean age at the time of death was 57 years old (± 15).
211
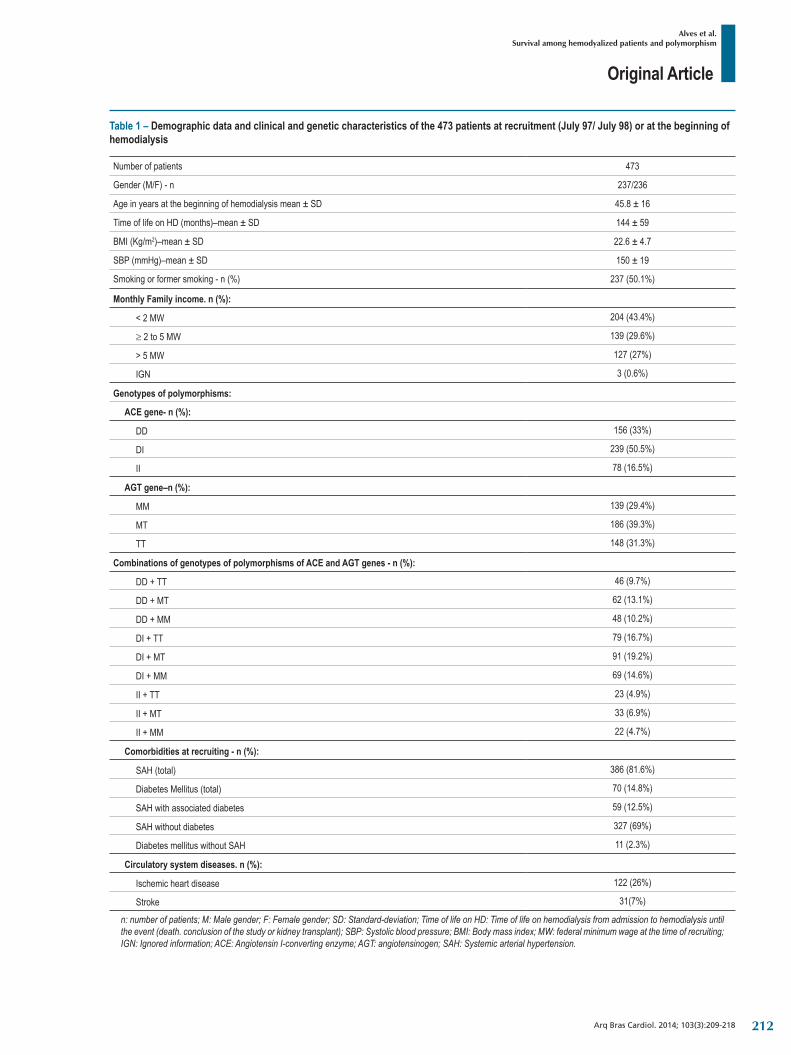
Original Article
Alves et al.Survival among hemodyalized patients and polymorphism
Arq Bras Cardiol. 2014; 103(3):209-218
Table 1 – Demographic data and clinical and genetic characteristics of the 473 patients at recruitment (July 97/ July 98) or at the beginning of hemodialysis
Number of patients 473
Gender (M/F) - n 237/236
Age in years at the beginning of hemodialysis mean ± SD 45.8 ± 16
Time of life on HD (months)–mean ± SD 144 ± 59
BMI (Kg/m2)–mean ± SD 22.6 ± 4.7
SBP (mmHg)–mean ± SD 150 ± 19
Smoking or former smoking - n (%) 237 (50.1%)
Monthly Family income. n (%):
< 2 MW 204 (43.4%)
≥ 2 to 5 MW 139 (29.6%)
> 5 MW 127 (27%)
IGN 3 (0.6%)
Genotypes of polymorphisms:
ACE gene- n (%):
DD 156 (33%)
DI 239 (50.5%)
II 78 (16.5%)
AGT gene–n (%):
MM 139 (29.4%)
MT 186 (39.3%)
TT 148 (31.3%)
Combinations of genotypes of polymorphisms of ACE and AGT genes - n (%):
DD+TT 46 (9.7%)
DD+MT 62 (13.1%)
DD+MM 48 (10.2%)
DI+TT 79 (16.7%)
DI+MT 91 (19.2%)
DI+MM 69 (14.6%)
II+TT 23 (4.9%)
II+MT 33 (6.9%)
II+MM 22 (4.7%)
Comorbidities at recruiting - n (%):
SAH (total) 386 (81.6%)
Diabetes Mellitus (total) 70 (14.8%)
SAHwithassociateddiabetes 59 (12.5%)
SAHwithoutdiabetes 327 (69%)
DiabetesmellituswithoutSAH 11 (2.3%)
Circulatory system diseases. n (%):
Ischemic heart disease 122 (26%)
Stroke 31(7%)
n: number of patients; M: Male gender; F: Female gender; SD: Standard-deviation; Time of life on HD: Time of life on hemodialysis from admission to hemodialysis until the event (death. conclusion of the study or kidney transplant); SBP: Systolic blood pressure; BMI: Body mass index; MW: federal minimum wage at the time of recruiting; IGN: Ignored information; ACE: Angiotensin I-converting enzyme; AGT: angiotensinogen; SAH: Systemic arterial hypertension.
212
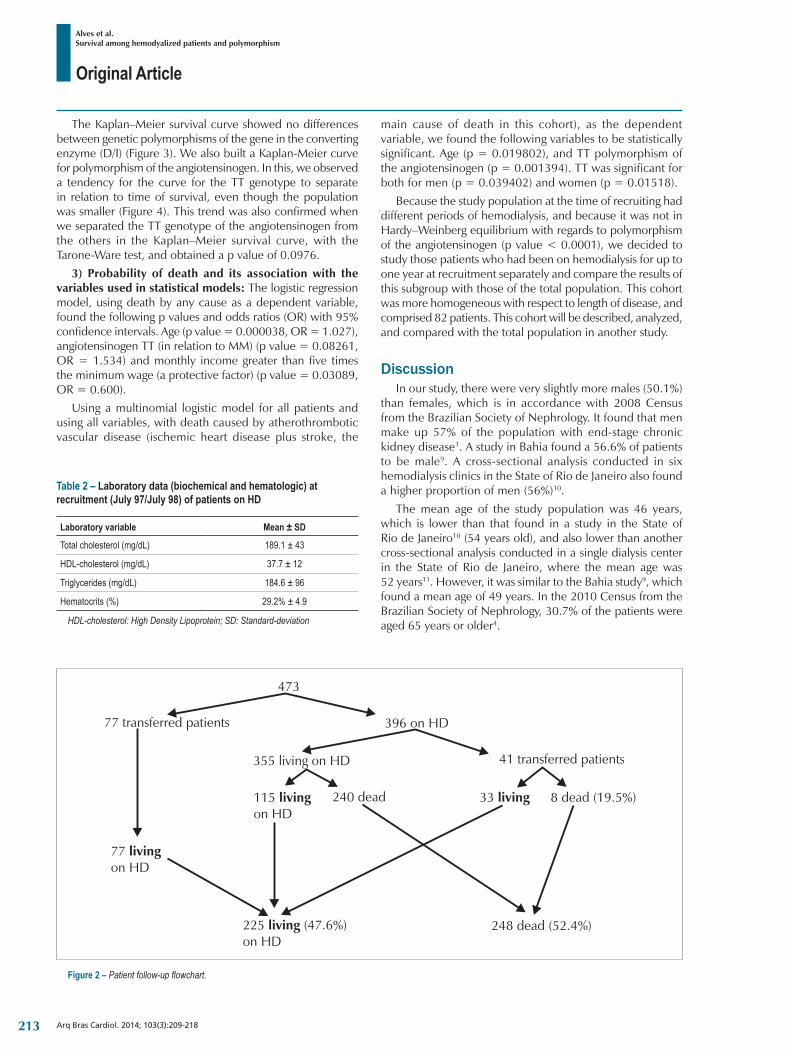
Original Article
Alves et al.Survival among hemodyalized patients and polymorphism
Arq Bras Cardiol. 2014; 103(3):209-218
Figure 2 – Patient follow-up flowchart.
The Kaplan–Meier survival curve showed no differences between genetic polymorphisms of the gene in the converting enzyme (D/I) (Figure 3). We also built a Kaplan-Meier curve for polymorphism of the angiotensinogen. In this, we observed a tendency for the curve for the TT genotype to separate in relation to time of survival, even though the population was smaller (Figure 4). This trend was also confirmed when we separated the TT genotype of the angiotensinogen from the others in the Kaplan–Meier survival curve, with the Tarone-Ware test, and obtained a p value of 0.0976.
3) Probability of death and its association with the variables used in statistical models: The logistic regression model, using death by any cause as a dependent variable, found the following p values and odds ratios (OR) with 95% confidence intervals. Age (p value = 0.000038, OR = 1.027), angiotensinogen TT (in relation to MM) (p value = 0.08261, OR = 1.534) and monthly income greater than five times the minimum wage (a protective factor) (p value = 0.03089, OR = 0.600).
Using a multinomial logistic model for all patients and using all variables, with death caused by atherothrombotic vascular disease (ischemic heart disease plus stroke, the
main cause of death in this cohort), as the dependent variable, we found the following variables to be statistically significant. Age (p = 0.019802), and TT polymorphism of the angiotensinogen (p = 0.001394). TT was significant for both for men (p = 0.039402) and women (p = 0.01518).
Because the study population at the time of recruiting had different periods of hemodialysis, and because it was not in Hardy–Weinberg equilibrium with regards to polymorphism of the angiotensinogen (p value < 0.0001), we decided to study those patients who had been on hemodialysis for up to one year at recruitment separately and compare the results of this subgroup with those of the total population. This cohort was more homogeneous with respect to length of disease, and comprised 82 patients. This cohort will be described, analyzed, and compared with the total population in another study.
DiscussionIn our study, there were very slightly more males (50.1%)
than females, which is in accordance with 2008 Census from the Brazilian Society of Nephrology. It found that men make up 57% of the population with end-stage chronic kidney disease1. A study in Bahia found a 56.6% of patients to be male9. A cross-sectional analysis conducted in six hemodialysis clinics in the State of Rio de Janeiro also found a higher proportion of men (56%)10.
The mean age of the study population was 46 years, which is lower than that found in a study in the State of Rio de Janeiro10 (54 years old), and also lower than another cross-sectional analysis conducted in a single dialysis center in the State of Rio de Janeiro, where the mean age was 52 years11. However, it was similar to the Bahia study9, which found a mean age of 49 years. In the 2010 Census from the Brazilian Society of Nephrology, 30.7% of the patients were aged 65 years or older4.
Table 2 – Laboratory data (biochemical and hematologic) at recruitment (July 97/July 98) of patients on HD
Laboratory variable Mean ± SD
Total cholesterol (mg/dL) 189.1 ± 43
HDL-cholesterol (mg/dL) 37.7 ± 12
Triglycerides (mg/dL) 184.6 ± 96
Hematocrits (%) 29.2% ± 4.9
HDL-cholesterol: High Density Lipoprotein; SD: Standard-deviation
213
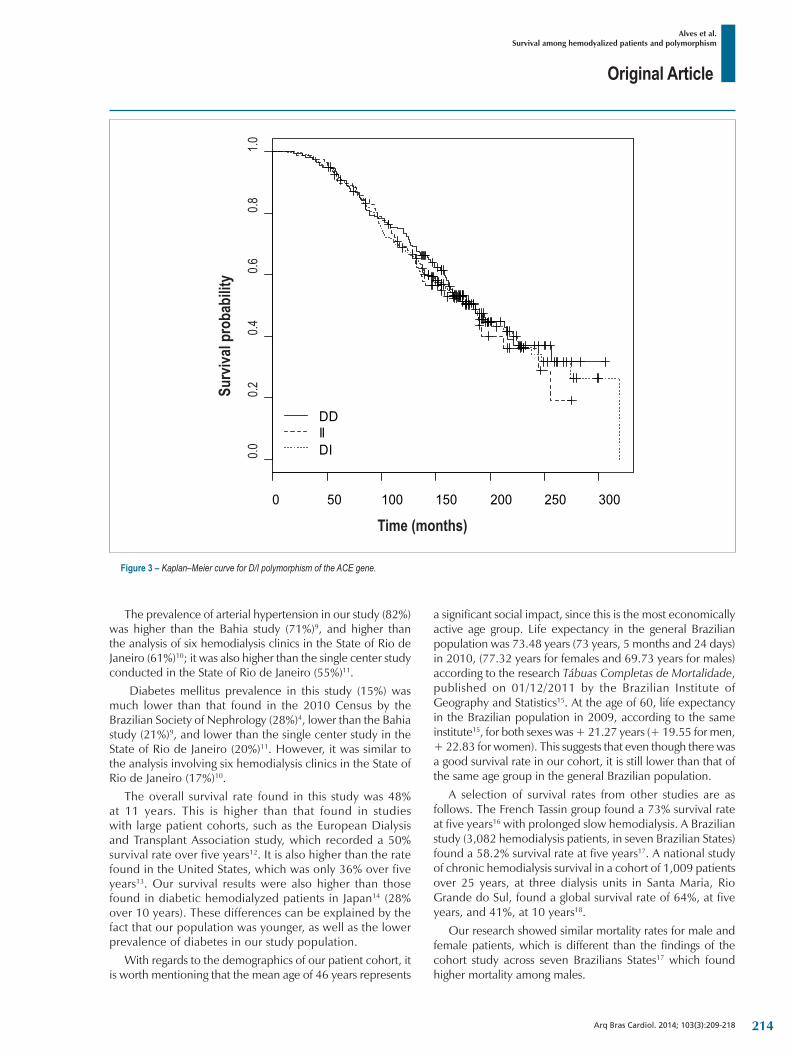
Original Article
Alves et al.Survival among hemodyalized patients and polymorphism
Arq Bras Cardiol. 2014; 103(3):209-218
Figure 3 – Kaplan–Meier curve for D/I polymorphism of the ACE gene.
0 50 100 150 200 250 300
0.0
0.2
0.4
0.6
0.8
1.0
Tempo (meses)
Pro
babi
lidad
e de
sob
revi
da
DDIIDI0.0
1.00.8
0.6
Time (months)
0.40.2Su
rviva
l pro
babi
lity
The prevalence of arterial hypertension in our study (82%) was higher than the Bahia study (71%)9, and higher than the analysis of six hemodialysis clinics in the State of Rio de Janeiro (61%)10; it was also higher than the single center study conducted in the State of Rio de Janeiro (55%)11.
Diabetes mellitus prevalence in this study (15%) was much lower than that found in the 2010 Census by the Brazilian Society of Nephrology (28%)4, lower than the Bahia study (21%)9, and lower than the single center study in the State of Rio de Janeiro (20%)11. However, it was similar to the analysis involving six hemodialysis clinics in the State of Rio de Janeiro (17%)10.
The overall survival rate found in this study was 48% at 11 years. This is higher than that found in studies with large patient cohorts, such as the European Dialysis and Transplant Association study, which recorded a 50% survival rate over five years12. It is also higher than the rate found in the United States, which was only 36% over five years13. Our survival results were also higher than those found in diabetic hemodialyzed patients in Japan14 (28% over 10 years). These differences can be explained by the fact that our population was younger, as well as the lower prevalence of diabetes in our study population.
With regards to the demographics of our patient cohort, it is worth mentioning that the mean age of 46 years represents
a significant social impact, since this is the most economically active age group. Life expectancy in the general Brazilian population was 73.48 years (73 years, 5 months and 24 days) in 2010, (77.32 years for females and 69.73 years for males) according to the research Tábuas Completas de Mortalidade, published on 01/12/2011 by the Brazilian Institute of Geography and Statistics15. At the age of 60, life expectancy in the Brazilian population in 2009, according to the same institute15, for both sexes was + 21.27 years (+ 19.55 for men, + 22.83 for women). This suggests that even though there was a good survival rate in our cohort, it is still lower than that of the same age group in the general Brazilian population.
A selection of survival rates from other studies are as follows. The French Tassin group found a 73% survival rate at five years16 with prolonged slow hemodialysis. A Brazilian study (3,082 hemodialysis patients, in seven Brazilian States) found a 58.2% survival rate at five years17. A national study of chronic hemodialysis survival in a cohort of 1,009 patients over 25 years, at three dialysis units in Santa Maria, Rio Grande do Sul, found a global survival rate of 64%, at five years, and 41%, at 10 years18.
Our research showed similar mortality rates for male and female patients, which is different than the findings of the cohort study across seven Brazilians States17 which found higher mortality among males.
214
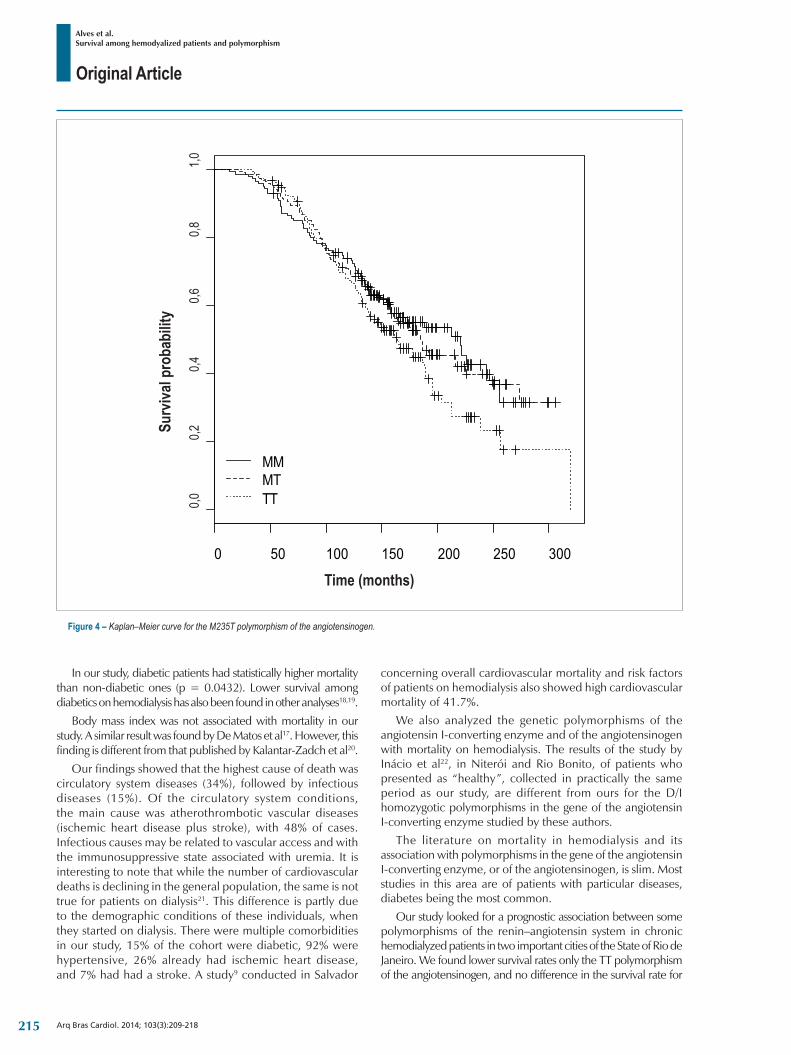
Original Article
Alves et al.Survival among hemodyalized patients and polymorphism
Arq Bras Cardiol. 2014; 103(3):209-218
Figure 4 – Kaplan–Meier curve for the M235T polymorphism of the angiotensinogen.
0 50 100 150 200 250 300
0.0
0.2
0.4
0.6
0.8
1.0
Tempo (meses)
Pro
babi
lidad
e de
sob
revi
da
MMMTTT0,0
1,00,8
0,60,4
0,2
Time (months)
Surv
ival p
roba
bilit
y
In our study, diabetic patients had statistically higher mortality than non-diabetic ones (p = 0.0432). Lower survival among diabetics on hemodialysis has also been found in other analyses18,19.
Body mass index was not associated with mortality in our study. A similar result was found by De Matos et al17. However, this finding is different from that published by Kalantar-Zadch et al20.
Our findings showed that the highest cause of death was circulatory system diseases (34%), followed by infectious diseases (15%). Of the circulatory system conditions, the main cause was atherothrombotic vascular diseases (ischemic heart disease plus stroke), with 48% of cases. Infectious causes may be related to vascular access and with the immunosuppressive state associated with uremia. It is interesting to note that while the number of cardiovascular deaths is declining in the general population, the same is not true for patients on dialysis21. This difference is partly due to the demographic conditions of these individuals, when they started on dialysis. There were multiple comorbidities in our study, 15% of the cohort were diabetic, 92% were hypertensive, 26% already had ischemic heart disease, and 7% had had a stroke. A study9 conducted in Salvador
concerning overall cardiovascular mortality and risk factors of patients on hemodialysis also showed high cardiovascular mortality of 41.7%.
We also analyzed the genetic polymorphisms of the angiotensin I-converting enzyme and of the angiotensinogen with mortality on hemodialysis. The results of the study by Inácio et al22, in Niteroi and Rio Bonito, of patients who presented as “healthy”, collected in practically the same period as our study, are different from ours for the D/I homozygotic polymorphisms in the gene of the angiotensin I-converting enzyme studied by these authors.
The literature on mortality in hemodialysis and its association with polymorphisms in the gene of the angiotensin I-converting enzyme, or of the angiotensinogen, is slim. Most studies in this area are of patients with particular diseases, diabetes being the most common.
Our study looked for a prognostic association between some polymorphisms of the renin–angiotensin system in chronic hemodialyzed patients in two important cities of the State of Rio de Janeiro. We found lower survival rates only the TT polymorphism of the angiotensinogen, and no difference in the survival rate for
215

Original Article
Alves et al.Survival among hemodyalized patients and polymorphism
Arq Bras Cardiol. 2014; 103(3):209-218
the D/I polymorphism of the angiotensin I-converting enzyme. Such results, showing a worse prognosis for the TT genotype, are similar to those found in analyses by Buraczynska et al23, Lovati et al24 and Miguel et al27. The differences found by the last two studies mentioned may have been due to the cohort being composed entirely of diabetics.
The study by Bzome et al25 was designed to assess arterial hypertension complications. There was no association found between D/I polymorphisms of the angiotensin I-converting enzyme and poorer outcomes, unlike the findings in studies by Sakka et al28, Losite et al29, van der Sman-de Beer et al30, Yoshida et al26, Perez-Oller et al31; Lovati et al24. These studies found decreasing survival rates for the DD genotype of the angiotensin I-converting enzyme, and many of them had short follow-up periods for a population of diabetics. Other studies32-34 did not find any association for polymorphisms of the angiotensin I-converting enzyme or of the angiotensinogen. These studies also had short follow-ups and were conducted in a specific population with diabetic nephropathy.
Study limitationsThe analysis of only two genetic polymorphisms in a highly
complex system, such as the renin–angiotensin system is a limiting factor. The absence of other important variables to analyze the survival among hemodialyzed patients, such as hemoglobin, calcium, vitamin D, parathormone, erythropoietin, phosphorus, C-reactive protein, and serum albumin can also be limiting, as was the lack of information about the associations and dosages of medicines used by these patients.
ConclusionsThe survival rate in our population was considered low
when compared to the general population of the same age group. However, the survival in this cohort was high
when compared to other studies involving Brazilian and North-American chronic hemodialyzed patients, as well as in comparison to most European studies. The main cause of death was circulatory system diseases, for both sexes, especially in older age groups, followed by infectious diseases and diabetes mellitus. In this study, it was not possible to demonstrate an association between polymorphisms in the gene that codifies the angiotensin I-converting enzyme (D/I) and mortality in hemodialyzed patients. The TT polymorphism of the M235 T angiotensinogen, age, and monthly family income were the variables that were associated with mortality in this cohort.
Author contributionsConception and design of the research: Alves M, Silva NAS,
Salis LHA; Acquisition of data: Alves M, Oliveira JMF; Analysis and interpretation of the data: Alves M, Silva NAS, Salis LHA, Godoy PH; Statistical analysis: Pereira BB, Nascimento EM; Writing of the manuscript: Alves M; Critical revision of the manuscript for intellectual content: Alves M, Silva NAS, Salis LHA, Oliveira JMF.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis article is part of the thesis of Doctoral submitted by
Mauro Alves, from Universidade Federal do Rio de Janeiro.
1. Sesso R, Lopes AA, Thome FS, Bevilacqua JL, Romão Junior JE, Lugon J. Relatorio do censo brasileiro de diálise, 2008. J Bras Nefrol. 2008;30(4):233-8.
2. National Institutes of Health (NIH). National Institutes of Diabetes and Digestive and Kidney Disease. U.S. Renal Data System. 2009 USRDS Annual Data Report. Bethesda. [Accessed on 2010 Feb 10]. Available from: htpp://www.usrds.org
3. Sesso RC, Lopes AA, Thome FS, Lugon JR, Burdmann EA. Brazilian dialysis census, 2009. J Bras Nefrol. 2010;32(4):374-8.
4. Sociedade Brasileira de Nefrologia, Censo 2010. [Acesso 2011 dez 20]. Disponível em: htpp://www.sbn.org.br/censo.asp
5. Silva Júnior AC, Lopes H, Lotaif LD, Amodeo C, Piegas LS. Novos fatores de risco cardiovascular. Rev Soc Cardiol Estado de São Paulo. 2007;17(1):50-9.
6. Canziane ME. Doenças cardiovasculares na doença renal crônica. J Bras Nefrol. 2005;26(supl. 1):20-1.
7. Romão Junior JE. Doença renal crônica: definição, epidemiologia e classificação. J Bras Nefrol. 2004;26(3 supl.1:1-5.
8. Sesso R, Gordon P. Dados disponíveis sobre a doença renal crônica no Brasil. J Bras Nefrol. 2007;29(1, supl. 1):9-12.
9. Almeida FA, Machado FC, Moura JA Jr, Guimarães AC. Mortalidade global e cardiovascular e fatores de risco de pacientes em hemodiálise. Arq Bras Cardiol. 2010;94(2):187-92, 201-6, 190-5.
10. Miguel JB, Strogoff de Matos JP, Ruzany F, Miguel CS, Miguel SJ, Naveiro LT, et al. Associação do índice tornozelo-braço com inflamação e alterações minerais osseas em pacientes em hemodiálise. Arq Bras Cardiol. 2011;96(5):405-9.
11. Miguel SB, Miguel JB, Velarde LG, Sampaio Ede A, Matos JP, Lugon JR. Prevalencia e correlatos de doença vascular no exame de ultrassom em pacientes em hemodiálise. Arq Bras Cardiol. 2011;96(4):260-5.
12. European Renal Association. European Dialysis and Transplant Association. ERA-EDTA Registry: ERA-EDTA Registry 2006 Annual Report. Academic Medical Center, Department of Medical Informatics, Amsterdam; 2008.
13. United States Renal Data System (US RDS) 2008. U.S. Renal Data System, USRDS 2008. Annual Data Report: Atlas of chronic kidney disease and end-stage renal disease in the United States. National Institutes of Health. (HIH); 2008.
References
216
Original Article
Alves et al.Survival among hemodyalized patients and polymorphism
Arq Bras Cardiol. 2014; 103(3):209-218
14. Imai E, Yamagata K, Iseki K, Iso H, Horio M, Mkino H, Hishida A, et al. Kidney disease screening program in Japan: history, outcome and perspectives. Clin J Am Soc Nephrol. 2007;2(6):1360-6.
15. Instituto Brasileiro de Geografia e Estatística. (IBGE). Tábuas Completas de Mortalidade. [Acesso em 2012 jan 6]. Disponível: http://www.ibge.gov.br
16. Innes A, Charra B, Burden RP, Morgan AG, Laurent G. The effect of long, slow haemodialysis on patient survival. Nephrol Dial Transplant. 1999;14(4):919-22.
17. De Matos JP, Almeida JR, Guinsburg A, Marelli C, Barra AB, Vasconcellos MS, et al. Avaliação da sobrevida de cinco anos em hemodiálise no Brasil: uma coorte de 3.082 pacientes incidentes. J Bras Nefrol. 2011;33(4):436-41.
18. Da Silva LA, Mezzomo NF, Pansard HM, Arantes LC, Rempel W, Argenta LC, et al. Sobrevida em hemodiálise crônica: estudo de uma coorte de 1.009 pacientes em 25 anos. J Bras Nefrol. 2009;31(3):190-7.
19. Peres LA, Matsuo T, Delfino VD, Peres CP, Almeida Netto JH, Ann HK, et al. [Increase in prevalence of diabetes mellitus as a cause of dialytic end-stage renal disease: analysis of 20 years in the west regional of Paraná]. Arq Bras Endocrinol Metabol. 2007;51(1):111-5.
20. Kalantar-Zadch K, Streja E, Kovesdy CP, Oreopoulos A, Noori N, Jing J, et al. The obesity paradox and mortality associated with surrogates of body size and muscle mass in patients receiving hemodialysis. Mayo Clin Proc. 2010;85(11):991-1001.
21. Mailloux LU, Henrich WL. Patient survival and maintenance dialysis. Up To Date, 2005. [Access in 2011 Mar 20]. Available from: http://www.uptodate.com/subscribers/tutorial/index.asp
22. Inácio J, Goulart Filho LR, Vieira GS. Frequencia genotípica e alelicas do gene do polimorfismo da ECA I/D na população brasileira. Biosci J. 2004;20(1):47-51.
23. Buraczynska M, Ksiazek P, Drop A, Zaluska W, Spasiewicz D, Ksiazek A. Genetic polymorphisms of the renin-angiotensin system in end-stage renal disease. Nephrol Dial Transplant. 2006;21(4):979-83.
24. Lovati E, Richard A, Frey BM, Frey FJ, Ferrari P. Genetic polymorphisms of the renin-angiotensin-aldosterone system in end-stage renal disease. Kidney Int. 2001;60(1):46-54.
25. Bzoma B, Debska-Slizień A, Dudziak M, Raczyńska K, Slizień W, Brylowska A, et al. [Genetic predisposition to systemic complications of arterial hypertension in maintenance haemodialysis patients]. Pol Merkur Lekarski. 2008;25(147):209-16.
26. Yoshida H, Kuriyama S, Atsumi Y, Tomonari H, Mitarai T, Hamaguchi A, et al. Angiotensin I converting enzyme gene polymorphism in non-insulin dependent diabetes mellitus. Kidney Int. 1996;50(2):657-64.
27. Padro-Miguel A, Alía-Ramos P, González-Alvarez MT, Navarro-Moreno MA. Survival in type 2 diabetic patient in dialysis and the number of risk alleles in polymorphisms of the renin-angiotensin system genes. Clin Biochem. 2009;42(1-2):5-11.
28. Sakka Y, Babazono T, Sato A, Ujihara N, Iwamoto Y. ACE gene polymorphism, left ventricular geometry, and mortality in diabetic patients with end-stage renal disease. Diabetes Res Clin Pract. 2004;64(1):41-9.
29. Losito A, Parente B, Cao PG, Jeffery S, Afzal AR. ACE gene polymorphism and survival in atherosclerotic renovascular disease. Am J Kidney Dis. 2000;35(2):211-5.
30. van der Sman-de Beer F, Verhagen C, Rombach SM, Boorsma P, van Manen JG, Korevaar JC, et al; NECOSAD Study Group. ACE I/D is associated with mortality in a cohort study of patients starting with dialysis. Kidney Int. 2005;68(5):2237-43.
31. Perez-Oller L, Torra R, Badenas C, Milà M, Darnell A. Influence of the ACE gene polymorphism in the progression of renal failure in autosomal dominant polycystic kidney disease. Am J Kidney Dis. 1999;34(2):273-8.
32. Aucella F, Margaglione M, Vigilante M, Gatta G, Grandone E, Forcella M, et al. PAI-1 4G/5G and ACE I/D gene polymorphisms and the occurrence of myocardial infarction in patients on intermittent dialysis. Nephrol Dial Transplant. 2003;18(6):1142-6.
33. Wetmore JB, Johansen KL, Sen S, Hung AM, Lovett DH. An angiotensin converting enzyme haplotype predicts survival in patients with end stage renal disease. Hum Genet. 2006;120(2):201-10.
34. Higashiuesato Y, Tana T, Tozawa M, Iseki C, Iseki K, Fukiyama K, et al. Angiotensin-converting enzyme (ACE) insertion/deletion polymorphism and survival in a cohort of chronic hemodialysis patients. Clin Nephrol. 2002;58(5):370-5.
217

Original Article
Alves et al.Survival among hemodyalized patients and polymorphism
Arq Bras Cardiol. 2014; 103(3):209-218 218
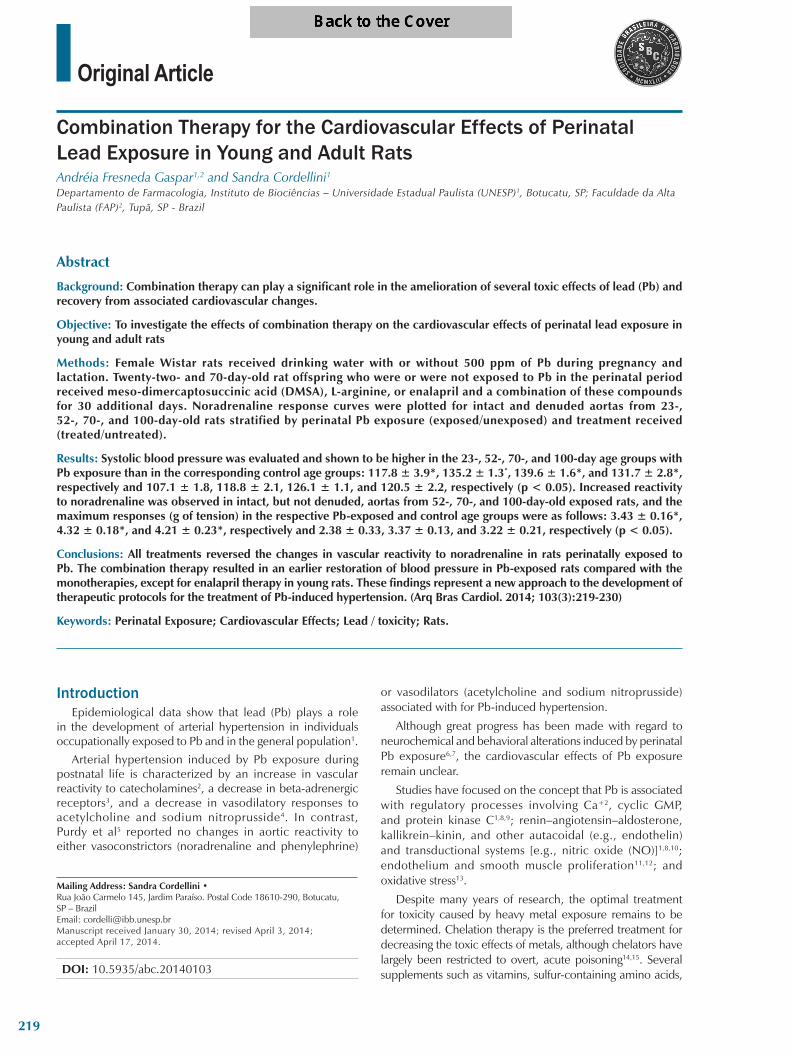
Original Article
Combination Therapy for the Cardiovascular Effects of Perinatal Lead Exposure in Young and Adult RatsAndreia Fresneda Gaspar1,2 and Sandra Cordellini1Departamento de Farmacologia, Instituto de Biociências – Universidade Estadual Paulista (UNESP)1, Botucatu, SP; Faculdade da Alta Paulista (FAP)2, Tupã, SP - Brazil
Mailing Address: Sandra Cordellini •Rua João Carmelo 145, Jardim Paraíso. Postal Code 18610-290, Botucatu, SP – BrazilEmail: [email protected] received January 30, 2014; revised April 3, 2014; accepted April 17, 2014.
DOI: 10.5935/abc.20140103
Abstract
Background: Combination therapy can play a significant role in the amelioration of several toxic effects of lead (Pb) and recovery from associated cardiovascular changes.
Objective: To investigate the effects of combination therapy on the cardiovascular effects of perinatal lead exposure in young and adult rats
Methods: Female Wistar rats received drinking water with or without 500 ppm of Pb during pregnancy and lactation. Twenty-two- and 70-day-old rat offspring who were or were not exposed to Pb in the perinatal period received meso-dimercaptosuccinic acid (DMSA), L-arginine, or enalapril and a combination of these compounds for 30 additional days. Noradrenaline response curves were plotted for intact and denuded aortas from 23-, 52-, 70-, and 100-day-old rats stratified by perinatal Pb exposure (exposed/unexposed) and treatment received (treated/untreated).
Results: Systolic blood pressure was evaluated and shown to be higher in the 23-, 52-, 70-, and 100-day age groups with Pb exposure than in the corresponding control age groups: 117.8 ± 3.9*, 135.2 ± 1.3*, 139.6 ± 1.6*, and 131.7 ± 2.8*, respectively and 107.1 ± 1.8, 118.8 ± 2.1, 126.1 ± 1.1, and 120.5 ± 2.2, respectively (p < 0.05). Increased reactivity to noradrenaline was observed in intact, but not denuded, aortas from 52-, 70-, and 100-day-old exposed rats, and the maximum responses (g of tension) in the respective Pb-exposed and control age groups were as follows: 3.43 ± 0.16*, 4.32 ± 0.18*, and 4.21 ± 0.23*, respectively and 2.38 ± 0.33, 3.37 ± 0.13, and 3.22 ± 0.21, respectively (p < 0.05).
Conclusions: All treatments reversed the changes in vascular reactivity to noradrenaline in rats perinatally exposed to Pb. The combination therapy resulted in an earlier restoration of blood pressure in Pb-exposed rats compared with the monotherapies, except for enalapril therapy in young rats. These findings represent a new approach to the development of therapeutic protocols for the treatment of Pb-induced hypertension. (Arq Bras Cardiol. 2014; 103(3):219-230)
Keywords: Perinatal Exposure; Cardiovascular Effects; Lead / toxicity; Rats.
IntroductionEpidemiological data show that lead (Pb) plays a role
in the development of arterial hypertension in individuals occupationally exposed to Pb and in the general population1.
Arterial hypertension induced by Pb exposure during postnatal life is characterized by an increase in vascular reactivity to catecholamines2, a decrease in beta-adrenergic receptors3, and a decrease in vasodilatory responses to acetylcholine and sodium nitroprusside4. In contrast, Purdy et al5 reported no changes in aortic reactivity to either vasoconstrictors (noradrenaline and phenylephrine)
or vasodilators (acetylcholine and sodium nitroprusside) associated with for Pb-induced hypertension.
Although great progress has been made with regard to neurochemical and behavioral alterations induced by perinatal Pb exposure6,7, the cardiovascular effects of Pb exposure remain unclear.
Studies have focused on the concept that Pb is associated with regulatory processes involving Ca+2, cyclic GMP, and protein kinase C1,8,9; renin–angiotensin–aldosterone, kallikrein–kinin, and other autacoidal (e.g., endothelin) and transductional systems [e.g., nitric oxide (NO)]1,8,10; endothelium and smooth muscle proliferation11,12; and oxidative stress13.
Despite many years of research, the optimal treatment for toxicity caused by heavy metal exposure remains to be determined. Chelation therapy is the preferred treatment for decreasing the toxic effects of metals, although chelators have largely been restricted to overt, acute poisoning14,15. Several supplements such as vitamins, sulfur-containing amino acids,
219

Original Article
Fresneda-Gaspar & CordelliniCombination therapy for Pb cardiovascular effects
Arq Bras Cardiol. 2014; 103(3):219-230
antioxidants, and essential minerals are also used to address metal toxicity15. Combination therapy is a novel and better approach to the treatment of metal poisoning14,15. Because little experimental evidence is available, there is a requirement for in-depth investigations in this field.
On the basis of the abovementioned reports, we investigated combination therapies for the treatment of Pb-induced cardiovascular toxicity. The effects of maternal Pb exposure during pregnancy and lactation on blood pressure and aortic reactivity were investigated in young and adult rat offspring, with focus on endothelial and smooth muscle cells. We then evaluated the therapeutic effects of the following drugs administered either alone or in combination on the adverse cardiovascular effects of perinatal Pb exposure in young and adult rats: meso-dimercaptosuccinic acid (DMSA), a chelating agent and scavenger of reactive oxygen species (ROS)16,17; L-arginine, a precursor of NO18; and enalapril, an angiotensin-converting enzyme inhibitor.
Methods
Animals and Pb exposure Adult Wistar rats were obtained from University of São
Paulo facilities and used as the parent generation. The animals were mated at the age of 90 days (two females and one male per cage). On pregnancy day 0 (determined by the presence of sperm in vaginal smears), the females were divided into nonexposed and Pb-exposed groups and were housed alone. The drinking water in the cages housing the females was altered with 500 ppm Pb (as Pb acetate) or tap water. A group of animals received sodium acetate to equalize acetate exposure between groups. The Pb exposure regimen was chosen on the basis of previous studies6,7,19. To prevent the formation of a Pb precipitate, 0.5 mL of glacial acetic acid was added while stirring to 1000 mL of each solution (sodium acetate and Pb). Pb exposure lasted throughout pregnancy and lactation (Figure 1). At birth, the number of pups per litter was recorded, following which all litters were culled to eight pups. Whenever possible, only male rats were kept within the litter, and females were kept just to maintain equal litter sizes. Pups were weaned at 22 days of age on tap water and evaluated at 23 and 70 days of age (Figure 1). Age-matched controls received sodium acetate during the same periods as that of Pb exposure. Maternal body weights were measured on pregnancy day 0, the day before delivery, after delivery, and at weaning. Pup weights were recorded at birth and weekly until 100 days of age.
Lights in the animal room were set on a 12:12-h light-dark cycle, with the temperature maintained at 22 ± 1°C. The animals were fed with regular laboratory chow. Animal procedures were performed in accordance with the principles and guidelines of the National Council for Control of Animal Experimentation (protocol no. 25/05-CEEA).
Measurement of blood pressureBeginning at 22 days of life, systolic blood pressure was
determined weekly in conscious rats using the tail-cuff plethysmographic method (Narco Bio-Systems, Inc.,
Houston, TX). The rats were prewarmed for approximately 10 min and placed into a restrainer for blood pressure measurement. Three consecutive recordings (approximately 1 min apart) were obtained, and the mean of these three measurements was recorded.
Determination of Pb levels in bloodWhole blood was collected from the hearts of anesthetized
(urethane, 1.25 g/kg) female rats at weaning and pups at 23, 52, 70, and 100 days of age.
Blood was prepared for Pb analysis, which was conducted using a microwave dissolution procedure utilizing a DGT-100 plus microwave digestion apparatus (Provecto, Brazil). Nitric acid was added to the digestion vessels containing 1 mL of blood.
Pb levels in whole blood were determined using an atomic absorption spectrophotometer GBC AA 932 (EEA-flame)20. The recovery of Pb that was externally added to control samples was found to be consistently greater than 96%. A standard addition method was applied during determination to eliminate possible matrix interference. Whole-blood Pb levels were expressed in micrograms per deciliter. The detection limit was 5 µg/dL.
TherapyA group of 22- and 70-day-old rats who were or
were not exposed to Pb in the perinatal period received DMSA, L-arginine, enalapril, or the combination of these compounds for 30 additional days (Figure 1). DMSA was orally administered at 60 mg/kg by gastric gavage two times a day (30 mg/kg per dose) for 5 days a week. L-arginine (1.0%) was administered through drinking water consumed ad libitum. Enalapril was also administered through drinking water (approximately 5 mg/day/rat). Age-matched controls received tap water.
Experimental protocolsImmediately after the blood samples were collected, the
thoracic aorta was excised and trimmed free of adhering fat and connective tissue. Two transverse rings measuring approximately 4 mm in length were cut and mounted at the optimal length for recording isometric tension in organ chambers. One ring served as a control, while the endothelium was mechanically removed from the other by gently rubbing the luminal surface. These samples constituted the intact and denuded aortas, respectively. The organ baths contained Krebs–Henseleit solution (7 mL) comprising (in mM) NaCl (113.0), KCl (4.7), CaCl2 (2.5), NaHCO3 (25.0), MgSO4 (1.1), KH2PO4 (1.2), ascorbic acid (0.11), and glucose (11.1). The bathing fluid was maintained at 37oC and was saturated with a gas mixture of 95% O2 and 5% CO2. The preparations were allowed to equilibrate for at least an hour under a resting tension of 1.5 g, which is optimal for inducing maximum contraction. Tension was recorded using an F-60 microdisplacement myograph (Narco Bio-Systems Inc., Houston, Texas, USA) and displayed on a physiograph. Intact and denuded aortas from rats who were or were not exposed to Pb were studied in parallel.
220
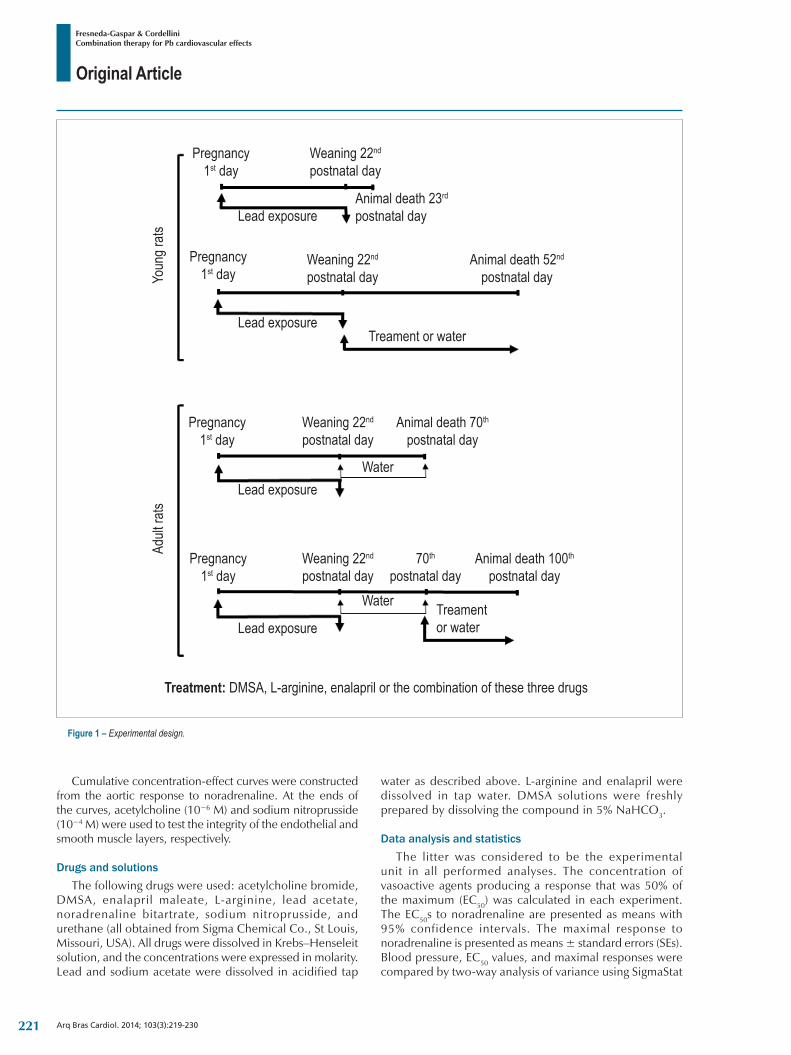
Original Article
Fresneda-Gaspar & CordelliniCombination therapy for Pb cardiovascular effects
Arq Bras Cardiol. 2014; 103(3):219-230
Cumulative concentration-effect curves were constructed from the aortic response to noradrenaline. At the ends of the curves, acetylcholine (10−6 M) and sodium nitroprusside (10−4 M) were used to test the integrity of the endothelial and smooth muscle layers, respectively.
Drugs and solutionsThe following drugs were used: acetylcholine bromide,
DMSA, enalapril maleate, L-arginine, lead acetate, noradrenaline bitartrate, sodium nitroprusside, and urethane (all obtained from Sigma Chemical Co., St Louis, Missouri, USA). All drugs were dissolved in Krebs–Henseleit solution, and the concentrations were expressed in molarity. Lead and sodium acetate were dissolved in acidified tap
water as described above. L-arginine and enalapril were dissolved in tap water. DMSA solutions were freshly prepared by dissolving the compound in 5% NaHCO3.
Data analysis and statisticsThe litter was considered to be the experimental
unit in all performed analyses. The concentration of vasoactive agents producing a response that was 50% of the maximum (EC50) was calculated in each experiment. The EC50s to noradrenaline are presented as means with 95% confidence intervals. The maximal response to noradrenaline is presented as means ± standard errors (SEs). Blood pressure, EC50 values, and maximal responses were compared by two-way analysis of variance using SigmaStat
Figure 1 – Experimental design.
Youn
g rats
Adult
rats
Pregnancy 1st day
Pregnancy 1st day
Pregnancy 1st day
Pregnancy 1st day
Weaning 22nd
postnatal day
Weaning 22nd
postnatal day
Weaning 22nd postnatal day
Weaning 22nd postnatal day
Animal death 70th postnatal day
70th postnatal day
Animal death 100th
postnatal day
Animal death 23rd
postnatal day
Animal death 52nd postnatal day
Leadexposure
Leadexposure
Leadexposure
Leadexposure
Treamentorwater
Treament orwater
Water
Water
Treatment: DMSA, L-arginine, enalapril or the combination of these three drugs
221

Original Article
Fresneda-Gaspar & CordelliniCombination therapy for Pb cardiovascular effects
Arq Bras Cardiol. 2014; 103(3):219-230
3.2 software. Pb and treatment were the factors included in the analysis. A P-value of <0.05 was considered statistically significant. Tukey’s multiple comparisons test was used to test differences among means. Other parameters (body weight, number of pups, and Pb determination) are also presented as means ± standard errors and were compared using the Mann–Whitney test, which was conducted using InStat 4.0 software.
Results
Body weight, number of pups, blood Pb levels, and blood pressure
Pb exposure did not affect the body weight of the mothers and pups (Table 1) as well as the number of pups per litter (control: 11.3 ± 0.4, Pb: 10.5 ± 0.5, p > 0.05; number of litters per group, 10–20).
Pb levels in blood samples from the mothers and the 23-, 52-, 70- and 100-day-old rats were significantly higher than those in the respective controls (Table 2). After Pb discontinuation, the blood Pb levels in exposed rats decreased but remained higher than those in control rats (Table 2). The different treatment protocols resulted in a significant decrease in blood Pb levels in the 52- and 100-day-old rats (Table 2). These decreases reached values similar to those observed in control rats of the same age, except in rats treated with L-arginine, in which blood Pb levels remained high compared with those in controls (Table 2).
Systolic blood pressure was not altered by sodium acetate exposure compared with those after tap water exposure (data not shown). Systolic blood pressure showed a gradual increase during postnatal development (Figures 2 and 3). Moreover, the values observed in Pb-exposed rats were significantly higher than those in controls (Figures 2 and 3).
All treatments decreased the blood pressure of Pb-exposed young rats to levels near those in unexposed animals. This reversal in blood pressure occurred at the age of 49, 35, 28, and 28 days, respectively, with L-arginine, DMSA, enalapril, and combination therapy (Figure 2). Similar reversals in blood pressure were observed in Pb-exposed adult rats treated with L-arginine, enalapril, and combination therapy at the age of 84, 84, and 77 days, respectively (Figure 3). Although DMSA treatment decreased blood pressure in Pb-exposed adult rats, this value was similar to that observed in both unexposed and Pb-exposed untreated rats (Figure 3).
Vascular reactivityThe reactivity of intact and denuded aortas in Pb-exposed
rats was not altered by sodium acetate exposure compared with that in aortas from rats that received tap water (data not shown). Gavage did not cause any change in aortic reactivity (data not shown). Neither Pb exposure nor the treatments altered the reactivity of denuded aortas to noradrenaline (Tables 3 and 4).
Removal of the endothelium caused a leftward shift of the noradrenaline response curve, which was similar in aortas from both controls and Pb-exposed rats, irrespective of treatment received or not (Tables 3 and 4). This procedure also resulted
in an increase in the maximum response to noradrenaline in aortas from different experimental groups (Tables 3 and 4). After removal of the endothelium, the maximum response to noradrenaline was similar in the aortas from all experimental groups (Tables 3 and 4).
With regard to intact aortas, no change was observed in the maximum response to noradrenaline in 23-day-old pups exposed to Pb in the perinatal period (Table 3). In contrast, an increase in the reactivity of intact aortas was observed in 52-, 70-, and 100-day-old rats exposed to Pb in the perinatal period (Table 3). Independent of the protocol, the noradrenaline sensitivity of aortas with intact endothelium did not differ (Tables 3 and 4).
The different treatments did not alter the reactivity of intact aortas from nonintoxicated rats to noradrenaline (Tables 3 and 4). However, L-arginine, DMSA, enalapril, and combination therapy were effective in decreasing the Pb-induced increase in maximum aortic response to levels similar to those in the respective controls (Tables 3 and 4).
Discussion Public health authorities use high levels to define blood Pb
levels of concern in nonpregnant women, with 40 µg/dL being the adult reference value in many countries.
We must recognize that a significant proportion of nonpregnant women with blood Pb levels ≥ 40 µg/dL can become pregnant and potentially expose their infants to the risk of adverse health effects caused by Pb21. Maternal and fetal blood Pb levels are nearly identical because Pb crosses the placenta unencumbered. This has provoked a concern about increased blood Pb levels among all females of childbearing age because a great proportion of pregnancies are unplanned. Finally, pregnant women without symptoms frequently remain in contact with the source of exposure during pregnancy and lactation, particularly in developing countries.
The severity of effects and the extent to which the cardiovascular system is affected by Pb appear to be influenced most directly by Pb levels, duration of Pb exposure, and other factors such as the route of exposure and individual life phase22,23. In the present work, we investigated cardiovascular alterations in rats exposed to Pb in utero and during lactation that were born to females with blood Pb levels of approximately 50 µg/dL. The Pb exposure regimen had no effect on the weight of the females and the pups at birth, at weaning, and during postnatal life or on the number of pups per litter. All animals appeared healthy, and none showed signs of toxicity.
However, the Pb exposure protocol resulted in an increase in systolic blood pressure in association with changes in vascular reactivity. The sustained increase in blood pressure observed in weaned, young and adult rats perinatally exposed to Pb confirms the results of previous reports that showed a positive association between blood Pb levels and arterial hypertension23,24.
Investigation of the manner in which Pb affects vascular endothelial and smooth muscle cells was the goal of the present study. Changes in the balance of endothelial contracting and
222
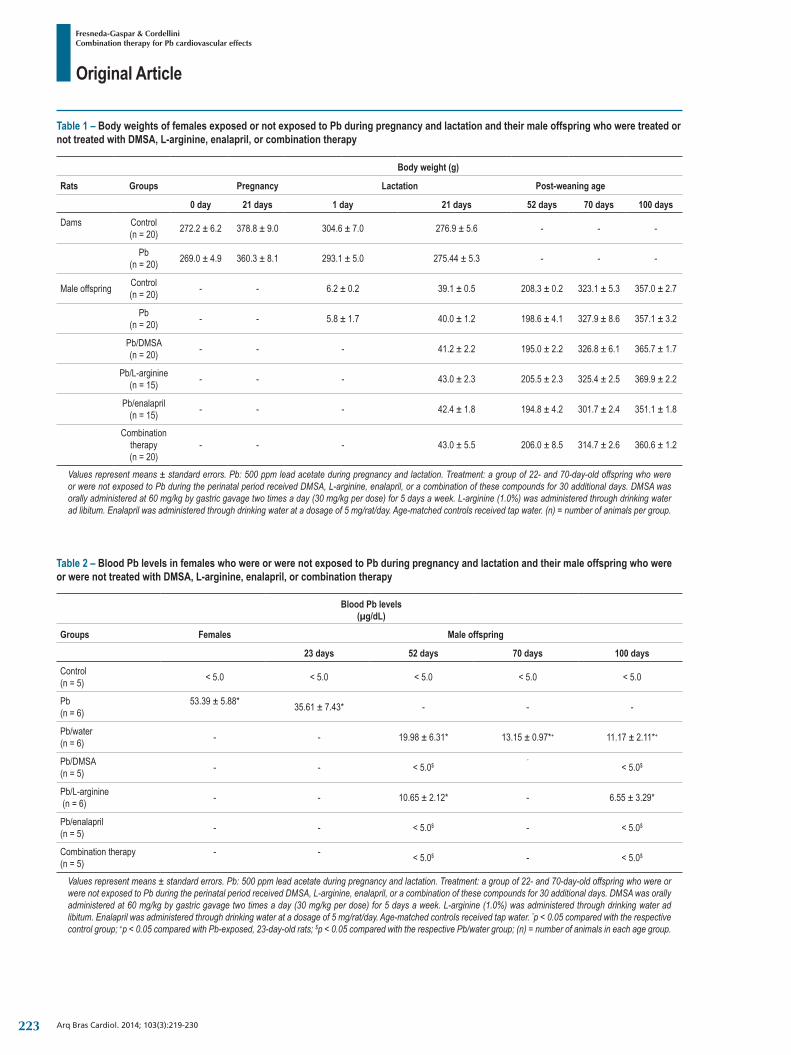
Original Article
Fresneda-Gaspar & CordelliniCombination therapy for Pb cardiovascular effects
Arq Bras Cardiol. 2014; 103(3):219-230
Table 1 – Body weights of females exposed or not exposed to Pb during pregnancy and lactation and their male offspring who were treated or not treated with DMSA, L-arginine, enalapril, or combination therapy
Body weight (g)
Rats Groups Pregnancy Lactation Post-weaning age
0 day 21 days 1 day 21 days 52 days 70 days 100 days
Dams Control(n = 20) 272.2 ± 6.2 378.8 ± 9.0 304.6 ± 7.0 276.9 ± 5.6 - - -
Pb(n = 20) 269.0 ± 4.9 360.3 ± 8.1 293.1 ± 5.0 275.44 ± 5.3 - - -
Male offspring Control(n = 20) - - 6.2 ± 0.2 39.1 ± 0.5 208.3 ± 0.2 323.1 ± 5.3 357.0 ± 2.7
Pb(n = 20) - - 5.8 ± 1.7 40.0 ± 1.2 198.6 ± 4.1 327.9 ± 8.6 357.1 ± 3.2
Pb/DMSA(n = 20) - - - 41.2 ± 2.2 195.0 ± 2.2 326.8 ± 6.1 365.7 ± 1.7
Pb/L-arginine(n = 15) - - - 43.0 ± 2.3 205.5 ± 2.3 325.4 ± 2.5 369.9 ± 2.2
Pb/enalapril(n = 15) - - - 42.4 ± 1.8 194.8 ± 4.2 301.7 ± 2.4 351.1 ± 1.8
Combination therapy(n = 20)
- - - 43.0 ± 5.5 206.0 ± 8.5 314.7 ± 2.6 360.6 ± 1.2
Values represent means ± standard errors. Pb: 500 ppm lead acetate during pregnancy and lactation. Treatment: a group of 22- and 70-day-old offspring who were or were not exposed to Pb during the perinatal period received DMSA, L-arginine, enalapril, or a combination of these compounds for 30 additional days. DMSA was orally administered at 60 mg/kg by gastric gavage two times a day (30 mg/kg per dose) for 5 days a week. L-arginine (1.0%) was administered through drinking water ad libitum. Enalapril was administered through drinking water at a dosage of 5 mg/rat/day. Age-matched controls received tap water. (n) = number of animals per group.
Table 2 – Blood Pb levels in females who were or were not exposed to Pb during pregnancy and lactation and their male offspring who were or were not treated with DMSA, L-arginine, enalapril, or combination therapy
Blood Pb levels(µg/dL)
Groups Females Male offspring
23 days 52 days 70 days 100 days
Control(n = 5) < 5.0 < 5.0 < 5.0 < 5.0 < 5.0
Pb(n = 6)
53.39 ± 5.88* 35.61 ± 7.43* - - -
Pb/water(n = 6) - - 19.98 ± 6.31* 13.15 ± 0.97*+ 11.17 ± 2.11*+
Pb/DMSA(n = 5) - - < 5.0$
-< 5.0$
Pb/L-arginine (n = 6) - - 10.65 ± 2.12* - 6.55 ± 3.29*
Pb/enalapril(n = 5) - - < 5.0$ - < 5.0$
Combination therapy(n = 5)
- - < 5.0$ - < 5.0$
Values represent means ± standard errors. Pb: 500 ppm lead acetate during pregnancy and lactation. Treatment: a group of 22- and 70-day-old offspring who were or were not exposed to Pb during the perinatal period received DMSA, L-arginine, enalapril, or a combination of these compounds for 30 additional days. DMSA was orally administered at 60 mg/kg by gastric gavage two times a day (30 mg/kg per dose) for 5 days a week. L-arginine (1.0%) was administered through drinking water ad libitum. Enalapril was administered through drinking water at a dosage of 5 mg/rat/day. Age-matched controls received tap water. *p < 0.05 compared with the respective control group; +p < 0.05 compared with Pb-exposed, 23-day-old rats; $p < 0.05 compared with the respective Pb/water group; (n) = number of animals in each age group.
223
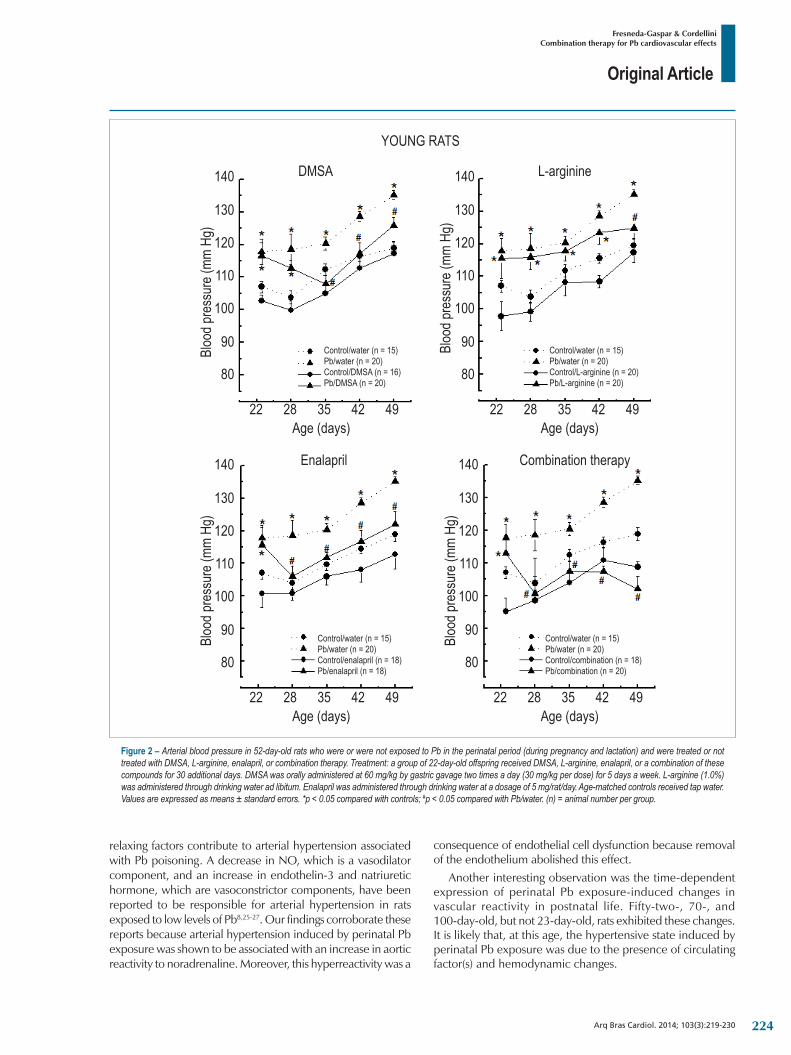
Original Article
Fresneda-Gaspar & CordelliniCombination therapy for Pb cardiovascular effects
Arq Bras Cardiol. 2014; 103(3):219-230
relaxing factors contribute to arterial hypertension associated with Pb poisoning. A decrease in NO, which is a vasodilator component, and an increase in endothelin-3 and natriuretic hormone, which are vasoconstrictor components, have been reported to be responsible for arterial hypertension in rats exposed to low levels of Pb8,25-27. Our findings corroborate these reports because arterial hypertension induced by perinatal Pb exposure was shown to be associated with an increase in aortic reactivity to noradrenaline. Moreover, this hyperreactivity was a
consequence of endothelial cell dysfunction because removal of the endothelium abolished this effect.
Another interesting observation was the time-dependent expression of perinatal Pb exposure-induced changes in vascular reactivity in postnatal life. Fifty-two-, 70-, and 100-day-old, but not 23-day-old, rats exhibited these changes. It is likely that, at this age, the hypertensive state induced by perinatal Pb exposure was due to the presence of circulating factor(s) and hemodynamic changes.
Figure 2 – Arterial blood pressure in 52-day-old rats who were or were not exposed to Pb in the perinatal period (during pregnancy and lactation) and were treated or not treated with DMSA, L-arginine, enalapril, or combination therapy. Treatment: a group of 22-day-old offspring received DMSA, L-arginine, enalapril, or a combination of these compounds for 30 additional days. DMSA was orally administered at 60 mg/kg by gastric gavage two times a day (30 mg/kg per dose) for 5 days a week. L-arginine (1.0%) was administered through drinking water ad libitum. Enalapril was administered through drinking water at a dosage of 5 mg/rat/day. Age-matched controls received tap water. Values are expressed as means ± standard errors. *p < 0.05 compared with controls; #p < 0.05 compared with Pb/water. (n) = animal number per group.
YOUNG RATS
Bloo
d pre
ssur
e (mm
Hg)
Bloo
d pre
ssur
e (mm
Hg)
Bloo
d pre
ssur
e (mm
Hg)
Bloo
d pre
ssur
e (mm
Hg)
DMSA140 140
140140
130 130
130130
120 120
120120
110 110
110110
100 100
100100
90 90
9090
80 80
8080
22 22
2222
28 28
2828
35 35
3535
42 42
4242
49 49
4949
L-arginine
Control/water(n=15)
Control/water(n=15)
Control/water(n=15)
Control/water(n=15)
Pb/water(n=20)
Pb/water(n=20)
Pb/water(n=20)
Pb/water(n=20)
Control/L-arginine (n = 20)
Control/combination (n = 18)
Control/DMSA (n = 16)
Control/enalapril (n = 18)
Pb/L-arginine (n = 20)
Pb/combination (n = 20)
Pb/DMSA (n = 20)
Pb/enalapril (n = 18)
Enalapril Combination therapy
Age (days)
Age (days)
Age (days)
Age (days)
224
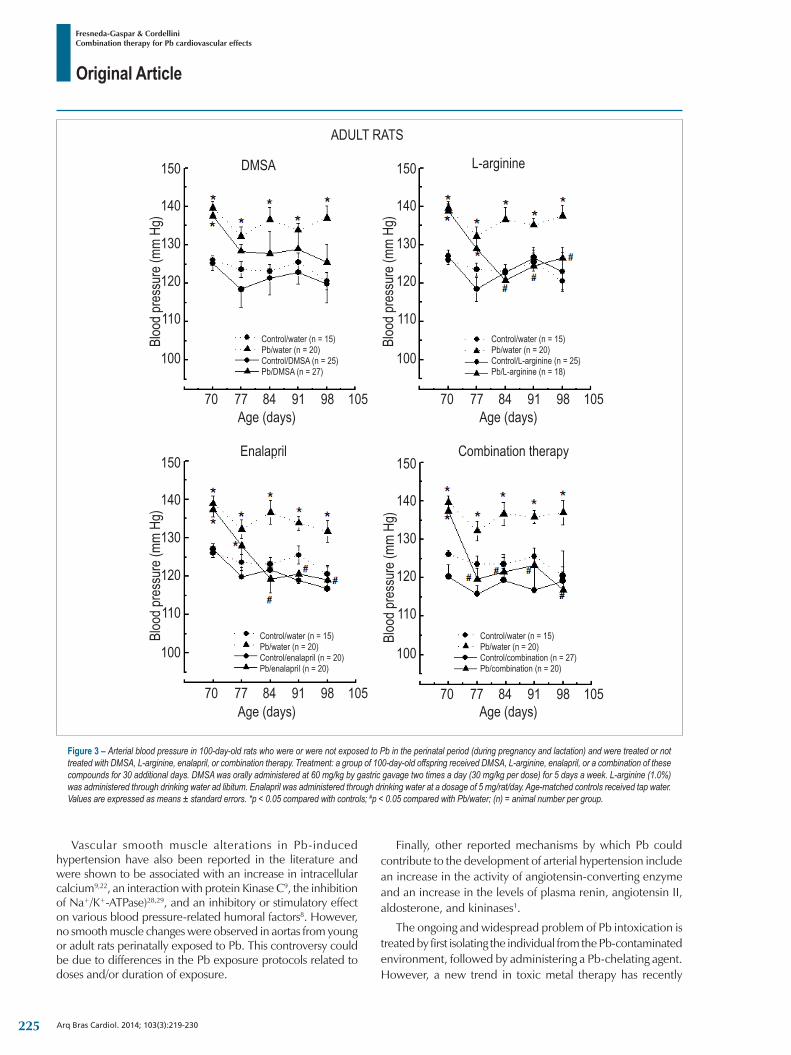
Original Article
Fresneda-Gaspar & CordelliniCombination therapy for Pb cardiovascular effects
Arq Bras Cardiol. 2014; 103(3):219-230
Vascular smooth muscle alterations in Pb-induced hypertension have also been reported in the literature and were shown to be associated with an increase in intracellular calcium9,22, an interaction with protein Kinase C9, the inhibition of Na+/K+-ATPase)28,29, and an inhibitory or stimulatory effect on various blood pressure-related humoral factors8. However, no smooth muscle changes were observed in aortas from young or adult rats perinatally exposed to Pb. This controversy could be due to differences in the Pb exposure protocols related to doses and/or duration of exposure.
Finally, other reported mechanisms by which Pb could contribute to the development of arterial hypertension include an increase in the activity of angiotensin-converting enzyme and an increase in the levels of plasma renin, angiotensin II, aldosterone, and kininases1.
The ongoing and widespread problem of Pb intoxication is treated by first isolating the individual from the Pb-contaminated environment, followed by administering a Pb-chelating agent. However, a new trend in toxic metal therapy has recently
Figure 3 – Arterial blood pressure in 100-day-old rats who were or were not exposed to Pb in the perinatal period (during pregnancy and lactation) and were treated or not treated with DMSA, L-arginine, enalapril, or combination therapy. Treatment: a group of 100-day-old offspring received DMSA, L-arginine, enalapril, or a combination of these compounds for 30 additional days. DMSA was orally administered at 60 mg/kg by gastric gavage two times a day (30 mg/kg per dose) for 5 days a week. L-arginine (1.0%) was administered through drinking water ad libitum. Enalapril was administered through drinking water at a dosage of 5 mg/rat/day. Age-matched controls received tap water. Values are expressed as means ± standard errors. *p < 0.05 compared with controls; #p < 0.05 compared with Pb/water; (n) = animal number per group.
150
150
150
150
140
140
140
140
130
130
130
130
120
120
120
120
110
110
110
110
100
100
100
100
70
70
70
70
77
77
77
77
84
84
84
84
91
91
91
91
98
98
98
98
105
105
105
105
ADULT RATSBl
ood p
ress
ure (
mm H
g)
Bloo
d pre
ssur
e (mm
Hg)
Bloo
d pre
ssur
e (mm
Hg)
Bloo
d pre
ssur
e (mm
Hg)
DMSA
Age (days)
Age (days)
Age (days)
Age (days)
Enalapril Combination therapy
L-arginine
Control/water(n=15)
Control/water(n=15) Control/water(n=15)
Control/water(n=15)Pb/water(n=20)
Pb/water(n=20) Pb/water(n=20)
Pb/water(n=20)Control/DMSA (n = 25)
Control/enalapril (n = 20) Control/combination (n = 27)
Control/L-arginine (n = 25)Pb/DMSA (n = 27)
Pb/enalapril (n = 20) Pb/combination (n = 20)
Pb/L-arginine (n = 18)
225
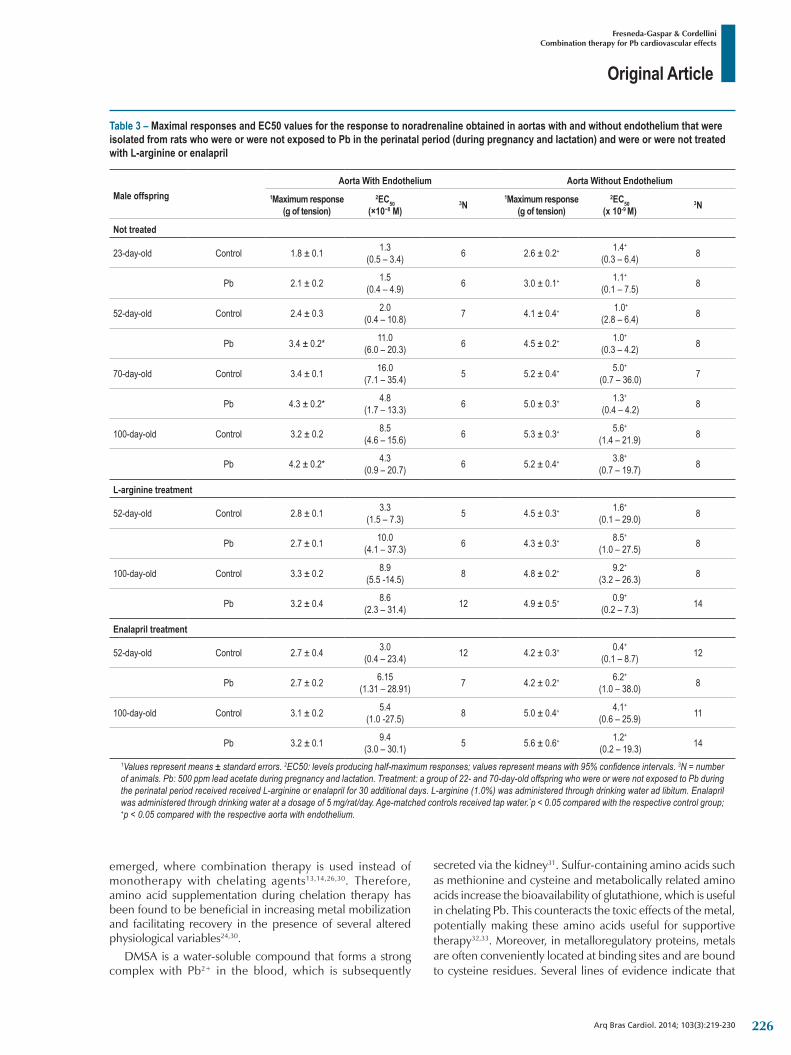
Original Article
Fresneda-Gaspar & CordelliniCombination therapy for Pb cardiovascular effects
Arq Bras Cardiol. 2014; 103(3):219-230
Table 3 – Maximal responses and EC50 values for the response to noradrenaline obtained in aortas with and without endothelium that were isolated from rats who were or were not exposed to Pb in the perinatal period (during pregnancy and lactation) and were or were not treated with L-arginine or enalapril
Male offspringAorta With Endothelium Aorta Without Endothelium
1Maximum response(g of tension)
2EC50 (×10−8 M)
3N1Maximum response
(g of tension)2EC50
(x 10-9 M)3N
Not treated
23-day-old Control 1.8 ± 0.1 1.3 (0.5 – 3.4) 6 2.6 ± 0.2+ 1.4+
(0.3 – 6.4) 8
Pb 2.1 ± 0.2 1.5(0.4 – 4.9) 6 3.0 ± 0.1+ 1.1+
(0.1 – 7.5) 8
52-day-old Control 2.4 ± 0.3 2.0 (0.4 – 10.8) 7 4.1 ± 0.4+ 1.0+
(2.8 – 6.4) 8
Pb 3.4 ± 0.2* 11.0 (6.0 – 20.3) 6 4.5 ± 0.2+ 1.0+
(0.3 – 4.2) 8
70-day-old Control 3.4 ± 0.1 16.0 (7.1 – 35.4) 5 5.2 ± 0.4+ 5.0+
(0.7 – 36.0) 7
Pb 4.3 ± 0.2* 4.8 (1.7 – 13.3) 6 5.0 ± 0.3+ 1.3+
(0.4 – 4.2) 8
100-day-old Control 3.2 ± 0.2 8.5 (4.6 – 15.6) 6 5.3 ± 0.3+ 5.6+
(1.4 – 21.9) 8
Pb 4.2 ± 0.2* 4.3 (0.9 – 20.7) 6 5.2 ± 0.4+ 3.8+
(0.7 – 19.7) 8
L-arginine treatment
52-day-old Control 2.8 ± 0.1 3.3 (1.5 – 7.3) 5 4.5 ± 0.3+ 1.6+
(0.1 – 29.0) 8
Pb 2.7 ± 0.1 10.0 (4.1 – 37.3) 6 4.3 ± 0.3+ 8.5+
(1.0 – 27.5) 8
100-day-old Control 3.3 ± 0.2 8.9 (5.5 -14.5) 8 4.8 ± 0.2+ 9.2+
(3.2 – 26.3) 8
Pb 3.2 ± 0.4 8.6 (2.3 – 31.4) 12 4.9 ± 0.5+ 0.9+
(0.2 – 7.3) 14
Enalapril treatment
52-day-old Control 2.7 ± 0.4 3.0 (0.4 – 23.4) 12 4.2 ± 0.3+ 0.4+
(0.1 – 8.7) 12
Pb 2.7 ± 0.2 6.15 (1.31 – 28.91) 7 4.2 ± 0.2+ 6.2+
(1.0 – 38.0) 8
100-day-old Control 3.1 ± 0.2 5.4 (1.0 -27.5) 8 5.0 ± 0.4+ 4.1+
(0.6 – 25.9) 11
Pb 3.2 ± 0.1 9.4 (3.0 – 30.1) 5 5.6 ± 0.6+ 1.2+
(0.2 – 19.3) 14
1Values represent means ± standard errors. 2EC50: levels producing half-maximum responses; values represent means with 95% confidence intervals. 3N = number of animals. Pb: 500 ppm lead acetate during pregnancy and lactation. Treatment: a group of 22- and 70-day-old offspring who were or were not exposed to Pb during the perinatal period received received L-arginine or enalapril for 30 additional days. L-arginine (1.0%) was administered through drinking water ad libitum. Enalapril was administered through drinking water at a dosage of 5 mg/rat/day. Age-matched controls received tap water.*p < 0.05 compared with the respective control group; +p < 0.05 compared with the respective aorta with endothelium.
emerged, where combination therapy is used instead of monotherapy with chelating agents13,14,26,30. Therefore, amino acid supplementation during chelation therapy has been found to be beneficial in increasing metal mobilization and facilitating recovery in the presence of several altered physiological variables24,30.
DMSA is a water-soluble compound that forms a strong complex with Pb2+ in the blood, which is subsequently
secreted via the kidney31. Sulfur-containing amino acids such as methionine and cysteine and metabolically related amino acids increase the bioavailability of glutathione, which is useful in chelating Pb. This counteracts the toxic effects of the metal, potentially making these amino acids useful for supportive therapy32,33. Moreover, in metalloregulatory proteins, metals are often conveniently located at binding sites and are bound to cysteine residues. Several lines of evidence indicate that
226
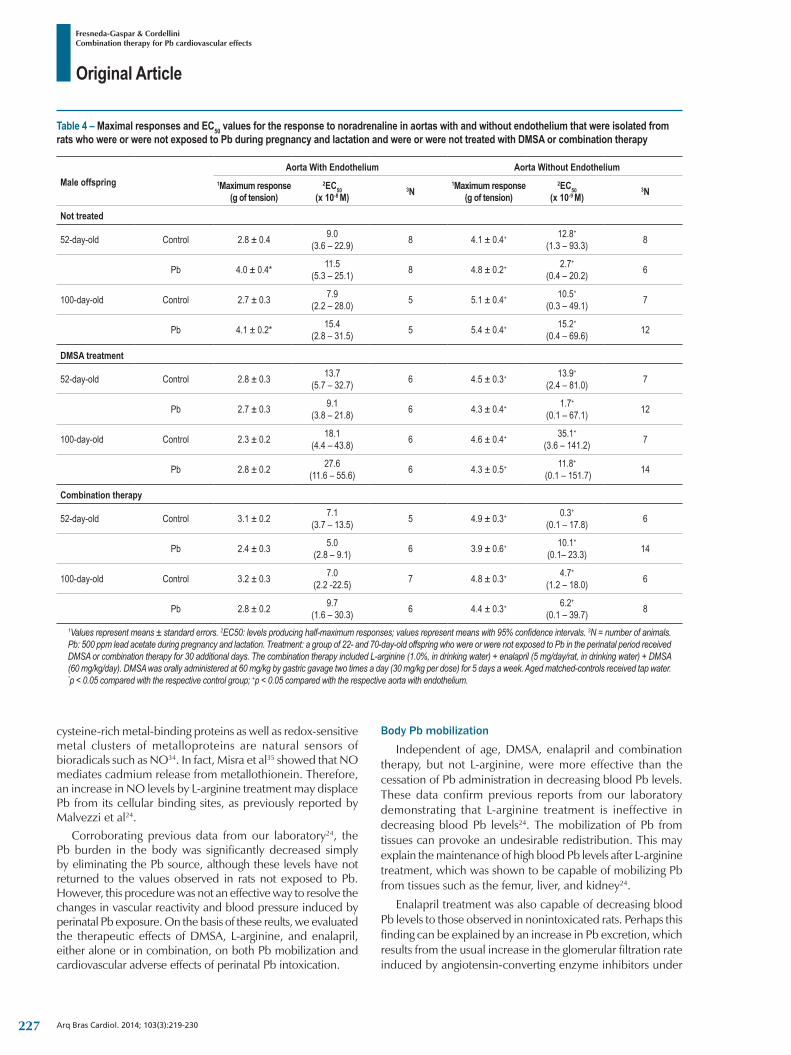
Original Article
Fresneda-Gaspar & CordelliniCombination therapy for Pb cardiovascular effects
Arq Bras Cardiol. 2014; 103(3):219-230
Table 4 – Maximal responses and EC50 values for the response to noradrenaline in aortas with and without endothelium that were isolated from rats who were or were not exposed to Pb during pregnancy and lactation and were or were not treated with DMSA or combination therapy
Male offspringAorta With Endothelium Aorta Without Endothelium
1Maximum response(g of tension)
2EC50 (x 10-8 M)
3N1Maximum response
(g of tension)2EC50
(x 10-9 M)3N
Not treated
52-day-old Control 2.8 ± 0.4 9.0 (3.6 – 22.9) 8 4.1 ± 0.4+ 12.8+
(1.3 – 93.3) 8
Pb 4.0 ± 0.4* 11.5 (5.3 – 25.1) 8 4.8 ± 0.2+ 2.7+
(0.4 – 20.2) 6
100-day-old Control 2.7 ± 0.3 7.9 (2.2 – 28.0) 5 5.1 ± 0.4+ 10.5+
(0.3 – 49.1) 7
Pb 4.1 ± 0.2* 15.4 (2.8 – 31.5) 5 5.4 ± 0.4+ 15.2+
(0.4 – 69.6) 12
DMSA treatment
52-day-old Control 2.8 ± 0.3 13.7 (5.7 – 32.7) 6 4.5 ± 0.3+ 13.9+
(2.4 – 81.0) 7
Pb 2.7 ± 0.3 9.1 (3.8 – 21.8) 6 4.3 ± 0.4+ 1.7+
(0.1 – 67.1) 12
100-day-old Control 2.3 ± 0.2 18.1 (4.4 – 43.8) 6 4.6 ± 0.4+ 35.1+
(3.6 – 141.2) 7
Pb 2.8 ± 0.2 27.6(11.6 – 55.6) 6 4.3 ± 0.5+ 11.8+
(0.1 – 151.7) 14
Combination therapy
52-day-old Control 3.1 ± 0.2 7.1(3.7 – 13.5) 5 4.9 ± 0.3+ 0.3+
(0.1 – 17.8) 6
Pb 2.4 ± 0.3 5.0(2.8 – 9.1) 6 3.9 ± 0.6+ 10.1+
(0.1– 23.3) 14
100-day-old Control 3.2 ± 0.3 7.0 (2.2 -22.5) 7 4.8 ± 0.3+ 4.7+
(1.2 – 18.0) 6
Pb 2.8 ± 0.2 9.7(1.6 – 30.3) 6 4.4 ± 0.3+ 6.2+
(0.1 – 39.7) 8
1Values represent means ± standard errors. 2EC50: levels producing half-maximum responses; values represent means with 95% confidence intervals. 3N = number of animals. Pb: 500 ppm lead acetate during pregnancy and lactation. Treatment: a group of 22- and 70-day-old offspring who were or were not exposed to Pb in the perinatal period received DMSA or combination therapy for 30 additional days. The combination therapy included L-arginine (1.0%, in drinking water) + enalapril (5 mg/day/rat, in drinking water) + DMSA (60 mg/kg/day). DMSA was orally administered at 60 mg/kg by gastric gavage two times a day (30 mg/kg per dose) for 5 days a week. Aged matched-controls received tap water. *p < 0.05 compared with the respective control group; +p < 0.05 compared with the respective aorta with endothelium.
cysteine-rich metal-binding proteins as well as redox-sensitive metal clusters of metalloproteins are natural sensors of bioradicals such as NO34. In fact, Misra et al35 showed that NO mediates cadmium release from metallothionein. Therefore, an increase in NO levels by L-arginine treatment may displace Pb from its cellular binding sites, as previously reported by Malvezzi et al24.
Corroborating previous data from our laboratory24, the Pb burden in the body was significantly decreased simply by eliminating the Pb source, although these levels have not returned to the values observed in rats not exposed to Pb. However, this procedure was not an effective way to resolve the changes in vascular reactivity and blood pressure induced by perinatal Pb exposure. On the basis of these reults, we evaluated the therapeutic effects of DMSA, L-arginine, and enalapril, either alone or in combination, on both Pb mobilization and cardiovascular adverse effects of perinatal Pb intoxication.
Body Pb mobilization
Independent of age, DMSA, enalapril and combination therapy, but not L-arginine, were more effective than the cessation of Pb administration in decreasing blood Pb levels. These data confirm previous reports from our laboratory demonstrating that L-arginine treatment is ineffective in decreasing blood Pb levels24. The mobilization of Pb from tissues can provoke an undesirable redistribution. This may explain the maintenance of high blood Pb levels after L-arginine treatment, which was shown to be capable of mobilizing Pb from tissues such as the femur, liver, and kidney24.
Enalapril treatment was also capable of decreasing blood Pb levels to those observed in nonintoxicated rats. Perhaps this finding can be explained by an increase in Pb excretion, which results from the usual increase in the glomerular filtration rate induced by angiotensin-converting enzyme inhibitors under
227

Original Article
Fresneda-Gaspar & CordelliniCombination therapy for Pb cardiovascular effects
Arq Bras Cardiol. 2014; 103(3):219-230
conditions of low glomerular filtration, similar to that observed in cases of Pb poisoning36. In fact, Pb also affects kidney function; the glomerular filtration rate appears to be affected by the lowest blood Pb levels. A decreased glomerular filtration rate has been consistently observed in populations with a mean blood Pb level of <20 µg/dL. Moreover, the increase in blood pressure and decrease in the glomerular filtration rate are closely related and probably share synergistic effects21.
Blood pressureIndependent of age, all treatments inhibited the increase
in blood pressure induced by perinatal Pb exposure. However, in contrast to other therapies, DMSA alone
was not effective in completely normalizing the blood pressure of adult rats perinatally exposed to Pb. This result corroborates previous data from our laboratory showing that 30-day DMSA treatment is unable to completely reverse the sustained increase in systolic blood pressure observed in rats exposed to Pb during adult life24. Contrasting reports from the literature have shown that DMSA treatment is capable of abolishing Pb-induced hypertension16,37. This discrepancy may be due to differences in the dosing protocols and treatment duration because these parameters are important for reversing Pb-induced hypertension38. Another possibility can involve differences in the mechanisms underlying the maintenance of Pb-induced hypertension that are related to different periods of animal development. This hypothesis is based on the fact that treatment with DMSA is completely effective in restoring Pb-induced hypertension in young, but not adult, rats.
L-arginine showed an increased latency in the expression of beneficial effects on blood pressure in young rats compared with that in adult rats. The opposite was observed during treatment with enalapril. Moreover, L-arginine treatment was shown to be more effective than DMSA treatment in the reversal of blood pressure in adult, but not young, rats. These observations also support the hypothesis that there are distinct mechanisms for the maintenance of Pb-induced hypertension during different periods of life.
Finally, combination therapy induced an earlier restoration of blood pressure in Pb-exposed young rats compared with the monotherapies, except for enalapril monotherapy. One possible explanation would be the additional effects of L-arginine, which is an NO precursor, DMSA, which is a chelating agent and scavenger of ROS, and enalapril, which is a renin–angiotensin system inhibitor, on blood pressure. Because the heart rate is higher in young animals than in adult animals, and because the presence of enalapril increases glomerular filtration, one can expect a higher excretion of Pb in young rats. This fact can explain the similar efficacy between enalapril and combined therapy in restoring the blood pressure of young rats exposed to Pb and the higher efficacy of combination therapy in adult rats.
Vascular reactivityIndependent of postnatal age, all treatments were able
to resolve the changes in vascular reactivity induced by perinatal Pb exposure. We speculate that Pb-induced changes in vascular reactivity were caused by decreased NO and/or
by a ROS and that the provision of additional NO through administration of the substrate L-arginine could act as an ROS scavenger and/or directly as a vasodilator, thus resolving the vascular changes. In addition to its chelating action, DMSA may also act as a scavenger of ROS that may contribute to the improvement in changes in vascular reactivity induced by Pb exposure16,39. Some other reported mechanisms by which Pb can contribute to the development of arterial hypertension are an increase in the angiotensin-converting enzyme activity and an increase in the plasma levels of renin, angiotensin II, aldosterone, and kininases1. In the present study, enalapril normalized the functional changes in vascular reactivity induced by perinatal Pb exposure. This result corroborates with those of previous studies showing that strategies interrupting the renin–angiotensin system also decrease cardiovascular alterations in a variety of hypertensive states, including those caused by Pb exposure36.
Most conventional chelators are compromised by side effects, particularly their binding to essential metals, which decreases their efficacy. As a result, there is no safe and effective treatment for Pb poisoning13,30. Therefore, combination therapy may play a significant and important role in the abation of several toxic effects of Pb compared with monotherapies, in addition to their impressive effects in terms of blood pressure recovery. In this context, this study advances our understanding of the cardiovascular effects of perinatal Pb exposure and can aid in the development of a new therapeutic protocol for the treatment Pb-induced hypertension.
Acknowledgements
We are grateful to Mr. Alaor Aparecido Almeida and CEATOX-IBB-UNESP for aid in the determination of blood Pb levels and Fundação de Amparo à Pesquisa do Estado de São Paulo-FAPESP (process numbers: 03/06760-5 and 04/00640-0) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior/PROAP for financial support.
Author contributionsConception and design of the research, Acquisition of data,
Analysis and interpretation of the data, Statistical analysis and Writing of the manuscript: Fresneda-Gaspar A, Cordellini S; Obtaining financing and Critical revision of the manuscript for intellectual content: Cordellini S.
Potential Conflict of InterestNo potential conflict of interest relevant to this article
was reported.
Sources of FundingThis study was funded by FAPESP and CAPES/PROAP.
Study AssociationThis article is part of the thesis of Doctoral submitted by
Andreia Fresneda Gaspar from UNESP.
228
Original Article
Fresneda-Gaspar & CordelliniCombination therapy for Pb cardiovascular effects
Arq Bras Cardiol. 2014; 103(3):219-230
1. Vaziri ND. Mechanisms of lead-induced hypertension and cardiovascular disease. Am J Physiol Heart Circ Physiol. 2008;295(2):H454-65.
2. Skoczynska A, Juzwa W, Smolik R, Szechinski J, Behal FJ. Response of the cardiovascular system to catecholamines in rats given small doses of lead. Toxicology. 1986;39(3):275-89.
3. Tsao DA, Yu HS, Cheng JT, Ho CK, Chang HR. The change of beta-adrenergic system in lead-induced hypertension. Toxicol Appl Pharmacol. 2000;164(2):127-33.
4. Marques M, Millás I, Jimenez A, García-Colis C, Rodriguez-Feo JA, Velasco S, et al. Alteration of the soluble guanylate cyclase system in the vascular wall of lead-induced hypertension in rats. J Am Soc Nephrol. 2001;12(12):2594-600.
5. Purdy RE, Smith JR, Ding Y, Oveisi F, Vaziri ND, Gonick HC. Lead-induced hypertension is not associated with altered vascular reactivity in vitro. Am J Hypertens. 1997;10(9 Pt 1):997-1003.
6. Moreira EG, Rosa GJ, Barros SB, Vassillieff VS, Vassilieff I. Antioxidant defense in rat brain regions after developmental lead exposure. Toxicology. 2001;169(2):145-51.
7. Moreira EG, Vassilieff I, Vassillieff VS. Developmental lead exposure: behavioral alterations in the short and long term. Neurotoxicol Teratol. 2001;23(5):489-95.
8. Khalil-Manesh F, Gonick HC, Weiler EW, Prins B, Weber MA, Purdy RE. Lead-induced hypertension: possible role of endothelial factors. Am J Hypertens. 1993;6(9):723-9.
9. Watts SW, Chai S, Webb RC. Lead acetate-induced contraction in rabbit mesenteric artery: interaction with calcium and protein kinase C. Toxicology. 1995;99(1-2):55-65.
10. Nava-Ruiz C, Mendez-Armenta M, Ríos C. Lead neurotoxicity: effects on brain nitric oxide synthase. J Mol Histol. 2012;43(5):553-63.
11. Fujiwara Y, Kaji T, Yamamoto C, Sakamoto M, Kozuka H. Stimulatory effect of lead on the proliferation of cultured vascular smooth-muscle cells. Toxicology. 1995;98(1-3):105-10.
12. Kaji T, Fujiwara Y, Hoshino M, Yamamoto C, Sakamoto M, Kozuka H. Inhibitory effect of lead on the proliferation of cultured vascular endothelial cells. Toxicology. 1995;95(1-3):87-92.
13. Flora SJ, Mittal M, Mehta A. Heavy metal induced oxidative stress and its possible reversal by chelation therapy. Indian J Med Res. 2008;128(4):501-23.
14. Flora SJ, Pachauri, V. Chelation in metal intoxication. Int J Environ Res Public Health. 2010;7(7):2745-88.
15. Sears ME. Chelat ion: harness ing and enhancing heavy metal detoxification--a review. Scientific World Journal. 2013;2013:219840.
16. Khalil-Manesh F, Gonick HC, Weiler EW, Prins B, Weber MA, Purdy R, et al. Effects of chelation treatment with dimercaptosuccinic acid (DMSA) on lead-related blood pressure changes. Environ Res. 1994;65(1):86-99.
17. Cory-Slechta DA. Mobilization of lead over the course of DMSA chelation therapy and long term efficacy. J Pharmacol Exp Ther. 1988;246(1):84-91.
18. Mayer B, Hemmes B. Biosynthesis and action of nitric oxide in mammalian cells. Trends Biochem Sci. 1997;22(12):477-81.
19. Wang J, Wu J, Zhang Z. Oxidative Stress in mouse brain exposed to lead. Ann Occup Hyg. 2006;50(4):405-9.
20. Athanasopoulos, N. Flame Methods Manual GBC for Atomic Absorption. Australia: Vitoria; 1994. p. 1-11.
21. Agency for Toxic Substances & Diseases Registry. (ATSDR). Toxicological profile for lead [Internet]. Atlanta: ATSDR; 2007 [Cited on 2014 Apr 2]. Available from: http://www.atsdr.cdc.gov/toxprofiles/tp.asp?id=96&tid=22.
22. Kopp SJ, Barron JT, Tow JP. Cardiovascular actions of lead and relationship to hypertension: a review. Environ Health Perspect. 1988;78:91-9.
23. Vaziri ND, Gonick HC. Cardiovascular effects of lead exposure. Indian J Med Res. 2008;128(4):426-35.
24. Malvezzi CK, Moreira EG, Vassilieff I, Vassilieff VS, Cordellini S. Effect of L-arginine, dimercaptosuccinic acid (DMSA) and the association of L-arginine and DMSA on tissue lead mobilization and blood pressure level in plumbism. Braz J Med Biol Res. 2001;34(10):1341-6.
25. Heydari A, Norouzzadeh A, Khoshbaten A, Asgari A, Ghasemi A, Najafi S, et al. Effects of short-term and subchronic lead poisoning on nitric oxide metabolites and vascular responsiveness in rat. Toxicol Lett. 2006;166(1):88-94.
26. Patrick L. Lead toxicity, a review of the literature. Part 1: Exposure, evaluation, and treatment. Altern Med Rev. 2006;11(1):2-22.
27. Grizzo LT, Cordellini S. Perinatal lead exposure affects nitric oxide and cyclooxygenase pathways in aorta of weaned rats. Toxicol Sci. 2008;103(1):207-14.
28. Weiler E, Khalil-Manesh F, Gonick HC. Effects of lead and low-molecular-weight endogenous plasma inhibitor on the kinetics of sodium-potassium-activated adenosine triphosphatase and potassium-activated p-nitrophenylphosphatase. Clin Sci. 1990;79(2):185-92.
29. Hart WM Jr, Titus EO. Sulfhydryl groups of sodium-potassium transport adenosine triphosphatase. J Biol Chem. 1973;248(13):4674-81.
30. Kalia K, Flora SJ. Strategies for safe and effective therapeutic measures for chronic arsenic and lead poisoning. J Occup Health. 2005;47(1):1-21.
31. Hamidinia SA, Erdahl WL, Chapman CJ, Steinbaugh GE, Taylor RW, Pfeiffer DR. Monensin improves the effectiveness of meso-dimercaptosuccinate when used to treat lead intoxication in rats. Environ Health Perspect. 2006;114(4):484-93.
32. Kachru DN, Khandelwal S, Tandon SK. Influence of methionine supplementation in chelation of lead in rats. Biomed Environ Sci. 1989;2(3):265-70.
33. Quig D. Cysteine metabolism and metal toxicity. Altern Med Rev. 1998;3(4):262-70.
34. Drapier JC, Bouton C. Modulation by nitric oxide of metalloprotein regulatory activities. Bioessays. 1996;18(7):549-56.
35. Misra RR, Hochadel JF, Smith GT, Cook JC, Waalkes MP, Wink DA. Evidence that nitric oxide enhances cadmium toxicity by displacing the metal from metallothionein. Chem Res Toxicol. 1996;9(1):326-32.
36. Ng HY, Tain YL, Lee YT, Hsu CY, Chiou TT, Huang PC, et al. Renin angiotensin system blockade ameliorates lead nephropathy. Biochem Biophys Res Commun. 2013;438(2):359-63.
37. Ding Y, Vaziri ND, Gonick HC. Lead-induced hypertension II. Response to sequential infusions of L-arginine, superoxide dismutase, and nitroprusside. Environ Res. 1998;76(2):107-13.
38. Pappas JB, Nuttall KL, Ahlquist JT, Allen EM, Banner W Jr. Oral dimercaptosuccinic acid and ongoing exposure to lead: effects on heme synthesis and lead distribution in a rat model. Toxicol Appl Pharmacol. 1995;133(1):121-9.
39. Patrick L. Lead toxicity part II: the role of free radical damage and the use of antioxidants in the pathology and treatment of lead toxicity. Altern Med Rev. 2006;11(2):114-27.
References
229

Original Article
Fresneda-Gaspar & CordelliniCombination therapy for Pb cardiovascular effects
Arq Bras Cardiol. 2014; 103(3):219-230 230

Original Article
Assessing Strategies for Heart Failure with Preserved Ejection Fraction at the Outpatient ClinicAntonio Jose Lagoeiro Jorge, Maria Luiza Garcia Rosa, Mario Luiz Ribeiro, Luiz Claudio Maluhy Fernandes, Monica Di Calafiori Freire, Dayse Silva Correia, Patrick Duarte Teixeira, Evandro Tinoco MesquitaUniversidade Federal Fluminense, Niterói, RJ − Brazil
Mailing Address: Antonio José Lagoeiro Jorge •Rua Coronel Bittencourt, 66, Boa Vista. Postal Code 24900-000, Maricá, RJ – BrazilE-mail: [email protected]; [email protected] received January 16, 2014; revised manuscript February 04, 2014; accepted April 16, 2014.
DOI: 10.5935/abc.20140120
Abstract
Background: Heart failure with preserved ejection fraction (HFPEF) is the most common form of heart failure (HF), its diagnosis being a challenge to the outpatient clinic practice.
Objective: To describe and compare two strategies derived from algorithms of the European Society of Cardiology Diastology Guidelines for the diagnosis of HFPEF.
Methods: Cross-sectional study with 166 consecutive ambulatory patients (67.9±11.7 years; 72% of women). The strategies to confirm HFPEF were established according to the European Society of Cardiology Diastology Guidelines criteria. In strategy 1 (S1), tissue Doppler echocardiography (TDE) and electrocardiography (ECG) were used; in strategy 2 (S2), B-type natriuretic peptide (BNP) measurement was included.
Results: In S1, patients were divided into groups based on the E/E’ ratio as follows: GI, E/E’ > 15 (n = 16; 9%); GII, E/E’ 8 to 15 (n = 79; 48%); and GIII, E/E’ < 8 (n = 71; 43%). HFPEF was confirmed in GI and excluded in GIII. In GII, TDE [left atrial volume index (LAVI) ≥ 40 mL/m2; left ventricular mass index LVMI) > 122 for women and > 149 g/m2 for men] and ECG (atrial fibrillation) parameters were assessed, confirming HFPEF in 33 more patients, adding up to 49 (29%). In S2, patients were divided into three groups based on BNP levels. GI (BNP > 200 pg/mL) consisted of 12 patients, HFPEF being confirmed in all of them. GII (BNP ranging from 100 to 200 pg/mL) consisted of 20 patients with LAVI > 29 mL/m2, or LVMI ≥ 96 g/m2 for women or ≥ 116 g/m2 for men, or E/E’ ≥ 8 or atrial fibrillation on ECG, and the diagnosis of HFPEF was confirmed in 15. GIII (BNP < 100 pg/mL) consisted of 134 patients, 26 of whom had the diagnosis of HFPEF confirmed when GII parameters were used. Measuring BNP levels in S2 identified 4 more patients (8%) with HFPEF as compared with those identified in S1.
Conclusion: The association of BNP measurement and TDE data is better than the isolated use of those parameters. BNP can be useful in identifying patients whose diagnosis of HF had been previously excluded based only on TDE findings. (Arq Bras Cardiol. 2014; 103(3):231-237)
Keywords: Heart Failure; Ambulatory Care; Echocardiography, Doppler; Natriuretic Peptides.
IntroductionHeart failure with preserved ejection fraction (HFPEF)
is currently the most common form of heart failure (HF), mainly because of the accelerated population aging and high prevalence of comorbidities. Morbidity and mortality of HFPEF are elevated, similarly to those of HF with reduced ejection fraction1. Diagnosing HFPEF is one of the great challenges in outpatient clinic practice, in which the patient usually has intolerance to effort and evidence of neither pulmonary
nor systemic congestion1-3. Despite the lack of an effective treatment4,5, it has been well established in the literature that patients with HFPEF should benefit from the control of risk factors present in HFPEF6-8.
The European Society of Cardiology Diastology Guidelines has proposed updated algorithms for the diagnosis and exclusion of HFPEF in ambulatory patients by using tissue Doppler echocardiography (TDE) and measuring plasma levels of natriuretic peptides9. That systematization in Brazil is still little used by outpatient clinicians, mainly because of the difficulty in having access to TDE and natriuretic peptide measurements.
This study was aimed at describing and comparing two strategies, one of which with no measurement of B-type natriuretic peptide (BNP), both derived from the algorithms proposed by the European Society of Cardiology Diastology Guidelines9 for the diagnosis of HFPEF in ambulatory patients with signs or symptoms of HF.
231

Original Article
Jorge et al.Diagnosis of HFPEF at the outpatient clinic
Arq Bras Cardiol. 2014; 103(3):231-237
Methods
PopulationThis is a cross-sectional study with non-probability
sampling. A convenience sample was selected and included 166 consecutive ambulatory patients with clinical suspicion of HF, assessed from June 2008 to October 2010. The patients had left ventricular ejection fraction (LVEF) ≥ 50%.
In this study, we established two strategies [strategy 1 and strategy 2 (S1 and S2, respectively)] based on the algorithms of the European Society of Cardiology Diastology Guidelines to confirm the diagnosis of HFPEF, which requires the following conditions to be satisfied: signs or symptoms of HF; LVEF ≥ 50%; left ventricular end-diastolic volume index (LVEDVI) ≤ 97 mL/m2; and diastolic dysfunction. In S1, TDE and electrocardiography (ECG) parameters were used; in S2, in addition to those TDE and ECG parameters, BNP measurements were used9.
In S1, diastolic dysfunction was diagnosed by use of TDE and based on an E/E’ ratio > 15. If the E/E’ ratio was between 8 and 15, suggesting diastolic dysfunction, other TDE measurements, such as LV mass index (LVMI, > 122 g/m2 and > 149 g/m2 for women and men, respectively), left atrial volume (LAV) index (LAVI, > 40 mL/m2) and E/A ratio < 0.5, with deceleration time of the E wave (DT) > 280 ms, were used to confirm the diagnosis. Atrial fibrillation on ECG with an E/E’ ratio between 8 and 15 also confirmed the diagnosis of HFPEF7.
In S2, BNP measurements were initially combined with the TDE and ECG parameters already described.
Patients with severe heart valve disease, definitive pacemaker, pericardial diseases, severe chronic obstructive pulmonary disease submitted to heart surgery in the last six months were excluded from this study.
Tissue Doppler EchocardiographyTissue Doppler echocardiography was performed
with a Vivid 7 device (GE Medical Systems, Horten, Norway), and analyzed with the EchoPAC software by an experienced observer with no previous knowledge of the other results. The procedure was performed according to the recommendations for chamber quantification of the American Society of Echocardiography (ASE) and the European Association of Echocardiography (EAE)10. Systolic function was assessed by measuring LVEF.
The LAV indexed to body surface was obtained by use of the biplanar method of discs (modified Simpson’s rule) with four- and two-chamber apical view during the end of left ventricular systole. The parameters of diastolic function were estimated by using the mean of five consecutive heartbeats. The initial (E) and late (A) transmitral flow and the DT of the E wave were measured. The myocardial relaxation velocity at the beginning of diastole (E’) was measured by use of TDE on the septal and lateral segments of the mitral ring, and the mean of those measurements was obtained. All exams were digitally recorded for future analyses and reviews.
ElectrocardiographyAll patients underwent 12-lead ECG (Dixtal, Brazil) at rest
to identify the presence of atrial fibrillation.
B-type natriuretic peptideBNP was measured in whole blood samples by using Alere
Triage BNP Test (Biosite, USA), which is a rapid fluorescence immunoassay to be used with the Triage Meter for the quantitative measurement of BNP. The BNP values were expressed as pg/mL.
Statistical analysisThe statistical analysis was performed using the Statistical
Package for the Social Science® (SPSS®) software, version 17.0. Continuous variables with normal distribution were expressed as means ± standard deviation, and the differences were assessed with Student t test or Analysis of Variance (ANOVA). Continuous variables whose distributions were not normal were presented as medians, and the differences were assessed with Mann-Whitney U test or Kruskal-Wallis-H test. Categorical variables were presented as absolute and relative frequencies, and the differences were assessed with Pearson’s chi-square test. Spearman rank correlation (rho) was used to assess the association between BNP levels and clinical and echocardiographic variables. The statistical significance level of 0.05 was adopted.
Ethical considerationsThis study is in accordance with the principles established in
the Declaration of Helsinki, and its protocol was approved by the Ethics Committee of the Universidade Federal Fluminense (protocol 00410.258.000-08). All patients provided written informed consent.
ResultsThis study assessed 166 patients (mean age, 67.9 ± 11.7 years;
72% of women), whose major clinical, echocardiographic and laboratory characteristics are shown in Table 1.
Strategy 1The patients were divided into three groups according to
their E/E’ ratio values (Table 2), and were assessed according to the European Society of Cardiology Diastology Guidelines criteria, as follows: group I, patients with E/E’ > 15 (n = 16; 9%); group II, patients with E/E’ ranging from 8 to 15 (n = 79; 48%); and group III, patients with E/E’ < 8 (n = 71; 43%). Group I patients had their diagnosis of HFPEF confirmed, while group III patients had the diagnosis of HFPEF excluded.
The 79 group II patients underwent analysis of other TDE parameters and ECG, and the findings were as follows: LAVI > 40 mL/m2 in 20 women (25%); LVMI > 122 g/m2 for women or > 149 g/m2 for men in 5 patients (6%); E/A ratio < 0.5 with DT > 280 ms not found in any patient; and atrial fibrillation on ECG of 2 patients (15%). Those findings allowed to diagnose HFPEF in 33 patients (42%) and to exclude it in 46 (58%) (Figure 1).
232
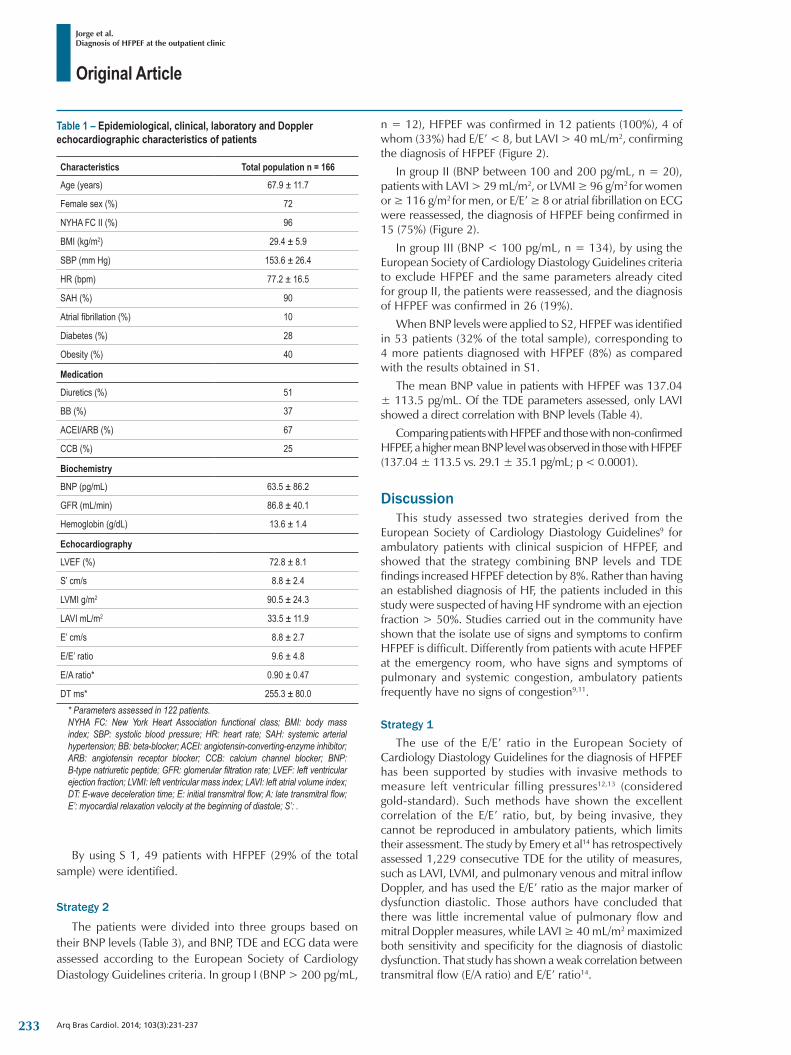
Original Article
Jorge et al.Diagnosis of HFPEF at the outpatient clinic
Arq Bras Cardiol. 2014; 103(3):231-237
Table 1 – Epidemiological, clinical, laboratory and Doppler echocardiographic characteristics of patients
Characteristics Total population n = 166
Age (years) 67.9 ± 11.7
Femalesex(%) 72
NYHA FC II (%) 96
BMI (kg/m2) 29.4 ± 5.9
SBP (mm Hg) 153.6 ± 26.4
HR (bpm) 77.2 ± 16.5
SAH (%) 90
Atrialfibrillation(%) 10
Diabetes (%) 28
Obesity (%) 40
Medication
Diuretics (%) 51
BB (%) 37
ACEI/ARB (%) 67
CCB (%) 25
Biochemistry
BNP (pg/mL) 63.5 ± 86.2
GFR (mL/min) 86.8 ± 40.1
Hemoglobin (g/dL) 13.6 ± 1.4
Echocardiography
LVEF (%) 72.8 ± 8.1
S’ cm/s 8.8 ± 2.4
LVMI g/m2 90.5 ± 24.3
LAVI mL/m2 33.5 ± 11.9
E’ cm/s 8.8 ± 2.7
E/E’ ratio 9.6 ± 4.8
E/A ratio* 0.90 ± 0.47
DT ms* 255.3 ± 80.0* Parameters assessed in 122 patients.NYHA FC: New York Heart Association functional class; BMI: body mass index; SBP: systolic blood pressure; HR: heart rate; SAH: systemic arterial hypertension; BB: beta-blocker; ACEI: angiotensin-converting-enzyme inhibitor; ARB: angiotensin receptor blocker; CCB: calcium channel blocker; BNP: B-type natriuretic peptide; GFR: glomerular filtration rate; LVEF: left ventricular ejection fraction; LVMI: left ventricular mass index; LAVI: left atrial volume index; DT: E-wave deceleration time; E: initial transmitral flow; A: late transmitral flow; E’: myocardial relaxation velocity at the beginning of diastole; S’: .
By using S 1, 49 patients with HFPEF (29% of the total sample) were identified.
Strategy 2
The patients were divided into three groups based on their BNP levels (Table 3), and BNP, TDE and ECG data were assessed according to the European Society of Cardiology Diastology Guidelines criteria. In group I (BNP > 200 pg/mL,
n = 12), HFPEF was confirmed in 12 patients (100%), 4 of whom (33%) had E/E’ < 8, but LAVI > 40 mL/m2, confirming the diagnosis of HFPEF (Figure 2).
In group II (BNP between 100 and 200 pg/mL, n = 20), patients with LAVI > 29 mL/m2, or LVMI ≥ 96 g/m2 for women or ≥ 116 g/m2 for men, or E/E’ ≥ 8 or atrial fibrillation on ECG were reassessed, the diagnosis of HFPEF being confirmed in 15 (75%) (Figure 2).
In group III (BNP < 100 pg/mL, n = 134), by using the European Society of Cardiology Diastology Guidelines criteria to exclude HFPEF and the same parameters already cited for group II, the patients were reassessed, and the diagnosis of HFPEF was confirmed in 26 (19%).
When BNP levels were applied to S2, HFPEF was identified in 53 patients (32% of the total sample), corresponding to 4 more patients diagnosed with HFPEF (8%) as compared with the results obtained in S1.
The mean BNP value in patients with HFPEF was 137.04 ± 113.5 pg/mL. Of the TDE parameters assessed, only LAVI showed a direct correlation with BNP levels (Table 4).
Comparing patients with HFPEF and those with non-confirmed HFPEF, a higher mean BNP level was observed in those with HFPEF (137.04 ± 113.5 vs. 29.1 ± 35.1 pg/mL; p < 0.0001).
DiscussionThis study assessed two strategies derived from the
European Society of Cardiology Diastology Guidelines9 for ambulatory patients with clinical suspicion of HFPEF, and showed that the strategy combining BNP levels and TDE findings increased HFPEF detection by 8%. Rather than having an established diagnosis of HF, the patients included in this study were suspected of having HF syndrome with an ejection fraction > 50%. Studies carried out in the community have shown that the isolate use of signs and symptoms to confirm HFPEF is difficult. Differently from patients with acute HFPEF at the emergency room, who have signs and symptoms of pulmonary and systemic congestion, ambulatory patients frequently have no signs of congestion9,11.
Strategy 1The use of the E/E’ ratio in the European Society of
Cardiology Diastology Guidelines for the diagnosis of HFPEF has been supported by studies with invasive methods to measure left ventricular filling pressures12,13 (considered gold-standard). Such methods have shown the excellent correlation of the E/E’ ratio, but, by being invasive, they cannot be reproduced in ambulatory patients, which limits their assessment. The study by Emery et al14 has retrospectively assessed 1,229 consecutive TDE for the utility of measures, such as LAVI, LVMI, and pulmonary venous and mitral inflow Doppler, and has used the E/E’ ratio as the major marker of dysfunction diastolic. Those authors have concluded that there was little incremental value of pulmonary flow and mitral Doppler measures, while LAVI ≥ 40 mL/m2 maximized both sensitivity and specificity for the diagnosis of diastolic dysfunction. That study has shown a weak correlation between transmitral flow (E/A ratio) and E/E’ ratio14.
233
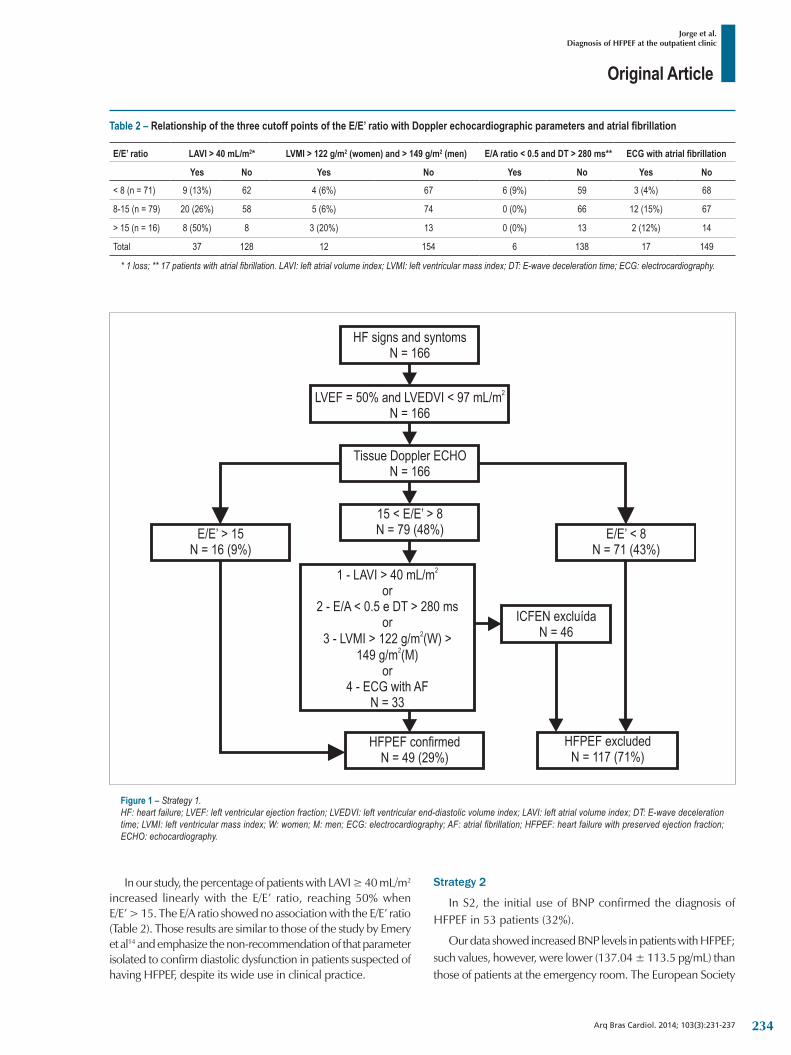
Original Article
Jorge et al.Diagnosis of HFPEF at the outpatient clinic
Arq Bras Cardiol. 2014; 103(3):231-237
Table 2 – Relationship of the three cutoff points of the E/E’ ratio with Doppler echocardiographic parameters and atrial fibrillation
E/E’ ratio LAVI > 40 mL/m2* LVMI > 122 g/m2 (women) and > 149 g/m2 (men) E/A ratio < 0.5 and DT > 280 ms** ECG with atrial fibrillation
Yes No Yes No Yes No Yes No
< 8 (n = 71) 9 (13%) 62 4 (6%) 67 6 (9%) 59 3 (4%) 68
8-15 (n = 79) 20 (26%) 58 5 (6%) 74 0 (0%) 66 12 (15%) 67
> 15 (n = 16) 8 (50%) 8 3 (20%) 13 0 (0%) 13 2 (12%) 14
Total 37 128 12 154 6 138 17 149
* 1 loss; ** 17 patients with atrial fibrillation. LAVI: left atrial volume index; LVMI: left ventricular mass index; DT: E-wave deceleration time; ECG: electrocardiography.
In our study, the percentage of patients with LAVI ≥ 40 mL/m2 increased linearly with the E/E’ ratio, reaching 50% when E/E’ > 15. The E/A ratio showed no association with the E/E’ ratio (Table 2). Those results are similar to those of the study by Emery et al14 and emphasize the non-recommendation of that parameter isolated to confirm diastolic dysfunction in patients suspected of having HFPEF, despite its wide use in clinical practice.
Figure 1 – Strategy 1.HF: heart failure; LVEF: left ventricular ejection fraction; LVEDVI: left ventricular end-diastolic volume index; LAVI: left atrial volume index; DT: E-wave deceleration time; LVMI: left ventricular mass index; W: women; M: men; ECG: electrocardiography; AF: atrial fibrillation; HFPEF: heart failure with preserved ejection fraction; ECHO: echocardiography.
Strategy 2
In S2, the initial use of BNP confirmed the diagnosis of HFPEF in 53 patients (32%).
Our data showed increased BNP levels in patients with HFPEF; such values, however, were lower (137.04 ± 113.5 pg/mL) than those of patients at the emergency room. The European Society
234
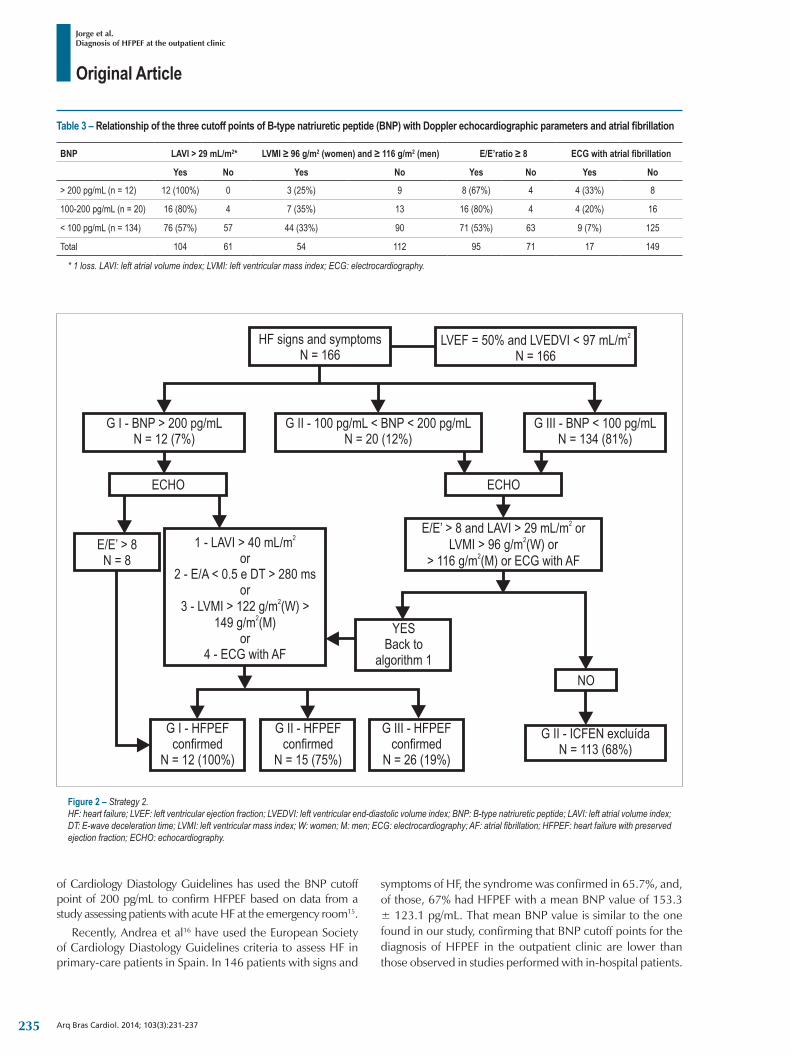
Original Article
Jorge et al.Diagnosis of HFPEF at the outpatient clinic
Arq Bras Cardiol. 2014; 103(3):231-237
Figure 2 – Strategy 2.HF: heart failure; LVEF: left ventricular ejection fraction; LVEDVI: left ventricular end-diastolic volume index; BNP: B-type natriuretic peptide; LAVI: left atrial volume index; DT: E-wave deceleration time; LVMI: left ventricular mass index; W: women; M: men; ECG: electrocardiography; AF: atrial fibrillation; HFPEF: heart failure with preserved ejection fraction; ECHO: echocardiography.
of Cardiology Diastology Guidelines has used the BNP cutoff point of 200 pg/mL to confirm HFPEF based on data from a study assessing patients with acute HF at the emergency room15.
Recently, Andrea et al16 have used the European Society of Cardiology Diastology Guidelines criteria to assess HF in primary-care patients in Spain. In 146 patients with signs and
symptoms of HF, the syndrome was confirmed in 65.7%, and, of those, 67% had HFPEF with a mean BNP value of 153.3 ± 123.1 pg/mL. That mean BNP value is similar to the one found in our study, confirming that BNP cutoff points for the diagnosis of HFPEF in the outpatient clinic are lower than those observed in studies performed with in-hospital patients.
Table 3 – Relationship of the three cutoff points of B-type natriuretic peptide (BNP) with Doppler echocardiographic parameters and atrial fibrillation
BNP LAVI > 29 mL/m2* LVMI ≥ 96 g/m2 (women) and ≥ 116 g/m2 (men) E/E’ratio ≥ 8 ECG with atrial fibrillation
Yes No Yes No Yes No Yes No
> 200 pg/mL (n = 12) 12 (100%) 0 3 (25%) 9 8 (67%) 4 4 (33%) 8
100-200 pg/mL (n = 20) 16 (80%) 4 7 (35%) 13 16 (80%) 4 4 (20%) 16
< 100 pg/mL (n = 134) 76 (57%) 57 44 (33%) 90 71 (53%) 63 9 (7%) 125
Total 104 61 54 112 95 71 17 149
* 1 loss. LAVI: left atrial volume index; LVMI: left ventricular mass index; ECG: electrocardiography.
235
Original Article
Jorge et al.Diagnosis of HFPEF at the outpatient clinic
Arq Bras Cardiol. 2014; 103(3):231-237
Table 4 – Correlation between B-type natriuretic peptide (BNP) and Doppler echocardiographic parameters
Pearson p value
E/E’ ratio 0.318 < 0.0001
LAVI (mL/m2) 0.631 < 0.0001
E/A ratio 0.115 0.164
LVMI (g/m2) 0.078 0.320
E: initial transmitral flow; E’: myocardial relaxation velocity at the beginning of diastole; A: late transmitral flow; LAVI: left atrial volume index; LVMI: left ventricular mass index.
The European Society of Cardiology Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure recommends the routine measurement of natriuretic peptides in patients suspected of having HF. Those guidelines establish the BNP cutoff point of 35 pg/mL for ambulatory patients to exclude both HFPEF and HF with reduced ejection fraction (HFREF)17.
In our study, HFPEF could be found by use of TDE parameters in 20% of the patients whose BNP levels ranged from 35 to 100 pg/mL, which makes TDE indispensable in that group of patients.
The comparison between BNP levels and the TDE parameters used to diagnose HFPEF evidenced a positive association between BNP increase and LAVI (Table 4); in addition, all patients with BNP levels > 200 pg/mL had increased LAVI, which confirmed the diagnosis of HFPEF.
Four patients (2.5%) had an E/E’ ratio < 8, which would exclude the diagnosis of HFPEF, but their BNP level > 200 pg/mL and LAVI > 40 mL/m2 confirmed the diagnosis.
The classical diagnosis of HF is based on the presence of symptoms and signs of HF in association with cardiac structural or functional abnormalities usually demonstrated on Doppler echocardiography. That concept, however, has diagnostic difficulties for patients with HFPEF, who have mainly diastolic dysfunction17.
In epidemiological studies, the prevalence of HFPEF can range from 13% to 75% of the HF cases, depending on the diagnostic criteria used. There is great diversity in the criteria used to determine the presence of HF, in the populations studied and in the methods evaluating left ventricular function. This hinders their use in clinical practice, and because patients with HFPEF do not meet the classical definition of HF, they end up neglected and poorly assessed18.
The use of BNP measurements in association with TDE and ECG data, as shown in this study, can be a good option to confirm the diagnosis of HFPEF in ambulatory patients, considering that the BNP levels are consistently increased in patients with symptoms of HF and BNP is an excellent marker of diastolic dysfunction19.
LimitationsThis study has limitations related to its sample size. In
addition, no data on the difference of the Ar wave (retrograde blood flow into the pulmonary veins) and the A wave (forward transmitral flow) [(Ard – Ad)] were provided, because of the technical difficulties for obtaining that parameter (less than 50% of the patients), as already reported in other studies13,19.
ConclusionThis study assessed two strategies for the diagnosis of heart
failure with preserved ejection fraction, or its exclusion, based on algorithms established by the European Society of Cardiology Diastology Guidelines. This study showed that the association of B-type natriuretic peptide measurement and tissue Doppler echocardiography data is better than the use of those parameters isolated. B-type natriuretic peptide can be useful in identifying patients whose diagnosis of HF had been previously excluded based only on tissue Doppler echocardiographic findings.
Author contributionsConception and design of the research: Jorge AJL, Ribeiro
ML, Mesquita ET; Acquisition of data: Jorge AJL, Ribeiro ML, Fernandes LCM, Freire MD; Analysis and interpretation of the data: Jorge AJL, Rosa MLG, Ribeiro ML; Statistical analysis: Rosa MLG; Writing of the manuscript: Jorge AJL, Correia DS, Teixeira PD, Mesquita ET; Critical revision of the manuscript for intellectual content: Jorge AJL, Rosa MLG, Mesquita ET.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis article is part of the thesis of master submitted by Antonio
Jose Lagoeiro Jorge, from Universidade Federal Fluminense.
236
Original Article
Jorge et al.Diagnosis of HFPEF at the outpatient clinic
Arq Bras Cardiol. 2014; 103(3):231-237
1. Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355(3):251-9.
2. Desai A. Current understanding of heart failure with preserved ejection fraction. Curr Opin Cardiol. 2007;22(6):578-85.
3. Vasan RS, Benjamin EJ, Levy D. Prevalence, clinical features and prognosis of diastolic heart failure: an epidemiologic perspective. J Am Coll Cardiol. 1995;26(7):1565-74.
4. Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJ, et al. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-Preserved Trial. Lancet. 2003;362(9386):777-81.
5. Massie BD, Carson PD, McMurray JD, Komajda M, McKelvie R, Zile MR, et al. Irbesartan in patients with heart failure and preserved ejection fraction. N Engl J Med. 2008;359(23):2456-67.
6. Hsia J, Margolis KL, Eaton CB, Wenger NK, Allison M, Wu L, et al. Prehypertension and cardiovascular disease risk in the Women’s Health Initiative. Circulation. 2007;115(7):855-60.
7. Psaty BM, Lumley T, Furberg CD, Schellenbaum G, Pahor M, Alderman MH, et al. Health outcomes associated with various antihypertensive therapies used as first-line agents: a network meta-analysis. JAMA. 2003;289(19):2534-44.
8. Beckett NS, Peters R, Fletcher AE, Staessen JA Liu L, Dumitrascu D, et al; HYVET Study Group. Treatment of hypertension in patients 80 years of age or older. N Engl J Med. 2008;358(18):1887-98.
9. Paulus WJ, Tschöpe C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;28(20):2539-50.
10. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al, Recommendations for chamber quantification. Eur J Echocardiogr. 2006;7(2):79-108.
11. Fonseca C, Morais H, Mota T, Matias F, Costa C, Gouveia-Oliveira A, et al. The diagnosis of heart failure in primary care: value of symptoms and signs. Eur J Heart Fail. 2004;6(6):795-800, 821-2.
12. Dokainish H, Zoghbi WA, Lakkis NM, Al-Bakshy F, Dhir M, Quinones MA, et al. Optimal noninvasive assessment of left ventricular filling pressures: a comparison of tissue Doppler echocardiography and B-type natriuretic peptide in patients with pulmonary artery catheters. Circulation. 2004;109(20):2432-9.
13. Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, et al. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A comparative simultaneous Doppler-catheterization study. Circulation. 2000;102(15):1788-94.
14. Emery WT, Jadavji I, Choy JB, Lawrance RA. Investigating the European Society of Cardiology Diastology Guidelines in a practical scenario. Eur J Echocardiogr. 2008;9:685-91.
15. Maisel AS, McCord J, Nowak RM, Hollander JE, Wu AH, Duc P, et al; Breathing Not Properly Multinational Study Investigators. Bedside B-type natriuretic peptide in the emergency diagnosis of heart failure with reduced or preserved ejection fraction. J Am Coll Cardiol. 2003;41(11):2010-7.
16. Andrea R, Falces C, Sanchis L, Sitges M, Heras M, Brugada J. Diagnostico de la insuficiencia cardíaca con fraccion de eyeccion preservada o reducida mediante una consulta de alta resolucion. Aten Primaria. 2013;45(4):184-92.
17. McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Bohm M, Dickstein K, et al; ESC Committee for Practice Guidelines. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33(14):1787-847. Erratum in Eur Heart J. 2013;34(2):158.
18. Thomas MD, Fox KF, Coats AJS, Sutton GC. The epidemiological enigma of heart failure with preserved systolic function. Eur J Heart Fail. 2004;6(2):125-36.
19. Yamamoto K, Burnett Jr JC, Jougasaki M, Nishimura RA, Bailey KR, Saito Y, et al. Superiority of brain natriuretic peptide as a hormonal marker of ventricular systolic and diastolic dysfunction and ventricular hypertrophy. Hypertension. 1996;28(6):988-94.
References
237
Original Article
Elevated Blood Pressure and Obesity in Childhood: A Cross-Sectional Evaluation of 4,609 SchoolchildrenCaroline Filla Rosaneli1, Cristina Pellegrio Baena1, Flavia Auler1, Alika Terumi Arasaki Nakashima1, Edna Regina Netto-Oliveira2, Amauri Bássoli Oliveira2, Luiz Cesar Guarita-Souza1, Marcia Olandoski1, Jose Rocha Faria-Neto1
Pontíficia Universidade Catolica do Paraná1, Curitiba, PR; Universidade Estadual de Maringá2, Maringá, PR - Brazil
Mailing Address: José Rocha Faria-Neto •Escola de Medicina - PUCPR - Rua Imaculada Conceição, 1155, Prado Velho. Postal Code 80215-901, Curitiba, PR – BrazilE-mail: [email protected] received November 16, 2013; revised manuscript April 27, 2014; accepted May 09, 2014.
DOI: 10.5935/abc.20140104
Abstract
Background: The incidence of obesity in children is increasing worldwide, primarily in urbanized, high-income countries, and hypertension development is a detrimental effect of this phenomenon.
Objective: In this cross-sectional study, we evaluated the prevalence of excess weight and its association with high blood pressure (BP) in schoolchildren.
Methods: Here 4,609 male and female children, aged 6 to 11 years, from 24 public and private schools in Maringa, Brazil, were evaluated. Nutritional status was assessed by body mass index (BMI) according to cutoff points adjusted for sex and age. Blood pressure (BP) levels above 90th percentile for gender, age and height percentile were considered elevated.
Results: The prevalence of excess weight among the schoolchildren was 24.5%; 16.9% were overweight, and 7.6% were obese. Sex and socioeconomic characteristics were not associated with elevated BP. In all age groups, systolic and diastolic BP correlated with BMI and waist and hip measurements, but not with waist-hip ratio. The prevalence of elevated BP was 11.2% in eutrophic children, 20.6% in overweight children [odds ratio (OR), 1.99; 95% confidence interval (CI), 1.61–2.45], and 39.7% in obese children (OR, 5.4; 95% CI, 4.23–6.89).
Conclusion: Obese and overweight children had a higher prevalence of elevated BP than normal-weight children. Our data confirm that the growing worldwide epidemic of excess weight and elevated BP in schoolchildren may also be ongoing in Brazil. (Arq Bras Cardiol. 2014; 103(3):238-244)
Keywords: Hypertension; Pediatric Obesity; Child; Prevalence; Epidemiology.
IntroductionThe incidence of obesity and high blood pressure (BP)
has increased considerably in children and adolescents and is strongly associated with the development of further disease in adulthood1-7 Moreover, because the incidence of obesity is rising in early phases of life, certain diseases, such as hypertension and diabetes, are becoming a public health issue.
In the 1990s, the prevalence of hypertension among children and adolescents was approximately 2 to 3%8. Currently, the prevalence varies from 1 to 13% depending on the methodology used9. Because obesity has become epidemic in developing countries, the incidence of hypertension also may be increasing. Recognition and awareness of this problem are needed to encourage development of future preventive strategies against excess weight and its complications.
Brazil has intrinsic discrepancies and socioeconomic inequalities in common with other developing nations. In Brazil, there have been few studies showing a correlation between BP and obesity in children. Thus, the purpose of the present cross-sectional study was to evaluate the prevalence of excess weight and its association with high BP in schoolchildren.
MethodsThis study was designed using the national register
of children enrolled in schools in the metropolitan area of Maringa, a city in southern Brazil with a high Human Development Index (0.841) and a high Gini Index (0.56). Maringa has an economy primarily based on agriculture, commerce, and services. At the time this study was planned, Maringa had a population of approximately 356,000 people and 24,723 students between the ages of 6 and 11 years.
In 2006, there were 202 schools in the city of Maringa (public and private schools in the urban area) with an enrollment of 22,302 children aged 6.0 to 11 years. For sample size calculation, considering that the expected prevalence of excess weight was unknown because of the lack of previous studies in the area, the prevalence was set to 50% as this value would produce the largest sample size (confidence limits 2% and
238

Original Article
Rosaneli et al.Obesity and hypertension in children
Arq Bras Cardiol. 2014; 103(3):238-244
confidence level 95%). A clustering sampling was performed considering each school as a sampling unit. Accordingly, the city was divided into 4 different geographical quadrants by taking the municipal cathedral located in the middle of the city as the intersection point of the north–south/east–west dividing line. Fifteen percent of the schools in the city were randomly selected and were selected according to the proportion of schools in each quadrant; the proportion between private and public schools was also considered. In anticipation of possible losses, 30% more children than the calculated sample size were invited to participate in the study (a total of 5,345 children from 24 schools). Data collection occurred between March and December 2006.
This cross-sectional study was approved by the Ethics Committee of the Universidade Estadual de Maringa (n. 016/2006) according to the norms of Resolution 196/96 of the National Health Council regarding research involving human beings.
The students enrolled in the selected schools and grades were notified of the study and instructed to take a term of consent document and questionnaire to their parent or guardian to obtain permission to participate in the study. One week later, the children were asked to hand in the signed authorization and evaluated at the school.
Children younger than 6 or older than 11 years were evaluated to avoid peer resentment, but their data were not entered in the sample. Children who either refused, did not receive authorization from their parent or guardian, whose forms were not filled out completely, or were absent from class on the day scheduled for data collection were excluded from the study.
Data collectionData collection was performed in the school environment
(in private classrooms) at prescheduled hours during a school day by a team of previously trained professionals10; these professionals were members of the Studies in Obesity and Exercise Research Group of the Universidade Estadual de Maringa (GREPO/UEM).
BP was measured and classified as proposed by the 4th Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents11 and was measured after the child had been lying down for at least 5 min, with the 2 measurements made 10 min apart. Values for sex, height, and age below the 90th percentile were considered normotensive, those between the 90th and 95th percentile were considered borderline, and those at the 95th percentile and above were considered to be elevated. The outcome measured in this study was elevated BP, which was determined for the elevated and borderline groups.
Weight and height measurements were performed in triplicate, and the mean value was used. The procedures used for weight and height evaluation followed those proposed by the World Health Organization12. The equipment used included a Tanita digital scale (Model 2202), with a capacity of 136 kg and ability to measure to the nearest 100 g, and a SECA stadiometer (Bodymeter 206). The nutritional profile was classified by body mass index (BMI) according to cutoff points adjusted for sex and age, as proposed by Cole13,14.
Waist and hip circumferences were obtained by using a metallic measuring tape with an accuracy of 0.1 mm, following the norms described previously15. These waist and hip parameters allowed construction of the waist-to-hip ratio (WHR), which was the quotient obtained by dividing the waist circumference by the hip circumference.
Socioeconomic level was determined according to the Brazilian Association of Research Firms (ABEP) criteria16, which considered the presence of consumer goods and educational level of the head of the household. As proposed in the ABEP criteria, educational level was classified as illiterate, primary education, middle education, high school, or superior (university). For our analysis, we divided the children into 2 groups according to heads of households with lower (illiterate, primary, and middle) and higher (high school and university) degree of education. In addition, for analysis purposes, the socioeconomic level was regrouped as follows: level A (classes A1 and A2), level B (classes B1 and B2), level C (C1 and C2), and level D, with A being the highest level and D being the lowest. Inconsistent data in the socioeconomic level of the household head were excluded only for these items.
Statistical analysisDescriptive statistical values were described as means ±
standard deviations (SDs) (quantitative variables) or frequencies and percentages (qualitative variables). Pearson’s correlation coefficients were estimated to evaluate the association between systolic and diastolic BP and anthropometric measures. For quantitative variables, one-way ANOVA was used to compare groups defined by BMI (underweight, eutrophic, overweight, and obese). Student’s t test was used to compare groups defined by BP levels. The chi-square test was used for comparing qualitative variables among groups. The logistic regression model was adjusted to assess factors associated with normal or borderline/elevated BP. All assumptions of logistic regression were checked and met. Variables with statistical significance in the univariate analysis were included in the multivariable model, and the results are shown as ORs [95% confidence interval (CI)]. Statistical significance was set at p < 0.05. SPSS v.14.0 software was used for data analysis.
ResultsThe characteristics of the 4,609 schoolchildren between
6 and 11 years of age enrolled in the study were analyzed with regard to their nutritional status (Table 1). In this study, 99.8% of the children declared their race to be white. Population age, type of school health behaviors, and socioeconomic status of the family were recorded.
Fifty-three percent of the children were female, and 78% were studying in public schools. Excess of weight was found in 24.5% of the sample; 16.9% of the children were overweight and 7.6% were obese. Being overweight was more prevalent in males than in females (p = 0.008). The prevalence of being overweight was higher in private than in public schools (22.2% and 15.4%, respectively, p < 0.001), and the distribution of weight varied significantly according to socioeconomic status stratum (p < 0.001).
239
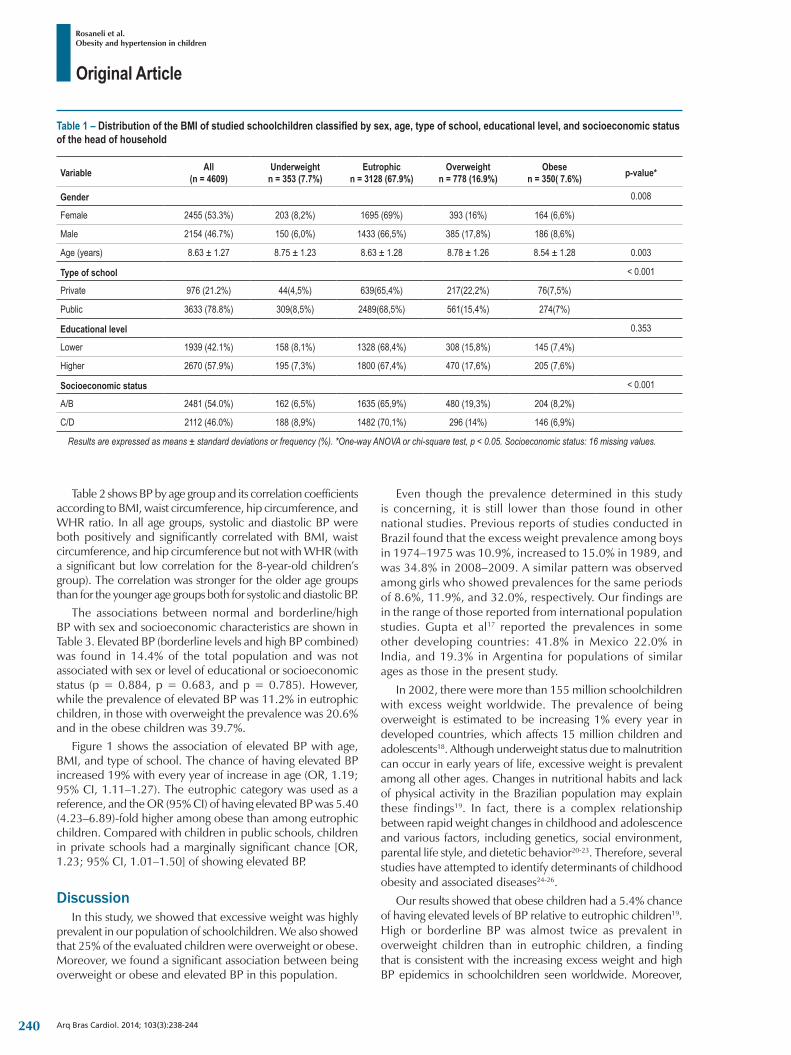
Original Article
Rosaneli et al.Obesity and hypertension in children
Arq Bras Cardiol. 2014; 103(3):238-244
Table 1 – Distribution of the BMI of studied schoolchildren classified by sex, age, type of school, educational level, and socioeconomic status of the head of household
Variable All(n = 4609)
Underweightn = 353 (7.7%)
Eutrophicn = 3128 (67.9%)
Overweightn = 778 (16.9%)
Obesen = 350( 7.6%) p-value*
Gender 0.008
Female 2455 (53.3%) 203 (8,2%) 1695 (69%) 393 (16%) 164 (6,6%)
Male 2154 (46.7%) 150 (6,0%) 1433 (66,5%) 385 (17,8%) 186 (8,6%)
Age (years) 8.63 ± 1.27 8.75 ± 1.23 8.63 ± 1.28 8.78 ± 1.26 8.54 ± 1.28 0.003
Type of school < 0.001
Private 976 (21.2%) 44(4,5%) 639(65,4%) 217(22,2%) 76(7,5%)
Public 3633 (78.8%) 309(8,5%) 2489(68,5%) 561(15,4%) 274(7%)
Educational level 0.353
Lower 1939 (42.1%) 158 (8,1%) 1328 (68,4%) 308 (15,8%) 145 (7,4%)
Higher 2670 (57.9%) 195 (7,3%) 1800 (67,4%) 470 (17,6%) 205 (7,6%)
Socioeconomic status < 0.001
A/B 2481 (54.0%) 162 (6,5%) 1635 (65,9%) 480 (19,3%) 204 (8,2%)
C/D 2112 (46.0%) 188 (8,9%) 1482 (70,1%) 296 (14%) 146 (6,9%)
Results are expressed as means ± standard deviations or frequency (%). *One-way ANOVA or chi-square test, p < 0.05. Socioeconomic status: 16 missing values.
Table 2 shows BP by age group and its correlation coefficients according to BMI, waist circumference, hip circumference, and WHR ratio. In all age groups, systolic and diastolic BP were both positively and significantly correlated with BMI, waist circumference, and hip circumference but not with WHR (with a significant but low correlation for the 8-year-old children’s group). The correlation was stronger for the older age groups than for the younger age groups both for systolic and diastolic BP.
The associations between normal and borderline/high BP with sex and socioeconomic characteristics are shown in Table 3. Elevated BP (borderline levels and high BP combined) was found in 14.4% of the total population and was not associated with sex or level of educational or socioeconomic status (p = 0.884, p = 0.683, and p = 0.785). However, while the prevalence of elevated BP was 11.2% in eutrophic children, in those with overweight the prevalence was 20.6% and in the obese children was 39.7%.
Figure 1 shows the association of elevated BP with age, BMI, and type of school. The chance of having elevated BP increased 19% with every year of increase in age (OR, 1.19; 95% CI, 1.11–1.27). The eutrophic category was used as a reference, and the OR (95% CI) of having elevated BP was 5.40 (4.23–6.89)-fold higher among obese than among eutrophic children. Compared with children in public schools, children in private schools had a marginally significant chance [OR, 1.23; 95% CI, 1.01–1.50] of showing elevated BP.
DiscussionIn this study, we showed that excessive weight was highly
prevalent in our population of schoolchildren. We also showed that 25% of the evaluated children were overweight or obese. Moreover, we found a significant association between being overweight or obese and elevated BP in this population.
Even though the prevalence determined in this study is concerning, it is still lower than those found in other national studies. Previous reports of studies conducted in Brazil found that the excess weight prevalence among boys in 1974–1975 was 10.9%, increased to 15.0% in 1989, and was 34.8% in 2008–2009. A similar pattern was observed among girls who showed prevalences for the same periods of 8.6%, 11.9%, and 32.0%, respectively. Our findings are in the range of those reported from international population studies. Gupta et al17 reported the prevalences in some other developing countries: 41.8% in Mexico 22.0% in India, and 19.3% in Argentina for populations of similar ages as those in the present study.
In 2002, there were more than 155 million schoolchildren with excess weight worldwide. The prevalence of being overweight is estimated to be increasing 1% every year in developed countries, which affects 15 million children and adolescents18. Although underweight status due to malnutrition can occur in early years of life, excessive weight is prevalent among all other ages. Changes in nutritional habits and lack of physical activity in the Brazilian population may explain these findings19. In fact, there is a complex relationship between rapid weight changes in childhood and adolescence and various factors, including genetics, social environment, parental life style, and dietetic behavior20-23. Therefore, several studies have attempted to identify determinants of childhood obesity and associated diseases24-26.
Our results showed that obese children had a 5.4% chance of having elevated levels of BP relative to eutrophic children19. High or borderline BP was almost twice as prevalent in overweight children than in eutrophic children, a finding that is consistent with the increasing excess weight and high BP epidemics in schoolchildren seen worldwide. Moreover,
240
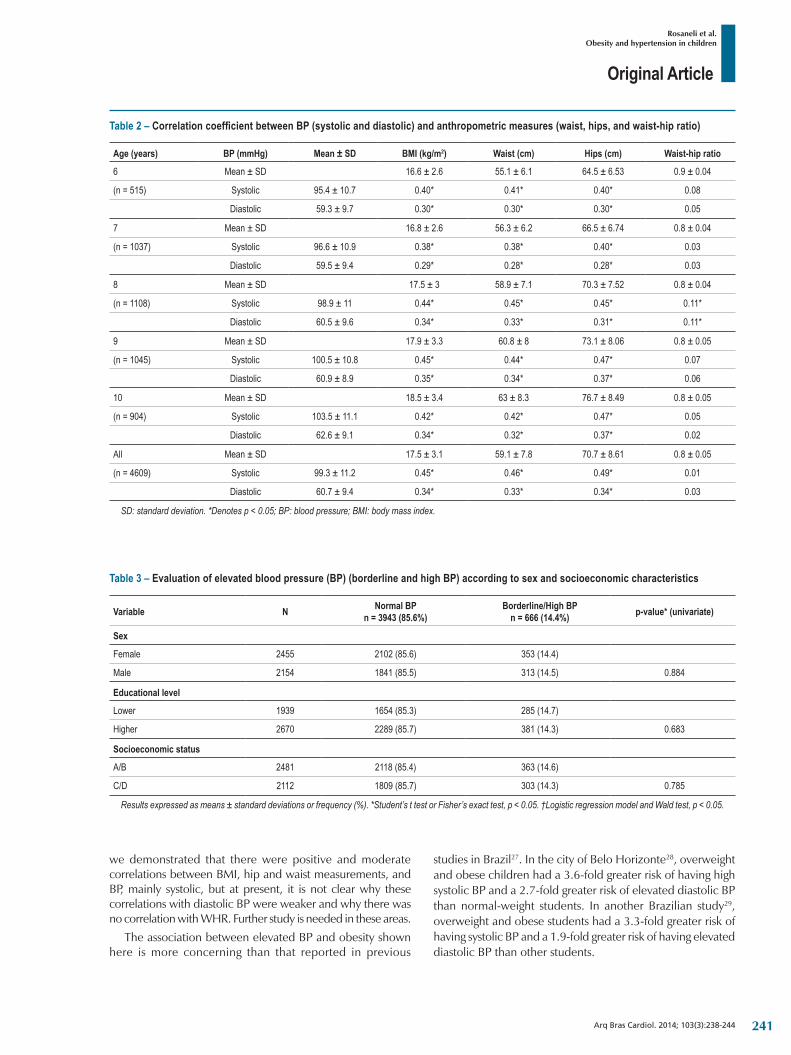
Original Article
Rosaneli et al.Obesity and hypertension in children
Arq Bras Cardiol. 2014; 103(3):238-244
Table 2 – Correlation coefficient between BP (systolic and diastolic) and anthropometric measures (waist, hips, and waist-hip ratio)
Age (years) BP (mmHg) Mean ± SD BMI (kg/m2) Waist (cm) Hips (cm) Waist-hip ratio
6 Mean ± SD 16.6 ± 2.6 55.1 ± 6.1 64.5 ± 6.53 0.9 ± 0.04
(n = 515) Systolic 95.4 ± 10.7 0.40* 0.41* 0.40* 0.08
Diastolic 59.3 ± 9.7 0.30* 0.30* 0.30* 0.05
7 Mean ± SD 16.8 ± 2.6 56.3 ± 6.2 66.5 ± 6.74 0.8 ± 0.04
(n = 1037) Systolic 96.6 ± 10.9 0.38* 0.38* 0.40* 0.03
Diastolic 59.5 ± 9.4 0.29* 0.28* 0.28* 0.03
8 Mean ± SD 17.5 ± 3 58.9 ± 7.1 70.3 ± 7.52 0.8 ± 0.04
(n = 1108) Systolic 98.9 ± 11 0.44* 0.45* 0.45* 0.11*
Diastolic 60.5 ± 9.6 0.34* 0.33* 0.31* 0.11*
9 Mean ± SD 17.9 ± 3.3 60.8 ± 8 73.1 ± 8.06 0.8 ± 0.05
(n = 1045) Systolic 100.5 ± 10.8 0.45* 0.44* 0.47* 0.07
Diastolic 60.9 ± 8.9 0.35* 0.34* 0.37* 0.06
10 Mean ± SD 18.5 ± 3.4 63 ± 8.3 76.7 ± 8.49 0.8 ± 0.05
(n = 904) Systolic 103.5 ± 11.1 0.42* 0.42* 0.47* 0.05
Diastolic 62.6 ± 9.1 0.34* 0.32* 0.37* 0.02
All Mean ± SD 17.5 ± 3.1 59.1 ± 7.8 70.7 ± 8.61 0.8 ± 0.05
(n = 4609) Systolic 99.3 ± 11.2 0.45* 0.46* 0.49* 0.01
Diastolic 60.7 ± 9.4 0.34* 0.33* 0.34* 0.03
SD: standard deviation. *Denotes p < 0.05; BP: blood pressure; BMI: body mass index.
Table 3 – Evaluation of elevated blood pressure (BP) (borderline and high BP) according to sex and socioeconomic characteristics
Variable N Normal BPn = 3943 (85.6%)
Borderline/High BPn = 666 (14.4%) p-value* (univariate)
Sex
Female 2455 2102 (85.6) 353 (14.4)
Male 2154 1841 (85.5) 313 (14.5) 0.884
Educational level
Lower 1939 1654 (85.3) 285 (14.7)
Higher 2670 2289 (85.7) 381 (14.3) 0.683
Socioeconomic status
A/B 2481 2118 (85.4) 363 (14.6)
C/D 2112 1809 (85.7) 303 (14.3) 0.785
Results expressed as means ± standard deviations or frequency (%). *Student’s t test or Fisher’s exact test, p < 0.05. †Logistic regression model and Wald test, p < 0.05.
we demonstrated that there were positive and moderate correlations between BMI, hip and waist measurements, and BP, mainly systolic, but at present, it is not clear why these correlations with diastolic BP were weaker and why there was no correlation with WHR. Further study is needed in these areas.
The association between elevated BP and obesity shown here is more concerning than that reported in previous
studies in Brazil27. In the city of Belo Horizonte28, overweight and obese children had a 3.6-fold greater risk of having high systolic BP and a 2.7-fold greater risk of elevated diastolic BP than normal-weight students. In another Brazilian study29, overweight and obese students had a 3.3-fold greater risk of having systolic BP and a 1.9-fold greater risk of having elevated diastolic BP than other students.
241
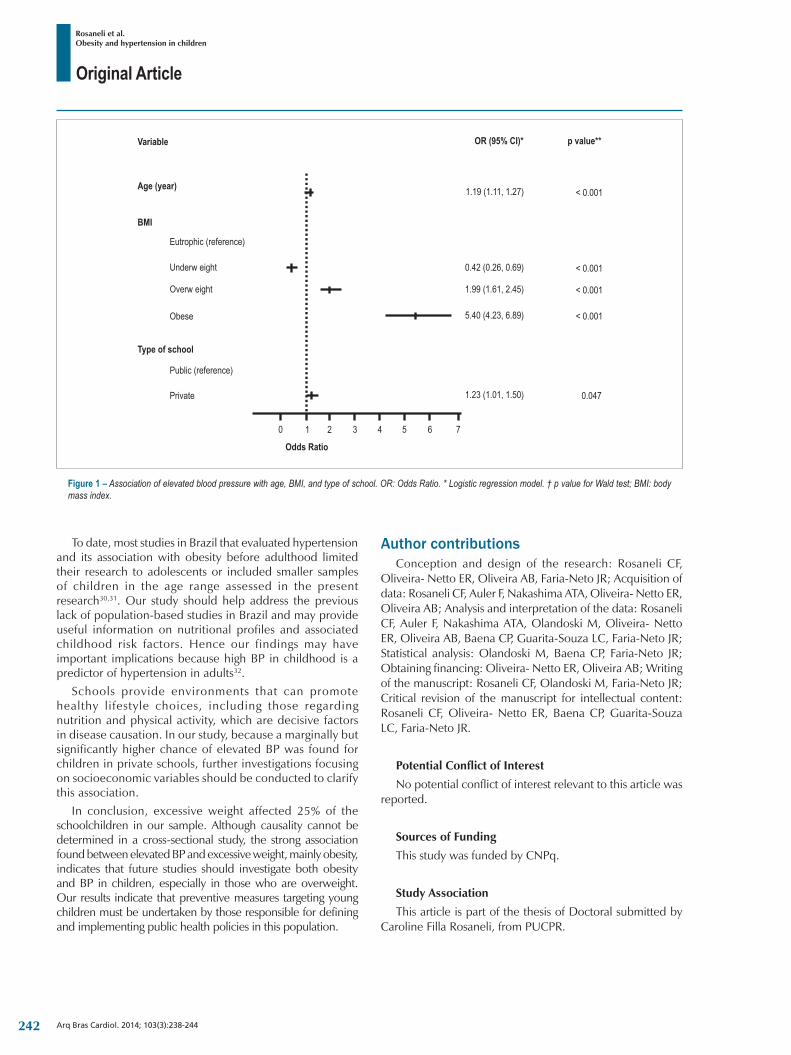
Original Article
Rosaneli et al.Obesity and hypertension in children
Arq Bras Cardiol. 2014; 103(3):238-244
Figure 1 – Association of elevated blood pressure with age, BMI, and type of school. OR: Odds Ratio. * Logistic regression model. † p value for Wald test; BMI: body mass index.
To date, most studies in Brazil that evaluated hypertension and its association with obesity before adulthood limited their research to adolescents or included smaller samples of children in the age range assessed in the present research30,31. Our study should help address the previous lack of population-based studies in Brazil and may provide useful information on nutritional profiles and associated childhood risk factors. Hence our findings may have important implications because high BP in childhood is a predictor of hypertension in adults32.
Schools provide environments that can promote healthy lifestyle choices, including those regarding nutrition and physical activity, which are decisive factors in disease causation. In our study, because a marginally but significantly higher chance of elevated BP was found for children in private schools, further investigations focusing on socioeconomic variables should be conducted to clarify this association.
In conclusion, excessive weight affected 25% of the schoolchildren in our sample. Although causality cannot be determined in a cross-sectional study, the strong association found between elevated BP and excessive weight, mainly obesity, indicates that future studies should investigate both obesity and BP in children, especially in those who are overweight. Our results indicate that preventive measures targeting young children must be undertaken by those responsible for defining and implementing public health policies in this population.
Author contributionsConception and design of the research: Rosaneli CF,
Oliveira- Netto ER, Oliveira AB, Faria-Neto JR; Acquisition of data: Rosaneli CF, Auler F, Nakashima ATA, Oliveira- Netto ER, Oliveira AB; Analysis and interpretation of the data: Rosaneli CF, Auler F, Nakashima ATA, Olandoski M, Oliveira- Netto ER, Oliveira AB, Baena CP, Guarita-Souza LC, Faria-Neto JR; Statistical analysis: Olandoski M, Baena CP, Faria-Neto JR; Obtaining financing: Oliveira- Netto ER, Oliveira AB; Writing of the manuscript: Rosaneli CF, Olandoski M, Faria-Neto JR; Critical revision of the manuscript for intellectual content: Rosaneli CF, Oliveira- Netto ER, Baena CP, Guarita-Souza LC, Faria-Neto JR.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
This study was funded by CNPq.
Study Association
This article is part of the thesis of Doctoral submitted by Caroline Filla Rosaneli, from PUCPR.
242
Original Article
Rosaneli et al.Obesity and hypertension in children
Arq Bras Cardiol. 2014; 103(3):238-244
1. Constantine E, Merritt C. Hypertensive emergencies in children: Identification and management of dangerously high blood pressure. Minerva Pediatr. 2009;61(2):175-84.
2. Monego ET, Jardim PC. Determinants of risk of cardiovascular diseases in schoolchildren. Arq Bras Cardiol. 2006;87(1):37-45.
3. Burke V, Beilin LJ, Dunbar D, Kevan M. Associations between blood pressure and overweight defined by new standards for body mass index in childhood. Prev Med. 2004;38(5):558-64.
4. Sharma M. School-based interventions for childhood and adolescent obesity. Obes Rev. 2006;7(3):261-9.
5. Barba G, Troiano E, Russo P, Strazzullo P, Siani A. Body mass, fat distribution and blood pressure in southern italian children: Results of the arca project. Nutr Metab Cardiovasc Dis. 2006;16(4):239-48.
6. Ribeiro JC, Guerra S, Oliveira J, Andersen LB, Duarte JA, Mota J. Body fatness and clustering of cardiovascular disease risk factors in portuguese children and adolescents. Am J Hum Biol. 2004;16(5):556-62.
7. Williams CL, Hayman LL, Daniels SR, Robinson TN, Steinberger J, Paridon S, et al. Cardiovascular health in childhood: a statement for health professionals from the Committee on Atherosclerosis, Hypertension, and Obesity in the Young (AHOY) of the Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2002;106(1):143-60. Erratum in Circulation. 2002;106(9):1178.
8. Rosa AA, Ribeiro JP. High blood pressure in children and adolescents: determinant factors. J Pediatr (Rio J). 1999;75(2):75-82.
9. Salgado CM, Carvalhaes JTA. Hipertensão arterial na infância. J Pediatr (Rio J). 2003;79 Suppl 1:S115-24.
10. Oliveira-Filho A, Oliveira AA, Oliveira ER, Kurata DM, Pineda M. Variabilidade intra-avaliador e interavaliadores de medidas antropometricas. Acta Sci Health Sci. 2007;29 (1):1-5.
11. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114(Suppl 2):555-76.
12. Physical status: the use and interpretation of anthropometry. Report of a who expert committee. World Health Organ Tech Rep Ser. 1995;854:1-452.
13. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ. 2000;320(7244):1240-3.
14. Cole TJ, Flegal KM, Nicholls D, Jackson AA. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ. 2007;335(7612):194.
15. Lohman TG, Roche AF, Martorell R. Anthropometric standardization reference manual. Champaign (IL): Human Kinetics Books; 1988.
16. Associação Brasileira de Empresas de Pesquisa (ABEP). Criterio de classificação econômica 2008. São Paulo; 2008.
17. Gupta N, Goel K, Shah P, Misra A. Childhood obesity in developing countries: Epidemiology, determinants, and prevention. Endocr Rev. 2012;33(1):48-70.
18. Lobstein T, Baur L, Uauy R; IASO International Obesity TaskForce. Obesity in children and young people: a crisis in public health. Obes Rev. 2004;5 Suppl 1:4-104.
19. Ministerio da Saúde. Pesquisa de orçamentos familiares 2008-2009: antropometria e estado nutricional de crianças, adolescentes e adultos no Brasil. Brasília; 2010.
20. Nunes MM, Figueiroa JN, Alves JG. Overweight, physical activity and foods habits in adolescents from different economic levels, Campina Grande (PB). Rev Assoc Med Bras. 2007;53(2):130-4.
21. Taveras EM, Berkey CS, Rifas-Shiman SL, Ludwig DS, Rockett HR, Field AE, et al. Association of consumption of fried food away from home with body mass index and diet quality in older children and adolescents. Pediatrics. 2005;116(4):e518-24.
22. Monteiro P, Victora C, Barros F. Fatores de risco sociais, familiares e comportamentais para obesidade em adolescentes. Rev Panam Salud Publica. 2004;16(4):250-8.
23. Coon KA, Goldberg J, Rogers BL, Tucker KL. Relationships between use of television during meals and children’s food consumption patterns. Pediatrics. 2001;107(1):E7.
24. Araújo TL, Lopes MV, Cavalcante TF, Guedes NG, Moreira RP, Chaves ES, et al. Análise de indicadores de risco para hipertensão arterial em crianças e adolescentes. Rev Esc Enferm USP. 2008:42(1):20-6.
25. Molina Mdel C, Faria CP, Montero MP, Cade NV, Mill JG. Cardiovascular risk factors in 7-to-10-year-old children in Vitoria, Espirito Santo state, Brazil. Cad Saude Publica. 2010;26(5):909-17.
26. Rosaneli CF, Auler F, Manfrinato CB, Rosaneli CF, Sganzerla C, Bonatto MG, et al. Evaluation of the prevalence and nutritional and social determinants of overweight in a population of schoolchildren: a cross-sectional analysis of 5,037 children. Rev Assoc Med Bras. 2012;58(4):472-6.
27. Pinto SL, Silva RdCR, Priore SE, Assis AM, Pinto EdJ. Prevalence of pre-hypertension and arterial hypertension and evaluation of associated factors in children and adolescents in public schools in Salvador, Bahia State, Brazil. Cad Saude Publica. 2011;27(6):1065-76.
28. Ribeiro RQ, Lotufo PA, Lamounier JA, Oliveira RG, Soares JF, Botter DA. Additional cardiovascular risk factors associated with excess weight in children and adolescents: the Belo Horizonte heart study. Arq Bras Cardiol. 2006;86(6):408-18.
29. Ribeiro RC, Coutinho M, Bramorski MA, Giuliano IC, Pavan J. Association of the waist-to-height ratio with cardiovascular risk factors in children and adolescents: the three cities heart study. Int J Prev Med. 2010;1(1):39-49.
30. Christofaro DG, Andrade SM, Fernandes RA, Ohara D, Dias DF, Freitas Júnior IF, et al. Prevalencia de fatores de risco para doenças cardiovasculares entre escolares em londrina - pr: Diferenças entre classes econômicas. Rev Bras Epidemiol. 2011;14 (1):27-35.
31. Alvarez MM, Vieira AC, Sichieri R, Veiga GV. Prevalence of metabolic syndrome and of its specific components among adolescents from Niteroi city, Rio de Janeiro state, Brazil. Arq Bras Endocrinol Metabol. 2011;55(2):164-70.
32. Beck CC, Lopes AS, Pitanga FJ. Anthropometric indicators as predictors of high blood pressure in adolescents. Arq Bras Cardiol. 2011;96(2):126-33.
References
243
Original Article
Rosaneli et al.Obesity and hypertension in children
Arq Bras Cardiol. 2014; 103(3):238-244244

Original Article
Comparison of Postprandial Lipemia between Women who are on Oral Contraceptive Methods and Those who are notJefferson Petto1,2, Leila Monique Reis Vasques2, Renata Leão Pinheiro2, Beatriz de Almeida Giesta2, Alan Carlos Nery dos Santos2, Mansueto Gomes Neto2, Ana Marice Teixeira Ladeia1
Escola Bahiana de Medicina e Saúde Pública1; Faculdade Social da Bahia, Grupo de Pesquisa em Cardiologia2, Salvador, BA - Brazil
Mailing Address: Jefferson Petto •Av. Dom João VI, 275 - Brotas. Postal Code: 44657-086 - Salvador, BA – Brazil.E-mail: [email protected] received February 02, 2014; revised manuscript July 03/, 2014; accepted March 17, 2014.
DOI: 10.5935/abc.20140080
Abstract
Background: Postprandial Lipemia (PPL) is a physiological process that reflects the ability of the body to metabolize lipids. Even though the influence of oral contraceptives (OC) on PPL is not known, it is a known fact that their use increases fasting lipid values.
Objective: To compare the PPL between women who are on OC and those who are not.
Methods: A prospective analytical study which assessed eutrophic women, aged between 18 and 28 years old, who were irregularly active and with fasting triglycerides ≤150 mg/dL. They were divided into two groups: oral contraceptive group (COG) and non-oral contraceptive group (NCOG). Volunteers were submitted to the PPL test, in which blood samples were collected in time 0 (12-hour fasting) and after the intake of lipids in times 180 and 240 minutes. In order to compare the triglyceride deltas, which reflect PPL, the two-tailed Mann-Whitney test was used for independent samples between fasting collections and 180 minutes (∆1) and between fasting and 240 minutes (∆2).
Results: Forty women were assessed and equally divided between groups. In the fasting lipid profile, it was observed that HDL did not present significant differences and that triglycerides in COG were twice as high in comparison to NCOG. Medians of ∆1 and ∆2 presented significant differences in both comparisons (p ≤0.05).
Conclusion: The results point out that women who are irregularly active and use OC present more PPL in relation to those who do not use OC, which suggests that in this population, its chronic use increases the risk of heart conditions. (Arq Bras Cardiol. 2014; 103(3):245-250)
Keywords: Contraceptives, Oral; Women; Metabolism; Insulin; Triglycerides; Cholesterol.
IntroductionPostprandial lipemia (PPL) is a physiological process
defined as the increased plasma triglyceride and esterified lipoprotein concentration after the intake of fats1. It reflects the ability of the body to metabolize lipids, being also known as postprandial clearance. In healthy adults, its peak is reached in the third or fourth hour after the intake of fats, and its cycle is completed between the sixth and the eighth hour2,3.
It began to be studied in the 1950s, however, it was first described in 1979, by Zilversmit, who reported the existence of a strong connection between PPL and the atherosclerotic process4. Currently, this relationship is well established, and the atherosclerotic disease is defined as a postprandial event5,6.
The magnitude and the amplitude of PPL are multifactorial, usually being prolonged for men7, showing increasing
tendency with age8, in carbohydrate-rich diets9, among smokers10 and obese people11. It is less common in physically active individuals12 and more present among diabetic13,14 and dyslipidemic patients15.
Even though up until now the influence of oral contraceptives (OC) on PPL is not known, some studies16-21 show that its use causes triglycerides to increase, as well as total cholesterol and low density lipoprotein, even at low-doses17. Therefore, this study aimed at comparing PPL of women who use OC and those who do not use it.
MethodsA prospective analytical study which assessed eutrophic
women aged from 18 to 28 years old, classified as being irregularly active by the long version of the International Physical Activity Questionnaire22, with fasting triglycerides ≤ 150 mg/dL.
Diabetic women, those who are dyslipidemic on drug treatment, with renal disease, with diagnosed hypo/hyperthyroidism, history of drunkenness or smoking, in a hypo/hypercaloric diet and on corticosteroids, diuretics or beta blockers were excluded. Sample calculation was conducted by considering alpha = 0.05 (bidirectional) and beta = 0.80, adopting a significant difference of 20% for
245

Original Article
Petto et al.Postprandial lipemia and oral contraceptive
Arq Bras Cardiol. 2014; 103(3):245-250
PPL between groups. Considering that the coefficient of variation of the triglyceride dose in the laboratory is 5%, and that a difference four times higher than the expected one invalidates this analytical coefficient of variation, 36 volunteers were necessary, that is, 18 volunteers in each group. Sample calculation was performed with GraphPad StatMate 2.0 for Windows.
The sample was composed in accordance with the pre-established criteria, being divided into two groups: oral contraceptive group (COG), formed by volunteers who had been on low-dose estradiol OC (15-30 mcg) for at least one year, and the non-oral contraceptive group (NCOG), composed by women who had not been on any type of hormone-based contraceptives for at least six months.
Data collectionThe selected volunteers answered a standard questionnaire
and were submitted to physical examinations, both aiming at collecting general information about the sample characteristics. The physical examination was comprised of measurements of heart rate and blood pressure at rest, as well as total body mass, height and waist circumference.
A pulse heart meter from Polar was used to measure heart rate. Blood pressure measurement was in accordance with the guidelines of the Brazilian Society of Hypertension23, and the instrument used was a tensiometer for mid-sized adult, calibrated by the National Institute of Metrology, Standardization and Industrial Quality (Inmetro), and a duo-sonic stethoscope, both from BD.
Height was measured by a Sanny professional stadiometer, 0.1 cm accuracy. Participants were barefoot, with gluteus and shoulders leaning on a vertical support. Total body mass was measured by a digital Filizola scale, with maximum capacity of 150 kg, verified by Inmetro, certified to establish the margin of error of ±100 g.
Waist circumference was obtained by a metallic and non-elastic measuring tape from Starrett, with measurement definition of 0.1 cm. The smallest curvature located between the last rib and the iliac crest was measured, without compressing the tissues24.
Body mass index (BMI) was calculated with measurements of mass and height, according to Quetelet’s equation: BMI = mass (kg)/height2 (m). The adopted cutoff points were the ones recommended by the IV Brazilian Guideline for Dyslipidemia and Atherosclerosis prevention, by the Department of Atherosclerosis of Brazilian Society of Cardiology25, that is, low weight (BMI <18.5), eutrophic (18.5 < BMI < 24.9), overweight (25 < BMI < 29.9) and obesity (BMI ≥30).
Postprandial lipemia testAll volunteers were submitted to a PPL test. After the
cannulation of the antecubital vein, blood samples were collected to measure triglycerides in time 0 (12-hour fasting) and after the intake of a substance containing 25 g of fat and of
a diet cereal bar, in times 180 and 240 minutes. Lipoprotein, glutamic pyruvic transaminase, glycemia and total cholesterol were measured only in the fasting period. All collections were performed by a trained professional in a laboratory adapted for this type of procedure.
The lipid compound was provided by Tecnovida and, from the 25 g of lipids, 15 g were monounsaturated, 8 g were poly-unsaturated and 2 g were saturated, which corresponds to 45% of the daily recommended intake of fats for a 2,000 kcal diet. The cereal bar had 0 g of carbohydrates, 1.2 g of proteins and 0.8 g of lipids. The bar was administered so that the intake of the lipid compound would be more palatable and so it would not cause gastric discomfort.
In the PPL test, volunteers were advised not to change their diet in the week of the test and not to practice any unusual physical effort, and also not to consume alcohol in the 24 hours prior to the test. The test was conducted between the fifth and the tenth day of the menstrual cycle, considering the lower hormone flows, and/or on the 28th day without medication (inactive phase), as recommended by Casazza et al26.
The values of triglycerides, total cholesterol and high-density lipoprotein were obtained by the enzymatic method. Values of low-density and very-low density lipoproteins were calculated by the Friedewald equation. Glutamic pyruvic transaminase was measured by the colorimetric method (Reitman-Frankel).
Ethical criteriaDuring the study, the guidelines concerning the research
on human beings in the Declaration of Helsinki and in Resolution 196/96 of the National Health Council were observed. This study was submitted to and approved by the Research Ethics Committee of the Science and Technology School of Salvador (protocol 3390).
All of the participants received detailed information about the objectives of the study, as well as about the risks and benefits involved in the procedures. They signed the informed consent form.
Statistical analysisIn order to verify data distribution, the symmetry and
the kurtosis tests were conducted, as well as Shapiro-Wilk. Deltas (Δ) that reflect PPL, that is, the variation of triglycerides between collection in the fasting period and at 180 min (Δ1) and 240 min (Δ2), did not present normal distribution, and were described as median and quartile interval. Therefore, in order to compare Δ1 and Δ2, the two-tailed Mann-Whitney test was used for independent samples.
The other variables and the peak points of PPL in 180 and 240 minutes presented normal distribution, being described as mean and standard-deviation. The two-tailed unpaired Student’s t-test was applied to compare these variables.
All of the analyses were conducted with the statistical package BioEstat 5.0, with a 5% significance level.
246
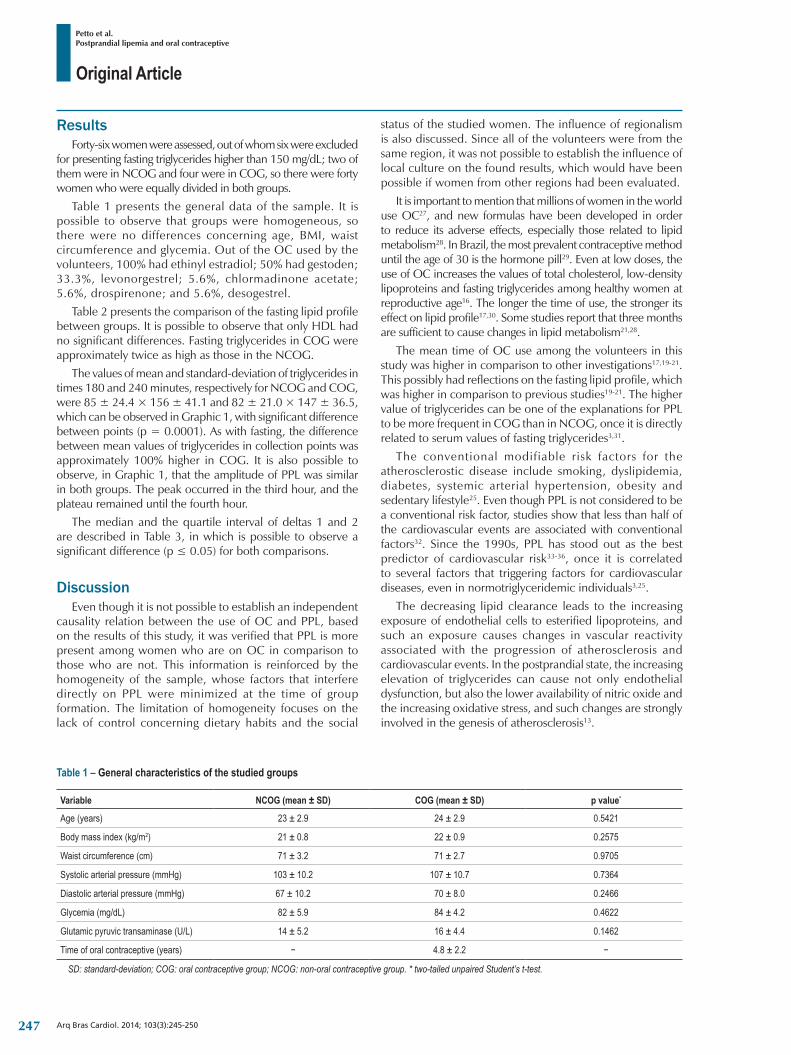
Original Article
Petto et al.Postprandial lipemia and oral contraceptive
Arq Bras Cardiol. 2014; 103(3):245-250
Table 1 – General characteristics of the studied groups
Variable NCOG (mean ± SD) COG (mean ± SD) p value*
Age (years) 23 ± 2.9 24 ± 2.9 0.5421
Bodymassindex(kg/m2) 21 ± 0.8 22 ± 0.9 0.2575
Waist circumference (cm) 71 ± 3.2 71 ± 2.7 0.9705
Systolic arterial pressure (mmHg) 103 ± 10.2 107 ± 10.7 0.7364
Diastolic arterial pressure (mmHg) 67 ± 10.2 70 ± 8.0 0.2466
Glycemia (mg/dL) 82 ± 5.9 84 ± 4.2 0.4622
Glutamic pyruvic transaminase (U/L) 14 ± 5.2 16 ± 4.4 0.1462
Time of oral contraceptive (years) − 4.8 ± 2.2 −
SD: standard-deviation; COG: oral contraceptive group; NCOG: non-oral contraceptive group. * two-tailed unpaired Student’s t-test.
ResultsForty-six women were assessed, out of whom six were excluded
for presenting fasting triglycerides higher than 150 mg/dL; two of them were in NCOG and four were in COG, so there were forty women who were equally divided in both groups.
Table 1 presents the general data of the sample. It is possible to observe that groups were homogeneous, so there were no differences concerning age, BMI, waist circumference and glycemia. Out of the OC used by the volunteers, 100% had ethinyl estradiol; 50% had gestoden; 33.3%, levonorgestrel; 5.6%, chlormadinone acetate; 5.6%, drospirenone; and 5.6%, desogestrel.
Table 2 presents the comparison of the fasting lipid profile between groups. It is possible to observe that only HDL had no significant differences. Fasting triglycerides in COG were approximately twice as high as those in the NCOG.
The values of mean and standard-deviation of triglycerides in times 180 and 240 minutes, respectively for NCOG and COG, were 85 ± 24.4 × 156 ± 41.1 and 82 ± 21.0 × 147 ± 36.5, which can be observed in Graphic 1, with significant difference between points (p = 0.0001). As with fasting, the difference between mean values of triglycerides in collection points was approximately 100% higher in COG. It is also possible to observe, in Graphic 1, that the amplitude of PPL was similar in both groups. The peak occurred in the third hour, and the plateau remained until the fourth hour.
The median and the quartile interval of deltas 1 and 2 are described in Table 3, in which is possible to observe a significant difference (p ≤ 0.05) for both comparisons.
DiscussionEven though it is not possible to establish an independent
causality relation between the use of OC and PPL, based on the results of this study, it was verified that PPL is more present among women who are on OC in comparison to those who are not. This information is reinforced by the homogeneity of the sample, whose factors that interfere directly on PPL were minimized at the time of group formation. The limitation of homogeneity focuses on the lack of control concerning dietary habits and the social
status of the studied women. The influence of regionalism is also discussed. Since all of the volunteers were from the same region, it was not possible to establish the influence of local culture on the found results, which would have been possible if women from other regions had been evaluated.
It is important to mention that millions of women in the world use OC27, and new formulas have been developed in order to reduce its adverse effects, especially those related to lipid metabolism28. In Brazil, the most prevalent contraceptive method until the age of 30 is the hormone pill29. Even at low doses, the use of OC increases the values of total cholesterol, low-density lipoproteins and fasting triglycerides among healthy women at reproductive age16. The longer the time of use, the stronger its effect on lipid profile17,30. Some studies report that three months are sufficient to cause changes in lipid metabolism21,28.
The mean time of OC use among the volunteers in this study was higher in comparison to other investigations17,19-21. This possibly had reflections on the fasting lipid profile, which was higher in comparison to previous studies19-21. The higher value of triglycerides can be one of the explanations for PPL to be more frequent in COG than in NCOG, once it is directly related to serum values of fasting triglycerides3,31.
The conventional modifiable risk factors for the atherosclerostic disease include smoking, dyslipidemia, diabetes, systemic arterial hypertension, obesity and sedentary lifestyle25. Even though PPL is not considered to be a conventional risk factor, studies show that less than half of the cardiovascular events are associated with conventional factors32. Since the 1990s, PPL has stood out as the best predictor of cardiovascular risk33-36, once it is correlated to several factors that triggering factors for cardiovascular diseases, even in normotriglyceridemic individuals3,25.
The decreasing lipid clearance leads to the increasing exposure of endothelial cells to esterified lipoproteins, and such an exposure causes changes in vascular reactivity associated with the progression of atherosclerosis and cardiovascular events. In the postprandial state, the increasing elevation of triglycerides can cause not only endothelial dysfunction, but also the lower availability of nitric oxide and the increasing oxidative stress, and such changes are strongly involved in the genesis of atherosclerosis13.
247
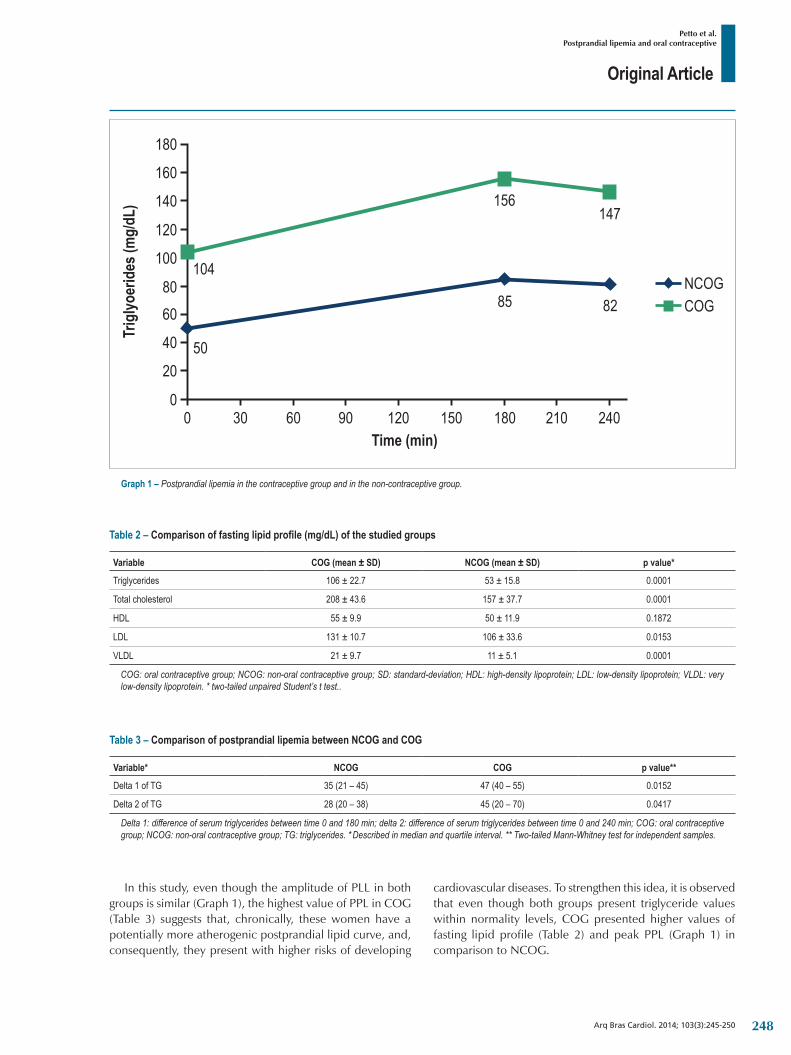
Original Article
Petto et al.Postprandial lipemia and oral contraceptive
Arq Bras Cardiol. 2014; 103(3):245-250
Graph 1 – Postprandial lipemia in the contraceptive group and in the non-contraceptive group.
Table 2 – Comparison of fasting lipid profile (mg/dL) of the studied groups
Variable COG (mean ± SD) NCOG (mean ± SD) p value*
Triglycerides 106 ± 22.7 53 ± 15.8 0.0001
Total cholesterol 208 ± 43.6 157 ± 37.7 0.0001
HDL 55 ± 9.9 50 ± 11.9 0.1872
LDL 131 ± 10.7 106 ± 33.6 0.0153
VLDL 21 ± 9.7 11 ± 5.1 0.0001
COG: oral contraceptive group; NCOG: non-oral contraceptive group; SD: standard-deviation; HDL: high-density lipoprotein; LDL: low-density lipoprotein; VLDL: very low-density lipoprotein. * two-tailed unpaired Student’s t test..
Table 3 – Comparison of postprandial lipemia between NCOG and COG
Variable* NCOG COG p value**
Delta 1 of TG 35 (21 – 45) 47 (40 – 55) 0.0152
Delta 2 of TG 28 (20 – 38) 45 (20 – 70) 0.0417
Delta 1: difference of serum triglycerides between time 0 and 180 min; delta 2: difference of serum triglycerides between time 0 and 240 min; COG: oral contraceptive group; NCOG: non-oral contraceptive group; TG: triglycerides. * Described in median and quartile interval. ** Two-tailed Mann-Whitney test for independent samples.
In this study, even though the amplitude of PLL in both groups is similar (Graph 1), the highest value of PPL in COG (Table 3) suggests that, chronically, these women have a potentially more atherogenic postprandial lipid curve, and, consequently, they present with higher risks of developing
cardiovascular diseases. To strengthen this idea, it is observed that even though both groups present triglyceride values within normality levels, COG presented higher values of fasting lipid profile (Table 2) and peak PPL (Graph 1) in comparison to NCOG.
248

Original Article
Petto et al.Postprandial lipemia and oral contraceptive
Arq Bras Cardiol. 2014; 103(3):245-250
1. Petto J, Batista AKMS, Oliveira CS, Ladeia AMT. Efeito agudo do exercício físico na lipemia pos-prandial: revisão. Rev Bras Fisiologia Exercício. 2012;11:111-4.
2. Petto J, Pereira JA, Britto RP, Sá CK, Souza LA, Ladeia AM. Efeito agudo imediato de uma sessão de exercício físico sobre a lipemia pos-prandial em jovens irregularmente ativos. Rev Bras Cardiol. 2013;26(2):100-5.
3. Lima JG, Nobrega ML, Bandeira F, Sousa AG. Dislipidemia pos-prandial como achado precoce em indivíduos com baixo risco cardiovascular. Arq Bras Endocrinol Metab. 2002; 46(3): 249-254.
4. Zilversmit DB. Atherogenesis: a postprandial phenomenon. Circulation. 1979;60(3):473-85.
5. Santos SC, Canashiro JA, Gebara OC, Aldrighi GJ, Vieira N, Nussbacher A, et al. Efeitos agudos dos estrogenios associados a progestogenios sobre a trigliceridemia e reatividade vascular pos-prandial. Arq Bras Cardiol. 2004;83(5):385-90.
6. Alipour A, Elite JW, Van Zaanen HC, Rietveld AP, Cabezas MC. Postprandial inflammation and endothelial dysfuction. Biochem Soc Trans. 2007;35(Pt 3):466-9.
7. Roche HM, Gibney MJ. Effect of long-chain n-3 polyunsaturated fatty acids on fasting and postprandial triacylglycerol metabolism. Am J Clin Nutr. 2000;71(1 Suppl):232S-7S.
8. Issa J, Diament J, Forti N. Lipemia pos-prandial: influencia do envelhecimento. Arq Bras Cardiol. 2007;85(1):15-9.
9. Harrison M, O’Gorman DJ, McCaffrey N, Hamilton MT, Zderic TW, Carson BP, et al. Influence of acut exercise with and whithout carbohydrate replacement on postprandial lipid metabolism. J Appl Phisiol (1985). 2009;106(3):943-9.
10. Axelsen M, Eliasson B, Joheim E, Lenner RA, Taskinen MR, Smith U. Lipid intolerance in smokers. J Intern Med. 1995;237(5):449-55.
11. Couillard C, Bergeron N, Prud’homme D, Bergon J, Tremblay A, Boachard C, et al. Postprandial triglyceride response in visceral obesity in men. Diabetes. 1988;47(6):953-60.
12. Herd SL, Lawrence JE, Malkova D, Murphy MH, Mastana S, Hardman AE. Postprandial lipemia in young men and woman of contrasting training status. J Appl Physiol (1985). 2000;89(5):2049-56.
13. Signori LU, Plentz RD, Irigoyen MC, Schaan BD. O papel da lipemia pos-prandial na genese da aterosclerose: particularidades do diabetes melittus. Arq Bras Endocrinol Metabol. 2007;51(2):222-31.
14. Enkhmaa B, Ozturk Z, Anuurad E, Berglund L. Postprandial lipoproteins and cardiovascular disease risk in diabetes mellitus. Curr Diab Rep. 2010;10(1):61-9.
15. Van Oostrom AJ, Alipour A, Plokker TW, Sniderman AD, Cabezas CM. The metabolic syndrome in relation to complement component 3 and postprandial lipemia in patients from an outpatient lipid clinic and healthy volunteers. Atherosclerosis. 2007;190(1):167-73.
16. Santos MC, Rebelo AC, Zuttin RS, Cesar MC, Catai AM, Silva E. Influencia do uso de contraceptivos orais nos níveis lipídicos e nas respostas cardiorrespiratorias de mulheres saudáveis e sedentárias. Rev Bras Fisioter. 2008;12(3):188-94.
17. Coelho VG, Caetano LF, Liberatore Junior Rdel R, Cordeiro JA, Souza DR. Perfil lipídico e fatores de risco para doenças cardiovasculares em estudantes de medicina. Arq Bras Cardiol. 2005;85(1):57-62.
18. Virdis A, Pinto S, Versari D, Salvetti G, Bernini G, Fruzzetti F, et al. Effect of oral contraceptives on endothelial function in the peripheral microcirculation of healthy women. J Hypertens. 2003;21(12):2275-80.
References
In this context, the meta-analysis conducted by Hokanson and Austin in 1996 showed that the magnitude of PPL in women is associated with an increase of 76% in the risk of developing a coronary disease, while among men this risk was of 32%37. Some studies point out that approximately 40% of individuals with premature coronary artery disease present with normal fasting lipid profile, but with delayed clearance during PPL35,38.
Also based on the results of this study, it is plausible to infer that women in COG are more prone to forming arterial and venous thrombi. OC and the increased PPL, independently, increase the activation of the blood-coagulation factor VII and inhibit the action of plasminogen, and these factors are proven to favor the formation of venous and arterial thrombi28,39.
Facing the exposed, it is recommended to assess the risks and benefits related to the prescription of this contraceptive method, as well as to conduct a strict clinical follow-up, especially concerning cardiovascular risks in this population. In order for the results in this study to be elucidated, some prospective cohort studies that measure the clinical outcomes and other variables of inflammatory response should be conducted.
ConclusionResults indicate that, among young, healthy and physically
inactive women, PPL is more present for those who are on oral contraceptives than for those who are not, which suggests that, in this population, the chronic use of oral contraceptives, even at low dosages, increases the risk of developing cardiovascular diseases.
AcknowledgementsTo the Laboratory of Clinical Pathology of Salvador (BA),
where all blood samples were collected for this study.
Author contributionsConception and design of the research: Petto J, Ladeia
AMT; Acquisition of data, Analysis and interpretation of the data and Writing of the manuscript: Petto J, Vasques LMR, Pinheiro RL, Giesta BA, Santos ACN, Gomes Neto M, Ladeia AMT; Statistical analysis and Critical revision of the manuscript for intellectual content: Petto J, Gomes Neto M, Ladeia AMT.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
This study was funded by FAPESB by awarding a PhD scholarship to Jefferson Petto.
Study Association
This article is part of the thesis of Doctorate submitted by Jefferson Petto from Escola Bahiana de Medicina e Saúde Pública.
249
Original Article
Petto et al.Postprandial lipemia and oral contraceptive
Arq Bras Cardiol. 2014; 103(3):245-250
19. Gaspard U, Endrikat J, Desager JP, Buicu C, Gerlinger C, Heithecker R. A randomized study on the influence of oral contraceptives containing ethinylestradiol combined with drospirenone or desogestrel on lipid and lipoprotein metabolism over a period of 13 cycles. Contraception. 2004;69(4):271-8.
20. Machado RB, Fabrini P, Cruz AM, Maia E, da Cunha Bastos A. Clinical and metabolic aspects of the continuous use of a contraceptive association of ethinyl estradiol (30 microg) and gestodene (75 microg). Contraception. 2004;70(5):365-70.
21. Wiegratz I, Stahlberg S, Manthey T, Sanger N, Mittmann K, Palombo-Kinne E, et al. Effects of an oral contraceptive containing 30 mcg ethinyl estradiol and 2 mg dienogest on lipid metabolism during 1 year of conventional or extended-cycle use. Contraception. 2010;81(1):57-61.
22. Matsudo S, Araújo T, Matsudo V, Andrade D, Andrade E, Oliveira LC, et al. Questionário internacional de atividade física (IPAQ): estudo de validade e reprodutibilidade no Brasil. Atividade Física & Saúde. 2001;6(2):5-18.
23. Sociedade Brasileira de Cardiologia, Sociedade Brasileira de Hipertensão, Sociedade Brasileira de Nefrologia. VI Diretrizes brasileiras de hipertensão. Arq Bras Cardiol. 2010;95(1 supl. 1):1-51. Erratum in: Arq Bras Cardiol. 2010;95(4):553.
24. World Health Organization (WHO). Obesity: preventing and manging the global epidemic – report of a WHO consultation on obesity. Geneva; 2000.
25. Sposito AC, Caramelli B, Fonseca FA, Bertolami MC, Afiune Neto A, Souza AD, et al.; Sociedade Brasileira de Cardiologia. IV Diretriz brasileira sobre dislipidemias e prevenção da aterosclerose. Arq Bras Cardiol. 2007;88(supl 1):1-18.
26. Casazza GA, Suh SH, Miller BF, Navazio FM, Brooks GA. Effects of oral contraceptives on peak exercise capacity. J Appl Physiol (1985). 2002;93(5):1698-702.
27. Burkman RT. Current perspectives on OCs. Dialogues in contraception. 2001. Summer,6(8):15-7.
28. Giribela CR, Rubira MC, Melo NR, Plentz RD, Angelis K, Moreno H, et al. Effect of a low-dose oral contraceptive on venous endothelial function in healthy young women: preliminary results. Clinics (Sao Paulo). 2007;62(2):151-8.
29. Vieira EM, Badiani R, Fabbro AL, Rodrigues Junior AL. Características do uso de metodos anticoncepcionais no estado de São Paulo. Rev Saúde Pública. 2001;36(3):263-70.
30. Foulon T, Payen N, Laporte F, Bijaoui S, Dupont G, Roland F, et al. Effects of two low-dose oral contraceptives containing ethinylestradiol and either desogestrel or levonorgestrel on serium lipds and lipoproteins with particular regard to LDL size. Contraception. 2001;64(1):11-6.
31. O’Meara NM, Lweis GF, Cabana VG, Iverius PH, Getz GS, Polonsky KS. Role of basal triglyceride and high-density lipoprotein in determination of postprandial lipid and lipoprotein responses. J Clin Endocrinol Metab. 1992;75(2):465-71.
32. Oliveira GH, Farmer JA. Novos fatores de risco cardiovasculares. Rev SOCERJ. 2003;16(3):183-93.
33. Lewis GF, O’Meara NM, Soltys PA, Blackman JD, Iverius PH, Druetzler AF, et al. Postprandial lipoprotein metabolism in normal and obese subjects: comparison after the vitamin A fat-loadging test. J Clin Endocrinol Metab. 1990;71(4):1041-50.
34. Mekki N, Christofilis MA, Charbonnier M, Atlan-Gepner C, Defoot C, Juhel C, et al. Influence of obesity and body fat distribution on postprandial lipemia and triglyceride- rich lipoproteins in adult women. J Clin Endocrinol Metab. 1999;84(1):184-91.
35. Patsch JR, Miesenböck G, Hopferwieser T, Mühlberger V, Knapp E, Dunn JK, et al. Relation of triglyceride metabolism and coronary artery disease: studies in the postprandial state. Arterioscler Thromb. 1992;12(11):1336-45.
36. Bansal S, Buring JE, Rifai N, Mora S, Sacks FM, Ridker PM. Fasting compared with nonfasting triglycerides and risk of cardiovascular events in women. JAMA. 2007;298(3):309-16.
37. Hokason JE, Austin MA. Plasma triglyceride level is a risk factor for cardiovascular disease independent of high-density lipoprotein cholesterol level: a meta-analysis of population-based prospective studies. J Cardiovasc Risk. 1996;3(2):213-9.
38. Genest JJ, McNamara JR, Salem DN, Schafer EJ. Prevalence of risk factors in men with premature coronary artery disease. Am J Cardiol. 1991;67(15):1185-9.
39. Roche HM, Gibney MJ. The impact of postprandial lipemia in accelerating atherothombosis. J Cardiovasc Risk. 2000;7(5):317-24.
250

Review Article
Multimodality Imaging of Heart Valve DiseaseRonak Rajani1, Rajdeep Khattar2, Amedeo Chiribiri3, Kelly Victor1, John Chambers1
Department of Cardiology, St. Thomas’ Hospital1, London; Department of Cardiology, Royal Brompton Hospital2, London; Divisions of Imaging Sciences, The Rayne Institute, St. Thomas’ Hospital3, London – United Kingdom
GlossaryVENC – Velocity Encoding – a specialized technique for
encoding flow-velocities on cardiac magnetic resonance imaging.
SSFP – Steady-State Free Precession – a gradient echo magnetic resonance imaging pulse sequence in which a steady, residual transverse magnetization is maintained between successive cycles.
AbstractUnidentified heart valve disease is associated with a
significant morbidity and mortality. It has therefore become important to accurately identify, assess and monitor patients with this condition in order that appropriate and timely intervention can occur. Although echocardiography has emerged as the predominant imaging modality for this purpose, recent advances in cardiac magnetic resonance and cardiac computed tomography indicate that they may have an important contribution to make. The current review describes the assessment of regurgitant and stenotic heart valves by multimodality imaging (echocardiography, cardiac computed tomography and cardiac magnetic resonance) and discusses their relative strengths and weaknesses.
Introduction Heart valve disease causes significant morbidity and
premature death but also carries a sizeable health economic burden. The population prevalence of moderate or severe valve disease is 2.5% in industrially developed countries1, but this rises to 13% at age ≥ 75 years. Therefore, as our population ages, clinicians will increasingly need to identify and monitor valve disease. Judging the appropriateness and timing of interventions will become progressively harder in the face of cardiac and extracardiac comorbidities.
Echocardiography is the cornerstone of assessing heart valve disease. It is affordable, accessible and backed by a strong evidence base (Table 1)2. However, cardiac magnetic resonance imaging and cardiac computed tomography (CT) are increasingly useful. This review addresses the roles and limitations of each of these modalities for the assessment of patients with heart valve disease.
The aortic valve
Echocardiography
Aortic stenosisAortic stenosis (AS) is differentiated from ‘sclerosis’ by a
reduction in valve opening (Figure 1) with a peak transaortic velocity > 2.5 m/s. It is graded using a minimum dataset of the peak velocity, mean pressure gradient and effective orifice area (EOA)a 3,4. (Table 1).
Echocardiography provides information on left ventricular (LV) systolic and diastolic anatomy and function. It also assesses the rest of the heart especially the aorta, the mitral valve and the right heart. Exercise echocardiography may reveal indications for surgery in patients with asymptomatic severe AS: symptoms (Class I), a fall in blood pressure below baseline (Class IIa) or an increase in mean gradient of > 20 mmHg (Class IIb)5.
Discrepant measures of Aortic Stenosis severityIt is relatively common to find that the velocity and gradient
are discrepant with the EOA. The first step should be to review the measurements (Table 2) looking for errors. Transvalvular gradients in the severe range and the EOA in the moderate range may be caused by erroneously low placement of the pulsed sample volume and the diameter of the LV outflow tract (LVOT) may be difficult to measure correctly. This situation can also be a genuine effect of increased flow for example as a result of sepsis, anaemia, or coexistent significant aortic regurgitation (AR).
If the velocity and gradient are moderate but the EOA is severe, the situation has a number of possible explanations. There is evidence that the cut-points for orifice area may not be valid and effective areas between 0.8 and 1.0 cm2 may sometimes be moderate rather than severe. The shape of the waveform and appearance and mobility of the valve may help to differentiate moderate from severe and it may also help to index EOA to body surface area (BSA).
KeywordsDiagnostic Imaging; Heart Valve Diseases; Cardiac Imaging;
Techniques / trends; Magnetic Resonance Imaging; Tomography.Mailing address: Ronak Rajani •Department of Cardiology, Westminster Bridge Road, St Thomas’ Hospital, London, SE1 7EH. United Kingdom.E-mail: [email protected] received October 28, 2013; revised January 7, 2014; accepted January 7, 2014.
DOI: 10.5935/abc.20140057
a
Where: AV: aortic valve; CSA: cross sectional area; EOA: effective orifice area; LVOT: left ventricular outflow tract; VTI: velocity-time integral.
251
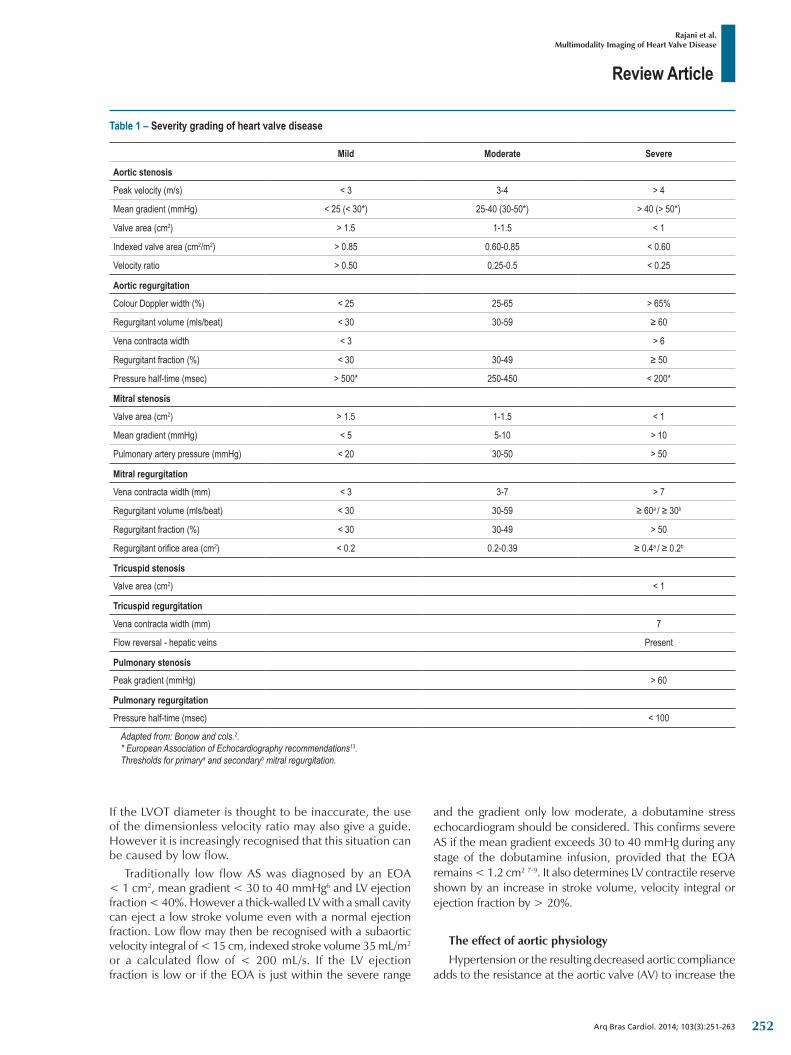
Review Article
Rajani et al.Multimodality Imaging of Heart Valve Disease
Arq Bras Cardiol. 2014; 103(3):251-263
Table 1 – Severity grading of heart valve disease
Mild Moderate Severe
Aortic stenosis
Peak velocity (m/s) < 3 3-4 > 4
Mean gradient (mmHg) < 25 (< 30*) 25-40 (30-50*) > 40 (> 50*)
Valve area (cm2) > 1.5 1-1.5 < 1
Indexedvalvearea(cm2/m2) > 0.85 0.60-0.85 < 0.60
Velocity ratio > 0.50 0.25-0.5 < 0.25
Aortic regurgitation
ColourDopplerwidth(%) < 25 25-65 > 65%
Regurgitant volume (mls/beat) < 30 30-59 ≥60
Venacontractawidth < 3 > 6
Regurgitant fraction (%) < 30 30-49 ≥50
Pressure half-time (msec) > 500* 250-450 < 200*
Mitral stenosis
Valve area (cm2) > 1.5 1-1.5 < 1
Mean gradient (mmHg) < 5 5-10 > 10
Pulmonary artery pressure (mmHg) < 20 30-50 > 50
Mitral regurgitation
Venacontractawidth(mm) < 3 3-7 > 7
Regurgitant volume (mls/beat) < 30 30-59 ≥60a /≥30b
Regurgitant fraction (%) < 30 30-49 > 50
Regurgitantorificearea(cm2) < 0.2 0.2-0.39 ≥0.4a /≥0.2b
Tricuspid stenosis
Valve area (cm2) < 1
Tricuspid regurgitation
Venacontractawidth(mm) 7
Flowreversal-hepaticveins Present
Pulmonary stenosis
Peak gradient (mmHg) > 60
Pulmonary regurgitation
Pressure half-time (msec) < 100
Adapted from: Bonow and cols.2.* European Association of Echocardiography recommendations13.Thresholds for primarya and secondaryb mitral regurgitation.
If the LVOT diameter is thought to be inaccurate, the use of the dimensionless velocity ratio may also give a guide. However it is increasingly recognised that this situation can be caused by low flow.
Traditionally low flow AS was diagnosed by an EOA < 1 cm2, mean gradient < 30 to 40 mmHg6 and LV ejection fraction < 40%. However a thick-walled LV with a small cavity can eject a low stroke volume even with a normal ejection fraction. Low flow may then be recognised with a subaortic velocity integral of < 15 cm, indexed stroke volume 35 mL/m2 or a calculated flow of < 200 mL/s. If the LV ejection fraction is low or if the EOA is just within the severe range
and the gradient only low moderate, a dobutamine stress echocardiogram should be considered. This confirms severe AS if the mean gradient exceeds 30 to 40 mmHg during any stage of the dobutamine infusion, provided that the EOA remains < 1.2 cm2 7-9. It also determines LV contractile reserve shown by an increase in stroke volume, velocity integral or ejection fraction by > 20%.
The effect of aortic physiology
Hypertension or the resulting decreased aortic compliance adds to the resistance at the aortic valve (AV) to increase the
252
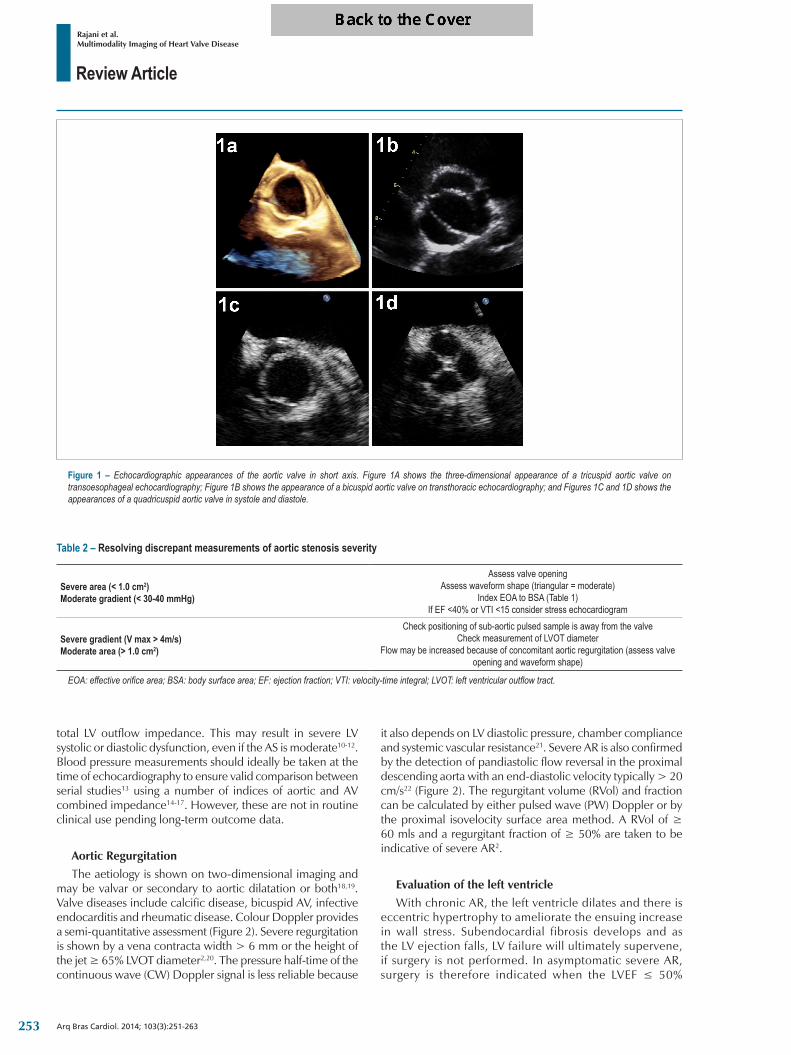
Review Article
Rajani et al.Multimodality Imaging of Heart Valve Disease
Arq Bras Cardiol. 2014; 103(3):251-263
Figure 1 – Echocardiographic appearances of the aortic valve in short axis. Figure 1A shows the three-dimensional appearance of a tricuspid aortic valve on transoesophageal echocardiography; Figure 1B shows the appearance of a bicuspid aortic valve on transthoracic echocardiography; and Figures 1C and 1D shows the appearances of a quadricuspid aortic valve in systole and diastole.
Table 2 – Resolving discrepant measurements of aortic stenosis severity
Severe area (< 1.0 cm2) Moderate gradient (< 30-40 mmHg)
Assess valve openingAssesswaveformshape(triangular=moderate)
IndexEOAtoBSA(Table1)If EF <40% or VTI <15 consider stress echocardiogram
Severe gradient (V max > 4m/s) Moderate area (> 1.0 cm2)
Checkpositioningofsub-aorticpulsedsampleisawayfromthevalveCheck measurement of LVOT diameter
Flowmaybeincreasedbecauseofconcomitantaorticregurgitation(assessvalveopeningandwaveformshape)
EOA: effective orifice area; BSA: body surface area; EF: ejection fraction; VTI: velocity-time integral; LVOT: left ventricular outflow tract.
total LV outflow impedance. This may result in severe LV systolic or diastolic dysfunction, even if the AS is moderate10-12. Blood pressure measurements should ideally be taken at the time of echocardiography to ensure valid comparison between serial studies13 using a number of indices of aortic and AV combined impedance14-17. However, these are not in routine clinical use pending long-term outcome data.
Aortic RegurgitationThe aetiology is shown on two-dimensional imaging and
may be valvar or secondary to aortic dilatation or both18,19. Valve diseases include calcific disease, bicuspid AV, infective endocarditis and rheumatic disease. Colour Doppler provides a semi-quantitative assessment (Figure 2). Severe regurgitation is shown by a vena contracta width > 6 mm or the height of the jet ≥ 65% LVOT diameter2,20. The pressure half-time of the continuous wave (CW) Doppler signal is less reliable because
it also depends on LV diastolic pressure, chamber compliance and systemic vascular resistance21. Severe AR is also confirmed by the detection of pandiastolic flow reversal in the proximal descending aorta with an end-diastolic velocity typically > 20 cm/s22 (Figure 2). The regurgitant volume (RVol) and fraction can be calculated by either pulsed wave (PW) Doppler or by the proximal isovelocity surface area method. A RVol of ≥ 60 mls and a regurgitant fraction of ≥ 50% are taken to be indicative of severe AR2.
Evaluation of the left ventricle With chronic AR, the left ventricle dilates and there is
eccentric hypertrophy to ameliorate the ensuing increase in wall stress. Subendocardial fibrosis develops and as the LV ejection falls, LV failure will ultimately supervene, if surgery is not performed. In asymptomatic severe AR, surgery is therefore indicated when the LVEF ≤ 50%
253
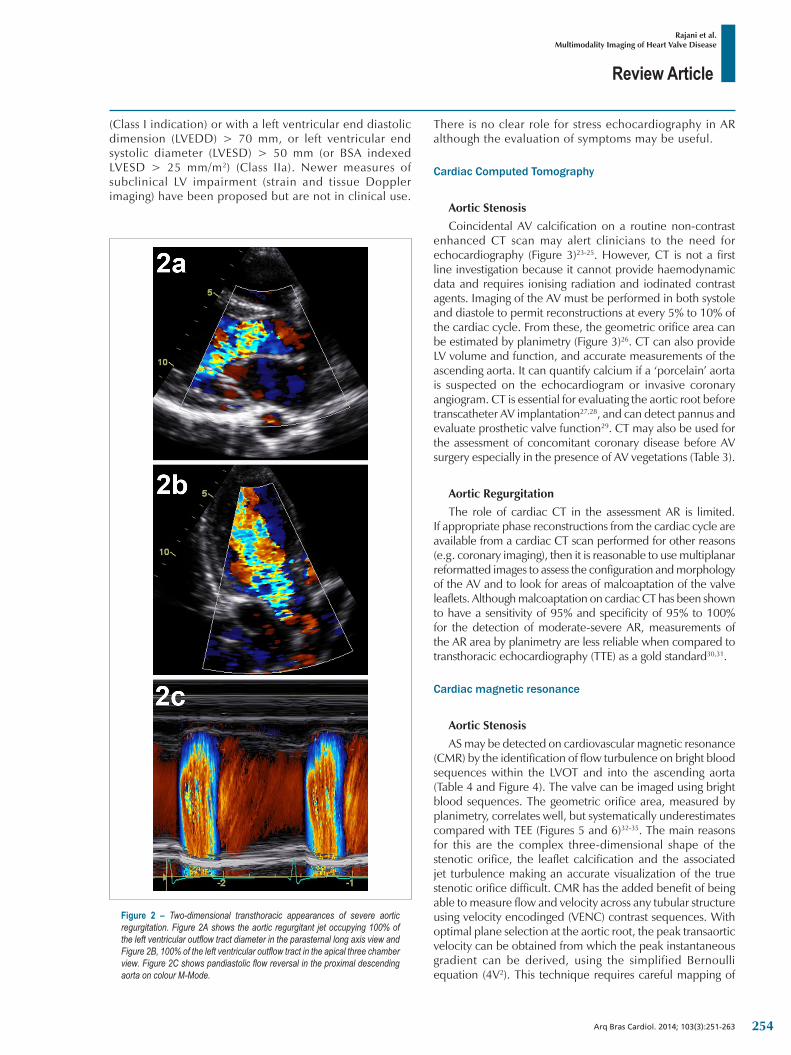
Review Article
Rajani et al.Multimodality Imaging of Heart Valve Disease
Arq Bras Cardiol. 2014; 103(3):251-263
Figure 2 – Two-dimensional transthoracic appearances of severe aortic regurgitation. Figure 2A shows the aortic regurgitant jet occupying 100% of the left ventricular outflow tract diameter in the parasternal long axis view and Figure 2B, 100% of the left ventricular outflow tract in the apical three chamber view. Figure 2C shows pandiastolic flow reversal in the proximal descending aorta on colour M-Mode.
(Class I indication) or with a left ventricular end diastolic dimension (LVEDD) > 70 mm, or left ventricular end systolic diameter (LVESD) > 50 mm (or BSA indexed LVESD > 25 mm/m2) (Class IIa). Newer measures of subclinical LV impairment (strain and tissue Doppler imaging) have been proposed but are not in clinical use.
There is no clear role for stress echocardiography in AR although the evaluation of symptoms may be useful.
Cardiac Computed Tomography
Aortic StenosisCoincidental AV calcification on a routine non-contrast
enhanced CT scan may alert clinicians to the need for echocardiography (Figure 3)23-25. However, CT is not a first line investigation because it cannot provide haemodynamic data and requires ionising radiation and iodinated contrast agents. Imaging of the AV must be performed in both systole and diastole to permit reconstructions at every 5% to 10% of the cardiac cycle. From these, the geometric orifice area can be estimated by planimetry (Figure 3)26. CT can also provide LV volume and function, and accurate measurements of the ascending aorta. It can quantify calcium if a ‘porcelain’ aorta is suspected on the echocardiogram or invasive coronary angiogram. CT is essential for evaluating the aortic root before transcatheter AV implantation27,28, and can detect pannus and evaluate prosthetic valve function29. CT may also be used for the assessment of concomitant coronary disease before AV surgery especially in the presence of AV vegetations (Table 3).
Aortic RegurgitationThe role of cardiac CT in the assessment AR is limited.
If appropriate phase reconstructions from the cardiac cycle are available from a cardiac CT scan performed for other reasons (e.g. coronary imaging), then it is reasonable to use multiplanar reformatted images to assess the configuration and morphology of the AV and to look for areas of malcoaptation of the valve leaflets. Although malcoaptation on cardiac CT has been shown to have a sensitivity of 95% and specificity of 95% to 100% for the detection of moderate-severe AR, measurements of the AR area by planimetry are less reliable when compared to transthoracic echocardiography (TTE) as a gold standard30,31.
Cardiac magnetic resonance
Aortic StenosisAS may be detected on cardiovascular magnetic resonance
(CMR) by the identification of flow turbulence on bright blood sequences within the LVOT and into the ascending aorta (Table 4 and Figure 4). The valve can be imaged using bright blood sequences. The geometric orifice area, measured by planimetry, correlates well, but systematically underestimates compared with TEE (Figures 5 and 6)32-35. The main reasons for this are the complex three-dimensional shape of the stenotic orifice, the leaflet calcification and the associated jet turbulence making an accurate visualization of the true stenotic orifice difficult. CMR has the added benefit of being able to measure flow and velocity across any tubular structure using velocity encodinged (VENC) contrast sequences. With optimal plane selection at the aortic root, the peak transaortic velocity can be obtained from which the peak instantaneous gradient can be derived, using the simplified Bernoulli equation (4V2). This technique requires careful mapping of
254
Review Article
Rajani et al.Multimodality Imaging of Heart Valve Disease
Arq Bras Cardiol. 2014; 103(3):251-263
Figure 3 – Cardiac computed tomography of a bicuspid aortic valve. Figure 3A shows the morphology and distribution of aortic valve calcium in a patient with a bicuspid aortic valve on a multiplanar reformatted image. Figure 3B shows planimetry of the bicuspid aortic valve and Figure 3C the ascending aorta anatomy.
Table 3 – Cardiac computerized tomography and the assessment of the aortic valve
Cardiac computerized tomography
Aortic stenosis
Valve morphology
Aorticvalvecalcification
Accurate aortic annulus size
Aortic dimensions
Aortic valve planimetry
TAVI assessment
Coronary assessment
Aortic regurgitation
Valve morphology
Leafletmal-coaptation
Aortic dimensions
Coronary assessment
Suspected endocarditisAortic root abscesses
Localised aneurysm formation
TAVI: transcatheter aortic heart valve.
the area of interest for each frame of the cardiac cycle and an appropriate selection of maximum velocity to be programmed into the pulse sequence to avoid aliasing. Peak gradients across the AV by VENC correlate well, but slightly underestimate, the peak gradient obtained CW Doppler on TTE36-38.
Cardiac magnetic resonance is the gold standard method of measuring LV mass and volume and can also assess systolic and diastolic LV function. It can differentiate sub-valvular and supravalvular stenosis by inplane velocity mapping. It can assess the whole aorta, which may be important in patients with a bicuspid AV, in whom the echocardiographic window does not permit adequate imaging above the root. New studies suggest that CMR detects myocardial fibrosis using late Gadolinium enhancement, which may portend a worse clinical outcome39.
Aortic RegurgitationThis can be identified by the detection of diastolic backwards
flow into the LVOT upon steady-state free precession (SSFP) cine imaging in the three-chamber/LVOT view (Figure 5). An accurate quantification of RVol and fraction can then be obtained using inplane flow imaging which is able to measure both the forward flow and the regurgitant flow across the AV. From this, the regurgitant fraction can be derived [(RVol/forward flow) x 100]. This technique is dependent upon careful tracing around the area of interest of each frame of the cardiac cycle and the selection of the correct plane at which to measure the forward and regurgitant flows (Figure 5)40. CMR’s excellent reproducibility for AR flow and LV volumes is useful for serial examinations when determining the timing of surgery41,42.
The mitral valve
Echocardiography
Mitral RegurgitationMitral Regurgitation (MR) may be primary (organic)
or secondary (functional). Primary causes include mitral
255
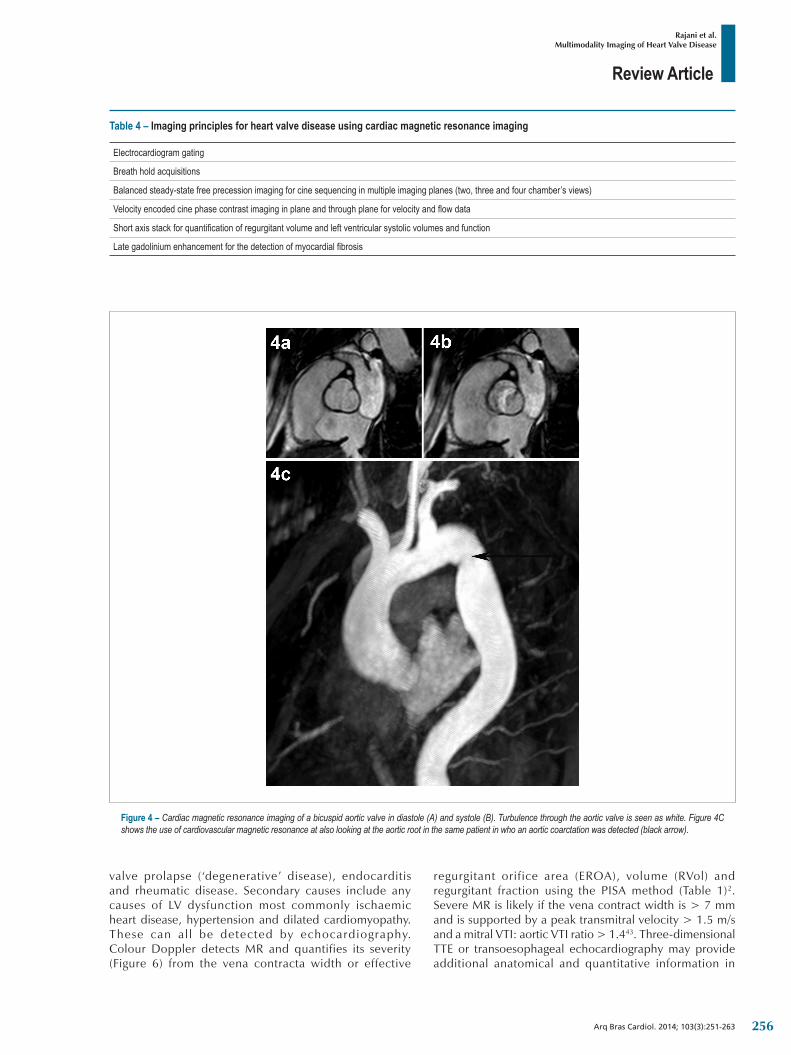
Review Article
Rajani et al.Multimodality Imaging of Heart Valve Disease
Arq Bras Cardiol. 2014; 103(3):251-263
Figure 4 – Cardiac magnetic resonance imaging of a bicuspid aortic valve in diastole (A) and systole (B). Turbulence through the aortic valve is seen as white. Figure 4C shows the use of cardiovascular magnetic resonance at also looking at the aortic root in the same patient in who an aortic coarctation was detected (black arrow).
Table 4 – Imaging principles for heart valve disease using cardiac magnetic resonance imaging
Electrocardiogram gating
Breath hold acquisitions
Balancedsteady-statefreeprecessionimagingforcinesequencinginmultipleimagingplanes(two,threeandfourchamber’sviews)
Velocityencodedcinephasecontrastimaginginplaneandthroughplaneforvelocityandflowdata
Shortaxisstackforquantificationofregurgitantvolumeandleftventricularsystolicvolumesandfunction
Lategadoliniumenhancementforthedetectionofmyocardialfibrosis
valve prolapse (‘degenerative’ disease), endocarditis and rheumatic disease. Secondary causes include any causes of LV dysfunction most commonly ischaemic heart disease, hypertension and dilated cardiomyopathy. These can al l be detected by echocardiography. Colour Doppler detects MR and quantifies its severity (Figure 6) from the vena contracta width or effective
regurgitant orifice area (EROA), volume (RVol) and regurgitant fraction using the PISA method (Table 1)2. Severe MR is likely if the vena contract width is > 7 mm and is supported by a peak transmitral velocity > 1.5 m/s and a mitral VTI: aortic VTI ratio > 1.443. Three-dimensional TTE or transoesophageal echocardiography may provide additional anatomical and quantitative information in
256
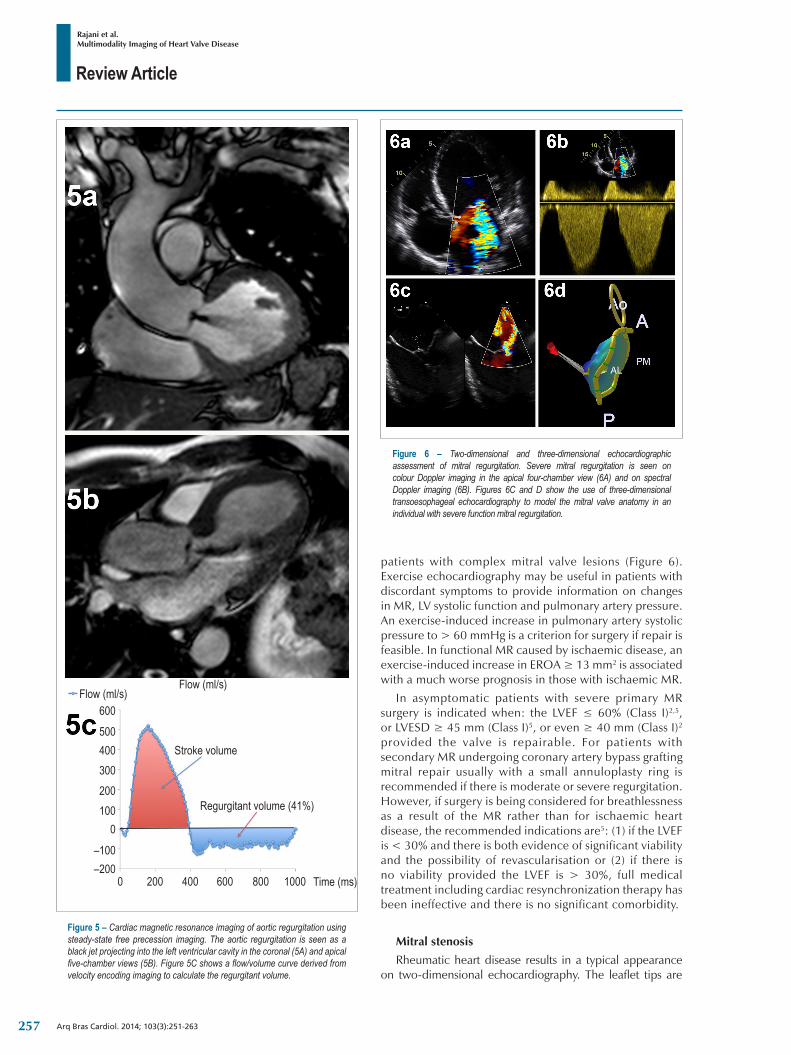
Review Article
Rajani et al.Multimodality Imaging of Heart Valve Disease
Arq Bras Cardiol. 2014; 103(3):251-263
Figure 6 – Two-dimensional and three-dimensional echocardiographic assessment of mitral regurgitation. Severe mitral regurgitation is seen on colour Doppler imaging in the apical four-chamber view (6A) and on spectral Doppler imaging (6B). Figures 6C and D show the use of three-dimensional transoesophageal echocardiography to model the mitral valve anatomy in an individual with severe function mitral regurgitation.
patients with complex mitral valve lesions (Figure 6). Exercise echocardiography may be useful in patients with discordant symptoms to provide information on changes in MR, LV systolic function and pulmonary artery pressure. An exercise-induced increase in pulmonary artery systolic pressure to > 60 mmHg is a criterion for surgery if repair is feasible. In functional MR caused by ischaemic disease, an exercise-induced increase in EROA ≥ 13 mm2 is associated with a much worse prognosis in those with ischaemic MR.
In asymptomatic patients with severe primary MR surgery is indicated when: the LVEF ≤ 60% (Class I)2,5, or LVESD ≥ 45 mm (Class I)5, or even ≥ 40 mm (Class I)2 provided the valve is repairable. For patients with secondary MR undergoing coronary artery bypass grafting mitral repair usually with a small annuloplasty ring is recommended if there is moderate or severe regurgitation. However, if surgery is being considered for breathlessness as a result of the MR rather than for ischaemic heart disease, the recommended indications are5: (1) if the LVEF is < 30% and there is both evidence of significant viability and the possibility of revascularisation or (2) if there is no viability provided the LVEF is > 30%, full medical treatment including cardiac resynchronization therapy has been ineffective and there is no significant comorbidity.
Mitral stenosis
Rheumatic heart disease results in a typical appearance on two-dimensional echocardiography. The leaflet tips are
Figure 5 – Cardiac magnetic resonance imaging of aortic regurgitation using steady-state free precession imaging. The aortic regurgitation is seen as a black jet projecting into the left ventricular cavity in the coronal (5A) and apical five-chamber views (5B). Figure 5C shows a flow/volume curve derived from velocity encoding imaging to calculate the regurgitant volume.
Flow(ml/s)Flow(ml/s)
600500400300200100
0
–100
0 200 400 600 800 1000–200
Stroke volume
Regurgitant volume (41%)
Time (ms)
257

Review Article
Rajani et al.Multimodality Imaging of Heart Valve Disease
Arq Bras Cardiol. 2014; 103(3):251-263
b MVA = 220 PHalf-timeWhere: MVA: mitral valve area; PHalf-time: pressure half-time.
thickened and commissural fusion results in diastolic bowing of the leaflets in a hockey-stick shaped deformity. The chordae tendinae are also thickened and become matted together. Planimetry of the mitral valve orifice area should be performed using the parasternal short axis on a zoomed mid-diastolic frame13. Three-dimensional transthoracic or transoesophageal echocardiography may be useful to select the correct plane for planimetry. A CW Doppler recording across the mitral valve enables the measurement of the mean transmitral gradient and the pressure half-time. The pulmonary artery systolic pressure is estimated using the tricuspid regurgitation (TR) peak velocity (4 x TR V max) added to an estimated of right atrial mean pressure provided by the size and response of the IVC to a sniff. From the pressure half-time, an estimation of valve area can be madeb 44.
The grade of mitral stenosis (MS) can then be estimated (Table 1).
Valve EOA can be estimated using the continuity equation or proximal isovelocity surface area method. Exercise echocardiography is indicated in patients with severe symptoms despite apparently only moderate MS. Exercise-induced increases in mean gradient to ≥ 15 mmHg or pulmonary artery systolic pressures to ≥ 60 mmHg are indications for intervention provided that balloon mitral valvuloplasty is feasible2. This is possible in the absence of bicommissural or severe single commissural calcification, severe chordal involvement, calcification and immobility of the valve, more than mild MR, left atrial thrombus and the requirement for intervention for severe involvement of other valves or the coronary arteries45.
Cardiac Computed Tomography
Mitral RegurgitationThe EROA can be measured by planimetry and this has
been shown to correlate well with TEE46. Additional information available from cardiac CT includes mitral annulus size, mitral valve leaflet length and calcification, chordae tendinae thickening, left atrial size and the detection of pulmonary oedema. Although cardiac CT with cine imaging can reliably detect and localise segmental leaflet prolapse, this is not routinely performed.
Mitral stenosisCardiac CT is particularly suited to the detection of mitral
valve leaflet, commissural and annulus calcification. For an evaluation of the valve components, a reconstruction at 65% of the R-R interval for the open mitral valve and a reconstruction at 5% of the R-R interval are recommended for the closed mitral valve. The geometric orifice area is measured by direct planimetry and has been shown to correlate well with TEE (R = 0.88; p < 0.001)47. Additional information obtainable is left atrial size, left atrial appendage thrombus, right ventricular (RV) hypertrophy and radiographic evidence of pulmonary oedema and pulmonary hypertension.
Cardiac magnetic resonance imaging
Mitral RegurgitationMR is initially seen as a net loss of signal across the mitral
valve representing flow turbulence on SSFP and gradient echo sequences. For a complete anatomical assessment of the mitral valve bright blood cine sequences should be acquired in the two, three and four chamber planes, along with a full LV short-axis stack. Following this, a basal slice from the short axis stack should be selected where the mitral valve is seen. Oblique slices may then be taken perpendicular to the line of coaptation working down from the A1-P1 juncture inferiorly down to the A3-P3 juncture every 5 mm with no inter-slice gap48. This system permits the accurate localisation of regurgitant jets and helps to localise dysfunctional mitral valve leaflet scallops. The RVol can be estimated using the LV stroke volume and forward flow within the aorta at the level of the sinus of valsalva using VENC contrast mapping. The regurgitant fraction is then calculated as the [(RVol/LV stoke volume) x 100]49,50.
Mitral stenosisCardiac magnetic resonance imaging is not used routinely
for the assessment of mitral stenosis. Mitral inflow turbulence may be seen on SSFP in-plane imaging and the mitral valve area may be measured using carefully placed through-plane SSFP imaging. Although this technique has been shown to correlate well with echo derived areas51,52 it is often limited by the presence of atrial fibrillation and problems with electrocardiogram gating.
The tricuspid valve
EchocardiographyCauses of primary (organic) tricuspid valve disease include
rheumatic disease, endocarditis, prolapse and carcinoid. Secondary (functional) TR is caused by abnormalities of the RV either as a result of infarction, volume or pressure overload. Colour Doppler imaging is the mainstay for quantification with severe TR shown by a vena contracta width ≥ 7 mm. Although a vena contracta width < 6 mm is suggestive of less than moderate regurgitation, there are no well validated cut-offs for differentiating mild from moderate TR53. Additional markers of severe TR are a pulsed Doppler peak E velocity ≥ 1 m/s, a dense CW signal with a fast upstroke (Figure 7) and prominent flow reversal in the hepatic veins54. In severe compensated TR, the RV may be normal in size but hyperdynamic. With time, the RV dilates progressively and may become hypodynamic as shown by a tricuspid annulus excursion < 15 mm or a systolic maximum tissue Doppler velocity at the base of the RV free wall of < 11 cm/s55.
In severe tricuspid stenosis (TS), the leaflets will be restricted although there may be relatively little thickening compared with left-sided rheumatic disease. Severe stenosis
258
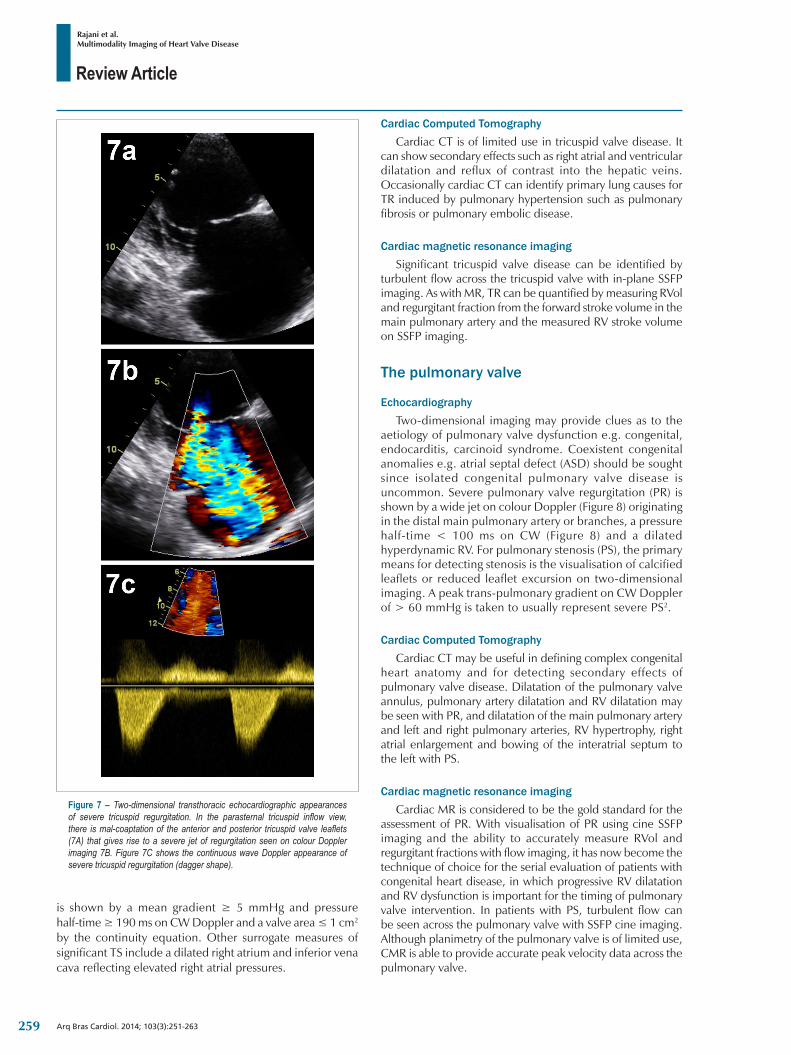
Review Article
Rajani et al.Multimodality Imaging of Heart Valve Disease
Arq Bras Cardiol. 2014; 103(3):251-263
Figure 7 – Two-dimensional transthoracic echocardiographic appearances of severe tricuspid regurgitation. In the parasternal tricuspid inflow view, there is mal-coaptation of the anterior and posterior tricuspid valve leaflets (7A) that gives rise to a severe jet of regurgitation seen on colour Doppler imaging 7B. Figure 7C shows the continuous wave Doppler appearance of severe tricuspid regurgitation (dagger shape).
is shown by a mean gradient ≥ 5 mmHg and pressure half-time ≥ 190 ms on CW Doppler and a valve area ≤ 1 cm2 by the continuity equation. Other surrogate measures of significant TS include a dilated right atrium and inferior vena cava reflecting elevated right atrial pressures.
Cardiac Computed TomographyCardiac CT is of limited use in tricuspid valve disease. It
can show secondary effects such as right atrial and ventricular dilatation and reflux of contrast into the hepatic veins. Occasionally cardiac CT can identify primary lung causes for TR induced by pulmonary hypertension such as pulmonary fibrosis or pulmonary embolic disease.
Cardiac magnetic resonance imagingSignificant tricuspid valve disease can be identified by
turbulent flow across the tricuspid valve with in-plane SSFP imaging. As with MR, TR can be quantified by measuring RVol and regurgitant fraction from the forward stroke volume in the main pulmonary artery and the measured RV stroke volume on SSFP imaging.
The pulmonary valve
EchocardiographyTwo-dimensional imaging may provide clues as to the
aetiology of pulmonary valve dysfunction e.g. congenital, endocarditis, carcinoid syndrome. Coexistent congenital anomalies e.g. atrial septal defect (ASD) should be sought since isolated congenital pulmonary valve disease is uncommon. Severe pulmonary valve regurgitation (PR) is shown by a wide jet on colour Doppler (Figure 8) originating in the distal main pulmonary artery or branches, a pressure half-time < 100 ms on CW (Figure 8) and a dilated hyperdynamic RV. For pulmonary stenosis (PS), the primary means for detecting stenosis is the visualisation of calcified leaflets or reduced leaflet excursion on two-dimensional imaging. A peak trans-pulmonary gradient on CW Doppler of > 60 mmHg is taken to usually represent severe PS2.
Cardiac Computed TomographyCardiac CT may be useful in defining complex congenital
heart anatomy and for detecting secondary effects of pulmonary valve disease. Dilatation of the pulmonary valve annulus, pulmonary artery dilatation and RV dilatation may be seen with PR, and dilatation of the main pulmonary artery and left and right pulmonary arteries, RV hypertrophy, right atrial enlargement and bowing of the interatrial septum to the left with PS.
Cardiac magnetic resonance imagingCardiac MR is considered to be the gold standard for the
assessment of PR. With visualisation of PR using cine SSFP imaging and the ability to accurately measure RVol and regurgitant fractions with flow imaging, it has now become the technique of choice for the serial evaluation of patients with congenital heart disease, in which progressive RV dilatation and RV dysfunction is important for the timing of pulmonary valve intervention. In patients with PS, turbulent flow can be seen across the pulmonary valve with SSFP cine imaging. Although planimetry of the pulmonary valve is of limited use, CMR is able to provide accurate peak velocity data across the pulmonary valve.
259
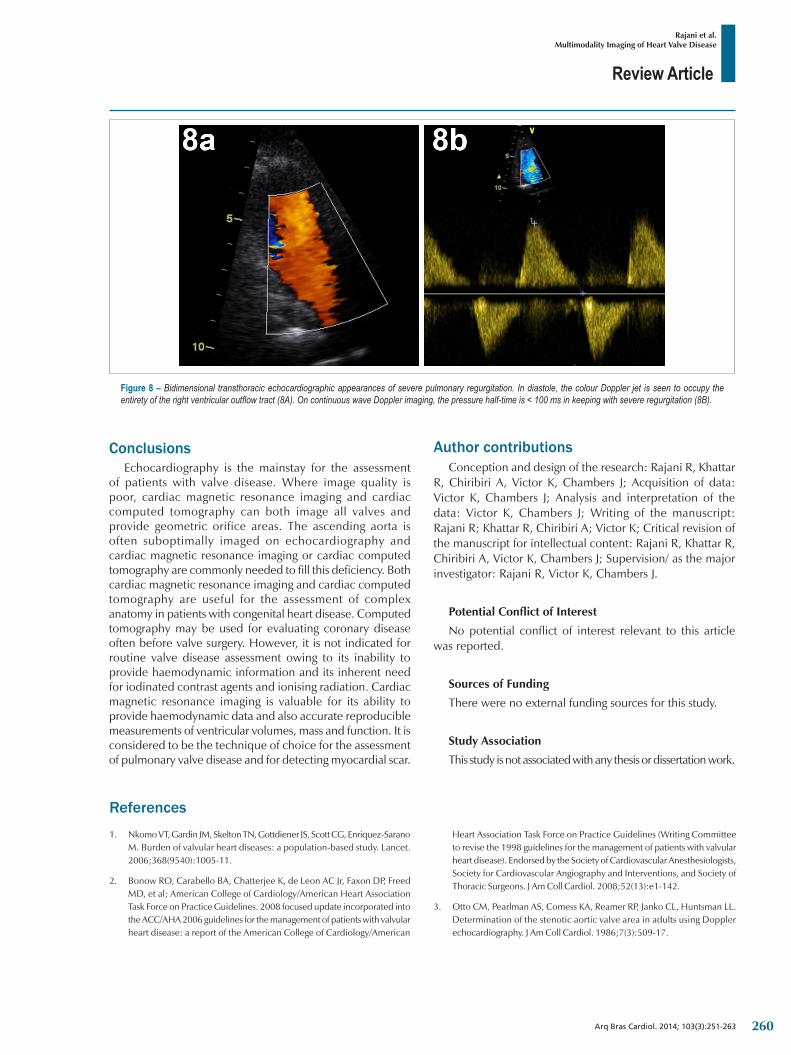
Review Article
Arq Bras Cardiol. 2014; 103(3):251-263
Figure 8 – Bidimensional transthoracic echocardiographic appearances of severe pulmonary regurgitation. In diastole, the colour Doppler jet is seen to occupy the entirety of the right ventricular outflow tract (8A). On continuous wave Doppler imaging, the pressure half-time is < 100 ms in keeping with severe regurgitation (8B).
Rajani et al.Multimodality Imaging of Heart Valve Disease
ConclusionsEchocardiography is the mainstay for the assessment
of patients with valve disease. Where image quality is poor, cardiac magnetic resonance imaging and cardiac computed tomography can both image all valves and provide geometric orifice areas. The ascending aorta is often suboptimally imaged on echocardiography and cardiac magnetic resonance imaging or cardiac computed tomography are commonly needed to fill this deficiency. Both cardiac magnetic resonance imaging and cardiac computed tomography are useful for the assessment of complex anatomy in patients with congenital heart disease. Computed tomography may be used for evaluating coronary disease often before valve surgery. However, it is not indicated for routine valve disease assessment owing to its inability to provide haemodynamic information and its inherent need for iodinated contrast agents and ionising radiation. Cardiac magnetic resonance imaging is valuable for its ability to provide haemodynamic data and also accurate reproducible measurements of ventricular volumes, mass and function. It is considered to be the technique of choice for the assessment of pulmonary valve disease and for detecting myocardial scar.
Author contributionsConception and design of the research: Rajani R, Khattar
R, Chiribiri A, Victor K, Chambers J; Acquisition of data: Victor K, Chambers J; Analysis and interpretation of the data: Victor K, Chambers J; Writing of the manuscript: Rajani R; Khattar R, Chiribiri A; Victor K; Critical revision of the manuscript for intellectual content: Rajani R, Khattar R, Chiribiri A, Victor K, Chambers J; Supervision/ as the major investigator: Rajani R, Victor K, Chambers J.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any thesis or dissertation work.
1. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368(9540):1005-11.
2. Bonow RO, Carabello BA, Chatterjee K, de Leon AC Jr, Faxon DP, Freed MD, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American
ReferencesHeart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52(13):e1-142.
3. Otto CM, Pearlman AS, Comess KA, Reamer RP, Janko CL, Huntsman LL. Determination of the stenotic aortic valve area in adults using Doppler echocardiography. J Am Coll Cardiol. 1986;7(3):509-17.
260
Review Article
Rajani et al.Multimodality Imaging of Heart Valve Disease
Arq Bras Cardiol. 2014; 103(3):251-263
4. Zoghbi WA, Farmer KL, Soto JG, Nelson JG, Quinones MA. Accurate noninvasive quantification of stenotic aortic valve area by Doppler echocardiography. Circulation. 1986;73(3):452-9.
5. Vahanian A, Alfieri O, Andreotti F, Antunes MJ, Baron-Esquivias G, Baumgartner H, et al; Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC); European Association for Cardio-Thoracic Surgery (EACTS). Guidelines on the management of valvular heart disease (version 2012): The Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2012;33(19):2451-96.
6. Chambers J. Low “gradient”, low f low aort ic s tenosis . Heart . 2006;92(4):554-8.
7. Monin JL, Quere JP, Monchi M, Petit H, Baleynaud S, Chauvel C, et al. Low-gradient aortic stenosis: operative risk stratification and predictors for long-term outcome: a multicenter study using dobutamine stress hemodynamics. Circulation. 2003;108(3):319-24.
8. Nishimura RA, Grantham JA, Connolly HM, Schaff HV, Higano ST, Holmes DR Jr. Low-output, low-gradient aortic stenosis in patients with depressed left ventricular systolic function: the clinical utility of the dobutamine challenge in the catheterization laboratory. Circulation. 2002;106(7):809-13.
9. Takeda S, Rimington H, Chambers J. The relation between transaortic pressure difference and flow during dobutamine stress echocardiography in patients with aortic stenosis. Heart. 1999;82(1):11-4.
10. Aronow WS, Schwartz KS, Koenigsberg M. Correlation of serum lipids, calcium and phosphorus, diabetes mellitus, aortic valve stenosis and history of systemic hypertension with presence or absence of mitral anular calcium in persons older than 62 years in a long-term health care facility. Am J Cardiol. 1987;59(4):381-2.
11. Antonini-Canterin F, Huang G, Cervesato E, et al. Symptomatic aortic stenosis: does systemic hypertension play an additional role? Hypertension. 2003;41(6):1268-72.
12. Kadem L, Dumesnil JG, Rieu R, Durand LG, Garcia D, Pibarot P. Impact of systemic hypertension on the assessment of aortic stenosis. Heart. 2005;91(3):354-61.
13. Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. Eur J Echocardiogr. 2009;10(1):1-25. Erratum in: Eur J Echocardiogr. 2009;10(3):479.
14. Garcia D, Pibarot P, Dumesnil JG, Sakr F, Durand LG. Assessment of aortic valve stenosis severity: a new index based on the energy loss concept. Circulation. 2000;101(7):765-71.
15. Briand M, Dumesnil JG, Kadem L, Tongue AG, Rieu R, Garcia D, et al. Reduced systemic arterial compliance impacts significantly on left ventricular afterload and function in aortic stenosis: implications for diagnosis and treatment. J Am Coll Cardiol. 2005;46(2):291-8.
16. Lancellotti P, Donal E, Magne J, Moonen M, O’Connor K, Daubert JC, et al. Risk stratification in asymptomatic moderate to severe aortic stenosis: the importance of the valvular, arterial and ventricular interplay. Heart. 2010;96(17):1364-71.
17. Hachicha Z, Dumesnil JG, Bogaty P, Pibarot P. Paradoxical low-flow, low-gradient severe aortic stenosis despite preserved ejection fraction is associated with higher afterload and reduced survival. Circulation. 2007;115(22):2856-64.
18. Wan CK, Suri RM, Li Z, Orszulak TA, Daly RC, Schaff HV, et al. Management of moderate functional mitral regurgitation at the time of aortic valve replacement: is concomitant mitral valve repair necessary? J Thorac Cardiovasc Surg. 2009;137(3):635-40.
19. Unger P, Dedobbeleer C, Van Camp G, Plein D, Cosyns B, Lancellotti P. Mitral regurgitation in patients with aortic stenosis undergoing valve replacement. Heart. 2010;96(1):9-14.
20. Lancellotti P, Tribouilloy C, Hagendorff A, Moura L, Popescu BA, Agricola E, et al; European Association of Echocardiography. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 1: aortic and pulmonary regurgitation (native valve disease). Eur J Echocardiogr. 2010;11(3):223-44.
21. Griffin BP, Flachskampf FA, Siu S, Weyman AE, Thomas JD. The effects of regurgitant orifice size, chamber compliance, and systemic vascular resistance on aortic regurgitant velocity slope and pressure half-time. Am Heart J. 1991;122(4 Pt 1):1049-56.
22. Tribouilloy C, Avinee P, Shen WF, Rey JL, Slama M, Lesbre JP. End diastolic flow velocity just beneath the aortic isthmus assessed by pulsed Doppler echocardiography: a new predictor of the aortic regurgitant fraction. Br Heart J. 1991;65(1):37-40.
23. Messika-Zeitoun D, Aubry MC, Detaint D, Bielak LF, Peyser PA, Sheedy PF, et al. Evaluation and clinical implications of aortic valve calcification measured by electron-beam computed tomography. Circulation. 2004;110(3):356-62.
24. Cowell SJ, Newby DE, Burton J, White A, Northridge DB, Boon NA, et al. Aortic valve calcification on computed tomography predicts the severity of aortic stenosis. Clin Radiol. 2003;58(9):712-6.
25. Koos R, Kuhl HP, Muhlenbruch G, Wildberger JE, Gunther RW, Mahnken AH. Prevalence and clinical importance of aortic valve calcification detected incidentally on CT scans: comparison with echocardiography. Radiology. 2006;241(1):76-82.
26. Shah RG, Novaro GM, Blandon RJ, Whiteman MS, Asher CR, Kirsch J. Aortic valve area: meta-analysis of diagnostic performance of multi-detector computed tomography for aortic valve area measurements as compared to transthoracic echocardiography. Int J Cardiovasc Imaging. 2009;25(6):601-9.
27. Willson AB, Webb JG, Labounty TM, Achenbach S, Moss R, Wheeler M, et al. 3-dimensional aortic annular assessment by multidetector computed tomography predicts moderate or severe paravalvular regurgitation after transcatheter aortic valve replacement: a multicenter retrospective analysis. J Am Coll Cardiol. 2012;59(14):1287-94.
28. Jilaihawi H, Kashif M, Fontana G, Furugen A, Shiota T, Friede G, et al. Cross-sectional computed tomographic assessment improves accuracy of aortic annular sizing for transcatheter aortic valve replacement and reduces the incidence of paravalvular aortic regurgitation. J Am Coll Cardiol. 2012;59(14):1275-86.
29. Konen E, Goitein O, Feinberg MS, Eshet Y, Raanani E, Rimon U, et al. The role of ECG-gated MDCT in the evaluation of aortic and mitral mechanical valves: initial experience. AJR Am J Roentgenol. 2008;191(1):26-31.
30. Feuchtner GM, Dichtl W, Schachner T, Müller S, Mallouhi A, Friedrich GJ, et al. Diagnostic performance of MDCT for detecting aortic valve regurgitation. AJR Am J Roentgenol. 2006;186(6):1676-81.
31. Feuchtner GM, Dichtl W, Muller S, Müller S, Jodocy D, Schachner T, et al. 64-MDCT for diagnosis of aortic regurgitation in patients referred to CT coronary angiography. AJR Am J Roentgenol. 2008;191(1):W1-7.
32. Debl K, Djavidani B, Seitz J, Nitz W, Schmid FX, Muders F, et al. Planimetry of aortic valve area in aortic stenosis by magnetic resonance imaging. Invest Radiol. 2005;40(10):631-6.
33. John AS, Dill T, Brandt RR, Rau M, Ricken W, Bachmann G, et al. Magnetic resonance to assess the aortic valve area in aortic stenosis: how does it compare to current diagnostic standards? J Am Coll Cardiol. 2003;42(3):519-26.
34. Kupfahl C, Honold M, Meinhardt G, Vogelsberg H, Wagner A, Mahrholdt H, et al. Evaluation of aortic stenosis by cardiovascular magnetic resonance imaging: comparison with established routine clinical techniques. Heart. 2004;90(8):893-901.
35. Reant P, Lederlin M, Lafitte S, Serri K, Montaudon M, Corneloup O, et al. Absolute assessment of aortic valve stenosis by planimetry using cardiovascular magnetic resonance imaging: comparison with
261
Review Article
Arq Bras Cardiol. 2014; 103(3):251-263
Rajani et al.Multimodality Imaging of Heart Valve Disease
transesophageal echocardiography, transthoracic echocardiography, and cardiac catheterisation. Eur J Radiol. 2006;59(2):276-83.
36. Kilner PJ, Manzara CC, Mohiaddin RH, Pennell DJ, Sutton MG, Firmin DN, et al. Magnetic resonance jet velocity mapping in mitral and aortic valve stenosis. Circulation. 1993;87(4):1239-48.
37. Eichenberger AC, Jenni R, von Schulthess GK. Aortic valve pressure gradients in patients with aortic valve stenosis: quantification with velocity-encoded cine MR imaging. AJR Am J Roentgenol. 1993;160(5):971-7.
38. Caruthers SD, Lin SJ, Brown P, Watkins MP, Williams TA, Lehr KA, et al. Practical value of cardiac magnetic resonance imaging for clinical quantification of aortic valve stenosis: comparison with echocardiography. Circulation. 2003;108(18):2236-43.
39. Dweck MR, Joshi S, Murigu T, Alpendurada F, Jabbour A, Melina G, et al. Midwall fibrosis is an independent predictor of mortality in patients with aortic stenosis. J Am Coll Cardiol. 2011;58(12):1271-9.
40. Myerson SG. Heart valve disease: investigation by cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2012;14:7.
41. Aurigemma G, Reichek N, Schiebler M, Axel L. Evaluation of aortic regurgitation by cardiac cine magnetic resonance imaging: planar analysis and comparison to Doppler echocardiography. Cardiology. 1991;78(4):340-7.
42. Honda N, Machida K, Hashimoto M, Mamiya T, Takahashi T, Kamano T, et al. Aortic regurgitation: quantitation with MR imaging velocity mapping. Radiology. 1993;186(1):189-94.
43. Tribouilloy C, Shen WF, Rey JL, Adam MC, Lesbre JP. Mitral to aortic velocity-time integral ratio: a non-geometric pulsed-Doppler regurgitant index in isolated pure mitral regurgitation. Eur Heart J. 1994;15(10):1335-9.
44. Thomas JD, Weyman AE. Doppler mitral pressure half-time: a clinical tool in search of theoretical justification. J Am Coll Cardiol. 1987;10(4):923-9.
45. Wilkins GT, Weyman AE, Abascal VM, Block PC, Palacios IF. Percutaneous balloon dilatation of the mitral valve: an analysis of echocardiographic variables related to outcome and the mechanism of dilatation. Br Heart J. 1988;60(4):299-308.
46. Alkadhi H, Wildermuth S, Bettex DA, Plass A, Baumert B, Leschka S, et al. Mitral regurgitation: quantification with 16-detector row CT--initial experience. Radiology. 2006;238(2):454-63.
47. Messika-Zeitoun D, Serfaty JM, Laissy JP, Berhili M, Brochet E, Iung B, et al. Assessment of the mitral valve area in patients with mitral stenosis by multislice computed tomography. J Am Coll Cardiol. 2006;48(2):411-3.
48. Chan KM, Wage R, Symmonds K, Rahman-Haley S, Mohiaddin RH, Firmin DN, et al. Towards comprehensive assessment of mitral regurgitation using cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2008;10:61.
49. Kon MW, Myerson SG, Moat NE, Pennell DJ. Quantification of regurgitant fraction in mitral regurgitation by cardiovascular magnetic resonance: comparison of techniques. J Heart Valve Dis. 2004;13(4):600-7.
50. Kizilbash AM, Hundley WG, Willett DL, Franco F, Peshock RM, Grayburn PA. Comparison of quantitative Doppler with magnetic resonance imaging for assessment of the severity of mitral regurgitation. Am J Cardiol. 1998;81(6):792-5.
51. Djavidani B, Debl K, Lenhart M, Seitz J, Paetzel C, Schmid FX, et al. Planimetry of mitral valve stenosis by magnetic resonance imaging. J Am Coll Cardiol. 2005;45(12):2048-53.
52. Djavidani B, Debl K, Buchner S, Lipke C, Nitz W, Feuerbach S, et al. MRI planimetry for diagnosis and follow-up of valve area in mitral stenosis treated with valvuloplasty. Rofo. 2006;178(8):781-6.
53. Lancellotti P, Moura L, Pierard LA, Agricola E, Popescu BA, Tribouilloy C, et al. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 2: mitral and tricuspid regurgitation (native valve disease). Eur J Echocardiogr. 2010;11(4):307-32.
54. Gonzalez-Vilchez F, Zarauza J, Vazquez de Prada JA, Martín Durán R, Ruano J, Delgado C, et al. Assessment of tricuspid regurgitation by Doppler color flow imaging: angiographic correlation. Int J Cardiol. 1994;44(3):275-83.
55. Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation. 2008;117(13):1717-31.
262

Review Article
Arq Bras Cardiol. 2014; 103(3):251-263263

Letter to the Editor
Is Sildenafil a Therapeutic Option for Noncompaction?Josef Finsterer and Claudia StöllbergerKrankenanstalt Rudolfstiftng, Vienna, Austria
To the editorWith interest we read the article by Redondo et al1
about a 6yo male with heart failure and left-ventricular hypertrabeculation/noncompaction (LVHT)1. We have the following comments and concerns.
Though LVHT is congenital in the majority of the cases, there are some cases in which LVHT is not present on previous echocardiographies (acquired LVHT)2. In such cases, LVHT may be truly absent or hidden. Hidden LVHT may occur if there is severe myocardial thickening or severe dilatation.
We do not agree that pulmonary embolism is a major complication of LVHT1. LVHT is an abnormality of the left ventricle. Thus, LVHT is frequently associated with ischemic stroke or systemic embolism due to emboli originating from the intertrabecular recessus of the left ventricular myocardium.
LVHT is not directly attributable to a single genetic defect. It is rather a secondary reaction to primary affection of the heart by a genetic or chromosomal defect3. Typically, it does not occur in each carrier of a mutation, but only in some rare cases, without knowing the cause of this selectivity.
The presented case is interesting for the beneficial effect of sildenafil for heart failure. Did sildenafil also have a beneficial effect on the trabeculations? Did the amount of trabeculae
regress? Did the ratio non-compacted layer to compacted layer decrease during therapy?
The authors mention that LVHT was first described in 1932 on autopsy. It would be interesting to know the reference of this observation, since there is ongoing debate about the first description of LVHT.
LVHT is frequently associated with neuromuscular disorders (NMDs). Was the patient ever seen by a myologist to rule out a NMD? Did the patient present with features of a NMD, such as weakness, wasting, fatigue, exercise intolerance, or double vision? Was the family history positive for NMD?
Occasionally, LVHT is associated with pulmonary hypertension4. Was the pressure of the pulmonary artery measured, and, if increased, did sildenafil also have a beneficial effect on this parameter, since it is also given in this indication?
We do not agree that LVHT in adults occurs only in the absence of other concomitant structural cardiac diseases. In adults, LVHT has been described in association with Ebstein’s anomaly or aortic root dilatation5.
Overall, there is a need to thoroughly investigate patients with LVHT, not only for cardiac disease but also for extra-cardiac manifestations. A comprehensive appreciation is necessary to optimize the management of LVHT patients.
Mailing Address: Josef Finsterer •Postfach 20, Vienna. 1180, AustriaEmail: [email protected] received Abril 11, 2014; revised manuscript June 25, 2014; accepted June 25, 2014.
KeywordsH e a r t D e f e c t s , C o n g e n i t a l ; H e a r t Fa i l u r e ;
Cardiomyopathy, Dilated/complications; Phosphodiesterase Inibitors/therapeutic use.
1. Redondo AC, Fuenmayor G, Shiraishi KS, Fontes SR, Elias PF, Souza R, Jatene IB. Sildenafil for Noncompaction Cardiomyopathy Treatment in a Child: Case Report. Arq Bras Cardiol. 2014;102(3):27.
2. Finsterer J, Stöllberger C, Schubert B. Acquired left ventricular noncompaction as a cardiac manifestation of neuromuscular disorders. Scand Cardiovasc J 2008;42(1):25-30.
3. Finsterer J. Cardiogenetics, neurogenetics, and pathogenetics of left ventricular hypertrabeculation/noncompaction. Pediatr Cardiol 2009;30(5):659-81.
4. Tian T, Liu Y, Gao L, Wang J, Sun K, Zou Y, et al. Isolated left ventricular noncompaction: clinical profile and prognosis in 106 adult patients. Heart Vessels.2013;Oct 2.[Epub ahead of print]
5. Hajj-Chahine J, Allain G, Tomasi J, Jayle C, Corbi P. Aortic root replacement in a patient with left ventricular noncompaction. Ann Thorac Surg. 2014;97(1):e1-3.
References
DOI: 10.5935/abc.20140131
264

Letter to the Editor
Josef FinstererIs sildenafil a therapeutic option for noncompaction?
Arq Bras Cardiol. 2014; 103(3):264-265 265
Anatomopathological Session
Case 4/2014 - A 66-Year-Old Man with Acute Myocardial Infarction and Death in Asystole after Primary Coronary AngioplastyWilma Noia Ribeiro, Alice Tatsuko Yamada, Luiz Alberto BenvenutiInstituto do Coração (InCor) HC-FMUSP, São Paulo, SP - Brazil
Mailing Addres: Vera Demarchi Aiello •Avenida Dr. Enéas de Carvalho Aguiar, 44, subsolo, bloco I, Cerqueira César. Postal Code 05403-000, São Paulo, SP – BrazilE-mail: [email protected], [email protected]
KeywordsMyocardial Infarction; Heart Arrest; Angioplasty,
Balloon, Coronary.
A 66-year-old man sought medical care at the hospital due to severe chest pain lasting for 24 hours. The patient was aware of being hypertensive and was a smoker. Without any prior symptom, he started to have severe chest pain and sought emergency medical care after about 24 hours, due to pain persistence.
At physical examination (August 13, 2005, 10 PM) he had a heart rate of 90 bpm and blood pressure of 110/70 mmHg. Lung examination showed no alterations. Heart assessment showed a systolic murmur in the lower left sternal border and mitral area.
The initial electrocardiogram (August 13, 2005, 22 h) showed HR of 100 bpm, sinus rhythm, 1st-degree atrioventricular block (PR 240 ms), low-voltage QRS complexes in the frontal plane, QRS complex electrical alternans and extensive ongoing anterior wall infarction (QS V1 to V6, ST elevation in the same leads and QS in the inferior wall, II, III and aVF) (Figure 1).
Acetylsalicylic acid by oral route and 5 mg of intravenous metoprolol were administered. The patient had bradycardia and cardiorespiratory arrest in pulseless electrical activity, reversed after five minutes. He developed hypotension and peripheral hypoperfusion and was transferred to InCor (The Heart Institute).
On admission he had received heparin and continuous intravenous norepinephrine. BP was 60/30 mmHg.
The ECG (August 13, 2005, 11:36 PM) disclosed heart rate of 116 bpm, junctional escape rhythm with sinus arrest and atrial extrasystoles); low-voltage QRS complex in the frontal plane, extensive ongoing anterior acute myocardial infarction, inactive area in the inferior wall; presence of ST elevation at V1 to V5 and ST depression in leads I, II and aVF; ST elevation in aVR (Figure 2).
Coronary angiography was indicated, which disclosed anterior interventricular branch occlusion and images
suggestive of intracoronary thrombus, lesion of 70% in the circumflex artery, 50% in the right coronary artery and 70% in the ostium of the right posterior descending branch. Angioplasty was performed with stent implant in the anterior interventricular artery, but distal flow was not restored. This was followed by cardiac arrest in asystole, which did not respond to treatment and the patient died.
Clinical Aspects This clinical case reports on a 66-year-old hypertensive
patient, long-term smoker, who sought medical care due to acute chest pain. The main diagnostic hypothesis for this clinical case is of acute coronary syndrome.
Chest pain is one of the most common reasons for seeking emergency care and remains a challenge for the clinician, due to the difficulty in differentiating between non-emergency diagnoses and those of high morbidity and mortality, such as acute coronary syndrome (ACS), aortic dissection and pulmonary thromboembolism.
In the assessment of acute chest pain, there are three basic parameters for its management: clinical examination (clinical history and physical examination), electrocardiogram (ECG) and myocardial necrosis markers. They should be analyzed together to provide a safer approach to the patient, especially when it is necessary ruling out ACS. Chest radiography, chest Computed Tomography Angiography (CTA), echocardiography and other tests may be useful in the differential diagnosis.
Approximately 15-25% of patients presenting in the ER with chest pain are diagnosed with acute coronary syndrome, and this represents its more frequent clinical manifestation1. Therefore, in the first step of the evaluation, which is the clinical examination, the greater determinant of an ischemic etiology is the characteristic presence of angina.
Angina is often described as a burning or compression sensation or difficulty breathing, located in the precordial region or any other region of the chest, radiating to the neck, shoulder and left arm. It usually increases in intensity within minutes and may be accompanied by symptoms such as nausea and sweating. It can be triggered by physical or emotional stress and relieved by rest or use of nitrates. It should also be remembered that ACS can occur without obvious precipitating factors and be asymptomatic or present as ischemic equivalent, especially in the elderly and diabetic patients with autonomic dysfunction (dyspnea, syncope and pre-syncope).
On the other hand, there are characteristics of pain that make the diagnosis of ACS unlikely, such as pleuritic pain (reproduced by respiratory movements) located with the fingertip, pain in meso/hypogastrium region and reproduction of pain with local
Section Editor: Alfredo José Mansur ([email protected])
Associated Editors: Desidério Favarato ([email protected])
Vera Demarchi Aiello ([email protected])
DOI: 10.5935/abc.20140129
e31
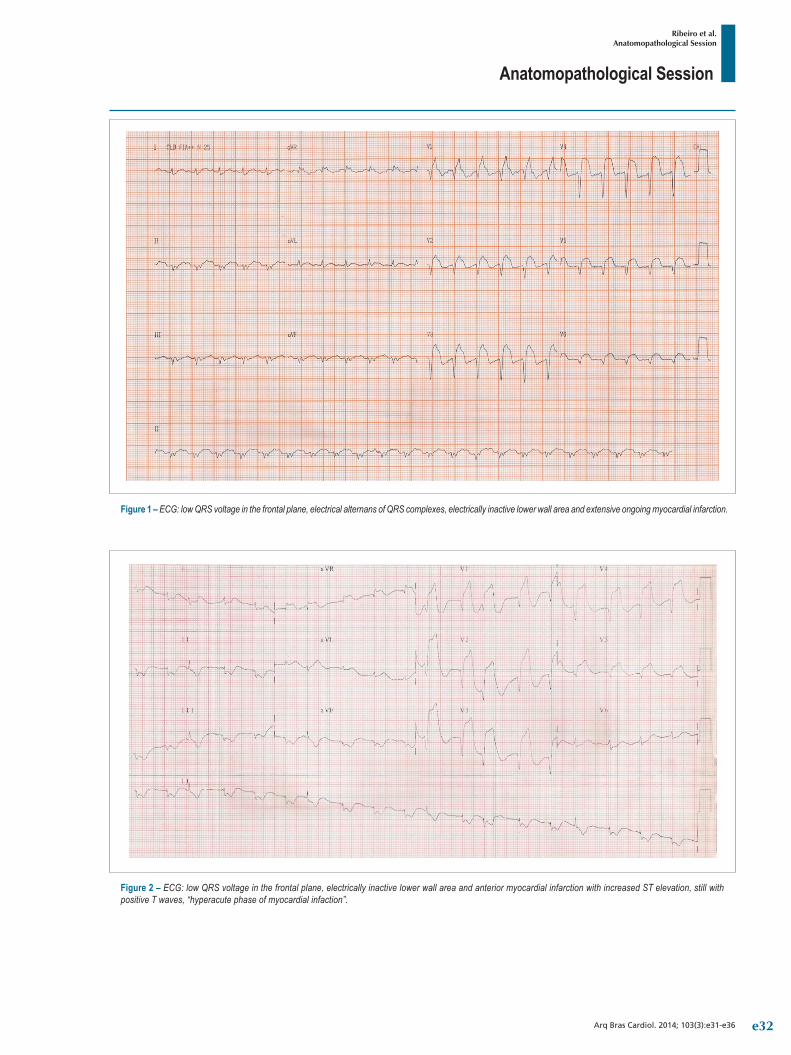
Anatomopathological Session
Ribeiro et al.Anatomopathological Session
Arq Bras Cardiol. 2014; 103(3):e31-e36
Figure 1 – ECG: low QRS voltage in the frontal plane, electrical alternans of QRS complexes, electrically inactive lower wall area and extensive ongoing myocardial infarction.
Figure 2 – ECG: low QRS voltage in the frontal plane, electrically inactive lower wall area and anterior myocardial infarction with increased ST elevation, still with positive T waves, “hyperacute phase of myocardial infaction”.
e32

Anatomopathological Session
Ribeiro et al.Anatomopathological Session
Arq Bras Cardiol. 2014; 103(3):e31-e36
palpation or movement. These features raise the suspicion of other differential diagnoses such as pericarditis, pleuritis, gastrointestinal or musculoskeletal diseases.
In the present case report, the patient presented with prolonged chest pain, which does not rule out acute coronary syndrome (ACS), but raises the possibility of some condition associated with this coronary picture, such as pericarditis or mechanical complications.
Among the most important risk factors for atherosclerotic disease risk are dyslipidemia, diabetes mellitus, hypertension, male gender, older age, obesity/metabolic syndrome, smoking, sedentary lifestyle, chronic kidney disease, depression and stress. This patient had some risk factors that contributed to the development of coronary artery disease: age, male gender, hypertension and smoking.
Patients with chest pain and ACS often have a nonspecific physical examination, with less than 20% of them showing significant alterations in the initial evaluation2. This becomes important by helping in the detection of differential diagnoses (e.g., pericardial friction rub in pericarditis) or by inferring the presence of risk factors for coronary artery disease (abdominal or carotid murmur, among others).
However, when findings resulting from an ACS are present, they indicate a worse prognosis due to mechanical complications or due to a large area of myocardium at risk and ventricular dysfunction (hypotension, tachycardia, pulmonary edema and mitral regurgitation murmur secondary to ischemia).
The electrocardiogram is important in the diagnostic, prognostic and therapeutic approach and must be obtained within 10 minutes after the presentation of patients with ongoing chest pain2. A normal electrocardiographic tracing does not exclude the possibility of ACS and a serial ECG is indicated, which increases its sensitivity and helps differentiating between acute and chronic alterations.
The patient reported in this clinical case had, at the admission ECG performed at another service, ST-segment elevation in the anterior wall, suggesting the hypothesis of acute coronary syndrome with ST-segment elevation. However, this ECG also showed low voltage and electrical alternans of the QRS complex, which suggests large pericardial effusion or even cardiac tamponade.
The main hypothesis for this pericardial effusion is a mechanical complication of myocardial infarction: left ventricular free wall rupture. It occurs within 24 hours after infarction or between the third and fifth day, has an incidence of 0.8 to 6.2% and is more common in an extensive myocardial infarction, in the elderly, women and hypertensive patients. Its clinical course is variable3 and may be acute and severe, leading to sudden death or subacute, with nonspecific clinical manifestations.
Other mechanical complications that may be present in myocardial infarction are papillary muscle and interventricular septum rupture. These complications do not present with significant pericardial effusion and normal pulmonary auscultation in this patient also makes the diagnosis of papillary muscle rupture less likely. This clinical condition presents with pulmonary congestion due to volume overload secondary to acute mitral regurgitation.
Another diagnostic hypothesis for this patient presenting with chest pain and pericardial effusion would be aortic dissection. Pain, in these cases, is usually of sudden onset and strong intensity since the beginning (unlike angina pain, which often increasingly escalates). It is often described as excruciating and its location reflects the site and progression of the dissection. Autonomic signs (pallor, profuse sweating) are greatly associated.
In aortic dissection, physical examination may disclose hypertensive crisis, differences between limb pulses, signs of pleural and pericardial effusion, diastolic murmur of aortic regurgitation, different from the systolic murmur detected in this clinical case. The extension of the dissection to other vessels can lead to other symptoms corresponding to ischemia of the organs irrigated by them: cerebrovascular accident, acute myocardial infarction, mesenteric ischemia, etc.
Another diagnostic hypothesis for the clinical case is pulmonary embolism. The absence of pulmonary symptoms, mainly dyspnea, makes this hypothesis less likely. It is the most common symptom of this disease, occurring in over 78% of the patients4. Sudden chest pain of sudden onset and very often pleuritic, affects up to 44% of patients4. Cough and hemoptysis may also occur. Additionally, there was no mention is made on admission at the other service, of right ventricular dysfunction manifestations, such as jugular stasis and hypotension.
The patient, an hour and 36 minutes after his admission at the Heart Institute, was submitted to coronary angiography with left anterior descending artery angioplasty. However, he developed asystole and cardiac arrest.
The main diagnoses for the final clinical picture are cardiogenic shock and/or distributive shock due to cardiac tamponade, discussed below.
The hypothesis of cardiogenic shock should be considered, as the patient had an extensive acute myocardial infarction without culprit artery reperfusion even after percutaneous revascularization attempt. However, this diagnosis cannot fully explain the patient’s clinical condition, such as the absence of pulmonary congestion, which usually follows an acute myocardial failure.
Considering the patient’s history, late cardiac tamponade seems to have been the main precipitating factor of the final clinical picture in this case. The electrocardiographic findings commonly observed in cardiac tamponade are low voltage and electrical alternans of the QRS complex, observed in the case. Although physical examination made no reference to clinical findings suggestive of tamponade, such as jugular stasis or muffled heart sounds, we cannot exclude this diagnostic hypothesis.
An echocardiography could have been performed to confirm this diagnosis, which is the most widely used noninvasive method for diagnostic investigation of this pathology. The ventriculography in this context would not be informative, as it was a free wall rupture with cardiac tamponade and thus, it would not allow the visualization of contrast leakage into the pericardial cavity.
e33

Anatomopathological Session
Ribeiro et al.Anatomopathological Session
Arq Bras Cardiol. 2014; 103(3):e31-e36
This is a patient with myocardial infarction that came at the emergency room more than 24 hours after the onset of the event and who probably had a mechanical complication of myocardial infarction: ventricular free wall rupture.
Most deaths from myocardial infarction occur in the first hours of disease onset, with 40-65% occurring within the first hour and approximately 80% in the first 24 hours5,6. The recently implemented therapies for MI treatment have been proven to modify patient evolution and prognosis. However, the effectiveness of most of these measures is time-dependent and delay in seeking medical care may have been the factor that likely contributed to the clinical outcome of the patient in this case report. (Dr. Wilma Noia Ribeiro, Dr. Alice Tatsuko Yamada)
Diagnostic hypotheses: Acute myocardial infarction with mixed shock (cardiogenic - distributive) by mechanical complication - free wall rupture with tamponade (Dr. Wilma Noia Ribeiro, Dr. Alice Tatsuko Yamada)
NecropsyThe heart weighed 414 g. The myocardium of the left
ventricular anterosseptal wall and right ventricular anterior wall was softened, slightly yellowish in color, characterizing extensive transmural acute myocardial infarction. There was an obvious narrowing of the affected anterosseptal wall, with ventricular septum rupture in the anterior region of its mid portion, with a ventricular septal defect measuring 10 mm in its longest axis. The other left ventricular walls showed to be slightly hypertrophic and there was a small area of fibrosis in the postero-inferior region of the ventricular septum. There was also moderate right ventricular dilation (Figure 3).
Histological analysis confirmed the presence of myocardial infarction, with marked neutrophil infiltration, confirming histological dating of 24-48 hours of onset. Another small ongoing microinfarction was observed in the posterior region of the ventricular septum, in addition to the previously described small area of fibrosis (healed infarction), compatible with approximately 7-10 days of evolution.
There was superficial fibrin deposition in the epicardium, with the presence of reactive inflammatory infiltrate. Examination of the initial segment of the left anterior descending artery showed fatty atherosclerotic plaques with areas of marked thinning of the fibrous cap that covered the lipid core and 80% of obstruction.
There were also areas of plaque rupture and hemorrhage, with acute thrombosis in the first and second centimeters of that artery (Figs. 4 and 5).
The lungs weighed 1,208 g together and showed alveolar edema. The kidneys showed irregular surface and retention cysts, with hyaline arteriolosclerosis on histological examination. The aorta showed mild / moderate degree of atherosclerosis. (Dr. Luiz Alberto Benvenuti)
Anatomopathological diagnoses. Coronary atherosclerosis; acute myocardial infarction involving the left ventricular anterosseptal wall and the right ventricular anterior wall; rupture of the ventricular septum, with VSD; acute pulmonary edema (cause of death) (Dr. Luiz Alberto Benvenuti).
CommentsThis is the case report of a 66-year-old man with systemic
hypertension and a chronic smoker that presented with acute severe chest pain. After medical assessment, he was diagnosed with acute myocardial infarction and the patient underwent
Figure 3 – Cross-section of the ventricles showing left ventricular transmural infarction of the anterosseptal wall (asterisks) and of the right ventricular anterior wall (arrows). The explorer shows the VSD secondary to septal rupture. Observe the ventricular wall thinning and the small area of fibrosis in the ventricular septum (arrowhead).
e34
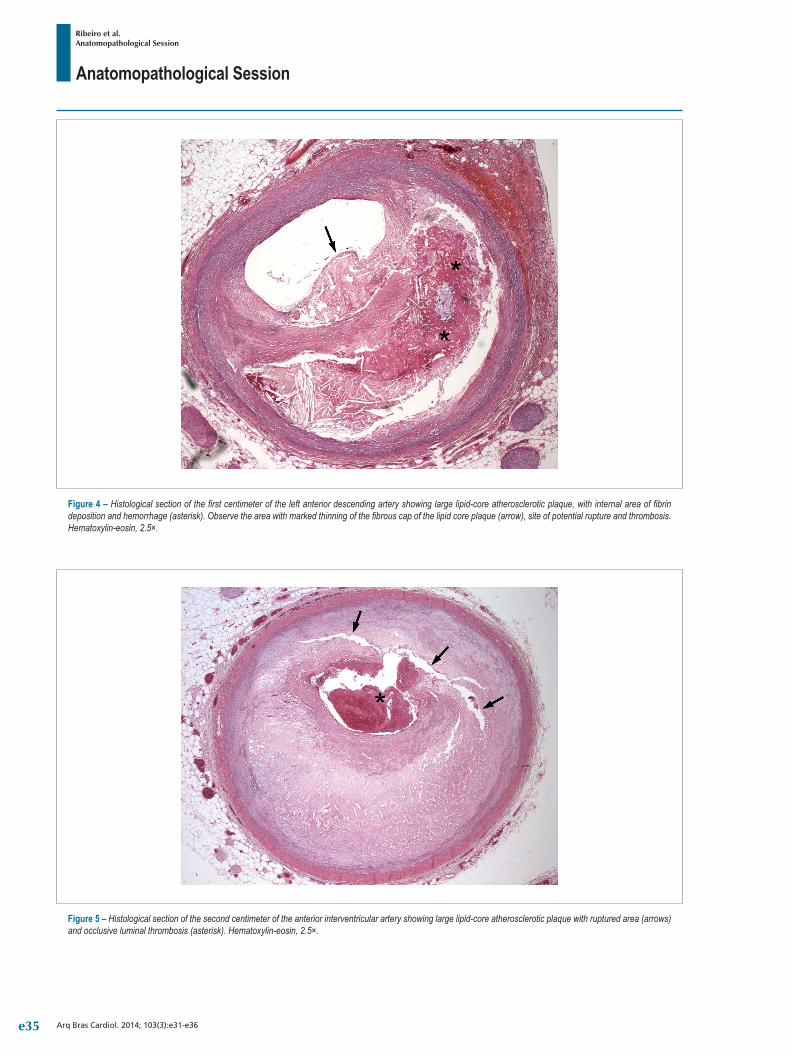
Anatomopathological Session
Ribeiro et al.Anatomopathological Session
Arq Bras Cardiol. 2014; 103(3):e31-e36
Figure 4 – Histological section of the first centimeter of the left anterior descending artery showing large lipid-core atherosclerotic plaque, with internal area of fibrin deposition and hemorrhage (asterisk). Observe the area with marked thinning of the fibrous cap of the lipid core plaque (arrow), site of potential rupture and thrombosis. Hematoxylin-eosin, 2.5×.
Figure 5 – Histological section of the second centimeter of the anterior interventricular artery showing large lipid-core atherosclerotic plaque with ruptured area (arrows) and occlusive luminal thrombosis (asterisk). Hematoxylin-eosin, 2.5×.
e35

Anatomopathological Session
Ribeiro et al.Anatomopathological Session
Arq Bras Cardiol. 2014; 103(3):e31-e36
coronary angiography, which disclosed proximal occlusion of the left anterior descending artery with images suggesting the presence of thrombi. He was submitted to balloon-angioplasty in the affected segment without restoration of distal coronary flow (unsuccessful procedure) and the patient developed irreversible cardiac arrest and died.
The autopsy confirmed acute myocardial infarction, which was very extensive, affecting the left ventricular anterosseptal wall and the right ventricular anterior wall. Histological dating was 24-48 hours of onset, consistent with the clinical history. It is noteworthy the fact that the detailed examination of the ventricular septum showed the presence of two previous microinfarctions, an old (healed) one and an ongoing one.
The presence of atherosclerosis of the coronary arteries was identified, with massive plaques in the proximal segment of the left anterior descending artery, which resulted in chronic obstruction of 80% of the lumen. The fatty plaques
had extensive lipid cores and there were areas of marked thinning of the fibrous cap that covered the cores, as well as areas of rupture associated with acute thrombosis of the remaining lumen in the first two centimeters of the left anterior descending artery. It is known that acute coronary occlusions with luminal thrombosis are usually associated with large lipid-core plaques, which undergo rupture due to the instability of their thin fibrous cap7, as observed in this case.
Aside from the great extent of the infarcted area, the patient developed an important mechanical complication of acute myocardial infarction, the occurrence of ventricular septal rupture with the establishment of VSD8 - which certainly aggravated his hemodynamic condition, progressing to cardiogenic shock -, acute pulmonary edema and death. It should be emphasized that the patient had two classic risk factors for atherosclerosis and myocardial infarction: systemic hypertension and chronic smoking9. (Dr. Luiz Alberto Benvenuti)
1. Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med. 2000; 342(16):1163-70.
2. Piegas LS, Feitosa G, Mattos LA, Nicolau JC, Rossi Neto JM, Timerman A , et al. Sociedade Brasileira de Cardiologia. Diretriz da Sociedade Brasileira de Cardiologia sobre tratamento do infarto agudo do miocárdio com supradesnível do segmento ST. Arq Bras Cardiol. 2009; 93(6 supl.2):e179-e264.
3. Becker RC, Gore JM, Lambrew C, Weaver WD, Rubison RM, French WJ, et al. A composite view of cardiac rupture in the United States National Registry of Myocardial Infarction. J Am Coll Cardiol. 1996; 27(6):1321-6.
4. Miniat M, Prediletto R, Formichi B, Marini C, Di Ricco G, Tornelli L, et al. Accuracy of clinical assesment in the diagnosis of pulmonary embolism. Am J Respir Crit Care Med. 1999; 159(3):864-71.
5. Kannel WB, Cupples LA, D’Agostino RB. Sudden death risk in overt coronary heart disease: the Framingham Study. Am Heart J. 1987; 113(3):799-804.
6. Tunstall-Pedoe H, Kuulasmaa K, Amouyel P, Arveiler D, Rajakangas AM, Pajak A. Myocardial infarction and coronary deaths in the World Health Organization MONICA Project. Registration procedures, event rates, and case-fatality rates in 38 populations from 21 countries in four continents. Circulation. 1994; 90(1):583-612.
7. Fleg JL, Stone GW, Fayad ZA, Granada JF, Hatsukami TS, Kolodgie FD, et al. Detection of high-risk atherosclerotic plaque: report of the NHLBI Working Group on current status and future directions. JACC Cardiovasc Imaging. 2012; 5(9):941-55.
8. Birnbaum Y, Fishbein MC, Blanche C, Siegel RJ. Ventricular septal rupture after acute myocardial infarction. N Engl J Med. 2002; 347(18):1426-32.
9. Land in i L , Leone A . Smok ing and hyper tens ion: e f fec t s on clinical, biochemical and pathological variables due to isolated or combined action on cardiovascular system. Curr Pharm Des. 2011; 17(28):2987-3001.
References
e36

Case Report
Sudden Cardiac Death and Short QT SyndromeMaria Lícia Ribeiro Cury Pavão, Viviane Cristina Ono, Elerson Arfelli, Marcus Vinícius Simões, José Antonio Marin Neto, André SchmidtDivisão de Cardiologia do Departamento de Clínica Médica do Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo, São Paulo, SP - Brazil
Mailing Address: André Schmidt •Avenida dos Bandeirantes n 3900 Bairro Campus Universitario Monte Alegre Postal Code 14048-900 Ribeirão Preto, São Paulo, SP - BrazilE-mail: [email protected], [email protected] Manuscript received May 23, 2013; revised manuscript July 03, 2013; accepted December 17, 2013.
KeywordsDeath, sudden; short QT syndrome; concealed accessory
atrioventricular pathway.
DOI: 10.5935/abc.20140133
IntroductionThe evaluation of patients recovered from sudden death
(SD) is based on diagnostic investigation aiming to identify structural heart diseases or exclusion of noncardiac diseases and metabolic disorders. After exclusion of these pathologies, one is faced with sudden cardiac death (SCD) without structural heart disease, in which electrical and latent heart diseases account for up to 56% of cases, while the remaining is considered idiopathic disease ¹. This latter group has been gradually reduced due to the increasing characterization of molecular mechanisms that generate potentially lethal arrhythmias. We report the case of a young patient recovered from SCD, with no apparent structural heart disease, probably due to electrical heart disease associated with occult anomalous bundle and both diagnoses being possible according to the available means in clinical practice.
Case ReportMale patient, Caucasian, 23 years old, single, printing
technician, referred with a three-month history of intense palpitations and loss of consciousness during a soccer match. According to the reports of witnesses, the patient was taken to the nearest Basic Health Unit (BHU), a five-minute trajectory, as he was unconscious and unresponsive to stimuli and cardiopulmonary arrest (CPA) in asystole was verified by the physician present at the BHU. Cardiopulmonary resuscitation was initiated, with total CPR time of 25 minutes. The patient was then taken to the local ICU, where he was treated with induced hypothermia (32-34ºC) for 24 h. There was complete neurological recovery and he was discharged in five days.
The patient reported having palpitations triggered by great exertion lasting 30-40 minutes, with no associated symptoms, which improved with rest since the age of 14 years. He reported two episodes of loss of consciousness: at 18, while swimming, he had palpitations, no other associated symptoms; right after leaving the pool, he lost
consciousness, with rapid recovery and no mental confusion or sphincter release; at 19, while playing soccer, he had an episode of syncope with the same characteristics.
He had no other known diseases or history of SD in the family. He denied alcoholism, smoking, use of illicit drugs or medications. On physical examination, no abnormalities were observed, especially in the cardiovascular system. He was admitted for investigation and the following test results were obtained:
- Electrocardiogram (ECG): Sinus rhythm, 55 bpm, PR interval: 130 ms, QRS: 60 ms, QTc: 349 ms (maximum slope method and Framingham formula), J-point to T-wave-peak interval: 220 ms (Figure 1).
- Stress test: Treadmill Ramp Protocol (4.5km/h to 9 km/h/ 6% to 16%); 15.7 MET. Maximum HR: 200 bpm. No arrhythmias. Pre-stress HR and QTc intervals, peak and recovery, respectively: 94 bpm, 431 ms, 200 bpm, 422 ms, 130 bpm, 404 ms.
- Holter: Sinus rhythm. Mean HR: 79 bpm, minimum, 53 bpm (sleep) and maximum of 179 bpm (watching a game). Normal RR range. Two isolated ventricular extrasystoles. Rare atrial extrasystoles.
- Echocardiogram: Cardiac chambers of normal dimensions; ejection fraction of 77%, preserved segmental motility.
- Cardiac MRI: Ejection fraction: 67% (left ventricle) and 60% (right ventricle). Morphologically normal heart. Absence of regional alterations in contractility. No areas of delayed myocardial enhancement after paramagnetic contrast.
- Cardiac catheterization: Coronary arteries with normal origin and trajectory and free of obstructive lesions.
- Electrophysiological study: normal AH and HV intervals (AH = 70 ms; HV = 38 ms)
Atrial stimulation: ventricular activation through AV node; Normal Wenckebach point (350 ms). Atrioventricular induction by orthodromic reentrant tachycardia (AVT) with retrograde atrial activation starting earlier in the distal coronary sinus electrogram (accessory pathway with exclusively retrograde conduction in the lateral portion of the mitral annulus) (Figure 1).
Ventricular stimulation: eccentric retrograde atrial activation, starting earlier in the distal coronary sinus electrogram (Figure 1).
Radiofrequency ablation performed via accessory pathway.
QTc interval measurements (Bazett's formula): 338 msec (pre-ablation), 388 ms (post-ablation) and 342 ms after isoproterenol (3 mcg/kg/min).
e37
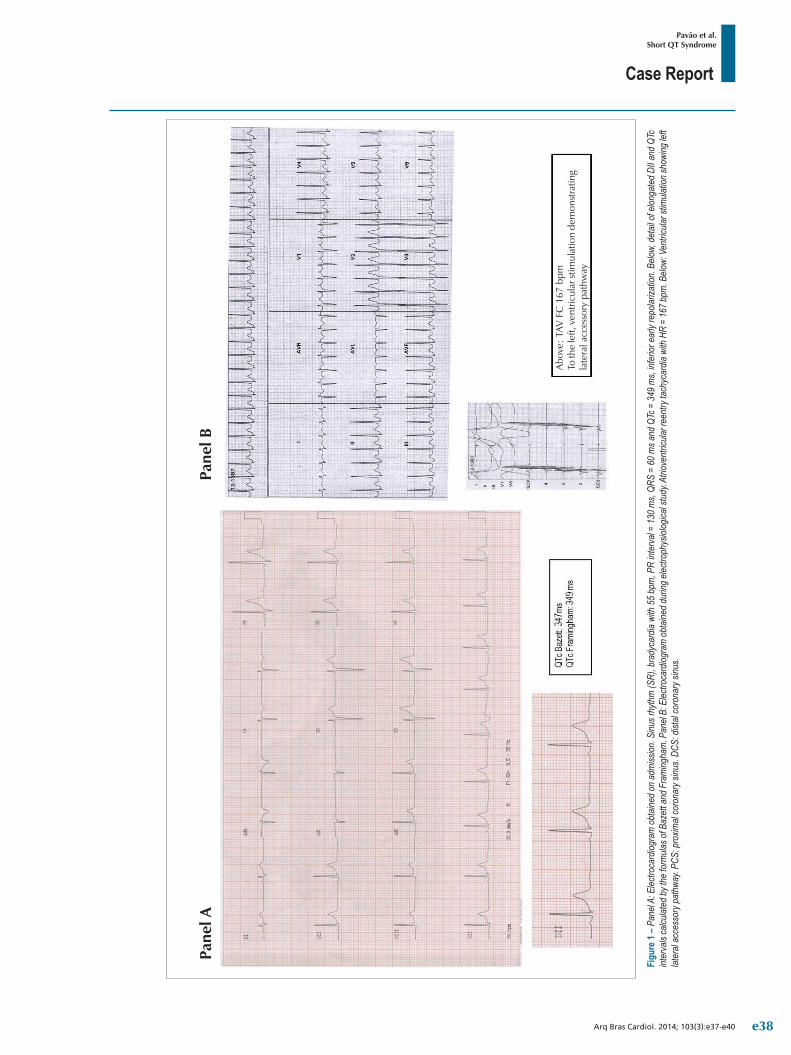
Case Report
Pavão et al.Short QT Syndrome
Arq Bras Cardiol. 2014; 103(3):e37-e40
Figu
re 1
– Pan
el A:
Elec
troca
rdiog
ram
obt
ained
on
adm
ission
. Sinu
s rhy
thm
(SR)
, bra
dyca
rdia
with
55
bpm
, PR
inter
val =
130
ms,
QRS
= 60
ms a
nd Q
Tc =
349
ms,
infer
ior e
arly
repo
lariza
tion.
Belo
w, d
etail
of e
longa
ted
DII a
nd Q
Tc
inter
vals
calcu
lated
by th
e for
mula
s of B
azet
t and
Fra
ming
ham
. Pan
el B:
Elec
troca
rdiog
ram
obta
ined d
uring
elec
troph
ysiol
ogica
l stu
dy. A
triov
entri
cular
reen
try ta
chyc
ardia
with
HR
= 16
7 bpm
. Belo
w: V
entri
cular
stim
ulatio
n sho
wing
left
later
al ac
cess
ory p
athw
ay. P
CS: p
roxim
al co
rona
ry si
nus.
DCS:
dist
al co
rona
ry si
nus.
Pane
l APa
nel B
Abo
ve: T
AV F
C 1
67 b
pmTo
the
left,
ven
tricu
lar s
timul
atio
n de
mon
stra
ting
late
ral a
cces
sory
pat
hway
e38
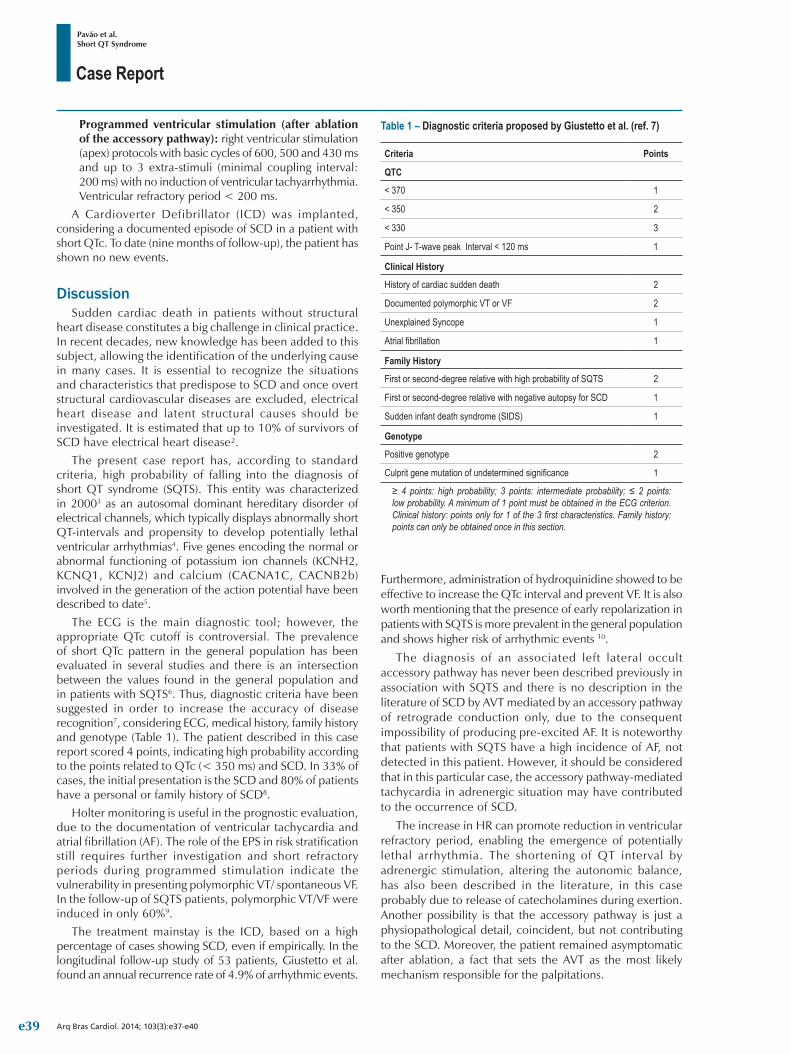
Case Report
Pavão et al.Short QT Syndrome
Arq Bras Cardiol. 2014; 103(3):e37-e40
Table 1 – Diagnostic criteria proposed by Giustetto et al. (ref. 7)
Criteria Points
QTC
< 370 1
< 350 2
< 330 3
Point J- T-wave peak Interval < 120 ms 1
Clinical History
History of cardiac sudden death 2
Documented polymorphic VT or VF 2
Unexplained Syncope 1
Atrial fibrillation 1
Family History
First or second-degree relative with high probability of SQTS 2
First or second-degree relative with negative autopsy for SCD 1
Sudden infant death syndrome (SIDS) 1
Genotype
Positive genotype 2
Culprit gene mutation of undetermined significance 1
≥ 4 points: high probability; 3 points: intermediate probability; ≤ 2 points: low probability. A minimum of 1 point must be obtained in the ECG criterion. Clinical history: points only for 1 of the 3 first characteristics. Family history: points can only be obtained once in this section.
Programmed ventricular stimulation (after ablation of the accessory pathway): right ventricular stimulation (apex) protocols with basic cycles of 600, 500 and 430 ms and up to 3 extra-stimuli (minimal coupling interval: 200 ms) with no induction of ventricular tachyarrhythmia. Ventricular refractory period < 200 ms.
A Cardioverter Defibrillator (ICD) was implanted, considering a documented episode of SCD in a patient with short QTc. To date (nine months of follow-up), the patient has shown no new events.
DiscussionSudden cardiac death in patients without structural
heart disease constitutes a big challenge in clinical practice. In recent decades, new knowledge has been added to this subject, allowing the identification of the underlying cause in many cases. It is essential to recognize the situations and characteristics that predispose to SCD and once overt structural cardiovascular diseases are excluded, electrical heart disease and latent structural causes should be investigated. It is estimated that up to 10% of survivors of SCD have electrical heart disease².
The present case report has, according to standard criteria, high probability of falling into the diagnosis of short QT syndrome (SQTS). This entity was characterized in 20003 as an autosomal dominant hereditary disorder of electrical channels, which typically displays abnormally short QT-intervals and propensity to develop potentially lethal ventricular arrhythmias4. Five genes encoding the normal or abnormal functioning of potassium ion channels (KCNH2, KCNQ1, KCNJ2) and calcium (CACNA1C, CACNB2b) involved in the generation of the action potential have been described to date5.
The ECG is the main diagnostic tool; however, the appropriate QTc cutoff is controversial. The prevalence of short QTc pattern in the general population has been evaluated in several studies and there is an intersection between the values found in the general population and in patients with SQTS6. Thus, diagnostic criteria have been suggested in order to increase the accuracy of disease recognition7, considering ECG, medical history, family history and genotype (Table 1). The patient described in this case report scored 4 points, indicating high probability according to the points related to QTc (< 350 ms) and SCD. In 33% of cases, the initial presentation is the SCD and 80% of patients have a personal or family history of SCD8.
Holter monitoring is useful in the prognostic evaluation, due to the documentation of ventricular tachycardia and atrial fibrillation (AF). The role of the EPS in risk stratification still requires further investigation and short refractory periods during programmed stimulation indicate the vulnerability in presenting polymorphic VT/ spontaneous VF. In the follow-up of SQTS patients, polymorphic VT/VF were induced in only 60%9.
The treatment mainstay is the ICD, based on a high percentage of cases showing SCD, even if empirically. In the longitudinal follow-up study of 53 patients, Giustetto et al. found an annual recurrence rate of 4.9% of arrhythmic events.
Furthermore, administration of hydroquinidine showed to be effective to increase the QTc interval and prevent VF. It is also worth mentioning that the presence of early repolarization in patients with SQTS is more prevalent in the general population and shows higher risk of arrhythmic events 10.
The diagnosis of an associated left lateral occult accessory pathway has never been described previously in association with SQTS and there is no description in the literature of SCD by AVT mediated by an accessory pathway of retrograde conduction only, due to the consequent impossibility of producing pre-excited AF. It is noteworthy that patients with SQTS have a high incidence of AF, not detected in this patient. However, it should be considered that in this particular case, the accessory pathway-mediated tachycardia in adrenergic situation may have contributed to the occurrence of SCD.
The increase in HR can promote reduction in ventricular refractory period, enabling the emergence of potentially lethal arrhythmia. The shortening of QT interval by adrenergic stimulation, altering the autonomic balance, has also been described in the literature, in this case probably due to release of catecholamines during exertion. Another possibility is that the accessory pathway is just a physiopathological detail, coincident, but not contributing to the SCD. Moreover, the patient remained asymptomatic after ablation, a fact that sets the AVT as the most likely mechanism responsible for the palpitations.
e39

Case Report
Pavão et al.Short QT Syndrome
Arq Bras Cardiol. 2014; 103(3):e37-e40
1. Modi S, Krahn AD. Sudden cardiac arrest without overt heart disease.Circulation. 2011 Jun 28;123(25):2994-3008.
2. Weaver ED, Robles de Medina EO. Sudden death in patients without structural heart disease J Am Coll Cardiol. 2004;43:1137–1144.
3. Gussak I, Brugada P, et al. Idiopathic short QT interval: a new clinical syndrome? Cardiology. 2000;94(2):99-102.
4. Gaita F, Giustetto C, et al. Short QT Syndrome: a familial cause of sudden death. Circulation. 2003;108(8):965-70.
5. Bellocq C, van Ginneken AC, et al. Mutation in the KCNQ1 gene leading to the short QT-interval syndrome. Circulation. 2004;109(20):2394-7.
6. Kobza R, Roos M, et al. Prevalence of long and short QT in a young population of 41,767 predominantly male Swiss conscripts. Heart rhythm. 2009;6(5):652-7.
7. Gollob MH, Redpath CJ, et al. The short QT syndrome: proposed diagnostic criteria. Journal of the American College of Cardiology. 2011;57(7):802-12.
8. Giustetto C, Schimpf R, et al. Long-term follow-up of patients with short QT syndrome. Journal of the American College of Cardiology. 2011;58(6):587-95.
9. Schimpf R, Bauersfeld U, et al. Short QT syndrome: successful prevention of sudden cardiac death in an adolescent by implantable cardioverter-defibrillator treatment for primary prophylaxis. Heart rhythm. 2005;2(4):416-7.
10. Watanabe H, Makiyama T, et al. High prevalence of early repolarization in short QT syndrome. Heart rhythm . 2010;7(5):647-52.
References
Thus, the case reported here is unique considering the likely association of SQTS with early repolarization pattern and left lateral occult accessory pathway. It should also be noted that the appropriate assessment of ventricular repolarization is of utmost importance for the diagnosis of abnormal repolarization syndromes.
Author contributionsConception and design of the research: Cury-Pavao MLR,
Schmidt A; Acquisition of data: Cury-Pavao MLR, Ono VC, Arfelli E; Writing of the manuscript: Cury-Pavao MLR; Analysis and interpretation of the data: Arfelli E, Schmidt A; Critical revision of the manuscript for intellectual content: Simões MV, Marin-Neto JA, Schmidt A.
Potential Conflict of Interest No potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis study is not associated with any thesis or dissertation work.
e40

Viewpoint
Cylinder Mania in Valvulopathy Back to the FutureMax GrinbergInCor-HC-FMUSP, São Paulo, SP - Brazil
Mailing address: Max Grinberg •Rua Manoel Antonio Pinto, 4 ap. 21A, Paraisópolis. Postal Code 05663-020, São Paulo, SP - BrazilE-mail: [email protected]; [email protected] received January 28, 2014; revised manuscript January 28, 2014; accepted April 29, 2014.
KeywordsHeart Valve Diseases; Stethoscopes / utilization; Heart
Auscultation / trends.
DOI: 10.5935/abc.20140134
I called the instrument a cylinder and experimented ways to build it […] Paris became a center of stetho-acoustic
training [...] cylinder mania spread [...] patients from many countries preferred to be examined by those who were
skilled with the cylinder1.
PreambleThe progressive decreasing glamour of being an expert
restricted the application of cardiac stethoscope auscultation in valvulopathy with excellence (CSAVE).
Brazil preserves groups of “Stethophyllus sp” (STH), rare specimens of cardiologists who form colonies of the CSAVE practice, in environments surrounded by technology all over the place. I am part of this group.
Let’s make it clear: STH is not old-fashioned, CSAVE is not Jurassic, and the stethoscope is not a piece that is missing from the museum. Being a vassal of sovereign clinics, the members of STH believe in the permanence of the stethoscope and in the strong integrating power of the starting point of CSAVE, with the other findings from the multisensorial physical examination, scientific concepts and information from technology2,3.
The members of STH accept that the golden age of the cylinder of Laënnec died with William Bart Osler, about 100 years ago4. But they understand that fidelity should persist. There is no reason to conjecture the fate of CSAVE in the face of Doppler echocardiography similarly, just because cardiac percussion was overcome by the x-ray.
Present from the PastCSAVE is an important inheritance. A possible beginning
for this patrimony was the prophecy by Robert Hooke (1653-1703): “I could clearly hear the human heart beat […], who knows, by the moving sounds of internal organs we may be able to discover the tasks performed in several offices and stores of the human body, and then we acknowledge that the instrument or machine is broken5.”
About one century later, the invention of the stethoscope made it easier to observe that varieties of heart sounds were correlated with anatomic valve peculiarities found post mortem6,7, and they influenced the way the doctor interacted with the patient7.
Laënnec’s cylinder became a symbol of the so called cognitive techniques6. And also of the doctor, since it was a personal object available 24 hours a day, every day. It is portable, light and malleable, and it does not require a special environment, exteriorizing the noisy sound source that the heart becomes due to the occurrence of valvulopathy. Besides, it is not related to guidelines for orientations of application. Books summarized the information, but they did not despise systematizations.
The lack of recent original communications about new heart sounds reveals the depletion of knowledge generation and has “nothing to add” to the semiology utility8,9. The first one took place after the conduction of studies about physiological bases, and there is no prediction of a brand new modality of valvulopathy followed by a yet unknown murmur. The second one is known as: “The starting point is the conduction of anamnesis and complete physical examinations, especially cardiac auscultation10.”
Certain behaviors of clinical reasoning privation throughout anamnesis and physical examination were a result of known alterations in the act of being a doctor and, as a consequence, of being a cardiologist11. In the five generations that currently live together in Brazilian cardiology, it is not difficult to see wide variations in the construction of diagnostic hypotheses pari passu with each fact or collected data.
The hasty documentation, without the use of thought for further analysis, put to an end the concentration and selective focus on each heart sound, patient after patient. As a consequence, the learning curve and the maintenance of skills in propedeutics by hearing were highly immobilized. Besides, the “use manuals”, detailed books about CSAVE, stopped being published decades ago due to the lack of demand, thus leading the knowledge to be restricted to professors and general cardiology books.
A pedagogic premise is cruel: it is impossible to teach what one has not learned. And the domino effect stands out among us: the broken Hippocratic transmission from expert professors, generation after generation of cardiologists. It is a universal phenomenon. In the United States, for instance, the decreasing proficiency in cardiac auscultation brought to light the highly potential damage in the expertise of bedside diagnosis12. However, it is not clear if the uneasiness has brought positive effects8,13.
Explanations for the declining care with CSAVE involve some factors: time, not enough financial compensation and vision of the “outsourced” diagnostic skill for imaging tests, such as the Doppler echocardiography8,13-15.
e41

Viewpoint
GrinbergCylinder mania back to the future
Arq Bras Cardiol. 2014; 103(3):e41-e44
On the other hand, the technological enhancement of the stethoscope, with the objective of bringing progress to the act of teaching by means of the amplification, recording, reproduction, graphic visual and simultaneity of auscultators, is not available for the continuity of the learning process.
It is impossible to deny it, but CSAVE is encouraged by the interest to practice it. The “hearing training” supported in other data that are present in the heart physical examination reproduces what the older doctors did; by being integrated with other available methods, it is an advantage in relation to old school14. Therefore, CSAVE is the bedside guide for “dialogues” with complementary methods.
In the early XXI century, Brazil experiences non-increasing rheumatic heart disease in adolescents, and increasing aortic stenosis among the elderly in outpatient clinics of valvulopathy. The CSAVE provides observational standards to the several age groups. It is one of the reasons why CSAVE was careless and downgraded: a) explanation for data in the anamnesis; b) referral after positive diagnoses; c) alert for valvulopathy, which was unknown up until then. Besides, the lack of attention with heart sounds abbreviates the cozy and pro-therapeutic doctor-patient connection9,15-17.
The STHThe STH may analyze diagnoses fast, completely,
with high specificity, excellent cost-benefit relationship and personal satisfaction – for instance, the important insufficiency of the mitral valve caused by the rupture of the chordae tendineae. They do not need much propedeutic action to explain acute and severe heart failure, or to conjecture etiopathogenic therapy.
STH is not nostalgic. They see the benefit renewed in the propedeutic patrimony built by remarkable masters of semiotics3, many of whom were immortalized as eponymous and transformed in metonymy (I auscultated Austin Flint, Rivero Carvallo disappeared, Gallavardin cleared it up).
STH emphasizes that CSAVE may have a relevant role in the application of innovations. In the 1980s, the appearance of a systolic murmur during a sequence of dilations in mitral valvuloplasty by a balloon cathether began to mark therapeutic conclusion, in order to avoid the development of acute mitral insufficiency with the desire to maximize the mitral valve area.
However, the STH recognizes that technological modernity dismisses certain stages of classic CSAVE, and it also eliminates them from teaching programs. It is the case of quantifying the period of time between the second sound and the mitral opening snap – 0.04-0.10 s –, as the level of left atrial hypertension and, ipso facto, the severity of mitral stenosis.
With this concept, and being aware of the limitations of capturing sounds and the silence of form morphologies, such as thrombi and vegetation, the STH works for the security of making a statement concerning rare dissociations of information. An example of this ethical commitment to “revise” technology is the reasoning about the chances of identifying if a discrete valvular regurgitation with Doppler, not auscultated by the doctor, is real or false positive.
An Essential MatterIt is worth to ask: STH, what is the current role of CSAVE
in the diagnosis of valvular lesion in Brazil (by considering the use of a conventional stethoscope)?
The STH member who makes “valves”, especially the one who associates teaching duties, will answer with a categorical ‘indispensable’. Of course, he knows their numbers are not high in cardiology, but he will justify that, in order to give a solid nucleus to the diagnosis, CSAVE is not a complementary test or a superfluous one to admit options of application level. Technology is not an enemy of CSAVE, the only concern lies upon its poor use18.
STH will take the time to be solidary and available for colleagues who might even be outside the island, however, who would respond similarly to them, talking about reasons for which they do not have the expertise or how they lost it due to lack of use. But they will be reductionist if the argument is the work overload, which sacrifices the effort of the cardiologist for CSAVE.
There are many devil’s advocates outside the islands. They publicize that CSAVE defends the “excuses” caused by imprecisions with individual variations and acoustic window effects15; that it is a luxury for only a few, and a waste of time for many, and that there is more quality in quantitative and hemodynamic information in other methods8,13.
Due to the opinions about downgrading the hierarchy of CSAVE, the STH reminds us that it is complex to attribute causes to a “non-auscultation” or a “weird auscultation”, and that the unusual and the aphonic will not stop existing. It reinforces the motto of professionalism from STH: good auscultation, better diagnosis.
The subjectivism about veracity and falsehood of CSAVE may be criticizable; however, it has always accompanied the state of the art. The fact that CSAVE was originated by truly positive isolated cases is historical, and was developed based on the observance of the low chances of false negatives in small similar groups of patients; the references were necropsy, cardiac catheterism and phonomechanocardiography.
Obstacles to conjectures of randomized, double-blind and multicenter studies maintain the high observational focus on the islands – it is worth to remember that Austin Flint (1812-1886) became famous for observing two cases, and José Manuel Rivero Carvallo (1905-1993) reported 11 cases, being 10 positive ones.
A few studies, also because of etiopathogeny-variety biases and diverse patterns of reference as to level of severity8,13,19, did not provide results for the construction of evidence. How to translate the murmur sensitivity of Austin Flint, ranging from 0-50% for moderate discrete aortic insufficiency, and from 52-100% for moderate to important aortic insufficiency?19
On the other hand, CSAVE presents high sensitivity and high specificity for the identification of asymptomatic patients with valvulopathy with the purposes of check-up, release for surgical procedures, admission for work and planning sports activities20.
e42

Viewpoint
GrinbergCylinder mania back to the future
Arq Bras Cardiol. 2014; 103(3):e41-e44
1. Grinberg M. Laënnec e o estetoscópio. Símbolos da clínica moderna. Arq Bras Cardiol. 1995;65(1):65-72.
2. Lembo NJ, Dell´Italia LJ, Crawford MH, O’Rourke RA. Bedside diagnosis of systolic murmurs. N Engl J Med. 1988;318(24):1572-8.
3. Rappaport MB, Sprague HB. Physiologic and physical laws that govern auscultation and their clinical application: the acoustic stethoscope and the electrical amplifying stethoscope and stethosgraph. Am Heart J. 1941;21:257-318.
4. Markel H. The stethoscope and the art of listening . N Engl J Med. 2006;354(6):551-3.
5. McKusick VA, Sharpe WD, Warner AO. An exhibition oh the history of cardiovascular sound including the evolution of the sthetoscope. Bull Hist Med. 1957;31(5):463-87.
6. Leatham A. Auscultation of the heart. Lancet. 1958;272(7050):757-66.
7. Reynolds HY. President’s address: R.T.H. Laënnec, M.D.--clinicopathologic observations using the sthetoscope, made chest Medicine more scientific. Trans Am Clin Climatol Assoc. 2004;115:1-29.
8. Vukanovic-Criley JM, Criley S, Warde CM, Boker JR, Guevara-Matheus L, Churchill WH et al. Competency in cardiac examination skills in medical students, trainees, physicians and faculty: a multicenter study. Arch Intern Med. 2006;166(6):610-6.
9. Hanna IR, Silverman ME. A history of cardiac auscultation and some of its contributors. Am J Cardiol. 2002;90(3):259-67.
10. Tarasoutchi F, Montera MW, Grinberg M, Barbosa MR, Piñeiro DJ, Sánchez CR, et al. Diretriz brasileira de valvopatias. SBC 2011 / I Diretriz Interamericana de Valvopatias - SIAC 2011. Arq Bras Cardiol. 2011;97(5 supl. 3):1-67.
11. Fred HL. Hyposkillia: deficiency of clinical skills. Tex Heart Inst J. 2005;32(3):255-7.
12. Mangione S, Nieman LZ, Gracely E, Kaye D. The teaching and practice of cardiac auscultation during internal Medicine and cardiology training: A Nationwide Survey. Ann Intern Med. 1993;119(1):47-54.
13. Mangione S, Nieman LZ. Cardiac auscultation skills of internal medicine and family practice trainees: a comparison of diagnostic proficiency. JAMA. 1997;278(9):712-22.
References
The routine that “pleases” STH rejuvenates CSAVE. Joviality, on the one hand, is a magnet for the iron will of youth towards good cardiology practices. The attraction has taken promising steps.
PerspectivesSTH is hopeful. It has reasons to believe in the celebrations of
the bi-centenary of the invention of the stethoscope, which will take place in 2016, besides registering a historical reverence to the period between two creative figures: the Breton doctor Réné Théophile Hyacinte Laënnec (1721-1826) and the cardiologist David Littmann (1906-1981), from Harvard Medical School. The STH predicts space to celebrate the fact that CSAVE has reconquered the young strength of being a doctor in Brazil.
We can retake something that has been taken from us, as taught by Lucius Anneus Seneca (4 BC-AD 65). In medicine, the Hippocratic atavism provides it. The STH feels the wind moving towards favorable directions, moving the perception that existing as a doctor requires studying, in order to extract alone the highest possible number of data from the patient. Young students in university or in postgraduate programs seize the opportunity of the optional internship and take part in the STH.
Between March, 2012, and December, 2013, for instance, the expressive number of 175 young people, among students and interns coming from 70% of the Brazilian states, attended ad libitum a busy university community of STH, for tertiary care to patients with valvulopathy.
It is known that motivation clears the senses, and that long lasting dedication elevates self-esteem. It became clear that such a combination had the ability to waken in the apprentices of STH, after each lesson learned by their own senses, the will to reach the maximum level of sound capture, to analyze the patient further, to go through focuses, to look for positions, to make maneuvers and to be eager to have a STH ear – master to discover what is inaudible or to clarify what has been auscultated.
Brazil has the advantages of prospecting and polishing the several semiotic jewels in valvulopathy “straight from the
source”, and not from cold mannequins with recorders. The real circumstances of each examination provoke facilitating points of reference, which reinforce retention and memory. Therefore, it is natural to accumulate sound quality to present the normality or the abnormality of cardiac rhythm, the opening (mitral opening snap, Austin Flint murmur) and the closure of valves (first and second sounds), ventricular filling (third and fourth sounds), atrioventricular flow, ejection and regurgitation (characteristic murmurs, snaps, Valsalva and Rivero-Carvallo maneuvers), atrial contraction (presystolic accentuation) and inflammation (pericardial friction, Carey Coombs murmur, continuous murmur in the fistula due to infectious endocarditis).
I wish each one of these young students – and many more – could become a multiplier. That their stethoscopes could work as a real metaphor of the art of medicine and science18. It is the Hippocratic contribution of STH for the rebirth of CSAVE in Brazil. It will be cylinder mania back to the future!
Author contributionsConception and design of the research, Acquisition of
data, Writing of the manuscript and Critical revision of the manuscript for intellectual content: Grinberg M.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any thesis or dissertation work.
e43

Viewpoint
GrinbergCylinder mania back to the future
Arq Bras Cardiol. 2014; 103(3):e41-e44
14. Tavel ME. Cardiac auscultation: a glorious past and it does have a future! Circulation. 2006;113(9):1255-9.
15. Craige E. Should auscultation be rehabil i tated? N Engl J Med. 1988;318(24):1611-3.
16. Sackett DL. The rational clinical examination: a primer on the precision and accuracy of the clinical examination. JAMA. 1992;267(19):2638-44.
17. Sackett DL, Rennie D. The science of the art of the clinical examination [Editorial.] JAMA. 1992;267(19):2650-2.
18. Mangione S. The stethoscope as a metaphor. Cleve Clin J Med. 2012;79(8):545-6.
19. Babu AN, Kymes SM, Carpenter Fryer SM. Eponyms and the diagnosis of aortic regurgitation: what says the evidence? Ann Intern Med. 2003;138(9):736-42.
20. Roldan CA, Shively BK, Crawford MH. Value of the cardiovascular physical examination for detecting valvular heart disease in asymptomatic subjects. Am J Cardiol. 1996;77:1327-31.
e44